Embed Size (px)
Citation preview
Anxiety disorders
IV year teachingChristopher Gale
Department of Psychological MedicineDunedin School of Medicine
Anxiety is….… a subjective experience of unpleasant anticipation,
accompanied by characteristic behavioural and physiological responses (e.g. avoidance, vigilance and arousal)
Evolutionary value: to protect individuals from danger. Present in most/?all higher animals – ? universal mechanism
by which organisms adapt to adverse conditions. Symptoms:
Cognitive (feelings of apprehension, fear)Cognitive (feelings of apprehension, fear) Physical symptoms (shortness of breath, trembling, palpitations etc);Physical symptoms (shortness of breath, trembling, palpitations etc); Endocrine and physiological changesEndocrine and physiological changes
Spectrum
Normal Emotion Pathological State
severe symptoms & functional impairment
Panic. Overwhelming sense of impending doom or
disaster. Physical symptoms.
Tachycardia.Tachycardia. Shortness of Breath.Shortness of Breath. Chest pain.Chest pain. Tingling lips and extremities.Tingling lips and extremities. Nausea, vomiting, diarrhoeaNausea, vomiting, diarrhoea Weakness. Collapse.Weakness. Collapse.
If specific → Phobia. If random → Panic disorder
Anxiety
Sense of fear around an event or stimulus → distress, or panic.
May be specific May be generalized (multiple topics of anxiety,
most of the day, nearly every day) Can lead to:
AvoidanceAvoidance Self medication with substances.Self medication with substances. Ritualisation of behaviour. Ritualisation of behaviour.
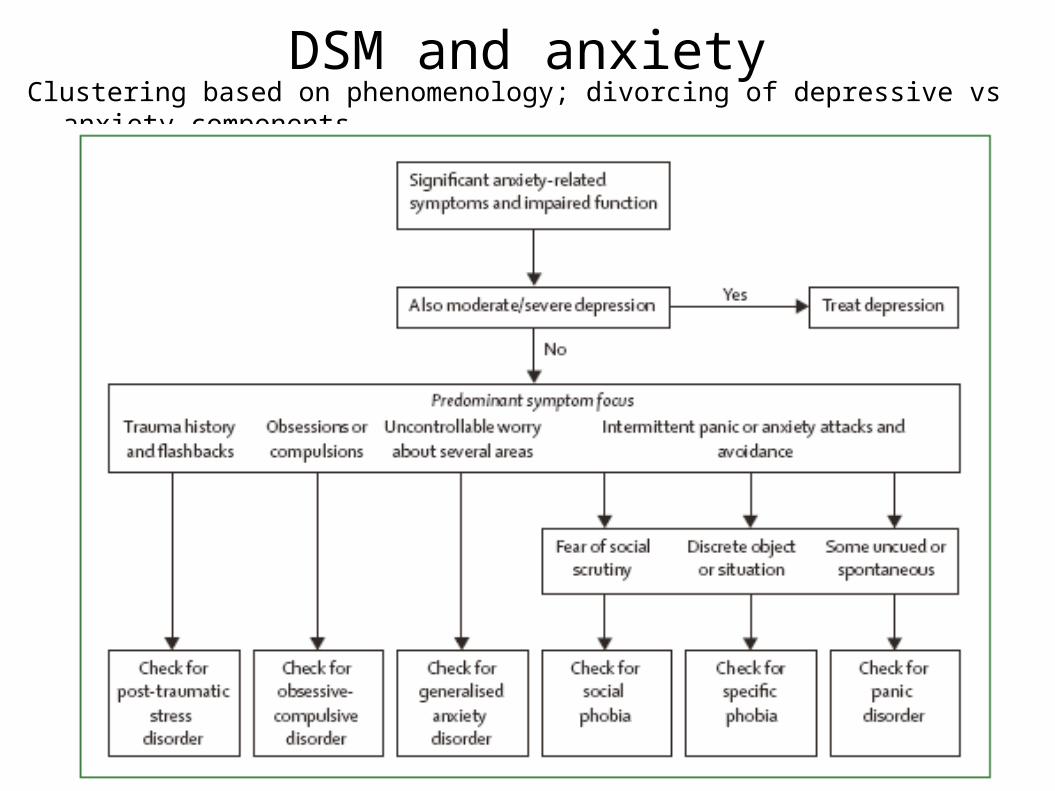
DSM and anxietyClustering based on phenomenology; divorcing of depressive vs anxiety components
Obsessions, compulsions.
Obsession is an unwanted, repeated distressing thought that is seen as:
From one's own mind.From one's own mind. Distressing.Distressing. Not controlled.Not controlled.
