Embed Size (px)
DESCRIPTION
apache
Citation preview

J
O
NpM
HMTMKa
b
a
ARRAA
KAMPS
I
sst2
tT
h0
ARTICLE IN PRESSG ModelJCC-870; No. of Pages 9
Journal of Cardiology xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Journal of Cardiology
jo ur nal home page: www.elsev ier .com/ locate / j j cc
riginal article
ew scoring system (APACHE-HF) for predicting adverse outcomes inatients with acute heart failure: Evaluation of the APACHE II andodified APACHE II scoring systems
irotake Okazaki (MD)a, Akihiro Shirakabe (MD, PhD)a,∗, Noritake Hata (MD, PhD)a,asanori Yamamoto (MD, PhD)a, Nobuaki Kobayashi (MD, PhD)a,
akuro Shinada (MD, PhD)a, Kazunori Tomita (MD)a, Masafumi Tsurumi (MD)a,asato Matsushita (MD)a, Yoshiya Yamamoto (MD)a, Shinya Yokoyama (MD, PhD)a,
uniya Asai (MD, PhD)b, Wataru Shimizu (MD, PhD, FJCC)b
Division of Intensive Care Unit, Chiba Hokusoh Hospital, Nippon Medical School, Chiba, JapanDepartment of Cardiovascular Medicine, Nippon Medical School, Tokyo, Japan
r t i c l e i n f o
rticle history:eceived 2 December 2013eceived in revised form 4 February 2014ccepted 19 February 2014vailable online xxx
eywords:cute heart failure syndromeortality
rognosiscoring
a b s t r a c t
Background: No scoring system for assessing acute heart failure (AHF) has been reported.Methods and results: Data for 824 AHF patients were analyzed. The subjects were divided into an alive(n = 750) and a dead group (n = 74). We constructed a predictive scoring system based on eight significantAPACHE II factors in the alive group [mean arterial pressure (MAP), pulse, sodium, potassium, hematocrit,creatinine, age, and Glasgow Coma Scale (GCS); giving each one point], defined as the APACHE-HF score.The patients were assigned to five groups by the APACHE-HF score [Group 1: point 0 (n = 70), Group 2:points 1 and 2 (n = 343), Group 3: points 3 and 4 (n = 294), Group 4: points 5 and 6 (n = 106), and Group5: points 7 and 8 (n = 11)]. A higher optimal balance was observed in the APACHE-HF between sensitivityand specificity [87.8%, 63.9%; area under the curve (AUC) = 0.779] at 2.5 points than in the APACHE II(47.3%, 67.3%; AUC = 0.558) at 17.5 points. The multivariate Cox regression model identified belongingto Group 5 [hazard ratio (HR): 7.764, 95% confidence interval (CI) 1.586–38.009], Group 4 (HR: 6.903,95%CI 1.940–24.568) or Group 3 (HR: 5.335, 95%CI 1.582–17.994) to be an independent predictor of
3-year mortality. The Kaplan–Meier curves revealed a poorer prognosis, including all-cause death andHF events (death, readmission-HF), in Group 5 and Group 4 than in the other groups, in Group 3 than inGroup 2 or Group 1, and in Group 2 than in Group 1.Conclusions: The new scoring system including MAP, pulse, sodium, potassium, hematocrit, creatinine,age, and GCS (APACHE-HF) can be used to predict adverse outcomes of AHF.© 2014 Published by Elsevier Ltd on behalf of Japanese College of Cardiology.
ntroduction
The Acute Physiology and Chronic Health Evaluation (APACHE)coring system was first established in 1981 to predict the progno-is in patients receiving intensive care (Fig. 1A) [1]. Subsequently,
Please cite this article in press as: Okazaki H, et al. New scoripatients with acute heart failure: Evaluation of the APACHE II
http://dx.doi.org/10.1016/j.jjcc.2014.03.002
he APACHE II, III, and IV systems were published over the past0 years [2–4].
∗ Corresponding author at: Division of Intensive Care Unit, Chiba Hokusoh Hospi-al, Nippon Medical School, 1715 Kamagari, Inzai, Chiba 270-1694, Japan.el.: +81 476 99 1111; fax: +81 476 99 1911.
E-mail address: [email protected] (A. Shirakabe).
ttp://dx.doi.org/10.1016/j.jjcc.2014.03.002914-5087/© 2014 Published by Elsevier Ltd on behalf of Japanese College of Cardiology.
The APACHE II system consists of three parts, including theacute physiology score, chronic health points, and age points.The total number of points for the three parts is calculated as theAPACHE II score. This score has been reported to be predictiveof adverse outcomes in patients requiring intensive care, suchas those with respiratory disease, severe pancreatitis, or severesepsis [5–9]. However, this scoring system involves many factors,as described above; therefore, it cannot be applied easily, andclinicians hesitate to use it in every patient.
In previous observational studies, various predictive factors for
ng system (APACHE-HF) for predicting adverse outcomes inand Modified APACHE II scoring systems. J Cardiol (2014),
detecting adverse outcomes in acute heart failure (AHF) patientshave been identified, including age [10], anemia [11], renal insuf-ficiency [12,13], poor liver function [14], high uric acid [15], highlactate [16], low cholesterol [12,16], elevated blood glucose [17],

Please cite this article in press as: Okazaki H, et al. New scoring system (APACHE-HF) for predicting adverse outcomes inpatients with acute heart failure: Evaluation of the APACHE II and Modified APACHE II scoring systems. J Cardiol (2014),http://dx.doi.org/10.1016/j.jjcc.2014.03.002
ARTICLE IN PRESSG ModelJJCC-870; No. of Pages 9
2 H. Okazaki et al. / Journal of Cardiology xxx (2014) xxx–xxx
Fig. 1. Definition of each scoring system. (A) The APACHE II scoring system was defined in this study. (B) The Modified APACHE II scoring system was constructed based on thesignificant APACHE II factors in the alive group [mean blood pressure (BP), sodium, potassium, creatinine, age, and Glasgow Coma Scale (GCS)] and was given points based onthe APACHE II system. (C) The APACHE-HF scoring system was constructed based on the significant APACHE II factors in the alive group (mean BP, pulse, sodium, potassium,creatinine, hematocrit, age, and GCS) and was given one point for each cut-off value. The cut-off value for each factor was defined by the receiver-operating characteristic(ROC) curve as follows: mean BP [91.5 mmHg, area under the ROC curve (AUC) = 0.678, p < 0.001), pulse (110.5 beats/min, AUC = 0.594, p = 0.008), sodium (137.5 mmol/L,AUC = 0.613, p = 0.001), potassium (4.85 mmol/L, AUC = 0.601, p = 0.004), hematocrit (36.95 mg/dL, AUC = 0.617, p = 0.001), creatinine (1.475 mg/dL, AUC = 0.676, p < 0.001), age(71.5 years, AUC = 0.572, p = 0.042) and GCS (13.5, AUC = 0.567, p = 0.058)].

