Embed Size (px)
Citation preview

APPENDIX K
DEPARTMENTAL QUALITY ASSURANCE PROCEDURES
RADIATION ONCOLOGY
PAGE
PROSTRATE BRACHYTHERAPY PRESCRIPTION................................. 205
CALIBRATION CHECK OF THERAGENICS Pd-103 SEEDS........................ 206
PROCEDURE FOR SEED HANDLING.......................................... 207-208
PROCEDURE FOR DAY OF IMPLANT ........................................ 209-211
PROCEDURE FOR DAY FOLLOWING IMPLANT ................................. 212-213
HDR TREATMENT RECORD AND PRESCRIPTION FORM HDR-100................... 214
NUCLETRON OPERATING PROCEDURES ...................................... 215 HDR Ir-192 SOURCE EXCHANGE AND CALIBRATION PROCEDURES................ 216-217
NUCLETRON HDR PATIENT TREATMENT CHECKS............................... 218
INTRACAVITARY BRACHYTHERAPY PRESCRIPTION............................. 219
BRACHYTHERAPY AND RADIOPHARMACEUTICAL TREATMENT...................... 220
CESIUM THERAPY RECORD ............................................... 221
PATIENT ROOM SURVEY ................................................. 222
CESIUM WARD RECEIPT ................................................. 223
NURSING PRECAUTIONS FOR PATIENTS RECEIVING BRACHYTHERAPY............. 224
BRACHYTHERAPY SUMMARY SHEET ......................................... 225
CHECKLIST FOR MEDICAL APPLICATION OF HDR............................. 226-231
ONCOLOGY RADIOACTIVE MATERIAL INSPECTION SHEET....................... 232-235
204

Medical University of South CarolinaRadiation Oncology Department
Permanent Implant: Prostrate Brachytherapy Prescription
Name: ______________________ Birth Date: ____________ SS#: ______________________Rad Onc # ___________________ Rad Oncol.: ___________ Ref. Phys. _________________Primary Site: ________________ Isotope: ______________ Date of Implant: ____________
Treatment Plan:
Radionuclide: ____________________
Number of sources (seeds): _______________________
Source strength: ____________ mCi per seed
Treatment Site: _____ Prostrate, _____ other
Dosimetric Objective: ______ Gy to _____ of PTV
MD Signature _______________________ Date: ______________
Oral Revision:
Oral revision of Treatment Plan _______ (C heck if applicable).
Description of Revision:______________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
Documented By: ________________________
Final Treatment:
Date: ____________ Patient Identified by two methods: ______ name, ______ DOB, ______ SS#
Radionuclide: _________________________
Number of sources (seeds): _________________________
Source Strength at Loading ______________mCi per seed
Treatment Site: _____ Prostrate, _____ other
Number of seeds recovered in Cysto: _________________________
Total # of seeds Implanted: _________________________
MD Signature _____________________ Date: ______________
205

Medical University of South CarolinaRadiation Oncology Department
CALIBRATION CHECK OF THERAGENICS Pd-103 SEEDS
DATE: RO#: P.O.#:
PATIENT: IMPLANT DATE: DR: Milito
MANUFACTURER: Theragenics Corp. LOT#: MODEL: 200
MANUFAC TURER � S CALIBRATION DATE: AT 12:00 EST.
NO. OF SEEDS:
ACTIVITY/SEED: mCi on (Manufacturer � s value)
TOTAL ACTIVITY: mCi on (Manufacturer � s value)
ELAPSED DAYS DECAY FACTOR
TOTAL ACTIVITY: mCi on (Manufacturer � s value)ACTIVITY/SEED: mCi on (Manufacturer � s value)
Activity was measured using C NMC AtomLab 44 E Brachythera py Programm able Electrometer with
CNM C Model 44D R e-entrant Ionization Chamber calibrated 10/7/99 by K&S Associates ADCL using seed holder
with narrowed tip for seed - red scribe set to top of � holder clamp � .
Seed # RdgPd-103
Setting ***
CalibrationFactor*
(mCi/Rdg)
Calc.Activity(mCi)
CalibrationFactor
(Pd-103)**
Calc.Activity(mCi)
PercentError
%
1 1.005 0.7752 #DIV/0!
2 1.005 0.7752 #DIV/0!
3 1.005 0.7752 #DIV/0!
4 1.005 0.7752 #DIV/0!
5 1.005 0.7752 #DIV/0!
6 1.005 0.7752 #DIV/0!
7 1.005 0.7752 #DIV/0!
8 1.005 0.7752 #DIV/0!
9 1.005 0.7752 #DIV/0!
10 1.005 0.7752 #DIV/0!
11 1.005 0.7752 #DIV/0!
12 1.005 0.7752 #DIV/0!
13 1.005 0.7752 #DIV/0!
14 1.005 0.7752 #DIV/0!
15 1.005 0.7752 #DIV/0!
SUM:
AVG #DIV/0! #DIV/0!
%STD: #DIV/0!
*NEW CHAMBER CALIBRATION FACTOR ON 10/7/99 by K&S Associates ADCL**Using Manufacturer �s Pd-103 calibration factor (divide by 1.29 to get manufacturer �s value)***per Larry Bryson. K&S Associates ADCL
CHECKED BY: ____________________________ DATE: __________________
APPROVED BY: ____________________________ DATE: __________________
206

