Embed Size (px)
Citation preview

Application of the Onion model to assess
the extent of missing tuberculosis cases
by the National Programmes
Dr Amal Bassili
Stop TB unit, WHO, Regional Office for the Eastern Mediterranean
Surveillance Workshop
Cairo Sheraton
Cairo, Egypt, 27-29 October, 2009
2/3/2010 1

Background
• In 2007, the estimated number of smear positive
pulmonary tuberculosis was 259,885 cases while
the notified number of cases was 155, 481
• The Region achieved a case detection rate (CDR)
of 60% and did not achieve the global target of
70%
• This would mean that as many as 103,954 smear
positive TB patients (i.e. 40% of the total) may
not have had access to appropriate TB care
2/3/2010 2

Background: Causes of low case
detection
• Suboptimal quality of TB care: for example,
– laboratory diagnosis is not always extensive or accurate.
– Management of TB suspects is not yet well established.
– Health care providers in public and private sectors are not fully involved.
– Complex emergencies are affecting TB care in countries particularly those with a high burden of TB.
– Awareness of TB is not always high in the community, and TB is often heavily stigmatized.
– the care-seeking behavior of patients and the health systems responses are extremely dynamic and complex, and do not follow any stereotyped patterns.
2/3/2010 3

Methodology of the guide • A guide with a stepwise approach was developed aiming at
evaluating the efficiency of case finding activities.
• This guide was tested and then used in several programme review missions in the countries of the EMR. The approach is based on the patient’s pathway to care from the community to the diagnostic and treatment centres for TB.
• The below hypothetical Onion-shaped model depicts this approach. Each layer of this “Onion” describes one step taken by the patient, from outer-most layer to inner-most layer, in the pathway to care and also indicates the relevant programmatic activities according to the Stop TB strategy.
2/3/2010 4

2/3/2010 5
Diagnosed & reported
cases by TBMU
Step 1: ACSM
Step 2: Public-Private mix, Suspect management
Step 3: Public-Public mix, Suspect management
Step 4: Suspect management
Step 5:Laboratory diagnosis
Step 6:DOT with Treatment supportMonitoring and Evaluation Drug managementContact managementHIV/TBMDR-TB
Undetected cases at
laboratory of TBMU
Undetected cases at out-
patient units of TBMU
Undetected cases at
public health facilities
Undetected cases at
private health facilities
Undetected TB cases
in community
Estimated
TB incidence
Onion model to detect the undetected TB cases

Methodology of the guide • In order to measure the performance of activities in
the layers of the model, a set of indicators was developed for each layer of the model
• All the indicators were reported in the WHO compendium of indicators.
• Several sources were used to collect the necessary data: – Global TB Data Collection Form of WHO,
– programme review mission reports,
– countries’ reports,
– operational research studies, and
– the web-based quarterly reporting system from the countries of the Region to the WHO EMRO, the “EMRO DOTS Quarterly online (DQ online).”
2/3/2010 6

Methodology of the guide
– For each step, the recommended level (target)
was in principle defined and the performance of
the indicator was evaluated using a 4-point Likert
scale (1 worst and 4 best)
– If the indicator could not be evaluated due to lack
of information or due to the absence of the
related activities, a “zero” score was given.
2/3/2010 7

Methodology of the guide • All the indicators were given the same weight except the following:
– TB suspect register coverage, and the treatment success rate. These were given double weight.
• a good coverage of suspect register in the TBMUs and PHCs enhances timely identification of TB suspects at their first point of care in the health system.
• successful treatment is the most effective measure to control the disease. While this indicator is not implicated in the case finding process, it is strongly correlated with the programme performance .
– The sale of anti-TB drugs in private pharmacies was given a triple weight, provided it is supported by evidence. Experience has shown that, whenever the sale of anti-TB drugs is banned in the private pharmacies, the non-NTP providers refer their diagnosed cases to be treated at the NTP.
• This situation proved to be the most effective intervention to detect almost all cases in the country, especially, in the presence of good community accessibility to public health services.
2/3/2010

