Embed Size (px)
Citation preview

1.DURFEE - EL MONTE CITY UNIFIED SCHOOL DISTRICT MURCHISON - LA UNIFIED SCHOOL DISTRICT
a. A parent or student/patient is a member of the committee. Not Met: Nob. A school official (e.g., teacher, administrator) is a member of the committee. Fully Met: Principal, Community representativec. An SBHC medical professional is a member of the committee. Fully Met: Nurse practitioner, medical assistant, nurse d. An SBHC oral health professional is a member of the committee. Fully Met: Dentist - Adjunct Faculty, Associate Dean, Registered
Dentist Hygienists, Registered Dentist Assistantse. Other members: Fully Met: Organization Facilitator [Roberta Villanueva (replacing
Connie Wahalley)]; Decapo Daca
f. Members identify and discuss issues related to the integration of comprehensive oral health services into SBHC.
Fully Met: Discuss at the quarterly Oral Health Team Meetings; communication with Western U Director of Community Outreach, COH Program Manager
g. Members provide input into the development of standardized policies, plans, and operating procedures. Partially Met: Need to discuss standardization of policies, plans and operating procedures with Dr. Kim Uyeda, DirectorStudent Medical Services, Community Partnerships and Medi-Cal Programs; Files and documentation protocol
2.
a. Administrative services (e.g., reception, appointments, billing) are shared. Fully Met: Special LAUSD manual was created for Murchison to allow coordination of services.
b. Support service staff (e.g., case managers, benefit counselors) are shared. Partially met: Nothing formal a this time.c. Standard operating procedures are in place to ensure that students enrolled in SBHC receive oral health
exams and needed treatment (e.g., referral and care coordination protocols).Fully Met: Training of dental students to conduct tratments; referral and care coordination protocols X-ray equipment was not there month of April; otherwise
d. One enrollment form covers consent for all health services (e.g., behavioral, medical, oral health) offered by SBHC.
Fully Met: Consent forms distributed by dental clinical staff, school nurses, medical clinic staff, WIC, and Head Start
e. Standard operating procedures are in place to ensure the coordination of all health services (e.g., continuity of care, case-management protocols) offered by SBHC.
Partially met: Nothing formal at this time.
f. Plan exists for recruiting and retaining all health professionals (e.g., behavioral, medical, oral health) and other key staff.
Fully Met: Continuing education units are available for staff who undergo training. Secondary providers are also invited to attend.
3.
a. All health records and access to health records are in compliance with HIPAA and FERPA rules, if applicable.
Fully met: Yes.
b. SBHC participates in the Center for Medicare & Medicaid Services’ Meaningful Use program. No; N/Ac. SBHC participates in the American Academy of Pediatrics’ Chapter Alliance for Quality Improvement
Electronic Health Record program.
4.a. A multidisciplinary team develops patient-care plans.
b. Care coordination is used to ensure that oral health treatment plans are completed.c. All health professionals participate in case/chart reviews on a regular basis.
Fully met: WesternU School Based Oral Health ManualFully met?: Dental adjunct faculty from WesternU audit
Fully met: Nurses referring to school based oral health center: principals, administrative assistants, health services chair, nurses, dentists, RDH, and RDAs
Fully Met: Western U dental clinic School Based Oral Health Center
Fully Met: Consent forms distributed by dental clinical staff, school nurses, medical clinic staff, WIC, and Head StartFully Met: Western U dental clinic School Based Oral Health Center Manual; Healthy Teeth Toolkit stores information and treatment urgency is assessed to determine when they need to be scheduled to be seen by the clinic.
Fully Met: Inter-professional Training, Inter-professional education for dental students (called IPE - Interprofessional Education)
Fully Met: Outlined in WesternU School Based Oral Health Manual
No; N/ANot participating in this particular alliance but are involved in Pediatric medical and dental organizations.Not participating in this particular alliance but are involved in Pediatric medical and dental
organizations.
Fully met: Nurses referring to school based oral health center: principals, administrative assistants, health services chair, nurses, dentists, RDH, and RDAs
Fully met: WesternU School Based Oral Health ManualFully met?: Dental adjunct faculty from WesternU audit
Fully Met: Parent liasonFully Met: Principal, Health AssistantFully Met: Nurse, Health Services Chair
Fully Met: Dentist - Adjunct Faculty, Associate Dean, Registered Dentist Hygienists, Registered Dental AssistantsFully Met: Western U and COH administrative staff: Program Manager
Fully Met: Discuss at the quarterly Oral Health Team Meetings; communication with Western U Director of Community Outreach, COH Program Manager
Fully Met: Use OfficeAlly software for scheduling; Eval*U used for documenting services; School Based Oral Health Center Manual
Fully Met: Western U dental clinic School Based Oral Health Center Manual created to coordinate between dental clinic and school based health center
Fully Met: Social Worker, Health Assistant
Maternal and Child Health BureauSchool-Based Comprehensive Oral Health Services Grant Program
Integrating Oral Health Care Services into School-Based Health Centers
Integration Worksheet
All health records (behavioral, medical, and oral health) are electronic, in compliance with privacy regulations, and are shared with all SBHC staff.
Policies, plans, and operating procedures for all health professionals involved in the integration of health services delivered in SBHC are standardized.
SBHC advisory committee has diverse representation, and its meetings address the planning, implementation, and oversight of the integration process.
Category, Variables, and Attributes
Delivery-System Design
Indicator or Data Used to Determine if Attribute is Fully Met, Partially Met, or Not Met
Delivery of primary health care by SBHC is provided using an integrative approach.
Appendix A COH Integration Report
1
Category, Variables, and Attributes
Delivery-System Design
Indicator or Data Used to Determine if Attribute is Fully Met, Partially Met, or Not Met
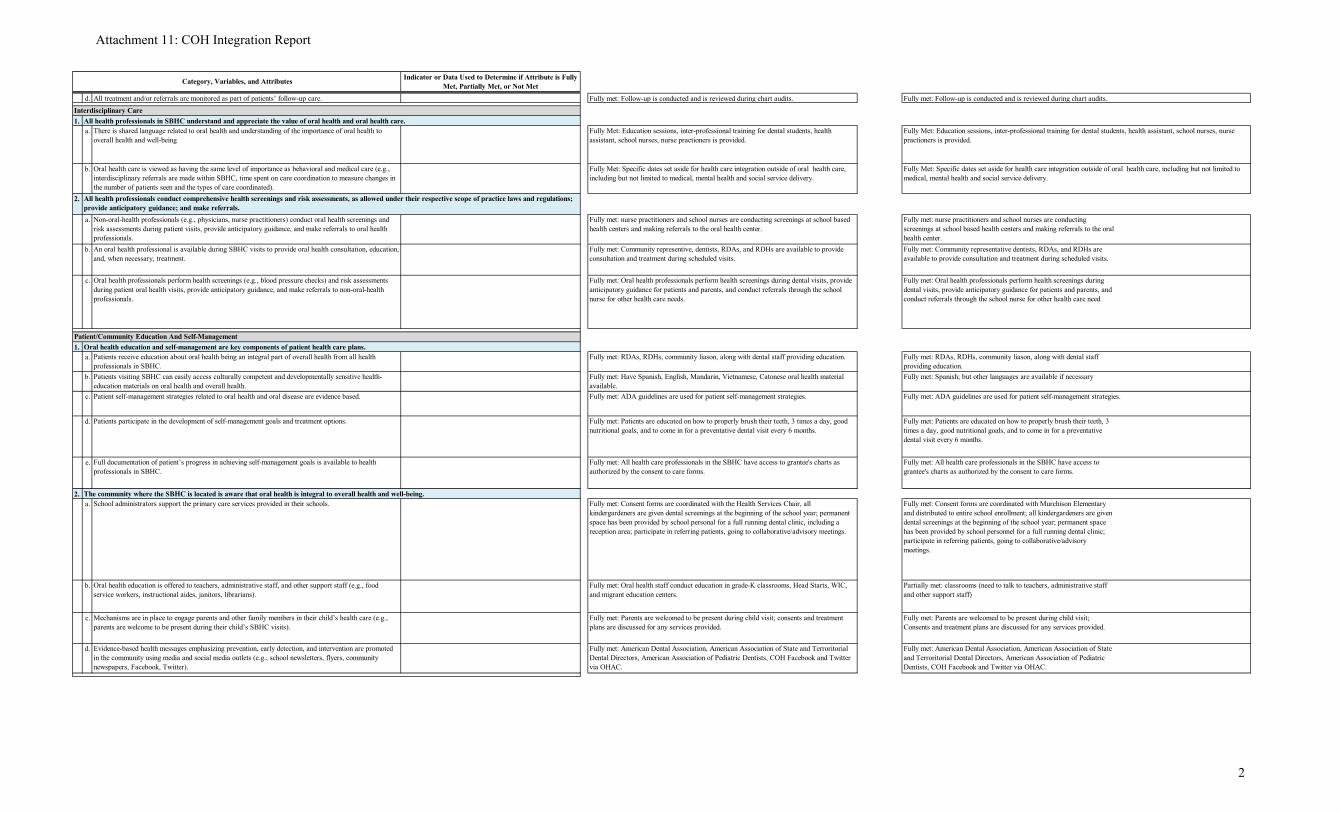
d. All treatment and/or referrals are monitored as part of patients’ follow-up care.
1.a. There is shared language related to oral health and understanding of the importance of oral health to
overall health and well-being
b. Oral health care is viewed as having the same level of importance as behavioral and medical care (e.g., interdisciplinary referrals are made within SBHC, time spent on care coordination to measure changes in the number of patients seen and the types of care coordinated).
2.
a. Non-oral-health professionals (e.g., physicians, nurse practitioners) conduct oral health screenings and risk assessments during patient visits, provide anticipatory guidance, and make referrals to oral health professionals.
Fully met: nurse practitioners and school nurses are conducting screenings at school based health centers and making referrals to the oral health center.
b. An oral health professional is available during SBHC visits to provide oral health consultation, education, and, when necessary, treatment.
Fully met: Community representative dentists, RDAs, and RDHs are available to provide consultation and treatment during scheduled visits.
c. Oral health professionals perform health screenings (e.g., blood pressure checks) and risk assessments during patient oral health visits, provide anticipatory guidance, and make referrals to non-oral-health professionals.
Fully met: Oral health professionals perform health screenings during dental visits, provide anticipatory guidance for patients and parents, and conduct referrals through the school nurse for other health care need
1.a. Patients receive education about oral health being an integral part of overall health from all health
professionals in SBHC.Fully met: RDAs, RDHs, community liason, along with dental staff providing education.
b. Patients visiting SBHC can easily access culturally competent and developmentally sensitive health-education materials on oral health and overall health.
Fully met: Spanish; but other languages are available if necessary
c. Patient self-management strategies related to oral health and oral disease are evidence based.
d. Patients participate in the development of self-management goals and treatment options. Fully met: Patients are educated on how to properly brush their teeth, 3 times a day, good nutritional goals, and to come in for a preventative dental visit every 6 months.
e. Full documentation of patient’s progress in achieving self-management goals is available to health professionals in SBHC.
Fully met: All health care professionals in the SBHC have access to grantee's charts as authorized by the consent to care forms.
2.a. School administrators support the primary care services provided in their schools. Fully met: Consent forms are coordinated with Murchison Elementary
and distributed to entire school enrollment; all kindergardeners are given dental screenings at the beginning of the school year; permanent space has been provided by school personnel for a full running dental clinic; participate in referring patients, going to collaborative/advisory meetings.
b. Oral health education is offered to teachers, administrative staff, and other support staff (e.g., food service workers, instructional aides, janitors, librarians).
Partially met: classrooms (need to talk to teachers, administrative staff and other support staff)
c. Mechanisms are in place to engage parents and other family members in their child’s health care (e.g., parents are welcome to be present during their child’s SBHC visits).
Fully met: Parents are welcomed to be present during child visit; Consents and treatment plans are discussed for any services provided.
d. Evidence-based health messages emphasizing prevention, early detection, and intervention are promoted in the community using media and social media outlets (e.g., school newsletters, flyers, community newspapers, Facebook, Twitter).
Fully met: American Dental Association, American Association of State and Terroritorial Dental Directors, American Association of Pediatric Dentists, COH Facebook and Twitter via OHAC.
Fully Met: Education sessions, inter-professional training for dental students, health assistant, school nurses, nurse practioners is provided.
Fully Met: Specific dates set aside for health care integration outside of oral health care, including but not limited to medical, mental health and social service delivery.
Fully met: ADA guidelines are used for patient self-management strategies.
Fully met: Follow-up is conducted and is reviewed during chart audits.Fully met: Follow-up is conducted and is reviewed during chart audits.Interdisciplinary Care
Patient/Community Education And Self-Management
All health professionals conduct comprehensive health screenings and risk assessments, as allowed under their respective scope of practice laws and regulations; provide anticipatory guidance; and make referrals.
Oral health education and self-management are key components of patient health care plans.
The community where the SBHC is located is aware that oral health is integral to overall health and well-being.
All health professionals in SBHC understand and appreciate the value of oral health and oral health care.Fully Met: Education sessions, inter-professional training for dental students, health assistant, school nurses, nurse practioners is provided.
Fully Met: Specific dates set aside for health care integration outside of oral health care, including but not limited to medical, mental health and social service delivery.
Fully met: nurse practitioners and school nurses are conducting screenings at school based health centers and making referrals to the oral health center.
Fully met: Community representive, dentists, RDAs, and RDHs are available to provide consultation and treatment during scheduled visits.
Fully met: Oral health professionals perform health screenings during dental visits, provide anticipatory guidance for patients and parents, and conduct referrals through the school nurse for other health care needs.
Fully met: RDAs, RDHs, community liason, along with dental staff providing education.
Fully met: Have Spanish, English, Mandarin, Vietnamese, Catonese oral health material available.Fully met: ADA guidelines are used for patient self-management strategies.
Fully met: Patients are educated on how to properly brush their teeth, 3 times a day, good nutritional goals, and to come in for a preventative dental visit every 6 months.
Fully met: All health care professionals in the SBHC have access to grantee's charts as authorized by the consent to care forms.
Fully met: Consent forms are coordinated with the Health Services Chair, all kindergardeners are given dental screenings at the beginning of the school year; permanent space has been provided by school personal for a full running dental clinic, including a reception area; participate in referring patients, going to collaborative/advisory meetings.
Fully met: Oral health staff conduct education in grade-K classrooms, Head Starts, WIC, and migrant education centers.
Fully met: Parents are welcomed to be present during child visit; consents and treatment plans are discussed for any services provided.
Fully met: American Dental Association, American Association of State and Terroritorial Dental Directors, American Association of Pediatric Dentists, COH Facebook and Twitter via OHAC.
Attachment 11: COH Integration Report
2
Category, Variables, and Attributes
Delivery-System Design
Indicator or Data Used to Determine if Attribute is Fully Met, Partially Met, or Not Met
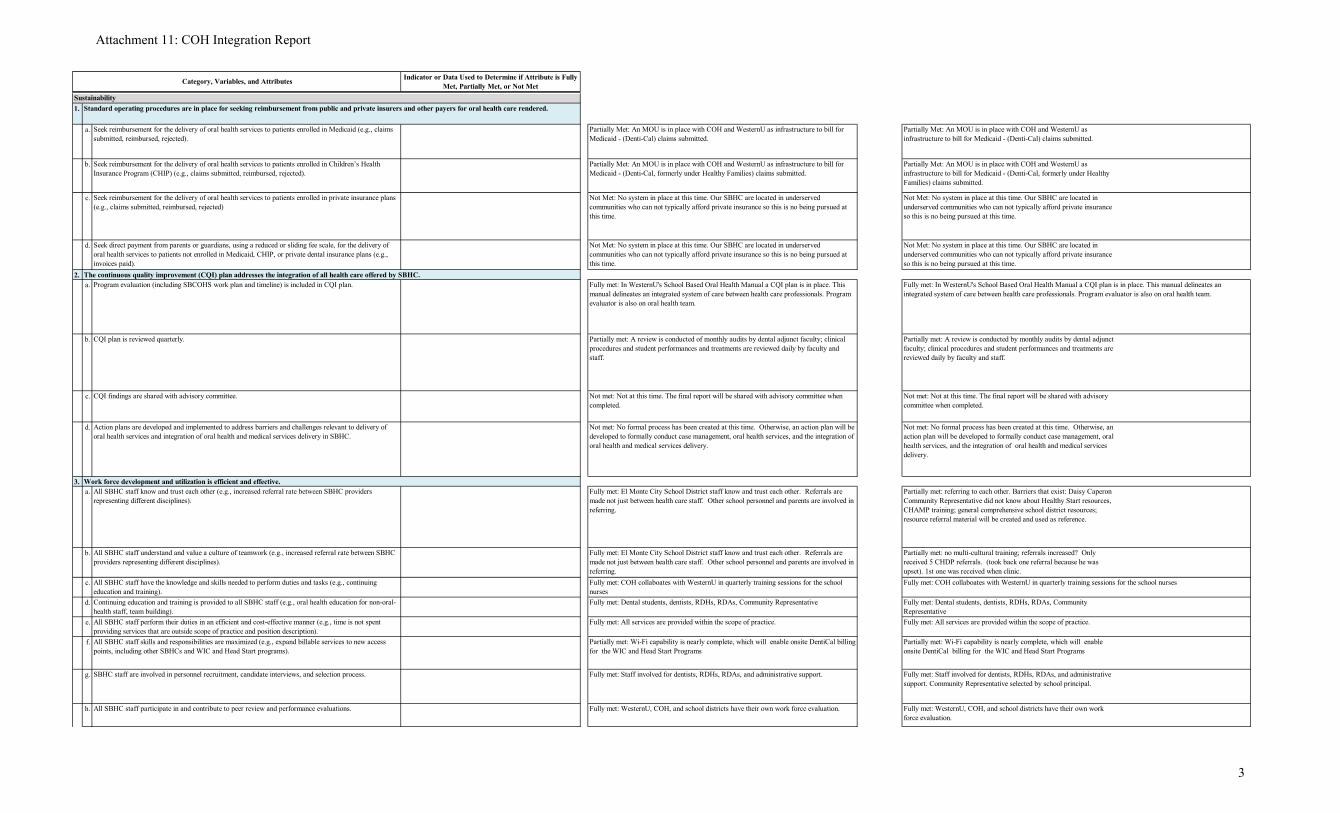
1.
a. Seek reimbursement for the delivery of oral health services to patients enrolled in Medicaid (e.g., claims submitted, reimbursed, rejected).
Partially Met: An MOU is in place with COH and WesternU as infrastructure to bill for Medicaid - (Denti-Cal) claims submitted.
b. Seek reimbursement for the delivery of oral health services to patients enrolled in Children’s Health Insurance Program (CHIP) (e.g., claims submitted, reimbursed, rejected).
Partially Met: An MOU is in place with COH and WesternU as infrastructure to bill for Medicaid - (Denti-Cal, formerly under Healthy Families) claims submitted.
c. Seek reimbursement for the delivery of oral health services to patients enrolled in private insurance plans (e.g., claims submitted, reimbursed, rejected)
Not Met: No system in place at this time. Our SBHC are located in underserved communities who can not typically afford private insurance so this is no being pursued at this time.
d. Seek direct payment from parents or guardians, using a reduced or sliding fee scale, for the delivery of oral health services to patients not enrolled in Medicaid, CHIP, or private dental insurance plans (e.g., invoices paid).
Not Met: No system in place at this time. Our SBHC are located in underserved communities who can not typically afford private insurance so this is no being pursued at this time.
2.a. Program evaluation (including SBCOHS work plan and timeline) is included in CQI plan.
b. CQI plan is reviewed quarterly. Partially met: A review is conducted by monthly audits by dental adjunct faculty; clinical procedures and student performances and treatments are reviewed daily by faculty and staff.
c. CQI findings are shared with advisory committee. Not met: Not at this time. The final report will be shared with advisory committee when completed.
d. Action plans are developed and implemented to address barriers and challenges relevant to delivery of oral health services and integration of oral health and medical services delivery in SBHC.
Not met: No formal process has been created at this time. Otherwise, an action plan will be developed to formally conduct case management, oral health services, and the integration of oral health and medical services delivery.
3.a. All SBHC staff know and trust each other (e.g., increased referral rate between SBHC providers
representing different disciplines).Partially met: referring to each other. Barriers that exist: Daisy Caperon Community Representative did not know about Healthy Start resources, CHAMP training; general comprehensive school district resources; resource referral material will be created and used as reference.
b. All SBHC staff understand and value a culture of teamwork (e.g., increased referral rate between SBHC providers representing different disciplines).
Partially met: no multi-cultural training; referrals increased? Only received 5 CHDP referrals. (took back one referral because he was upset). 1st one was received when clinic.
c. All SBHC staff have the knowledge and skills needed to perform duties and tasks (e.g., continuing education and training).
d. Continuing education and training is provided to all SBHC staff (e.g., oral health education for non-oral-health staff, team building).
Fully met: Dental students, dentists, RDHs, RDAs, Community Representative
e. All SBHC staff perform their duties in an efficient and cost-effective manner (e.g., time is not spent providing services that are outside scope of practice and position description).
Fully met: All services are provided within the scope of practice.
f. All SBHC staff skills and responsibilities are maximized (e.g., expand billable services to new access points, including other SBHCs and WIC and Head Start programs).
Partially met: Wi-Fi capability is nearly complete, which will enable onsite DentiCal billing for the WIC and Head Start Programs
g. SBHC staff are involved in personnel recruitment, candidate interviews, and selection process. Fully met: Staff involved for dentists, RDHs, RDAs, and administrative support. Community Representative selected by school principal.
h. All SBHC staff participate in and contribute to peer review and performance evaluations. Fully met: WesternU, COH, and school districts have their own work force evaluation.
Fully met: In WesternU's School Based Oral Health Manual a CQI plan is in place. This manual delineates an integrated system of care between health care professionals. Program evaluator is also on oral health team.
Fully met: COH collaboates with WesternU in quarterly training sessions for the school nurses
The continuous quality improvement (CQI) plan addresses the integration of all health care offered by SBHC.
Work force development and utilization is efficient and effective.
Standard operating procedures are in place for seeking reimbursement from public and private insurers and other payers for oral health care rendered.Sustainability
Not Met: No system in place at this time. Our SBHC are located in underserved communities who can not typically afford private insurance so this is no being pursued at this time.
Fully met: In WesternU's School Based Oral Health Manual a CQI plan is in place. This manual delineates an integrated system of care between health care professionals. Program evaluator is also on oral health team.
Partially met: A review is conducted of monthly audits by dental adjunct faculty; clinical procedures and student performances and treatments are reviewed daily by faculty and staff.
Not met: Not at this time. The final report will be shared with advisory committee when completed.
Not met: No formal process has been created at this time. Otherwise, an action plan will be developed to formally conduct case management, oral health services, and the integration of oral health and medical services delivery.
Partially Met: An MOU is in place with COH and WesternU as infrastructure to bill for Medicaid - (Denti-Cal) claims submitted.
Partially Met: An MOU is in place with COH and WesternU as infrastructure to bill for Medicaid - (Denti-Cal, formerly under Healthy Families) claims submitted.
Not Met: No system in place at this time. Our SBHC are located in underserved communities who can not typically afford private insurance so this is no being pursued at this time.
Partially met: Wi-Fi capability is nearly complete, which will enable onsite DentiCal billing for the WIC and Head Start Programs
Fully met: Staff involved for dentists, RDHs, RDAs, and administrative support.
Fully met: WesternU, COH, and school districts have their own work force evaluation.
Fully met: El Monte City School District staff know and trust each other. Referrals are made not just between health care staff. Other school personnel and parents are involved in referring.
Fully met: El Monte City School District staff know and trust each other. Referrals are made not just between health care staff. Other school personnel and parents are involved in referring. Fully met: COH collaboates with WesternU in quarterly training sessions for the school nurses Fully met: Dental students, dentists, RDHs, RDAs, Community Representative
Fully met: All services are provided within the scope of practice.
Attachment 11: COH Integration Report
3

Category, Variables, and Attributes
Delivery-System Design
Indicator or Data Used to Determine if Attribute is Fully Met, Partially Met, or Not Met
i. Orientation for new employees provides training on the importance of oral health to overall health and well-being.
Fully met: SBHC staff and dental staff trained to educated population.Fully met: SBHC staff and dental staff trained to educated population.
Attachment 11: COH Integration Report
4

Appendix A Spatial Analysis Used to Identify Additional Feeder Schools and Potential Clinic Sites
Iden%fying*Need*and*Loca%on*for*Services**
47*
Spa%al*analysis*conducted**• Loca%on*(s)**iden%fied**• Coordina%on*with:**
• Head*Start*programs*• Early*Educa%on*Centers*• WICs*• Schools*• Hospitals*• Dental*providers*• Other*community*agencies*• Community*health*navigators*

APPENDIX A Continuous Quality Improvement Plan - Grant Number: H47MC23162
The Center for Oral Health Dental Management Team will take the lead in implementing the CQI Plan for the dental component of the two LAUSD SBHCs. The methodology that will be used to assess continuous quality improvement will include five specific program areas: 1) quality of program administration; 2) quality of patient care; 3) regulatory adherence; 4) optimization of California Medicaid and CHIP dental billing; and the 5) dental program business plan.
1. Program Quality –Programmatic Administration
The assessment of programmatic administration will include measures that fall into five categories identified by the Association of State and Territorial Dental Directors (ASTDD) Best Practices Project.1 The Best Practices for State and Community Oral Health Programs: School- Based Dental Sealant Programs2 lists the following review criteria for program planning and evaluation: Impact, Effectiveness/Efficiency, Demonstrated Sustainability, Collaboration/Integration and Objectives/Rationale. The following measures have been incorporated into this evaluation: Impact
Program Data: Student population and program data will be gathered from school, SBHC and patient records. Measures included: • percentage of children eligible for Free and Reduced Lunch Program by school; • number and percentage of children whose parents provided informed consent; • number and percentage of children who actually participated; • number and percentage of children who received at least one dental sealant; • number and percentage of children who presented with urgent needs; • number and percentage of children referred for follow-up • number and percentage of children who had documented treatment completed
Effectiveness
Technical Quality: A two step process will be undertaken by program evaluators to ascertain the technical (clinical) quality of the program and patient services. First, patient records will be reviewed and information relative to health status and services data will be collected. This information will be compared to data subsequently collected by the evaluators during on-site, school-based intra-oral examinations. Comparison data will include: • untreated dental decay • teeth needing urgent care • sealant information: intact; partially intact; not present
Quality Assurance: Two checklists, derived from a variety of key clinical resources3,4 have been 1AssociationofStateandTerritorialDentalDirectors.BestPracticesProject.http://www.astdd.org/index.php?template=bestpractices.html
2AssociationofStateandTerritorialDentalDirectors.BestPracticesProject.SchoolBasedDentalSealantsPrograms.http://www.astdd.org/school-based-dental-sealant-programs/3Massachusetts’CollegeofPharmacyandHealthSciences,ForsythSchoolofDentalHygiene’s2009PolicyandProcedureManual
4CommonwealthMobileOralHealthServicesProgramPolicyandProcedureManual

APPENDIX A Continuous Quality Improvement Plan - Grant Number: H47MC23162
drafted. The purpose of these checklists is to assess policies, standard operating procedures and practices related to: Quality Assurance: Two checklists, derived from a variety of key clinical resources5,6 have been drafted. The purpose of these checklists is to assess policies, standard operating procedures and practices related to: 1) general program administration; and 2) treatment services and documentation. These items will be either integrated or cross-referenced with the existing SBHC QA program. The following items are included in the checklists: General Program Treatment Services and Documentation · Anti-DiscriminationPolicy· StudentswithDisabilities· MissionStatement;ProgramGoalsand
Objectives· PrinciplesofPractice· ServicesProvided· ScheduleofOperation:Months/Hours· AfterHourCoverage· CancellationPolicy· FeeSchedule· NoticeofPatientRights· ConfidentialityStatement· ReleaseofInformation· PatientComplaintsandIncidents· HandlingofSuspectedChildAbuse· MedicalEmergencies· EmergencyContactNumbers· FirstAid/MedicalEmergencyForm· EmergencyMedical/PersonnelRoles· MedicalEmergencyResponsePlan· MOAwithLocalProviders· LinkagetoaDentalHome· Student/PatientAppointments· Student/PatientAppointmentScheduling· RolesandResponsibilitiesofProgramStaff· ProfessionalAttireandBehavior· Licensure/certificationofprogramstaff
· ContinuousQualityAssurance· CORI· InformedConsent· MobileClinicSet-upandBreakdown· ComprehensiveDentalExamination· HealthStatus-DiagnosisDocumentation· TreatmentPlan· DispositionofPatient· Prophylaxis· FluorideTreatment· DentalSealants· TemporaryRestorations· ADA,AAPDProf.Guidelines· TreatmentNotes:· ParentalReports· MedicalRecordsandStorage· SchoolReports· UrgentCareReferral· Non-urgentCareReferral· Follow-up· RecordDocumentation· DataProcessing· PublicandPrivateInsuranceBilling· InfectionControl· SharpsInjuryandBloodbornePathogen· SharpsInjury/PostExposureFollow-up· WasteManagement
Efficiency Two measures will be used to assess the overall efficiency of the program:
5Massachusetts’CollegeofPharmacyandHealthSciences,ForsythSchoolofDentalHygiene’s2009PolicyandProcedureManual
6CommonwealthMobileOralHealthServicesProgramPolicyandProcedureManual