Medical University of South CarolinaRadiation Oncology Department
PROCEDURE FOR SEED HANDLING
1. Upon Receipt of Seeds from Radiation Safety:
A. Seeds must be counted and calibrated.
1. Recommended counting seeds to an intermediate container in groups of tens inorder to reduce the number of seeds in any group that must be recounted in case oferror or confusion. Do all counting on the Plexiglas tray provided. Place everytenth seed into the calibrator and count.
2. A minimum of least 10 seeds must be placed in the calibrator and calibrated oneat a time.
2. Preparation of Loading Seeds into Needles:
A. The Plexiglas tray located in the 250 Room should be placed on the short counter to theright of the door as you enter the 250 Room.
1. Open a pillow case on the tray to provide a light-colored resilient surface to workon.
a. Seeds have a tendency to � skitter � when they fall on a hard smoothsurface.
2. Assemble and arrange the vacuum-assisted seed loader on the working tray withthe pump on your strong side (right-handedness Vs. left-handedness). The powerdistribution cord and switch should be on the side nearest the door for easy accessby the person helping to count.
3. The following instruments should be at hand:
a. Special seed handling forcepsb. Special seed handling hemostatc. Modified sponge forceps (11-inch)d. Modified curved forceps (11-inch)e. Metal rulerf. Spare pigg. Stainless steel bowl (3-inch)h. Slip shield set with wrenchi. Eberline G-M counter with pancake probe
4. The following materials are needed:
a. The appropriate number of needles as determined by the computer-generated plan supplied by the physician or physicist plus one unopenedpackage of 5 needles.
207
Medical University of South CarolinaRadiation Oncology Department
PROCEDURE FOR SEED HANDLING CONT.
b. 5 mm catgut spacers (minimum of one spacer per seed)c. One (1) package of bone wax
B. Position needles with stylets in place into the slip shields.
1. Seat the needles all the way to the cap of the slip shield being carefulNOT to damage the point of the needle.
2. Tighten the set screw on the slip shield with the allen wrench provided.
a. DO NOT OVER-TIGHTEN!
3. Mark the slip shield with the number of seeds it is to contain.
C. Load needles with the vacuum-assisted seed loader in accordance with the manufacturer �sinstructions. The needle is loaded from the sharo end.
1. Each seed placed into the needle must be preceded by a spacer.
a. A three seed needle would have a spacer-seed (1)-spacer-seed (2)-spacer-seed (3).Always begin with a spacer and end with a seed!
2. Two persons must be present to count and verify seed loading.
3. Seal each loaded needle with bone wax by pushing needle through bone wax,giving a slight twist. Remove and replace slip shield cover.
4. Use caution and be gentle when replacing stylets.
a. If bone wax is pushed out, then the needle must be reloaded.
5. Place the completed needle with slip shield cover into the carrier.
a. Whenever possible the individual tilting blocks on the carrier should belabeled with the seed per needle count.
6. Fill out the radioactive materials tag and carry the set to Sterile Processing (firstfloor of Children �s Hospital) to be GAS sterilized. Log in the seeds in the SterileProcessing logbook.
7. Survey the preparation area for any lost or stray seeds.
8. Store all equipment and materials in their proper place.
208
Medical University of South CarolinaRadiation Oncology Department
PROCEDURE FOR DAY OF IMPLANT
1. Load the following supplies on the utility cart marked � RAD ONC �
A. Sterile Supplies:
1. Package with � L � block2. Package with needle array block, template, seed and needle manipulation block3. Genesis Pan with needle set and seeds
B. Items to be � Flashed � upon arrival at OR:
1. Special seed handling forceps2. Special seed handling hemostats3. Lead pig marked � OR �4. Modified sponge forceps5. Modified curved forceps6. Metal ruler
C. Spare package of five (5) sterile needles
D. Eberline G-M counter with pancake probe
E. Copy of treatment plan showing needle distribution and the lot number of the seeds thatyou are using.
F. Two packages (2 needles each) of Prostrate Fixation Needles.
2. Change to scrubs and be at OR 20-30 minutes prior to patient �s scheduled time.
A. Scrubs including cap and mask are required but not normally required to � scrub � handsand gown.
B. Give items to Nurse to be flashed.
C. Assist Nurse in setting up apparatus.
1. The needle array block should be nearest the patient at the foot of the table.
a. The remainder of the sterile equipment should be logically placed alongside of the needle block. However, the exact position will depend on theOR that you are in.
2. Open the square needle package and place spare needles in the needle seedmanipulation block on the � L � block PRN.
3. The needle set must be opened and placed on the table for the doctor who will bescrubbed and gowned.
209

Medical University of South CarolinaRadiation Oncology Department
PROCEDURE FOR DAY OF IMPLANT CONT.
D. Read the needle distribution plan to the doctor and double check the location and seedcount of the needles as they are placed in the needle array block.
1. Use of the phonetic alphabet is useful in avoiding confusion but it is not vital.
E. Place the G-M counter on one of the non-sterile table.
1. Ensure that the RAD ONC doctor knows its location.
F. Place your name and phone/beeper number on the board in the OR.
G. Mark the � rad onc � utility cart further by a large strip of tape marked � RAD ONC, DoNot Use �
1. Leave the Genesis pan with the radioactive materials tag visible on the cart.
2. Place the cart out of the way outside of the OR. NOTE: Use any precautionsnecessary to prevent loss of the utility cart and Genesis pan.
3. At commencement of cystoscopy you will be called to the OR.
A. Verify seed work area is no longer sterile.
B. Extrude seeds from unused needles, count and place in pig.
C. Survey work area with G-M counter for misplaced seeds.
1. If seeds are located, count and place in pig.
D. Be prepared to accept any seeds that may be located and recovered by cystoscopy. Countand place in pig.
E. Survey suction machine, bedding, urine, trash and bedding for errant seeds. If located,count and place in pig.
F. When patient has departed room, make one last survey of the OR so cleanup cancommence.
G. INVENTORY ALL YOUR INSTRUMENTS; place on the utility cart and return toRadiation Oncology.
1. The template must be cleaned and decontaminated by the OR staff.
a. Ask them to return the template with the rest of the ultrasound equipmentto Urology.
b. Pick up the template the next day at Module 11.
210
Medical University of South CarolinaRadiation Oncology Department
PROCEDURE FOR DAY OF IMPLANT CONT.
4. When the procedure is finished in the OR:
A. Be sure to have the urology resident put in his orders to have RAD ONC notified whenthe patient is sent from recovery to his room.
1. Have the doctor to order all linens, dressings, and urine to be saved.
B. When the patient is in his room:
1. Attach the Radioactive materials sign to his room door.
2. Attach the pig marked � radioactive materials � in a prominent position in theroom.
a. This pig is for Nursing to use if they should find a seed.
3. Place � Nursing Precautions for Patients receiving Radioactive Brachytherapyfor Prostrate Cancer � form in the patient �s chart.
a. Note that the urine is to be saved.
4. Fill out and place into the patient �s chart a � Permanent Implant Room SurveyForm �.
C. In the Radiation Oncology Department:
1. Make an entry in the R/O patients chart on the progress notes.
a. Include date, number of seeds, average activity, total activity, number ofneedles, how and by whom they were placed.
2. Complete the log book located in the Dosimetry Office.
211
Medical University of South CarolinaRadiation Oncology Department
PROCEDURE FOR DAY FOLLOWING IMPLANT
A. When Nursing notifies the Radiation Oncology Department, the room must be surveyed.
1. Using the G-M counter with the pancake probe, survey the patient �s room, linen, trashand urine.
a. If seeds are located, count them and place in the pig provided.
2. When the room is clear of radioactive materials, remove the Radioactive Materials signfrom the door.
a. Notify Nursing that the room is clear.
b. Make an entry in the patient �s chart on the progress notes to the effect that theroom is clear and ready for normal occupancy.
B. Place all recovered seeds into the pig they were shipped in.
1. To be performed in Radiation Oncology spaces.
2. This includes all seeds.
a. Those recovered from the patient �s room.
b. Those recovered from the OR.
c. Any that may have been left over from the loading.
3. Fill out the white Radiation Safety form on disposition of radioactive materials.
a. Radiation Safety would have delivered the seeds and had you sign for them on theoriginal disposition form.
4. Seeds and form are turned over to Radiation Safety for disposal.
C. Make an entry in the patient �s R/O chart on the Progress Notes stating that the room wassurveyed, clear and ready for normal occupancy.
D. Pick up the template from Module 11 and prepare your sterile packs for the next procedure.
212

