Embed Size (px)
Citation preview
71
CHAPTER 5
Aphasia GroupCommunication Treatment:
The Aphasia Center ofCalifornia Approach
ELLEN BERNSTEIN-ELLIS AND ROBERTA J. ELMAN
Philosophy of Program
The Aphasia Center of California (ACC)opened its doors as a nonprofit organiza-tion in September 1996. Housed withina Senior Center in Oakland, California,the ACC was the first independent not-for-profit organization dedicated to pro-viding direct services to individuals withaphasia in the United States. Our aphasiagroups began in 1994 when the NationalEaster Seal Research Program funded ourstudy to investigate the efficacy of groupcommunication treatment for aphasia.Asreviewed in Chapter 1, the results of thestudy were positive (Elman & Bernstein-Ellis, 1999a,b). Both statistical and anec-dotal data told us that the establishmentof the ACC would allow us to offer agreatly needed service to adults withaphasia and their caregivers.
The Center’s mission statement is toencourage and expand communicationand quality of life for all those affected byaphasia. Our philosophy and provision ofservice are consistent with a social modelof health care (Elman,2005).The followingfour core values guide the organization:
■ Choice■ Shared leadership■ Age-appropriate services■ Community building
Currently, we offer nine communicationgroups. We also offer, on an as-neededbasis, a caregiver support group and, ona rotating basis, the Book ConnectionTM
program, which provides reading andwriting practice in a book club format,and the News Forum, which focuses onthe reading and discussion of currentevents. We also have offered a class on
05_Elman_71-94 9/15/06 10:39 PM Page 71

using the Internet (Elman, 2001). Addi-tionally, we offer a weekly exercise classand an art class co-facilitated by theAdult Education Department of the localschool district.We are committed to pro-viding a “treatment array” that our mem-bers feel best serves their interests andneeds (Elman, 1998).
Several factors converged to forge thephilosophical foundation of the ACC.First, we felt the urgent need to developa viable, effective model for providingaphasia treatment in view of changes inhealth care provision and reimbursement.With the emergence of managed care,our treatment environment dramaticallychanged.The number of visits authorizedby insurance carriers shrank. The natureof aphasia wasn’t changing, but the timewe had to treat communication deficitswas, and this reduction had serious impli-cations. It was becoming the norm that apatient who would have previously re-ceived a 3- to 6-month treatment author-ization was now authorized for only 6 to10 visits (Elman & Bernstein-Ellis, 1995).This forced a significant restructuring of our treatment goals and priorities(Elman, 1994, 1998, 1999a, 2005).
We struggled with many questionsabout the impact of managed care onour clinical approach. What type of com-munication goals could reasonably bemet in the course of 10 sessions? Whichgoals would have the greatest impact ona client’s quality of life at the conclusionof our brief clinical contact (Elman,1994)? What treatment techniques andapproaches, many of which were devel-oped on the basis of lengthy treatmenttrials, would now be effective in a much-abbreviated clinical trial (Elman, 2006)?Individuals who recognized that theywould benefit from additional treatmentoften did not have the financial resources
to pursue private-pay options. Althoughwe still valued individual treatment foraphasia, we were forced to consider lowercost and efficacious options for meetingthe needs of our clients.
Another primary factor that guidedformation of the ACC reflected our con-scious decision to consider aphasia as achronic disorder (Elman, 1998, 2005; Lyon& Shadden, 2001; Sarno, 2004). Regard-less of whether stroke survivors withaphasia received 10 therapy sessions or50, many were left with residual deficitsthat had both significant and lasting im-pacts on their lives (Elman & Bernstein-Ellis, 1995, 1999b; Holland, 1992; Lyon,1992, 1997; Parr, Byng, Gilpin, & Ireland,1997; Pound, Parr, Lindsay, & Woolf,2001; Sarno, 2004). Even our clients withmild aphasia told us that the onset of the disorder imposed lifelong changes intheir communicative abilities (Elman &Bernstein-Ellis, 1995). We consideredaphasia as any other chronic medical“condition” in which full recovery topremorbid status was unlikely (Elman,1998, 2005). For instance, with the onsetof diabetes, ongoing insulin treatmentmay be needed to manage the condition.It would be unethical to withdraw theinsulin after an arbitrary amount of timewithout substituting another treatment.Is it not surprising that some stroke sur-vivors become isolated and depressedafter discharge from a speech-languagetherapy program? What should we do toreplace the support and value that thetherapeutic environment once provided?Patients with diabetes are not “dis-charged” from the treatment designed to best manage their chronic disorder.We concluded that people with chronicaphasia deserved the same conceptualapproach of ongoing management to sup-port their communication impairment.
72 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 72

A useful analogy for the sustainedmanagement of aphasia may be that ofhealth club membership. People havemany personal reasons for joining a healthclub, such as improving their level of fitness or attempting weight reduction.When the goal is achieved, patrons arenot asked to leave the club. Rather, theyare encouraged to continue their partic-ipation in order to sustain their accom-plishment. The benefit of the exercisedoes not diminish once the goal is met.Some people continue to make improve-ments in their fitness level and actuallyexceed their original goal. Continuedhealth club membership may enhancethe chances that a person maintains thegains that he or she has made.
We suggest that health club member-ship and participation in an aphasia treat-ment group are remarkably similar. Eachparticipating member has a persistingcondition. Management of the conditionmay be enhanced by group treatmentsessions that facilitate the use of strate-gies to optimize communication. Gettingweekly “workouts” that promote success-ful communicative interactions may helpsustain gains made in individual therapy.Some members make new gains overtime because of the exposure to newstrategies via peer modeling, the oppor-tunity for practice and feedback, and thepsychosocial support offered by thegroup environment.
This sustained management approachis consistent with the World Health Orga-nization (WHO) framework, the Inter-national Classification of Impairments,Disabilities and Handicaps, ICF (WHO,2001), and the Life Participation Approachto Aphasia (LPAA). Please see Chapter 1for a brief description of the ICF and theLPAA. These frameworks indicate thatspeech-language pathologists should
address not only linguistic deficits ofaphasia but also any resulting activitylimitations, participation restrictions,and environmental barriers. We havelearned that some valuable treatmentgoals may take much longer to achievethan our training taught us to expect.Moreover, we have learned that our mem-bers with aphasia make gains beyondstandard periods for recovery (Elman &Bernstein-Ellis, 1999a, 1999b).ACC mem-bers and their families have told us aboutpersonal successes that significantly affectquality of life that they attribute, at leastin part, to participation in our groups.Through their stories, we’ve learned thatour members make changes and achievegoals that are not always captured byperformance on standardized speech andlanguage assessment tools but nonethe-less are a vital contribution to their adjust-ment to living with aphasia. (Elman,2005; LLPA Project Group, 2000, 2001;Pound et al., 2001).
A final factor was responsible for thecreation of the ACC. A 1989 visit to the Aphasia Centre of North York (nowthe Aphasia Institute) in Toronto, Canada,greatly influenced our perspective onaphasia groups. The treatment model wesaw was a source of clinical motivationand inspiration (Kagan, 1995, 1998;Kagan & Gailey, 1993; Kagan, Winckel,& Shumway, 1996). Its impact also hasbeen cited by other clinical “visitors”(Hersh, 1998; Beeson & Holland, 1994;Jordan & Kaiser, 1996).
Entry Criteria
After the completion of our researchstudy on the efficacy of group therapyfor aphasia (Elman & Bernstein-Ellis,
APHASIA GROUP COMMUNICATION TREATMENT 73
05_Elman_71-94 9/15/06 10:39 PM Page 73

