Embed Size (px)
Citation preview

Aorto-iliac & femoral intervention: Japanese evidences
Osamu Iida, MD
Kansai Rosai Hospital
Amagasaki, Hyogo, Japan

Learn From SVS 2015 guideline -Aorto-Iliac lesions-
SVS Lower Extremity Guidelines Writing Group, J Vasc Surg. 2015;61:2S-41S.
Recommendation (Grade 1) Intervention for aortoiliac occlusive disease (AIOD in Pts with IC
Level of evidence
We recommend endovascular interventions as first-line revascularization therapy for most patients with common iliac artery or external iliac artery occlusive disease causing IC.
B
We recommend direct surgical reconstruction (bypass, endarterectomy) in patients with reasonable surgical risk and diffuse AIOD not amenable to an endovascular approach, after 1) one or more failed attempts at EVT, or 2) in patients with combined occlusive and aneurysmal disease.
B
We recommend the use of covered stents for treatment of AIOD in the presence of severe calcification or aneurysmal changes where the risk of rupture may be increased after unprotected dilation.
B
In all patients undergoing revascularization for AIOD, we recommend assessing the CFA. If hemodynamically significant CFA disease is present, we recommend surgical therapy (endarterectomy) as first-line treatment. In patients with iliac artery disease and involvement of the CFA, we recommend hybrid procedures combining femoral endarterectomy with iliac inflow correction.
B
Summary of SVS 2015 AIOD guideline 1) EVT-first 2) Aneurysm and sever calcification 3) CFA disease involvement

Primary patencies were not statistically different among TASCII category. (TASCII A, B, C, D; 77.8%, 78.0%, 73.3%, 80.5% at 5-year, Logrank p=0.55)
TASC D II AI lesions
Soga Y, Iida O, et al. Circ J. 2012;76:2697-704.

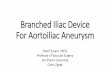
Endovascular approach for Leriche syndrome
Aodominal aorta to bilateral common iliac artery 100%⇒0% (10.0*100mm stent )

65 y/r Male, ambulatory status, life limiting claudication DM, ESRD (eGFR 36), CAD (post CABG)
AAA with severe AIOD was treated with EVAR.

Univariate model Unadjusted OR [95% CI]
Multivariate model 2 Adjusted OR [95% CI]
Age ≥ 80 y.o. 2.2 [1.5, 3.3]** 1.9 [1.3, 2.9]**
Male sex 0.8 [0.5, 1.3] ----
BMI < 18.5 kg/m2 1.2 [0.7, 2.0] ----
Diabetes mellitus 1.2 [0.8, 1.7] ----
Hypertension 1.0 [0.6, 1.6] ----
Hyperlipidemia 0.8 [0.5, 1.1] ----
Regular dialysis 1.1 [0.7, 1.7] ----
Cardiovascular disease 1.2 [0.8, 1.7] ----
Critical limb ischemia 2.8 [1.9, 4.2]** 2.3 [1.5, 3.4]**
TASC C or D 2.7 [1.9, 3.9]** 2.4 [1.6, 3.4]**
Femoral lesion 1.6 [1.1, 2.3]* ----
Below-the-knee lesion 1.9 [1.2, 3.1]** ----
Age >80 years, CLI and TASC C/D lesion were positively associated with perioperative complications (POC) after successful aorto-iliac (AI) stenting.
Iida , Soga Y, et al. Eur J Vasc Endovasc Surg. 2014;47:131-8.
-Predictors for future occurrence of POC-
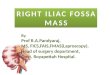
Incidence of Perioperative Complication in REAL-AI: 6.0% (126/2096)

0%
10%
20%
30%
0(n = 1085)
1(n = 677)
2(n = 207)
3(n = 43)
Occ
urr
en
ce o
f p
eri
op
era
tive
co
mp
licat
ion
s
Number of risk factors
Risk stratification for POC after AI stenting Risk factors: 1) Age ≥ 80 y.o. 2) CLI, 3) TASC C or D
Iida , Soga Y, et al. Eur J Vasc Endovasc Surg. 2014;47:131-8.