Medical University of South CarolinaRadiation Oncology Department
PROCEDURE FOR DAY FOLLOWING IMPLANT CONT.
1. Materials to be Pre-packaged and Sterilized the Week Before the Next Procedure:
A. Package 1: � L � block, window and base (to be gas sterilized)
B. Package 2: 1. Needle array holder (place upside down and load with remaining items.(To be steam sterilized)
2. Template and adjustment rods.
3. Seed and needle manipulation block.
2. Materials to flash 30 minutes prior to the scheduled procedure (can be done in one package):
A. Package 1: 1. � Diddler �
2. Special seed handling forceps
3. Special seed handling hemostats
4. Lead pig marked � OR �
5. Modified sponge forceps (11-inch)
6. Modified curved hemostats (11-inch)
7. Metal ruler
8. Slip shield wrench
3. Materials to be GAS Sterilized second day prior to procedure (i.e., Monday afternoon when theprocedure is on Wednesday)
A. Package 1: 1. Needle set loaded with seeds and spacers. (Carry to Sterile Processing. They will pack into a Genesis pan for protection. Needles are to beprocessed in an horizontal position. The external package cover willhave a Radioactive Materials tag attached. Loaded needles should notbe placed in the General Pickup bins when finished, they should be heldin the Office or at least in the Processing area for pickup.)
4. Carry to OR for use PRN.
A. 1 package of spare needles
B. 2 packages of Prostrate Fixation Needles
1. One package (of 2 needles) must be opened for use.
C. 1 package of spacers
213

Medical University of South CarolinaRadiation Oncology Department
HDR TREATMENT RECORD AND PRESCRIPTION FORM HDR-100
PATIENT: ____________________________________________ RT#: ________________________
PRESCRIPTION FORM DIAGRAM
INITIAL PRESCRIPTIONISOTOPE: Ir-192 DEVICE: Nucletron HDR SN 9349Dose delivered to:____________________________________Treatment Site: ______________________________________Time between fractions: _______________________________Dose/Fract: ________ No.Fract:_______Total Dose:________Signed: ________________________MD Date: ____________
INITIAL PRESCRIPTIONISOTOPE: Ir-192 DEVICE: Nucletron HDR SN 9349Dose delivered to:____________________________________Treatment Site: ______________________________________Time between fractions: _______________________________Dose/Fract: ________ No.Fract:_______Total Dose:________Signed: ________________________MD Date: ____________
INITIAL PRESCRIPTION
ISOTOPE: Ir-192 DEVICE: Nucletron HDR SN 9349
Dose delivered to:____________________________________
Treatment Site: ______________________________________
Time between fractions: _______________________________
Dose/Fract: ________ No.Fract:_______Total Dose:________
Signed: ________________________MD Date: ____________
TREATMENT RECORD
DATEFRACTION NO: 1 2 3 4 5 6ISOTOPE Ir-192 Ir-192 Ir-192 Ir-192 Ir-192 Ir-192No. OF CATHETERSAPPLICATORSDOSE THIS FRAC TION (cGy)SOU RCE STRE NGT H (Ci)No. OF DWELL POINTSTOTAL D WELL TIM E (Sec)PHYSIC S REVIEW (Physicist)TREATMENT AUTHORIZED BY (MD)TOTAL DOSE (cGy) TO DATEDELIVE RED B Y (Therapist)mR/hr POST TREATMENTSPECIAL PHYSICS REPORTMD REVIEW/DATE
214

Medical University of South CarolinaRadiation Oncology Department
NUCLETRON OPERATING PROCEDURES
The following operating procedures will be used in setting up and treating patients with the NucletronmHDR unit in Treatment Rooms 1, 2, and 3.
1. When the treatment is scheduled for one of the treatment rooms, the mHDR unit will be movedfrom the Storage Room to the specific treatment room by the Physics/Engineering staff.
2. The mHDR unit will be connected to the electrical power cables in the treatment room by thePhysics/Engineering staff.
3. The Nucletron control console cabinet will be moved to the treatment room console area andconnected to the power cables and interlock circuitry by the Physics/Engineering staff.
4. The units will be turned on and tested for proper operation by the Physics/Engineering staff.5. The proper operation of the door interlock system will be tested by the Physics/Engineering staff.6. The radiation monitoring system will be tested by the Physics/Engineering staff.7. The intercom and CCTV system will be tested by the Physics/Engineering staff.8. The Physics staff will perform the QA checks in the QA procedures the day of treatment.9. When the patient treatment plan is completed and approved by the attending physics, the Physics
staff will check the treatment data and the treatment plan in the treatment console.10. When all QA checks are satisfactorily completed, the therapist will take the patient into the
treatment room for treatment.11. A survey meter will be located at the control console during the treatment. It will be turned on
and checked prior to the treatment by the therapist.12. An emergency kit will be located near the console.13. A physicist and physician will be present during the treatment.14. Following the completion of the treatment, the therapist and physician will disconnect the
treatment unit from the patient, remove the treatment apparatus and remove the patient from thetherapy room.
15. The therapist will perform a radiation survey of the patient after the patient is removed from thetreatment room and log the results in the patient treatment form. A copy of this form will bephotocopied and placed in the HDR QA Log Book, under daily QA section.
16. The physician will complete the patient treatment chart and the physicist will check it.17. The physicist will log the treatment information into the HDR Treatment Log Book.18. The physicist will write a Special Physics Report for HDR Brachytherapy and place it into the
patient chart.19. The Physics/Engineering staff will disconnect the mHDR treatment unit and control console and
switch the door interlock system back to the linac mode.20. The Physics/Engineering staff will return the mHDR treatment unit and console cabinet to their
storage rooms and secure the rooms by locking them.
215