ING ModelJ
f Card
htplro
M
S
wNwHwdoHAts(npodr
P
h(
ttssfsttpvoo
Aastp
amrtTtAaMt
ARTICLEJCC-870; No. of Pages 9
H. Okazaki et al. / Journal o
yperkalemia [12], hyponatremia [18], brain-type natriuretic pep-ide (BNP), and left ventricular ejection fraction. With respect toatients with AHF, no predictive scoring system has been estab-
ished, and evaluations of the APACHE II system have rarely beeneported. We therefore evaluated the efficacy of the APACHE II andur newly established scoring system for AHF patients.
ethods
ubjects
Clinical data were collected from 824 patients with AHF whoere admitted to the intensive care unit at Chiba Hokusoh Hospital,ippon Medical School between January 2000 and July 2012. AHFas defined as either new-onset HF or decompensation of chronicF with symptoms sufficient to warrant hospitalization [19]. HFas diagnosed according to the Framingham criteria for a clinicaliagnosis of HF based on the satisfaction of two major criteria orne major and two minor criteria [20]. All patients had a New Yorkeart Association (NYHA) functional class of either Class III or IV.HF patients with one of the following criteria were admitted to
he intensive care unit (ICU) by physician’s decision in the presenttudy: (1) patients who need high projectile oxygen inhalationincluding mechanical support) to treat orthopnea, (2) patients whoeed intrope or mechanical support with low blood pressure, (3)atients who need many types of diuretics to improve the generalr lung edema. Patients with HF caused by acute coronary syn-rome were excluded from the study. All data were retrospectivelyetrieved from hospital medical records.
rocedure
AHF patients were divided into two groups according to in-ospital mortality: the alive group (n = 750) and the dead groupn = 74).
We established two new scoring systems for AHF comparinghe two groups. First, we compared the APACHE II score betweenhe two groups using a univariate analysis. Factors associated withignificantly more points in the alive group were selected to con-truct the new scoring system. The total score of the significantactors in the alive group was defined as the Modified APACHE IIcore. Second, we compared the data for APACHE II factors betweenhe two groups using a univariate analysis. We then scored theotal number of factors specific to survival discharge (giving oneoint for each factor), defined as the APACHE-HF score. The cut-offalue for each factor to give one point was defined by the receiver-perating characteristic (ROC) curves for the in-hospital mortalityf each factor.
We determined the scores (APACHE II, Modified APACHE II, andPACHE-HF) in each patient based on data obtained at admission,ccording to a previous report [2], and evaluated the sensitivity,pecificity, and positive and negative predictive value for differen-iating the alive and dead groups. ROC curves were calculated toredict the optimal cut-off values.
Furthermore, the mid-term prognosis was evaluated in terms ofll-cause death and HF events defined as all-cause death or read-ission due to HF. The patients were clinically followed up in a
outine outpatient clinic. For the patients followed up at other insti-utes, the final prognosis was determined via telephone contact.he patients were assigned to another two groups according tohe cut-off values of the ROC curves for the APACHE II, Modified
Please cite this article in press as: Okazaki H, et al. New scoripatients with acute heart failure: Evaluation of the APACHE II
http://dx.doi.org/10.1016/j.jjcc.2014.03.002
PACHE II, and APACHE-HF scores. The survival rates were thennalyzed using Kaplan–Meier curves according to the APACHE II,odified APACHE II, and APACHE-HF scores. The prognostic value of
he APACHE-HF score in these groups compared with that observed
PRESSiology xxx (2014) xxx–xxx 3
in the group with lowest point as the referent was assessed usinga Cox regression hazard model.
Statistical analysis
All data were statistically analyzed using the SPSS 20.0J softwareprogram (SPSS Japan Institute, Tokyo, Japan). All numerical datawere expressed as the mean ± standard deviation or median (rangeor 25–75% interquartile range) depending on normality. UnpairedStudent’s t-test or the Mann–Whitney U-test was used to comparethe two groups. Normality was assessed using the Shapiro–Wilk W-test. Comparisons of all proportions were made using a chi-squareanalysis. A p-value of less than 0.05 was considered to be statisti-cally significant. ROC curves were calculated to predict the cut-offvalues, and the sensitivity, specificity and area, under the ROC curve(AUC) were determined. The survival rates were analyzed betweenthe groups assigned based on the cut-off values of the ROC curvesfor each scoring system using Kaplan–Meier curves, and significantdifferences were calculated using the log-rank test. A Cox regres-sion analysis was performed to obtain the hazard ratios (HRs) for90-day mortality and 90-day HF events. Subsequently, a multivari-ate analysis was performed using the variables with a p-value of<0.05 in the univariate analysis to examine their independent asso-ciations with 90-day mortality and 90-day HF events. A p-value ofless than 0.05 was considered to be statistically significant.
Ethical concerns
The institutional review board at Chiba Hokusoh Hospital, Nip-pon Medical School approved the study protocol.
Results
Patient characteristics
The relationship between the treatment, including respiratorysupport and medications prescribed during the first 5 days, andin-hospital mortality are shown in Table 1. The patient cohortincluded 67.2% male subjects, with a median age of 74 years.The systolic blood pressure (BP) values were significantly lower,the number of NYHA class IV patients was significantly higher,the serum hemoglobin levels were significantly lower, the serumurinary acid levels were significantly higher, the serum BUN lev-els were significantly higher, the serum C-reactive protein (CRP)levels were significantly higher, and the serum BNP levels weresignificantly higher in the dead group than in the alive group.
Definition of the Modified APACHE II and APACHE-HF scoringsystems
Regarding the APACHE II score, the following six factors weresignificantly different between the alive group and the dead group:mean BP, sodium, potassium, creatinine, age, and Glasgow ComaScale (GCS) (Table 2). We constructed a predictive scoring systembased on the significant APACHE II factors in the alive group (meanBP, sodium, potassium, creatinine, age, and GCS; giving pointsbased on the APACHE II system), defined as the Modified APACHEII score (Fig. 1B).
On the other hand, the following eight factors were sig-nificantly different between the alive group and dead group:mean BP, pulse, sodium, potassium, hematocrit, creatinine, age,and GCS (Table 3). We constructed a predictive scoring sys-
ng system (APACHE-HF) for predicting adverse outcomes inand Modified APACHE II scoring systems. J Cardiol (2014),
tem based on the significant APACHE II factors in the alivegroup (mean BP, pulse, sodium, potassium, creatinine, hemat-ocrit, age, and GCS; giving one point based on each cut-off value),defined as the APACHE-HF score (Fig. 1C). The cut-off values for

Please cite this article in press as: Okazaki H, et al. New scoring system (APACHE-HF) for predicting adverse outcomes inpatients with acute heart failure: Evaluation of the APACHE II and Modified APACHE II scoring systems. J Cardiol (2014),http://dx.doi.org/10.1016/j.jjcc.2014.03.002
ARTICLE IN PRESSG ModelJJCC-870; No. of Pages 9
4 H. Okazaki et al. / Journal of Cardiology xxx (2014) xxx–xxx
Table 1Relationships between the patient characteristics and in-hospital survival.