1999a), we were able to open our pro-gram to the community at large. Cur-rently, the ACC allows any adult withaphasia to attend. Our members travel toour groups from six counties in the BayArea and some from more than 60 milesaway.The primary etiology for our groupmembers is either thromboembolic orhemorrhagic stroke. Some membershave had only a single documented cere-brovascular incident. Others have a his-tory of multiple strokes. We accept alllevels of aphasia severity, from the mostsevere to only mild aphasia. We do havemembers with less common causes suchas primary progressive aphasia, headinjury, brain abscess, or chemotherapy-induced aphasia, and some with aphasiaof unknown etiology. So long as thebehavioral characteristics are “aphasic-like” in nature, and other behaviors donot detract from participation, an indi-vidual is welcome to join. Although wedo not accept someone with a primarydiagnosis of dementia, some of our mem-bers are coping with various degrees ofcognitive decline.
There is no entry criterion for timepost-onset. Our members range from1 month post-stroke to more than 20 yearspost-stroke. A majority of our membersare from 3 months to 10 years post-onset,with an age range of 28 to 95 years. Wehave a variety of referral sources. Somemembers locate us through the localnewspaper, either from a feature storyabout the ACC or from a community bul-letin board listing. Other members comevia referral from local speech-languagepathologists at hospitals, outpatient ther-apy clinics, or private practices. Still othershear about the ACC through a personalgrapevine of information including friends,the ACC website or other websites, orour community outreach projects.
Assessment
During the research phase of our groupprogram, we were able to complete astandard battery of both quantitative andqualitative measures of speech-languageperformance and psychosocial status onevery member. Once we became a non-profit organization, we did not have theresources to complete these assessmentsas standard practice. We now gather rel-evant information at intake through sev-eral sources. There is typically a phoneinterview with either the potential mem-ber or with his or her caregiver. Fre-quently we are able to talk directly withthe previous speech-language patholo-gist. These contacts allow us to obtainmedical background, personal and socialinformation, and treatment history, andto glean a sense of communicative func-tioning across the modalities. Sometimeswe are able to obtain records with rele-vant assessment information. When wehave the services of a student intern, weare able to arrange for a few supervisedassessment sessions. We select membersfor whom we feel that the informationfrom a standard aphasia battery wouldhelp us to understand better their com-munication profile.
Once an individual is interested inattending our program, we choose agroup for that potential member toobserve, based on which of our groupshave an opening, as well as the person’sschedule. In addition, we consider howa person’s functioning and personalitymight interact with the current compo-sition of the group. Sometimes, becauseof logistical constraints, there is simplyno choice, but we have found that thegroups are remarkable in their ability toadapt to the diversity of their member-
74 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 74

ship. The first observation session in thegroup allows us to assess informally eachprospective participant’s communicativeand social style. Each member completesan emergency information form that pro-vides personal contacts, pertinent med-ical history, and current medications.Group composition is addressed furtherin the Clinical Techniques section laterin the chapter.
Treatment Goals
As we began to formulate the type ofgroups we wanted to promote, our expe-rience in Toronto helped guide our treat-ment model at the ACC. Our primarytreatment goals are to enhance communi-cation skills and maximize psychosocialwell-being and quality of life for individ-uals affected by aphasia. These primarygoals are achieved by focusing on severalwell-defined factors, discussed next.
Member and Family Education
We believe that people with aphasia andthose who care about them benefit fromunderstanding the nature of the commu-nication disorder. Most of our stroke sur-vivors and their families tell us that theyhad never heard of the word “aphasia”until after their stroke. Very little or nopatient education has been offered to amajority of our members before comingto the Center. Many of our membershave never met anyone else living withaphasia until they attend our groups, andthey report that they are grateful for theconnection they feel. We try to offermaterials that will enhance their under-standing of aphasia. If this is appropriate,
we encourage new members and theirfamilies to watch videotapes about apha-sia: What Is Aphasia? and Pathways:Moving beyond Stroke and Aphasia(Ewing & Pfaltzgraf, 1991a, 1991b). Wealso encourage a caregiver or familymember to sit in on a session to observehow our groups function. We offer aquarterly stroke education support groupfor members and family members, as wellas a caregivers’ group. Another source ofinformation and support is our biannualnewsletter, which features topics relatedto aphasia, ACC members, and activitiesat the Center. Copies of the ACC newslet-ter are available on the Center’s website(www.aphasiacenter.org).
Personal Goals
We try to promote an increased aware-ness of each members’ personal goalsand progress made toward those goals.We support attempts at communicativesituations personally relevant to eachmember. We have found that many mem-bers find it difficult to acknowledge theirgains and therefore benefit greatly fromthe recognition the group gives to them.
Conversational Practice:Expanding Participation
We firmly believe that both the desire toengage in adult conversation with peersand the benefits of conversational prac-tice cross all severity levels of aphasia.Experience has taught us that it typicallytakes more effort to promote cross-talkand member-led discussions in groupscomposed of members with moderate tosevere aphasia, but there remains a natu-ral motivation to share topics of mutual
APHASIA GROUP COMMUNICATION TREATMENT 75
05_Elman_71-94 9/15/06 10:39 PM Page 75

interest regardless of severity level(Elman, 2005; Kearns & Elman, 2001).
Capobianco and Mahli (1995) recog-nize the value of the group setting in that“patients congratulate each other, adviseeach other, and argue with each other—all of which are normal adult communi-cation activities” (p. 2). When a groupexpresses an interest in a topic or theme,there is a communicative spark that canthen be fanned by the clinical techniqueschosen to promote interaction and infor-mation exchange. We view the topic ortask as the springboard, rather than thevehicle, for sparking communicativeintent. More times than not, an intro-duced topic has been cast aside to followwhatever unpredictable conversationalpath the group finds more interesting andthus more conversationally productive.
Sharing personally relevant topicspromotes connections among the mem-bers. New friendships develop. Further-more, members have the opportunity to assume or reclaim a variety of socialroles. We have been influenced byresearch that shows strong relationshipsamong variables such as positive health,social connectedness, and purpose in life(Ryff & Singer, 1998, 2000; Ryff, Singer, &Love, 2004). We work to help our mem-bers connect with one another, as wellas to assist them in re-creating their ownidentities and future selves (Markus &Nurius, 1986).
For instance, one of our members,L.T., suffered a stroke in her late 40s thatleft her with severe physical and commu-nication impairments. Even now, 8 yearspost-onset, she has no speech except for some vocalizations when crying orlaughing. A former youth gospel choirdirector, L.T. had a busy social calendarthat included many community events.After her stroke, she withdrew to her
home and refused to see friends orattend any church-related activities. Afterstrong urging from her family, L.T.attended a communication group at theACC. Over time, we worked to developher expressive outputs of short graphicmessages, typing short messages on a“low-tech” electronic device, commu-nicative drawing, facial expressions, andgestures. With the support of her family,and after taking the Internet computerclass, L.T. focused on developing hercomputer skills. She developed com-puter-generated lists to help us trackbirthdays. She then began developingpersonalized greetings for birthdays,thank you notes, get-well cards, and any other special occasion, that she cir-culated to get signatures. L.T., despite her profound post-stroke deficits, wasadmired and respected for her contribu-tions to the Center. The staff relied onher to track upcoming birthdays. Shebecame the “social manager” at the ACC,a role that played an important part ofher life before her stroke. As anotherstroke survivor explained, the reason shelikes being part of the group is thateveryone is in “the same boat.” Sheobserved that whereas her old friendsmostly see what she can no longer do,her new ACC friends see her for whatshe can do.
Communicative Strategies
We focus on improving the ability toconvey a message using whatever strat-egy is most useful for that individual.Typically, our focus is on content ex-change instead of on linguistic accuracy.A variety of strategies to facilitate thesuccessful exchange of information aremodeled by the clinician and the group
76 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 76