Medical University of South CarolinaRadiation Oncology Department
HDR Ir-192 SOURCE EXCHANGE AND CALIBRATION PROCEDURES
The Ir-192 source used in the Nucletron Microselectron HDR is changed approximately every threemonths. Following each source exchange, the new source is calibrated to determine its true activity byone of the staff medical physicists. The entire procedure for the source exchange and calibration is givenbelow.
1. Receiving New Source
Nucletron notifies the Section of Medical Physics as to the date the new source will arrive. Oncethe source reaches the department, it is placed in Room 165Q. Within three hours of arrival, awipe test is done of the source container to detect any removable contamination. (Wipes can beobtained from the MUSC Radiation Safety Office. Physicist can wipe the surface of the HDRsource container and submit the wipe in an envelope to RSO for counting.) The container is notto be opened until a negative wipe test result is received. Within a week of receiving the source,a service engineer from Nucletron should arrive to carry out the source exchange.
2. Exchanging Old Source with New Source
When the Nucletron engineer arrives, he removes the old source from the HDR unit and depositsit in the empty pig which is kept in the Room 165Q. With the old source out, preventivemaintenance is carried out by the engineer on the unit. Upon completion of this preventivemaintenance, the engineer installs the new source in the unit. The old source is packed in itsshipping container and kept in Room 165Q until pickup. To arrange for the pickup of the oldsource the physicist in charge of the source exchange contacts Nucletron (1-800-336-2249 - askfor RSO) and informs (via fax or phone) them of the transportation index (T.I.) Of the source, thedecayed activity of the source and the source number (there is a form in the HDR SourceExhcange file for faxing). The appropriate documents are then sent to the physicist by Nucletronand return shipment is made by Federal Express.
3. Source Calibration
Once the new source is in place in the HDR unit, one of the departmental medical physicistscalibrates the source to determine its actual activity. The steps required to perform thecalibration are the following.
a. Warm up the Atom Lab calibrator for at least 30 min. prior to making calibrationmeasurements.
b. Use the insert with the long catheter and secure it at the RED mark on the holder.
c. Connect the end of the catheter to the first index of the HDR unit.
d. From outside the treatment room, program the HDR console for � dwell position 1, length995 mm, dwell time 60 sec � and record the electrometer reading in nanoAmp. In theHDR calibration form. Repeat this 3 more times. Using these measurements, and thecalibration factors of the well chamber and electrometer, the source activity isdetermined. With the calibration setup timer linearity is also checked by takingelectrometer readings for different dwell times eg. 30, 60, 120 and 180 sec. and plot theelectrometer readings against the dwell times.
216
Medical University of South CarolinaRadiation Oncology Department
e. Once the source activity has been determined and is found to be in acceptable agreement(< 3%) with the activity stated on the manufacturer �s certificate, the new activity(measured) is entered into the HDR console memory and the HDR treatment planningcomputer program.
4. Documentation:
The following documents are kept on record (in the � HDR Source Exchange Doc. � Log book) for eachsource exchange.
1. The Certificate for Sealed Source which comes with each source from MallinckrodtDiagnostica.
2. The pink and white delivery slip.
3. The Nucletron Radiation Survey/Source Exchange document from the Nucletron engineer.
4. The Nucletron Field Service Report.
5. The departmental Incoming Package Survey sheet.
6. The wipe test results.
7. Record of Source Calibration done by department physicist (includes source calibration, andtimer linearity check).
8. Declaration of Dangerous Goods for outgoing source.
9. Copy of Federal Express airbill for outgoing source.
10. Copy of Shippers Instructions for outgoing source.
11. Photocopies of Radioactive package labels for outgoing source indicating the T.I. and decayedactivity.
12. Wipe Tests results for outgoing source.
217