Characteristic Total (n = 824) Dead group (n = 74) Alive group (n = 750) p-Value
Age (years) 74 (65–80) 74 (64–80) 76 (70–81) 0.041Gender (male, %) 554 (67.2%) 44 (59.5%) 510 (68.0%) 0.153Type (new onset, %) 544 (66.0%) 43 (58.1%) 501 (66.8%) 0.157
EtiologyIschemic heart disease (yes, %) 554 (67.2%) 44 (59.5%) 510 (68.0%) 1.000Cardiomyopathy (yes, %) 141 (17.1%) 14 (18.9%) 127 (16.9%) 0.630Hypertensive heart disease (yes, %) 143 (17.4%) 7 (9.5%) 136 (18.1%) 0.076Valvular (yes, %) 117 (21.5%) 20 (27.0%) 157 (20.9%) 0.236Others (yes, %) 22 (2.7%) 2 (2.7%) 20 (2.7%) 1.000
Past medical historyHypertension (yes, %) 612 (74.3%) 47 (63.5%) 565 (75.3%) 0.036Diabetes mellitus (yes, %) 341 (41.4%) 32 (43.2%) 309 (41.2%) 0.805Dyslipidemia (yes, %) 374 (45.4%) 25 (33.8%) 349 (46.5%) 0.038
Vital signs and statusSBP (mmHg) 160 (132–186) 131 (107–168) 162 (138–188) <0.001SBP > 140 mmHg (yes, %) 559 (67.8%) 31 (41.9%) 528 (70.4%) <0.001SBP 100–140 mmHg (yes, %) 232 (28.2%) 29 (39.2%) 203 (27.1%) 0.031SBP < 100 mmHg (yes, %) 66 (8.0%) 13 (17.6%) 53 (7.1%) 0.005Diastolic blood pressure (mmHg) 90 (70–100) 80 (62–90) 90 (72–100) <0.001LVEF (%) 35.0 (25–46) 32 (22–45) 35 (24–46) 0.150LVEF > 40% (%) 295 (36.0%) 23 (31.9%) 272 (36.4%) <0.001NYHA (IV, %) 667 (80.9%) 66 (89.2%) 601 (80.1%) 0.003
Laboratory dataTotal bilirubin (mg/dL) 0.6 (0.4–0.8) 0.7 (0.4–1.0) 0.6 (0.4–0.8) 0.166Urinary acid (mg/dL) 6.8 (5.5–8.1) 7.7 (5.9–9.6) 6.7 (5.3–8.0) 0.001BUN (mg/dL) 23.2 (17.9–33.1) 36.4 (21.5–48.7) 22.7 (17.5–31.8) <0.001Hemoglobin (g/dL) 12.5 (10.7–14.5) 11.3 (10.3–14.2) 12.5 (10.8–14.5) 0.001CRP (mg/dL) 0.56 (0.19–1.78) 1.44 (0.56–4.58) 0.52 (0.17–1.63) <0.001BNP (pg/mL) 805 (415–1403) 1363 (927–1787) 753 (399–1312) <0.001
Respiratory supportEndotracheal intubation (yes, %) 209 (25.4%) 36 (48.6%) 173 (23.1%) <0.001NPPV (yes, %) 310 (37.6%) 24 (32.4%) 286 (38.1%) 0.380
Medication (cases) during the first 5 daysFurosemide (yes, %) 781 (94.8%) 66 (89.2%) 715 (95.3%) 0.047Nitroglycerin (yes, %) 594 (69.1%) 37 (50.0%) 557 (74.3%) <0.001Nicorandil (yes, %) 95 (11.5%) 11 (14.9%) 84 (11.2%) 0.341Carperitide (yes, %) 449 (54.5%) 45 (60.8%) 404 (53.9%) 0.272Dopamine (yes, %) 238 (28.9.0%) 41 (55.4%) 197 (26.3%) <0.001Dobutamine (yes, %) 117 (21.5%) 36 (48.6%) 141 (18.8%) <0.001ACE-I/ARB (yes, %) 333 (40.4%) 17 (22.9%) 316 (42.1%) 0.001�-Blocker (yes, %) 196 (23.8%) 16 (21.6%) 180 (24.0%) 0.775Spironolactone (yes, %) 296 (35.9%) 18 (24.3%) 278 (37.1%) 0.031
OutcomeICU hospitalization (days) 5 (3–7) 7 (4–17) 5 (3–7) <0.001Total hospitalization (days) 29 (18–49) 30 (13–82) 29 (18–47) 0.489
SBP, systolic blood pressure; LVEF, left ventricular ejection fraction measured on echocardiography; NYHA, New York Heart Association; BUN, blood urea nitrogen; CRP,C-reactive protein; BNP, brain natriuretic peptide; NPPV, non-invasive positive pressure ventilation; ACE-I, angiotensin-converting enzyme inhibitor ARB, angiotensin IIreceptor blocker; ICU, intensive care unit.p-Value between the alive group and dead group determined according to unpaired Student’s t-test and Mann–Whitney U-test.
Table 2Relationships between the APACHE II score and in-hospital mortality.
All (n = 825) Alive group (n = 750) Dead group (n = 75) p-Value
Total APSBody temperature (◦C) 0.39 ± 0.57 0.38 ± 0.55 0.51 ± 0.67 0.162Mean blood pressure (mmHg) 1.51 ± 1.36 1.54 ± 1.36 1.22 ± 1.33 0.036Pulse (beats/min) 1.53 ± 1.23 1.54 ± 1.22 1.39 ± 1.24 0.227Respiratory rate (per min) 1.36 ± 1.20 1.36 ± 1.19 1.38 ± 1.27 0.920A-aDO2 (FiO2 > 0.5) or PaO2 (FiO2 < 0.5) 0.91 ± 1.46 0.90 ± 1.45 1.00 ± 1.52 0.778pH 1.59 ± 1.60 1.59 ± 1.60 1.58 ± 1.51 0.985Sodium (mmol/L) 0.05 ± 0.35 0.04 ± 0.31 0.18 ± 0.60 0.001Potassium (mmol/L) 0.22 ± 0.66 0.19 ± 0.61 0.46 ± 0.91 0.021Hematocrit (%) 0.55 ± 0.90 0.54 ± 0.90 0.61 ± 0.88 0.511Creatinine (mg/dL) 0.96 ± 1.35 0.90 ± 1.32 1.61 ± 1.51 <0.001White blood cell (/m3) 0.16 ± 0.44 0.16 ± 0.44 0.14 ± 0.40 0.873
Age points 5.05 ± 1.26 5.01 ± 1.29 5.39 ± 0.90 0.027Chronic health points 0.53 ± 1.54 0.51 ± 1.52 0.68 ± 1.63 0.386Glasgow Coma Scale 0.94 ± 2.49 0.88 ± 2.40 1.59 ± 2.90 0.006
APS, acute physiology score.p-Value between the alive group and dead group determined according to Mann–Whitney U-test.