APPENDIX A Continuous Quality Improvement Plan - Grant Number: H47MC23162
• Adequate number children who utilize dental services within the SBHC. • Medicaid reimbursements sufficient to sustain the program
Demonstrated Sustainability To measure the viability and ongoing sustainability of the program, a comprehensive analysis of the current operating budget, income, expenses, mechanisms for billing and managing accounts receivable and personnel management will be conducted.
Collaboration/Integration To measure the strength of the collaborative arrangement between COH, LAUSD and the Murchison and Plasencia SBHC, MOUs and contracts will be current, signed and on file. : • Current documented MOUs and/or contracts on file
Objectives/Rationale Evaluators will assess the degree to which the program’s goals and objectives are linked to state and/or national oral health goals and objectives. The measures used to assess this criterion include Healthy People 2020 National Oral Health Objectives: • OH 2.1; OH2.2; OH 2.3 Reduce the proportion of children, adolescents with untreated
dental decay.
2. Program Quality—Patient Care To assess the quality of patient care, the proposed measures were derived from a report published in the Institute of Medicine entitled, Crossing the Quality Chasm: A New Health System for the 21st Century.7 The IOM Report identifies six “aims” from which to assess patient care. The following measures were developed within the framework of those six aims:
Safe
• Patient or provider injuries noted • Details of the incident(s) documented • Corrective action taken and noted • California dental regulations followed related to provider scope to
practice/ services • AAPD and ADA Clinical Guidelines and standards of care followed • CDC Infection Control Guidelines followed • HIPAA regulations followed
Effective • Services provided are evidenced-based • AAPD and ADA clinical guidelines and recommendations followed • Target highest need, at-risk populations
7InstituteofMedicine.CrossingtheQualityChasm:ANewHealthSystemforthe21stCentury.Washington:NationalAcademyPress;2005

APPENDIX A Continuous Quality Improvement Plan - Grant Number: H47MC23162
Patient Centered • Evidence of informed consent obtained and documented • Evidence of parent input documented i.e. parent satisfaction survey • Culturally and linguistically appropriate materials
Timely • Time out of classroom is limited to 30 minutes • Waiting time is less than ten minutes
Efficient • Need to repeat sealant application less than or equal to 10% • Efficient use of manpower to impact the greatest number of children • Treatment plans are completed within 6 months of dental
examination
Equitable • All children within the selected schools are invited to participate • All services offered comply with professional standards of care • All children/schools are offered the same services
3. Regulatory Adherence Evaluators will assess the degree to which program administrators adhere to state and federal regulations regarding Medicaid and CHIP billing. Claims data will be used for this analysis. CDT procedure codes D0001 through D9999. The following specific queries will be used: D0150 – Comprehensive Dental Examination; D1203 – Topical application of fluoride (child); D1206 – Topical fluoride varnish; D1351 – Dental sealant; D2940 – Sedative filling; and D2999 – Unspecified restorative procedure by report. Other regulatory adherence will be evaluated and included in the results section under “Assessment of Patient Care.” 4. Optimization of California Medicaid/CHIP Billing To assess the optimization of Medicaid/CHIP billing practices and potential loss in billing revenue, the evaluators will look at several key factors:
• Actual frequency of services billed • Actual collections by child per month • Reimbursement costs for dental prophylaxis not billed by number of children who had received at least one dental service (i.e. lack of insurance; inability to pay; eligibility issues) • Timeliness of billing Medicaid in relation to date services were performed • Appropriate use of CDT codes

The Center For Oral Health
SBOHC Operations Manual
The Center For Oral Health SBOHC Operations Manual
Table of Contents
Introduction ............................................................................................ 3-‐ 5 Letter From Executive Director .................................................................... 6
School Based Oral Health Clinics General Information ....................... 7-‐ 12
Setting Up Facility ............................................................................ 13-‐ 23
Common Procedure ........................................................................ 24-‐ 32
Procedure Outcome ......................................................................... 33-‐ 35
Daily Operations ............................................................................... 36-‐ 46
Finance ............................................................................................. 45-‐ 57
Evaluation ........................................................................................ 58-‐ 62
Marketing ........................................................................................ 63-‐ 66
Policy, Licenses, Safety Compliance, and Taxes .............................. 67-‐ 78
Fire, Earthquake, and Natural Disaster Protocols ........................... 79-‐ 82
Appendix A-‐ Setting up Facility ........................................................ 83-‐ 97
Appendix B-‐ Daily Operations ........................................................ 98-‐ 116
Appendix C-‐ Finance Policies ...................................................... 117-‐ 123
Appendix D-‐ Evaluation .............................................................. 124-‐ 125
Appendix E-‐ Marketing ................................................................ 126-‐ 133
Appendix F-‐ Policy, Licenses, Safety Compliance, and Taxes ...... 134-‐ 138
Appendix G-‐ Fire, Earthquake, and Natural Disaster Protocols .. 139-‐ 140
References & Credits .................................................................. 141-‐ 143

THE CENTER FOR ORAL HEALTH
3
Introduction Mission
Vision
Goals
The Center For Oral Health SBOHC Operations Manual
Welcome!
The Center for Oral Health (COH), founded in 1985, is a non-‐profit organization dedicated to promoting public oral health, with a focus on children and vulnerable populations. COH collaborates with national, state, and local partners to develop innovative community-‐based strategies for improving oral health outcomes. COH has offices in Northern and Southern California. The need for oral health care is the most prevalent unmet health care need among Children and Adolescents.1 Despite interest and advances in disease prevention, dental caries continues to take a heavy toll on a child’s health and well-‐being across all socioeconomic, racial, and ethnic groups. However, It remains the highest among children in lower-‐economic environments.2 COH has developed an Operation’s Manual for the integration of comprehensive oral health care-‐ School-‐Based Oral Health Clinic’s (SBOHC). This manual will educate healthcare providers on how to startup a sustainable and fiscally responsible school-‐based oral health clinic, based on a 70% (at least) Medicaid (Denti-‐Cal) patient index and is specific to the State of California. However the business manual can be tailored to other states and accessible to both public and private Oral Health Organizations/Professionals across the nation whom are interested in starting and facilitating a sustainable SBOHC. Vision:
The Center For Oral Health-‐ SBOHC will be a premier center for integrative education and innovation; creation of high-‐quality, accessible, affordable, patient-‐centered, interprofessional oral health programs that document the improvement of the oral health status of patients, while being financially responsible.
Mission:
Our Mission is to improve oral health, especially of vulnerable populations, through innovation, research, education and advocacy.
Goals:
Center For Oral Health-‐ SBOHC’s work will focus on four goals, in order to achieve our
1 Newacheck PW, McManu M, Foz HB, Hung YY, Halfon N. 2000. Access to health care for children with special health care needs. Pediatrics 105(4 Pt 1):760-‐766. 2 Center For Oral Health. 2014. HRSA Final Modified

THE CENTER FOR ORAL HEALTH
5
vision and execute our mission:
A. Engage and encourage California Residents whom are eligible for Denti-‐Cal, according to the Federal Poverty Level Eligibility Standards, to increase their oral health knowledge and optimum health outcomes
B. Address the oral health needs of pre-‐school, elementary, and middle-‐school children in underserved communities within the State of California, including children with Medicaid and or Children’s Health Insurance Program (CHIP)
C. Demonstrate a successful integration of cultural competence, nutrition and oral health education, and comprehensive oral health services in all School Based Oral Health Clinics
D. Create a sustainable and permanent dental home for children ages 0-‐14 years of age, whom reside in California at one of our School Based Oral Health Clinics
The Center For Oral Health SBOHC Operations Manual
Letter from Conrado E. Barzaga, MD, Executive Director, Center for Oral Health
Dear community partners,
The Center for Oral Health is pleased to present this school-based oral health program operation manual. Led by dedicated dental professionals, progress is being made, school district by school district across the country on the path to ending dental disease among underserved children. These successes show that it’s possible to offer high quality of dental care for all children.
The reality of no children without dental care is something we can and will achieve; yet we know some of our most vulnerable families are most affected by the lack of dental care. This is why the Center for Oral Health is working to expand the capacity to effectively offer dental care in a sustainable way.
This school-based oral health program operation manual is designed just for you: Use it to learn what the Center for Oral Health has learned about school-based oral health programs to end dental disease among children and how to get involved. This manual contains information, fact sheets and other resources to help you advance your program, work with school districts, understand the financial demands of school-based programs, the public policies that help ensure the quality of these programs, and how to effectively run the program to ensure its viability.
No organization can eliminate dental disease alone. We need everyone, particularly those clinics with the capacity to increase affordable dental care, to achieve this milestone. By expanding access to affordable dental care at school sites, you can make a difference.
Thank you for using and sharing the manual we now offer to you, and for your dedication to this important cause. Together, we can end dental diseases, one school at a time.
Sincerely,
Conrado E. Barzaga, MD Executive Director Center for Oral Health

THE CENTER FOR ORAL HEALTH
7
School Based Oral Health Clinics General
Information Who We Serve
Cost Effectiveness
Need For School Based Oral Health Clinics
Benefits of School Based Oral Health Clinics

The Center For Oral Health SBOHC Operations Manual
School Based Oral Health Clinics General Information
School Based Oral Health Clinics (SBOHC) are small dental clinics located in or near a School facility that specialize in preventative and comprehensive Oral Care for children 0-‐14 years old. SBOHC’s are responsible for Diagnostic Screenings and Comprehensive Procedures. For the purposes of this manual, we have based all our findings and recommendations off of the Los Angeles Unified School District (LAUSD)-‐ Murchison Street Elementary School 2010-‐2014 and El Monte City School District (EMCSD)-‐ Gidley Elementary School 2012-‐2014 SBOHC Frequency Statistics and Operation Procedures. Who We Serve: The SBOHC’s Principles of Practice are to establish dental homes for children enrolled in a primary education institution. The Center For Oral Health-‐ SBOHC’s serve patients 0-‐14 years of age in the State of California, for comprehensive care and treatment. Furthermore, all children within the school and in its surrounding areas will be seen irrespective of their family’s ability to pay. No child will be refused treatment for any emergency and urgent care. Comprehensive dental care will be available for every child & used on a case-‐by-‐case basis depending on need. 3 On a case-‐by-‐case basis, as well as for emergencies only, SBOHC’s will open the dental clinic to individuals 15+. All emergency patients will need to complete the full patient registration forms, and will minimally be screened and diagnosed through visual and radiographic interpretation. If a patient cannot be treated at a SBOHC site, the patient will be referred to another dental clinic. Cost Effectiveness: School Based Oral Health Clinics have allowed dental professionals to expand the types of services provided to local low-‐income residents in a cost effective manner. These services benefit the Dentist, Public Schools and Low-‐Income families whom are seen at a SBOHC. When working at a SBOHC, the Dentist has significantly low start-‐up and operating costs compared to a brick and mortar Dental Clinic. SBOHC’s allow children direct access to dental services without having to leave their primary education
3http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf
THE CENTER FOR ORAL HEALTH
9
institution. Which in thus, increases the school’s Average Daily Attendance (ADA) score. A schools’ ADA score dictates the amount of revenue the school receives from their district. Acute pain caused by dental caries have a strong effect on children and their families. Early tooth loss caused by tooth decay can result in failure to thrive, impaired speech development, and reduced self-‐esteem.4 Children are often unable to verbalize their oral pain, therefore regular dental check-‐ups are very important for young children. 5 Children and adolescents with poor oral health status’s are more likely to experience oral pain, miss school, and perform poorly in school compared to their peers whom have better oral health. Among elementary and high school students from families with low incomes, those with toothaches in the last 6 months are almost four times as likely as those without toothaches in the last 6 months to have a grade point average below 2.8. When children’s acute oral health problems are treated, their learning and school-‐attendance records improve. 6 Need for School Based Oral Health Clinics: A decade ago, dental caries and access to oral health care on a national level was identified as a critical need and serious problem with the landmark release of the 2000 Surgeon’s General Report on Oral Health. In particular, the report summarized that dental caries is one of the most common diseases among children and adolescents ages 5 to 17 years old, occurring far more frequently than asthma or hay fever. The Surgeon General subsequently released a Call for Action, to “promote access to oral health care for all Americans, especially the disadvantaged and minority children found to be at greatest risk for severe medical complications resulting from minimal oral care and treatment.” 7
The rate of dental caries among the general population has decreased significantly over the past two decades. But the more recent 2007 CDC report entitled, Tends in Oral Health Status: United States, 1988-‐1994 and 1999-‐2004 revealed that the disease particularly among children ages 2-‐5 is on the rise again. Data from the third National Health and Nutrition Examination Survey (NHANES III), 1988-‐1994 and 1999-‐2004
4 U.S Department of Health and Human Services. 200. Healthy People 2010 Objectives for improving Health: Focus Area 21—Oral Health. Washington, DC: US. Department of Health and Human Services. http://dx.doiorg/10.1016/j.jpeds.2012.05.025 5 Ramage S. 2000. The impact of dental disease on school performance: The view of the school nurse. Journal of the Southeastern Society of Pediatric Dentistry 6(2):26 6 Seirawan H, Faust S, Muligan R. 2012. The impact of oral health on the academic performance of disadvantaged children. American Journal of Public Health 102(9):1729-‐1734 http://ajph.aphapublications.org/doi/abs/10.2105/AJPH.2011.300478. 7U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health 2000.
The Center For Oral Health SBOHC Operations Manual
revealed a 15.2% rise in dental caries prevalence among this cohort during the indicated time period. 8 The reasons for this increase are unknown, but it is speculated that the increased use of bottled waters, lack of community water fluoridation and changes in demographics nationwide may be contributing factors.
In addition, untreated dental caries continues to exist in school-‐aged children and adolescent youth, especially those who have not had earlier access to fluoride, preventive dental sealants or a dental home. Data from the third National Health and Nutrition Examination Survey (NHANES III), 1988-‐1994 and 1999-‐2004 reveal rates of untreated caries in children ages 2-‐4 at 16.26%, ages 6-‐8 at 28.45% and 12-‐15 at 17.87% respectively. More needs to be done to address these treatment needs and increase access to comprehensive oral health care services.9
National and Statewide Perspective
Access to oral health care is not evenly distributed among people living in the United States. People who are poor are less likely to receive dental care. A decade ago only one third of children living at or below the federal poverty level visited a dentist in the past year, compared to 70% of children living in families with incomes over 400% of the federal Poverty level.10 Recent needs assessments on a national level have clearly documented that the disparities in the receipt of oral health care services are particularly problematic with certain populations; these populations include low-‐income rural and urban residents, minority groups and disadvantaged, low-‐income youth.
The state of California is not immune from these national statistics and recent studies have verified that oral health access remains high on the priority list for overall health care services. The study “Mommy Hurts to Chew,” conducted in 2006 by Dental Health Foundation assessed the oral health of California’s 3rd graders with the result that the oral health of California’s children is substantially worse than national objectives set forth by Healthy People 2010. Additionally, this same study found that of 25 states surveyed, only Arkansas ranked below California in kids’ dental health11
Local Perspective:
The presence of factors and determinations that are known to be associated with high rates of dental disease include lower socio-‐economic communities and children from racial and ethnic minority groups. LAUSD serves some of the most underserved communities in the nation. The critical role of the SBOHC is to service children in an area designated as extremely “high need” and “underserved”. Targeted school areas are in medically underserved areas, primary care health professional shortage areas and or 8 Plan and operation of the Third National Health and Nutrition Examination Survey, 1988-‐94. National Center for Health Statistics. Vital Health Stat 1 (32). 1994 9 Dental Health Foundation DBA the Center For Oral Health 10 U.S. General Accounting Office. Oral Health: Dental Disease is a Chronic Problem Among Low-‐Income and Vulnerable Populations. DC: U.S. General Accounting Office, 2000. 11 Dental Health Foundation. Mommy, It Hurts to Chew. Oakland, CA: Dental Health Foundation, 2006
THE CENTER FOR ORAL HEALTH
11
both.12
LAUSD students come from largely Hispanic and presumably recent-‐immigrant families. There is also significant poverty among students, with the vast majority participating in the Free Lunch Program-‐ Families with incomes below 133% Federal Poverty Level. The students in these targeted school areas are higher risk than the state average in every health indicator used in needs assessments. Because of this striking disparity, these low-‐income children are at risk for dental caries and would benefit from the delivery of comprehensive oral health services at an their established school. 13
Compelling evidence contained in the annual 2009-‐2010 Murchison Street Elementary SBOHC, validate the critical need for comprehensive oral health care services among children enrolled in this center. Of the 3,951 visits to LAUSD-‐ Murchison Street Elementary school in 2009-‐2010, 1314 of those visits involved a dental screening. Of those, 684 children presented with dental caries and 827 had notable poor oral hygiene and or gingivitis. In 2013-‐2014 EMCSD-‐Gidley Elementary School saw a total of 1,811 visits, 1518 of those visits involved Children. 84% of all procedures done at EMCSD-‐ Gidley Elementary School were Preventive and Diagnostic. This data represents a subset of the actual need, as dental screenings were not provided to all enrolled children of the SBOHC.
The California School Board Association: The California School Boards Association and the Dental Health Foundation have created a guidebook, Integrating Oral Health into School Health Programs and Policies, to serve as a comprehensive approach to oral health education policy in schools. The primary objectives are to educate school board members and communities on the critical link between oral health and academic achievement, develop a policy framework that supports local organization and solutions, share knowledge of best oral health practices in school, encourage school-‐based oral health projects and partnerships in local communities, develop a comprehensive guide to oral health community services. (Available at: http://www.cenerfororalhealth.org/index-‐new.html)
Benefits of School Based Oral Health Clinics: School-‐based dental programs are especially important for reaching children from low-‐income families, who are less likely to receive private dental care. 14 School Based Oral Health Clinics provide the following: 12 Dental Health Foundation DBA the Center For Oral Health 13 Los Angeles Unified School District: Student Medical Services. School Health Center Demographics. Los Angeles, CA: Los Angeles Unified School District 14 http://www.cdc.gov/oralhealth/dental_sealant_program/

The Center For Oral Health SBOHC Operations Manual
A. Oral health hygiene instruction B. Increased School ADA score C. Reduces economic lose for Students and their family; due to no lose in school
absenteeism and work day productivity D. Screen low income children (twice a year) to detect signs of dental disease

THE CENTER FOR ORAL HEALTH
13
Setting Up Facility Site Selection Process
Program Staff
Start-‐Up and Operation Costs
Supplies & Equipment

The Center For Oral Health SBOHC Operations Manual
Setting Up Facility
Starting a SBOHC can be challenging, however once up and running the benefits will outweigh the challenges -‐ both financially and personally. Center for Oral Health’s SBOHC Operations Manual is meant to guide Dental Directors through the Start-‐up process and help answer many of their questions. This section, “Setting Up Facility” will help Dental Directors with selecting and securing a school home, staff requirements, start-‐up and operation costs, as well as choosing the appropriate supplies & equipment.
Site Selection Process: Locate A School Home Dental Directors should locate Five Potential Elementary Schools, no more than 10 miles from their primary practice. We recommend that Dental Directors select at least five potential schools, because it may take a few tries to convince/show school administration the importance of your program.
Selected schools should have a population of 350 students or more and at least 70% of its students should be enrolled in the “Free and Reduced Meal” program. Ideally SBOHC sites should have a Child Health and Disability Program (CHDP).
Policies and Procedures For SBOHC Selection Once the Dental Director has selected five potential elementary schools, he/she will need to initiate contact. The best persons to contact would be the principle of each school and the Districts Superintendent. The following maps out the appropriate steps a Dental Director would need to follow, in order to make initial contact with potential Schools.
A. Obtain School District Organizational Chart
B. Obtain School District Directory I. Human Services Division Directory
C. Contact Key People to Introduce SBOHC’s: I. Principle/Superintendent II. School Nurse and or School Health Professionals III. Student Health and Human Services Division Directors -‐Organization
Facilitator, Oral Health Nurse Children’s Health access and Denti-‐Cal Program (CAMP)
IV. Whoever Dental Director has a connection with in their selected School

THE CENTER FOR ORAL HEALTH
15
District
D. Schedule a meeting with Superintendent I. Present PowerPoint-‐ benefits of program II. Give Program Information Handout
E. Once a particular school is interested, start negotiation process and create a Memorandum of Understanding (MOU) for SBOHC Site
I. Terms of Agreement II. Location III. Description of Services IV. Access to Services V. Informed Consent of Parents VI. Communication between Provider and School/District VII. Hours of Service VIII. Non-‐Discrimination in Services IX. Staffing X. Non-‐discrimination in Employment XI. Conflict of Interest XII. Performance Goals XIII. Quality Assurance/Quality Improvement XIV. Community Participation XV. Furnishings and Equipment XVI. Bio-‐Hazardous Waste XVII. Public Health Reporting Requirements XVIII. Public Announcements and Literature XIX. Insurance XX. General Indemnity XXI. Charges for Clinic Services XXII. Financial Responsibility and Support XXIII. Reports & Records XXIV. Government Requirements XXV. Delegation and Assignment XXVI. Termination XXVII. Arbitration XXVIII. Amendments XXIX. Debarment, Suspension, or ineligibility for award XXX. Confidentiality of Agreement XXXI. Governing Laws, Jurisdiction and Venue XXXII. Authority
F. Service Delivery Application
I. TB Tests within 6 Months of Start Date II. California Department of Justice Check Background Check (DOJ)

The Center For Oral Health SBOHC Operations Manual
III. License Number-‐ From Doing Business As (DBA) IV. Resume/CV
G. Final Signature from Superintendent Tip: Section A-‐E will take a Minimum of 3-‐6 months to Complete
H. Discuss Appropriate Room Space with School’s Principle I. Hire Staff and Buy Equipment, refer to “Setting Up Facility-‐ Program Staff & Equipment” J. Start Advertising SBOHC; refer to “Marketing” Section
Locate Appropriate Room A SBOHC’s location should be in an open operatory room with signs indicating its site. Portable units are self-‐contained, but for sanitary reasons SBOHC sites much have running water and drainage. This room must also be equipped with electricity. Unused classrooms are ideal, however a nursing office or storage area would suffice.
Program Staff:
The following lists the roles and responsibilities of a 2-‐Chair SBOHC staff. All Job Descriptions are gathered from the American Dental Association. 15 Dental Director Education Requirements Healthcare professionals are required to have an advanced university degree in a field relevant to the work of The Center For Oral Health-‐ SBOHC Required Credentialing
• Valid California Dental License • Current CPR Certification • Current DEA Certification • National Provider Identifier (NPI) • Proof of Hepatitis B Vaccination or Declination Statement • Tuberculosis Skin Test results and follow-‐up needs on file • Other Vaccinations as required
Language Requirements Proficiency in English and sites Threshold Language is required.
15 American Dental Association Website-‐ http://www.ada.org/en/

THE CENTER FOR ORAL HEALTH
17
“Threshold Language” means a language identified as the primary language, as indicated on the Medicaid Eligibility Data System (MEDS), of 3,000 beneficiaries or five percent of the beneficiary population, whichever is lower, in an identified geographic area. Knowledge of the local language of the SBOHC site where the position is located in is an asset to the clinic and patients. Duties and Responsibilities -‐ Oversee the entire SBOHC including all front and back office personnel -‐ Responsible for evaluating the quality of care provided by staff -‐ Implement the Quality Assurance plan, which include but not limited to -‐ Chart Audits -‐ X-‐Ray radiation inspections -‐ Spore test review -‐ Updates in dental materials and procedures -‐ Testing of the Medical Emergency Response Equipment -‐ Guiding Registered Dental Assistant and completing procedures if needed -‐ Reviewing and signing progress notes at the conclusion of the patient treatment -‐ Assisting with Scheduling, Patient Conflicts, and Referrals Registered Dental Assistant Education Requirements Healthcare professionals are required to have an advanced university degree in a field relevant to the work of The Center For Oral Health-‐ SBOHC Required Credentialing
• Valid California Dental Hygiene License • Current CPR Certification • Proof of Hepatitis B Vaccination or Declination Statement • Tuberculosis Skin Test results and follow-‐up needs on file • Other Vaccinations as required
Language Requirements Proficiency in English and sites Threshold Language is required. “Threshold Language” means a language identified as the primary language, as indicated on the Medicaid Eligibility Data System (MEDS), of 3,000 beneficiaries or five percent of the beneficiary population, whichever is lower, in an identified geographic area. Knowledge of the local language of the SBOHC site where the position is located in is an asset to the clinic and patients Duties and Responsibilities

The Center For Oral Health SBOHC Operations Manual
-‐ Organization of inventory and stocking of dental materials, disposables, and instruments -‐ Dental material, sterilization, daily clinic spore tests, radiology compliance, OSHA and infection control compliance -‐ Maintain the Medical Emergency cart (Emergency First Aid Kit, Blood Pressure cuff/Machine) and Oxygen tank -‐ Maintenance and repair of all machinery including but not limited to -‐ Nomad (Portable X-‐Ray unit) -‐ X-‐Ray sensors -‐ Portable equipment -‐ Dental chairs -‐ Ultrasonic -‐ Autoclave -‐ Transportation of Nomad Between SBOHC locations -‐ Performing all CDA approval RDA duties as needed -‐ Responsible for but not limited to -‐ Assisting Faculty Preceptors -‐ Taking Radiographs -‐ Sterilizing Equipment -‐ Re-‐Stocking -‐ Organizing -‐ Translate Site Coordinator Education Requirements Healthcare professionals are required to have an advanced university degree in a field relevant to the work of The Center For Oral Health-‐ SBOHC We recommend a minimum of a 2-‐year Associates Degree and School District Employee Required Credentialing
• Current CPR Certification • Proof of Hepatitis B Vaccination or Declination Statement • Tuberculosis Skin Test results and follow-‐up needs on file • Other Vaccinations as required
Language Requirements Proficiency in English and sites Threshold Language is required. “Threshold Language” means a language identified as the primary language, as indicated on the Medicaid Eligibility Data System (MEDS), of 3,000 beneficiaries or five percent of the beneficiary population, whichever is lower, in an identified geographic area. Knowledge of the local language of the SBOHC site where the position is located in is an asset to the clinic and patients.
THE CENTER FOR ORAL HEALTH
19
Duties and Responsibilities -‐ Upkeep of patient charts -‐ Recording of patient’s active/inactive status in the patient’s chart -‐ Random selection of charts for chart auditing by SBOHC Dental Director -‐ Maintaining the periodic or recall examination dates for all active patients -‐ Schedule Appointments -‐ Assisting with patient representatives who respond to patients’ issues and concerns as they arise within the SBOHC system -‐ Translate
Licensure/Certification of Program Staff All faculty, staff, and students are certified in the BLS and Medical Emergency training. Furthermore, prior to entering at the SBOHC, the faculty, staff, and student must be certified in HIPAA through an online course and pass the associated quiz. The faculty and staff are required to complete a FERPA course annually. Prior to entering the SBOHC-‐ all staff should be trained in OSHA and Infection Control through a combination of online resources and hands-‐on training. (See Section Documentation, Licenses, Permits, & Taxes) Start Up & Operation Costs: Dental Directors should use the following chart to determine Start-‐Up and Operation Costs. The Start-‐Up and Operation Costs Chart shows costs for a 2-‐Chair One-‐day (about 8 Hours) a week SBOHC. Reviewing this chart will enable Dental Directors to determine what size SBOHC facility they can afford to run and staff. Underlying Assumptions: No expenses required for rent, site maintenance, and or utilities. 2-‐Chair, about 8 hours a week.
The Center For Oral Health SBOHC Operations Manual
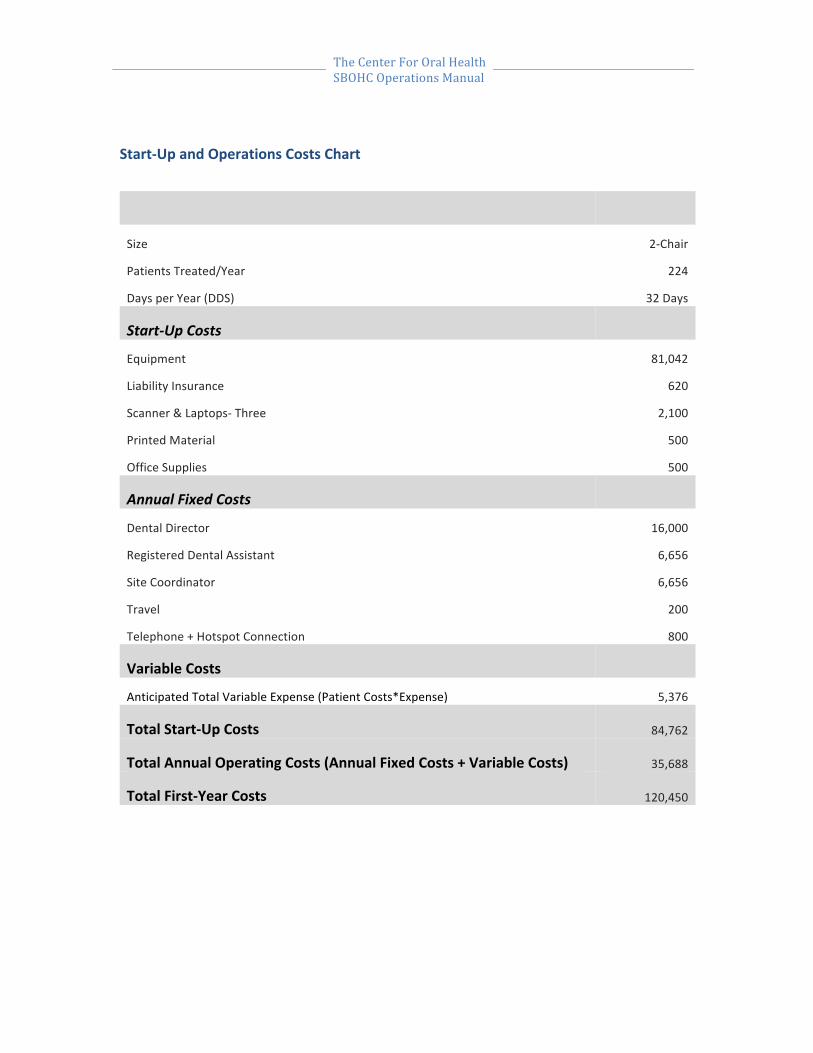
Start-‐Up and Operations Costs Chart
Size 2-‐Chair
Patients Treated/Year 224
Days per Year (DDS) 32 Days
Start-‐Up Costs
Equipment 81,042
Liability Insurance 620
Scanner & Laptops-‐ Three 2,100
Printed Material 500
Office Supplies 500
Annual Fixed Costs
Dental Director 16,000
Registered Dental Assistant 6,656
Site Coordinator 6,656
Travel 200
Telephone + Hotspot Connection 800
Variable Costs
Anticipated Total Variable Expense (Patient Costs*Expense) 5,376
Total Start-‐Up Costs 84,762
Total Annual Operating Costs (Annual Fixed Costs + Variable Costs) 35,688
Total First-‐Year Costs 120,450