PM
AM
Medical University of South CarolinaRadiation Oncology Department
NUCLETRON HDR PATIENT TREATMENT CHECKS
PATIENT: _______________________ R.O# __________ DATE: ___________ TIME:_________
TREATM ENT PRESCRIPTION :____________________________cGy AT __________________
APPLICATOR: ____________________________________________ #CA THETERS: _________
SPECIAL NOTES:__________________________________________________________________
A. PRE-TREATMENT CHEC KLIST: (ALL ITEMS MUST BE SATISFACTORY BEFORE TREATMENT
CAN PROCEED)
1. Patient Identification verified by two means? . . . . . . . . . . . . . . . . . . . . . . . . . .YES ______ NO ______
2. Treatment Rx (Form HDR-100) completed by physician?. . . . . . . . . . . . . . . . YES ______ NO ______
3. Patient Consent Form is signed? . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . YES ______ NO ______
4. Computer Tx plan complete and apporved by physician?. . . . . . . . . . . . . . . . YES ______ NO ______
5. Computer Tx plan downloaded into treatment console?. .. . . . . . . . . . . . . . . . YES ______ NO ______
6. Note any discrepancies between computer plan and console plan? . . . . . . . . . YES ______ NO ______
7. Does current console source strength and computer plan match within 1%?. YES ______ NO ______
8. Does current console source strength match daily decay chart within 1%?. . YES ______ NO ______
9. Has printed treatment plan been approved by physician?.. . . . . . . . . . . . . . . . YES ______ NO ______
10. Are all treatment tubes correctly attached to the Selectron and patient?. . . . .YES ______ NO ______
11. Is the patient comfortable and instructed regarding the treatment? . . . . . . . . YES ______ NO ______
12. Are the intercom and TV monitors operating properly? . . . . . . . . . . . . . . . . . YES ______ NO ______
13. Door/emergency interlocks fuctional? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .YES ______ NO ______
14. Battery Back-up checked?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .YES ______ NO ______
15. Positional accuracy checked?. . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . YES ______ NO ______
16. Emergency Interrupt Functional?. . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . .. YES ______ NO ______
B. POST-TREATMENT CHEC KLIST:
1. Note any patient complaints?. . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .YES ______ NO ______
(Explain:) ___________________________________________________________________________________
_________ ___________________________________________________________________________________
2. Have copies of the treatment log and data been placed into patient chart? . . .YES ______ NO ______
3. Have all disposable items been properly bagged, tagged and disposed of? . . . YES ______ NO ______
4. Have all reusable items been cleaned and sterilized? . . . . . . . . . . . . . . . . . . . . .YES ______ NO ______
5. Have all HDR items been returned to their proper location? . . . . . . . . . . . . . . YES ______ NO ______
6. Has patient treatment information been entered into HDR logbook?. . . . . . .. YES ______ NO ______
7. Has patient been surveyed after source removal? . . . . . . . . . . . . . . . . . . . . . . ..YES ______ NO ______
8. G-M Su rvey meter readings: Eberline E-120 , SN: ________ __;
check Source Reading: (x1 Scale): _______
9. Patient Surv ey Readin gs:
mR/hr @ surface of patient: ________________; mR/hr at 1 foot from patient: ___________
CHECKED BY: ______________________________________ RT(T); DATE: ___________________
RADIATION TH ERAPIST
218
Size =
Total Time (h)
Mg-h
Total mg-h
Time in
Day in
Date in
Time out
Day out
Date out
Source#
IsotopeSource Strength (mgRaEq)
Tandem/Vag. Cylinder
LeftOvoid
RightOvoid
1 Cs-137
2 Cs-137
3 Cs-137
4 Cs-137
5 Cs-137
6 Cs-137
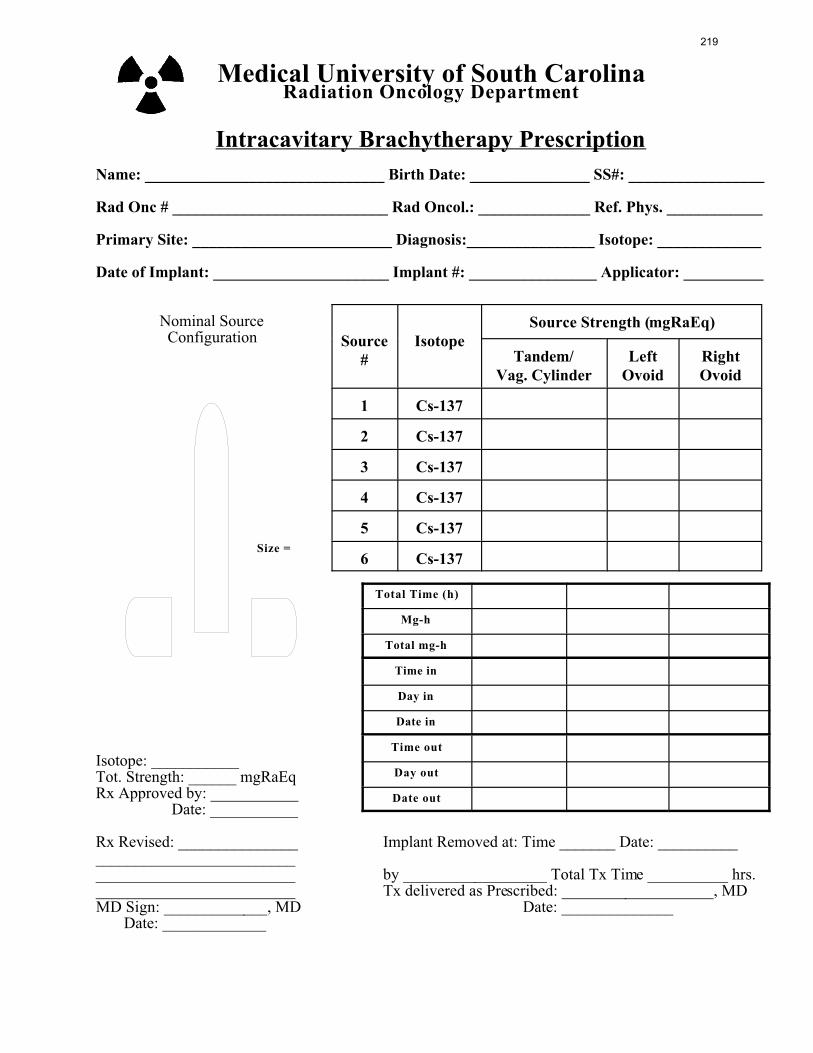
Medical University of South CarolinaRadiation Oncology Department
Intracavitary Brachytherapy Prescription
Name: ______________________________ Birth Date: _______________ SS#: _________________
Rad Onc # ___________________________ Rad Oncol.: ______________ Ref. Phys. ____________
Primary Site: _________________________ Diagnosis:________________ Isotope: _____________
Date of Implant: ______________________ Implant #: ________________ Applicator: __________
Nominal Source Configuration
Isotope: ___________Tot. Strength: ______ mgRaEqRx Approved by: ___________ Date: ___________
Rx Revised: _______________ Implant Removed at: Time _______ Date: ____________________________________________________________ by __________________ Total Tx Time __________ hrs._________________________ Tx delivered as Prescribed: ___________________, MDMD Sign: _____________, MD Date: ______________ Date: _____________
219

Radiation Oncology, Brachytherapy and Radiopharmaceutical Treatment
Verification
1. Patient Name: _______________________________________
2. Patient #: ___________________________________________
3. Attending Physician: __________________________________
4. Date: _______________________________________________
5. Dose Prescription:_____________________________________________________________
6. Site of Treatment:_____________________________________________________________
7. Radionuclide to be used: _______________________________________________________
8. Form: _______________________________________________________________________
9. Activity: _____________________________________________________________________
10. Method of administration: ______________________________________________________
11. Activity proposed to be used: ____________________________________________________
12. Activity actually used: _________________________________________________________
13. Reason for deviation: __________________________________________________________
14. Patient ID verified by: a. person ______________________________
b. date ________________________________
c. method 1 ____________________________
d. method 2 ____________________________
15. Sources to be used verified by: a. person 1. _______________ 2. _______________
b. date _____________________________________
c. Method __________________________________
16. Sources removed (if applicable) __________________________________________________
17. Date ____________________________
18. Exposure level at 1 meter at time of source removal or patient discharge__________________________ by _______________________ date ____________________
19. Comments: ___________________________________________________________________
_____________________________________________________________________________
220

CESIUM THERAPY RECORDMEDICAL UNIVERSITY HOSPITALRadiation Oncology Department
Name _________________________Sex ________ Age ______ Hospital No. ____________________
Clinical Diagnosis ____________________________________________________________________
Histologic Report ____________________________________________________________________
Location of Lesion Treated ____________________________________________________________
Method of Lesion Treated _____________________________________________________________
Method of Cesium application _______________________Technique_________________________
Therapist _________________________________________Assistant _________________________
Time ofapplication
date signature Total Amt. Cesium _________________mg.
Duration _________________________hrs.
Proposed Dose ___________________mgrs.
ProposedTime ofRemoval
date signature No. Mr. Sizemm.
Filtermm. Pt.
LinearIntensity
Actual Timeof Removal
date signature
Total Time Applicator Was in Place
Calculated Tissue Dosage: (gamma r & mg hrs)
Diagram & Remarks:
221

MEDICAL UNIVERSITY OF SOUTH CAROLINARadiation Oncology Department
PATIENT ROOM SURVEY
(Name Plate Stamp)
PATIENT: ______________________ ROOM: __________in @ _____________________ am/pm on _________out @ ____________________ am/pm on _________
Total hours: _____________________ By: ______________
Total amount of _________ used: _________ mgm-Ra-EquivSource #1: _____ #2 _____ #3 _____ #4 _____ #5 ____ #6 ____
Radiation Readings in Room: (mR/hr) at Bed Location: _____(See Diagram Below for appropriate Roo m Bed Layo ut to Select)
222