Key Findings of FP Revascularization Based on Current Guideline
-Stenting for FP lesions- ESC 2011: Primary stent implantation should be considered in femoropopliteal TASC B lesions. (IIA, level B)
AHA 2013: Primary stent placement is not recommended in the femoral, popliteal, or tibial arteries. (Level of Evidence: C)
SVS 2015: For intermediate-length lesions in the SFA, we recommend the adjunctive use of self-expanding nitinol stents (with or without paclitaxel) to improve the midterm patency of angioplasty. (Grade 1, level B)
Some practice guidelines advise against primary stenting in
patients with intermittent claudication, whereas others recommend primary stenting in short- or intermediate-length lesions or in the
event of acute PTA failure.

REtrospective multicentre AnaLysis for FemoroPopliteal stenting
Design: Retrospective multicenter Analysis Period: From Jan. 2004 to Dec. 2011 Participant: 13 Japanese cardiovascular centers Enrollment: 2742 pts (3471 limbs)
Kokura Memorial HP
Kansai Rosai HP
Hyogo College of
Medicine HP
Shin Koga HP Matsuyama Red Cross HP
Juntendo Univ.
Nerima HP
Fukuoka Red Cross HP
Kanazawa Medical
Univ. HP
Tokai Univ. HP
YamagataUniv.
School of Medicine
Saiseikai Yokohama-city
Eastern HP
Shinshu University HP
Sendai Kousei HP

Efficacy (durability) of EVT with stenting for FPD
The overall primary patencies were 90.4%, 66.9% and 63.2% at 1, 3 and 5 years,
and the secondary patencies were 90.4%, 87.3% and 86.2% at 1, 3 and 5 years
Soga Y, Iida O, et al. J Vasc Surg. 2011;54:1058-66.
5 years
Primary patency: 63.2%, Secondary patency: 86.2%

Four year follow-up angiography
Stent fracture is risk for adverse event in chronic phase -Pseudo aneurysm and surgical conversion-

Stent fracture is risk for adverse event in chronic phase -Distal embolization with vessel occlusion-

Classification and clinical impact of restenosis after femoropopliteal stenting
Variables Univariate Analysis Multivariate Analysis
HR (95% CI) p Value HR (95% CI) p Value
ISR class III 2.90 (1.83–4.56) < 0.01 2.44 (1.33–4.48) < 0.01
Lesion length 1.004 (1.002–1.007) < 0.01 1.001 (0.998–1.005) 0.50
Reference vessel diameter 0.62 (0.44–0.87) < 0.01 0.63 (0.44–0.89) < 0.01
Early restenosis 1.92 (1.13–3.23) 0.02 1.60 (0.94–2.73) 0.09
Study subjects: 116 patients (133 limbs) Lesion length: 91.4 ± 67.1 mm RVD: 5.4 ± 0.7 mm
Class I Focal ISR group
( ≤ 50 mm in length)
Class II Diffuse ISR group
( > 50 mm in length)
Class III Totally occluded
ISR group
Predictors of Recurrent ISR
Visual estimate on angiography
Class I: 29% Class II: 38% Class III: 33%
Tosaka A, Soga Y, Iida O, et al. J Am Coll Cardiol. 2012;59:16–23.

Classification and clinical impact of restenosis after femoropopliteal stenting
Conclusion: Although balloon angioplasty for the stenotic ISR group is feasible, the freedom from recurrent ISR and occlusion after balloon angioplasty are remarkable low for totally occluded ISR.
Class III Totally occluded
ISR group
Tosaka A, Soga Y, Iida O, et al. J Am Coll Cardiol. 2012;59:16–23.

Cumulative 5-year rate of in-stent occlusion in 2447 limbs after FP stenting with nitinol stents
in-stent occlusion(ISR class III) rate 5.2%@1 year
11.2%@3 years 16.4%@5 years
Class III Totally occluded
ISR group
Dohi T, Iida O, et al. J Vasc Surg 2014;59:1009-15.

