PowerPoint Presentation
Aortic Pathology Angioclub CaseAlex Copelan M.D.William Beaumont
HospitalOctober 24, 2013Chief Complaint And History Of Present
IllnessCC: Pain between shoulder bladesHPI: 60 year-old male
transferred from outside hospitals Emergency Department after
awakening earlier in morning with the sudden onset of severe
piercing back pain radiating to his chest. He had never experienced
similar pain. Pain was non-positional and unrelenting. He denied
associated shortness of breath, syncope or pre-syncope, nausea or
vomiting, and numbness or weakness. He denied illicit drug use.
2Other Relevant HistoryPast Medical History: Hypertension,
Diabetes, Obesity, Atrial FibrillationPast Surgical History: None
relevantSocial History: 40-year pack per day smoker, chronic
alcoholism, no illicit drugsFamily History: Hypertension (both
parents)Medications: Carvedilol, Aspirin (325 mg/day),
MetforminAllergies: None
Non-Invasive Imaging
Widened Mediastinum
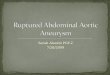
Non-Contrast-Enhanced CT: Regions containing fresher blood (blue
arrow) are more radiodense than regions containing older blood (red
arrow) and this may provide insight as to the initial sight of
hemorrhage. This is known as the sentinel clot sign. There was no
hemorrhage extension into the pericardium as demonstrated by the
low attenuation of the pericardial fluid (yellow arrow)21 HU40 HU69
HUNon-Invasive Imaging
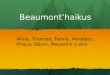
Contrast-enhanced CT: Eight cm saccular aneurysm (yellow arrow)
in the distal aortic arch is identified.
Site of aneurysmal rupture is evident as focal out-pouching of
contrast (blue arrow)
Focal hemorrhage identified just anterior to the diverticulum of
Kommerell (red arrow)
Mediastinal hematoma is evident (green arrow)
Note the right-sided aortic arch with order of branching
vessels: left carotid, right carotid, right subclavian, left
subclavian (white arrow) with diverticulum of Kommerell.Diagnosis
And Panel DiscussionDiagnosis: Ruptured thoracic aortic aneurysm,
right-sided aortic arch with aberrant left subclavian
arteryTreatment OptionsTotal Aortic Arch RepairGold Standard but
requires cardiopulmonary bypass, complex circulation management and
significant morbidityThoracic EndoVascular Aortic Repair
(TEVAR)When implemented alone, mainly utilized for unbranched
segment of aorta between left subclavian and celiac arteriesHybrid
Aortic Arch RepairIncludes ascending aorta-based debranching or
cervical extra-anatomical bypasses followed by stent-graftingCan be
performed in higher-risk patients but not suitable in patients
requiring cardiopulmonary bypass or in those with Type A
dissections, and it is an extra-anatomical repairPotential
Complications of InterventionTotal Aortic Arch Repair (compared to
hybrid procedure) Requires cardiopulmonary bypass and circulatory
arrest whereas hybrid procedure does not Increased operative
timeIncreased blood lossLonger hospital stayEndovascular Stent
GraftingMust have sufficient proximal landing zones to avoid
blockage of left or right common carotid artery and potential
strokeHybrid ProcedureAvoids cardiopulmonary bypass and circulatory
arrest but still has associated complicationsRenal impairment,
respiratory failure, paraplegia, stroke, embolism, endoleak, and
femoral access site complicationsInterventionHybrid Procedure:
Aortic arch debranching using Dacron branched graft and
endovascular stent graftingMedian sternotomy and exposure of aorta
and great vessels10 mm straight Dacron graft was anastomosed to the
body of a 16 mm x 8 mm bifurcated graft16 mm portion of the graft
was anastomosed end-to-side to the ascending aortaOne limb of the
graft was left long and anastomosed end-to-end to the right common
carotid arterySecond limb of the graft was anastomosed end-to-side
to the subclavian arteryThird limb of the trifurcated graft did not
lie smoothly, therefore, a section of this was divided and
anastomosed end-to-end to the left common carotid and then
re-anastomosed to the main graftIntervention
Thoracic Aortography:Debranching and graft placement in the
proximal ascending aorta (white arrow) allows for a sufficient
landing zone for stent graft to repair the diseased aorta without
threatening cerebral blood flowCalibrated pigtail catheter (blue
arrow) placed in ascending aorta through right femoral approach and
utilized in order to select appropriate stent sizeLeft subclavian
(green arrow), left carotid (purple arrow), right carotid (red
arrow), and right subclavian (yellow arrow) InterventionLunderquist
wire was placed through left femoral approachIntroducer for
endovascular prostheses was placed over Lunderquist wireDistally, a
40 x 15 Gore endovascular prosthesis was placed and then through
this proximally a 45 x 20 endovascular prosthesis was placedBalloon
angioplasty (yellow arrow) of stent grafts was performedPigtail
catheter was re-advanced into ascending aorta and angiography was
again performed and demonstrated patent flow (red arrow) through
the grafted vessels without evidence of endoleak
Summary
-60 year-old male presented with piercing back pain radiating to
his chest
-Non-invasive imaging demonstrated a ruptured thoracic aortic
aneurysm and right-sided aortic arch with aberrant left subclavian
artery
-Treatment options included total aortic arch repair, TEVAR, and
hybrid procedure
-Patient was ultimately deemed best suited for hybrid procedure
consisting of aortic debranching utilizing Dacron branched graft
and endovascular stent grafting