MEDICAL UNIVERSITY OF SOUTH CAROLINARadiation Oncology Department
CESIUM WARD RECEIPT
DATE: _______________________________________
TIME OF INSERTION: __________________AM/PM
NUMBER OF HOURS: _________________________
TIME OF REMOVAL: ___________________AM/PM
APPLICATORS & LOADING
SOURCES, NUMBER & DESCRIPTION:
_____________________________________________________________________
_____________________________________________________________________
TOTAL NUMBER OF SOURCES: ______________________________________
REMOVAL OF CESIUM:
REMOVED BY: ___________________ DATE: _____________ TIME: _________AM/PM
CHECKED BY: ___________________ DATE: _____________ TIME: _________AM/PM
RECEIVED IN CESIUM ( � RADIUM � ) ROOM: ____________________________ AM/PM
SURVEY READINGS:
READING AT 1 METER (3 FEET): ___________________mR/hr
READING AT DOOR: _______________________________mR/hr
READING AFTER CESIUM REMOVED FROM PATIENT AND
ROOM: ____________________________________________mR/hr
223

MEDICAL UNIVERSITY OF SOUTH CAROLINARadiation Oncology Department
NURSING PRECAUTIONS FOR PATIENTS RECEIVING RADIOACTIVEBRACHYTHERAPY
PATIENT: ___________________ PATIENT #: ___________________ ROOM #: ____________was administered ________mg-Ra-Eq of _________ on (Date:) __________ at (Time:) _________AM/PMBy: ____________________________________ M.D.; Pager #: ______________________ Phone: (2-3271)
NO VISITORS ARE ALLOWED IN ROOM DURING TREATMENT
PLEASE OBSERVE THE FOLLOWING NURSING PRECAUTIONS UNTIL ALL SOURCES ARE REMOVED FROM PATIENT AND ROOM IS SURVEYED.
1. All brachytherapy patients must be placed in a private bathroom. If only one brachytherapypatient is to be placed in a room, place the patient in a bed farthermost from the door.
2. Portable lead shielding may be required to reduce personnel exposure at bedside. Please standbehind this shield when attending the patient, if possible.
3. The patient shall remain in the room while the source(s) are in place. If the patient accidently orintentionally removes the source(s) from his/her body, IMMEDIATELY CONTACT THERESIDENT ON DUTY. He/She will place the source(s) in a portable shielded carrier. UNDERNO CIRCUMSTANCES SHOULD YOU PICK UP OR TOUCH THE SOURE(S). In the eventof lost, damaged, or ruptured source(s), CONTACT THE ABOVE PHYSICIAN AND THEMUSC RADIATION SAFETY OFFICER (2-4255). Stop all traffic into or out of the area andturn off all room air-conditioning or ventilation. Close the door and label � Contaminated Area-Do Not Enter without Protective Clothing! �
4. The patient must be surveyed after all source(s) are removed from the room and the results of thesurvey shall be noted in the patient �s chart and the MUSC Cesium Ward Receipt form. Theroom also shall be thoroughly surveyed before release for use.
5. Patient excreta may be disposed of in the normal manner unless noted otherwise in theseinstructions:
6. Nursing personnel attending the patient may be required to wear film badge monitors at thediscretion of the MUSC Radiation Safety Officer (RSO). If issued by the RSO, the film badgemonitor is to be worn either at waist level, on a pocket, or on the collar. Film badge monitors areto be worn ONLY by the individual to whom they are issued. Contact the RSO (2-4255) ifadditional monitors are needed.
7. Only designated residents, radiation oncology residents, attending radiation oncologists, radiationphysicists, radiation oncology dosimetrists, radiation therapists, or RSOs shall removebrachytherapy sources from a patient.
8. In case of death, DO NOT REMOVE THE BODY FROM THE ROOM until the RSO (2-4255)has issued appropriate instructions. Contact the RSO, Radiation Oncology (2-3271) or theCentrex Operator (2-2123) for emergency phone numbers or pager numbers if no answer at eitheroffice.
224
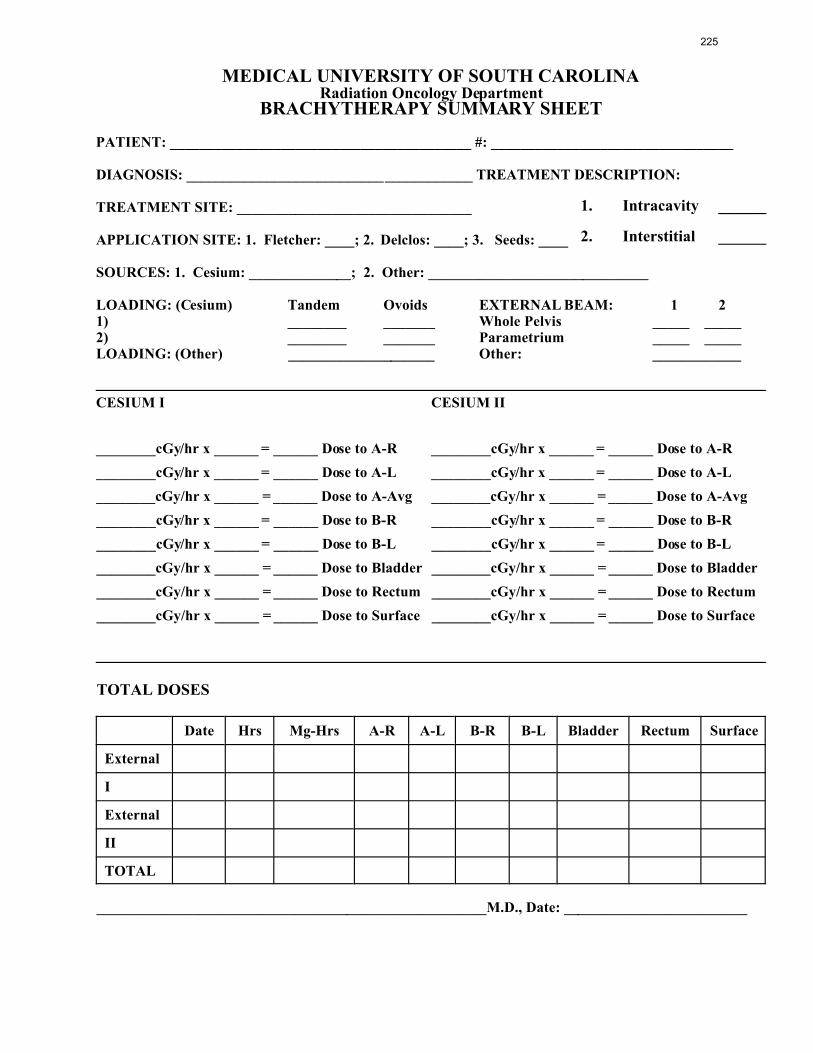
1. Intracavity ______
2. Interstitial ______
MEDICAL UNIVERSITY OF SOUTH CAROLINARadiation Oncology Department
BRACHYTHERAPY SUMMARY SHEET
PATIENT: _________________________________________ #: _________________________________
DIAGNOSIS: _______________________________________ TREATMENT DESCRIPTION:
TREATMENT SITE: ________________________________
APPLICATION SITE: 1. Fletcher: ____; 2. Delclos: ____; 3. Seeds: ____
SOURCES: 1. Cesium: ______________; 2. Other: ______________________________
LOADING: (Cesium) Tandem Ovoids EXTERNAL BEAM: 1 21) ________ _______ Whole Pelvis _____ _____2) ________ _______ Parametrium _____ _____LOADING: (Other) ____________________ Other: ____________
CESIUM I CESIUM II
________cGy/hr x ______ = ______ Dose to A-R ________cGy/hr x ______ = ______ Dose to A-R
________cGy/hr x ______ = ______ Dose to A-L ________cGy/hr x ______ = ______ Dose to A-L
________cGy/hr x ______ = ______ Dose to A-Avg ________cGy/hr x ______ = ______ Dose to A-Avg
________cGy/hr x ______ = ______ Dose to B-R ________cGy/hr x ______ = ______ Dose to B-R
________cGy/hr x ______ = ______ Dose to B-L ________cGy/hr x ______ = ______ Dose to B-L
________cGy/hr x ______ = ______ Dose to Bladder ________cGy/hr x ______ = ______ Dose to Bladder
________cGy/hr x ______ = ______ Dose to Rectum ________cGy/hr x ______ = ______ Dose to Rectum
________cGy/hr x ______ = ______ Dose to Surface ________cGy/hr x ______ = ______ Dose to Surface
TOTAL DOSES
Date Hrs Mg-Hrs A-R A-L B-R B-L Bladder Rectum Surface
External
I
External
II
TOTAL
_____________________________________________________M.D., Date: _________________________
225