members during discussions, includingthe use of natural gestures, personalizednotebooks, environmental resources suchas maps, newspapers, communicativedrawing, and graphic supplementation.The specifics of these techniques are dis-cussed later in this chapter.
Conversational Initiation
We focus on increasing initiation in con-versational exchanges. Davis and Wilcox(1981, 1986) emphasize the importanceof sharing the communicative burden ina conversation. Our clinical experiencehas revealed that it is typical for an indi-vidual with aphasia to assume a morepassive, responder role, while the personwithout aphasia becomes the initiator.This was particularly true in our clientswith moderate to severe aphasia. Ourgroups focus on both the initiator andthe responder roles in conversations. Webelieve it is essential for the therapist tomaximize the member’s opportunity todirect the discussion. This is differentfrom traditional didactic treatment mod-els, which often place the primaryresponsibility for leading the group onthe therapist (Elman, 2000).
Conversational Cross-Talk
We promote “cross-talk” or exchangesamong group members. It is easy to fallinto a “tea-party” or talk-show host pat-tern in which exchanges bounce backand forth between therapist and client—from the clinician to a member and thenback to the clinician, who again initiatesthe exchange with the next memberaround the table. The goal of our groups,however, is to promote follow-up on
group member topics via questions andcomments by other members in thegroup.
These treatment goals required thatwe embark into new clinical territory.The skills needed to facilitate participant-shared groups were markedly differentfrom those used to direct individual ther-apy sessions. Making changes in our clin-ical style was much more difficult thananticipated. As one student intern aptlydescribed, “It looks so easy when I ob-serve the group, but when I try to do it,I’m surprised at how hard it is. It’s likewhen you are skiing down hill and yousee a rock straight ahead. You know youshould avoid it, but for some reason you run straight into it. I know I need tochange course with the group, but some-how I still head straight for that rock.”Wehope that our discussion in the ClinicalTechniques section will help guide otherclinicians around at least a few of theclinical obstacles that we experiencedwhile learning to facilitate groups.
Documentation of Progress
The challenge of providing services as anonprofit organization with limitedresources has eliminated our ability toinvest large amounts of time in formalreassessments. As previously mentioned,we occasionally are able to utilize theservices of student interns to evaluatemembers who have not been recentlyassessed. Informal conversations withmembers and their families allow us totrack reports of changes in communica-tive or psychosocial status. At staff meet-ings, we discuss changes that have beenobserved during group sessions. Infor-mal logs have been helpful in tracking
APHASIA GROUP COMMUNICATION TREATMENT 77
05_Elman_71-94 9/15/06 10:39 PM Page 77

anecdotal information. We also keep in-teresting samples of writing and commu-nicative drawings to allow for comparisonover time. We hope that with additionalfinancial support, we will be able toinvest more time in documenting prog-ress. Part of the challenge lies in ourinterest to access tools that providemeaningful information, including qual-ity of life changes. There are few toolsavailable that are appropriate for usewith people with aphasia, althougheffort and focus have increased in recentyears to address this need (Blackstone &Berg, 2003; Elman, 2005; Frattali, 1996,1998; Frattali, Thompson, Holland, Wohl,& Ferketic, 1995; Simmons-Mackie, 2001;Simmons-Mackie & Damico, 1996.) SeeChapter 3 for an overview of various out-come measures.
Case Study
The following brief case study illustratesthe outcomes of a rather typical ACC par-ticipant. J.B., a 48-year-old white female,suffered a hemorrhagic stroke that lefther with a moderately severe nonfluentaphasia and right-sided paralysis. Unableto live independently, she resided with herparents. She started in an ACC communi-cation group approximately 6 monthsafter her stroke, subsequent to dischargefrom individual speech-language therapy.At entry, her performance score for the Aphasia Quotient (AQ) portion of the Western Aphasia Battery (WAB) was65.2. Her interactions during group wereslow and laborious. She needed constantcoaching to use communicative strate-gies. Most notable was her poor eye contact. She spent most of the sessionlooking down at the table. Initiation ofcommunicative interactions was mark-
edly impaired. She expressed frustrationand depression over the loss of her jobas a school bus driver, her loss of inde-pendence, and her loss of an activesocial schedule.
J.B. attended group once weekly. Thegroup encouraged her to utilize graphicattempts and communicative drawing asstrategies to help convey content. Theclinician asked the group members tocue J.B. regarding her eye contact. Dis-cussions frequently addressed the psy-chosocial issues with which she wasstruggling, and group members offeredsupport, perspective, and experience. Shebegan to attempt some of the group’ssuggestions, starting with buying a wrist-watch with large clear numbers and usinga small notebook to track basic biograph-ical and personal information. Over a 2-year period, her successful spokencommunicative attempts increased inphrase length and content. There was anoticeable improvement in her eye con-tact and social skills. She moved backinto her own home and began livingindependently. J.B. learned how to takepublic transportation, including givinginstructions to the receptionist regardingher paratransit schedule. She started anexercise class at a local YMCA. She alsoparticipated in a reading and writingclass and an art class at the ACC.
It has been remarkable to watch J.B.emerge as a mentor to other participantswith aphasia in the communicationgroups. She began to take people underher wing and successfully hooked upseveral new members with the publictransportation system for disabled citizens.She became pivotal in group discussionsfor initiating cross-talk. She introducednew topics and would ask follow-upquestions without prompting. Periodicreadministration of the WAB showed
78 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 78

steady gains in her AQ across time. HerWAB AQ after 4 years of participation atthe ACC was 89.0. She was thrilled withthe improvement it represented, yet itwas a small aspect of the success sheexperienced.
J.B.’s WAB AQ has remained steady at 90.6 after 8 years of participation at the ACC. Her progress in the social-communicative arenas of her life contin-ues to be impressive. Personal goals shehas achieved during the last several yearsinclude independent travel to see her sis-ter in another state, speaking at publicforums to express her opinions on localissues such as building a casino in herneighborhood, organizing the invitationsand reservations for a holiday breakfast,designing and selling her own line ofgreeting cards to family and friends, andrejoining her church choir. One remark-able achievement included leading morethan 100 ACC members and guests for asing-along at the Center’s annual winterholiday party. We also appreciate andadmire J.B.’s commitment to fund-raisingefforts at the ACC. During the past severalyears, she has collected the most nameson her sponsor list for our annual Walkto Talk event.
Despite her ongoing challenges withword finding, processing complex audi-tory input, reading, and writing, J.B. con-tinues to inspire and support othersthrough the encouragement she offers,as well as through the model she pro-vides. She clearly embraces the philoso-phy of living fully with aphasia. Mostnotably, she has found an outlet for herdeeply altruistic nature through herinteractions with other group members.J.B.’s outcomes demonstrate what we’veobserved to varying degrees with manyof our members.These observations haveconvinced us that “an individual with
aphasia should not be expected to dis-continue activities or groups that enhancesocialization, conversation and/or reinte-gration back into community activities,through the reduction of communicativebarriers” (Elman, 1998, p. 230).
Clinical Techniques
ACC group sessions are 90 minutes long.Most groups range in size from 4 to 9members, with 5 to 7 the preferred tar-get number. Through experience, we’vefound that it may be more difficult tokeep the conversational ball rolling withgroups of fewer than 4 members. Like-wise, with groups larger than 10 mem-bers, it is difficult to give everyoneample time to participate. We’ve learnedthat there are no hard and fast rulesregarding group composition. Rather,the clinician’s personal preferenceshould be the primary guide. Two ACCclinicians prefer to form groups usingseverity as the lead attribute for place-ment. The tendency is to group mem-bers with mild to moderate aphasiatogether, and members with moderate tosevere aphasia together. Thus, peoplewith moderate aphasia often work wellin either group. Grouping by severityseems to accommodate discussionsabout adjustment issues associated withthe severity of the communication disor-der. Our groups composed of peoplewith milder aphasia seem to particularlyappreciate the opportunity to havequicker-paced, philosophical discussionsthat members with a greater degree ofaphasia may have trouble following. Onthe other hand, one clinician at the ACCprefers to have a mixture of aphasiaseverities in her groups. She feels that
APHASIA GROUP COMMUNICATION TREATMENT 79
05_Elman_71-94 9/15/06 10:39 PM Page 79