Methodology of the guide
• The percentage summation score for each component and all the components was calculated as follows: (Sum of scores obtained/Maximum scores that could be
obtained) X 100.
• Then the percentage summation score of the studied component and all the components was expressed as falling between 0 and 100%, with the highest percentage reflecting a better performance related to that component.
• The 95% confidence interval (CI) around the proportion was calculated. Data analysis was performed using excel.
2/3/2010 9

Application of the methodology
The model with its indicators was applied in 3
countries of the Region:
Jordan, Syria and North Sudan
2/3/2010 10

1. ACSM
Indicators
Target Measurement Wt Score
1
Score 2 Score 3 Score 4
Use of TV, radio,
print media as
communication
tool
To become the
source of
information for
the community
No. of TV or radio
announcements, or
printed media
1 None printed
materials
Additiona
l media
activities
Full strategy
implemented
Knowledge about
TB among TB
patients and
community
Improved over
time
Proportion of
individuals with
correct knowledge
about TB
1 <25% 25-50% 50-75% >75%
Level of stigma
related to TB
among TB
patients and
community
Reduced over
time
Mean percent score of
stigma related to TB
1 >75% 50-75% 25-50% <25%
Patient delay Reduced over
time (target 2
weeks)
Duration between the
onset of symptoms and
their first visit to
health facilities
1 Mean
≥≥≥≥60day
s
Mean
31-60
days
Mean
14-30
days
≤≤≤≤2 weeks
First care-seeking
behavior of
patients
TB centres
(TBMUs or
PHCs)
Proportion of patients
that visited TB centres
1 <25% 25-50% 50-75% >75%
Civil society
engagement
Increased over
time
% of patients
supported by NGO
1 0-25% 25-50% 50-75% >75%
2/3/2010 11

Indicators Jordan
2007-2008
Score Syria
2007-2008
Score North Sudan
2007-2008
Score
Use of TV, radio, print
media as communication
tool
Limited to printed
materials
2 Limited to
printed
materials
2 Limited to
printed
materials
2
Knowledge about TB
among TB patients and
community
79% of TB suspects in
the community had
adequate knowledge
about TB
4 61% of patients
had adequate
knowledge
about TB.
3 50.5% had
adequate
knowledge
about the
disease
3
Level of stigma related to
TB among TB patients
and community
Mean percent score 71%
for TB suspects in the
community
2 High among
patients but not
yet studied in
the community
2 The average
score of stigma
in the
community was
54.7% in 2008
2
Patient delay (duration
between onset of
symptoms till their first
visit)
Mean of 7.4(3.9) days for
TB suspects in the
community
4 -Mean
(SD)=80.4(79.0)
1 69.7(28.1) in
2006
1
First health seeking
behavior of patients
Public health centres for
92% of the community
living at >30 km from the
TB centre, followed by
the private sector
4 Public health
centres for 21%
of patients
1 Public health
centres for 90%
of community
4
Civil society engagement
(% of patients supported
by NGOs)
>75% 4 25-50% 2 <25% 1
2/3/2010 12

2-3 PPM
Indicators
Target Measurement Weight Score 1 Score 2 Score 3 Score 4
Presence of PPM
focal person, task
force and
guidelines
Yes Present or not 1 None Focal
point
Focal
point and
guidelines
Focal
point, task
force and
guidelines
Non-NTP facilities
engaged out of
planned
100% No. of non-NTP health
facilities participating in
TB care (DOTS) / Total no.
of targeted (X100)
1 0-25% 25-50% 50-75% >75%
% of suspects
referred from
private and public
non-NTP sector
Increase
over time
No. of suspects referred
from non-NTP providers /
total number of suspects
identified by NTP(X100)
1 0-10% 10-25% 25-50% >50%
% of TB cases
detected by public
and private non-
NTP provider
Increase
over time
Number of TB cases
detected by non-NTP
providers/total number of
cases (X100)
1 0-10% 10-25% 25-50% >50%
Sale of TB Drugs
in private
pharmacies
No Extent of sale of anti-TB
drugs in private pharmacies
3 >50% of
population
25-50% of
population
5-25% of
population
No or
negligible
(<5%)
No. of training
sessions for PPM
out of planned
100% No. of training sessions /
total planned (X100)
1 0-25% 25-50% 50-75% >75%2/3/2010 13