THE CENTER FOR ORAL HEALTH
21
Supplies & Equipment: Each Dental Director will be responsible for obtaining Supplies & Equipment. The Supplies & Equipment purchased, will vary from site to site. Some Dental Directors may choose to use Supplies & Equipment from their private practice and purchase additional pieces as/if needed. For the purposes of this manual, we have based all our findings and recommendation off of the LAUSD-‐ Murchison Street Elementary School 2010-‐2014 and EMCSD-‐ Gidley Elementary School 2012-‐2014 SBOHC Supplies & Equipment List. Only material approved by the American Dental Associations Council on Dental Therapeutics may be used in SBOHC facilities. Portable Dental Delivery System Vendors 16
Manufacturer Website A-‐Dec Inc www.a-‐dec.com Aseptico www.aseptico.com ASI Medical Inc www.asimedical.net Bell Dental Products LLC www.belldental.com DNTL works www.DNTworks.com M-‐DEC www.portabledentistry.com Henry Schein www.henryschein.com Safari Dental www.safaridental.com A complete list of the various portable equipment products from these manufacturers can be seen on their Web sites. Additional resource information for dental suppliers and manufacturers can be found in the ADA's Dental Buying Guide.16 Characteristics For Choosing Portable Dental Equipment16
Transportability-‐ How easily it can be moved and utilized Durability-‐ Likelihood of malfunction because of constantly moving the units Ergonomic Characteristics-‐ Creation of an efficient working environment Delivery System Capabilities-‐ Capacity for effective dental treatment provision Infection Control-‐ Meeting OSHA’s requirements for cleanliness and asepsis Maintenance-‐ How to avoid “Downtime” Ease of Assembly/Disassembly-‐ Starting and Finishing Noise Level-‐ How loud is it and can it be modified
16 http://www.mobile-‐portabledentalmanual.com
The Center For Oral Health SBOHC Operations Manual
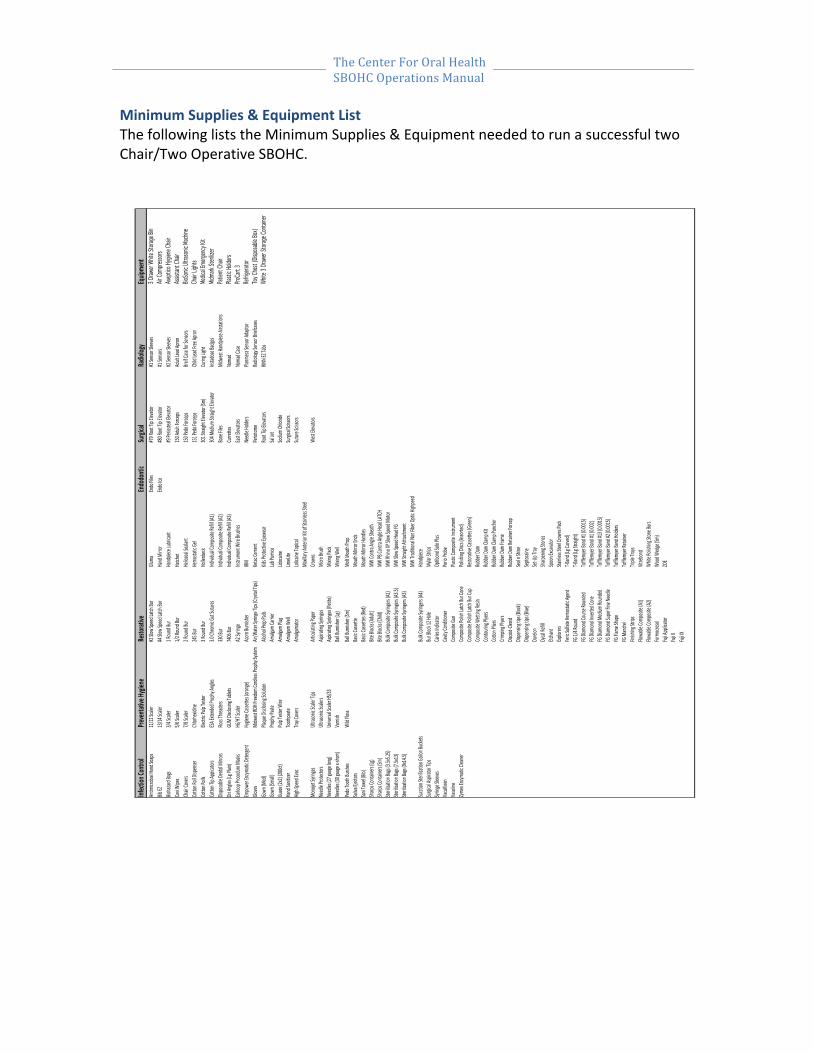
Minimum Supplies & Equipment List The following lists the Minimum Supplies & Equipment needed to run a successful two Chair/Two Operative SBOHC.
Infect
ion)Co
ntrol
Preven
tative
)Hygie
neRe
storat
iveEn
dodo
ntic
Surgi
calRa
diolog
yEq
uipme
ntAn
timicrob
ial,Ha
nd,So
aps
11/12
,Scale
r#2,Slo
w,Spe
ed,La
tch,Bu
rGlu
maEndo
,Files
#79,R
oot,T
ip,Elev
ator
#1,Se
nsor,S
leeves
3 Draw
er Wh
ite St
orage
BinBib
,EZ13
/14,Sc
aler
#4,Slo
w,Spe
ed,La
tch,Bu
rHa
nd,M
irror
Endo
,Ice#80,R
oot,T
ip,Elev
ator
#1,Se
nsors
Air Co
mpres
sors
Biohazar
d,Bags
3/4,Sc
aler
1,Rou
nd,Bu
rHa
ndpie
ce,Lub
ricant
#9,Pe
rioste
al,Elev
ator
#2,Se
nsor,S
leeves
Asept
ico Hy
giene
Chair
Cavi,W
ipes
5/6,Sc
aler
1/2,Ro
und,B
urHa
tchet
150,A
dult,F
orcep
sAd
ult,Le
ad,Ap
ronAs
sistan
t Chai
rCh
air,Co
vers
7/8,Sc
aler
2,Rou
nd,Bu
rHe
lioseal
,Seala
nt150,P
edo,F
orcep
sBre
if,Case
,for,S
ensor
sBio
Sonic
Ultra
sonic M
achine
Cotto
n,Roll,
Dispe
nser
Chlor
hexid
ine245,B
urHe
mosta
tic,Ge
l151,P
edo,F
orcep
sCh
ild,Lea
d,Free
,Apron
Chair
Lights
Cotto
n,Rolls
Electr
ic,Pulp
,Teste
r3,R
ound
,Bur
Hollen
beck
301,S
traigh
t,Elev
ator,(S
m)Cu
ring,L
ight
Medic
al Eme
rgency
Kit
Cotto
n,Tip,A
ppica
tors
ESA,Ex
tende
d,Prop
hy,An
gles
3.0,Ch
romic,G
ut,Sut
ures
Individ
ual,Co
mposi
te,Re
fill,(A1
)30
4,Med
ium,St
raight
,Elevat
orIns
tadose
,Badge
sMid
mark
Steriliz
erDis
posab
le,Den
tal,M
irrors
Floss,Threa
ders
330,B
urInd
ividual,Co
mposi
te,Re
fill,(A2
)Bo
ne,Fil
esMi
dwest
,Hand
piece,
Airsta
tions
Patien
t Chai
rDri
,Angle
s,(Lg,P
lain)
GUM,
Disclo
sing,T
ablet
s7406,Bu
rInd
ividual,Co
mposi
te,Re
fill,(A3
)Cu
rrette
sNo
mad
Plastic
Holde
rsEar
loop,P
roced
ure,M
asks
H6/H7,S
caler
A2,Sy
ringe
Instru
ment,
Wire,
Brushe
sEas
t,Elev
ators
Noma
d,Case
ProCa
rt 3Em
powe
r,Enzy
matic,
Deter
gent
Hygie
ne,Ca
ssette
s,(oran
ge)Acorn
,Burni
sher
IRMNe
edle,H
olders
Planm
eca,Se
nsor,A
dapto
rRef
rigera
torGlo
vesMi
dwest
,RDH,F
reedo
m,Co
rdless
,Prop
hy,Sys
temAir
/Wate
r,Syri
nge,Tip
s,(Crys
tal,Tip
s)Ke
tac,Ce
ment
Perio
tome
Radio
logy,S
ensor
,Brief
cases
Toy C
hest (
Dispo
sable B
ox)Go
wn,(M
ed)
Plaqu
e,Disc
losing
,Solut
ionAlc
ohol,P
rep,Pa
dsKid
s,Prot
ective
,Eyew
earRo
ot,Tip
,Elevat
orsRIN
N,EZ,T
abs
White
3 Dra
wer S
torage
Conta
iner
Gown
,(Small)
Proph
y,Past
eAm
algam
,Carrie
rLab
,Pumi
ceSal
,Jet
Guaze
,(2x2)
,(200
ct)Pu
lp,Test
er,Wi
reAm
algam
,Plug
Lidoca
ineSod
ium,Ch
loride
Hand
,Sanit
izer
Tooth
paste
Amalg
am,W
ellLim
eLite
Surgic
al,Scis
sors
High,S
peed
,Evac
Tray,C
overs
Amalg
amato
rLol
icaine
,Topic
alSut
ure,Sc
issors
Mono
jet,Sy
ringes
Ultras
onic,S
caler,
Tips
Articu
lating
,Pape
rMa
xillary
,Anter
ior,Kit
,of,St
ainles
s,Stee
l,Cro
wns
West,E
levato
rsNe
edle,P
rotect
orsUlt
rason
ic,Scal
ersAsp
iratin
g,Syri
nges
Micro
,Brush
Need
les,(2
7,gauge,
long)
Unive
rsal,Sc
aler,H
5/33
Aspira
ting,S
yringe
s,(Peti
te)Mi
xing,P
ads
Need
les,(3
0,gauge,
x`sho
rt)Va
rnish
Ball,B
urnish
er,(Lg
)Mi
xing,W
ellPe
do,To
oth,Bu
rshes
Wild,F
loss
Ball,B
urnish
er,(Sm
)Mo
lt,Mou
th,Pro
pSal
iva,Eje
ctors
Basic
,Casse
tteMo
uth,M
irror,E
nds
Sani,To
wel,(B
ib)Ba
sic,Ca
ssette
s,(Red
)Mo
uth,M
irror,H
andle
sSha
rps,Co
ntaine
rs,(Lg)
Bite,B
locks,
(Adult
)MW
,Contr
a,Angl
e,She
athSha
rps,Co
ntaine
rs,(Sm
)Bit
e,Bloc
ks,(Ch
ild)MW
,PB,Co
ntra,A
ngle,H
ead,LA
TCH
Sterili
zation
,Bags,
(3.5x5
.25)
Bulk,C
ompo
site,Sy
ringer
s,(A1)
MW,Rh
ino,XP
,Slow,S
peed
,Moto
rSte
rilizat
ion,Ba
gs,(7.
5x13)
Bulk,C
ompo
site,Sy
ringer
s,(A3.5
)MW
,Slow,S
peed
,Head,FG
Sterili
zation
,Bags,
(9x14
.5)Bu
lk,Com
posite
,Syrin
gers,(A
3)MW
,Strai
ght,At
ttachm
ent
Succtio
n,Ster
ilizati
on,Ga
llon,Bu
ckets
Bulk,C
ompo
site,Sy
ringer
s,(A4)
MW,Tr
aditio
nal,N
on,Fib
er,Op
tic,Hig
hpeed
,Ha
ndpie
ceSur
gical,A
spirat
or,Tip
sBu
r,Bloc
k,12,H
oleMy
lar,St
rips
Syring
e,Slee
vesCarie
s,Indic
ator
Optib
ond,S
olo,Plu
sVa
cuKlee
nCavit
y,Con
dition
erPe
rio,Pr
obe
Vasol
ineCo
mposi
te,Gu
nPla
stic,Co
mposi
te,Ins
trume
ntZym
ex,Enzym
atic,C
leane
rCo
mposi
te,Po
lish,La
tch,Bu
r,Con
ePo
lishing
,Discs
,(Asso
rted)
Comp
osite,
Polish
,Latch
,Bur,C
upRe
storat
ive,Ca
ssette
s,(Gree
n)Co
mposi
te,We
tting,R
esin
Rubb
er,Da
mCo
ntouri
ng,Ply
ersRu
bber,
Dam,
Clamp
,KitCo
tton,P
liers
Rubb
er,Da
m,Cla
mp,Pu
ncher
Crimp
ing,Ply
ersRu
bber,
Dam,
Frame
Discoi
d`Cleo
idRu
bber,
Dam,
Retai
ner,F
orcep
Dispe
nsing,
tips,(B
lack)
Seal,n,
Shine
Dispe
nsing,
tips,(B
lue)
Septoc
aine
Durel
onSet
`Up,Tr
ayDy
cal,Re
fillSha
rpenin
g,Ston
esEtc
hant
Spoon
,Excav
ator
Explor
ersSta
inless,Ste
el,Crow
ns,Pac
kFer
ic,Sulf
ate,He
mosta
tic,Ag
ent
T`Band,(
Lg,Cu
rved)
FG,1/
4,Rou
ndT`B
and,(
Lg,Str
aight)
FG,Di
amon
d,Cou
rse,Ro
unde
dTo
fflemy
er,Ba
nd,#1
,(0.00
15)
FG,Di
amon
d,Inve
rted,C
one
Toffle
myer,
Band
,#1,(0
.002)
FG,Di
amon
d,Med
ium,Ro
unde
dTo
fflemy
er,Ba
nd,#1
3,(0.0
015)
FG,Di
amon
d,Sup
er,Fin
e,Need
leTo
fflemy
er,Ba
nd,#2
,(0.00
15)
FG,Fla
me,Sh
ape
Toffle
myer,
Band
,Holde
rsFG
,Mandre
lTo
fflemy
er,Re
taine
rFin
ishing
,Strip
sTri
ple,Tr
aysFlo
wable
,Comp
osite,
(A1)
Vitreb
ond
Flowa
ble,Co
mposi
te,(A2
)Wh
ite,Po
lishing
,Ston
e,Burs
Formo
cresol
Wood
,Wed
ge,(Sm
)Fuj
i,App
licator
ZOE
Fuji,II
Fuji,IX
THE CENTER FOR ORAL HEALTH
23
Setting Up Facility Appendix A1-‐A7 Appendix A1: Sample School District Organization Chart-‐ LAUSD Organization Chart Appendix A2: Sample School District Directory-‐ LAUSD Human Services Division Directory Appendix A3: Memorandum of Understanding (MOU) Template & SBOHC Sample Appendix A4: LAUSD-‐ Murchison Street Elementary School Setting Up Facility Check-‐List Appendix A5: EMCSD-‐ Gidley Elementary School Floor Plan Appendix A6: LAUSD-‐ Murchison Street Elementary School Capacity and Costs Table Appendix A7: LAUSD-‐ Murchison Street Elementary School Equipment Price List

The Center For Oral Health SBOHC Operations Manual
Most Common Procedures
Diagnostic
Preventive
Restorative
Endodontics
Oral & Maxillofacial Surgery
Adjunctive General Services
EMUSD-‐ Gidley Elementary School Procedure Distribution for Children
THE CENTER FOR ORAL HEALTH
25
Most Common Procedures
Treatment of dental disease through early intervention includes services deemed necessary to control the early stages of disease. These services are not complicated in nature and usually, more than one procedure can be accomplished in an appointment. The following section lists common procedures preformed at SBOHC’s. The following procedures are not limited to SBOHC’s nor does it indicate all the procedures that can and should be preformed at a SBOHC. We recommended that each SBOHC purchase a copy of the CDT 2014-‐ Dental Procedure Codes Guide by The American Dental Association, for a complete list of dental procedures with definitions and Current Dental Terminology Codes (CDT). All CDT Codes and definitions listed in the “Most Common Procedures” Section were gathered from the CDT 2014-‐ Dental Procedure Codes Guide by The American Dental Association. 17 Diagnostic Clinical Oral Exams D0120 Periodic Dental Examination
An evaluation performed to determine any change in patients dental or medical health status since pervious comprehensive or periodic examination
D0140 Limited Oral Evaluation (Problem Focused)
Limited to problem area, not an assessment of routine dental needs. An evaluation or re-‐evaluation limited to a specific oral health problem. Typically patients present specific problem: Emergencies, Trauma, Acute Infections, Etc.
D0145 Oral Evaluation for Patient Under Three Years of Age Diagnostic and preventative services performed for a child under the age of three, preferably within the first six months of the eruption of the first primary tooth, including recording the oral and physical health history, evaluation of caries susceptibility, development of an appropriate preventive oral health regimen and communication with an counseling of the child’s parent, legal guardian and/or primary caregiver.
D0150 Comprehensive Oral Evaluation
17 CDT 2014-‐ Dental Procedure Codes Guide by The American Dental Association

The Center For Oral Health SBOHC Operations Manual
Thorough evaluation/recording of hard and soft tissues. Typically, would include evaluation of patient’s medical history and a general health assessment. It should include the evaluation and recording of dental caries, missing or unerupted teeth, restorations, occlusal relationships, periodontal conditions, hard and soft tissue anomalies, etc.
D0170 Re-‐evaluation-‐Limited, problem Focused (Established Patient; Not Post-‐
Operative Visit) A detailed extensive problem focused evaluation entails extensive
diagnostic and cognitive modalities based on the findings of a comprehensive oral evaluation. Integration of more extensive diagnostic modalities to develop a treatment plan for a specific problem is required. The condition requiring this type of evaluation should be described and documented.
Example of conditions requiring this type of evaluation may include
dentofacial anomalies, complicated perio-‐prosthetic conditions, complex temporomandibular dysfunction, facial pain of unknown origin, conditions requiring muti-‐disciplinary consultation, etc.
D0180 Comprehensive Periodontal Evaluation (New or Established Patient) This procedure is indicated for patients showing signs or symptoms of
periodontal disease and for patients with risk factors such as smoking and diabetes. It includes evaluation of periodontal conditions, probing and charting, evaluation and recording of the patient’s dental and medical history and general health assessment. It may include the evaluation and recording of dental caries, missing or unerupted teeth, restorations, occlusal relationships and oral cancer evaluation.
Radiographs/Diagnostic Imaging With the following limitations:
-‐ Full mouth radiographs and or/panoramic radiograph-‐ once/3 years -‐ Supplemental Bitewings-‐ Once/6 months
D0210 Intraoral Radiographs (Complete Series of Radiographic Images)
A radiographic survey of the whole mouth, usually consisting of 14-‐22 periapical and posterior bitewing images intended to display the crowns and roots of all teeth, periapical areas and alveolar bone
D0220 Intraoral Radiograph (Periapical first Image) D0230 Intraoral Radiograph (Periapical Additional Image)

THE CENTER FOR ORAL HEALTH
27
D0240 Intraoral Radiograph (Occlusal Image) D0270 Bitewing (Single Images) D0272 Bitewing (Two Images) D0273 Bitewing (Three Images) D0274 Bitewing (Four Images) D0350 Oral/Facial Photographic Image Obtained Intraorally or Extraorally Tests and Examinations D0417 Collection and Preparation of Saliva Sample For Laboratory Diagnostic
Testing Oral Pathology Laboratory D0601 Caries Risk Assessment and Documentation (With a Finding of Low Risk) Using Recognized Assessment Tools D0602 Caries Risk Assessment and Documentation (With a Finding of
Moderate Risk) Using Recognized Assessment Tools D0603 Caries Risk Assessment and Documentation (With a Finding of High
Risk) Using Recognized Assessment Tools Preventative Prophylaxis D1110 Adult Prophylaxis (Once/6 Months)
Removal of plaque, calculus and stains from the tooth structures in the permanent and transitional dentition. It is intended to control local irritational factors
D1120 Child Prophylaxis (Once/6 Months If Calculus Is Present)
Removal of plaque, calculus and strains from the tooth structures in the primary and transitional dentation. It is intended to control local irritational factors

The Center For Oral Health SBOHC Operations Manual
Fluoride Treatments Prescription strength fluoride product designed solely for use in the dental office, delivered to the dentition under the direct supervision of a dental professional. Fluoride must be applied separately from prophylaxis paste D1206 Topical Fluoride Varnish
Therapeutic application for moderate to high caries risk to patients
D1208 Topical Application of Fluoride Other Preventive Services D1310 Nutritional Counseling For Control of Dental Disease
Counseling on food selection and dietary habits as part of treatment and control of periodontal disease and caries
D1330 Oral Hygiene Instructions
This may include instructions for home care. Examples include tooth brushing techniques, flossing, and use of special oral hygiene aids.
D1351 Sealant-‐Per Tooth
Mechanically and/or chemically prepared enamel surface sealed to prevent decay
D1352 Preventive Resin Restoration in a Moderate to High Caries Risk Patient-‐
Permanent Tooth Conservation restoration of an active cavitated lesion in a pit or fissure that does not extend into dentin; includes placement of a sealant in any radiating non-‐carious fissures or pits.
Restorative Attending Dentists are given the responsibility of determining the materials to be used in any given restoration based upon the specific physical and cosmetic requirements of that restoration and its environment. Only material approved by the American Dental Associations Council on Dental Therapeutics may be used in any dental facility. It is recommended that primary posterior teeth having multiple surfaces of carious involvement be restored with stainless steel crowns.
THE CENTER FOR ORAL HEALTH
29
The restoration of primary anterior teeth (incisors) should be attempted in early stages. When caries have involved multiple surfaces of these teeth, the decision not to restore them may be valid, owing to the inconsequential implications of the early loss of these teeth and to the trauma which their restoration requires, The decision to place steel crowns on anterior primary teeth shall, therefore, be left to each, individual clinic dental director. Amalgam Restorations (Primary and Secondary Dentition) Tooth preparation, all adhesives (including amalgam bonding agents), liners and bases are included as part of the restoration. If pins are used, they should be reported separately D2140 Amalgam-‐ One Surface, Primary or Permanent D2150 Amalgam-‐ Two Surface, Primary or Permanent D2160 Amalgam-‐ Three Surface, Primary or Permanent Resin-‐Based Composite Restoration-‐Direct D2330 Resin-‐Based Composite (One Surface, Anterior) D2331 Resin-‐ Based Composite (Two Surfaces, Anterior) D2332 Resin-‐Based Composite (Three Surfaces, Anterior) D2391 Resin-‐Based Composite (One Surface, Posterior)
Used to restore a carious lesion into the dentin or a deeply eroded area into the dentin. Not a preventive procedure
D2392 Resin-‐Based Composite (Two Surfaces, Posterior) D2393 Resin-‐Based Composite (Three Surfaces, Posterior) Other Restorative Services D2930 Prefabricated Stainless Steel Crown (Primary Tooth) D2940 Protective Restoration to protexct tooth or relieve plain
Direct placement of a restorative material to protect tooth and/or tissue form. This procedure may be used to relieve pain, promote healing, or
The Center For Oral Health SBOHC Operations Manual
prevent further deterioration. Not to be used for endodontic access closure, or as a base or liner under restoration
Endodontic Pulpotomy
D3220 Therapeutic pulpotomy or pulpectomy (Primary Teeth Only) Pulpotomy is the surgical removal of a portion of the pulp with the aim of maintain the vitality of the remaining portion by means of an adequate dressing
§ To be preformed on primary or permanent teeth § This is not to be construed as the first stage of root canal therapy § Not to be used for apexogenesis
Non-‐Surgical Periodontal Service D4341 Periodontal Scaling and Root Planing (Four or More Teeth Per
Quadrant) This procedure involves instrumentation of the crown and root surface of the teeth to remove plaque and calculus from these surfaces. It is indicated for patients with periodontal disease and is therapeutic, not prophylactic, in nature. Root planning is the definitive procedure designed for the removal of cementum and dentin that is rough, and/or permeated by calculus or contaminated with toxins or microorganisms. Some soft tissue removal occurs. This procedure may be used as a definitive treatment in some stages of periodontal disease and/or as part of pre-‐surgical procedures in others.
Oral & Maxillofacial Surgery Extractions D7111 Extraction, Coronal Remnants (Deciduous Tooth)
Removal of soft tissue-‐ Retained Coronal Remnants D7140 Extraction, Eruption tooth or Exposed Root (Elevation and/or Forceps
Removal) Includes routine removal of tooth structure, minor smoothing of socket bone, and closure, as necessary

THE CENTER FOR ORAL HEALTH
31
D7250 Surgical Removal of Residual Tooth Root (Cutting Procedure) Includes cutting of soft tissue and bone, removal of tooth structure, and closure
Adjunctive General Services Professional Visits D9430 Office Visit for Observation (No Other Services Performed) Miscellaneous Services D9951 Occlusal Adjustment
May also be known as equilibration; reshaping the occlusal surfaces of teeth to create harmonious contract relationships between the maxillary and mandibular teeth. Presently includes discing/odontoplasty/enamoplasty. Typically reported on a “per visit” basis. This should not be reported when the procedure only involves bite adjustment in the routine post-‐ delivery care for a direct/indirect restoration or fixed/removable prosthodontics.