ARTICLE IN PRESSG ModelJJCC-870; No. of Pages 9
H. Okazaki et al. / Journal of Cardiology xxx (2014) xxx–xxx 5
Table 3Relationships between the APACHE II data and in-hospital mortality.
All (n = 824) Alive group (n = 750) Dead group (n = 74) p-Value
Total APSBody temperature (◦C) 36.3 (35.7–36.8) 36.2 (35.7–36.8) 36.4 (35.2–36.9) 0.750Mean blood pressure (mmHg) 112.0 (94–130) 113 (95–131) 97 (77–114) <0.001Pulse (beats/min) 114 (95–132) 116 (96–132) 105 (82–125) 0.008Respiratory rate (per min) 30 (23–35) 30 (24–35) 30 (23–35) 0.411PaO2 (mmHg) 86.7 (65.5–128.7) 85.8 (65.5–123.8) 96.1 (67.2–147.5) 0.136pH 7.32 (7.20–7.42) 7.32 (7.19–7.42) 7.21 (7.19–7.40) 0.873Sodium (mmol/L) 140 (137–142) 140 (138–142) 137 (135–141) 0.001Potassium (mmol/L) 4.3 (3.9–4.7) 4.2 (3.9–4.7) 4.4 (3.9–5.2) 0.004Hematocrit (%) 38.0 (33.2–43.7) 38.5 (33.7–44.0) 34.7 (30.7–39.7) 0.001Creatinine (mg/dL) 1.16 (0.91–1.73) 1.13 (0.89–1.67) 1.63 (1.15–2.55) <0.001White blood cell (/m3) 9775 (7600–12,653) 9795 (7645–12,668) 9625 (6890–12,353) 0.300
Age (years) 74 (65–80) 74 (64–80) 76 (70–81) 0.041Chronic health points 0 (0–0) 0 (0–0) 0 (0–0) 0.386Glasgow Coma Scale 15 (15–15) 15 (15–15) 15 (13–15) 0.006
APS, acute physiology score.p-Value between the alive group and dead group determined according to Mann–Whitne
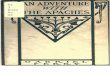
Fig. 2. ROC curves for each scoring system. The APACHE II system demonstrated anoptimal balance between sensitivity and specificity (47.3% and 67.3%; AUC = 0.588,p = 0.012) at 17.5 points (black line), while the Modified APACHE II system demon-strated an optimal balance between sensitivity and specificity (51.4% and 69.4%, AUC0.590, p = 0.001) at 9.5 points (blue line) and the APACHE-HF system demonstratedan optimal balance between sensitivity and specificity (87.8% and 63.9%, AUC 0.779,p < 0.001) at 2.5 points (red line). ROC, receiver-operating characteristic; AUC, areau
e(sA((
Ps
tsvaa(s
potassium, creatinine, hematocrit, age, and GCS, exhibited signifi-
nder the ROC curve; HF, heart failure.
ach factor were defined by ROC curves as follows: mean BP91.5 mmHg, AUC = 0.678), pulse (110.5 beats/min, AUC = 0.594),odium (137.5 mmol/L, AUC = 0.613), potassium (4.85 mmol/L,UC = 0.601), hematocrit (36.95 mg/dL, AUC = 0.617), creatinine
1.475 mg/dL, AUC = 0.676), age (71.5 years, AUC = 0.572), and GCS13.5, AUC = 0.567).
redictive value of the Modified APACHE II and APACHE-HFcoring systems
The APACHE II demonstrated an optimal balance between sensi-ivity and specificity (47.3% and 67.3%; AUC = 0.588) at 17.5 points,electing 9.5 points for the Modified APACHE II score as a cut-offalue (sensitivity 51.4%, specificity 69.4%, AUC 0.590). Meanwhile,
cut-off value of 2.5 points for the APACHE-HF score produced
Please cite this article in press as: Okazaki H, et al. New scoripatients with acute heart failure: Evaluation of the APACHE II
http://dx.doi.org/10.1016/j.jjcc.2014.03.002
n optimal balance (sensitivity 87.8%, specificity 63.9%, AUC 0.779)Fig. 2). A higher optimal balance was observed in the APACHE-HFcore than in the APACHE II or Modified APACHE II scores.
y U-test.
Based on these cut-off values, the patients were divided into lowor high groups for each scoring system. The Kaplan–Meier survivalcurves showed that the prognosis, including all-cause death, didnot differ between the patients with an APACHE II score of ≤17 andthose with an APACHE II score of ≥18. Meanwhile, the prognosiswas significantly poorer in the patients with a Modified APACHE IIscore of ≥10 than in those with a Modified APACHE II score of ≤9 andin the patients with an APACHE-HF score of ≥3 than in those withan APACHE II-HF score of ≤2 (Fig. 3A, C, and E). The Kaplan–Meiersurvival curves showed that the prognosis, including HF events, wassignificantly poorer in the patients with an APACHE II score of ≥18,a Modified APACHE II score of ≥10, and an APACHE-HF score of ≥3than in those with an APACHE II score of ≤17, a Modified APACHE IIof ≤9, and an APACHE-HF score of ≤2, respectively (Fig. 3B, D, andF).
The patients were assigned to five groups based on the APACHE-HF score [Group 1: point 0 (n = 70), Group 2: points 1 and 2 (n = 343),Group 3: points 3 and 4 (n = 294), Group 4: points 5 and 6 (n = 106)and Group 5: points 7 and 8 (n = 11)].
The multivariate Cox regression model identified belong-ing to Group 3 (HR: 7.700, 95%CI 0.935–63.421), Group 4(HR: 12.357, 95%CI 1.388–110.010), or Group 5 (HR: 18.361, 95%CI1.478–228.145) as independent predictors of 90-day mortality(Table 4). Furthermore, the multivariate Cox regression model iden-tified belonging to Group 2 (HR: 3.253, 95%CI 1.173–9.019), Group3 (HR: 5.298, 95%CI 1.842–15.238), Group 4 (HR: 6.201, 95%CI2.040–18.846), or Group 5 (HR: 9.413, 95%CI 2.432–36.436) as inde-pendent predictors of HF events during the 90-day follow-up period(Table 4). The Kaplan–Meier curves revealed a poorer prognosis,including all-cause death and HF events, in Group 5 and Group 4than in the other groups, in Group 3 than in Group 2 or Group 1,and in Group 2 than in Group 1 (Fig. 4).