Indicators Jordan
2007-2008
Score Syria
2007-2008
Score Sudan
2007-2008
Score
Presence of PPM focal
person or task force and
guidelines
Yes 4 Yes 4 Yes, newly
appointed,
guidelines
developed in 2009
1
Non-NTP facilities
engaged out of planned
100% 4 1160 out of a total of
1540 public health
facilities (75%). All the
162 (100%) private health
facilities are engaged.
4.00 184 out of a total of
443 public health
facilities (41.5%).
The private sector
engaged is
negligible.
2
% of suspects referred
from public and private
sector
58% 4 6858 out of a total of
12,498 suspects (54.9%)
were referred from public
and private non-NTP
providers
4.00 Data not available 0
% of TB cases detected
by public and private
non-NTP providers
66% 4 66% from private and
19% from public
4.00 4% from public
sector and none
from the private
sector
1
Sale of TB Drugs in
private pharmacies
None 12 None 12 Yes 3
No. of training sessions
and trained personnel
for PPM
<25% of
planned
1 <25% of planned 1 <25% of planned 1
2/3/2010 14

4 Suspect
management
Indicators
Target Measurement Weight Score 1 Score 2 Score 3 Score 4
% of suspects that
have had sputum
smear examination
100% No. of suspects who
had their sputum
examined at
laboratory / No. of
suspects identified
at outpatient units
(X100)
1 <75% 75-90% 90-95% >95%
% of suspects
diagnosed as sputum
smear positive TB
≈≈≈≈10% No. of suspects with
positive smears /
total no. of
suspects(X100)
1 >20% 15-20% >10-15% ≤≤≤≤10%
TB suspect register
coverage in the
outpatient
departments (TBMUs
and PHCs) (or PAL
coverage including
the use of suspect
register)
100% No. of outpatient
departments
(TBMUs and PHCs)
with suspect
registers / all
outpatient
departments (X100)
2 0-25% 25-50% 50-75% >75%
2/3/2010 15

Indicators Jordan
2007-2008
Score Syria
2007-2008
Score Sudan
2007-2008
Score
% of suspects that have
had sputum smear
examination
100% 4 95% 4 NA 0
% of suspects
diagnosed as sputum
smear positive TB
5.1% 4 7% 4 NA 0
% of health facilities
with TB suspect
register (TBMUs and
PHCs) /PAL activity
coverage including
suspect register
100% 8 in TBMUs only 6 None 0
2/3/2010 16

5 Laboratory
Indicators
Target Measurement Weigh
t
Score 1 Score 2 Score 3 Score 4
Size of population per
functioning diagnostic
laboratory
(microscopy)
1 lab
per 50-
250,000
populat
ion
Total population / No.
of functioning
diagnostic laboratories
1 1 lab per
>550,000
pop
1 lab per
300,000-
550,000
pop
1 lab per
250,000-
300,000
pop
1 lab per
<250,000
population
Extent of EQA
coverage for direct
smear microscopy
100% No. of diagnostic units
submitting slides for
EQA / Total no. of
diagnostic units (X100)
1 <50% 50-75% 75-99% 100%
Proportion of
microscopy
laboratories that
failed to show
adequate performance
0% No. of laboratories
that reported major
error (high false
positive (HFP) or high
false negative (HFN)) /
No. of laboratories
covered by the EQA
system (X100)
1 >10% 5-10% 1-5% 0%
2/3/201017

5 Laboratory
Indicators
Target Measurement Weigh
t
Score 1 Score 2 Score 3 Score 4
Proportion of lab
personnel trained out
of planned
100%
% of lab personnel
trained
out of planned
1 <50% 50-75% 75-99% 100%
% of supervisory
visits with feedback
reports to lab out of
planned
100% No. of supervisory
visits conducted / No.
of supervisory visits
planned (X100)
1 <50% 50-75% 75-99% 100%
Primary defaulter rate 0% No. of SS+ cases
detected at laboratory)
– (No. of smear
positive TB cases
registered for
treatment) / No of SS+
cases detected at
laboratory (X100)
1 >10% 5-10% 1-5% 0%
Proportion of smear
positive cases among
all pulmonary TB
cases
60-70% No. of smear positive
TB cases / No. of all
pulmonary TB cases
(X100)
1 <40% 40-50% 50-60% >60%
2/3/201018

