Embed Size (px)
Citation preview

!!
!
“REPTILE MEDICINE AND SURGERY” by Douglas R. Mader

!
!!!

!

22 Veterinary Times
KATHRYN CHAPPELL graduated from the University of Bristol in 2007, has worked in animal rescue and rehoming, and spent the past year running the veterinary unit at the National Animal Welfare Trust (London and Home Counties). Her main areas of interest are behaviour, welfare, stray animal rehabilitation and intensive care nursing.
value on human contact and displayed frenzied attention-seeking behaviours towards staff. Initially, these dogs seemed to benefit from attention. How-ever, it can increase their frus-tration, and separation anxiety develops in a high proportion of kennelled dogs (Figure 2).
Extreme displacement and stereotypical activities are regu-larly seen as a consequence of approach-avoidance conflict and boredom in barren environ-ments. These behaviours are indicative of a period of sig-nificantly compromised welfare and, once established, often continue for many years after the period of poor welfare, and can last for life.
Previous studies suggest that stereotypical behaviours may lower cortisol, and help an ani-mal cope with its situation. If generalisations are to be made from this study, three main types of reactions to kennelling were seen: dogs that would settle down and try to accept the situation; dogs that became very
active and would pace, weave, jump, circle and perimeter-run, frequently accompanied by a kind of psychogenic polydipsia; and dogs that were highly fear-ful in kennels. The latter would refrain from eating, drinking, uri-nating and defecating for as long as possible, “freezing” rigidly for long periods of time, and avoid-ing eye contact (Figure 3).
Behaviour data did not well represent the stress of these inactive dogs. The study did not show the extent of stress caused by aggression between dogs in neighbouring or opposite ken-nels (Figure 4).
ConclusionDespite the variety of sex, age, breed and individual past experience, the study showed significant qualitative evidence of physical changes that were indicative of poor welfare and chronic stress.
Addit ional detai ls of this study’s behavioural aspects are provided in the article’s forth-coming second part.
AcknowledgementsI would like to express my appre-ciation to the following for their advice and support during this study: John Bradshaw, Emily Blackwell, Rachel Casey, the University of Bristol’s depart-ment of clinical veterinary sci-ence, and the RSPCA Bristol Dogs and Cats Home. ■
■ REAL COST OF KENNELLING DOGS – from page 21
THIS interesting case high-lights the challenges of treat-ing this exotic species.
The inland bearded dragon (Pogona vitticeps), also known as the central bearded dragon, is a species of agamid lizard that is native to the semi-arid wood-land, arid woodland and rocky desert regions of Australia.
They are commonly kept as pets and exhibited in zoos. Their life span can be up to 12 years and they typically weigh up to 500g at adult size.
PresentationAn eight-year-old male inland bearded dragon presented with a three-month history of decreased appetite (with selec-tive feeding of soft fruit and mealworms), 10 per cent loss in body weight, and mandibu-lar swelling. The diet offered also included crickets and vegeta-bles (Table 1).
The lizard was housed alone in a medium-sized vivarium meas-uring approximately 45cm× 76cm×60cm. Temperatures in the vivarium ranged from 35 to 40ºC in the hot spot during
the day, reducing to 25 to 27ºC during the night. The humid-ity ranged between 30 and 40 per cent. A broad-spectrum 100W ultraviolet light provided a 12-hour photoperiod.
On clinical examination, the bearded dragon was alert, but in thin body condition with promi-nent pelvic bones and a body-weight of 380g.
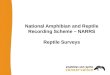
Oral examination revealed bilateral mandibular swelling, moderate erythema and severe gingival recession with pocketing in the caudal third of the mandi-bles (Figure 1).
Calculus deposition and puru-lent material were found on the mandibular and maxillary arcade, primarily on the exposed bone and in the mandibular pockets.
No other abnormalities were found on examination.
Further diagnostics and treatmentA blood sample was obtained from the ventral coccygeal vein using aseptic venipuncture. Con-scious dorsoventral and hori-zontal lateral radiography of the skull were performed (Figures 2 and 3). Radiography, haem-atology and biochemistry were all unremarkable.
A diagnosis was made of severe bilateral periodontal dis-ease, primarily involving the mandibular dental arcade with some disease on the maxillary arcade. There was no evidence of osteomyelitis.
