Embed Size (px)
Citation preview

“You Can Observe a Lot By Just Watching”
Wayne J. Morgan, MD, CM

Disclosures
• Genentech
– Epidemiological Study of Cystic Fibrosis, Scientific Advisory Group
• CF Foundation
– Data Safety Monitoring Board
– Registry/Comparative Effectiveness Research Committee

What is the CF Foundation
Patient Registry?

How has the CFF Patient Registry grown?
Knapp et al. Ann Am Thorac Soc 13:1173-1179, 2016.

The CFF Patient Registry Today
Inclusion criteria• Seen at CF care center• Consent to participate
Data collected at• Diagnosis• Clinic Visits• Hospitalizations / Home
IV treatments• Annually
Download a copy at CFF.org/InsightCF.

Where are CF Foundation-accredited care programs?

~34,500100%
~31,00090%
28,98384%
Who is followed in the Registry?Based on birth rates and CFTR allele prevalence, it is estimated
that there are about 34,500 persons with CF in the United States
6% do not consent toparticipate in Registry
Followed at US CF Care Centers
Followed in theCF Foundation Patient Registry
in 2015

How complete are Registry data?
95+%
90-<95%
80-<90%
FTR mutation (94%)
(90%)
Date of Birth
Sex
Race
Hispanic origin
FEV1
Weight
Height
Respiratory Cultures
Knapp et al. Ann Am Thorac Soc 13:1173-1179, 2016.

How accurate are Registry data?
95+%
90-<95%
80-<90%
Knapp et al. Ann Am Thorac Soc 13:1173-1179, 2016.
Demographic variables
Hospitalizations
Anthropometric measures
Respiratory cultures
Medications

Medical data accuracy
95+%
90-<95%
80-<90%
Knapp et al. Ann Am Thorac Soc 13:1173-1179, 2016.
Pancreatic enzymes (99%)Dornase alfa (94%)
Azithromycin (90%)Hypertonic saline
Inhaled tobramycin
Inhaled aztreonam
(89%)
(83%)
(83%)

Modified from Cystic Fibrosis Data Network http://www.cysticfibrosisdata.org/

Where are we now?

Survival for people with CF
12-year
improvement
8-year
improvement
Annual Data Report 2015, CF Foundation Patient Registry

Life expectancy by age
Annual Data Report 2015, CF Foundation Patient Registry

-3% 0% 3% 6%
B. cepacia complex
A. xylosoxidans
S. maltophilia
MRSA
P. aeruginosa
H. influenzae
S. aureus
Infection prevalence by age and over time
Salsgiver et al. Chest 149(2): 390-400, 2016.
Cross-sectional Prevalence, 2015
People
with
CF
Prevalence Change, 2006-2012
Patients
Annual Data Report 2015, CF Foundation Patient Registry

What is the CF Treatment Burden?
Annual Data Report 2015, CF Foundation Patient Registry
of people with CF take all three
inhaled medications
Chest Physiotherapy


Changing demographics: Adults with CF
CDC. Behavioral Risk Factor Surveillance System Survey Data, 2015Annual Data Report 2014, CF Foundation Patient Registry
ADULTS
CHILDREN
4,392 Adults 14,955 Adults >100 Adult CF Programs

What have we learned about CF and its care?

0
5
10
15
20
CFF Patient Registry data use
Publications
Year

What factors impact survival?
Liou et al. Am J Epidemiol. 2001 Feb 15;153(4): 345-52.
-50 -40 -30 -20 -10 0 10 20
Pulmonary Exacerbation
B. cepacia
S. aureus
CF-Related Diabetes
Weight-for-Age z-Score
Pancreatic Sufficiency
Age (5 years)
Female vs. Male
FEV1 % Predicted Equivalence
S. aureus
B. cepacia