Compulsions are a ritualised repeated behaviour that is seen by the patient as preventing or minimising risk of feared event occuring eg hand washing, checking doors locked.
Traumatic event.
Out of ordinary life events. Risk of death or severe injury (including fear of)
or witnessing same. Would be seen as distressing by most people. Examples
Living in war zone.Living in war zone. Physical or sexual assaultPhysical or sexual assault Car crashesCar crashes
Although panics are not traumatic as such can have similar post event sequelae.
Following trauma
Nightmares: of event. Flashbacks. Like nightmares, full re
experience of event including all senses and the sense of fear. Can be stimulated by certain triggers of the trauma (including therapy) or may occur randomly.
Foreshortened future. Lack of confidence in planning years, weeks or days at work or relationships.
Emotional numbness.
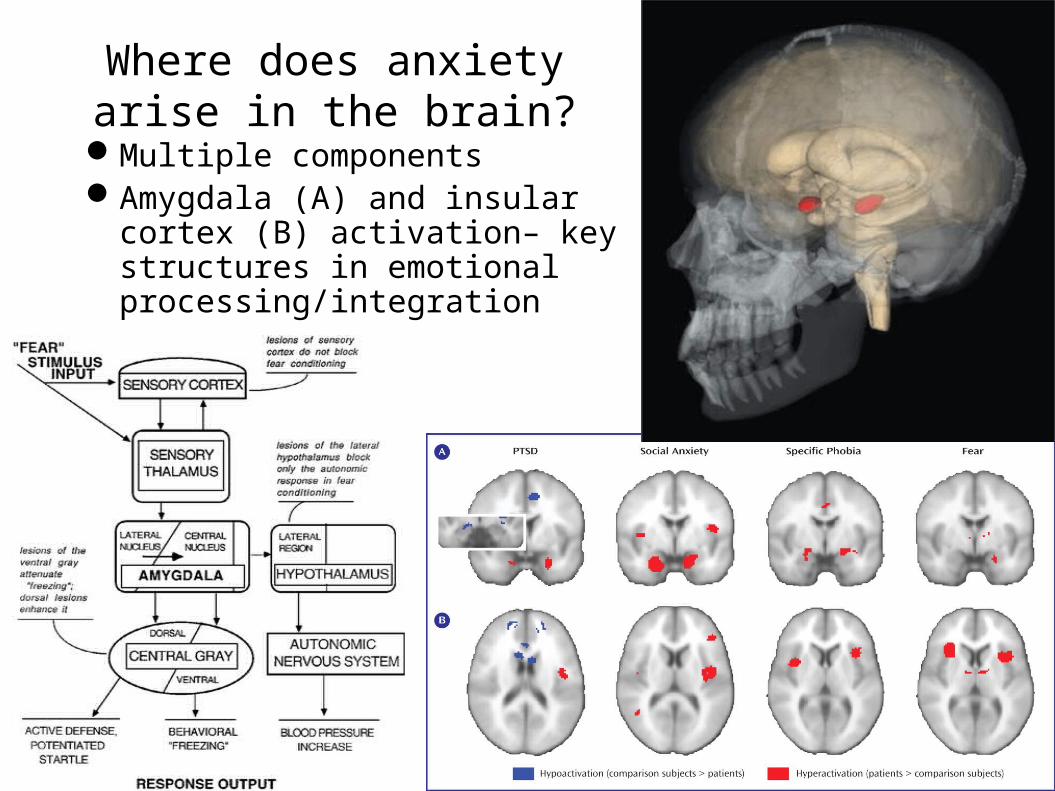
Where does anxiety arise in the brain?