Discussion
In the present study, the APACHE II scoring system did notexhibit an adequate AUC. Furthermore, the Modified APACHE IIscoring system was inadequate to predict the mid-term mortality.
The new scoring system named APACHE-HF, which compriseda combination of parameters, including mean BP, pulse, sodium,
ng system (APACHE-HF) for predicting adverse outcomes inand Modified APACHE II scoring systems. J Cardiol (2014),
cantly higher sensitivity and specificity with an adequate AUC andcould be used to predict adverse mid-term outcomes in patientswith AHF.

Please cite this article in press as: Okazaki H, et al. New scoring system (APACHE-HF) for predicting adverse outcomes inpatients with acute heart failure: Evaluation of the APACHE II and Modified APACHE II scoring systems. J Cardiol (2014),http://dx.doi.org/10.1016/j.jjcc.2014.03.002
ARTICLE IN PRESSG ModelJJCC-870; No. of Pages 9
6 H. Okazaki et al. / Journal of Cardiology xxx (2014) xxx–xxx
0.0
0.2
0.4
0.6
0.8
1.0
0 30 60 90
APACHE -HF ≤ 2 (n=413)
APACHE -HF ≥ 3 (n=411)
0.0
0.2
0.4
0.6
0.8
1.0
0 30 60 90
APACHE -HF ≤ 2 (n=413)
APACHE -HF ≥ 3 (n=411)
0.0
0.2
0.4
0.6
0.8
1.0
0 30 60 90
Modified APACH E I I ≤ 9 (n=558)
Modified APACH E I I ≥ 10 (n=266)
0.0
0.2
0.4
0.6
0.8
1.0
0 30 60 90
Modified APACH E I I ≤ 9 (n=558)
Modified APACH E I I ≥ 10 (n=266)
0.0
0.2
0.4
0.6
0.8
1.0
0 30 60 90
APACHE II ≤ 17 (n=544)
APACHE II ≥ 18 (n=280)
0.0
0.2
0.4
0.6
0.8
1.0
0 30 60 90
APACHE II ≤ 17 (n=544)
APACH E II ≥ 18 (n=280)
No. at RiskLowHigh
No. at RiskLowHigh
544280
507255
487249
466234
544280
497255
469241
439218
No. at RiskLowHigh
No. at RiskLowHigh
413411
390367
382352
387322
413411
390362
371339
359298
No. at RiskLowHigh
No. at RiskLowHigh
558266
518239
503231
487213
558266
515237
488222
463194
APACHEII
APACHE -HF
Modified A PACHE II
All cause death
All cause death
All cause d eath
HF event
HF event
HF event
days
days
days
days
days days
P<0.0 01 P<0.0 01
P<0.0 01P<0.0 01
P=0.1 51P=0.0 91
APACHEII
Modified A PACHE II
APACHE -HF
(A) (B)
(C) (D)
(F)(E)
Cum
ula�
ve e
vent
Cum
ula�
ve su
rviv
alCu
mul
a�ve
surv
ival
Cum
ula�
ve e
vent
Cum
ula�
ve e
vent
Cum
ula�
ve su
rviv
al
Fig. 3. Kaplan–Meier curves for each scoring system. (A) The prognosis, including all-cause death, did not differ between the patients with an APACHE II score of ≤17 andthose with an APACHE II score of ≥18. (B) The prognosis, including HF events, was significantly poorer in the patients with an APACHE II score of ≥18 than in those with anAPACHE II score of ≤17. (C) The prognosis, including all-cause death, was significantly poorer in the patients with a Modified APACHE II score of ≥10 than in those with aModified APACHE II score of ≤9. (D) The prognosis, including HF events, was significantly poorer in the patients with a Modified APACHE II score of ≥10 than in those witha Modified APACHE II score of ≤9. (E) The prognosis, including all-cause death, was significantly poorer in the patients with an APACHE-HF score of ≥3 than in those withan APACHE II-HF score of ≤2. (F) The prognosis, including HF events, was significantly poorer in the patients with an APACHE-HF score of ≥3 than in those with an APACHEII-HF score of ≤2. HF, heart failure.

ARTICLE IN PRESSG ModelJJCC-870; No. of Pages 9
H. Okazaki et al. / Journal of Cardiology xxx (2014) xxx–xxx 7
Table 4Cox regression analysis of the associations between 90-days cumulative mortality and events, and the clinical findings.
Univariate analysis Multivariate analysis
HR 95%CI p-Value HR 95%CI p-Value
90-days mortalityPoints of APACHE-HF score
Group 1 (point 0) 1.000 1.000Group 2 (point 1, point 2) 1.221 0.147–10.139 0.854 1.110 0.127–9.694 0.925Group 3 (point 3, point 4) 7.603 1.038–55.694 0.046 7.700 0.935–63.421 0.058Group 4 (point 5, point 6) 17.522 2.366–129.756 0.005 12.357 1.388–110.010 0.024Group 5 (point 7, point 8) 20.637 2.147–198.405 0.009 18.361 1.478–228.145 0.024
Adjusting factorsAPACHE II (per 1 point increase) 1.054 1.013–1.097 0.009 1.011 0.936–1.092 0.780Modified APACHE II (per 1 point increase) 1.120 1.061–1.183 <0.001 0.992 0.879–1.120 0.900LVEF (per 1% increase) 0.987 0.970–1.003 0.987NYHA (class IV) 2.352 1.015–5.451 0.046 2.486 0.918–6.729 0.073Total bilirubin (per 0.1 mg/dL increase) 1.011 0.997–1.026 0.120BUN (per 1.0 mg/dL increase) 1.026 1.017–1.036 <0.001 1.015 1.002–1.029 0.024Hemoglobin (per 1.0 g/dL increase) 0.861 0.786–0.945 0.002 1.107 0.974–1.258 0.118BNP (per 10 pg/mL increase) 1.002 1.001–1.003 0.007 1.001 0.999–1.003 0.269
90-days HF EventsPoints of APACHE-HF score
Group 1 (point 0) 1.000 1.000Group 2 (point 1, point 2) 4.315 1.582–11.769 0.004 3.253 1.173–9.019 0.023Group 3 (point 3, point 4) 7.047 2.597–19.125 <0.001 5.298 1.842–15.238 0.002Group 4 (point 5, point 6) 10.723 3.870–29.717 <0.001 6.201 2.040–18.846 0.001Group 5 (point 7, point 8) 14.126 4.135–48.261 <0.001 9.413 2.432–36.436 0.001
Adjusting factorsAPACHE-II (per 1 point increase) 1.032 1.011–1.053 0.002 0.983 0.946–1.021 0.371Modified APACHE II (per 1 point increase) 1.082 1.050–1.115 <0.001 1.039 0.978–1.103 0.220LVEF (per 1% increase) 0.991 0.983–0.999 0.033 0.989 0.980–0.998 0.023NYHA (class IV) 1.723 1.189–2.497 0.004 1.778 1.165–2.715 0.008Total bilirubin (per 0.1 mg/dL increase) 1.086 0.996–1.184 0.061BUN (per 1.0 mg/dL increase) 1.019 1.013–1.025 <0.001 1.013 1.005–1.020 0.001Hemoglobin (per 1.0 g/dL increase) 0.925 0.883–0.968 0.001 1.021 0.954–1.092 0.553BNP (per 10 pg/mL increase) 1.001 1.001–1.002 0.001 1.000 0.999–1.001 0.461
H ction fb
A
hsloescstbttd
trTTwftpfaihtr
R, hazard ratio; CI, confidence interval; HF, heart failure, LVEF, left ventricular ejelood urea nitrogen; CRP, C-reactive protein; BNP, brain natriuretic peptide.