Premedication with 0.4mg/kg butorphanol was given intra-muscularly and the lizard was maintained at an environmental temperature of about 30ºC for 20 minutes. Anaesthesia induc-
tion was achieved by face mask. Intubation was carried out with a 2mm endotracheal tube, and ventilation was provided using five per cent isoflurane and 1.0L/minute oxygen in a pressure-driven small animal ventilator.
Anaesthesia was maintained using 1.5 to two per cent iso-flurane in 1.0L/minute oxygen. Intermittent positive-pressure ventilation was provided at a fre-quency of 10 breaths per minute at 5cm H2O throughout the anaesthetic to mimic previously observed resting respiratory rates and coelomic excursions.
Monitoring included audi-ble doppler ultrasonography to monitor the heart, pulse oxime-try positioned in the oesophagus and cloacal temperature using a vital scan monitor.
A deep swab of the perio-dontal pocket was taken for bacterial and fungal culture; this was performed at both 25ºC and 37ºC. Antibiotic sensitivity testing was also carried out.
Ultrasonic scaling was per-formed on both the maxillary and mandibular dental arcades to remove the calculus. After scal-ing, moderate bilateral gingival hyperplasia was revealed on the mandibular dental arcade. The gingival pockets were flushed with 0.1 per cent chlorhexidine acetate oral solution; this was continued daily for four weeks.
Ceftazidime 20mg/kg, given subcutaneously every 72 hours, was started one week prior to
the procedure and continued for a further four weeks. Anaesthetic recovery was unremarkable, and spontaneous respiration resumed within 30 minutes of the isoflurane being turned off.
Dietary modification was ini-tiated. The lizard was fed an increased proportion of harder and larger invertebrates and firm vegetables. The frequency of feeding firm fruit was also decreased (Table 1). These modifications were accepted within a few days.
The aerobic and anaerobic bacterial culture was negative; however, a heavy growth of Candida albicans was isolated. Itraconazole 5mg/kg was given orally every 24 hours for seven days. Re-examination of the
patient after four weeks found no gingival erythema or puru-lent material, although the gum recession was unchanged.
DiscussionPeriodontal disease is common in captive lizards with acro-dont dentition, such as agamids and chameleons1.
Unlike pleurodont teeth seen in most lizards and all snakes, acrodont teeth are not regu-larly replaced and are simple triangular teeth ankylosed to the mandibles and maxilla.
A longitudinal ridge of bone, only covered by a thin layer of stratified squamous epithelium, is exposed between the teeth and gingival margin. There is no perio- dontal ligament. This exposed
BRIGITTE REUSCHBVetMed(Hons), CertZooMed, MRCVS
describes an underweight lizard that was treated with ultrasonic scaling and dietary modification, and explains why reptiles with acrodont dentition are predisposed to periodontal conditions
Bearded dragon with periodontal disease: exotic practice challenge
CLINICAL REPTILIA
Figure 1. The patient had periodontal disease on the mandible.
¿
Three methods of givingequine pain relief
HOLD, STRUGGLE,SQUIRT
DISGUISE, FEED,WAIT
TEAR, POUR,RELAX
The choice is a no-brainer
Further information is available from: Janssen Animal Health,50-100 Holmers Farm Way, High Wycombe, Bucks HP12 4EG, UKTel: +44 (0)1494 567555 Email: [email protected]. JanssenAnimal Health is a division of Janssen Cilag Ltd. DANILONEquidos contains suxibuzone. Legal category POM-V .
NSAID for horses, with suxibuzone, the nextgeneration phenylbutazone pro-drug
JAN238 DanThree Ad 183x128:Layout 1 21/5/09 10:13 Page 1
VT39.22 master IC.indd 22 28/05/2009 11:13

23June 8, 2009
bone is a common site for plaque and bacterial deposition, leading to periodontal disease.
This case illustrates the typi-cal presentation of an inland bearded dragon – a commonly kept agamid – with periodontal disease. The aetiology of this disease in lizards with acrodont dentition appears to be primarily due to an inappropriate captive diet. A survey of 21 wild-caught agamids and five chameleons found no evidence of periodon-tal disease2, whereas a case report describing this condition in 42 captive agamids and cha-meleons has been published1.