Multiple componentsAmygdala (A) and insular cortex (B)
activation– key structures in emotional processing/integration
(Etkin Am J Psych 2007)
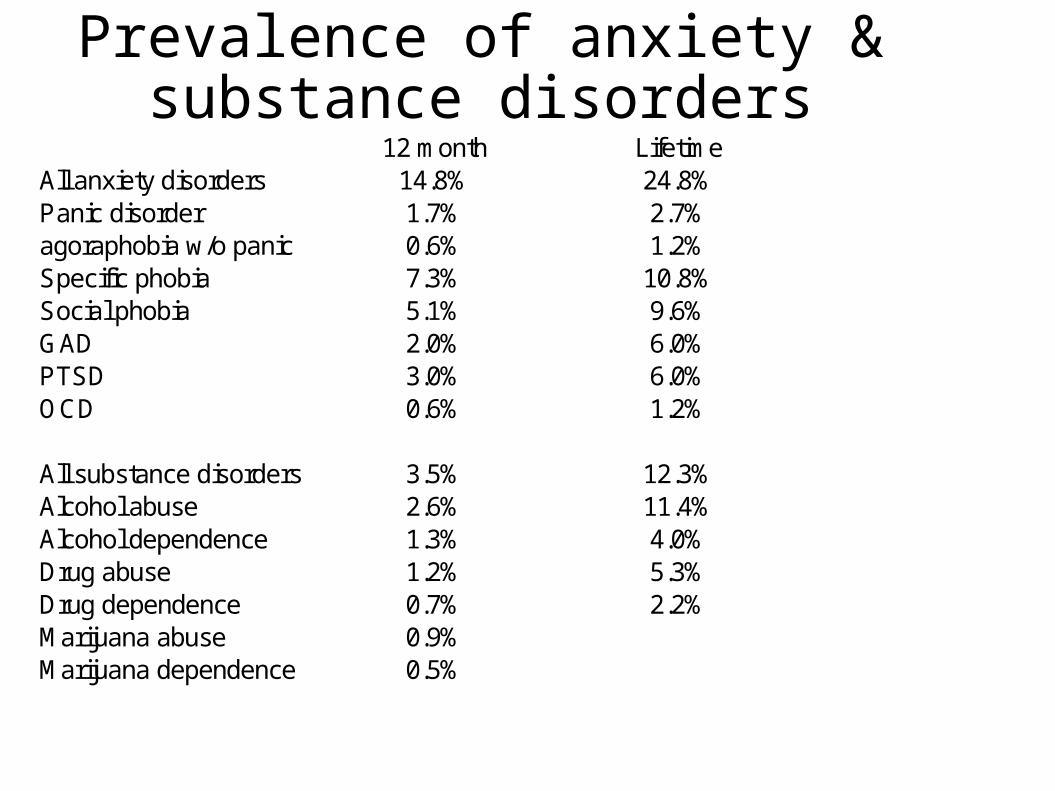
Prevalence of anxiety & substance disorders
12 month LifetimeAll anxiety disorders 14.8% 24.8%Panic disorder 1.7% 2.7%
0.6% 1.2%Specific phobia 7.3% 10.8%Social phobia 5.1% 9.6%GAD 2.0% 6.0%PTSD 3.0% 6.0%OCD 0.6% 1.2%
All substance disorders 3.5% 12.3%Alcohol abuse 2.6% 11.4%Alcohol dependence 1.3% 4.0%Drug abuse 1.2% 5.3%Drug dependence 0.7% 2.2%Marijuana abuse 0.9%Marijuana dependence 0.5%
agoraphobia w/o panic
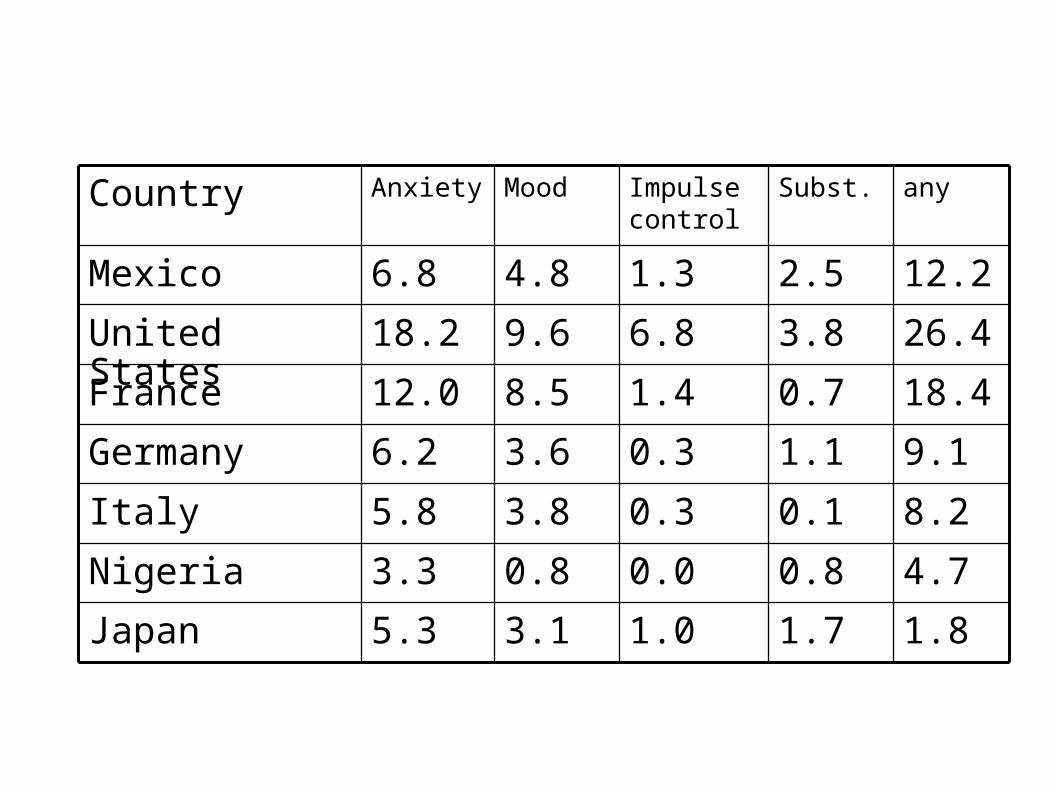
Rate of disorders: WHO surveys, selected countries.