PACHE II scoring system and AHF
The APACHE II scoring system was first published in 1985, and itas been demonstrated that an increased APACHE II score on admis-ion can be used to predict a worse in-hospital mortality and poorong-term prognosis in intensive care patients [2]. The availabilityf this scoring system has also been reported in the setting of bothndogenous and various surgical diseases requiring intensive care,uch as respiratory disease, abdominal sepsis, including acute pan-reatitis, trauma, and postoperative diseases [6–9]. However, thiscoring system has not been evaluated in AHF patients. Moreover,he APACHE II scoring system involves many factors and is cum-ersome to apply; therefore, clinicians tend to hesitate to calculatehe score in all patients. It is necessary to develop a scoring systemhat can be more easily and immediately applied in the emergencyepartment.
In the present study, the APACHE II scoring system was foundo have an inadequate AUC, while the Modified APACHE II sco-ing system could not be used to predict the mid-term mortality.his might be due to inadequacies in the APACHE II point system.he APACHE II scoring scale was originally developed for patientsith various diseases requiring care in the intensive care unit. In
act, the majority of patients evaluated in the original study ofhe APACHE II scoring system had non-cardiac diseases. Cardiacatients comprised only 14.7% of cases, with HF patients accountingor less than 1.5%. We therefore created a new scoring system suit-ble for HF patients based on a simple point method. This system
Please cite this article in press as: Okazaki H, et al. New scoripatients with acute heart failure: Evaluation of the APACHE II
http://dx.doi.org/10.1016/j.jjcc.2014.03.002
s defined as the APACHE-HF system, which exhibits significantlyigher sensitivity and specificity with an adequate AUC comparedo the APACHE II and Modified APACHE II systems. Based on theesults of the present study, a combination of parameters, including
raction measured on echocardiography; NYHA, New York Heart Association; BUN,
mean BP, pulse, sodium, potassium, creatinine, hematocrit, age, andGCS, may be used to predict adverse outcomes of AHF.
Predictive factors for AHF
In previous observational studies, various predictive factors fordetecting adverse outcomes in AHF patients have been identified.Among these factors, we showed the mean BP, pulse, sodium, potas-sium, creatinine, hematocrit, age, and GCS at the time of admissionto be predictive factors in AHF patients.
An age over 70 or 75 years has been reported to be associatedwith a poor prognosis [12,14]. In addition, hypotension is one of themost important determinants of the prognosis. Gheorghiade et al.reported that a systolic pressure under 120 mmHg at the time ofadmission was associated with a poor prognosis compared with asystolic pressure over 120 mmHg [10,21]. It has also been reportedthat a diastolic pressure under 100 mmHg or 90 mmHg on admis-sion is associated with poor mortality [14,22]. According to a studyof mean arterial BP, a diastolic pressure under 90 mmHg is a strongpredictor of AHF [23]. We used the pulse rate as a substitute forheart rate, which is a strong predictor of cardiovascular mortal-ity and morbidity in the general population [24]. With respect toAHF, Aaronson et al. found, in a study of 268 ambulatory patientswith advanced HF, that the resting heart rate was the best pre-dictor of an adverse outcome [25,26]. In another example, Ishiiet al. showed that a heart rate over 113 beats/min on admissionis associated with a better cardiac event-free survival rate than a
ng system (APACHE-HF) for predicting adverse outcomes inand Modified APACHE II scoring systems. J Cardiol (2014),
heart rate under 112 beats/min [27]; these findings support ourresults. Hyponatremia is the most common electrolyte abnormalityin patients with AHF. In several large clinical trials, hyponatremiawas demonstrated to predict a poor prognosis [14,20,28]. The

ARTICLE ING ModelJJCC-870; No. of Pages 9
8 H. Okazaki et al. / Journal of Card
APACHE -HF
No. at RiskGroup 1Group 2Group 3Group 4Group 5
7034329410611
65317262819
63315242728
663242718610
All cause death
HF event
days
days0.0
0.2
0.4
0.6
0.8
1.0
0 30 60 90
Group 1 Group 2
Group 3 Group 4
Group 5
0.0
0.2
0.4
0.6
0.8
1.0
0 30 60 90
Group 1 Group 2
Group 3 Group 4
Group 5
No. at RiskGroup 1Group 2Group 3Group 4Group 5
7034329410611
65306250809
62297225667
663242668610
P < 0.001
P < 0.001Cum
ula�
ve e
vent
Cum
ula�
vesu
rviv
al
Fig. 4. Kaplan–Meier curves for the APACHE-HF scoring system. (A) TheKaplan–Meier curves revealed a poorer prognosis, including all-cause death, inGroup 5 and Group 4 than in the other groups, in Group 3 than in Group 2 or Group1, and in Group 2 than in Group 1. (B) The Kaplan–Meier curves revealed a poorerpif
ptstrtuivttk
rognosis, including HF events, in Group 5 and Group 4 than in the other groups,n Group 3 than in Group 2 or Group 1, and in Group 2 than in Group 1. HF, heartailure.