this promotes modeling and coachingopportunities, while enriching the vari-ety of interactions within the group. Weare convinced that either approach toforming groups works exceedingly well.
We’ve been questioned if a personwith Wernicke’s aphasia can benefitfrom a group setting. We indeed advo-cate integrating our members with poorauditory comprehension into our groups.The need for these members to developfunctional social conversation skills isjust as relevant as it is for those memberswith nonfluent aphasia. Our memberswith Wernicke’s aphasia typically needmore time and practice than our mem-bers with nonfluent aphasia to success-fully incorporate communication strate-gies such as the use of a communicationbook or communicative drawings. Thegroups provide an opportunity for consis-tent ongoing practice and reinforcementof progressive attempts at communica-tion. We have found that members withWernicke’s aphasia benefit greatly fromthe peer modeling.they receive. For aspecific example of the benefits of groupparticipation for individuals with Wer-nicke’s aphasia, see the section on com-munication resources later in the chapter.
As group members enter the Center’sprimary therapy room, the first order of business is to locate the appropriatenametag from the wall hanger that boastsover 70 names. Members wear nametagsat every session to promote the access ofnames during conversational exchanges.Our groups provide a warm welcome toparticipants. There is a deliberate effortto greet everyone who comes in the door.Coffee or other beverages are distributedby a group member who is willing tohelp with hospitality related tasks. Fam-ily members often are busy greeting oneanother and talking with the clinician
about relevant points of information.Once everyone is settled around thetable, any guest for the day is introducedand handed a temporary nametag. Werequest that family members periodicallyobserve, and we get a variety of otherobservers including potential membersand their family members. Typically, werequest that they join us around the tableand participate as a group member. Weprefer not to let visitors sit back in thecorner and watch us interact. Inclusionof visitors in the group promotes a morenatural conversation environment andprovides novelty and variety in terms ofconversational partners. Group mem-bers are responsible for introductionsand for getting to know the guest.
When the group is ready to start, wetry to follow up on a conversational ele-ment from the previous week and get asense of any priority topic that thegroup is interested in discussing. Ourgroups have evolved over time from hav-ing preplanned “themes” to having “top-ical” discussions—whatever is most rele-vant to their interests that day. Lookingback at our early philosophical discus-sions, we realized that relying on themeswas a safety net. In the beginning, it felttoo overwhelming to go into a groupwithout some sort of structured clinicalplan.As previously mentioned, our “best”interactive, participatory discussions typ-ically ranged in topic far from the pre-planned theme, so we learned that suc-cess did not rely on having a specific setof tasks or topics. Now, we rotate tasksor topics depending on the immediatecontext of the day. Some discussions aremore structured than others, such asthose addressing stroke education, role-playing communicative situations, inter-viewing guests, or sharing keepsakes orphotos. Other discussions are less struc-
80 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 80

tured, such as those involving currentevents, personal activities, vacation/holi-day plans, post-stroke adjustment discus-sions, and personal interests and hobbies.Our focus is directed to the techniquesneeded to promote conversational ini-tiation and to facilitate the exchange ofinformation regardless of whatever taskor topic rotates across the conversationalmenu of the group.
Increasing ConversationalInitiation
Increasing conversational control andinitiation of our members with aphasia is a primary goal of our groups. There are a variety of techniques that we havefound useful for addressing this goal.
Directing the Facilitator’s Role to aSpecific Group Member
This technique consists of asking a groupmember to lead the discussion about a specific topic. A peer facilitator cangather opinions about an upcoming elec-tion, survey each person’s favorite typeof pie, or inquire about everyone’s week-end. This technique can be adaptedacross severity levels. Some membersmay need only a key word to help formu-late a query, whereas others may benefitfrom a written script to prompt the ques-tion. Scripting, or conversational coach-ing, refers to writing out either a fewwords to a full sentence and handing it to the member, who either reads itdirectly or uses it as a springboard (Bee-son & Holland, 1994; Hopper, Holland, &Rewega, 2002). Allowing a member tofacilitate the discussion becomes partic-ularly dynamic when the member incharge takes on an active role and goes
beyond the question at hand. The groupis at its best when the follow-up ques-tions and feedback come from their peerfacilitator, rather than from the clinician.
“Passing the Question” or“Passing the Ball”
This time the facilitator’s role is sharedaround the table. The group discusses acertain topic. As each person concludesa turn, he or she restates the question ortopic for the next person. This methodensures that each member gets a turn toinitiate and to respond. It helps to putthe focus on the members, instead ofallowing a clinical “tea party” betweenthe clinician and the group members.This technique also lends itself to adap-tation across severity levels. Memberswith mild aphasia may elaborate on theoriginal question or theme, whereas non-verbal members may establish a commu-nicative gesture to engage their partner.
Addressing a Member’sParticipation Level
We ask, “Who hasn’t had a turn yet?” or“Who’s been too quiet?” This works bestwhen the group members begin to mon-itor one another’s participation levelsand try to ensure that everyone has hada turn.
Requesting That MembersGenerate a Topic
We ask members to bring in news arti-cles, personal items, photos, or anythingof interest. We ask the group, “What doyou want to talk about?” This promotesnovelty and humor—both essential ele-ments for successful groups. Our bestgroups are ones that share laughter.
APHASIA GROUP COMMUNICATION TREATMENT 81
05_Elman_71-94 9/15/06 10:39 PM Page 81

Frequently, it is a group member whofirst recognizes the humor in a situationor initiates a joke. The shared laughtercrosses aphasia types and severity.
Peer “Scaffolding” or Cueing
This refers to the opportunity for one ormore group members to help anothergroup member around some sort of com-municative block. Instead of the clinician’sproviding a cue, the clinician asks, “Whocan help Mrs. X get her message across?”This technique works well when multiplemembers offer help. By building on oneanother’s attempts, members are able toclarify the message.The group recognizesthat the message has been directed bythe group, rather than by the clinician.
Encouraging Peer Feedback
Frequently, it’s the other group memberswho won’t allow someone to “bail out”when faced with a communicative block.Instead, group members will display sup-port by passing a pad of paper to encour-age a drawing or writing attempt, or onemember will offer his or her communica-tion book for the “blocked” member touse, or will request that the memberslow down or speak louder. Membersdirectly tell one another, “Yes you can!”or “Try to do it,” and these exchangesseem to have more impact coming froma peer than from a clinician.
Peer Volunteers
We have asked members with mild apha-sia to volunteer in our mild to moderateaphasia groups, and we’ve asked mem-bers with either mild or severe aphasiato volunteer in our moderate to severeaphasia groups. Volunteers are selectedfor their ability to model good commu-
nicative strategies or interactions. One ofour most outstanding volunteers, L.I.,had severely impaired auditory compre-hension, with verbal output basically lim-ited to “Hey, mom.” However, he couldglean contextual information and useenvironmental resources in an extraordi-nary manner. L.I. could link a long stringof functional gestures or combine multi-ple communicative elements in a draw-ing to convey complex information. Hefrequently initiated conversational topicsusing these strategies. The group as awhole benefited from his modeling ofgestures and drawings.
“Personalizing” the Discussion
It is important to move from the keytopic at hand to people’s personal expe-riences or opinions about that topic. Forinstance, if a member brings up a newsitem about France, there is opportunityfor a series of related questions, such as“Who has been to France?” or “Who likesFrench cuisine?” or “What French movieshave you seen?” Although the key topicoften can hold the group’s interest,sometimes it is the related questions thatspark the real conversation.
Increasing Exchange ofInformation
Another primary goal of our groups is to facilitate exchange of information, andwe utilize several techniques for thatpurpose as well.
Supporting the Flow of Ideas withGraphic Attempts orCommunicative Drawing
We frequently encourage members todraw or write to enhance their message.
82 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 82

Pads of paper and pens are standarditems on the group’s table. These are dis-tributed to everyone in every group,regardless of severity. The clinician alsouses drawing and graphics as a standardway to emphasize content or to confirminformation. We prompt members: “Canyou draw or write it?” or “How else canyou show me what you mean?” Membersoften will exchange different ways ofapproaching a drawing and usually aredelighted to offer a better version thanthe clinician’s! Some members seem tohave a natural affinity for drawing and,with support and guidance, use it veryeffectively. Others need a higher level of support, training, and modeling. It isbeyond the scope of this chapter toreview the skills needed for communica-tive drawing. Please refer to the work ofLyon (1995) for a detailed description of this useful technique.
Graphic Choices
As described by Garrett and Beukelman(1992), the clinician presents severalviable responses to a member for him orher to indicate the preferred choice. Forexample, if we’re discussing favorite cui-sine, we might write “Mexican, French,Indian, Italian” in a clear column on apad of paper and present it to memberswho are primarily nonverbal, or whohave severely impaired auditory compre-hension. When members are permittedto select the item themselves, they cantake the lead in responding.
Natural Gestures
We frequently ask, within the context ofa conversation, “How can you show methat?” Sometimes brief, simple gesturesare sufficient, and other times more elab-orate gestures help to convey the mes-
sage. Once again, it is sometimes thegroup members who generate a betterway to show something compared withthe clinician’s model.
Communicative Resources
We make sure that maps, newspapers,number lines, visual scales, photos, anillustrated travel dictionary, and a calen-dar are always available. If memberscan’t remember the name of the moviethey saw, the movie section of the news-paper is available. If members can’t recallthe name of the place they plan to go onvacation, an appropriate map is withinarm’s reach. We have laminated severalversions of maps, including our localregion, the United States, and the world.When trying to hone in on how much anonverbal member likes something, weuse a laminated number line. There is asad face over the number 1 and a happyface over the number 10. Our memberscarefully select where their response fallsalong this continuum.We also encouragemembers to grab matchbooks, take-outmenus, or business cards when they goto a restaurant so they can share thisinformation with other group members.The use of these items allows the mem-bers, instead of the clinician, to take thelead in providing the information.
Some of our members benefit from per-sonalized notebooks. These have takenmany forms, from adaptations of commer-cial products to family-generated versions.Size and complexity also have varied.Most include a section for weekly events,family, friends, pets, places, restaurantsand food, photos, and basic information.We have found that some membersquickly utilize the notebook, whereasothers slowly gain facility.
One of our success stories involves a member with moderate Wernicke’s
APHASIA GROUP COMMUNICATION TREATMENT 83
05_Elman_71-94 9/15/06 10:39 PM Page 83