HR (95% CI) Unadjusted Adjusted HR (95% CI)
Female 1.91 (1.45-2.53) 1.61 (1.21-2.15)
Age-years 1.00 (0.99-1.02)
Non-ambulatory 1.38 (0.89-2.14)
Diabetes 0.78 (0.59-1.03)
Hemodialysis 0.91 (0.64-1.29)
CLI 1.76 (1.31-2.37) 1.50 (1.11-2.04)
TASC C/D 3.46 (2.50-4.78) 3.30 (2.38-4.56)
Aspirin 0.90 (0.59-1.37) 0.96 (0.63-1.47)
Thienopyridine 0.93 (0.74-1.31) 0.94 (0.70-1.25)
Warfarin 0.82 (0.50-1.36) 0.82 (0.50-1.35)
Ref. vessel diameter 0.78 (0.66-0.93) 0.89 (0.74-1.07)
Stent size used 0.78 (0.66-0.92) 0.85 (0.71-1.02)
-Predictors of in-stent occlusion-
Dohi T, Iida O, et al. J Vasc Surg 2014;59:1009-15.
Cumulative 5-year rate of in-stent occlusion in 2447 limbs after FP stenting with nitinol stents

In-stent occlusion case assessed by angioscopy
In-stent occlusion
Ostium Neointimal
proliferation
Inside Amount of red Soft thrombus

Case: 80-YO, Male Zilver PTX DES for ISR Class II (Pre, Post, 1 Year Angiogram)
Lt-SFA: 90% (ISR) →0% (Zilver PTX 7×120 mm 3 stents)
Pre Post 1 year after EVT

Primary patency@2-year Primary DES: 74.8% PTA with provisional BMS: 57.3% Optimal PTA: 53.4% PTA: 26.5%
Sustained safety and effectiveness of PES for FP lesions; 2-year follow-up
Dake MD, et al. J Am Coll Cardiol 2013;61:2417-2487.

ZilvEr PTX for tHe Femoral ArterY and Proximal Popliteal ArteRy. -Prospective multicenter registry-
Study design Subjects
Prospective, multicenter registry PAD with femoro-popliteal lesion
*ISR lesion was also included
Primary endpoint
Primary patency
Incidence of stent thrombosis
Procedure
Initial: IVUS was mandatory for assessing vessel diameter.
12 months: angiography for assessing restenosis was mandatory.
Iida O, et al. JACC Cardiovasc Interv. 2015;8:1105-12.

Lesion characteristics (n = 831)
Pre-treatment % stenosis 90 ± 15 Chronic total occlusion 378 (45%) Restenosis 198 (24%) In-stent restenosis 124 (15%) Lesion length, cm 17 ± 10 Distal vessel diameter, mm 5.2 ± 1.0 Calcification 541 (65%) No below-the-knee run-off vessel 56 (7%) IVUS-evaluated distal EEM area, mm2 (n = 583) 28 ± 10
Post-treatment % stenosis after stent implantation 4 ± 9 IVUS-evaluated MSA, mm2 (n = 597) 15 ± 4
Lower limb characteristics (n = 797)
Critical limb ischemia 255 (32%) TASC C/D lesions 467 (58%)
Iida O, et al. JACC Cardiovasc Interv. 2015;8:1105-12.

0%
10%
20%
30%
40%
50%
MALE Restenosis
1-y
ear
inci
de
nce
rat
e
One-year incidence of restenosis was estimated to be 37%, while 1-year MALE was observed in 22%, indicating that MALE accounted for 58% in lesions with restenosis.
One-year incidence of restenosis and MALE
Iida O, et al. JACC Cardiovasc Interv. 2015;8:1105-12.

1-year restenosis rate was as low as 15% in cases with none of these risk factors, whereas it reached 51% in those with ≥ 2 risk factors
1) lesion length ≥ 16 cm
2) EEM area ≤ 27 mm2
3) MSA ≤ 12 mm2
0%
10%
20%
30%
40%
50%
60%
0(n = 146)
1(n = 192)
2-3(n = 231)
1-y
ear
inci
de
nce
Number of risk factors
MALE RestenosisRisk factors for restenosis
No. of risk factors & restenosis/MALE incidence
Iida O, et al. JACC Cardiovasc Interv. 2015;8:1105-12.