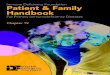
How do CFTR genotypes affect phenotypes?
Adapted from http://www.umd.be/CFTR/W_CFTR/gene.html
Cl -Cl -Cl -
Cl -
Cl - Cl -
Unaffected Class I
synthesis
Class II
maturation
XX
X
Class III
regulation
Class IV
conductance
X
Cl -Cl -
X
Cl -Cl -
Class V
quantity
‘severe’ mutations ‘mild’ mutations

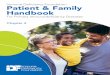
How do CFTR genotypes affect phenotypes?
McKone et al. Lancet. 2003 May 17;361(9370):1671-6.
Cl -Cl -Cl -
Cl -
Cl - Cl -
Unaffected Class I
synthesis
Class II
maturation
XX
X
Class III
regulation
Class IV
conductance
X
Cl -Cl -
X
Cl -Cl -
Class V
quantity
Age at Diagnosis (yrs) 2.6 12.0
FEV1 % Predicted 78 93
Pancreatic Insufficient (%) 92 70
P. aeruginosa (%) 59 43
Mortality Rate (per 1000) 20.4 21.2 16.0 7.8 9.1

Contributors to phenotype
Cutting et al, Nat Rev Genet. 2015 January; 16(1): 45-56

90
94
98
102
106
FEV1 % Predictedat 6 Years
Age (years) when First Reached 50th WFA Percentile
What are the pulmonary impacts of early life nutrition?
80
85
90
95
100
105
FEV1 % Predictedat 6 Years
Weight-for-Age Percentile at 3 Years
Weight-for-Age (WFA) at 3 Years
and FEV1 at 6 Years
Age when First Reached 50th WFA Percentile
and FEV1 at age 6
Sanders et al. J Pediatr 2015;167:1081-8.Konstan MW et al. J Pediatr 2003;142(6):624-30.

What do we know about lung function decline?
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
Mean FEV1
Rate of Change (%pred/yr)
Age Group (Years)
Rate of FEV1 Decline by Age
Konstan et al. J Pediatr 2007;151:134-9 Dasenbrook et al. Poster 489. NACFC 2015
Predictors of Decline
Female Sex
Low BMI Percentile
Crackles
P. aeruginosa infection
S. aureus Infection
B. cepacia complex Infection
Prior Pulmonary Exacerbations
FEV1 ≥100% Predicted
FEV1 Variability
Konstan et al. J Pediatr 2007;151:134-9Cogen et al. Pediatr Pulmonol. 2015 Aug;50(8):763-70Waters et al. Eur Respir J. 2012 Jul;40(1):61-6.Morgan et al. J Pediatr. 2016 Feb;169:116-21
Pancreatic Sufficiency
Wheezing
F508del Heterozygote Genotype
Diagnosis by Newborn Screening
slower
faster

Sanders DB et al. Am J Respir Crit Care Med 2010; 182:627-632.
Exacerbation
BaselineBest in prior
6 months
What are the long-term implications ofpulmonary exacerbations for lung function decline?
75%
≥90% recovery
≥90% Recovery
81% 85%
≥90% Recovery
15% of patients failed to recover
90% of their Baseline FEV1

What predicts pulmonary exacerbations?
IV-Treated
Exacerbations in
the Prior Year
-1.1% predicted
per year
-1.8% predicted
per year
Median Days to Next Exacerbation (with 95% CI)
Past IV-Treated Exacerbations are the Strongest Predictor
of Future ExacerbationsMean Rate of
FEV1 Loss
Waters et al. Eur Respir J. 2012;40(1):61-6VanDevanter et al. J Cyst Fibros 2016;15;372-379

IV Treatment after ≥10% Acute FEV1 Decline
Morgan et al. J Peds. 2013;163(4):1152-7
Odds of IV Treatment Highest vs Lowest
FEV1 Deciles: 0.15 (95% CI 0.12, 0.20)
Patients Treated
FEV1 %
Predicted
Decile
>50%
<25%
It's like déjà vu all over again
Personal communication, J Ostrenga - CFFPR 2015

Can we evaluate the effectiveness of treatment?