aphasia whose computer-savvy husbandcreated both a purse-sized and largerbinder-sized personal notebook. Becauseshe is an accomplished artist, he scannedcopies of her artwork into both of theseversions. He also created a family treediagram and imported photos for eachmember. Although her verbal output isseverely limited, she quickly began usingher notebooks to initiate topics and con-vey a wide range of information. A realsuccess was that she was able to coach anewer member with moderate to severeWernicke’s aphasia to use his notebookmore effectively. Initially, he seemedoblivious to the notebook. He then beganto model her behavior of putting hiscommunication binder on the table atthe start of each group session. Eventu-ally, he began to do this even without hervisual model. If he was asked about hisfamily, she would lean over and help himflip to the photo section of his note-book. Over time, he began to initiateusing his communication book to pro-vide information. Her peer modeling andcuing seemed to promote more progressthan encouragement from his family orthe clinician.
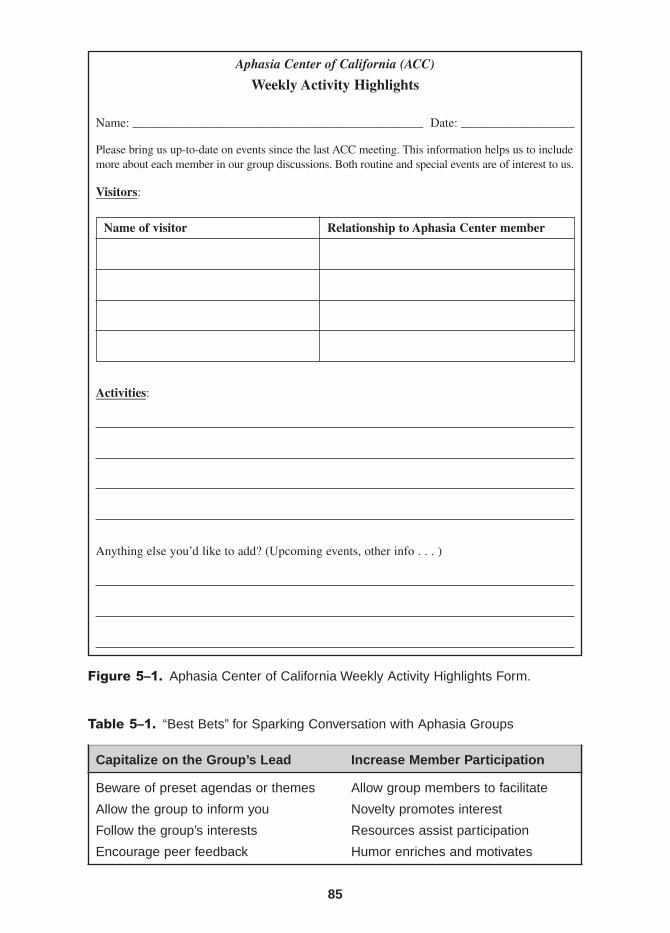
“Weekly Activity Highlights” Form
Families are coached to summarize high-lights and routine items that occur eachweek in a special form (Figure 5–1).Information about a trip to the grocerystore, a new outfit, or a weekly hair ap-pointment can provide a tremendousamount of potential conversational mate-rial. Some members attempt to completethe information form themselves eachweek. For various members, the formacts like a script, and they take the leadin sharing the information with thegroup. For members who are nonverbal,
the form allows the clinician to gain somespecific, personally relevant informationthat can be used to involve that partic-ular member in the discussion. Theseforms provide a gateway to participationfor members who are less able to initiatecontent, as well as for members withmoderate to severe fluent aphasia.
Table 5–1 summarizes some of our“best bets” for sparking dynamic conver-sation in aphasia groups.
Management Issues
Along with the helpful techniques pre-sented earlier, we’ve also learned some“management issues” inherent to thegroup setting that are important to ad-dress. One such issue involves handlingone or two group members who becomeoverly dominant. These members mayoccupy more than their fair share of thegroup’s conversational time. In manycases, these members may not be sensi-tive to monitoring their own turn taking.One solution is to ask that member to bein charge of making sure that everyoneparticipates. We ask him or her to “helpus include each and every member ofthe group.” Sometimes we are even moredirective and state that we need time foreach person to respond.
The clinician is always at high risk fordominating the group. It can be hard forthe clinician not to dominate by virtue ofexpertise. Although there is a definitetendency for the clinician to jump inimmediately and provide needed cues,it’s important to learn to involve thegroup members in problem solving anycommunicative obstacles. The clinicianneeds to ask, “What can Mary do to gether message across?” or “Could someoneshow another way to draw an airplane?”
84 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 84
Aphasia Center of California (ACC)
Weekly Activity Highlights
Name: ______________________________________________ Date: __________________
Please bring us up-to-date on events since the last ACC meeting. This information helps us to includemore about each member in our group discussions. Both routine and special events are of interest to us.
Visitors:
Name of visitor Relationship to Aphasia Center member
Activities:
Anything else you’d like to add? (Upcoming events, other info . . . )
Figure 5–1. Aphasia Center of California Weekly Activity Highlights Form.
85
Table 5–1. “Best Bets” for Sparking Conversation with Aphasia Groups
Capitalize on the Group’s Lead Increase Member Participation
Beware of preset agendas or themes Allow group members to facilitate
Allow the group to inform you Novelty promotes interest
Follow the group’s interests Resources assist participation
Encourage peer feedback Humor enriches and motivates
05_Elman_71-94 9/15/06 10:39 PM Page 85