The Center For Oral Health SBOHC Operations Manual
EMUSD-‐ Gidley Elementary School Procedure Distribution for Children (Ages 0-‐18)
The following lists actual data collected from a current COH SBOHC. In 2013-‐2014 EMCSD-‐Gidley Elementary School had a total of 1,811 visits, 1,518 of those visits involved Children. 84% of all procedures preformed at EMCSD-‐ Gidley Elementary School were Preventive and Diagnostic
Academic Year 2013-‐2014
CDT Classification Distribution for Children (Ages 0-‐18) CDT Classification Frequency Diagnostic 573 Preventive 756 Restorative 124 Endodontic 2 Periodontics 0 Prosthodontics 0 Implant Services 0 Oral and Maxillofacial Surgery 24 Orthodontics 0 Misc. 39 Total 1,518
Diagnostic 38%
Preventive 50%
Restorative 8%
Oral and Maxillofacial Surgery 2%
Misc. 2%
Procedure Distribution for Children (Ages 0-‐18)

THE CENTER FOR ORAL HEALTH
33
Procedure Outcome Measure Outcome
When is Referral Necessary?
Incase of an Emergency
The Center For Oral Health SBOHC Operations Manual
Procedure Outcome
Measure Outcome: Historically the ratio of “decayed, missing, filled “ teeth has been the benchmark of quantifying dental treatment from year to year. Comparing oral health records of patients is still the most efficient way to gauge progress in healthy mouths. The patients that attend regular check-‐ups, have the healthiest mouths and spend the least amount of money overall on Dental Treatments. Dental Directors should use their choice of standard identifying measurement tools to categorize the Oral Health Status of each patient.
LAUSD-‐ Murchison Street Elementary School ASA Classifications 18 ASA I Normal Healthy Patient ASA II Patient with mild systemic disease that does not interfere with daily
activity, or patient with a significant health risk factor (e.g. Smoking, Alcohol Abuse, Gross Obesity)
ASA III Patient with moderate to severe systemic disease that is no incapacitating, but may alter daily activity
ASA IV Patient with severe systemic disease that is incapacitating and is a constant threat to life
When is Referral Necessary?
Referrals to specialty clinics are a common situation. Any referral should be made when needed treatment cannot be provided at a SBOHC site. The cause of a referral could mean lack of knowledge or lack of equipment at SBOHC site. No treatment should be initiated that cannot be successfully completed on SBOHC sites. Dental Directors should make a resource list for patients that may need referrals. This list should include Dentists in the area that are located no more than 10 miles from SBOHC’s site. Refer to the Daily Operation Procedures Section-‐ Referral Process for more information. Incase of an Emergency:
Any treatment facility is legally obliged to provide an emergency number to each patient it exams or provides treatment to.
18http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

THE CENTER FOR ORAL HEALTH
35
An Emergency number should be given to patients incase of an emergency situation that may occur outside of SBOHC site (Dental Director On Call Number). In case of an extreme emergency, tell patient to call 911

The Center For Oral Health SBOHC Operations Manual
Daily Operations SBOHC Daily Set-‐Up
SBOHC Daily Breakdown
Diagnostic Screenings
Comprehensive Maintenance & Treatment
Frequency of Screenings
Referral Process
Complications

THE CENTER FOR ORAL HEALTH
37
Daily Operations SBOHC Daily Set-‐Up19
1. Per security protocol, upon arrival at the SBOHC Site, the Site Coordinator is to sign in all members at the school’s front office.
2. Prior to set-‐up, ensure that no dental chairs, units, furniture is out of place. 3. RDA-‐ Set up all Radiographic equipment/materials in designated areas. RDA will
be responsible for obtaining and returning the NOMAD, X-‐ray sensors, and laptop to and from appropriate storage locations.
4. RDA-‐ Set up sterilization Station. Dental Units, Sterilization, Cavitron Units, and Ultrasonic all require distilled water
5. Remove Autoclavable instruments/cassettes from storage and place at designated areas
6. Replenish all disposable materials, if needed 7. Print out the current day’s clinic schedule 8. Referencing clinic schedule, pull all patient folders from filling cabinet (For
returning/recall patients) or Have blank Forms ready (New Patient) 9. Set up trays for each planned procedure
SBOHC Daily Supplies & Equipment Maintenance19
1. Proceed with planned clinic services in line with OSHA compliance 2. After each procedure, throw all disposable items in designated trash bins, and
Cavi-‐wipe all portable equipment and chair. Restorative composite guns, composite carpules, cavitron device, slow-‐speed motors, and FUJI guns, can all be Cavi-‐wiped
3. All sharps are to be placed in designated Sharps Container 4. All Biohazard Bags are to be disposed of in the Biohazard Waste Container 5. All equipment (Expect for cavitron tips and handpieces) can be placed in the
Ultrasonic. All equipment should then be placed in autoclavable bags and placed in Autoclave machine
19http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

The Center For Oral Health SBOHC Operations Manual
SBOHC Daily Breakdown:20
1. Breakdown all Dental Chairs and units and store in designated area 2. Breakdown sterilization station and store in designated area
a. Any instruments not yet sterilized by the end of the day must be clearly labeled for the next clinic day. Communicate directly with RDA
3. RDA will be responsible for obtaining and returning the NOMAD, X-‐ray sensors, and laptop to and from appropriate storage locations.
4. Ensure all equipment/materials are wiped clean and stored back into their designated areas or bags
5. Accordance with Environmental Health & Safety Guidelines, all autoclaves are to be monitored and tested weekly for effectiveness in killing microorganisms.
6. Upon departure, the Site Coordinator is to sign out all members at schools front office
Diagnostic Screenings:20 Dental Radiology Procedures When a patient first enters the SBOHCs, a clinical examination will be undertaken to determine which type of images (if any) will result in the greatest diagnostic yield. The patient’s medical and dental histories (With emphasis on recent dental radiographs) will be evaluated prior to making any exposures. Portable NOMAD units should be used at the SBOHC along with the 0, 1, or 2 SENSORS. The patient images are then transferred into the Dental Electronic System corresponding to the patient’s chart.
• All new patients will receive a radiographic series consistent with their dental needs. This will range from combinations of a classic adult or pediatric images to various horizontal, vertical and bitewing images. Periodic radiographic evaluations at intervals of 6, 12, 18 or 24 months will be based on individual patient needs and disease experience
• Images will be created by RDA, and reviewed by Dental Director for technical quality and diagnostic yield
• The radiology record will indicate the data of exposure, number of exposures made, and signature confirming the adequacy of the images
Tip: The AAPD and ADA published guidelines for prescribing dental radiographs geared toward children (infants, toddler, and adolescents) as well as special needs.
20http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

THE CENTER FOR ORAL HEALTH
39
Diagnostic Screening Event A SBOHC should preform a Diagnostic Screening Event-‐ screen an entire grade, one classroom at a time, until whole school is complete-‐ once a year. The actual Diagnostic Screening process is usually done class-‐by-‐class utilizing tongue blade and light. Entire Schools can be screened in two to five days depending on the size of the school. The following lists the procedures for conducting a SBOHC Diagnostic Screening event.
A. Screening Event I. Site Coordinator-‐ Distribute Parent Consent Forms to entire Elementary
School via Teachers a. Two Weeks Before Screening Event
II. Teachers-‐ Return completed Consent Forms to Site Coordinator III. Site Coordinator-‐ Check each returned Consent Form
a. Parent Signature b. Insurance
IV. Site Coordinator-‐ Obtain Two copies of each classrooms roster a. Students first and last name b. Students Gender c. Students Birthdate
V. Site Coordinator-‐ Highlight Student names that will be participating in Screening Event
a. One Copy-‐ Used for SBOHC File b. One Copy-‐ Used for Day of Event
VI. Site Coordinator-‐ Separate completed consent forms by Teacher/Classroom
VII. Site Coordinator-‐ Obtain large Manila Envelopes (One for each Teacher/Classroom) and staple the appropriate highlighted Day of Event Roster to each envelope (One envelope and Roster for each Teacher/Classroom)
VIII. Site Coordinator-‐ Place Consent Forms in appropriate Manila Envelope (Organized by Teacher/Classroom)
IX. Site Coordinator-‐ Organize each Manila Envelopes by grade X. Site Coordinator-‐ File other highlighted Roster for SBOHC Records (By
Grade and Teacher)
B. Day of Screening Event
I. Site coordinator-‐ Manila Envelopes containing Consent Forms with Day of Event Roster stapled to front should be ready (separated by Grade and Teacher).
The Center For Oral Health SBOHC Operations Manual
II. Parent Volunteer-‐ Using Manila Envelopes containing Consent Forms with Day of Event Roster stapled to front, retrieve participating students (Class by Class-‐ Entire Grade at a Time)
III. At SBOHC site Students should come in a straight line and wait for direction
a. Create Waiting Area for Students b. Let them Color and Read Educational Material c. Parent Volunteer & SBOHC Staff Help Watch Children
IV. Site Coordinator-‐ Using Manila Envelopes containing Consent Forms with Day of Event Roster stapled to front, One by one students will come to front desk and be verified by Site Coordinator
a. Students Consent Form b. Students First and Last name c. Students Birthdate d. Student Address e. If a child is 4 to 6 years old-‐ ask for their first and last name and their mom or dads name
V. Site Coordinator-‐ After child is verified, give them their Consent Form a. Child will give Consent Form to Dentist for screening purposes
VI. Dental Director-‐ Conduct Diagnostic Screening a. Child should brush their own teeth-‐ Under direction from Dental Director and or RDA b. Visual-‐ Utilizing tongue blade and light c. Record Findings on Consent Form d. Apply Fluoride Varnish
VII. Site Coordinator-‐ After Screening collect Consent Forms a. Place check mark next to name and date student was seen
VIII. Site Coordinator-‐ Prepare Parent Treatment Letters a. Indicate what procedures were preformed and Recommendations
Check-‐In Process Time: 6 to 10 minutes Patient Wait Time: 15 to 30 minutes (Depending on the class size)
C. After Screening Event
I. Site Coordinator-‐ Give Parent Treatment Letters to Teachers and ask that they distribute to the appropriate student
II. Site Coordinator-‐ Start making Comprehensive Appointments a. Urgent Students first

THE CENTER FOR ORAL HEALTH
41
Comprehensive Procedures:
Scheduling Appointments Each SBOHC Site should use an Electronic Scheduling System. When scheduling appointments for Comprehensive procedures, the Site Coordinator should collect the patient’s full name, phone number, insurance type, and reason for visit. If the SBOHC is unable to treat a patient, the Site Coordinator should refer the patient to a nearby Dental Clinic.
SBOHC’s should not see a whole classroom at once unless the SBOHC is conducting a Diagnostic Screening Event. However we recommend that the Site Coordinator schedule two students from the same classroom simultaneously, this way the students see a friendly face next to them and feel more at ease.
Scheduling and organizing the clinic’s appointments depend on treatment and instruments available. It is the Site Coordinators responsibility to schedule around major tests, field trips, and school wide events. The Site Coordinators should work with individual teachers and determine what time is best for individual classrooms.
Tip: Site Coordinators should be mindful of their patients lunch period. Some procedures require that the child not eat for 30 min after their appointment. For example if the patient receives a filing and the child has lunch at 11:30am, the Site Coordinator should schedule that patient for 10am (30 Minute Appointments). 10am allows the child ampule time to recuperate before their lunch period. Cancellation and Rescheduling Appointments21 The Site Coordinator manages the Cancellation and Rescheduling of patient appointments. If the patient chooses not to schedule a new appointment, the Site Coordinator should record both the call and or discussion in the patient’s treatment record. If the patient/guardian states that the child has a new dental home and will no longer be a patient at the SBOHC, the Site Coordinator should note the change of dental homes in the patient’s chart and place the patient as “inactive.” All cancellations and no-‐shows should also be reflected in the Electronic Scheduling System as another way to document the patients scheduling history.
Patient Check-‐In When Patients enter the SBOHC, Site Coordinators should have patient fill out the appropriate paperwork. Dental Directors can choose to use the same paper work as their primary practice. Site Coordinators should enter all information into the SBOHC Electronic System (Different From Electronic Scheduling System) and file all hard copies.
21http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf
The Center For Oral Health SBOHC Operations Manual
Comprehensive Procedures After Initial Diagnostic Screenings, comprehensive exams should be performed in the SBOHC on a regular bases, based on patient need and Clinics ability. The following lists the procedures for conducting a SBOHC Comprehensive Procedure.
A. Check-‐In Process
I. Site Coordinator-‐ Hand Patient Appropriate Patient Paperwork to sign II. Site Coordinator-‐ After Appropriate Patient Paperwork is completed, Site Coordinator should review Forms, go over important information with Patient, and Verify insurance information
a. Health Status b. Last dental visit c. Reason for their visit d. Dental Insurance Information
III. Site Coordinator-‐ While patient waits, offer the patient preventative education literature on Dental Hygiene
IV. Site Coordinator-‐ Check patient’s insurance information (if haven’t done already) and enter patient’s identifying/Insurance Information into SBOHC’s Electronic System.
Check-‐ In Process Time: 10 to 15 Minutes
B. Maintenance & Treatment Process
I. RDA-‐ Preforms X-‐Rays a. Patient Signs Image Release Form b. Enter X-‐Rays into Electronic Dental System
II. Dental Director-‐ Preforms Appropriate Procedure a. Enter CDT Codes into Electronic Dental System
Maintenance & Treatment Time: 15 to 20
C. Follow-‐up Activities
1. Dental Director/Site Coordinator-‐ After a patient leaves the treatment chair, use Patient Electronic System to fill out Patient Treatment Plan
a. Indicate procedure preformed b. Indicate if patients needs more treatment and or needs to schedule a
follow-‐up appointment
Tip: On bottom of Parent Letter the Site Coordinator should add encouraging words. For Example: The child was scared at first but we went based on the child’s pace of comfort and the Child did great. It is okay to call the parents right after treatment is
THE CENTER FOR ORAL HEALTH
43
done just to let them know how everything went and what was done. Parents like to be informed that their child did well during the examination; this process will help build SBOHC’s reputation as Child Focus & Child Friendly
2. Patients 0-‐14 years old should receive a farewell goodie bag a. Coloring book b. Nutritional paper c. Pencil d. Tooth Brush e. Dental Floss f. Sticker
Tip: When the child comes back a second time they receive should a toy
3. Patient 15+ years old, patients leaves with their next appointment or a note for job
Frequency of Screenings: The frequency of screenings varies from site to site. However for the purposes of this manual, we have based all our findings and recommendation on the LAUSD-‐ Murchison Street Elementary School 2010-‐2014 and EMCSD-‐ Gidley Elementary School 2012-‐2014 SBOHC Frequency Statistics. Each SBOHC should have a team of three: Dental Director (.2 FTE), Registered Dental Assistant (.2 FTE) and Site Coordinator (.2 FTE). Clinics should remain open at least one day a week and accommodate two chairs. The Dental Director should see an average of 1.7 Patients Per Hour Recommended Patients Per Day-‐ 12 to 14 Procedures Per Patient-‐ 3 Referral Process: Referrals to specialty clinics are a common situation. A referral should be made when needed treatment cannot be provided at SBOHC site. The following lists the process for making a referral.22
1. Site Coordinator-‐ complete Referral Form and make three copies a. To the Patient or Parent/Guardian
22http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

The Center For Oral Health SBOHC Operations Manual
b. For the Patient’s Chart c. Given/Sent to the Referral Clinic
2. Site Coordinator-‐ note referral in Patient’s Chart and log referral a. Noting the day and time of SBOHC appointment b. Referral Location c. Patient’s Phone Number
3. Site Coordinator-‐ inform patient that costs may be associated with the referrals 4. Site Coordinator-‐ If considered an Emergency, SBOHC Staff should telephone the
referred Dental Clinic and arrange Patient’s appointment a. Confirm appointment time b. Confirm arrival of patient
i. If Patient does not show-‐ SBOHC Staff should contact Patient and reestablish the needed appointment
5. Site Coordinator-‐ If the referral is not an emergency, SBOHC Staff may elect to confirm referral at next patient visit
6. Site Coordinator-‐ Follow-‐up care for the patient will be scheduled on a case-‐by-‐case basis
Urgent and Non-‐Urgent Case Referrals The SBOHC will allow flexibility on the schedule to, at minimum, conduct a limited oral examination for emergency patients. On a case-‐by-‐case basis, the SBOHC will be able to perform the dental treatment, or refer directly to an outside dental clinic. Because procedures are limited at the SBOHC (i.e. no Surgical procedures or complete endodontic are preformed), patients requiring these treatments will be automatically referred. The SBOHC will make every effort to help patients requiring emergency care or who have been referred for dental emergencies from other offices, in one of the following ways: 23
1. Will see the patient for immediate treatment 2. After an examination will prescribe appropriate medications to relieve the pain
and/or infection until an appointment can be scheduled 3. Refer patient to a medical clinic for medical evaluation and needed prescriptions
until the dental clinic can schedule an appointment for requited care 4. Refer the Patient to another Dental Clinic 5. Refer the Patient to the nearest Hospital Emergency Room
Referrals To Other Providers The SBOHCs my deem it necessary to refer a patient to another provider if:23
1. SBOHC is not able to attend to the patients problem 23http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf
THE CENTER FOR ORAL HEALTH
45
2. SBOHC examines the Patients and determines that the patient would be better served seeking care from a specialist, or another provider better trained to treat the patient’s problem
When a SBOHC refers a Patient to another Dental Clinic, it will do the following: 1. SBOHC Site Coordinator will complete Referral Form and make three copies Complications: In spite of the best efforts in diagnosis, treatment planning, and technique, the outcome of a procedure(s) is sometimes less than desirable. A poor result does not necessarily suggest that a practitioner is guilty of negligence or other wrongdoing. However, when complications occur, it is mandatory that the Dental Director immediately begin to address the problem in an appropriate manner. In most instances the Dental Director should discuss the problem with the patient or parent/guardian. When possible, the dental director should avoid admitting guilt or liability. Examples of such situations are loss or failure to recover a root tip, perforation of the maxillary sinus, damage to adjust teeth, inadvertent fracture of surrounding bone, separated endodontic file, etc. In theses instances, the Dental Director should clearly outline proposed management of the problem including specific instructions to the patient, further treatment that may be necessary, and referral to an oral surgeon when appropriate. If referral to a specialist is deemed necessary, the referral can be completed at that time to a near by clinic with a pediatric dentist and or specialist. It is very important that the malpractice carrier be notified of any potential litigation. If a patient threatens to discuss the problem with an attorney, the malpractice carrier must be notified. It is also important that the Dental Director refrain from entering into any arguments with the patient or parent/guardian, and should not admit liability or negligence. Finally, it is imperative that the chart record accurately reflects the details of the occurrence. No additions, deletions, or changes of any short should be made in the patient’s record at a later date. Records must not be misplaced or destroyed according to records retention policies. 24
24http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf
The Center For Oral Health SBOHC Operations Manual
Daily Operations Appendix B1-‐B14 Appendix B1: Sample Teacher Cover Letter Appendix B2: Sample Parent/Guardian Consent Form (English & Spanish) Appendix B3: Sample Patient Registration Form Appendix B4: Sample New Parent Consent to Use and Disclosure of Health Information For Treatment, Payment, or Healthcare Operations Appendix B5: Permission to Share Information Form Appendix B6: Informed Consent Form Appendix B7: Basic Surgical Treatment Consent Form Appendix B8: Confidential Medical & Dental History For a Minor Patient Appendix B9: Confidential Medical & Dental History For An Adult Appendix B10: Dental Examination Worksheet Appendix B11: Periodontal Charting Appendix B12: Patient X-‐ray Summary Appendix B13: Image Release Form Appendix B14: School Absence Release

THE CENTER FOR ORAL HEALTH
47
Finance Policies SBOHC Fee Schedule
Denti-‐Cal Billing Process
Denti-‐Cal Reimbursement
Break-‐Even Analysis
Managing Finances

The Center For Oral Health SBOHC Operations Manual
Finance Policies SBOHC Fee Schedule: All procedures performed at a SBOHC should be recorded using a standard coding system. Standardized dental procedure coding, such as The Current Dental Terminology (CDT), has been in existence since 1990. Federal regulations arising from HIPPA required all payers and providers adopt The CDT coding system in 2003. All SBOHC’s are required to use CDT coding when assessing their sites fee schedule.
The types of Insurance accepted at each SBOHC will vary from site to site. However for the purposes of this manual, we have based all our findings and recommendation on the LAUSD-‐ Murchison Street Elementary School 2010-‐2014 and EMCSD-‐Gidley Elementary School 2012-‐2014 SBOHC Fee Schedule. We recommend, that when accepting Private Insurance, each SBOHC uses “The Usual, Customary and Reasonable” Billing System for Payment Rates and Reimbursements (associated with The Dental Directors Primary Practice). 25 SBOHC Accepts Medicaid-‐ Denti-‐Cal Coverage We recommend that at least 70% of SBOHC patients pay with Denti-‐Cal Dental Coverage. Refer to Break-‐Even Analysis for more information. Denti-‐Cal In July 1965, legislation created the optional state medical assistance program known as Medicaid. This program provided for Federal Government to match state funds for a comprehensive healthcare program. In November 1965, California State Legislation was signed, implementing the state program called Medi-‐Cal; Denti-‐Cal was subsequently established to provide access to dental care. SBOHC Accepts Private Insurance-‐ Indemnity & Managed-‐Care We recommend that 15% of SBOHC patients pay with Private Insurance. Refer to Break-‐Even Analysis for more information.
Usual, Customary and Reasonable (UCR) The amount paid for a medical service in a geographic area based on what providers in the area usually charge for the same or similar medical service. 26
25http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf 26 http://www.dol.gov/ebsa/pdf/SBCUniformGlossary.pdf

THE CENTER FOR ORAL HEALTH
49
SBOHC Accepts Non-‐Insurance-‐ Cost absorbed by Dental Director About 15% of SBOHC patients will have non-‐insurance. We recommend that Dental Directors absorb the cost of helping non-‐insured patients and treat these patients free of charge. Refer to Break-‐Even Analysis for more information. Tip: Each SBOHC will have a different Reimbursement Fee Schedule based on the different private insurance plans accepted. In The State of California there are multiple Indemnity and Managed-‐Care dental plans. We suggest that each clinic create a list similar to (Appendix C1), which includes CDT codes and reimbursement rates for each insurance plan.
Denti-‐Cal Billing Process:
We recommend each Dental Director use an Electronic System for billing and patient records, associated with their primary practice. The Medical Biller should process claims electronically on a daily bases and follow the same filing practices as one would in their primary practice. Each SBOHC is required to have an Internet connection, in order to access an Electronic System. The following lists the steps for filling a Denti-‐Cal Claim.27
1. Check Eligibility
A. Required: I. Benefits ID Card Number (BIC) II. National Provider Identification (NPI) B. Check Patient Eligibility: I. Online: https://www.Medi-‐Cal.ca.gov/eligibility/login.asp a. Print the screen that verifies patient eligibility II. Automated System: (800) 456-‐2387 a. Enter NPI
b. BIC (*key and 123 for position) c. Patients Birthday (month and year of birth) d. Date of service (month and year of birth)
i. Combination of letter and numbers will indicate the patient is eligible ii. Check once per month for update
C. Keep Records: I. Copy of BIC (Scan into Electronic Dental Record) II. Copy of Photo ID
27http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

The Center For Oral Health SBOHC Operations Manual
a. Verify the cardholder is the same person as patient III. Eligibility Status
2. Check Treatment History A. Automated System: (800) 423-‐0507 I. Press 0 to speck to operator II. Will Need The Following: a. NPI Number b. Office Number for Provider c. Provider Information i. Dentist Name ii. Address-‐ Suite/Apt/City/State/Zip Code 3. Making A Claim
A. Electronic Billing System will automatically create a claim once procedures are completed and have been placed in the Queue I. Medical Biller fills out Electronic Dental Form and Submits
B. Paper Form I. Special Projects (i.e D9430)
C. Fast Attach X-‐Rays I. X-‐rays must indicate which side is “Right or Left” otherwise claim will be denied
D. Claim Reimbursement usually takes 2 to 3 weeks 4. Check Status of Claim A. Clearing House
B. Automated System: (800) 423-‐0507 I. Press 0 to speck to operator
II. Will Need The Following: 1. Date of Service 2. BIC Number 3. Procedure Code Denti-‐Cal Reimbursement SBOHC Sites should file claims on the day of service rendered, for best reimbursement results. The site should use an Electronic Billing System to file each claim. The SBOHC can check the status of a claim through the sites clearinghouse. Refer to Denti-‐Cal Billing Process for step-‐by-‐step details on how to file Claims. The Denti-‐Cal Reimbursement Percentage Schedule28
28 Denti-‐Cal California Medi-‐Cal Dental Program Handbook

THE CENTER FOR ORAL HEALTH
51
• Six calendar months after the end of the month in which the service was performed are considered for full payment at 100 percent of the SMA
• Seven to Nine months after the end of the month in which the service was performed will be considered for payment at 75 percent of the SMA amount.
• Ten to Twelve months after the end of the month in which the service was performed will be considered for payment at 50 percent of the SMA amount.
Once Claim is approved, The SBOHC will receive a check (or Direct Deposit) in about 2 to 3 weeks, along with an Explanation of Benefits Packet. This Packet will explain how much the SBOHC received for each patient and if and why a claim was denied. Reviewing Denial Rates are very important for accessing and assuring sustainability. There are three separate, specific procedures, for asking Denti-‐Cal to reevaluate/appeal the denial or modification of a claim payment or a TAR authorization
Submitting a Claim Inquiry Form (CIF)29 To find out why payment of a claim was disallowed or to furnish additional information to Denti-‐Cal for reconsideration of a payment denial or modification, the provider should begin by submitting the Claim Inquiry Form (CIF) within six calendar months of the Explanation of Benefits (EOB) date. Check the box on the CIF marked “CLAIM REEVALUATION ONLY.” Make sure to send a separate CIF for each inquiry.
Reevaluation of a Notice of Authorization (NOA)29 Use the Notice of Authorization (NOA) to request a single reevaluation of modified or disallowed procedures on a TAR. Check the “Reevaluation is Requested” box in the upper right corner of the NOA. Do not sign the NOA when requesting reevaluation. Include any additional documentation for reconsideration and return the NOA to Denti-‐Cal
First–Level appeal29 If Denti-‐Cal upholds their original decision to disallow payment of the claim or authorization of treatment, the provider may request an appeal. In accordance with Title 22, Section 51015, of the California Code of Regulations (CCR), Denti-‐Cal has established an appeals procedure to be used by providers with complaints or grievances concerning the processing of Denti-‐Cal TAR/Claim forms for payment. The following procedures should be used by dentists to appeal the denial or modification of a TAR or claim for payment of services provided under the Denti-‐Cal Program
29 Denti-‐Cal California Medi-‐Cal Dental Program Handbook
The Center For Oral Health SBOHC Operations Manual
Provider First-‐Level Appeals Process:
• The provider must submit the appeal by letter to Denti-‐Cal within 90 days of the EOB denial date. Do not use CIFs for this purpose.
• The letter must specifically request a first-‐level appeal. • Send all information and copies to justify the request. Include all documentation
and radiographs. • The appeal should clearly identify the claim or TAR involved and describes the
disputed action. • First-‐level appeals should be directed to: Denti-‐Cal Attn: Provider First-‐Level
Appeals PO Box 13898 Sacramento, CA 95853-‐4898
Denti-‐Cal will acknowledge the written complaint or grievance within 21 calendar days of receipt. The Denti-‐Cal Provider Services will review the complaint or grievance, and a report of the findings and reasons for the conclusions will be sent to the SBOHC within 30 days of the receipt of the complaint or grievance. If review by Provider Services determines it necessary, the case may be referred to Denti-‐Cal Professional Review.
If the complaint or grievance is referred to Denti-‐Cal Professional Review, the provider will be notified that the referral has been made and a final determination may require up to 60 days from the original acknowledgement of the receipt of the complaint or grievance. Professional Review will make its evaluation and send findings and recommendations to the provider within 30 days of the date the case was referred to Professional Review.
Tip: The provider should keep copies of all documents related to the first-‐level appeal. Under Title 22 regulations, a Denti-‐Cal provider who is dissatisfied with the first-‐ level appeal decision may then use the judicial process to resolve the complaint. In compliance with Section 14104.5 of the Welfare and Institutions Code, the provider must “seek judicial remedy” no later than one year after receiving notice of the decision of the First Level Appeal.
How To Complete a CIF and or NOA Form30 Use CIF form for each CIF and or NOA Claim. Please print or type all information:
A. Billing Provider Name Enter the billing provider's name in either the “doing business as” format, such as HAPPY TOOTH DENTAL CLINIC, or in the last-‐name, first-‐name, middle-‐initial, title format, e.g., SMITH, JOHN J., DDS. This information should be consistent with that used when filing state and federal taxes.
30 Denti-‐Cal California Medi-‐Cal Dental Program Handbook
THE CENTER FOR ORAL HEALTH
53
B. Medi-‐Cal Provider Number Enter the Billing Provider Number (NPI). NOTE: The Provider Number must be present and correct on all forms.
C. Mailing Address and Telephone Number Enter the billing provider service office address where treatment is rendered. A service office address should be a street address, including city, state and zip code. A post office box cannot be used as a service office; however, it is acceptable in rural areas only to use a route number with a post office box number. If the service office address is different from the address where payment is received, then notify Denti-‐Cal so payment can be directed to the appropriate location. It is important to include the telephone number of the service office, including area code, so Denti-‐Cal can contact the provider if questions arise while processing the documents.
D. City, State, Zip Code Enter the city, state, and zip code where the service office is located.
E. Patient Name Enter the beneficiary's last name, first name, and middle initial.
F. Document Control Number (Claim Reevaluation Only) Enter the Document Control Number of the document in question. If you are inquiring about multiple claims submit one CIF only for each document in question.
G. Patient Medi-‐Cal ID Number Enter the BIC or Client Index Number (CIN).
H. Patient Dental Record Number (Optional) If the provider assigns a Dental Record Number or Account Number to a beneficiary, enter the assigned number that will be referenced on any subsequent correspondence from Denti-‐Cal
I. Date Billed Enter the date the claim or the TAR was originally mailed to Denti-‐Cal.
J. Inquiry Reason-‐ Check Only One Box Indicate if this inquiry is seeking the status of a TAR or Claim (“tracer”) or is requesting a reevaluation of a claim.
K. Remarks Use this area to provide any additional information needed to justify the inquiry being made. Include a copy of the claim, TAR, or NOA in question and any appropriate documentation radiographs and photos. Attach all related