The soft diet of the bearded dragon in this case study required minimal mastication, thereby predisposing it to plaque accu-mulation on the exposed bone and gingival margin.
As the condition progressed, the other clinical signs devel-oped. The gingival recession and pocket formation seen ventral to the bone was impacted with calculus and purulent material. This can often be a site for food impaction. In advanced cases, subcutaneous abscessation and severe osteomyelitis with patho-logical fractures may be seen. This was not seen in this case.
Other factors that may cause periodontal disease in lizards include immunocompromise due to concurrent disease or environmental stress and mal-nutrition. Historical findings of selective feeding of soft food and progressive weight loss are typical for this insidious condition, where disease is often advanced on first presentation.
Early stages of the disease are commonly mistaken for stoma-titis. Gingival recession, pocket formation and gingival hyper-plasia indicate severe chronic periodontal disease.
Progression to systemic dis-ease with septicaemia, pneumo-nia and hepatic thrombosis may be seen in some cases3, but not in this example.
An increase in anaerobes (for example, Bacteroides species) and spirochetes is reported in agamid lizards with periodontal disease1. No bacterial growth was achieved on culture of the deep swab taken from this case. This is not uncommon with samples sent in the post, as Bacteroides species rapidly die and may not be detected.
CLINICAL REPTILIA
Figure 2 (above). Lateral horizontal beam radiograph of the conscious bearded dragon’s skull.Figure 3. Dorsoventral radiograph of the bearded dragon’s skull, taken under general anaesthesia.
Competition for nutrients in the transport media may also cause culture failure. In this case example, the heavy fungal growth of C albicans probably affected the culture. Candida species was found to be the most common yeast isolated from a survey of 91 reptiles4. C albicans and C tropicalis have been asso-ciated with stomatitis in lizards, with C albicans having the high-est virulence. Mycotic disease is seen in immunocompromised reptiles. This case had both chronic disease and malnutrition; therefore, the lizard may have been immunocompromised. As yeasts are common oral com-mensals of reptiles3,4, a diagnosis of mycotic infection should, where possible, be made on histopathology. Biopsy was not considered appropriate for this case due to the location, chronic-ity and severity of disease.
Treatment was aimed at physi-cal removal of the calculus, puru-lent material and a presumptive secondary mixed bacterial and fungal infection. Systemic ceftazi-dime and itraconazole and topi-cal chlorhexidine were instigated and a good clinical response was seen within four weeks.
Modification to a diet that requires more mastication has been shown to reduce plaque formation and, in mild cases, prevent recurrence1. A regular dental examination every six months has been scheduled.
ConclusionThis case demonstrates a typi-cal presentation of a common condition seen in captive inland bearded dragons. The prognosis for recurrence of periodontal disease for this lizard is poor, as the gingival recession is per-manent and the pocket forma-tion makes it prone to calculus accumulation. However, dietary modification and regular dental scaling should manage the con-
TABLE 1. Diet and feeding structure of case study patient
Food item Quantity fed, prior to diagnosis
Quantity fed, after diagnosis
Fruit 15g, fed every other day. Banana, mango, berries, grapes, apple, pear, orange
10g, fed in 1cm cubes, twice a week. Apple, pear, pineapple, apricot, peach
Vegetables 15g, fed every other day. Grated carrot, swede, lettuce, broccoli, peppers
20g, fed in 1cm cubes, every other day. Carrot, broccoli, peppers, swede, radish, parsnip
Insects Fed every other day; 12 mealworms, one or two crickets
Five crickets; three to five locusts; two or three cockroaches
Leaves and weeds
None Offered when available: dandelion, clover, nasturtium flowers and leaves, bramble leaves
Supplement On every feed: Nutrobal (Vetark)
On every feed: Nutrobal, (Vetark)
dition and prevent further pro-gression to osteomyelitis, which would carry a grave prognosis.● Although few drugs are licensed for reptiles, the author notes that the use, in this species, of medications mentioned in this article has been widely reported.● The author thanks Sharon Redrobe and staff at Bristol Zoo Gardens for their contribution.● The author, along with Kevin Eatwell, will discuss exotic emer-
¿
gencies at a CPD event in New-castle on June 25. For full details, visit www.vet-cpd.co.uk
References1. McCraken H E (1999). Periodontal disease in lizards. In: Fowler M E and Miller E R (eds), Zoo and Wild Animal Medicine: Current Therapy (4th edn)
W B Saunders: Philadelphia: 252-257.2. McCraken H E and Birch C A (1994). Periodontal disese in lizards, Proceedings of the American Associa-tion of Zoo Veterinarians, Pittsburgh.