or “Who can show us a way to gesturedriving?” These methods all supportincreasing the members’ participationwhile reducing the clinician’s dominance.It’s crucial for the clinician to learn theboundaries between being a “commu-nication broker” and overfacilitating.Kagan (1995, 1998) refers to the highlevel of skill needed to unmask an apha-sic member’s competency. Beeson andHolland (1994) refer to the clinician’sability to be a “communication broker”by interpreting, facilitating, and guidingcommunicative exchanges among groupmembers.The challenge lies in balancingthese roles.
Group members often will offerstrategies, support, and empathy. When a clinician gives up tight control of thediscussion’s content, there is risk thatawkward or uncomfortable issues maycome up. Racial, religious, political, sex-ual, and gender-related topics frequentlygenerate strong feelings. It is absolutelyessential to establish ground rules forstandards of behavior. ACC staff haveagreed that individuals who openly pro-mote bigoted racial or religious attitudesare not welcome in our groups. That isnot to say that our members must agreeon heated topics. One of the specialattributes of the ACC is the wide diversityour group members possess with regardto cultural, economic, professional, andeducational backgrounds. Part of the suc-cess of the groups comes from the com-mon bond that forms from sharing lifewith aphasia. Differences make the dis-cussions more interesting and dynamic,and our members share a deep respectand appreciation for one another.
A clinician must learn how to balancethe techniques he or she chooses withthe severity and size of the group. Sometechniques are more labor intensive thanothers and may take too long in larger
groups, where it’s important to monitorthe amount of time each person has toparticipate. It typically takes longer tocommunicate and confirm informationwith a partner who has aphasia, whichcan impair the conversational flow. Thismay result in side conversations that de-tract from the main conversational focus.Group members learn when a memberneeds extra time to convey a message,and we encourage patience. It is thefacilitator’s role to bring the group backto a unified focus.
Facilitating participant-led groups pro-vides additional challenges for the clini-cian. The clinician must understand theunique “flavor” of each group. Somegroups are news oriented, whereas oth-ers prefer psychosocial issues or socialtopics. Groups flourish when the clini-cian can adjust to the preferences ofeach group. It’s also important for groupmembers to understand that it takes timeto form group bonds and cohesiveness.This facilitates the acclimation processand promotes realistic expectations fornew group members.
Another challenge is to be sensitive tothe appropriate yardstick of change forgroup members. A group composed ofadults with chronic aphasia needs toprogress beyond an emphasis on linguisticchanges to adaptations that have a posi-tive impact on the members’ quality of life.As discussed previously, it is important tounderstand issues of impairment, activitylimitations, and participation restrictionsin relation to aphasia (WHO, 2001).
Discharge Criteria
At the ACC, we do not believe in therapist-ordained discharge criteria. As discussedearlier, we consider aphasia to be a
86 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 86
chronic disorder that deserves continuedcommunication and psychosocial sup-port for as long as desired. ACC partici-pants self-determine both the frequencyand the duration of their attendance.As stated by Elman (1998), “rather than a therapist determining a discharge date,individuals with aphasia determinewhether they desire discharge from theprogram. And using a market-based sys-tem, they vote with their feet” (p. 230).
Reimbursement
As discussed in articles by Elman (1998,1999a), we have chosen to seek themajor part of reimbursement for ourgroups outside of the traditional healthcare reimbursement system. We dependprimarily on private fees for our speech-language pathologist–facilitated groups.
Participants who attend one group weeklycurrently pay $18 per session. For thoseparticipants who elect to attend twice aweek, the cost for the second visit is $12.Participants enroll in ACC groups by pur-chasing a $180 session card (Figure 5–2).They “spend” down this card as the ther-apist crosses off the cost at each sessionattended. The session card is composedof circles, each representing $6. Thislow-tech system allows the therapist tocross off sessions of either $18 (3 circles)or $12 (2 circles) on the same card.An additional advantage of this system is that there is no need to schedule“makeup” sessions if participants are illor have medical appointments. When allsessions on the card have been attended,participants make a decision regardingreenrollment. If they decide to continue inthe groups, they purchase a subsequent$180 card. In addition to private pay-ment directly from participants, several
APHASIA GROUP COMMUNICATION TREATMENT 87
draC noisseS ainrofilaC fo retneC aisahpA__________________ _________________
desahcruP etaD emaN tnapicitraP
__________________________seripxE etaD erutangiS ffatS
$ $ $ $ $ $ $ $ $ $
$ $ $ $ $ $ $ $ $ $
$ $ $ $ $ $ $ $ $ $
Figure 5–2. Aphasia Center of California Session Card.
05_Elman_71-94 9/15/06 10:39 PM Page 87

third party payers authorize payment forour treatment groups.
Because the ACC is a charitable non-profit organization, its board of directorsand staff members are committed tokeeping program fees affordable. In addi-tion, sliding fee reductions are availableto those with low incomes. This ap-proach permits all who can benefit toattend the Center. In addition, our recre-ational activities are co-facilitated by adulteducation instructors and are offered asa “value-added” service at no additionalcost to current ACC participants.
Considerations for Specialized Groups
As we’ve described, our communicationgroups focus on the exchange of per-sonal, educational, and social information,along with discussing relevant news,from personal to international. In otherwords, we talk about anything of interestgoing on in group members’ lives or inthe world around them. We also offerseveral specialized groups. Althoughthey are similar in their communicative-social goals to our communicationgroups, some additional considerationsare warranted.
Book ConnectionTM
The Book ConnectionTM is a weekly bookclub group that reads and discusses pop-ular adult literature. Please see the man-ual by Bernstein-Ellis and Elman (2006)for an in-depth discussion of the BookConnectionTM program. Consistent withreports in the literature (Parr, Byng,Gilpin, & Ireland, 1997), many of our
ACC members told us that losing theability to read for pleasure significantlydecreased their quality of life. Wedecided that a book club format couldprovide the opportunity for our mem-bers to connect with literature, as well aswith one another. In order to makebooks accessible to members with mildto moderately severe reading deficits, wedeveloped a series of “reading ramps.”Reading ramps are similar in purpose tothe communication ramps discussed byKagan and Gailey (1993)—both provideadaptations that allow an adult withaphasia to participate successfully in thesocial life of the community. Some of thereading ramps we use in the Book Con-nectionTM program include large-printbooks, books on tapes, and a variety of materials found through multipleresources (e.g., Internet, library, video,newspaper, and so on) that serve toenrich the connection to the story. Wealso develop chapter summaries andhighlights, vocabulary lists, characterguides, and a series of worksheets thatreinforce chapter content and helpexpress personal reactions to the story.A sample of these materials is availableon the ACC website (www.aphasiacenter.org).
We offer two Book ConnectionTM
groups: one for members with mild tomoderate aphasia and one for memberswith moderate to moderately severeaphasia. However, other sites that haveoffered this program have reported suc-cess in mixing severity levels in theirgroups (Elman et al., 2005). We havefound that severity of aphasia is not themost important parameter related tosuccessful group participation. Instead,critical factors appear to be an interest inreading, a willingness to try adaptivestrategies, and adequate auditory com-
88 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 88

prehension for social conversation. Theweekly Book ConnectionTM meetings typ-ically cover an hour’s worth of audio-tape, or about 20 to 30 pages of large-print reading. Members read and/orlisten to the book on their own. Somemembers choose to read just the chaptersummaries or highlights created to sup-port the book. Most books span a 6- to16-week period, depending on theirlength. The fee for the class is based onthe group facilitator cost, multiplied bythe number of weeks, plus the cost ofthe book, audiotapes, and copying.
The role of the clinician as a bookclub facilitator has both similarities toand differences from that of facilitator incommunication groups. As in communi-cation groups, the facilitator of a bookclub may need to function as a commu-nication broker for members with morelimited expressive output (Beeson &Holland, 1994; Kagan, 1998). Strategiesto promote increased initiation, parti-cipation, and information exchange, asdiscussed earlier, are still relevant. Inaddition to these communication grouptechniques and strategies, the book clubfacilitator may need to summarize thegeneral storyline to help reinforce storycontent. It also is important for the bookclub facilitator to keep in touch with thebook club members to determine howthey are juggling the “logistics” of thebook club.
It is important for the clinician not tobe the only “subject expert” when facili-tating a book club group with memberswho have mild to moderate aphasia.These members asked us for a largerrole. To help transfer the responsibilityfor leading the group, we encouragemembers to find and report on addi-tional information related to the book.They also take turns in the role of discus-
sion leader. This can take the form ofproviding a brief synopsis of the chapteror developing a list of questions designedto spark group discussion. It can be chal-lenging to guide a member in the role offacilitator while also being sensitive tothe other dynamics of group process.Wehave found that some members becomeso enthusiastic about the book that it ischallenging for them to maintain equaltalking time.
Our group members tell us that theweekly book club discussions are thebest part of this group. They enjoy the exchange of ideas and engaging dis-cussion. One member described her per-spective: “I gain a lot from others . . .group is wonderful . . . it’s dynamic . . .everyone can operate at a certain leveland feel success. Even if they can’tspeak, each person has ideas and energyand brings it to the class . . . you can bechallenged at any level.”
We have found that our Book Connec-tionTM groups develop special bonds thatcome from sharing a common storylineas well as personal experiences relatedto that story. There is a sense of mutualaccomplishment as members make theirway through the book.We recognize thisachievement with a variety of specialevents on the final session for the book.From viewing special videos, to havingguest speakers, to eating food themati-cally related to the book, the members ofthe group celebrate together. For mostmembers, it is the first time since theirstroke that they have read a book forpleasure.
News Forum
When the Book ConnectionTM is on hia-tus, we offer the News Forum groups.
APHASIA GROUP COMMUNICATION TREATMENT 89
05_Elman_71-94 9/15/06 10:39 PM Page 89