CHECKLIST FORMEDICAL PROGRAM APPLICATION
(REMOTE AFTERLOADING BRACHYTHERAPY DEVICES)
Yes No
1. Did the applicant submit the name and address for the proposed location of use in items 1a. 1b.
2. Did the applicant submit the following information pertaining to radioactive material requested and
the purpose used for in items 6 & 7:
Source
a. Radionuclide(s): ___________________
b. Activity (Ci): ____________
c. Manufacturer & Model Number(s): ____________________________________________
_________________________________________________________________________
d. Listed in the �Registry of Sealed Sources and Devices � . (List reference no. ____________)
Device
a. Manufacturer & Model Number(s): ____________________________________________
_________________________________________________________________________
b. Listed in the �Registry of Sealed Sources and Devices � . (List reference no. ____________)
c. Device type: LDR ______ MDR ______ HDR _______ Pulsed ______
3. Intended use:
a. Interstitial/Intracavitary
b. Intraluminal
c. Human only
d. Other: ___________________________________________________________________
4. Did the applicant subm it the full names of all physicians who will use or directly supervise the use
of radioac tive material.
5. Did the applicant include preceptor statement forms (DHEC form 814) for each physician requested
to be an authorized user.
a. Proper training and experience.
b. Licensed to practice medicine in S.C.
c. Preceptor statement signed for non-certified new users, etc. (Ref: Supplements A and B)
6. Did applicant submit training and experience for physicist. (Ref: RHA 4.15.12)
7. Did applicant submit information concerning their personnel training program:
Authorized Users and Device Operators
a. Subjects to be included in initial training.
226
b. � Hands On � operation training.
c. Trained operators present during use.
d. Annual retraining.
- Subjects to be included during retraining.
- � Hands on � emergency procedure implementation.
Instructors - Initial training
a. Name, affiliation, qualifications.
b. Experience with afterloading device(s).
Records of training maintained.
8. Did the ap plicant subm it the following info rmation co ncerning their facilities and eq uipment:
a. Dedicated Room (High, Pulsed, and Medium Dose Date)
- Annotated drawing.
- Scale.
- Room numbers (Room Identification).
- Shielding ma terial.
- Adjacent areas; restricted/unrestricted; include areas above and below treatment room.
b. Viewing system and intercom.
- Primary.
- Backup.
- Provision if primary system fails without backup.
c. Access co ntrol.
- Electrical interlock.
- System operation.
- Response to interruption.
- Commitment to suspe nd treatment if interlock malfunctions.
- Area controls (signs, locks, visible/audible alarms).
- Other radiation-produc ing devices.
- Method to prevent dual operation.
- Security of console keys.
d. Permanent radiation monitor.
- Visible notic e on entry.
227

- Back-up power sup ply.
- Operability check.
- Emergency entry provisions.
- Commitment to promptly repair/replace.
9. Compliance with restricted/unre stricted area radiation level limits.
a. Calculation s of maximu m radiation levels for restricted /unrestricted a reas to dem onstrate
compliance with RHA 3.5 and 3.13.
- Parameters used to calculate radiation levels (source strength, shielding materials, room
configuration, etc.).
- Anticipated workload d ata, occupancy factors.
- Dose calculations for individuals in restricted and unrestricted areas.
- Dose levels comply with RHA 3.5 and 3.13.
- Exemption from RHA 3.13.
- Need for exemption specified.
- Duration of exemption specified.
- Program to access and control dose.
b. Survey program to demonstrate compliance with RHA 3.16.
- Survey of device following source replacement or location of device changes.
c. Device label in accordance with RHA 3.24.
10. Personnel monitoring
a. Personnel dosimetry provided to appropriate personnel in compliance with RHA 3.17.
11. Survey instrum ents
a. Survey instruments satisfy RHA 4.13.6.
b. Daily operability checks.
c. Calibration performed annually in accordance with RHA 4.8.3.
d. Records of calibrations maintained in accordance with RHA 4.8.3.
12. Operating Procedures
a. Commitment to provide copies to device operators and post copies at device console.
b. Comm itment to pro vide verba l, as well as written instruc tion to individ uals provid ing safety
checks.
c. Procedures sub mitted include following comm itments:
- Device, console, and treatment room secured when not in use or unattended.
228