0%
1%
2%
3%
1 3 6 12
Cu
mu
lati
ve in
cid
en
ce o
f
ste
nt
thro
mb
osi
s
Follow-up period (months)
Cumulative incidence of stent thrombosis increased linearly over time during the follow-up, and reached almost 2% at 12 months.
Cumulative incidence of stent thrombosis in cases keeping at least 1 antiplatelet agents during the follow-up period
Iida O, et al. JACC Cardiovasc Interv. 2015;8:1105-12.

The interruption of antiplatelet agents during the follow-up was significantly associated with an increased ST risk.
0,1
1
10
100
3 agents 2 agents 1 agent No agent
Haz
ard
rat
io f
or
ste
nt
thro
mb
osi
s
Number of antiplatelet agents
No. of antiplatelet agents & stent thrombosis
Iida O, et al. JACC Cardiovasc Interv. 2015;8:1105-12.

Femoropopliteal ISR following DES
-Is there any difference ?-

Distribution of DES-ISR at 12 months
Class I (Focal)
Class II (Diffuse)
Class III (Occlusive)
Iida O, et al. JACC Cardiovasc Interv. 2015;8:1105-1112. Tosaka A, Soga Y, Iida O, et al. J Am Coll Cardiol. 2012;59:16–23.
Armstrong EJ, et al. Catheter Cardiovasc Interv. 2013;82:1168-74.
Class I (Focal)
29%
Class II (Diffuse)
38%
Class III (Occlusive)
33%
Class I (Focal)
38%
Class II (Diffuse)
29%
Class III (Occlusive)
33%
BMS Tosaka A
JACC 2012
BMS Armstrong EJ
CCI 2013

DES-ISR characteristics (vs. no-restenosis case)
Patent (n = 393)
Class I (focal)
(n = 106)
Class II (Diffuse) (n = 52)
Class III (occlusive)
(n = 52) P value
Age (years) 73±8 73±9 73±8 72±10 0.733
Male sex 283 (72%) 76 (72%) 33 (63%) 32 (62%) 0.292
Diabetes mellitus 258 (66%) 81 (76%) 36 (69%) 32 (62%) 0.147
Regular dialysis 96 (24%) 34 (32%) 19 (37%) 11 (21%) 0.111
Smoking 74 (19%) 24 (23%) 13 (25%) 14 (27%) 0.409
Critical limb ischemia 106 (27%) 26 (25%) 13 (25%) 14 (27%) 0.957
de novo Post-PTA restenosis In-stent restenosis
303 (77%) 34 (9%)
56 (14%)
75 (71%) 13 (12%) 18 (17%)
42 (81%) 6 (11%) 4 (8%)
32 (62%) 7 (13%) 13 (25%)
0.138
Calcification 232 (59%) 67 (63%) 37 (71%) 28 (54%) 0.251
Chronic total occlusion
163 (41%) 44 (42%) 28 (54%) 35
(67%)* 0.002
Lesion length (cm) 15±10 17±9 20±10* 19±10* 0.001
EEM area (mm2) 30±10 27±10* 25±8* 22±5* < 0.001
MSA (mm2) 16±4 14±4* 13±4* 13±3* < 0.001

One-year incidence of restenosis and MALE after re-EVT for in-DES restenotic lesion
0%
20%
40%
60%
80%
100%
Patentat 1 year
Re-EVT forClass I
Re-EVT forClass II
Re-EVT forClass III
Inci
de
nce
rat
e a
t ad
dit
ion
al o
ne
ye
ar Restenosis MALE

Take-Home Messages
Long-term outcomes after stent implantation for AI-disease are safe and durable in cases with TASC A-D lesions.
The ZEPHYR registry demonstrated real-world 1-year outcomes after Zilver-PTX implantation for FP lesions, including challenging cases. Lesion length, distal EEM area and MSA were independent predictors for restenosis.
Characteristics including CTO and EEM area at DES implantation were significantly associated with restenotic status one year after DES implantation.
One-year prognosis after re-EVT for DES-ISR lesions was suboptimal.

Thank you for your attention !

Aorto-iliac & femoral intervention: Japanese evidences
Osamu Iida, MD
Kansai Rosai Hospital
Amagasaki, Hyogo, Japan