The News Forum focuses on discussingcurrent events. This program beganwhen our members with mild to moder-ate aphasia expressed repeated frustra-tion with the challenges of participatingin discussions with families and friends,especially when the conversational focusturned to headline news. Although theywere able to maintain participation fordiscussions regarding personal topics,they found it much harder to participatewhen they had to cite specific names,events, or content related to news sto-ries. They felt relegated to a “nod andrespond” role at dinner parties and othersocial gatherings.To meet this challenge,we formed a group that focuses on read-ing and presenting news stories.
As with the Book ConnectionTM, weoffer two News Forum groups. Membersin both groups choose their own storiesfrom the newspaper, magazines, or theInternet to share each week. The diver-sity of the topics brought in by Forummembers is impressive and helps to keepthe discussions novel and unique. Rang-ing in subject from travel, to humaninterest to sports to news at all levels, thestories that members bring in generateinterest and adult discussion.
In our group with members who havemoderate to severe aphasia, the facilita-tor must decide how to maximize eachperson’s participation. For some mem-bers, we’ve developed worksheets tohelp them create a script for their story.Members complete these worksheets athome and then use their scripts todescribe the story to the group. Othermembers prefer to practice reading theheadlines to the group.The News Forumfacilitator can quickly skim the article,present the key facts, and foster a discus-sion around the topic. By generatingshort scripted questions related to the
story, the facilitator can engage memberswho need a springboard to participate.Sometimes the facilitator prepares twotypes of scripts: one that presents thefacts of the story and a second that pro-vides questions for other group mem-bers to ask about the story. Our NewsForum groups support both scripted andnonscripted interactions. The goal is to promote the use of communicativestrategies that best serve members in avariety of social interactions.
In our group with members who havemild to moderate aphasia, the partici-pants take the lead in presenting theirarticle. Many prefer to work from notesthat they have prepared at home. Somehighlight key content words and thenglance at the story as they lead the dis-cussion. Other group members are en-couraged to jump in and ask questions.This simulates the challenge of “real”conversation for the presenter andallows all group members practice in get-ting into an ongoing conversation. TheNews Forum facilitator monitors the bal-ance of group member participation andtracks conversational strategies beingused. One of the main goals for the facil-itator is to determine how to help eachperson utilize those strategies that allowfor the most communicative independ-ence and success.
Internet Classes
It is challenging for people with aphasiato learn from existing computer pro-grams or attend Internet classes. Com-puter instructors typically do not havethe needed skills to teach or communi-cate with people who have languageimpairments. The “digital divide” is greatfor all people with disabilities but is per-
90 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 90

haps largest for those with language disorders such as aphasia (Elman, 2001).Barriers must be overcome so that thosewith aphasia can achieve full participa-tion in the ever-growing digital economy(Elman, 2001; Elman, Ogar, & Elman,2000; Elman, Parr, & Moss, 2003).
Our ACC members told us repeatedlythat they wanted to learn how to accessthe Internet. Because of the wide rangeof computer ability and interests, wedecided to offer two Internet classes. Oneclass focuses on basic computer skillsneeded for such activities as using a per-sonal computer (PC), using a browser,and sending and receiving e-mail. Thesecond class focuses on more advancedInternet skills, such as those needed to usesearch engines, evaluate website informa-tion, and shop at e-commerce sites.
We use a computer classroom at theSenior Center for our Internet groups.We created a small local area network(LAN) in the computer classroom andconnected the machines together to a“digital subscriber line” (DSL) for fastaccess to the Internet. We also utilize anoverhead teaching monitor that allowsall members to view the instructor’scomputer. In this way, the instructor candemonstrate specific information andskills to all class members simultaneously.
Our Internet classes are more struc-tured and didactic than our other groups,in keeping with their purpose and con-tent. The instructor spends quite a bit oftime interacting one on one with individ-uals in the class in order to demonstratespecific skills. However, even Internetclasses provide opportunities for interac-tion among members.The class instructorcan place specific members side by sideso that they can instruct and learn fromone another. For example, one of our classparticipants was quite facile at using the
keyboard one-handed to access her e-mailaccount. She then worked with anotherclass member who was having muchmore difficulty in learning the necessarysteps. With added practice and peer sup-port, the second member achieved suc-cess, and both members were thrilled atbeing able to work together.
We determine the specific content forour Internet classes based on needsidentified by the specific members whoenroll. The instructor has a short inter-view with all enrolled members in orderto determine their “wish list” for theclass. In addition to creating this type ofcurriculum, it may be helpful for classinstructors to read through the Internettraining package prepared by The Uni-versity of Queensland. Developed to trainvolunteers how to teach Internet skills topeople with aphasia, it is available fordownload at the University’s website(www.shrs.uq.edu.au/cdaru/aphasiagroups). See Chapter 8 for more informa-tion on The University of QueenslandInternet program.
Conclusions
After a decade of experience, we findthat the greatest rewards of the ACC stillcome from the stories that our groupmembers and their families share with usabout the impact the ACC has had ontheir adjustment to living with aphasia.These stories highlight new communica-tive successes and improvements insocial adjustment. Most striking is thatthese changes continue no matter howmany years members have participatedin ACC programs. Our members con-tinue to demonstrate that there is no ceil-ing to personal growth or learning. We
APHASIA GROUP COMMUNICATION TREATMENT 91
05_Elman_71-94 9/15/06 10:39 PM Page 91