The Center For Oral Health SBOHC Operations Manual
radiographs/photos using the appropriate X-‐Ray envelope (i.e., the DC-‐214A or DC-‐214B).
L. Signature and Date The provider, or person authorized by the provider, must sign and date the form using blue or black ink. Rubber stamp signatures are not acceptable.
Mail the form to:
Denti-‐Cal California Medi-‐Cal Dental Program PO Box 15609 Sacramento, CA 95852
Break-‐Even Analysis:
The Break-‐Even Analysis varies from site to site. However for the purposes of this manual, we have based all our findings and recommendation on the LAUSD-‐ Murchison Street Elementary School 2010-‐2014 and Gidley Elementary School 2012-‐2014 SBOHC Frequency Statistics. Underlying Assumptions:
• No expenses required for rent, site maintenance, and utilities. • Salaries include Fringe Benefits. • Revenue Anticipated fees Based on Appendix C1: Sample Reimbursement Free
Schedule • Revenue Anticipated (Age Dependent)-‐ Patient Per Year (Denti-‐Cal) =
1 COE ($25) + 1 POE ($15) + 2 sets of 2 BWX ($10 × 2) + 2 sets of Fluoride Varnish ($18 × 2) + 2 Child Prophylaxis ($30 × 2) + 4 sealants ($88) = $244
• Revenue Anticipated-‐ Patient per Year (Private Insurance) = 1 COE ($90) + 1 POE ($50) + 2 sets of 2 BWX ($46× 2) + 2 sets of Fluoride Varnish ($45 × 2) + 2 Child Prophylaxis ($68× 2) + 4 sealants ($55 x 4)= $678
• All figures are subject to change and are dependent on individual SBOHC expenses and revenue
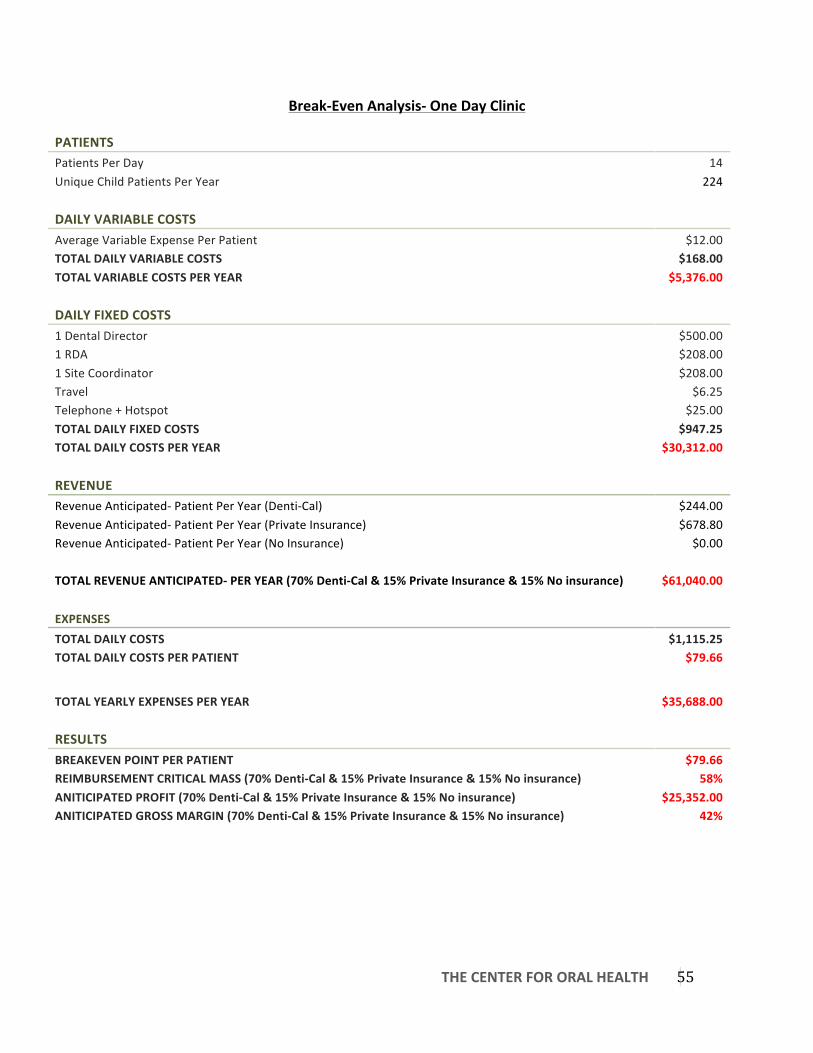
THE CENTER FOR ORAL HEALTH
55
Break-‐Even Analysis-‐ One Day Clinic
PATIENTS Patients Per Day 14 Unique Child Patients Per Year 224
DAILY VARIABLE COSTS Average Variable Expense Per Patient $12.00 TOTAL DAILY VARIABLE COSTS $168.00 TOTAL VARIABLE COSTS PER YEAR $5,376.00
DAILY FIXED COSTS 1 Dental Director $500.00 1 RDA $208.00 1 Site Coordinator $208.00 Travel $6.25 Telephone + Hotspot $25.00 TOTAL DAILY FIXED COSTS $947.25 TOTAL DAILY COSTS PER YEAR $30,312.00
REVENUE Revenue Anticipated-‐ Patient Per Year (Denti-‐Cal) $244.00 Revenue Anticipated-‐ Patient Per Year (Private Insurance) $678.80 Revenue Anticipated-‐ Patient Per Year (No Insurance) $0.00
TOTAL REVENUE ANTICIPATED-‐ PER YEAR (70% Denti-‐Cal & 15% Private Insurance & 15% No insurance) $61,040.00
EXPENSES TOTAL DAILY COSTS $1,115.25 TOTAL DAILY COSTS PER PATIENT $79.66
TOTAL YEARLY EXPENSES PER YEAR $35,688.00
RESULTS BREAKEVEN POINT PER PATIENT $79.66 REIMBURSEMENT CRITICAL MASS (70% Denti-‐Cal & 15% Private Insurance & 15% No insurance) 58% ANITICIPATED PROFIT (70% Denti-‐Cal & 15% Private Insurance & 15% No insurance) $25,352.00 ANITICIPATED GROSS MARGIN (70% Denti-‐Cal & 15% Private Insurance & 15% No insurance) 42%

The Center For Oral Health SBOHC Operations Manual
Managing Finances:
We recommend that each Dental Director create a separate bank account excusive to their SBOHC facility. If Direct Deposit’s are applicable, we recommend that the Dental Director use Direct Deposit’s for fast and efficient reimbursement payments.
The SBOHC site should actively monitor their financial status. The following demonstrates what we recommend each SBOHC use when monitoring their SBOHC finances.
• Profit and Loss (P&L) Statement • Budget-‐ Prediction vs. Actual

THE CENTER FOR ORAL HEALTH
57
Finance Policies Appendix C1-‐C5 Appendix C1: Sample Reimbursement Free Schedule-‐ LAUSD Murchison Street Elementary Appendix C2: Sample Claim Inquiry Form Appendix C3: 2-‐Year Break-‐Even Analysis Appendix C4: Sample P&L Statement Appendix C5: Sample Budget-‐ Prediction VS. Actual
Appendix C1 Note: Denti-‐Cal Rates-‐ Using the June 2014 Maximum Allowance Denti-‐Cal Rates. Dental or Medical health care services that are not covered by the Medi-‐Cal program are deemed “not a benefit.” Procedures that are performed in conjunction with, and as part of, another associated procedure are deemed “Global procedures.” Global procedures are not separately payable from the associated procedure.
Private Insurance Average: An average of multiple private insurance UCR rates throughout the Los Angeles County Area Appendix C4-‐ C5 Note: Sample P&L and Sample Budget-‐ Prediction VS. Actual taken from DentaQuest Institute “Map To The Future: Back Mapping School Based Oral Health To Achieve Financial Sustainability

The Center For Oral Health SBOHC Operations Manual
Evaluation Goal Setting
Measurable Objectives
Managing Reimbursement Denial Rates Effectively
Evaluating Success

THE CENTER FOR ORAL HEALTH
59
Evaluation Goal Setting: Before opening the doors of your SBOHC, Dental Directors should first set 3 to 5 goals. These goals must be measurable and be evaluated every one to two weeks. Dental Directors should ask themselves “How much money do I want to make from my clinic”, “How many patients/procedures per day do I need to treat in order to meet this goal” “How many days of the week do I want to work at the SBOHC”. Please keep the following objectives in mind when setting goals:
-‐ Understanding Capacity -‐ Using Appointment Schedule Strategically -‐ Manage No-‐Shows/Last Minute Cancellations -‐ Manage Emergencies Effectively -‐ Document Denti-‐Cal Patient -‐ Document Private Insurance Patient -‐ Manage Billing Process Effectively -‐ Manage Reimbursement Denial Rate Effectively -‐ SBOHC Productivity
Measurable Objectives:
Having the tools to evaluate a Dental Program’s financial performance is very important for a clinic’s sustainability and financial success.
Dental Directors should manage patient dental insurance types and frequency among the different types of insurance because within a SBOHC, dental Insurance dictates future revenue. Dental Directors should obtain their SBOHC’s schedule a week in advance, in order to check patient insurance status and to calculate the number of Denti-‐Cal Patients (70%-‐ 9 to 10 Patients per day), Private Insurance Patients (15%-‐ 1 to 2 patients per day), and Non-‐Insurance Patients (15%-‐ 1 to 2 patients per day). This allows the SBOHC to schedule more patients if needed, with the purpose of breaking-‐even and meeting financial goals.
The following Financial tools should be calculated every one to two weeks:31
31 DentaQuest Institute “Map To The Future: Back Mapping School Based Oral Health To Achieve Financial Sustainability”
The Center For Oral Health SBOHC Operations Manual
-‐ Number of visits-‐ Patient Count -‐ Number of visits-‐ Procedure Count -‐ Total Weekly Expenses (direct and indirect) -‐ Total Weekly Net Revenue (including all sources of revenue) -‐ Expense/visit -‐ Revenue/visit -‐ Transactions (procedures by ADA code) -‐ No-‐show rate-‐ Less than 15% -‐ Accounts receivable-‐ 90 days = 5% -‐ Emergency rate -‐ Number of New Patients -‐ Percentage of completed treatments -‐ Number of FTE providers (dentists) -‐ Break-‐Even Analysis -‐ Individual SBOHC Goals/Deliverables
Managing Reimbursement Denial Rates Effectively: In order to maximize efficacy, SBOHC’s should thoroughly review all “Explanation of Benefits” as they come in from Denti-‐Cal. SBOHC’s should keep their Reimbursement Denial Rates at and or below 5% in order to Maximize sustainability. (See Finance Reimbursement for more information on Explanation of Benefits) Evaluating Success: Sustainability is a buzzword for most of the programs related to access to care. We need to be able to recoup enough through Medicare-‐ Denti-‐Cal to justify the funding necessary to implement these clinics. That being said – all dental disease is preventable. That behooves us to emphasize the core modalities that will give us the results toward optimum dental health. Education, Fluoride treatments, Recall (maintenance) visits, and sealants are all ways to lower the needed utilization rate and keep patients healthy. The less we have to treat, the less costly it takes to provide health. The typical maintenance visits are the surest way to provide a roadmap as to how healthy a patient is getting. The lowering of the DMF ratio each visit is surely the best indicator. Ideally, a patient should get needed treatment completed and thereafter not need anything but maintenance. Patient Satisfaction Survey The Patient Satisfaction Survey is a short, easily administered questionnaire that is

THE CENTER FOR ORAL HEALTH
61
designed to provide the SBOHC with information and insight on patient’s view of the services rendered. There are four mechanisms to assess patient satisfaction with dental care received at the SBOHC:
1. All Patients receiving care during any clinic period can fill out a daily survey regarding the care that day. The data compiled from these surveys will be used to monitor the SBOHC coverage and services.
2. Following the completion of comprehensive care, the patient is asked to rate their satisfaction with the care received during the comprehensive care clinical exam.
3. During the six (6) month recall appointment or mid annually during patient care.
4. Patients who inform a SBOHC staff member that they wish to document their experience.
The data should be complied and maintained by the Dental Director and or Site Coordinator. The SBOHC should use survey results to design and track quality improvement over time. In addition, the information resulting from the surveys should serve as a guideline for suggesting program or infrastructure changes.

The Center For Oral Health SBOHC Operations Manual
Evaluation Appendix D1 Appendix N1: Sample Patient Satisfaction Survey Appendix N2: Self-‐Assessment
THE CENTER FOR ORAL HEALTH
63
Marketing Recruitment
Incentives
Education and Prevention Material

The Center For Oral Health SBOHC Operations Manual
Marketing Marketing strategies will vary from site to site. For the purposes of this manual, we have based all our findings and recommendation off of the LAUSD-‐ Murchison Street Elementary School 2010-‐2014 and EMCSD-‐ Gidley Elementary School 2012-‐2014 SBOHC Marketing approach. Recruitment: Opening a SBOHC can be very rewarding, however without patients there can be no Clinic. Marketing ones SBOHC is very important for recruitment and retention. When actively recruiting community members and school age children, the Site Coordinator is responsible for informing residents what a SBOHC is and what the Clinic can do for them and their family. The entire SBOHC Staff should be able to explain the different treatments offered, be able to help in the process of Denti-‐Cal enrollment, and be ready for scheduled Appointments.
The following lists appropriate recruitment tools:
• Parent/Guardian Pre-‐Service Letter • Parent/Guardian Consent Form • SBOHC Banner • SBOHC Information Brochure • SBOHC Information Flier • Social Media-‐ Facebook, Twitter
It is important that the Dental Director and Site Coordinator know their SBOHC surroundings. Is there a Head Start and or Daycare nearby? If so, the Site Coordinator should talk with the Head Start and Daycare owners; explain what a SBOHC is, what services the SBOHC offers, hours of operations and what types of Insurance the SBOHC takes. Reaching out to community members is a very important part of becoming a community driven and centered organization. The Site Coordinator should leave SBOHC Information Brochures and Bulletins at nearby establishments, where young children and families might attend often. (I.E. Parks, Laundromat, Grocery Store) Incentives
Both LAUSD-‐ Murchison Street Elementary School and EMCSD-‐ Gidley Elementary School SBOHC uses incentives to increase patient participation. This is a great way to build your SBOHC reputation and increase patient count.
For Example, Teacher Cover letters should state the following:

THE CENTER FOR ORAL HEALTH
65
“A $50 gift card to staples will be offered to the first 3 teachers whose classroom collects the most consent forms by such and such date”. Refer to Daily Operations Appendix B1 for am example of a Teacher Cover Letter & Marketing Appendix E for examples of using incentives to attract patients.
Education and Prevention Material:
The Site Coordinator should pass out Education Material during regular business hours to Patients and Parents/Guardians. Site Coordinators should be able to answer and or direct any questions a Patient and or Parent/Guardian may have about Dental Hygiene.
The Center For Oral Health SBOHC Operations Manual
Marketing Appendix E1-‐E5 Appendix E1: SBOHC Banner Template Appendix E2: SBOHC Information Brochure Appendix E3: Denti-‐Cal Information Letter Appendix E4: Principle Award Letter Appendix E5: Teacher Award Letter & Certificate Appendix E6: Education and Prevention Material

THE CENTER FOR ORAL HEALTH
67
Policy, Licenses, Safety Compliance, and Taxes SBOHC Policy
Licenses
State of California Regulations
Patient Bill of Rights
Safety Compliance
Taxes

The Center For Oral Health SBOHC Operations Manual
Patient Records, Licenses, Patient Care Policies, and Taxes
Patient Records: Ever SBOHC must keep accurate and complete Patient Dental Records, both handwritten as well as electronic through a secure web-‐based system. Dental Directors should use the same system they use in their Private Practice. Patient Dental Records should be kept in a locked and secure file box that is accessible by key only. The dental records are not to be transferred unless in a fireproof, locked, and secure file cabinet. All patients’ records should remain at its designated SBOHC locked and secured. SBOHC Staff are the only ones accessible to patient records. No other persons are allowed access to the patient records. Release of Patient Dental Records32
Release of patient dental records and information is limited to patient/patient/guardian only. Unless patient/parent/guardian specifies in the “Permission to Share Information” consent, no other individual is allowed accessibility to the patient’s records. Patient Dental Records Contain the Following32
1. Patient Registration Sheet, Signed by patient/parent/legal guardian 2. Copy of patients insurance or Medicaid Card 3. HIPPA, Notice of Privacy Practices, Permission to Share Information paper 4. Image Release Form 5. Medical History; Dental History, Social History Paper 6. Medical Release (As Needed) 7. Parent/Guardian Substitution (If Necessary) 8. Referrals 9. Dental Examination-‐ Intraoral/Extraoral examination form, CAMBRA, hard tissue charting and treatment plan on treatment planning worksheet; Periodontal recording sheet (If Necessary); in formed consents and post-‐operative instructions (On Case by Case Basis) 10. Progress Notes 11. X-‐ray Radiation Log 12. Copy of School Absence Release Form 13. Patients Digital X-‐rays in Electronic Billing System on secure network 32http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

THE CENTER FOR ORAL HEALTH
69
HIPAA, Notice of Privacy Practices, and Permission to Share Information All patients will be provided with a New Patient Consent Form to the Use and Disclosure of Health Information for Treatment, Payment, or Healthcare Operation. The patient will also be given a Notice of Privacy Practices Form, which will provide further information on uses and disclosures. Furthermore, the patients (or parents/guardians) are provided with a Permission to Share Information Form, which will allow the patient (or the patient’s parent/guardian) to give authorization to disclose health and dental information to the persons listed on the form. The forms are both in English and Spanish.33 Informed Consent The patients (or parent/guardian) will be provided a General Informed Consent on the Child Permission Slip for Free Dental Care Form or a General/Limited Treatment Consent Form for adults. The forms are both in English and Spanish.33
Medical History Documentation Patient Medical History is gathered from information provided on the Medical History Form For Minors (Children 0-‐17) years of age, or the Adult Medical History Form for any patients 18 years of age or older. The Medical History must be verbally reviewed with the patient or the patient’s parent or guardian. The forms are both in English and Spanish.33
Intraoral/Extraoral, Soft and Hard Tissue, and Clinical Findings For all comprehensive and periodic examinations, the patient will have an Intraoral/Extraoral examination-‐ including an oral cancer screening. In addition, the patient will undergo a soft and hard tissue examination, including but not limited to oral pathologies, TMJ, primary/permanent dentition classification both in the canines and first molars, and orthodontic review. The Clinical Findings Worksheet consists of recording all existing restorations, clinical findings, radiographic findings, and creating a recommended treatment per tooth. The Clinical Findings Worksheet will also list the periodontal treatment plan based on the amount of plaque and calculus present supra/sub-‐gingival, tissue health, and in permanent dentition-‐ recession and furcation involvement. Mobility would also be noted on the worksheet. 33
33http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf
The Center For Oral Health SBOHC Operations Manual
CAMBRA The Caries Management By Risk Assessment (CAMBRA) document gathers data based on the patient’s disease indicators, risk factors, and protective factors. By compiling the data, the patient’s caries risk is identified, and therefore, the proper treatment or recommendation of products can be specialized towards the patient. Treatment Plan The Treatment Planning Form will be a summary of periodontal and clinical findings with respective recommended treatments. The treatment, which includes both preventative and diagnostic treatment, will be sequenced and discussed with Patient or Parent/Guardian. The treatment plan will be initialed by the Dental Director as well as signed by the Patient or Parent/Guardian.34
Consent Forms
Prior to oral surgery and endodontic procedures (including pulpotomies), the Patient or Parent/Guardian will have to sign the informed Consent Forms in order to acknowledge the risks of the procedure. The Patient or Parent/Guardian will also be provided with post-‐op instructions related to the treatment. All other treatments (such as the exam, radiographs, preventative and periodical treatment, or restorative treatment) will be signed by the Patient or Parent/Guardian in The General Informed Consent Form. For emergency procedures, a General/Limited Consent Form is also available which will cover extractions and pulpectomies. 34
Patient Complaints and Incidents Patient Complaints A patient complaint is generally an expression of dissatisfaction from a patient or a person on behalf of the patient, which requires a response. Most SBOHC patient complaints will be considered informal complaints and resolved promptly, on the spot, by staff or faculty. For example, relatively minor patient complaints, such as appointment issues, will be resolved promptly, on the spot by staff present and would not require a written response. It is important that all information related to the complaint is documented in the patient’s chart. Patient complaints are to remain confidential and documented in the patient’s chart. Patient complaints are to remain confidential and only shared with SBOHC and School Staff who are relevant to the issue.34
34http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

THE CENTER FOR ORAL HEALTH
71
Tip: Grievances received in a language other than English will require formal translation of all written communications, and interpreter services are required for oral communications with the person making the complaint. If SBOHC Staff cannot resolve a patient’s complaint quickly informally, Staff must complete Complaint/Grievance Form. Within Four business days of receiving a complaint/grievance the Dental Director should do the following:35
1. Send Formal letter to the grievant to acknowledge receipt of the concern and to provide information regarding additional resources for complaint/grievance resolution 2. Maintain a record in the Complaint and Grievance Binder 3. Coordinate an investigation into the matter. The investigation should include, but is not limited to:
a. A review of documentation of the diagnosis and treatment plan b. A review of treatment notes c. Possible clinical exam of the patient d. Possible interviews of staff or persons involved.
Upon final resolution of the complaint/grievance, Dental Director will send a letter to the grievant. As required by federal law, the letter must provide the patient with written notice of its decision that contains:35
1. The name of The SBOHC contact person 2. The steps taken on behalf of the patient to investigate the grievance 3. The results of the grievance process 4. The date of completion of the investigation
A copy of the letter to the grievant will be entered into the Complaints and Grievance Binder. Licenses: All SBOHC Staff Members having direct contact with patients should have the appropriate credentialing. All SBOHC Staff is personally responsible for maintaining all credentials in current status.
35http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

The Center For Oral Health SBOHC Operations Manual
Dental Director
Required Credentialing36
• Valid California Dental License • Current CPR Certification • Current DEA Certification • National Provider Identifier (NPI) • Proof of Hepatitis B Vaccination or Declination Statement • Tuberculosis Skin Test results and follow-‐up needs on file • Other Vaccinations as required
Registered Dental Assistant Required Credentialing36
• Valid California Dental Hygiene License • Current CPR Certification • Proof of Hepatitis B Vaccination or Declination Statement • Tuberculosis Skin Test results and follow-‐up needs on file • Other Vaccinations as required
Site Coordinator Required Credentialing36
• Current CPR Certification • Proof of Hepatitis B Vaccination or Declination Statement • Tuberculosis Skin Test results and follow-‐up needs on file • Other Vaccinations as required
State of California Regulations In 2013, the State of California passed the Senate Bill Number 562, Galgiani. Dentists: Mobile or Portable Dental Units. Although passed, SB 562 has not been implemented yet. As of 2014, the state of California has no regulations implemented regarding Portable Dental Operations (PDO). [Approved by Governor October 7, 2013. Filed with Secretary of State October 7, 2013.]
36http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

THE CENTER FOR ORAL HEALTH
73
SB 562, GALGIANI. DENTISTS: MOBILE OR PORTABLE DENTAL UNITS
Existing law, the Dental Practice Act, provides for the licensure and regulation by the Dental Board of California of those engaged in the practice of dentistry. Existing law provides that a person practices dentistry if the person, among other things, manages or conducts as manager, proprietor, conductor, lessor, or otherwise, in any place where dental operations are performed. Existing law authorizes a dentist to operate one mobile dental clinic or unit that is registered and operated in accordance with regulations adopted by the board. Existing law exempts specified mobile units from those requirements. Other provisions of existing law, the Mobile Health Care Services Act, require, subject to specified exemptions, licensure by the State Department of Health Care Services to operate a mobile service unit. This bill would eliminate the one mobile dental clinic or unit limit and would require a mobile dental unit or a dental practice that routinely uses portable dental units, as defined, to be registered and operated in accordance with the regulations of the board. The bill would require any regulations adopted by the board pertaining to these matters to require the registrant to identify a licensed dentist responsible for the mobile dental unit or portable practice, and to include requirements for availability of follow up and emergency care, maintenance and availability of provider and patient records, and treatment information to be provided to patients and other appropriate parties. 37 Patient Care Policies Bill of Rights: Each SBOHC uses The State of California’s Patient Bill of Rights to describe the patient’s rights in obtaining and receiving treatment. This document is provided during registration to the patient seeking comprehensive oral health care at the SBOHC. The State of California’s Patient’s Bill of Rights are available in both English and Spanish. Refer to http://www.calpatientguide.org for more information.38 The State of California’s Patient’s Bill of Rights (Every SBOHC Patient is entitled to)38
• The most appropriate care the SBOHC can provide to address the Oral Health needs
• Considerate, Respectful and Confidential Care • Continuity and Completion of Treatment • Access to complete and current information about the patient’s condition
37https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=201320140SB562 38http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

The Center For Oral Health SBOHC Operations Manual
• Advance knowledge of the cost of treatment and explanation of treatment fees • Explanations of recommended treatment, alternate treatment, the option to
refuse treatment, and the risk of no treatment • Treatment that meets the standards of care in the Profession • Access to a patient advocate
Confidentiality and HIPPA To maintain the confidentially of patient information and medical records, California has enacted the following set of policies and standards to protect patients: The health Insurance Portability and Accountability Act of 1996 (HIPPA), the Health Information Technology for Economic and Clinical Health Act (HITECH Act), The California Confidentiality of Medical Information Act, The California Patient Access to Health Records Act, and other stet health information privacy laws.39
All SBOHC Staff Members are held accountable to the aforementioned policies and laws and have been fully informed about maintain patient confidentiality.39 OSHA & Infection Control Compliance Regulation of OSHA and Infection control is the responsibility of the SBOHC.
Infection Control Protocol It is the policy of the SBOHC that Standard Precautions, as defined by the Centers for Disease Control and Prevention (CDC), be followed at all times to assist in the prevention or the transmission of infectious agents to Healthcare Providers, SBOHC Staff, Students, Patients and Visitors.39 Biohazardous Waste and Sharp Products It is the policy of the SBOHC to preserve the health and safety of its Healthcare Providers, SBOHC Staff, Students and Patients through the proper identification and disposal of biohazards waste and sharp products.39 Procedure for the Disposal of Biohazardous Waste:39
1. The Central Biohazardous waste container marked Biohazardous Sharp Waste Bin is located inside SBOHC 2. SBOHC Staff will collect the Red Biohazardous Waste Bag and dispose of the Biohazardous waste bag to the central Biohazardous Sharp Waste Bin 3. The RDA will collect and dispose of the full Biohazardous waste bin by placing the mailing slip on the Biohazardous Sharp Waste Bin, and contacting the US postal service for pick-‐up
39http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

THE CENTER FOR ORAL HEALTH
75
Procedure for the Disposal of Sharps Products:40
1. Two labeled and red sharp containers are located within the open operatory room and next to the sink 2. SBOHC Staff will dispose of all sharps, including anesthetic cartridges in the sharps container 3. The RDA will dispose of all the full sharps container by placing the red marked sharps containers inside the Biohazardous Waste Sharps Bin along with the Red Biohazardous Waste Bags 4. The mailing slip will be placed on the outside of the Biohazardous Sharps Waste Bin and the US postal service should be called for pick-‐up Cleaning and Disinfecting of Dental Equipment Cleaning supplies, Ultrasonic Cleaning Solution, and Autoclave should be placed in a controlled area (i.e. Under the Sink, Locked Cabinet)40
At the Beginning of Each Day Lines should be flushed and purged with Ultrasonic Cleaning Solution diluted according to manufacturer instructions. Dental units, chairs, and all equipment should be wiped down using Cavi-‐wipes and out away. Wastewater should be disposed of.40
Daily Guidelines for Clinical Infection Control Patient material (e.g., Oral Microorganisms, blood, and saliva) can enter the dental water system during patient treatment. To clean water system, remove hand-‐piece, wipe with Cavi-‐Wipes, and place on tray for sterilization. Dispose of contaminated soiled waste in biohazard container. Place all instruments in cassettes for sterilization. Remove all gross debris remaining on the instruments prior to placement in cassettes for sterilization. Remaining dental materials/biologic material will result in difficulty of removal in the future, as well as malfunctioning of supplies.40
At the End of Each Day Raise patient chair halfway and place hand-‐piece pedal on the base of unit chair. Turn off Master Switch. Remove water bottle dispenser, discard any extra water and leave bottle to dry. Run suction lines with Biorex Solution.40
40http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

The Center For Oral Health SBOHC Operations Manual
Sterilization and Disinfection of Patient-‐Care Items41 Category Definition Process By Examples
Critical
Penetrate Soft Tissue or Bone
Sterilization Surgical Instruments Periodontal Scalars Surgical Dental Burs
Semi-‐Critical
Contact Mucous Membranes or Non-‐intact Skin
Sterilization or High-‐Level Disinfection
Dental Mouth Mirrors Amalgam Condensers Dental Hand pieces Most Hand Instruments
Non-‐Critical Contact on Intact Skin
Low-‐to-‐Intermediate-‐ Level Disinfection
X-‐Ray Head/Cone Blood-‐Pressure Cuff Facebow
Patient-‐care items (Dental Instruments, Devices, and Equipment) are categorized as Critical, Semi-‐Critical, or Non-‐Critical, depending on the potential risk for infection associated with their intended.41
• Critical items used to penetrate soft tissue or bone has the greatest risk
of transmitting infection and should be sterilized by heat. • Semi-‐Critical items touch mucous membranes or Non-‐Intact skin and
have a lower risk of transmission; because the majority of Semi-‐Critical items in dentistry are heat-‐tolerant, they also should be sterilized by using heat. If a Semi-‐Critical item is heat-‐sensitive, it should, at a minimum, be processed with high-‐level disinfection.
• Non-‐Critical patient-‐care items pose the least risk of transmission of infection, contacting only intact skin, which can serve as an effective barrier to microorganisms. In the majority of cases, cleaning, or if visibly soiled, cleaning followed by disinfection with an EPA-‐Registered hospital disinfectant is adequate.
• Cleaning or disinfection of certain Non-‐Critical patient-‐care items can be difficult or damage the surfaces; therefore, use of disposable barrier protection of these surfaces might be a preferred alternative
• FDA-‐cleared sterilant/high-‐level disinfectants and registered disinfectants must have clear label claims for intended use, and manufacturer instructions for use must be followed.
Personal Protective Equipment (PPE) It is the policy of the SBOHC to provide guidance to staff on what to wear for eye protection and how to use the sink as a substitute eyewash station. 41
41http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