Efficacy (clinical trials) ≠ Effectiveness (real world)
Clinical Trials
• Design optimized to demonstrate safety and efficacy may limit generalizability– Disease stage
– Co-morbidities
– Problematic respiratory infection
– Poor follow up
• Frequent visits with careful follow-up
• Standardization of management and outcome measures
• Attention to adherence
Real World
• All who may benefit often including those excluded from trial and/or off-label use
• Less frequent visits and follow-up
• Less standardization of management and outcome measures
• Longer duration of therapy
• Less attention to adherence

Confounding by indication:sicker patients receive more treatments
increased
mortality
reduced
mortality
Inhaled tobramycin (unadjusted)a
Inhaled tobramycin (adjusted)a
Inhaled tobramycin (adjusted)b
a- Rothman and Wentworth. Epidemiology. 2003;14(1): 55-9 b- Sawicki et al. Ped Pulm 2012; 47:44-52.
Effect of Inhaled Tobramycin on Survival2.8
1.2
0.79

Effectiveness of dornase alfa
70
75
80
85
90
Baseline 6 Months 12 Months
FEV1 % Predicted
After adjustment for cohort differences,
there was a mean 4.3% increase in FEV1 for patients treated with dornase alfa
Johnson et al. J Peds. 1999; 134(6); 734-9
Comparator Patients
Dornase alfa Patients

CFTR modulator effectivenessIndividuals from CFTR modulator clinical trials compared to
matched F508del homozygote Registry controls
Sawicki et al. Am J Respir Crit Care Med. 2015;192(7):836-842.
Konstan et al. NACFC 2016, Poster 180.Bessonova et al. NACFC 2016, Poster 494.

Was treatment with chronic macrolides increasing NTM risk?
Binder et al. Am J Respir Crit Care Med. 2013;188(7):807-12.
37% of CFFPR patients with new NTM in 2011
received chronic macrolides in 2010
51% of CFFPR patients without NTM in 2011
received chronic macrolides in 2010
Historical macrolide use was associated with a decreased risk of NTM isolation

Putting it all together…genetic
defect
survival
Modified from Liou, 2016
malnutrition
liver
disease
pancreatic
insufficiency
liver
transplant airway
infectionabnormal
secretions
height, weight
inflammation
sinusitis
transplantinfertility
lung
function
exacerbations
sex, age diabetes

How does the Registry support care teams?

CFFPR Center-Specific Report
Annual Center-specific reports

CFFPR Center-Specific Report
Annual Center-specific reports


VCU Quality
Improvement Program
How Registry data can drive quality:One program’s story….
75
80
85
90
95
100
105
2009 2010 2011 2012 2013 2014 2015
Median FEV1
% Predicted
Virginia Commonwealth University Pediatric Program
National Average
Ten Best Performing Centers
Schechter et al. Poster 546. NACFC 2016Year

How have we partnered to create change?
• Quality improvement and leadership development
• Care center peer-review accreditation process
• Evidence-based clinical practice guidelines
• Benchmarking to learn from best practice
• Engaging people with CF and their families

What comes next?

More to do…
• Continue using Registry to improve care and learn more about CF as a disease and its treatments
• Increase value of Registry at point of care
• Recognizing limitations
– Some important questions can only be answered by clinical trials
– Integrating other data sources to enhance Registry
• Abstract 482: Linking Transplant and CFFPR Registries
• Inviting CF community to participate in asking research questions

Acknowledgments
• Patients and their families
• CF data coordinators and CF Center care teams
• CF Foundation leadership
• Registry committee (Chairs C. Goss and E. Dasenbrook)
• Clinicians and researchers who use Registry and other data to
improve understanding of CF and patient care
• Registry team at CF Foundation• Bruce Marshall
• Alex Elbert, Kris Petren, Samar Rizvi, Shathiya Kesevan, Tom O’Neil
• Aliza Fink, Josh Ostrenga, Deena Loeffler, Victoria Danner
• Ase Sewall

www.CNN.com

To learn more and submit your research
questions, visit CFF.org/InsightCF.