- Only patient allowed in treatment room for medium/high dose rate afterloading device.
- When visitors are allowed for low and pulsed dose rate treatments, procedures shall be
established to insure the source is retracted into the shielded safe prior to entry of the
visitor(s) into the room and the maximum no. and length of visits allowed shall be
charted.
- Nursing personnel provided specific (written) instructions for patient care.
- Computer media used to load patient treatment parameters properly labeled, reused in
accordance with m anufacturer � s instructions.
- Survey of device and patient performed immediate ly following source retraction or
removal.
- Record of device and patient surveys maintained.
- Commitment to implement emergency procedures if source not fully retracted.
- Commitm ent not to co nduct treatm ents for which a decoup le or jamm ed source could no t
be remo ved expe ditiously.
- Authorized user and m edical physic ist or radiation safety officer pre sent during all
treatments using a medium, pulsed, or high dose rate afterloading device.
- Authorized user and m edical physic ist or radiation safety officer pre sent during all
treatments using a pulsed dose rate afterloading device or alternative commitment to
provide equivalent safety contro ls.
- Device operator present and available by telephone during treatments with low dose
afterloading device, authorized user and medical physicist or radiation safety officer
available for assistance.
d. Daily checks - descriptions submitted.
- Permanent radiation monitor tested with dedicated check source.
- Viewing an d intercom systems check ed for op erability.
- Source p osition indica tors checke d for ope rability.
- Treatment console operational function check and test of all indicators (lamps) and
displays.
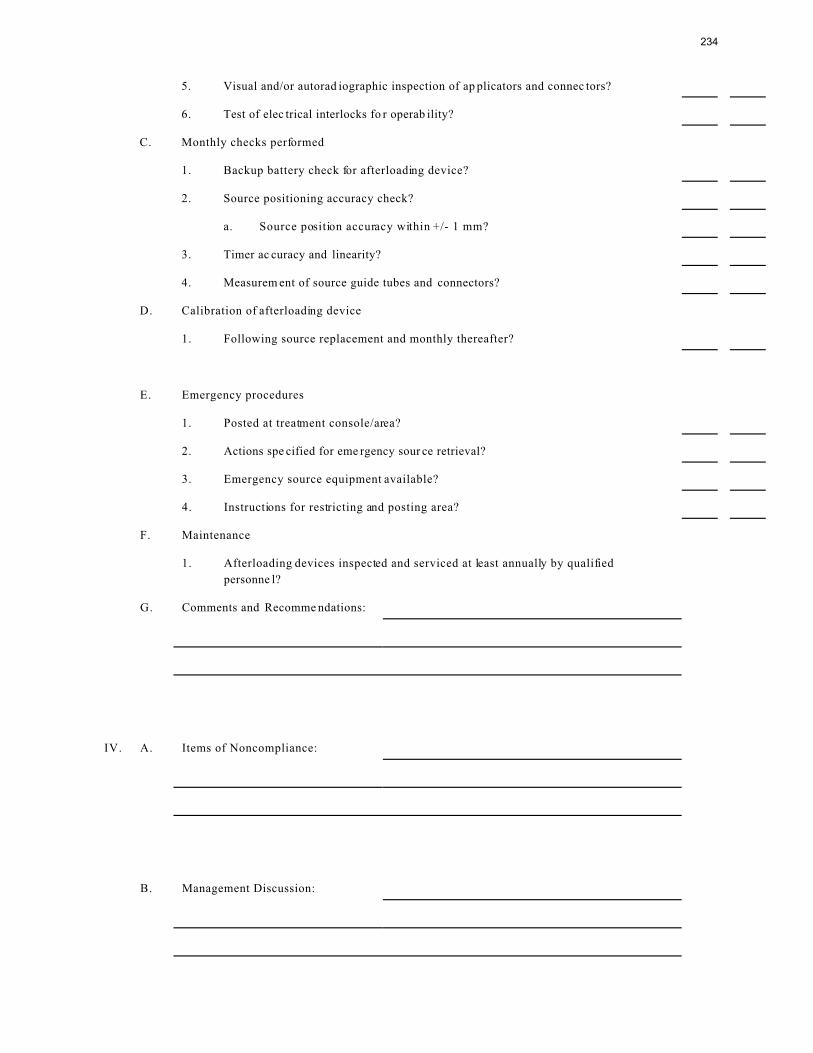
- Visual and/or autoradio graphic inspection of app licators and connectors.
- Test of electrical interlocks for operability, records of test maintained.
- Commitment to suspe nd treatments if interlock system malfunctions.
- Record of daily checks maintained.
e. Monthly safety checks - description submitted.
- Backup battery check for afterloading device.
- Source positioning accuracy checked.
- Source position accuracy within +/- 1mm.
229
- Procedure submitted.
- Timer ac curacy and linearity.
- Measuremen t of source guide tubes and connectors.
-Records maintained.
f. Calibration of afterloading device.
- Names and qu alifications of individuals performing calibrations.
- Experience with dosimetry system.
- Description of method used to determine exposure rate.
- Record of calibration maintained and conte nt.
- Notification o f radiation safety o ffice or med ical physicist if mea sured outp ut differs by
greater than 5% of expected value.
Dosimetry System.
- Calibrated by NIST /AAPM - approved lab at 2 year intervals.
- Calibration record maintained.
- Calibration frequency - following source replacement and monthly thereafter.
- Determina tion of sourc e homog eneity.
g. Method of conducting source inventories in accordance with RHA 4.8.6.7
(autoradiography, source replacement, etc.).
13. Emergency P rocedures.
a. Established by authorized user and RSO or medical physicist, posted at treatment
console/area.
- Specify when to implement p rocedures.
- Confirmation copies of pro cedures provide d to device ope rators.
- Actions spe cified for eme rgency sour ce retrieval.
- Step-by-Step actions for progressive equipment failures, specific instructions on which
steps may be applicab le for given circumstances and wh o will perform these actions.
- Requirem ent to notify autho rized user an d medica l physicist or RS O immed iately of any
problem requiring implementation.
- Appropriate telephone numbers posted.
-Instructions for restricting and posting area.
- Emergen cy source re covery eq uipment.
14. Maintenance
a. Performed only by manufacturer �s representatives or individuals specifically authorized by
NRC or Agreement State.
230

b. Records maintained for all maintenance and repair.
c. Afterloadin g device insp ected and serviced at lea st annually.
- Inspections performed by individuals authorized by N RC or Agree ment States.
- Records of inspections maintained.
d. Licensee employee authorized to perform device maintenance and repair.
- Has letter or certificate from manufacturer documenting training.
- Letter of certificate specifies those functions which the named individual is qualified to
perform.
15. Waste disposal
a. Transferred only to authorized recipient (manufacturer).
231

MEDICAL UNIVERSITY OF SOUTH CAROLINA
Radiation Oncology
Radioactive Material Inspection
Inspection Date: ______________ Previous Inspection Date: ____________
I. License Review Yes No
A. Copies of MUSC Radiation Safety Manuals, Titles A and B, Title 10CFR and MUSC
licensed user authorizations on hand.
Comments:
B. Are radio active mater ials being used only by autho rized pers onnel and accordin g to
approv ed proto col.
Comments:
C. Are personnel being adequately monitored for exposure and the exposures reviewed by
managem ent.
Comments:
D. Are ancillary personnel credentialed and/or have received proper on the job training.
Comments:
E. Unusual occurrences, incidents or misadministrations since last inspection.
Comments:
232