THE CENTER FOR ORAL HEALTH
77
Hand Hygiene It is the policy of the SBOHC that all Healthcare Providers, Staff Members, and Patients utilize hand-‐hygiene/hand-‐care techniques in order to reduce the transmission of pathogenic microorganisms to patients and other personnel. 42 Taxes: Dental Directors should report income according to the liability status of their Private Practice. Denti-‐Cal reimbursements are taxable income. Dental Directors should consult a tax attorney to make sure they are in compliance with the liability issues associated with their company status.
42http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

The Center For Oral Health SBOHC Operations Manual
Policy, Licenses, Safety Compliance, and Taxes F1-‐F3 Appendix F1: Radiation In Daily-‐Life Appendix F2: Personal Protective Equipment Chart Appendix F3: Senate Bill No. 562

THE CENTER FOR ORAL HEALTH
79
Fire, Earthquake, and Natural Disaster Protocols Fire, Earthquake, and Emergency Plan

The Center For Oral Health SBOHC Operations Manual
Fire, Earthquake, and Natural Disaster Protocols
Fire, Earthquake, and Emergency Plan: This plan sets out instructions and procedures for The SBOHC in the event of fire or emergency that occurs at the dental practice when Staff is present Fire & Emergency43
• In the event of a fire, call local fire department (911), notify other staff, patients, and visitors and exit the building. (Coordinate a safe spot to meet)
• The Staff are responsible for the accountability of the patients. A SBOHC Patient sign-‐in book should be used as a way to account for all patients safely exiting the building
• In the event of an earthquake, move safely to areas in the SBOHC that offer protection from or away from falling items. SBOHC Staff may direct patients and visitors to a safe area
• In the event of a power outage, and the practice relies on electric illumination, wait until eyes adjust to the low light prior to moving
Fire Prevention43
• When utilizing heat producing equipment, make sure that the area is clear of all fire hazards and all sources of potential fires are eliminated
• Have fire extinguishers available at all times when utilizing heat-‐producing equipment
• Know the location of fire-‐fighting equipment in the work area and have knowledge of its use and application. Use these devices only in cases of fire
• Portable fire extinguishers are inspected, maintained, and tested regularly. Records of inspections are maintained
• Keep all flammables away from ignition sources • Maintain sufficient access and working space around electric equipment
Exits43
• All exit doors and or openings must be clear and unobstructed at all times. • All exits are arranged so that it will not be necessary to travel towards any area
with a hazard in order to reach the nearest emergency and evacuation route.
43http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

THE CENTER FOR ORAL HEALTH
81
• Aisles and hallways shall be kept clear at all times Compressed Gas Cylinders (Oxygen)44
• All gas cylinders shall have their contents clearly marked on the outside of each cylinder
• Cylinders must be placed and secured in an upright position, including storage and transfer
• Cylinder valves must be protected with caps and guards when not in use • All leaking or defective cylinders must be removed from service promptly, tagged
as inoperable and placed in an open space removed from work area • All operators are required to inspect equipment prior to utilization
Regulated Waste44
• Hazardous waste, universal waste, and medical waste are stored in appropriate containers in designated areas. Secondary containment is provided fro liquid wastes
Training and Education in Fire and Emergency Safety44
• All SBOHC staff must receive education on precautionary measures for fire and emergency as stated above prior to started work, and whenever procedures are changed
• If SBOHC students are expected to use portable fire extinguishers, they must be trained on its use and hazards of extinguishing fire
• All SBOHC Staff must be trained on how to make a safe and orderly exit from the facility
44http://www.mchoralhealth.org/Projects/granteePDFs/Gidley%20SBOHC%20Clinic%20Operations%20Manual_vCOPYRIGHTED%202013.pdf

The Center For Oral Health SBOHC Operations Manual
Fire, Earthquake, and Natural Disaster Protocols Appendix G1 Sample General Office Safety Plan

THE CENTER FOR ORAL HEALTH
83
Setting Up Facility Appendix A1-‐A7

The Center For Oral Health SBOHC Operations Manual
Appendix A1: LAUSD-‐ Organization Chart
School Year
2013-2014Board SecretariatJefferson Crain
Board of Education
Superintendent
John Deasy
Sr. Deputy Superintendent School Operations
Michelle King
Chief Strategy OfficerOff Chief Strategy Officer
Matt Hill
DirectorBudget Svcs & Fin. Planning
Tony Atienza
DirectorCharter Schools
Jose Cole-Gutierrez
General CounselDavid Holmquist
Chief of School PoliceSteven Zipperman
Inspector GeneralKen Bramlett
LAUSD Organization Chart – Effective July 1, 2013
Personnel DirectorPersonnel Commission
Janalyn Glymph
Chief Financial OfficerOff Chief Financial Officer
Megan K. Reilly
Chief Operating OfficerOff Chief Operating Officer
Enrique Boull’t
Chief Information OfficerInformation Technology
Ronald Chandler
Executive DirectorData & Accountability
Cynthia Lim
Executive DirectorStud Health & Human Svcs.
Debra Duardo
Educational Services Ctrs.
Administrators of Operations (5)
ChiefIntensive Support & Interv.
Donna Muncey
Educational Services Ctrs.
InstructionalSuperintendents (5)
Executive DirectorCurriculum, Instruction
& School Support
Gerardo Loera
Executive Director Special Education
Sharyn Howell
Executive DirectorAdult & Career Education
Donna Brashear
DirectorAsset Management
Krizstina Tokes
DirectorMaintenance & Operations
Roger Finstad
DirectorProject Execution
Greg Garcia
DirectorFacilities Contracts
Yvette Merriman-Garrett
DirectorProgram Support Services
Raju Kaval
Chief Facilities ExecutiveFacilities
Mark Hovatter
Executive DirectorHuman Capital Initiatives
Drew Furedi
Executive DirectorTalent Management
Rachel Bonkovsky
DirectorFed. & State Ed. Programs
Deborah Ernst
DirectorStudent Integration Svcs.
Estelle Luckett
Assistant Superintendent School Operations
Earl Perkins
Chief of StaffInternal Affairs
Edgar Zazueta
Chief HR OfficerHuman Resources
Vivian Ekchian
Executive DirectorParent Community Student Services
Rowena Lagrosa
DirectorCommunications & Media Rel.
Thomas Waldman
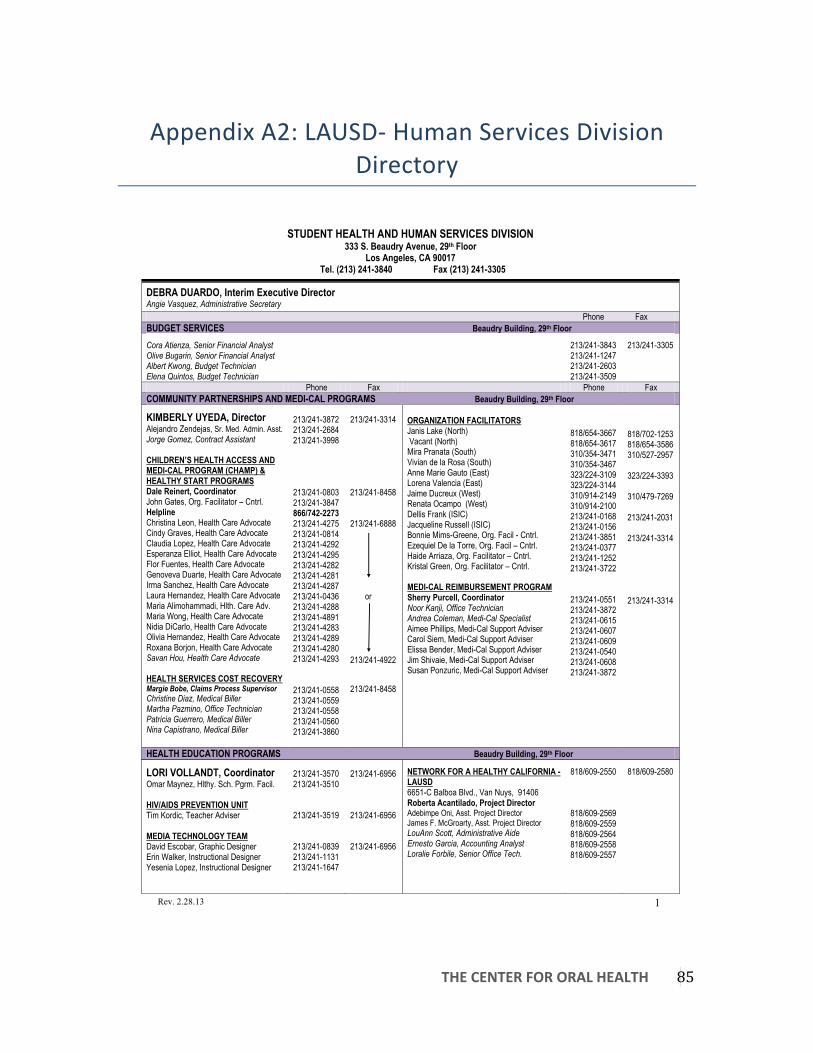
THE CENTER FOR ORAL HEALTH
85
Appendix A2: LAUSD-‐ Human Services Division Directory
STUDENT HEALTH AND HUMAN SERVICES DIVISION 333 S. Beaudry Avenue, 29th Floor
Los Angeles, CA 90017 Tel. (213) 241-3840 Fax (213) 241-3305
Rev. 2.28.13 1
DEBRA DUARDO, Interim Executive Director
Angie Vasquez, Administrative Secretary
Phone Fax BUDGET SERVICES Beaudry Building, 29th Floor
Cora Atienza, Senior Financial Analyst
Olive Bugarin, Senior Financial Analyst
Albert Kwong, Budget Technician
Elena Quintos, Budget Technician
213/241-3843 213/241-1247 213/241-2603 213/241-3509
213/241-3305
Phone Fax Phone Fax
COMMUNITY PARTNERSHIPS AND MEDI-CAL PROGRAMS Beaudry Building, 29th Floor
KIMBERLY UYEDA, Director Alejandro Zendejas, Sr. Med. Admin. Asst. Jorge Gomez, Contract Assistant
CHILDREN’S HEALTH ACCESS AND MEDI-CAL PROGRAM (CHAMP) & HEALTHY START PROGRAMS Dale Reinert, Coordinator John Gates, Org. Facilitator – Cntrl. Helpline Christina Leon, Health Care Advocate Cindy Graves, Health Care Advocate Claudia Lopez, Health Care Advocate Esperanza Elliot, Health Care Advocate Flor Fuentes, Health Care Advocate Genoveva Duarte, Health Care Advocate Irma Sanchez, Health Care Advocate Laura Hernandez, Health Care Advocate Maria Alimohammadi, Hlth. Care Adv. Maria Wong, Health Care Advocate Nidia DiCarlo, Health Care Advocate Olivia Hernandez, Health Care Advocate Roxana Borjon, Health Care Advocate Savan Hou, Health Care Advocate
HEALTH SERVICES COST RECOVERY Margie Bobe, Claims Process Supervisor Christine Diaz, Medical Biller
Martha Pazmino, Office Technician
Patricia Guerrero, Medical Biller
Nina Capistrano, Medical Biller
213/241-3872 213/241-2684 213/241-3998 213/241-0803 213/241-3847 866/742-2273 213/241-4275 213/241-0814 213/241-4292 213/241-4295 213/241-4282 213/241-4281 213/241-4287 213/241-0436 213/241-4288 213/241-4891 213/241-4283 213/241-4289 213/241-4280 213/241-4293 213/241-0558 213/241-0559 213/241-0558 213/241-0560 213/241-3860
213/241-3314 213/241-8458 213/241-6888 or 213/241-4922 213/241-8458
ORGANIZATION FACILITATORS Janis Lake (North) Vacant (North) Mira Pranata (South) Vivian de la Rosa (South) Anne Marie Gauto (East) Lorena Valencia (East) Jaime Ducreux (West) Renata Ocampo (West) Dellis Frank (ISIC) Jacqueline Russell (ISIC) Bonnie Mims-Greene, Org. Facil - Cntrl. Ezequiel De la Torre, Org. Facil – Cntrl. Haide Arriaza, Org. Facilitator – Cntrl. Kristal Green, Org. Facilitator – Cntrl. MEDI-CAL REIMBURSEMENT PROGRAM Sherry Purcell, Coordinator Noor Kanji, Office Technician
Andrea Coleman, Medi-Cal Specialist
Aimee Phillips, Medi-Cal Support Adviser Carol Siem, Medi-Cal Support Adviser Elissa Bender, Medi-Cal Support Adviser Jim Shivaie, Medi-Cal Support Adviser Susan Ponzuric, Medi-Cal Support Adviser
818/654-3667 818/654-3617 310/354-3471 310/354-3467 323/224-3109 323/224-3144 310/914-2149 310/914-2100 213/241-0168 213/241-0156 213/241-3851 213/241-0377 213/241-1252 213/241-3722 213/241-0551 213/241-3872 213/241-0615 213/241-0607 213/241-0609 213/241-0540 213/241-0608 213/241-3872
818/702-1253 818/654-3586 310/527-2957 323/224-3393 310/479-7269 213/241-2031 213/241-3314 213/241-3314
HEALTH EDUCATION PROGRAMS Beaudry Building, 29th Floor
LORI VOLLANDT, Coordinator Omar Maynez, Hlthy. Sch. Pgrm. Facil. HIV/AIDS PREVENTION UNIT Tim Kordic, Teacher Adviser MEDIA TECHNOLOGY TEAM David Escobar, Graphic Designer Erin Walker, Instructional Designer Yesenia Lopez, Instructional Designer
213/241-3570 213/241-3510 213/241-3519 213/241-0839 213/241-1131 213/241-1647
213/241-6956 213/241-6956 213/241-6956
NETWORK FOR A HEALTHY CALIFORNIA -LAUSD 6651-C Balboa Blvd., Van Nuys, 91406 Roberta Acantilado, Project Director Adebimpe Oni, Asst. Project Director James F. McGroarty, Asst. Project Director LouAnn Scott, Administrative Aide
Ernesto Garcia, Accounting Analyst
Loralie Forbile, Senior Office Tech.
818/609-2550 818/609-2569 818/609-2559 818/609-2564 818/609-2558 818/609-2557
818/609-2580

The Center For Oral Health SBOHC Operations Manual
STUDENT HEALTH AND HUMAN SERVICES DIVISION 333 S. Beaudry Avenue, 29th Floor
Los Angeles, CA 90017
Rev. 2.28.13 2
Phone Fax Phone Fax NURSING SERVICES 121 N. Beaudry Avenue, Los Angeles, 90012
DEE APODACA, DIRECTOR Monique Lowe, Senior Secretary Frances Yanez, Office Technician Lourdes Avila, Office Technician ASTHMA PROGRAM Yolanda Cuevas, School Nurse AUDIOMETRIC TESTING PROGRAM Carol Toyotome, Coordinator Alexandra Knepper, Senior Office Tech. CHILD HEALTH DISABILITY PROGRAM (CHDP) Connie Whalley, School Nurse COMMUNICABLE DISEASE (CD) PROGRAM CD Desk CD Reporting Barbara Woodard-Cox, School Nurse CONDOM AVAILABILITY PROGRAM Rick Loya, Project Connect Liaison DENTAL PROGRAM Roberta Villanueva, School Nurse
213/202-7580 213/202-7534 213/202-7588
213/202-7533 213/202-7575 213/202-7576 213/202-7525 213/202-7543 213-202-7595
213/580-6557 213/580-6557 213/580-6557 213/580-6558 213/580-6557 213/580-6557 213/580-6557
FIELD COORDINATORS Tricia Chicagus (ESC-North) 6505 Zelzah Avenue, Building #7 Reseda, 91335 Minoo Maasoumi (ESC-South) 1208 Magnolia Avenue, Gardena, 90247 Yolanda Lasmarias (ESC-East) 3921 Selig Place, Los Angeles, 90031 Ruby Pugh (ESC-West) 333 S. Beaudry Avenue, 20th Floor Los Angeles, 90017 Vickey Conley (ISIC) 333 S. Beaudry Avenue, 20th Floor Los Angeles, 90017 OTHER PROGRAMS Othello Childress, Field Coordinator Aurelio Cobangbang, Office Technician Diabetes Prevention Nurse Family Partnership Obesity Prevention Wellness Centers QUEENSCARE DENTAL/VISION PROGRAM Carmen Montes, School Nurse SPECIAL PROGRAMS Serop Hakimian, Field Coordinator AED/CPR Charter/Option Schools Infant Pre-School Program (ECE) Non-Public Schools Special Education Resource Program
818/654-1670
310/354-3550
323/224-3325
213/241-1902 213/241-0164 213/202-7530 213/202-7540 213/202-7531 213/202-7532
818/758-9961 310/523-3249 323/224-3105
213/241-2592 213/241-2031 213/580-6557 213/580-6557 213/580-6557
PUPIL SERVICES Beaudry Building, 29th Floor
ERIKA TORRES, INTERIM DIRECTOR Maria Castro, Coordinator Elsa Garcia-Sanda, District Counselor Maricela Serrano, District Counselor Nancy Soto, District Counselor Nicole Mitchell, District Counselor Sonia Solis, District Counselor Stephan Blustajn, District Counselor Teresa Garcia, District Counselor Wendy Tamaki-Ogata, District Counselor Yvette, Zavala, District Counselor Zhaira Gastelum, District Counselor Gloria Zuniga, Senior Office Tech. Luz Monreal, Senior Secretary
213/241-3844 213/241-8605 213/241-1759 213/241-1258 213/241-1663 213/241-0754 213/241-3930 213/241-0594 21/3241-3520 213/241-3523 213/241-7673 213/241-2218 213/241-3852 213/241-3844
213/241-6858
ATTENDANCE IMPROVEMENT PILOT PROGRAM Alicia Garoupa, Interim Coordinator Vacant , Lead Counselor (North) Linet Danoukh, Lead Counselor (North) Francis Fernandez, Lead Counselor (South) Michelle Castelo, Lead Counselor (South)
Martha Godinez, Lead Counselor (East) Nisha Narsai, Lead Counselor (East) Angela Garcia, Lead Counselor (West) Michelle Cauley, Lead Counselor (West) CITY PARTNERSHIP Emily Hernandez, Coordinator DIPLOMA PROJECT PROGRAM Tawnya Perry, Program Director Martha Calderon, Coordinator Leilani Morales, Central Counselor Chan Cao, PSA Aide Delisa Wright, PSA Aide
213/241-2620 818/654-3657 818/654-3657 310/354-3214 310-354-3293 213/241-3081 213/241-3061 310/914-2163 213/241-2798 213/241-3571 213/241-3858 213/241-3855 213/241-3522 213/241-3521
213/241-3521
213/241-3305 818-881-0772 310-771-0943 310-771-0943 213/241-6858 213/241-6858 310-974-7174 213/241-6858 213/241-6868 213/241-6858

THE CENTER FOR ORAL HEALTH
87
STUDENT HEALTH AND HUMAN SERVICES DIVISION 333 S. Beaudry Avenue, 29th Floor
Los Angeles, CA 90017
Rev. 2.28.13 3
Phone Fax Phone Fax PUPIL SERVICES – cont’d Beaudry Building, 29th Floor
FIELD COORDINATORS Pat Jimenez (ESC-North) 6505 Zelzah Avenue, Building #7, Reseda, 91335
Edith Miller, SARB Chairperson Krista Conley, SARB Chairperson Shira Scherb, PSA Counselor Dionne Ash (ESC-South) 1208 Magnolia Avenue, Gardena, 90247
Cecilia Alexander, SARB Chairperson Velma Davis, SARB Chairperson Erin Campbell (ESC-East) 2151 N. Soto Street, Los Angeles, 90017
Lissette Gomez, SARB Chairperson Yesenia Valadez, SARB Chairperson Selena Ledesma, PSA Counselor Pat Burt (ESC-West) 333 S. Beaudry Avenue, 20th Fl., Los Angeles, 90017
Garyn Valdemar, SARB Chairperson Stephanie Lartelier, SARB Chairperson Tamara Robinson, PSA Counselor Valerie Corcoran (ISIC) 333 S. Beaudry Avenue, 11th Floor Los Angeles, Ca 90017 Mario Vega, SARB Chairperson Rafael Rubalcava, SARB Chairperson Martha Lopez, PSA Counselor Wanda Soohoo, PSA Counselor FOREIGN STUDENT ADMISSIONS Nancy Gutierrez, Coordinator Elsa Garcia-Sanda, District Counselor Nicole Mitchell, District Counselor
FOSTER CARE PROGRAM AND NEGLECTED OR DELINQUENT YOUTH PROGRAM Norma Sturgis, Coordinator Karen Timko, Specialist Margaret Smith, Specialist Cheryl Wong, Secretary Chris Sanco, Counselor Aide Deirdre Washington, Counselor Aide Latrica Stewart, Counselor Aide Foster Care – Counselors La Shona Jenkins (South) Norlon Davis (West & ISIC) Maral Sousani (North & East)
818/654-5082
818/654-5087 818/654-5088 818/654-5084 310/354-3209
310/354-3211 310/354-3214 323/224-5905
323/224-5902 323/224-5916 323/224-5901 213/241-7858
213/241-0472 213/241-0461 213/241-0453 213/241-0101
21/3241-0192 213/241-0162 213/241-3903 213/241-3903
213/241-1759 213/241-0754
213/241-3848 213/241-3552 213/241-3551 213/241-3842 213/241-0761 213/241-0420 213/241-3553 310/354-3227 213/241-1273 818/654-5086
818/654-1618 310/771-0943
323/224-3105 213/241-4108 213/241-3350
213/241-6858 213/241-3305 310/771-0943 213/241-3305 818/654-1618
Neglected or Delinquent - Counselors Althea Howard (Central & ISIC) Cesar Chaparro (East) Christine Kae (Central) Dexter Goseng (West) Marcia Price (South) Paul Schuster (North) Sonia Avalos (Central) HOMELESS EDUCATION PROGRAM 121 N. Beaudry Avenue, Los Angeles, 90012
Nancy Gutierrez, Coordinator Raul Paniagua, Administrative Aide Counselors Ana Quintero, Special Population Angela Midgette Chandler (North) Crisalia Aranibar (South) Jaime Corral (East) Laura Ewing (West) Monica Santana (East/North) Tracy Peeples (South/West) Parent Resource Liaisons Tammy Wood (North/West) Lisa Thompson (East/South) PSA Aides Judy Luna Karla Arnold Rocio Esqueda ShaunDrea Brooks PERMITS AND STUDENT TRANSFERS 333 S. Beaudry Avenue, 29th Fl., Los Angeles, 90017
Nancy Gutierrez, Coordinator Kevin Paquini, PSA Aide Vacant, PSA Aide
213/241-0459 213/241-1687 213/241-0760 213/241-0467 310/354-3225 818/654-3635 213/241-0467 213/202-7581
213/202-7518 213/202-7511 213/202-7574 213/202-7516 213/202-7512 213/202-7513 213/202-7517 213/202-7515 213/202-7589 213/202-7523 213/202-7522 213/202-7519 213/202-7520 213/202-7521 213/241-3844
213/202-7524 213/202-7579
213/241-4108 213/241-3305 213/241-3305 213/241-4108 310/771-0943 818/881-0527 213/241-4108 213/580-6551
213/580-6551
213/580-6551 213/580-6551 213/241-6858
213/580-6551

The Center For Oral Health SBOHC Operations Manual
STUDENT HEALTH AND HUMAN SERVICES DIVISION 333 S. Beaudry Avenue, 29th Floor
Los Angeles, CA 90017
Rev. 2.28.13 4
Phone Fax Phone Fax SCHOOL MENTAL HEALTH Beaudry Building, 29th Floor PIA ESCUDERO, Director Cecilia Ramos, Interim Asst. Director Elena Jimenez, Organization Facilitator Daemion Nooner, Administrative Analyst Rosa Castaneda, Secretary Sandy Jones-Seck, Sr. Office Technician Steven Fong, Administrative Analyst Yamilet Renderos, Senior Secretary CRISIS COUNSELING INTERVENTION Ailleth Tom, Coordinator FIELD COORDINATORS Kezia Miller (North) 6651 Balboa Boulevard, Van Nuys, 91406 Joel Cisneros, Specialist Vacant, Specialist Karen Wallace – Interim Coord. (South) 97th Street School Mental Health Clinic 439 W. 97th Street, Los Angeles, 90003 Beatriz Garcia, Specialist, Specialist
Bell / Cudahy School Mental Health Clinic 7326 S. Wilcox Avenue, Cudahy, 90201 Gloria Granados, Specialist Carson Family Resource Center 340 W. 224th Street, Carson, 90745 Gage Satellite San Pedro School Mental Health Clinic 708 W. 8th Street, San Pedro, 90731 Vacant, Specialist
213/241-3841 213/241-0834 213/241-3516 213/241/0833 213/241-3841 213/241-0834 213/241-0831 213/241-3515
213/241-2174 818/758-2300 323/754-2856 323/869-1352 310/513-8070 323/371-8857 310/832-7545
213/241-3305 213/241-3305 818/996-9850 323/754-1843 323/564-5825 310/513-6766 310/833-8580
FIELD COORDINATORS - cont’d Socorro Valderrama (East) 2151 N. Soto Street, Los Angeles, 90032 Griffith Satellite
Ramona HS School Mental Health Clinic 231 S. Alma Ave., Room 128, L. A., 90063 Marlene Hollis, Specialist Roybal Learning Center (Wellness Clinic) 1200 W. Colton St., Los Angeles, 90026 Monica Puentes, Specialist Nancy Jefferson (West) Hyde Park School Mental Health Clinic 6519 S. 8th Ave., Bungalow. #46 Los Angeles, 90043 Kim Griffin-Esperon, Specialist Martha Marquez (ISIC) 333 S. Beaudry Ave., 11th Floor Los Angeles, 90017 INTERNS / FIELD INSTRUCTION LEAD Maria Hu-Cordova, Psychiatric Social Wkr. SUICIDE PREVENTION Isabel Vaquero, Psychiatric Social Worker TRAUMA SERVICES ADAPTATION CENTER Joshua Kaufman, Psychiatric Social Wkr. Julie Cho, Psychiatric Social Worker
323/224-3363 323/266-7421
323/266-7615 323/560-6415 323/560-6416 323/750-5167 213/241-2612 213/241-3514 213/241-1259 213/241-0832 213/241-3517
323/224-3140 323/266-7695 323/224-3140 323/759-2697 213/241-2031 213/241-3305 213/241-3305
213/241-3305
STUDENT MEDICAL SERVICES 121 N. Beaudry Avenue, Los Angeles, 90012
KIMBERLY UYEDA, DIRECTOR Jocelyn R. Zalewski, Medical Admin. Asst. Marisol De la Rocha, Student and Family Resources Navigator School Physicians Guilda Eshtehard (North) Stephanie Quarles (South) Patricia Nishikawa (East) Dayroosh Sami (West) Rosina Franco (ISIC)
213/202-7584 213/202-7577 213/202-7587
213/580-6559
THE CENTER FOR ORAL HEALTH
89
Appendix A3: Memorandum of Understanding (MOU) Template & Sample
MOU Template Agency
Organization Name/Title City, State, and Zip Code
MEMORANDUM of UNDERSTANDING
BETWEEN THE AGENCY AND SERVICE PROVIDER
SUBJECT: Format and Use of a Memorandum of Understanding 1. Purpose. This paragraph defines, in as few words as possible, the purpose of the memorandum of understanding and outlines the terms of the contract. 2. Reference. This paragraph will list the references that are directly related to the MOU. 3. Problem. Present a clear, concise statement of the problem, to include a brief background. 4. Scope. Add a succinct statement specifying the area of the MOU. 5. Understandings, agreements, support and resource needs. List the understandings, agreements, support and resource needs, and responsibilities of and between each of the parties or agencies involved in the MOU. 6. Specify a certain contracting period. (Example: The ending date of an MOU cannot exceed the end of the current fiscal year). 7. Specify monetary and performance terms. Explain payment rates with all rates agreed to by both parties. Designate specific time frames and dollar amounts to be paid upon completion of each identifiable task. 8. Include a monitoring component to determine contract compliance. If the terms of the MOU are not being fulfilled, allow for a termination clause. 9. Effective date. Enter the date the agreement will become effective.
SIGNATURE BLOCK XXXXXXXX, XXXX XXXXXXX, XXXXXX
SIGNATURE BLOCK XXXXXXXX, XXXX XXXXXXX, XXXXXX
(Date) (Date)

The Center For Oral Health SBOHC Operations Manual
SBOHC MOU Sample (University & Public Elementary)
AFFILIATION AGREEMENT BETWEEN SBOHC Name AND School Name
THIS AGREEMENT is entered into by and between SBOHC Name and School Name, hereinafter
referred to as “SBOHC Name,” and, hereinafter referred to as the “Facility.”
In consideration of the mutual agreements set forth herein, SBOHC Name and the Facility enter into this agreement on the terms and conditions set forth below.
SBOHC Name agrees to: 1. Appoint a faculty member as the Assistant Dean for Clinical Rotations to administer SBOHC’s Name responsibilities related to the clinical education program. 2. Assume responsibility for assuring compliance with the Evaluative Criteria for Accreditation of Education Programs for the Preparation of Doctors of Dental Medicine established by the Commission on Dental Accreditation (CODA). 3. Refer to the Facility only those students who have satisfactorily completed the prerequisite didactic portion of the curriculum. 4. Establish and maintain ongoing communication with the Clinical Education Coordinator (CEC) of the Facility on items pertinent to Dental Education. On-‐site visits will be arranged when appropriate and/or upon request by the Facility. 5. Inform the students of the Facility’s requirements for acceptance and direct the student to comply with the existing rules and regulations of the Facility. 6. Require student’s proof of health insurance coverage at the time of registration at SBOHC Name. 7. Provide students with accident insurance coverage that will cover up to $25,000 for injuries or accidents sustained by any of its students (subject to applicable limitations and exclusions contained in the statement of insurance) while participating in a supervised clinical education program in the United States. 8. Require all students to show proof of current immunization for tetanus, diphtheria, hepatitis B, measles, mumps, rubella, and varicella, and to have had a recent skin test for tuberculosis. 9. Maintain professional liability coverage in full force and effect for students during their clinical experience in the amount of $5,000,000 per occurrence/$5,000,000 aggregate. If this insurance coverage is not maintained by SBOHC Name, then SBOHC Name agrees to hold the Facility, its officers, employees, and authorized agents harmless against any and all liability and expenses that may be imposed by law against the Facility, its officers, employees, and authorized agents as a result of the negligent or wrongful acts or omissions of the students while they are in their clinical education experience at the Facility. 10. Prohibit the publication by the students, faculty or staff members of any material relative to their clinical education experience that has not been reviewed by the Facility and SBOHC Name, in order to assure that infringement of patient’s rights to privacy is avoided. Any article written by a student that has been based on information acquired through his/her clinical education experience must clearly reflect that SBOHC Name or Facility does not endorse the article, even where a review has been made prior to publication. This is accomplished by requiring the following disclaimer to appear with each such article written: “The opinion and conclusions presented herein are those of the author and do not necessarily represent the views of SBOHC Name or Facility.”
The Facility agrees to: 1. Designate a medical staff member as Clinical Education Coordinator (CEC) acceptable to SBOHC Name, who will be responsible for the supervision of the students and the planning and implementation of the clinical experience. The aforementioned individual shall meet the guidelines and/or criteria established by the CDM for the supervision of students in the clinical education setting.