resent study also demonstrated a correlation between hypona-remia and high mortality or HF events, and the cut-off value for theerum sodium level (Na 137 mmol/L.) was similar to the conven-ional definition of hyponatremia (Na < 135 mmol/L). Although theelationship between hematocrit and the prognosis of HF remainso be elucidated, anemia is a famous comorbidity of heart fail-re and has been reported to be a predictor of poor outcomes
n patients with chronic and acute HF [29]. Although most pre-
Please cite this article in press as: Okazaki H, et al. New scoripatients with acute heart failure: Evaluation of the APACHE II
http://dx.doi.org/10.1016/j.jjcc.2014.03.002
ious studies used the hemoglobin level as a marker of anemia,he present study employed hematocrit because it is a constitu-ive factor of the APACHE II score. Renal dysfunction is also wellnown to be a strong predictor of AHF, and the prognosis of AHF
PRESSiology xxx (2014) xxx–xxx
depends on the degree of renal dysfunction [30,31]. For example, inthe data from the AHEAD registry, patients with a creatinine levelof >120 mmol/L on admission had a poor prognosis [15]. In anotherreport, a serum creatinine level over 1.5 mg/dL or 2.0 mg/dL onadmission was found to be a predictor of mortality [22,23]. Becausepatients with AHF and anemia present more frequently with sig-nificant renal dysfunction, renal dysfunction as a predictor of AHFmay have relevance to anemia. No relationship between the serumpotassium level on admission and the prognosis of AHF has beenreported to date; however, this phenomenon may be explained byan association with renal dysfunction. The relationship betweenconsciousness disturbance on admission and AHF has not been ade-quately reported. Sicker AHF patients with shock and acidosis tendto exhibit consciousness disturbance on admission. The level ofconsciousness on admission is therefore a possible factor indicatingthe general condition of AHF patients.
No AHF scoring systems including these key factors for AHF havebeen previously reported; however, the development of a scoringsystem that can be applied more easily and immediately in theemergency department would be useful in the clinical setting fortreating AHF patients.
Study limitations
There are several limitations associated with the present studythat should be considered when interpreting the results. First, theoriginal APACHE II scoring system was based on the most deranged(worst) physiologic value observed during the initial 24-h timeperiod assuming that all pertinent physiologic values were avail-able. In the present study, we used vital signs and laboratory dataobtained on admission because AHF patients are in the most criti-cal condition on admission. Therefore, this system may not reflectthe worst condition of AHF patients. Second, the population evalu-ated in our study was limited to only patients admitted to the ICU,and AHF patients admitted to general wards were excluded fromthis study. However, the patients were seen by the “closed ICU” inour institute, and all physicians in “closed ICU” are cardiologists.Therefore, the majority of AHF patients were admitted to the ICU.For example, the rate of CS1, CS2, and CS 3 (67.8%, 28.1%, and 8%)patients were not different to the previous ATTEND registry withhospitalized HF (49.5%, 42.4%, and 7.9%) [32]. The patients’ selectionbias might be minimal in the present study. Third, we persisted withthe evaluation of original APACHE II, therefore, the scoring systemdid not include the widely accepted factors such as left ventricularejection fraction, NYHA class, blood urea nitrogen, hemoglobin, andBNP. Further study will be needed to evaluate these factors for thenext new scoring system.
Conclusion
The APACHE II scoring system cannot be used to adequately pre-dict the prognosis of patients with AHF. Our new scoring systemincluding mean BP, pulse, sodium, potassium, hematocrit, creati-nine, age, and GCS was found to be effective in predicting adverseoutcomes in AHF patients.
Disclosures
None declared.
ng system (APACHE-HF) for predicting adverse outcomes inand Modified APACHE II scoring systems. J Cardiol (2014),
Conflicts of interest
None declared.

ING ModelJ
f Card
A
ov
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
ARTICLEJCC-870; No. of Pages 9
H. Okazaki et al. / Journal o
cknowledgments
We are grateful to the staff of the ICU and the medical recordsffice at Chiba Hokusoh Hospital, Nippon Medical School for theiraluable assistance in collecting the medical data.
eferences
[1] Knaus WA, Zimmerman JE, Wagner DP, Draper EA, Lawrence DE. APACHE-AcutePhysiology and Chronic Health Evaluation: a physiologically based classifica-tion system. Crit Care Med 1981;9:591–7.
[2] Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity ofdisease classification system. Crit Care Med 1985;13:818–29.
[3] Knaus WA, Wagner DP, Draper EA, Zimmerman JE, Bergner M, Bastos PG, SirioCA, Murphy DJ, Lotring T, Damiano A, Harrell FE. The APACHE III prognosticsystem. Risk prediction of hospital mortality for critically ill hospitalized adults.Chest 1991;100:1619–36.
[4] Zimmerman JE, Kramer AA, McNair DS, Malila FM. Acute Physiology andChronic Health Evaluation (APACHE) IV: hospital mortality assessment fortoday’s critically ill patients. Crit Care Med 2006;34:1297–310.
[5] Jacobs S, Chang RW, Lee B. One year’s experience with the APACHE II severityof disease classification system in a general intensive care unit. Anaesthesia1987;42:738–44.
[6] Larvin M, McMahon MJ. APACHE-II score for assessment and monitoring ofacute pancreatitis. Lancet 1989;2:201–5.
[7] Del Bufalo C, Morelli A, Bassein L, Fasano L, Quarta CC, Pacilli AM, Gunella G.Severity scores in respiratory intensive care: APACHE II predicted mortalitybetter than SAPS II. Respir Care 1995;40:1042–7.
[8] Schein M. APACHE II score in abdominal sepsis. Arch Surg 1988;123:1288.[9] Goldhill DR, Sumner A. APACHE II, data accuracy and outcome prediction.
Anaesthesia 1998;53:937–43.10] Shiba N, Shimokawa H. Chronic heart failure in Japan: implications of the
CHART studies. Vasc Health Risk Manag 2008;4:103–13.11] van der Meer P, Postmus D, Ponikowski P, Cleland JG, O’Connor CM, Cotter
G, Metra M, Davison BA, Givertz MM, Mansoor GA, Teerlink JR, Massie BM,Hillege HL, Voors AA. The predictive value of short-term changes in hemoglobinconcentration in patients presenting with acute decompensated heart failure.J Am Coll Cardiol 2013;61:1973–81.
12] Spinar J, Parenica J, Vitovec J, Widimsky P, Linhart A, Fedorco M, Malek F, CihalikC, Spinarova L, Miklik R, Felsoci M, Bambuch M, Dusek L, Jarkovsky J. Base-line characteristics and hospital mortality in the Acute Heart Failure Database(AHEAD) Main registry. Crit Care 2011;15:R291.
13] Hata N, Yokoyama S, Shinada T, Kobayashi N, Shirakabe A, Tomita K, KitamuraM, Kurihara O, Takahashi Y. Acute kidney injury and outcomes in acute decom-pensated heart failure: evaluation of the RIFLE criteria in an acutely ill heartfailure population. Eur J Heart Fail 2010;12:32–7.
14] Ambrosy AP, Vaduganathan M, Huffman MD, Khan S, Kwasny MJ, Fought AJ,Maggioni AP, Swedberg K, Konstam MA, Zannad F, Gheorghiade M, EVERESTTrial Investigators. Clinical course and predictive value of liver function testsin patients hospitalized for worsening heart failure with reduced ejection frac-tion: an analysis of the EVEREST trial. Eur J Heart Fail 2012;14:302–11.