Indicators Jordan
2007-2008
Score Syria
2007-2008
Score Sudan
2007-2008
Score
Laboratory network coverage:
Number of population per
functioning diagnostic
laboratory (microscopy)
1 per 39,000 4 1 per
300,000 pop
3 1 lab per
120,372
population
4
Extent of EQA coverage for
direct smear microscopy
8% 1 14/65
(21.5%)
1 53% 2
Proportion of microscopy
laboratories that failed to
show adequate performance
0% 4 22% in 2008 1 60% 1
% of lab personnel trained out
of planned
50-75% 2 88% 3 <50% 1
% of laboratories supervisory
visits with feedback report
50-75% 2 80% 3 Inadequate
(less than
1/lab/year)
1
Primary defaulter rate 0% 4 0% 4 Up to 50%
in some
centres
1
Proportion of smear positive
cases among all pulmonary TB
cases
71% 4 62% 4 55.1% 3
2/3/2010 19

6 Quality of NTP
surveillance and case
management
Target Measurement Weight Score 1 Score 2 Score 3 Score
4
Report completeness 100% Number of submitted
reports from
TBMU/number of
expected reports (X100)
1 <50% 50-
75%
75-
99%
100%
Direct observation of
treatment (DOT)
100% No. of patients daily
supervised during the
entire treatment
period/ total no. of
cases treated(X100)
1 <50% 50-
75%
75-
99%
100%
Adherence to
standardized
treatment regimens
100% No. of cases treated
with correct treatment
regimens / Total no. of
cases eligible to the
regimen (X100)
1 <50% 50-
75%
75-
99%
100%
Treatment success
rate
>85% No. of smear positive
TB patients successfully
treated / No. of patients
registered (X100)
2 <75% 75-
80%
80-
85%
>85%
% of annual
supervisory visits with
feedback reports out
of planned at all levels
100% No. of supervisory visits
with feedback reports
at all levels/total No. of
planned visits at all
levels(X100)
1 <50% 50-
75%
75-
99%
100%
2/3/201020

6 Quality of NTP
surveillance and case
management
Target Measurement Wt Score 1 Score 2 Score 3 Score
4
% household contact
evaluated for TB (all
ages)
100% No. of household
contacts evaluated for
TB/ total No. of
household contacts
(X100)
1 <50% 50-75% >75-
95%
95-100%
% household contact
evaluated for TB
(under 5 years of age)
100% No. of household
contacts under 5
evaluated for TB/ total
No. of household
contacts under 5 years of
age
1 <50% 50-75% >75-
95%
95-100%
No. & % of household
contacts given INH
preventive therapy
(under 5 years of age)
100% No. of under 5 years old
household contacts given
INH preventive therapy /
No of under 5 years old
household contacts
(X100)
1 <50% 50-75% >75-
95%
95-100%
No and % of TB
patients tested for
HIV
Yes No of TB patients tested
for HIV/ total no. of TB
patients (X100)
1 <50% 50-75% >75-
95%
95-100%
% of TB patients
subjected to drug
susceptibility testing
(DST) out of eligible
ones
100% No of TB patients DST
tested /total no. of
eligible TB patients
(X100)
1 <50% 50-75% >75-
95%
95-100%
2/3/2010 21

Indicators Jordan
2007-2008
Score Syria
2007-2008
Score Sudan
2007-2008
Score
Report completeness 100% 4 70% in 2007 2 92.5% in 2007 3.00
Treatment supervision
& support
DOT in place 4 DOT in place 4 DOT is rarely
implemented
1
Adherence to
standardized treatment
regimens
Yes 4 Yes 4 Yes 4
Treatment success rate 71% 2 86% 8 81% 6
%of annual supervisory
visits with feedback
reports out of planned
from central to
intermediate and from
intermediate to
peripheral levels
75-99% 3 75-99% 3 Only 7 states
out of 15 were
subjected to
one supervisory
visit per year
from central
level
2
2/3/2010 22