THE CENTER FOR ORAL HEALTH
91
2. Require a student to render only those services that are within the student’s educational preparation and qualifications, and that are related to the objectives of the clinical education program. Provide the type and amount of supervision in proportion to the student’s level of competence. 3. Make access to emergency health care available to the student in case of accident or illness while at the Facility with the Facility not being responsible for any costs involved. 4. Advise SBOHC Name of any changes in its personnel, operation, or policies, which may affect the clinical experience. 5. Permit, upon reasonable request, the inspection of the clinical facilities, the services available for the clinical experience, student records, and other such items pertaining to the clinical education program by SBOHC Name and/or agencies charged with the responsibility for accreditation of the program. 6. Provide the student with a copy of the Facility’s existing rules, regulations, policies, and procedures with which the student is expected to comply. 7. Make available the physical facilities and equipment necessary to conduct the clinical experience and, Whenever possible, the use of library facilities, reference materials, reasonable study and storage space, and any other specialized learning materials. 8. Evaluate the performance of the student on a regular basis using the evaluation form supplied by SBOHC Name. The completed final evaluation shall be forwarded to SBOHC Name within ten (10) working days following the conclusion of the student’s clinical experience. 9. Advise SBOHC Name of any serious deficiency noted in the ability of the student to progress toward achievement of the stated objectives of the clinical experience. In the case of any such deficiency, the student, the Assistant Dean for Clinical Rotations, and Clinical Preceptor/Clinical Education Coordinator shall have the mutual responsibility to devise a plan by which the student may be assisted to achieve the stated objectives. 10. Comply with all federal, state, and local laws and ordinances concerning the confidentiality of student records and concerning human subject research, if students participate in such a research program. 11. Maintain professional liability coverage in full force and effect for the Facility, its officers, employees and authorized agents, while students are at the facility in the amount of $1,000,000 per Occurrence/$3,000,000 aggregate. If this insurance coverage is not maintained by the Facility, then the Facility agrees to hold SBOHC Name, its students, officers, employees, and authorized agents harmless against any and all liability and expenses that may be imposed by law against SBOHC Name, its students, officers, employees, and authorized agents, as a result of the negligent or wrongful acts or omissions of the Facility, its officers, employees and authorized agents.
Rights/Responsibilities of the Student SBOHC Name will notify each student that he or she is required to: 1. Provide prior to the commencement of the clinical experience such information as may be required by the Facility for the clinical education and guidance of the student, together with the student’s authorization for release of such information as permitted by law. 2. Abide by existing rules, regulations, policies, and procedures of the Facility and SBOHC Name. 3. Observe and respect all patient’s rights, confidences, and dignity. 4. Notify SBOHC Name and the Facility immediately whenever absence from the Facility becomes necessary. 5. Provide evidence of current health insurance coverage as may be requested by SBOHC Name and/or Facility. 6. Dress in appropriate clinical attire as established by SBOHC Name, and to secure transportation and living accommodations as necessary, to participate in the clinical experience.
SBOHC Name and the Facility mutually agree to: 1. Pursue the educational objectives for the clinical experience, devise methods for their attainment, and continually evaluate the effectiveness of the clinical experience in meeting the objectives. 2. Make no distinction among students covered by this Agreement on the basis of race, religion, sex,

The Center For Oral Health SBOHC Operations Manual
sexual orientation, creed, age, handicap, or national origin. For the purpose of this Agreement, distinctions on the grounds of race, religion, sex, sexual orientation, creed, age, handicap, or national origin include, but are not limited to the following: denying a student any available service or benefit of a facility; providing any service or benefit to a student which is different or is provided in a different manner or at a different time from that provided to other students under this Agreement; subjecting a student to segregation or separate treatment in any matter related to receipt of any advantage or privilege accorded to others receiving any service or benefits; treating a student or potential student differently from others in determining whether he/she satisfies any admission, enrollment, quota, eligibility, membership or any other requirement or condition which individuals must meet in order to be provided any service or benefit. 3. Acknowledge that the students of SBOHC Name are fulfilling specific requirements for clinical experience as part of a degree or certificate requirement, and therefore, the students of SBOHC Name are not to be considered employees of either SBOHC Name or the Facility, regardless of the nature or extent of the acts performed by them, for purposes of Worker’s Compensation, employee benefit programs, or any other purpose. 4. Withdraw from the clinical education program any student whose performance is unsatisfactory, whose performance presents a threat to patients or others, whose personal characteristics prevent desirable relationships within the Facility, or whose health status is a detriment to the student’s successful completion of the clinical education program. The Facility shall have the right to recommend that SBOHC Name make a withdrawal, provided such a request is in writing and includes a statement of the reason why the Facility recommends that the student be withdrawn. SBOHC Name may withdraw a student from the clinical program at any time, upon written notice to the Facility. 5. Determine the number of students able to participate in the Facility’s clinical education program, and the period of time for each student’s clinical experience. The planned schedule of student assignment will be made at least one month prior to the commencement of the student’s clinical experience, and may be altered by mutual agreement with due consideration given to both parties.
Terms of Agreement 1. This Agreement shall commence on the signature date by the Facility and shall remain effective for a term of three years upon execution by both parties. This Agreement will be automatically renewed at the term end after appropriate review by both parties, unless otherwise indicated in writing by one of the parties at least ninety (90) days prior to the end of the term. 2. It is understood and agreed that the parties to this Agreement may revise or modify this Agreement by written amendment when both parties agree to such amendment. 3. If either party wishes to terminate this Agreement prior to the end of its normal term, ninety (90) days written notice shall be given to the other party. However, any such termination by the Facility shall not be effective as to any student who was participating in program until such student has completed the clinical experience. 4. This Agreement shall be subject to and governed by the laws of the State of California. 5. Other considerations or additional considerations:

THE CENTER FOR ORAL HEALTH
93
FOR SBOHC Name: FOR THE FACILITY: School Full Name School Address
SIGNATURE BLOCK XXXXXXXX, XXXX XXXXXXX, XXXXXX
SIGNATURE BLOCK XXXXXXXX, XXXX XXXXXXX, XXXXXX
(Date) (Date)

The Center For Oral Health SBOHC Operations Manual
Appendix A4: LAUSD-‐ Murchison Elementary School Setting Up Facility Checklist
Setting Up Facility Checklist Should Include the Following Categories:
• School Name • Location • Miles From Primary Practice • Number of Students Enrolled • Percentage of Students with “Free and Reduced Meals” • School District Organization Chart • School District Directory • Completed MOU
Example:
School Name Location
Miles From Primary Practice
Number of Students Enrolled
Percentage of Students w/ "Free and Reduced Meal"
School District Org Chart
School District Directory MOU
1. Murchison Elementary
1501 Murchison Street Los Angeles, CA 90033 5 Miles 559 92.50% Yes Yes Complete
2.
3.
4.
5.
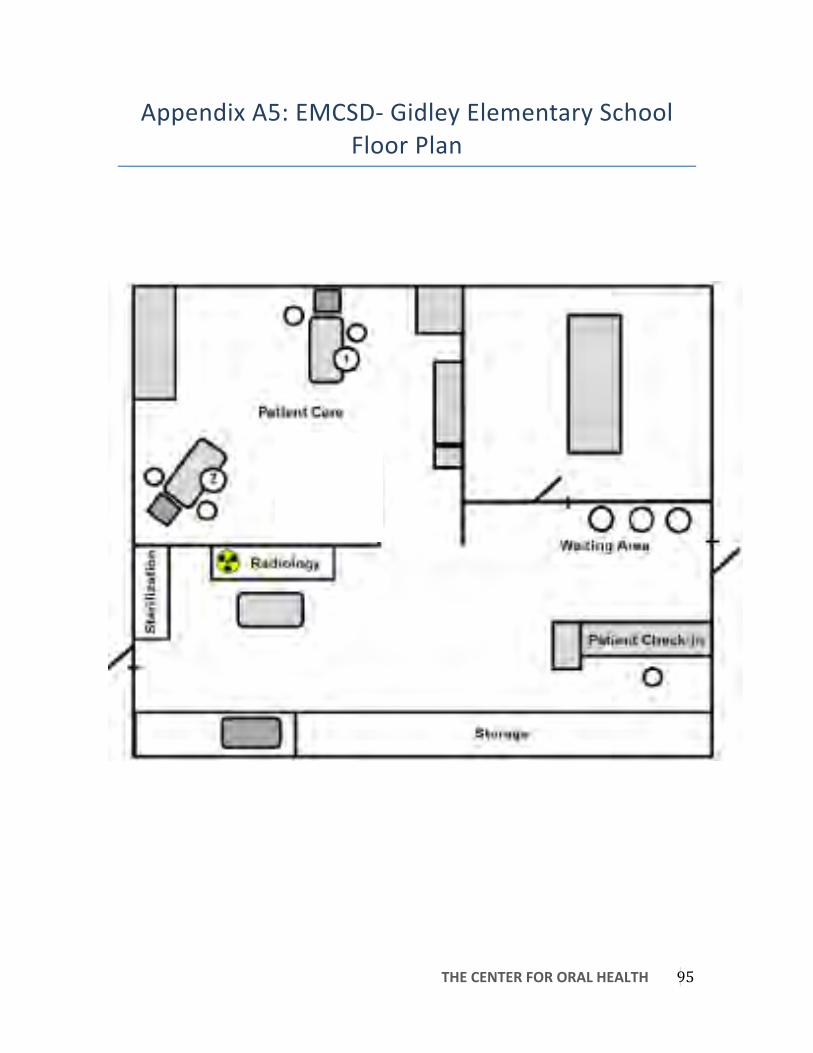
THE CENTER FOR ORAL HEALTH
95
Appendix A5: EMCSD-‐ Gidley Elementary School Floor Plan

The Center For Oral Health SBOHC Operations Manual
Appendix A6: LAUSD-‐ Murchison Street Elementary School Capacity and Costs Table
Capacity & Costs Table
Size 2-‐Chair Patients Treated/Year 224 Visits/Year (DDS) 32
Start-‐Up Costs Equipment 81,042 Liability Insurance 620 Scanner & Laptops-‐ Three 2,100 Printed Material 500 Office Supplies 1,000
Annual Fixed Costs Dental Director 16,000 Registered Dental Assistant 6,656 Site Coordinator 6,656 Travel 200 Telephone + Hotspot Connection 800
Variable Costs Anticipated Total Variable Expense (Patient Costs*Expense) 5,376
Total Start-‐Up Costs 84,762
Total Annual Operating Costs 35,688
Total First-‐Year Costs 120,450

THE CENTER FOR ORAL HEALTH
97
The Appendix A7: LAUSD-‐ Murchison Street Elementary School Equipment Price List
Supp
lies(&
(Equip
ment
Quan
tity
Price
(To
tal(Pr
iceQu
antity
Price
(To
tal(Pr
iceQu
antity
Price
(To
tal(Pr
iceQu
antity
Price
(To
tal(Pr
iceInf
ectio
n(Con
trol
Resto
rative
Endo
dontic
Antim
icrob
ial,Hand,S
oaps
2$5.00
$10.00
#2,Slow
,Speed,L
atch,Bur
3$15.00
$45.00
Glum
a2
$79.99
$159.98
Endo
,Files
1$12.79
$12.79
Bib,E
Z2
$10.76
$21.52
#4,Slow
,Speed,L
atch,Bur
3$15.00
$45.00
Hand
,Mirror
4$14.29
$57.16
Endo
,Ice
3$23.19
$69.57
Bioh
azard,B
ags
2$35.00
$70.00
1,Rou
nd,Bur
10$14.00
$140.00
Hand
piece,L
ubricant
1$42.29
$42.29
Surgi
cal
Cavi,Wipes
5$9.56
$47.80
1/2,R
ound
,Bur
5$120.00
$600.00
Hatche
t10
$23.00
$230.00
#79,R
oot,T
ip,Elevator
2$45.00
$90.00
Chair
,Covers
1$22.63
$22.63
2,Rou
nd,Bur
1$120.00
$120.00
Helioseal,Seala
nt8
$79.99
$639.92
#80,R
oot,T
ip,Elevator
2$45.00
$90.00
Cotto
n,Roll,D
ispen
ser
2$20.00
$40.00
245,B
ur1
$120.00
$120.00
Hemostatic,Gel
3$21.83
$65.49
#9,Pe
rioste
al,Ele
vator
2$35.00
$70.00
Cotto
n,Rolls
1$20.93
$20.93
3,Rou
nd,Bur
1$120.00
$120.00
Hollenb
eck
10$21.00
$210.00
150,A
dult,Forcep
s2
$168.00
$336.00
Cotto
n,Tip,App
icators
1$23.30
$23.30
3.0,C
hrom
ic,Gu
t,Sutures
2$41.99
$83.98
Individ
ual,Com
posite,R
efill,(A1)
3$52.70
$158.10
150,P
edo,Forcep
s2
$158.00
$316.00
Disposable,De
ntal,Mirrors
2$31.59
$63.18
330,B
ur1
$120.00
$120.00
Individ
ual,Com
posite,R
efill,(A2)
3$52.70
$158.10
151,P
edo,Forcep
s2
$158.00
$316.00
Dri,A
ngles
,(Lg,P
lain)
1$10.26
$10.26
7406,Bur
10$20.00
$200.00
Individ
ual,Com
posite,R
efill,(A3)
3$52.70
$158.10
301,S
traigh
t,Elev
ator,(Sm)
2$45.00
$90.00
Earlo
op,Pr
oced
ure,M
asks
10$13.00
$130.00
A2,Sy
ringe
4$54.05
$216.20
Instr
umen
t,Wire
,Brushes
2$13.00
$26.00
304,M
edium,St
raigh
t,Elev
ator
2$45.00
$90.00
Empo
wer,E
nzym
atic,De
tergen
t1
$28.76
$28.76
Acorn,B
urnisher
10$23.93
$239.30
IRM
1$59.25
$59.25
Bone
,Files
2$128.00
$256.00
Gloves
5$20.00
$100.00
Air/W
ater,Sy
ringe,Tips,(C
rysta
l,Tips)
2$45.00
$90.00
Ketac,C
emen
t2
$84.55
$169.10
Curre
ttes
2$17.00
$34.00
Gown
,(Med
)8
$15.00
$120.00
Alcoho
l,Prep,P
ads
1$9.00
$9.00
Kids,P
rotective
,Eyew
ear
2$19.29
$38.58
East,Ele
vators
2$54.00
$108.00
Gown
,(Small)
8$15.00
$120.00
Amalg
am,Carrie
r4
$35.00
$140.00
Lab,P
umice
1$15.43
$15.43
Need
le,Ho
lders
2$14.00
$28.00
Guaze,(
2x2),(2
00ct)
2$1.19
$2.38
Amalg
am,Plug
15$21.00
$315.00
Lidocain
e22
$25.00
$550.00
Perio
tome
1$63.00
$63.00
Hand
,Sanitizer
2$7.89
$15.78
Amalg
am,W
ell5
$25.64
$128.20
LimeLite
4$36.79
$147.16
Root,Tip,E
levators
2$50.00
$100.00
High,Sp
eed,E
vac
1$52.53
$52.53
Amalg
amator
1$337.00
$337.00
Lolicain
e,Top
ical
16$46.54
$744.64
Sal,Jet
2$12.59
$25.18
Mon
ojet,Sy
ringes
1$20.93
$20.93
Articulating,P
aper
3$8.79
$26.37
Maxilla
ry,Anterior,K
it,of,St
ainles
s,Steel,Crown
s1
$333.43
$333.43
Sodium
,Chloride
1$5.00
$5.00
Need
le,Protectors
2$11.84
$23.68
Aspiratin
g,Syringes
7$29.00
$203.00
Micro,Brush
3$25.00
$75.00
Surgica
l,Scis
sors
1$60.00
$60.00
Need
les,(2
7,gauge,long)
2$8.72
$17.44
Aspiratin
g,Syringes,(Pe
tite)
3$31.00
$93.00
Mixing,Pa
ds2
$13.59
$27.18
Suture,Sc
issors
2$50.00
$100.00
Need
les,(3
0,gauge,x_short)
2$8.72
$17.44
Ball,B
urnisher,(Lg)
10$20.00
$200.00
Mixing,W
ell1
$27.00
$27.00
West,E
levators
2$54.00
$108.00
Pedo
,Tooth,B
urshes
1$20.00
$20.00
Ball,B
urnisher,(Sm)
10$25.00
$250.00
Molt,M
outh,Pr
op3
$71.19
$213.57
Radio
logy
Saliva,E
jectors
2$3.00
$6.00
Basic
,Cassette
8$65.00
$520.00
Mou
th,M
irror,En
ds20
$5.00
$100.00
#1,Se
nsor,Sleeves
1$30.00
$30.00
Sani,To
wel,(Bib)
2$30.00
$60.00
Basic
,Cassette
s,(Re
d)10
$66.00
$660.00
Mou
th,M
irror,Handles
20$10.00
$200.00
#1,Se
nsors
1$7,000.00
$7,000.00
Sharps,Con
tainers,(Lg)
1$10.26
$10.26
Bite,Blocks,(Ad
ult)
2$13.59
$27.18
MW,Con
tra,Angle,Sheath
4$359.99
$1,439.96
#2,Se
nsor,Sleeves
1$12.79
$12.79
Sharps,Con
tainers,(Sm
)4
$8.52
$34.08
Bite,Blocks,(Ch
ild)
4$34.79
$139.16
MW,PB
,Con
tra,Angle,He
ad,LA
TCH
3$263.19
$789.57
Adult,Lead,A
pron
1$65.59
$65.59
Steriliz
ation,B
ags,(3.5x5.25
)1
$13.00
$13.00
Bulk,Co
mpo
site,S
yringers,(A1)
2$54.05
$108.10
MW,Rhino
,XP,Slow
,Speed,M
otor
4$1,014.99
$4,059.96
Breif
,Case,f
or,Se
nsors
1$70.00
$70.00
Steriliz
ation,B
ags,(7.5x13
)3
$15.00
$45.00
Bulk,Co
mpo
site,S
yringers,(A3.5)
2$54.05
$108.10
MW,Slow
,Speed,H
ead,F
G4
$300.00
$1,200.00
Child,Le
ad,Fr
ee,Apron
1$150.00
$150.00
Steriliz
ation,B
ags,(9x14
.5)
1$20.00
$20.00
Bulk,Co
mpo
site,S
yringers,(A3)
2$54.05
$108.10
MW,St
raigh
t,Atttachm
ent
4$425.99
$1,703.96
Curin
g,Ligh
t2
$400.00
$800.00
Succtio
n,Steriliza
tion,G
allon
,Buckets
1$6.43
$6.43
Bulk,Co
mpo
site,S
yringers,(A4)
2$54.05
$108.10
MW,Tr
adition
al,No
n,Fiber,Optic,
Highpe
ed,Handp
iece
4$509.99
$2,039.96
Insta
dose,Badges
1$90.00
$90.00
Surgica
l,Aspira
tor,T
ips
2$9.39
$18.78
Bur,B
lock,12
,Hole
6$28.00
$168.00
Myla
r,Strips
5$7.19
$35.95
Midwe
st,Ha
ndpiece,A
irstatio
ns1
$350.00
$350.00
Syrin
ge,Sleeves
1$17.37
$17.37
Carie
s,Ind
icator
4$23.83
$95.32
Optib
ond,S
olo,Plu
s2
$202.00
$404.00
Nomad
1$7,000.00
$7,000.00
VacuKle
en2
$52.79
$105.58
Cavit
y,Con
ditio
ner
1$47.99
$47.99
Perio
,Prob
e10
$13.00
$130.00
Nomad,Case
1$200.00
$200.00
Vasoline
1$17.00
$17.00
Compo
site,G
un1
$62.00
$62.00
Plastic,C
ompo
site,Instru
men
t10
$20.00
$200.00
Planm
eca,S
ensor,A
daptor
1$50.00
$50.00
Zymex,En
zymatic,Cleane
r1
$45.02
$45.02
Compo
site,P
olish
,Latch,B
ur,Con
e2
$67.00
$134.00
Polishing,Disc
s,(Assorte
d)1
$81.59
$81.59
Radiology,S
ensor,B
riefca
ses
1$150.00
$150.00
Preven
tative
(Hygie
neCo
mpo
site,P
olish
,Latch,B
ur,Cup
2$67.00
$134.00
Resto
rativ
e,Cassette
s,(Green)
10$86.00
$860.00
RINN
,EZ,Ta
bs1
$40.00
$40.00
11/12,S
caler
6$12.87
$77.22
Compo
site,W
ettin
g,Resin
2$50.00
$100.00
Rubb
er,Dam
8$14.00
$112.00
Equip
ment
13/14,S
caler
6$12.87
$77.22
Contou
ring,P
lyers
1$127.99
$127.99
Rubb
er,Dam
,Clam
p,Kit
1$67.00
$67.00
3,Drawe
r,White,St
orage,B
in1
$20.00
$20.00
3/4,S
caler
6$30.00
$180.00
Cotto
n,Pliers
10$23.00
$230.00
Rubb
er,Dam
,Clam
p,Pun
cher
2$67.00
$134.00
Air,C
ompressors
1$1,500.00
$1,500.00
5/6,S
caler
6$30.00
$180.00
Crim
ping,Plyers
1$127.99
$127.99
Rubb
er,Dam
,Fram
e3
$15.00
$45.00
Asep
tico,Hy
giene
,Chair
1$3,000.00
$3,000.00
7/8,S
caler
6$12.87
$77.22
Discoid_Cleo
id10
$20.00
$200.00
Rubb
er,Dam
,Retain
er,Fo
rcep
3$35.00
$105.00
Assistant,Chair
1$200.00
$200.00
Chlorhexidine
2$5.99
$11.98
Dispen
sing,t
ips,(Black)
4$21.00
$84.00
Seal,n,S
hine
1$48.79
$48.79
BioSon
ic,Ultra
sonic,M
achine
1$1,000.00
$1,000.00
Electric,Pu
lp,Te
ster
1$189.00
$189.00
Dispen
sing,t
ips,(Blue
)4
$21.00
$84.00
Septocain
e2
$47.49
$94.98
Chair
,Lights
3$50.00
$150.00
ESA,Extend
ed,Pr
ophy,Angles
2$55.99
$111.98
Durelon
1$62.00
$62.00
Set_U
p,Tray
5$8.79
$43.95
Med
ical,Emergency,K
it1
$94.00
$94.00
Floss,Th
readers
2$25.19
$50.38
Dycal,Refill
1$241.13
$241.13
Sharpe
ning,St
ones
4$21.00
$84.00
Midmark,S
terilize
r1
$5,000.00
$5,000.00
GUM,Disc
losin
g,Tablet
s2
$14.79
$29.58
Etchant
1$25.00
$25.00
Spoo
n,Excavator
10$21.00
$210.00
Patie
nt,Chair
2$200.00
$400.00
H6/H7,S
caler
6$30.00
$180.00
Explorers
10$14.70
$147.00
Stain
less,S
teel,Crow
ns,Pa
ck1
$204.00
$204.00
Plastic,H
olde
rs2
$10.00
$20.00
Hygie
ne,Cassette
s,(orange)
6$105.99
$635.94
Feric,Su
lfate,Hem
ostatic,Agent
2$14.39
$28.78
T_Ba
nd,(Lg,C
urved)
5$4.99
$24.95
ProC
art,3
2$7,000.00
$14,000.00
Midwe
st,RD
H,Freedo
m,Cordless,
Prop
hy,Sy
stem
1$1,325.00
$1,325.00
FG,1/
4,Rou
nd3
$114.39
$343.17
T_Ba
nd,(Lg,S
traigh
t)5
$4.99
$24.95
Refrigerator
1$200.00
$200.00
Plaqu
e,Disc
losin
g,Solution
1$7.99
$7.99
FG,Diam
ond,C
ourse
,Rou
nded
4$31.19
$124.76
Tofflem
yer,B
and,#
1,(0.00
15)
2$3.81
$7.62
Toy,C
hest,(Disp
osable,Bo
x)1
$50.00
$50.00
Prop
hy,Pa
ste4
$23.19
$92.76
FG,Diam
ond,Inverted,C
one
3$31.19
$93.57
Tofflem
yer,B
and,#
1,(0.00
2)5
$1.83
$9.15
White,3,Draw
er,St
orage,C
ontainer
1$10.00
$10.00
Pulp,Te
ster,W
ire1
$36.00
$36.00
FG,Diam
ond,M
edium,Rou
nded
3$22.23
$66.69
Tofflem
yer,B
and,#
13,(0
.001
5)5
$1.83
$9.15
Toothp
aste
10$24.00
$240.00
FG,Diam
ond,S
uper,Fine
,Needle
4$31.19
$124.76
Tofflem
yer,B
and,#
2,(0.00
15)
2$3.81
$7.62
Tray,Covers
1$15.00
$15.00
FG,Flam
e,Shape
5$39.99
$199.95
Tofflem
yer,B
and,H
olde
rs4
$10.00
$40.00
Ultra
sonic,S
caler
,Tips
5$183.00
$915.00
FG,M
andrel
2$15.03
$30.06
Tofflem
yer,R
etain
er10
$10.79
$107.90
Ultra
sonic,S
caler
s3
$395.00
$1,185.00
Finish
ing,S
trips
1$12.89
$12.89
Triple,Trays
1$37.00
$37.00
Unive
rsal,Scaler
,H5/33
6$32.32
$193.92
Flowa
ble,C
ompo
site,(
A1)
3$32.79
$98.37
Vitre
bond
1$200.12
$200.12
Varnish
1$165.00
$165.00
Flowa
ble,C
ompo
site,(
A2)
3$32.79
$98.37
White,Po
lishing,St
one,B
urs
2$20.00
$40.00
Wild,Floss
1$36.33
$36.33
Form
ocresol
1$91.99
$91.99
Woo
d,Wed
ge,(Sm)
3$32.79
$98.37
Fuji,A
pplicator
5$82.00
$410.00
ZOE
2$75.19
$150.38
Fuji,II
2$163.19
$326.38
Fuji,IX
2$207.99
$415.98
Total
$81,0
41.81
The Center For Oral Health SBOHC Operations Manual
Daily Operations Appendix B1-‐B14

THE CENTER FOR ORAL HEALTH
99
Appendix B1: Sample Teacher Cover Letter
The Center For Oral Health SBOHC Operations Manual
Appendix B2: Sample Parent/Guardian Consent Form
(English & Spanish)