are fortunate to be able to create differ-ent learning environments, such as theBook ConnectionTM, the News Forum,and Internet classes in response to theirneeds. Our members tell us that they feelconnected to the ACC community andthat this connection helps them to findgreater meaning in their lives. As ourgroup members help one another, theyalso help us achieve a better understand-ing of what quality of life means, espe-cially for living with aphasia.
References
Beeson, P., & Holland, A. (1994). Telerounds#19—Aphasia groups: An approach tolong-term rehabilitation. Tucson, AZ:National Center for Neurogenic Commu-nication Disorders.
Bernstein-Ellis, E., & Elman, R. (2006). TheBook ConnectionTM: A life participationbook club for individuals with acquiredreading impairment, Manual. Oakland,CA: Aphasia Center of California. Availableat: www.aphasiacenter.org
Blackstone, S., & Berg, M. (2003). Social net-works: A communication inventory forindividuals with complex communica-tion needs and their communicationpartners. Monterey, CA: AugmentativeCommunication.
Capobianco, R., & Mahli, L. (1995, October).Senior stroke group: A model for educa-tionally based group treatment. Focus ongeriatric care and rehabilitation (pp.1–8). Frederick, MD: Aspen Publishers.
Davis, G. (1986). Pragmatics and treatment.In R. Chapey (Ed.), Language interven-tion strategies in adult aphasia (2nd ed.,pp. 251–265). Baltimore: Williams &Wilkins.
Davis, G., & Wilcox, J. (1981). Incorporatingparameters of natural conversation inaphasia treatment. In R. Chapey (Ed.),
Language intervention strategies inadult aphasia (pp. 169–193). Baltimore:Williams & Wilkins.
Elman, R. (1994, October). Aphasia treatmentplanning in an outpatient medical rehabil-itation center:Where do we go from here?In C. Coehlo (Ed.), Neurophysiology andNeurogenic Speech and Language Disor-ders Special Interest Division 2 Newslet-ter (pp. 9–13). Rockville, MD: AmericanSpeech-Language Hearing Association.
Elman, R. (1998). Memories of the ‘plateau’:Health care changes provide an opportu-nity to redefine aphasia treatment and dis-charge. Aphasiology, 12, 227–231.
Elman, R. (1999a). Practicing outside thebox. ASHA, 41(6), 38–42.
Elman, R. (1999b). Long-term careapproaches to aphasia treatment and man-agement. In R. Elman (Ed.), ASHA SpecialInterest Division 2 Newsletter: Neuro-physiology and Neurogenic Speech andLanguage Disorders, 9(5), 15–17.
Elman, R. (2000). Working with groups: Neu-rogenic communication disorders and themanaged care challenge. [Videotape.] Rock-ville, MD: American Speech-Language-Hearing Association.
Elman, R. (2001). The Internet and aphasia:Crossing the digital divide. Aphasiology,15(10/11), 895–899.
Elman, R. (2005). Social and life participationapproaches to aphasia intervention. In L.LaPointe (Ed.), Aphasia and related neuro-genic language disorders (3rd ed., pp. 39–50). New York:Thieme Medical Publishers.
Elman, R. (2006). Evidence-based practice:What evidence is missing? Aphasiology,20, 103–109.
Elman R., & Bernstein-Ellis, E. (1995). What isfunctional? American Journal of Speech-Language Pathology, 4, 115–117.
Elman, R., & Bernstein-Ellis, E. (1999a). Theefficacy of group communication treat-ment in adults having chronic aphasia:Linguistic and communicative outcomemeasures. Journal of Speech, Language,and Hearing Research, 42, 411–419.
92 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 92
Elman, R., & Bernstein-Ellis, E. (1999b). Psy-chosocial aspects of group communicationtreatment: Preliminary findings. Seminarsin Speech and Language, 20, 65–72.
Elman, R., Bernstein-Ellis, E.,Watt, S., Sobel, P.,Giuffrida, E., Fink, R., et al. (2005, Novem-ber). Reading for pleasure: Aphasia bookclubs and quality of life. Seminar pre-sented at the annual convention of theAmerican Speech-Language-Hearing Asso-ciation, San Diego, CA.
Elman, R., Ogar, J., & Elman, S. (2000). Apha-sia: Awareness, advocacy, and activism.Aphasiology, 14(5/6), 455–459.
Elman, R., Parr, S., & Moss, B. (2003). TheInternet and aphasia: Crossing the digitaldivide. In S. Parr, J. Duchan, & C. Pound(Eds.), Aphasia inside out (pp. 103–116).Buckingham, UK: Open University Press.
Ewing, S., & Pfaltzgraf, B. (1991a). Pathways:Moving beyond stroke and aphasia.[Videotape.] Novi, MI: Epcom Enterprises.
Ewing, S., & Pfalzgraf, B. (1991b). What isaphasia? [Videotape.] Novi, MI: EpcomEnterprises.
Frattali, C.,Thompson, C., Holland A.,Wohl, C.,& Ferketic, M. (1995). American Speech-Language-Hearing Association FunctionalAssessment of Communication Skills forAdults. Rockville, MD: American Speech-Language-Hearing Association.
Frattali, C. (1996, December). Measuring dis-ability. In R.Warren (Ed.), Neurophysiologyand Neurogenic Speech and Language Dis-orders Special Interest Division 2 News-letter (pp. 7–10). Rockville, MD: AmericanSpeech-Language-Hearing Association.
Frattali, C. (Ed.). (1998). Measuring outcomesin speech-language pathology. New York:Thieme Medical Publishers.
Garrett, K., & Beukelman, D. (1992). Severeaphasia. In K. Yorkston (Ed.), Augmenta-tive communication in the medical set-ting (pp. 245–321). Tucson, AZ: Commu-nication Skill Builders.
Hersh, D. (1998). Beyond the ‘plateau’: Dis-charge dilemmas in chronic aphasia.Aphasiology, 12, 207–218.
Holland, A. (1992). Some thoughts on futureneeds and directions for research andtreatment of aphasia. NIDCD Monograph,2, 147–152.
Hopper, T., Holland, A. L., & Rewega, M.(2002). Conversational coaching: Treat-ment outcomes and future directions.Aphasiology, 16, 754–761.
Jordan, L., & Kaiser, W. (1996). Aphasia:A social approach. London: Chapman &Hall.
Kagan A. (1995). Revealing the competenceof aphasic adults through conversation:A challenge to health professionals. Topicsin Stroke Rehabilitation, 2, 15–28.
Kagan, A. (1998). Supported conversation foradults with aphasia: Methods and resourcesfor training conversation partners. Aphasi-ology, 12(9), 816–830.
Kagan, A., & Gailey, G. (1993). Functional isnot enough: Training conversation part-ners for aphasic adults. In A. Holland & M.Forbes (Eds.), Aphasia treatment: Worldperspectives (pp. 199–225). San Diego,CA: Singular Publishing.
Kagan, A., Winckel, J., & Shumway, E. (1996).Pictographic communication resources.Toronto: Aphasia Institute. Available at:www.aphasia.ca
Kearns, K., & Elman, R. (2001). Group ther-apy for aphasia: Theoretical and practicalconsiderations. In R. Chapey (Ed.). Lan-guage intervention strategies in aphasiaand related neurogenic communicationdisorders (4th ed., pp. 316–337). Balti-more: Lippincott Williams & Wilkins.
Kertesz, A. (1982). Western aphasia battery.New York: Grune and Stratton.
LLPA Project Group. (2000). Life participa-tion approach to aphasia: A statement ofvalues for the future. ASHA Leader, 5,4–6. Retrieved June 27, 2006, from http://www.asha.org/public/speech/disorders/LPAA.htm
LPAA Project Group. (2001). Life participa-tion approach to aphasia: A statement ofvalues for the future. In R. Chapey (Ed.),Language intervention strategies in
APHASIA GROUP COMMUNICATION TREATMENT 93
05_Elman_71-94 9/15/06 10:39 PM Page 93
aphasia and related neurogenic commu-nication disorders (4th ed., pp. 235–245).Baltimore: Lippincott Williams & Wilkins.
Lyon, J. (1992). Communicative use and par-ticipation in life for aphasic adults in nat-ural settings: The scope of the problem.American Journal of Speech and Lan-guage Pathology, 1, 7–14.
Lyon, J. (1995). Drawing: Its value as a com-munication aid for adults with aphasia.Aphasiology, 9, 33–94.
Lyon, J. (1997). Coping with aphasia. SanDiego, CA: Singular Publishing.
Lyon, J. (2000). Finding, defining, and refiningfunctionality in real-life for people con-fronting aphasia. In L. Worrall & C. Frattali(Eds.), Neurogenic communication disor-ders:A functional approach (pp. 137–161).New York: Thieme Medical Publishers.
Lyon, J., & Shadden, B. (2001). Treating lifeconsequences of aphasia’s chronicity. InR. Chapey (Ed.), Language interventionstrategies in aphasia and related neuro-genic communication disorders (4th ed.,pp. 297–315). Baltimore: Lippincott Wil-liams & Wilkins.
Markus, H., & Nurius, P. (1986). Possibleselves. American Psychologist, 41(9),954–969.
Parr, S., Byng, S., Gilpin, S., & Ireland, S.(1997). Talking about aphasia: Livingwith loss of language after stroke. Buck-ingham, UK: Open University Press.
Pound, C., Parr, S., Lindsay, J., & Woolf, C.(2000). Beyond aphasia: Therapies for
living with communication disability.Oxon, UK: Winslow Press.
Ryff, C., & Singer, B. (1998). The contours ofpositive human health. PsychologicalInquiry, 9(1), 1–29.
Ryff, C., & Singer, B. (2000). Interpersonalflourishing: A positive health agenda forthe new millennium. Personality & SocialPsychology Review, 4 (1), 30–44.
Ryff, C., Singer, M., & Love, G. (2004). Positivehealth: Connecting well-being with biol-ogy. Philosophical Transactions of theRoyal Society: Biological Sciences, 359,1383–1394.
Sarno, M. (2004). Aphasia therapies: Histori-cal perspectives and moral imperatives. InJ. Duchan & S. Byng (Eds.), Challengingaphasia therapies: Broadening the dis-course and extending the boundaries(pp. 19–31). London: Psychology Press.
Simmons-Mackie, N. (2001). Social approachesto aphasia intervention. In R. Chapey (Ed.),Language intervention strategies inaphasia and related neurogenic commu-nication disorders (4th ed., pp. 246–268).Baltimore: Lippincott Williams & Wilkins.
Simmons-Mackie, N., & Damico, J. (1996).Accounting for handicaps in aphasia: Com-municative assessment from an authenticsocial perspective. Disability and Reha-bilitation, 18, 540–549.
World Health Organization. (2001). Interna-tional classification of functioning, dis-ability and health: ICF. Geneva, Switzer-land: Author.
94 GROUP TREATMENT OF NEUROGENIC COMMUNICATION DISORDERS
05_Elman_71-94 9/15/06 10:39 PM Page 94