15] Malek F, Ostadal P, Parenica J, Jarkovsky J, Vitovec J, Widimsky P, Linhart A,Fedorco M, Coufal Z, Miklik R, Kruger A, Vondrakova D, Spinar J. Uric acid,allopurinol therapy, and mortality in patients with acute heart failure—resultsof the Acute HEart FAilure Database registry. J Crit Care 2012;27(737):
Please cite this article in press as: Okazaki H, et al. New scoripatients with acute heart failure: Evaluation of the APACHE II
http://dx.doi.org/10.1016/j.jjcc.2014.03.002
e11–24.16] Desmoulin F, Galinier M, Trouillet C, Berry M, Delmas C, Turkieh A, Massabuau
P, Taegtmeyer H, Smih F, Rouet P. Metabonomics analysis of plasma reveals thelactate to cholesterol ratio as an independent prognostic factor of short-termmortality in acute heart failure. PLoS ONE 2013;8:e60737.
[
PRESSiology xxx (2014) xxx–xxx 9
17] Mebazaa A, Gayat E, Lassus J, Meas T, Mueller C, Maggioni A, Peacock F, SpinarJ, Harjola VP, van Kimmenade R, Pathak A, Mueller T, Tavazzi L, Disomma S,Metra M, et al. Association between elevated blood glucose and outcome inacute heart failure: results from an international observational cohort. J AmColl Cardiol 2013;61:820–9.
18] Sato N, Gheorghiade M, Kajimoto K, Munakata R, Minami Y, Mizuno M,Aokage T, Asai K, Sakata Y, Yumino D, Mizuno K, Takano T, ATTEND Investi-gators. Hyponatremia and in-hospital mortality in patients admitted for heartfailure (from the ATTEND registry). Am J Cardiol 2013;111:1019–25.
19] Gheorghiade M, Zannad F, Sopko G, Klein L, Pina IL, Konstam MA, MassieBM, Roland E, Targum S, Collins SP, Filippatos G, Tavazzi L. Acute heart fail-ure syndromes: current state and framework for future research. Circulation2005;112:3958–68.
20] Nieminen MS, Harjola VP. Definition and epidemiology of acute heart failuresyndromes. Am J Cardiol 2005;96:5G–10G.
21] Gheorghiade M, Abraham WT, Albert NM, Greenberg BH, O’Connor CM, She L,Stough WG, Yancy CW, Young JB, Fonarow GC, OPTIMIZE-HF Investigators andCoordinators. Systolic blood pressure at admission, clinical characteristics, andoutcomes in patients hospitalized with acute heart failure. J Am Med Assoc2006;296:2217–26.
22] Moleerergpoom W, Hengrussamee K, Piyayotai D, Jintapakorn W, Sukhum P,Kunjara-Na-Ayudhya R, Suwanjutah T, Laothavorn P. Predictors of in-hospitalmortality in acute decompensated heart failure (Thai ADHERE). J Med AssocThai 2013;96:157–64.
23] Adamopoulos C, Zannad F, Fay R, Mebazaa A, Cohen-Solal A, Guize L, JuilliereY, Alla F. Ejection fraction and blood pressure are important and interactivepredictors of 4-week mortality in severe acute heart failure. Eur J Heart Fail2007;9:935–41.
24] Kannel WB, Kannel C, Paffenbarger Jr RS, Cupples LA. Heart rate and cardiovas-cular mortality: the Framingham Study. Am Heart J 1987;113:1489–94.
25] Aaronson KD, Schwartz JS, Chen TM, Wong KL, Goin JE, Mancini DM. Devel-opment and prospective validation of a clinical index to predict survival inambulatory patients referred for cardiac transplant evaluation. Circulation1997;95:2660–7.
26] Lanza GA, Fox K, Crea F. Heart rate: a risk factor for cardiac diseases and out-comes? Pathophysiology of cardiac diseases and the potential role of heart rateslowing. Adv Cardiol 2006;43:1–16.
27] Ishii S, Inomata T, Ikeda Y, Nabeta T, Iwamoto M, Watanabe I, Naruke T, Shi-nagawa H, Koitabashi T, Nishii M, Takeuchi I, Izumi T. Clinical significance ofheart rate during acute decompensated heart failure to predict left ventricu-lar reverse remodeling and prognosis in response to therapies in nonischemicdilated cardiomyopathy. Heart Vessels 2014;29:88–96.
28] Gheorghiade M, Abraham WT, Albert NM, Gattis Stough W, Greenberg BH,O’Connor CM, She L, Yancy CW, Young J, Fonarow GC, OPTIMIZE-HF Inves-tigators and Coordinators. Relationship between admission serum sodiumconcentration and clinical outcomes in patients hospitalized for heart failure:an analysis from the OPTIMIZE-HF registry. Eur Heart J 2007;28:980–8.
29] von Haehling S, Schefold JC, Hodoscek LM, Doehner W, Mannaa M, Anker SD,Lainscak M. Anaemia is an independent predictor of death in patients hospi-talized for acute heart failure. Clin Res Cardiol 2010;99:107–13.
30] Shirakabe A, Hata N, Kobayashi N, Shinada T, Tomita K, Tsurumi M, MatsushitaM, Okazaki H, Yamamoto Y, Yokoyama S, Asai K, Mizuno K. Long-term progno-stic impact after acute kidney injury in patients with acute heart failure. IntHeart J 2012;53:313–9.
31] Shirakabe A, Hata N, Kobayashi N, Shinada T, Tomita K, Tsurumi M, MatsushitaM, Okazaki H, Yamamoto Y, Yokoyama S, Asai K, Mizuno K. Prognostic impactof acute kidney injury in patients with acute decompensated heart failure. Circ
ng system (APACHE-HF) for predicting adverse outcomes inand Modified APACHE II scoring systems. J Cardiol (2014),
J 2013;77:687–96.32] Sato N, Kajimoto K, Keida T, Mizuno M, Minami Y, Yumino D, Asai K, Murai
K, Muanakata R, Aokage T, Sakata Y, Mizuno K, Takano T, TEND Investigators.Clinical features and outcome in hospitalized heart failure in Japan (from theATTEND Registry). Circ J 2013;77:944–51.









![Object Oriented Programming · strcpy(cor .name,”Cor ‘de boon’ Boonstra”); cor .sofi_no = 74365235; cor .name[8] = ‘B’; /* set the 9th index of cor.name */ taxp ->balance](https://img.pdfslide.us/doc/110x75/612a25c821562d768847824e/object-oriented-strcpycor-nameacor-ade-boona-boonstraa-cor-sofino.jpg)




![[Osprey] - [Men-At-Arms #186] - The Apaches](https://img.pdfslide.us/doc/110x75/5571f84e49795991698d1f16/osprey-men-at-arms-186-the-apaches.jpg)