THE CENTER FOR ORAL HEALTH
101

The Center For Oral Health SBOHC Operations Manual
Appendix B3: Sample Patient Registration Form

THE CENTER FOR ORAL HEALTH
103
Appendix B4: Sample New Parent Consent to Use and Disclosure of Health Information For
Treatment, Payment, or Healthcare Operations
The Center For Oral Health SBOHC Operations Manual
Appendix B5: Permission to Share Information Form

THE CENTER FOR ORAL HEALTH
105
Appendix B6: Informed Consent Form

The Center For Oral Health SBOHC Operations Manual
Appendix B7: Basic Surgical Treatment Consent Form

THE CENTER FOR ORAL HEALTH
107

The Center For Oral Health SBOHC Operations Manual
Appendix B8: Confidential Medical & Dental History For a Minor Patient
THE CENTER FOR ORAL HEALTH
109

The Center For Oral Health SBOHC Operations Manual
Appendix B9: Confidential Medical & Dental History For An Adult

THE CENTER FOR ORAL HEALTH
111

The Center For Oral Health SBOHC Operations Manual
Appendix B10: Dental Examination Worksheet

THE CENTER FOR ORAL HEALTH
113
Appendix B11: Periodontal Charting

The Center For Oral Health SBOHC Operations Manual
Appendix B12: Patient X-‐ray Summary

THE CENTER FOR ORAL HEALTH
115
Appendix B13: Image Release Form
The Center For Oral Health SBOHC Operations Manual
Appendix B14: School Absence Release

THE CENTER FOR ORAL HEALTH
117
Finance Policies Appendix C1-‐C5

The Center For Oral Health SBOHC Operations Manual
Appendix C1: Sample Reimbursement Free Schedule-‐ LAUSD Murchison Street Elementary
Denti-‐Cal
Private Insurance Average
Periodic Dental Examination $15.00 $50.00 Limited Oral Evaluation (Problem Focused) $35.00 $76.00 Oral Evaluation for Patient Under Three Years of Age Global $70.00 Comprehensive Oral Evaluation $25.00 $90.00 Re-‐evaluation-‐Limited, problem Focused (Established Patient) $75.00 $72.00 Comprehensive Periodontal Evaluation (New or Established Patient) Global $96.00
Intraoral Radiographs (Complete Series) $40.00 $132.00 Intraoral Radiograph (Periapical first Image) $10.00 $29.00 Intraoral Radiograph (Periapical Additional Image) $3.00 $25.00 Intraoral Radiograph (Occlusal Image) $10.00 $42.00 Bitewing (Single Images) $5.00 $29.00 Bitewing (Two Images) $10.00 $46.00 Bitewing (Three Images) Global $57.00 Bitewing (Four Images) $18.00 $50.00 Oral/Facial Photograhic Image Obtained Intraorally or Extraorally $6.00 $- Collected & Prep of Saliva Sample for Lab Diagnostic Test Not a
Benefit $- Caries Risk Assessment & Documentation (Low Risk) $-‐ $- Caries Risk Assessment & Documentation (Moderate Risk) $-‐ $- Caries Risk Assessment & Documentation (High Risk) $-‐ $- Adult Prophylaxis (Once/6 Months) $40.00 $92.00 Child Prophylaxis (Once/6 Months If Calculus Is Present) $30.00 $68.00 Topical Fluoride Varnish 0-‐5 $18.00 $45.00 Topical Fluoride Varnish 6-‐20 $8.00 $45.00 Topical Application of Fluoride 0-‐5 $18.00 $38.00 Topical Application of Fluoride 6-‐20 $8.00 $38.00 Sealant $22.00 $55.00 Preventive Resin Restoration in a Moderate to High Caries Risk Patient $22.00 $55.00 Amalgam-‐ One Surface, Primary or Permanent $39.00 $121.00

THE CENTER FOR ORAL HEALTH
119
Amalgam-‐ Two Surface, Primary or Permanent $48.00 $180.00 Amalgam-‐ Three Surface, Primary or Permanent $57.00 $219.00 Resin-‐Based Composite-‐ One Surface, Anterior $55.00 $163.00 Resin-‐ Based Composite-‐ Two Surfaces, Anterior $60.00 $204.00 Resin-‐Based Composite-‐ Three Surfaces, Anterior $65.00 $252.00 Resin-‐Based Composite (One Surface, Posterior) $39.00 $181.00 Resin-‐Based Composite (Two Surfaces, Posterior) $48.00 $235.00 Resin-‐Based Composite (Three Surfaces, Posterior) $57.00 $290.00 Prefabricated Stainless Steel Crown (Primary Tooth) $75.00 $275.00 Protective Restoration to protexct tooth or relieve plain $45.00 $124.00 Therapeutic pulpotomy or pulpectomy (Primary Teeth Only) $71.00 $202.00 Periodontal Scaling and Root Planing (4+ Teeth Per Quardrant) $50.00 $260.00 Extraction, Coronal Remnants (Deciduous Tooth) $41.00 $136.00 Extraction, Eruption tooth or Exposed Root (Elevation and/or Forceps Removal) $41.00 $175.00 Surgical Removal of Residual Tooth Root (Cutting Procedure $100.00 $309.00
Inhalation of Nitrous Oxide/Analgesia (Anxiolysis) $25.00 $42.00 Occlusal Adjustments $25.00 $173.00
The Center For Oral Health SBOHC Operations Manual
Appendix C2: Sample Claim Inquiry Form

THE CENTER FOR ORAL HEALTH
121
Appendix C3: 2-‐Year Break-‐Even Analysis
BREA
KEVE
N ANA
LYSIS B
ASED
ON DE
NTI-C
AL RE
IMBUR
SEMEN
TYea
r%One
Year%T
wo
AMOU
NTS%S
HOWN
%IN%U.
S.%DOL
LARS
PATIE
NTS
PATIE
NTS
Patie
nts%Pe
r%Day
14%%%%%
%%%%%%%%%%
%%%%%%%%%%
Patie
nts%Pe
r%Day
14%%%%%
%%%%%%%%%%
%%%%%%%%%%
Uniqu
e%Child
%Patie
nts%Pe
r%Year
224
%%%%%%%%%%
%%%%%%%%%%
%%Un
ique%C
hild%Pa
tients
%Per%Y
ear22
4%%%%%
%%%%%%%%%%
%%%%%%%
DAILY
+VAR
IABLE+C
OSTS
DAILY
+VAR
IABLE+C
OSTS
Avera
ge%Va
riable
%Expe
nse%Pe
r%Pati
ent%
$12.0
0Av
erage%
Varia
ble%Ex
pense
%Per%P
atien
t%$1
2.00
TOTA
L+DAILY+VAR
IABLE+C
OSTS
$168
.00
TOTA
L+DAILY+VAR
IABLE+C
OSTS
$168
.00
TOTA
L+VAR
IABLE+C
OSTS+PE
R+YEAR
$5,37
6.00
TOTA
L+VAR
IABLE+C
OSTS+PE
R+YEAR
$5,37
6.00
DAILY
+FIXE
D+CO
STS
DAILY
+FIXE
D+CO
STS
1%Den
tal%Di
rector
$500
.001%D
ental
%Direc
tor$5
00.00
1%RDA
$208
.001%R
DA$2
08.00
1%Site
%Coord
inator
$208
.001%S
ite%Co
ordina
tor$2
08.00
Travel
$6.25
Travel
$6.25
Telep
hone
%+%Hots
pot
$25.0
0Tel
epho
ne%+%H
otspo
t$2
5.00
TOTA
L+DAILY+FIXE
D+CO
STS
$947
.25
TOTA
L+DAILY+FIXE
D+CO
STS
$947
.25
TOTA
L+DAILY+CO
STS+P
ER+YE
AR$3
0,312
.00
TOTA
L+DAILY+CO
STS+P
ER+YE
AR$3
0,312
.00
REVE
NUE
REVE
NUE
Reven
ue%An
ticipated
S%Pati
ent%P
er%Yea
r%(Den
tiSCal)
$244
.00Re
venue
%Antici
pated
S%Pati
ent%P
er%Yea
r%(Den
tiSCal)
$244
.00Re
venue
%Antici
pated
S%Pati
ent%P
er%Yea
r%(Priv
ate%Insur
ance)
$678
.00Re
venue
%Antici
pated
S%Pati
ent%P
er%Yea
r%(Priv
ate%Insur
ance)
$678
.00Re
venue
%Antici
pated
S%Pati
ent%P
er%Yea
r%(No%Insu
rance)
$0.00
Reven
ue%An
ticipated
S%Pati
ent%P
er%Yea
r%(No%Insu
rance)
$0.00
TOTA
L+REV
ENUE
+ANT
ICIPAT
EDA+P
ER+YE
AR+(7
0%+Den
tiACa
l+&+15
%+Priva
te+In
surance+&
+15%+No
+insurance)
$61,0
40.00
TOTA
L+REV
ENUE
+ANT
ICIPAT
EDA+P
ER+YE
AR+(7
0%+Den
tiACa
l+&+15
%+Priva
te+In
surance+&
+15%+No
+insurance)
$61,0
40.00
EXPE
NSES
EXPE
NSES
TOTA
L+DAILY+CO
STS
$1,11
5.25
TOTA
L+DAILY+CO
STS
$1,11
5.25
TOTA
L+DAILY+CO
STS+P
ER+PA
TIENT
$79.66
TOTA
L+DAILY+CO
STS+P
ER+PA
TIENT
$79.66
STAR
TAUP
+COSTS
$85,7
56.00
STAR
TAUP
+COSTS
$0.00
TOTA
L+YEA
RLY+E
XPEN
SES+P
ER+YE
AR$1
21,44
4.00
TOTA
L+YEA
RLY+E
XPEN
SES+P
ER+YE
AR$3
5,688
.00
RESU
LTS
RESU
LTS
BREA
KEVE
N+PO
INT+P
ER+PA
TIENT
$79.66
BREA
KEVE
N+PO
INT+P
ER+PA
TIENT
$79.66
REIM
BURS
EMEN
T+CRITIC
AL+M
ASS+(70
%+De
ntiAC
al+&+15
%+Priva
te+In
surance+&
+15%+No
+insurance)
199%
REIM
BURS
EMEN
T+CRITIC
AL+M
ASS+(70
%+De
ntiAC
al+&+15
%+Priva
te+In
surance+&
+15%+No
+insurance)
58%
ANITI
CIPA
TED+PR
OFIT+(70%
+Den
tiACa
l+&+15
%+Priva
te+In
surance+&
+15%+No
+insurance)
A$60
,404.00
ANITI
CIPA
TED+PR
OFIT+(70%
+Den
tiACa
l+&+15
%+Priva
te+In
surance+&
+15%+No
+insurance)
$25,3
52.00
ANITI
CIPA
TED+GR
OSS+M
ARGIN+(70%
+Den
tiACa
l+&+15
%+Priva
te+In
surance+&
+15%+No
+insurance)
A99%
ANITI
CIPA
TED+GR
OSS+M
ARGIN+(70%
+Den
tiACa
l+&+15
%+Priva
te+In
surance+&
+15%+No
+insurance)
42%

The Center For Oral Health SBOHC Operations Manual
Appendix C4: Sample P&L Statement
14-‐Jan Feb-‐14 14-‐Mar
REVENUE
ACTUAL ACTUAL ACTUAL DENTI-‐CAL REMINBURSMENT
$4,782.40 $4,300.80 $5,025.20
PRIVATE INSURANCE REMINBUSMENT $2,221.80 $1,352.10 $2,345.60
TOTAL REVENUE
$7,004.20 $5,652.90 $7,370.80
EXPENSES SALARIES & BENEFITS
$3,664.00 $3,664.00 $3,664.00 TRAVEL
$25.00 $25.00 $25.00
TELEPHONE & HOTSPOT
$100.00 $100.00 $100.00
TOTAL EXPENSES
$3,789.00 $3,789.00 $3,789.00
NET INCOME
$3,215.20 $1,863.90 $3,581.80
• Sample P&L taken from DentaQuest Institute “Map To The Future: Back Mapping School Based Oral Health To Achieve Financial Sustainability”
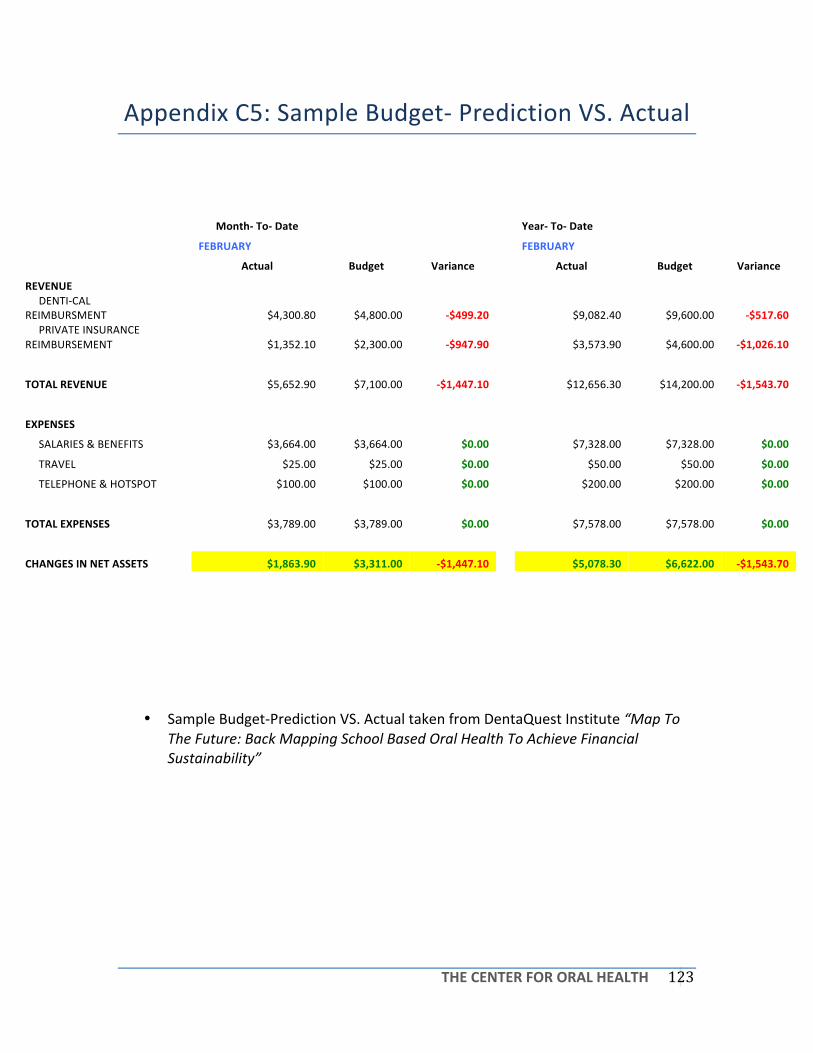
THE CENTER FOR ORAL HEALTH
123
Appendix C5: Sample Budget-‐ Prediction VS. Actual
Month-‐ To-‐ Date
Year-‐ To-‐ Date
FEBRUARY
FEBRUARY
Actual Budget Variance
Actual Budget Variance
REVENUE
DENTI-‐CAL REIMBURSMENT
$4,300.80 $4,800.00 -‐$499.20
$9,082.40 $9,600.00 -‐$517.60
PRIVATE INSURANCE REIMBURSEMENT
$1,352.10 $2,300.00 -‐$947.90
$3,573.90 $4,600.00 -‐$1,026.10
TOTAL REVENUE
$5,652.90 $7,100.00 -‐$1,447.10
$12,656.30 $14,200.00 -‐$1,543.70
EXPENSES SALARIES & BENEFITS
$3,664.00 $3,664.00 $0.00
$7,328.00 $7,328.00 $0.00
TRAVEL
$25.00 $25.00 $0.00
$50.00 $50.00 $0.00
TELEPHONE & HOTSPOT
$100.00 $100.00 $0.00
$200.00 $200.00 $0.00
TOTAL EXPENSES
$3,789.00 $3,789.00 $0.00
$7,578.00 $7,578.00 $0.00
CHANGES IN NET ASSETS
$1,863.90 $3,311.00 -‐$1,447.10
$5,078.30 $6,622.00 -‐$1,543.70
• Sample Budget-‐Prediction VS. Actual taken from DentaQuest Institute “Map To The Future: Back Mapping School Based Oral Health To Achieve Financial Sustainability”

The Center For Oral Health SBOHC Operations Manual
Evaluation Appendix D1-‐ D2

THE CENTER FOR ORAL HEALTH
125
Appendix D1: Sample Patient Satisfaction Survey

The Center For Oral Health SBOHC Operations Manual
Marketing Appendix E1-‐E6

THE CENTER FOR ORAL HEALTH
127
Appendix E2: SBOHC Information Brochure
CMOHS, Executive Director, and Partners For A Healthier Community, "CMOHS Brochure 2013." Www.cmohs.net (n.d.): 1-‐2. CMOHS. 2013. Web. 11 Aug. 2013.

The Center For Oral Health SBOHC Operations Manual
Appendix E3: Denti-‐Cal Information Letter
Denti&Cal*Information*
Medi&Cal & How to Apply*� Call$or$visit$your$local$County$Social$Services$office$and$ask$for$a$Medi5Cal$application$or$Apply$on5
line$(Not$DHCS)$� If$you$need$help$filling$out$the$forms,$call$the$county$social$services$agency.$$� Mail$or$take$your$application$with$the$required$verifications$(proof)$to$the$nearest$social$services$
���������������������������������������� �����������������������������������������������������please$send$what$you$have.$You$can$send$the$rest$later.$The$sooner$the$social$services$agency$receives$your$application,$the$sooner$your$case$may$be$processed$and$your$Medi5Cal$benefits$can$begin.$$
� If$you$get$SSI/SSP$payments,$your$Social$Security$administration$office$automatically$sets$up$Medi5Cal$for$you.$No$separate$application$for$Medi5Cal$is$needed.$You$will$get$your$Medi5Cal$card$(BIC)$in$the$mail.$$
� If$you$get$CalWORKs$payments,$the$county$social$services$agency$automatically$sets$up$Medi5Cal$for$you.$No$separate$Medi5Cal$application$is$needed.$You$will$get$your$Medi5Cal$card$(BIC)$in$the$mail.$
Do you qualify for Medi&Cal benefits? If you are enrolled in one of the following programs, you can get Medi&Cal: � SSI/SSP$� CalWorks$(AFDC)$� Refugee$Assistance$� Foster$Care$or$Adoption$Assistance$Program$ You can also get Medi&Cal if you are: � 65$or$older$� Blind$� Disabled$� Under$21$� Pregnant$� In$a$skilled$nursing$or$intermediate$care$home$� On$refugee$status$for$a$limited$time,$depending$how$long$you$have$been$in$the$United$States$� A$parent$or$caretaker$relative$or$a$child$under$21$if:$
The$child's$parent$is$deceased$or$doesn't$live$with$the$child,$or$The$child's$parent$is$incapacitated,$or$The$child's$parent$is$under$employed$or$unemployed$
� Have$been$screened$for$breast$and/or$cervical$cancer$(Breast$and$Cervical$Cancer$Treatment$Program)$
$$

THE CENTER FOR ORAL HEALTH
129
Contact$your$local$County$office$for$more$information$or$apply$on5line$at$www.benefitscal.org**(Not$DHCS).$$
*
Beneficiary Telephone Service Center at (800) 322-6384. The call is free. Medi-Cal dental program representatives are available 8:00 a.m. to 5:00 p.m., Monday through Friday to assist you. For more detailed information visit:
http://www.denti&cal.ca.gov/WSI/Bene.jsp?fname=BeneSrvcs*
GENERAL FAQS
1. How do I locate a dentist? For assistance on finding dentists who accept new patients for the Medi-Cal Dental Program, you may call toll-free (800) 322-6384, Monday through Friday, 8:00 a.m. to 5:00 p.m.
2. Can I be charged for services? Services that are included in the Medi-Cal Dental Program's scope of benefits are not chargeable to the Medi-Cal dental beneficiary. However, you are responsible for any Share of Cost amount. You are also responsible for the benefits available under the Medi-Cal Dental Program that duplicate those provided under any other contractual or legal entitlements you are receiving.
3. What is the Share of Cost program? If your income is more than the Medi-Cal limits for your family size, you will have to pay a certain amount only in the month you have medical expenses. The amount that you pay is called your Share of Cost (SOC). When you pay or promise to pay that amount, your SOC amount is considered met. Once you have met your SOC, Medi-Cal will pay the rest of your covered medical and dental bills for that month. For example, if your SOC is $50 and your medical bills for services covered by Medi-Cal for that month are $500, you must pay $50. You have then met your SOC and Medi-Cal will pay the remaining $450. You may satisfy your SOC amount through any medical provider such as your doctor, dentist, pharmacy, or optometrist.
4. Can I get a copy of my x-rays and records from my dentist? You may obtain a copy of your x-rays or records from your dentist; however, your dentist may charge you a reasonable fee for their reproduction.

The Center For Oral Health SBOHC Operations Manual
CMOHS, Executive Director, and Partners For A Healthier Community, "CMOHS Brochure 2013." Www.cmohs.net (n.d.): 1-‐2. CMOHS. 2013. Web. 11 Aug. 2013.
5. What is the best time to call the Medi-Cal Dental Program? The best time to call the Medi-Cal Dental Program is between 8:00 a.m. and 10:00 a.m Monday - Friday.
6. How do I check to see if I'm eligible for the Medi-Cal Dental Program? To check on your eligibility for Medi-Cal benefits, please contact your County Social Services office, listed in your local telephone book.
7. I have misplaced my Benefits Identification Card (BIC); how do I get a new one? Please contact your local County Social Services office, listed in your local telephone book.
8. I am currently enrolled in a prepaid health plan/managed care plan; how do I change plans? Call MAXIMUS, the State's Health Care Options Contractor at toll-free (800) 430-4263.
9. Can I change dentists in the middle of treatment? If services were prior authorized to one dentist and you wish to change your dentists, it is necessary that you write a letter indicating your change and have your new dentist submit that letter to the Medi-Cal Dental Program with his/her Treatment Authorization (TAR) form. The Medi-Cal Dental Program will contact your previous dentist to verify if any of the prior authorized services have been performed and will issue a new Notice of Authorization (NOA) as applicable.
10. What if I am denied services requested for prior authorization? If you are denied services that your dentist has requested prior authorization for, please contact your dentist to determine if a re-evaluation of the request could be made. You may also file a request through the Department of Social Services for a Fair Hearing by calling toll-free (800) 952-5253. You may also write to:
The Department of Social Services State Hearings Division P.O. Box 944243 MS 19-37 Sacramento, CA 94244-2430
To expedite your request, please include the Document Control Number (DCN). The DCN references the denied services.*

THE CENTER FOR ORAL HEALTH
131
Appendix E4: Sample Principal Award Letter
The Center For Oral Health SBOHC Operations Manual
Appendix E5: Sample Teacher Award Letter & Certificate

THE CENTER FOR ORAL HEALTH
133

The Center For Oral Health SBOHC Operations Manual
Policy, Licenses, Safety Compliance, and Taxes
Appendix F1-‐F3

THE CENTER FOR ORAL HEALTH
135
Appendix F1: Radiation In Daily-‐Life

The Center For Oral Health SBOHC Operations Manual
Appendix F2: Personal Protective Equipment Chart

THE CENTER FOR ORAL HEALTH
137
Appendix F3: Senate Bill No. 562
Senate Bill No. 562
CHAPTER 624
An act to amend Section 1657 of the Business and Professions Code,relating to dentists.
[Approved by Governor October 7, 2013. Filed withSecretary of State October 7, 2013.]
legislative counsel’s digest
SB 562, Galgiani. Dentists: mobile or portable dental units.Existing law, the Dental Practice Act, provides for the licensure and
regulation by the Dental Board of California of those engaged in the practiceof dentistry. Existing law provides that a person practices dentistry if theperson, among other things, manages or conducts as manager, proprietor,conductor, lessor, or otherwise, in any place where dental operations areperformed. Existing law authorizes a dentist to operate one mobile dentalclinic or unit that is registered and operated in accordance with regulationsadopted by the board. Existing law exempts specified mobile units fromthose requirements. Other provisions of existing law, the Mobile HealthCare Services Act, require, subject to specified exemptions, licensure bythe State Department of Health Care Services to operate a mobile serviceunit.
This bill would eliminate the one mobile dental clinic or unit limit andwould require a mobile dental unit or a dental practice that routinely usesportable dental units, as defined, to be registered and operated in accordancewith the regulations of the board. The bill would require any regulationsadopted by the board pertaining to these matters to require the registrant toidentify a licensed dentist responsible for the mobile dental unit or portablepractice, and to include requirements for availability of followup andemergency care, maintenance and availability of provider and patient records,and treatment information to be provided to patients and other appropriateparties.
The people of the State of California do enact as follows:
SECTION 1. Section 1657 of the Business and Professions Code isamended to read:
1657. (a) For the purposes of this section, the following definitions shallapply:
(1) “Mobile dental unit” means a self-contained facility, which mayinclude a trailer or van, in which dentistry is practiced that may be moved,towed, or transported from one location to another.
94

The Center For Oral Health SBOHC Operations Manual
(2) “Portable dental unit” means a self-contained unit housing equipmentused for providing dental treatment that is transported to, and used on atemporary basis at, nondental office locations.
(b) A mobile dental unit, or a dental practice that routinely uses portabledental units to provide treatment in nondental office locations, shall beregistered and operated in accordance with regulations established by theboard. These regulations shall not be designed to prevent or lessencompetition in service areas. The regulations shall require the registrant toidentify a licensed dentist responsible for the mobile dental unit or portablepractice, and shall include, but shall not be limited to, requirements foravailability of followup and emergency care, maintenance and availabilityof provider and patient records, and treatment information to be providedto patients and other appropriate parties. A mobile dental unit, or a dentalpractice using portable dental units, registered and operated in accordancewith the board’s regulations and that has paid the fees established by theboard, including a mobile dental unit registered for the purpose specifiedin subdivision (e), shall otherwise be exempt from this article and Article3.5 (commencing with Section 1658).
(c) A mobile service unit, as defined in subdivision (b) of Section1765.105 of the Health and Safety Code, and a mobile dental unit or portabledental unit operated by an entity that is exempt from licensure pursuant tosubdivision (b), (c), or (h) of Section 1206 of the Health and Safety Code,are exempt from this article and Article 3.5 (commencing with Section1658). Notwithstanding this exemption, the owner or operator of the mobileunit shall notify the board within 60 days of the date on which dental servicesare first delivered in the mobile unit, or the date on which the mobile unit’sapplication pursuant to Section 1765.130 of the Health and Safety Code isapproved, whichever is earlier.
(d) A licensee practicing in a mobile unit described in subdivision (c) isnot subject to subdivision (b) as to that mobile unit.
(e) Notwithstanding Section 1625, a licensed dentist shall be permittedto operate a mobile dental unit provided by his or her property and casualtyinsurer as a temporary substitute site for the practice registered by him orher pursuant to Section 1650 as long as both of the following apply:
(1) The licensed dentist’s registered place of practice has been renderedand remains unusable due to loss or calamity.
(2) The licensee’s insurer registers the mobile dental unit with the boardin compliance with subdivision (b).
O
94
— 2 —Ch. 624

THE CENTER FOR ORAL HEALTH
139
Fire, Earthquake, and Natural Disaster Protocols Appendix G1

The Center For Oral Health SBOHC Operations Manual
Appendix G1: Sample General Office Safety Plan

THE CENTER FOR ORAL HEALTH
141
References & Credits References
Credits

The Center For Oral Health SBOHC Operations Manual
Reference 1. Gidley SBOHC Clinic Operations Manual, 2012-‐ 2013
2. U.S Department of Health and Human Services-‐ Health Resources and Services
Administration. School-‐Based Comprehensive Oral Health Services Grant Program Application 2011
3. DentaQuest Institute. Map to the Future-‐ Back Mapping School Based Oral Health To Achieve Financial Sustainability, 2014
4. DentaQuest Institute. Safety Net Oral Health Financial Fundamentals-‐ Basic Financial Essentials. Doherty, Mark DMD. April, 2014
5. College of Dental Medicine Clinic Manual. Western University of Health Sciences College of Dental Medicine, 2011-‐2012.
6. University of the Pacific Arthur A. Dugoni School of Dentistry. Pacific Handbook, 2007.
7. Peng, Yawen. Pediatric Procedures Module. 2011.
8. CDA Compass. Worksheets adapted: Patient Bill of Rights, Breach of HIPAA Flow Chart, Dental Materials Fact Sheet, Refusal of Faculty/Student/Patient Post-‐Exposure Medical Evaluation, Ergonomics Checklist and Poster, Office Safety Checklist, Child Abuse/Neglect, Patient Complaint, Medical Release, Medical History (Minor).

THE CENTER FOR ORAL HEALTH
143
Credits 1. CHAN Staff (…)
2. WesternU DMD Faculty, Adjunct Faculty, and Staff (Dr. Marisa Watanabe, Dr.
Timothy Martinez, Mr. Josih Hostetler, and Dr. Dianne Tungol)





