Indicators Jordan
2007-2008
Score Syria
2007-2008
Score Sudan
2007-2008
Score
% household contact evaluated for
TB (all ages)
96-100% 4 42% 1 NA 0
% household contact evaluated for
TB (under 5 years of age)
NA 0 NA 0 NA 0
No. & % of household contacts given
INH preventive therapy (under 5
years of age)
100% 4 135/396
(34%)
1 Not in place 0
No and % of TB patients tested for
HIV
100% 4 14 1 671 in Q3,
2008, in 8
states out of
15 only
1
% of TB patients DST tested out of
eligible ones
100% 4 100% 4 None 0
% of MDR-TB under treatment 100% 4 23/41 (56%
in 2008)
2 None 0
2/3/2010 23

Summary table on the implementation of the Stop TB
strategy in the different countries
Components
(Domains)
No of
indicators
%
weightMax
score
Jordan Syria
N
Sudan
Score % Score % Score %
ACSM 6 18 24 20 83 13 54 13 54
PPM 6 18 32 29 91 29 91 9 28
Suspect
management 3 9 16 16 100 14 88 0 0
Laboratory
network 7 21 28 21 75 17 61 13 46
Treatment
and quality
of NTP
surveillance 11 33 48 39 81 31 65 17 35
Total 33 100 148 125 84 104 70 52 35
95% CI
(78-
91%)
(61-
79%)
(22-
48%)2/3/2010
24

2/3/2010 25
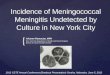
Correlation between CDR and Summation Score in 9 EMR countries
% summation score
9080706050403020100
CD
R (
%)
110
100
90
80
70
60
50
40
30
20
10
0
Yemen
syria
Pakistan
Oman
N Sudan
Jordan
Iran
Egypt
Afghanis
Rsq = 0.6162

2/3/2010 26

2/3/2010 27
Descriptive Statistics
70.3333 18.5135 9
58.1111 15.6800 9
CDR
SCORE
Mean Std. Deviation N
Correlations
1.000 .731*
. .025
9 9
.731* 1.000
.025 .
9 9
Pearson Correlation
Sig. (2-tailed)
N
Pearson Correlation
Sig. (2-tailed)
N
CDR
SCORE
CDR SCORE
Correlation is significant at the 0.05 level (2-tailed).*.

2/3/2010 28
TB notification rate (per 100 000 population)
0
2
4
6
8
10
12
14
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
New and relapse New smear-positive
Trend in TB notification in Jordan

2/3/2010 29
TB notification rate (per 100 000 population)
0
5
10
15
20
25
30
35
40
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
New and relapse New smear-positive
Trend in TB notification in Syria

2/3/2010 30
TB notification rate (per 100 000 population)
0
10
20
30
40
50
60
70
80
90
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
New and relapse New smear-positive
Trend in TB notification in North Sudan

Interpretation of the model• The national TB control programmes are encouraged to use
this model to evaluate the case finding processes in their countries and identify areas of weaknesses which should be targeted in future interventions.
• The summary table shows that the NTP performance scores in Jordan and Syria were 84% and 70%, respectively. This is consistent with the Case Detection rate these countries that exceeded 70% in 2007 , with the quality of their surveillance system and with the smooth annual decline (almost plateau phase) in their notifications
• Similarly, Sudan NTP reported a percent summation score of 35%, which is also consistent with the low Case detection rate of 31% in 2007, and with the increase in the annual trend of the disease due to inadequate TB control .
2/3/2010 31

Conclusion
• Countries are advised to use this tool to evaluate whether the situation is consistent with the case detection rate estimated for the country.
• For instance, if the evaluation showed that few gaps were identified while the estimated case detection rate is very low, they would conclude that the country case detection rate needs to be revisited. In such situation, it is recommended to approach WHO with the collected evidence to obtain the necessary technical assistance in carrying out one of the WHO recommended methods to estimate TB incidence in order to revisit the case detection rate and TB burden in that country.
2/3/2010 32