3. Redrobe S and Frye F L (2001). Hepatic thrombosis and other pathol-ogy associated with severe periodon-
BRIGITTE REUSCH graduated with honours from the RVC in 2002. After working as an exotic animal locum and a small animal assistant, she joined the Royal (Dick) School of Veterinary Studies as a small animal intern. She was appointed the first Rabbit Welfare Fund rabbit and zoo animal resident in the UK in 2004, based at Bristol Zoo Gardens and the University of Bristol. Brigitte ran a rabbit and exotic veterinary referral service in the south-west before returning to Edinburgh in 2008 as a lecturer in rabbit medicine and surgery at the R(D)SVS. She holds the RCVS zoological medicine certificate.
tal disease in the bearded dragon (Pogona vitticeps), Proceedings of the Association of Reptile and Amphibian Veterinarians:105-107.4. Kostka V M et al (1997). Review of the literature and investigations on the prevalance and consequences of yeasts in reptiles, Vet Rec 140: 282-287. ■
����
Palatable L-Lysine paste for cats
The fi rst UK L-Lysine-based supplement developed for veterinary use
Palatable paste formulated exclusively for kittens and adult cats
Vetoquinol UK Limited, Vetoquinol House, Great Slade, Buckingham Industrial Park, Buckingham, MK18 1PA. Tel: 01280 814500 Fax: 01280 825460 Email: offi [email protected] Website: www.vetoquinol.co.uk
NewNow
available
in the UK
2451
(QLV\O�)�$GYHUW����[����LQGG���� ������������������
VT39.22 master IC.indd 23 28/05/2009 11:14

PROCEEDINGS OF THE
NORTH AMERICAN VETERINARY CONFERENCE
VOLUME 20
JANUARY 7-11, 2006
ORLANDO, FLORIDA
SMALL ANIMAL EDITION Reprinted in the IVIS website (http://www.ivis.org) with the permission of the NAVC. For more information on future NAVC events, visit the NAVC website at www.tnavc.org

Exotics — Reptiles and Amphibians ______________________________________________________________________________________________
1671
MANAGEMENT OF PERIODONTAL DISEASE
IN LIZARDS
Scott J. Stahl, DVM, Diplomate ABVP (Avian) Stahl Exotic Animal Veterinary Services
Vienna, VA McCracken and Birch (1994) were the first to describe a periodontal disease-like condition in agamid lizards and old world chameleons. These lizards all acrodont teeth (not rooted, but simply attached to the surface of the mandibular and maxillary bones), which predisposes them to periodontal disease, stomatitis and potentially osteomyelitits. This unique dentition results in a thin gum line along the lateral surface of the mandibular and maxillary bones. When this fragile gum tissue is damaged or abraded bone is exposed and becomes readily permeable to bacteria. Commonly kept species of lizards seen in practice with acrodont dentition include bearded dragons, Asian water dragons, frilled dragons, and all old world chameleons. EXAMINATION AND DIAGNOSTICS On physical exam, these lizards often present with signs of stomatitis or swellings along the mandibular and maxillary bones. On close inspection these bones will be discolored, specifically green or brown-black, along their surfaces. Often lysis of bone is evident on presentation. Swellings of the soft tissue over the mandibular or maxillary bones is also common as the soft tissue adjacent to the periodontal disease becomes infected. Regular oral exams should be performed to inspect the gum line for signs of discoloration, irregularities in the surface, and loss of tissue. If suspicious lesions are present, gentle curettage with dental instrumentation is useful to assess soft tissue and bone involvement. Abnormal physical exam findings consistent with mandibular and maxillary bone involvement should be assessed with radiographs. Osteomyelitis in reptiles is characterized radiographically by bone lysis. Radiology is useful to assess the severity of the bone involvement and thus help to formulate a therapeutic regimen. Additionally, radiographs can be used to monitor therapeutic progress. Culture and sensitivity can be utilized to identify the bacterial (or fungal) organisms involved and to determine the most appropriate antimicrobial for treatment. Since mixed infections are common, both aerobic and anaerobic cultures should be taken. A sterile prep should be performed over the site to be sampled, and a sterile scalpel or needle should be used to collect a deep culture sample. Blood cultures may also be diagnostic as reptiles with osteomyelitis may often be septic. Biopsy of bone or associated soft tissue may also be useful as a method for identifying organisms involved. Histopathology of these lesions with special stains can help to identify other possible pathogens such as fungal organisms and mycobacteria.
Isaza and Jacobson (1995) found the most common bacterial organisms isolated in cases of osteopmyelitis in reptiles were gram-negative bacteria, including Salmonella spp., Aeromonas spp., Pseudomonas spp., Escherichia spp. and Morganella spp. They also fund gram-positive bacteria such as Streptococcus spp., Staphylococcus spp., and Corynebacterium spp., and anaerobic bacteria such as Clostidium spp. and Bacteriodes spp. were occasionally isolated from infected reptile bone, but often in conjunction with aerobic bacteria. TREATMENT Prior to treatment, the overall status of the patient must be assessed. Supportive care may need to be initiated prior to treating the disease. The reptile should be warmed to the high end of its preferred optimal temperature zone (POTZ). Fluid therapy should be initiated at 20-25 ml/kg daily as needed. After rehydration, and while awaiting the results of culture and sensitivity, the lizard may be started on a broad spectrum antibiotic regimen. Due to the high incidence of mixed bacterial infections and the severity of osteomyelitis, a combination of two antimicrobials is recommended initially (Isaza and Jacobson, 1995). Amikacin at 5mg/kg IM/SQ as an initial dose followed by 2.5 mg/kg IM/SQ every 72 hours OR enrofloxacin at 5-10 mg/kg IM/SQ/PO every 24-48 hours in combination with ceftazidine (20mg/kg IM/SQ every 72 hours) or carbenicillin (400 mg/kg IM every 24 hours) are good initial choices. Anaerobic and gram-positive bacteria may have resistance to enrofloxacin and amikacin, so antiobiotics such as ceftazidine (as above), ampicillin (20 mg/kg IM every 24 hours), and metronidazole (20-40 mg/kg PO every 24-72 hours) may be more appropriate or should be utilized concurrently with another drug depending on the results of culture and sensitivity. Aggressive surgical debridement of affected areas is important to open and expose the infected tissue. Standard wound flushing solutions with chlorhexidine or betadine can be used to aggressively flush wounds once or twice daily for several weeks. Unhealthy or discolored bone should be curreted and removed. Again, radiographs are important in helping to determine what bone(s) may need to be removed. A topical treatment which can be used to encourage deep local penetration of antibiotics after flushing is a solution of DMSO and amikacin (7.5 ml of DMSO is added to .25 ml of amikacin 50 mg/ml) or, depending on culture and sensitivity results, DMSO and enrofloxacin (7.5 ml of DMSO to 0.5 ml of injectable enrofloxacin 22.7 mg/ml). These solutions are typically applied once or twice daily, depending on the severity, for 3-4 weeks. Alternatively, silver sulfadiazine crème can be packed into the wound once daily after flushing. Osteomyelitis in reptiles must be treated in most cases for a minimum of 8-12 weeks and sometimes up to 6 months (Isaza and Jacobson, 1995). Treatment may not need to be as long if aggressive bone curettage is

The North American Veterinary Conference — 2006 ______________________________________________________________________________________________
1672
successfully utilized because the primary bacterial nidus has been eliminated. The prognosis for lizards with periodontal osteomyelitis and loss of bone is guarded to fair depending on severity and progression. Lifetime dental prophylaxis with an oral cleansing product (Maxiguard Oragel, Addison Biological Laboratory) will be necessary to reduce progression and minimize recurrence of osteomyelitis.
References 1. McCracken, H. and Birch, C.A.: Periodontal Disease
in Lizards. A Review of Numerous Cases. Proceedings of the American Association of Zoo Veterinarians, 1994, pp. 108-115.
2. Isaza R. and Jacobson, E.R. Non-nutritional Bone Diseases in Reptiles. In Current Veterinary Therapy, Vol. 13 ed. R.W. Kirk, 1357-1361. Philadelphia; W.B. Saunders Co., 1995.