1.81.71.03.15.3Japan
4.70.80.00.83.3Nigeria
8.20.10.33.85.8Italy
9.11.10.33.66.2Germany
18.40.71.48.512.0France
26.43.86.89.618.2United States
12.22.51.34.86.8Mexico
anySubst.Impulse control
MoodAnxietyCountry
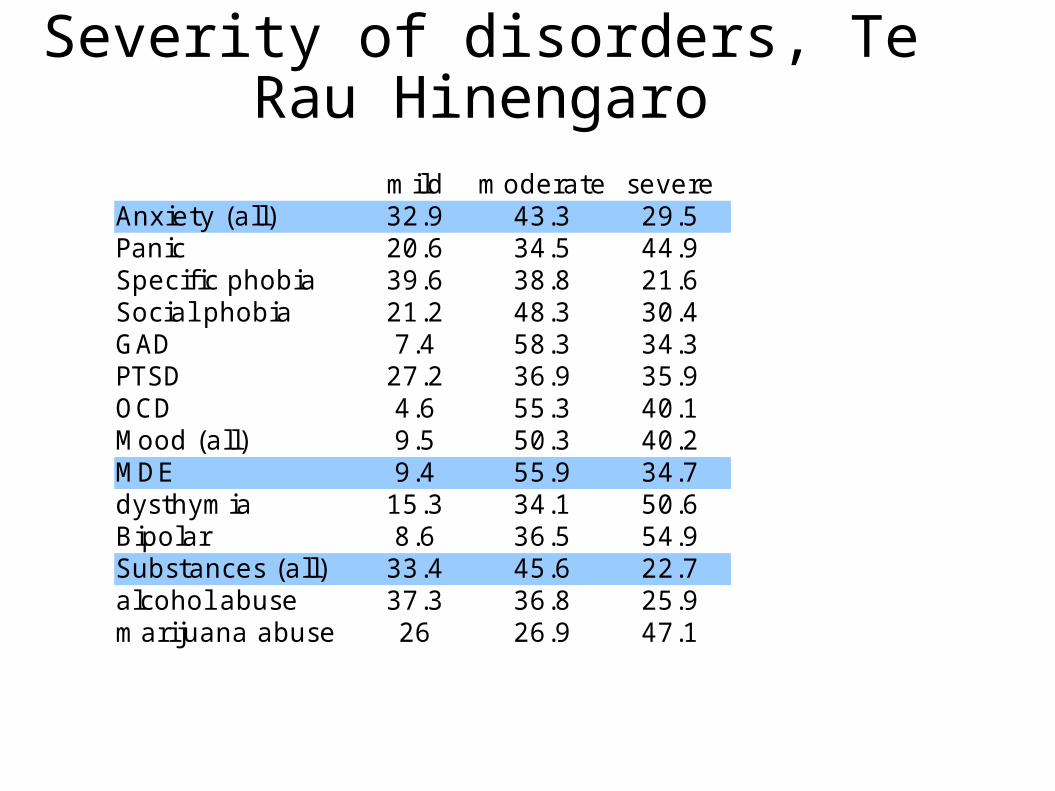
Severity of disorders, Te Rau Hinengaro
m ild m oderate severeAnxiet y (all) 32.9 43.3 29.5Panic 20.6 34.5 44.9Specif ic phobia 39.6 38.8 21.6Social phobia 21.2 48.3 30.4GAD 7.4 58.3 34.3PTSD 27.2 36.9 35.9OCD 4.6 55.3 40.1Mood (all) 9.5 50.3 40.2MDE 9.4 55.9 34.7dysthym ia 15.3 34.1 50.6Bipolar 8.6 36.5 54.9Substances (all) 33.4 45.6 22.7alcohol abuse 37.3 36.8 25.9m arijuana abuse 26 26.9 47.1
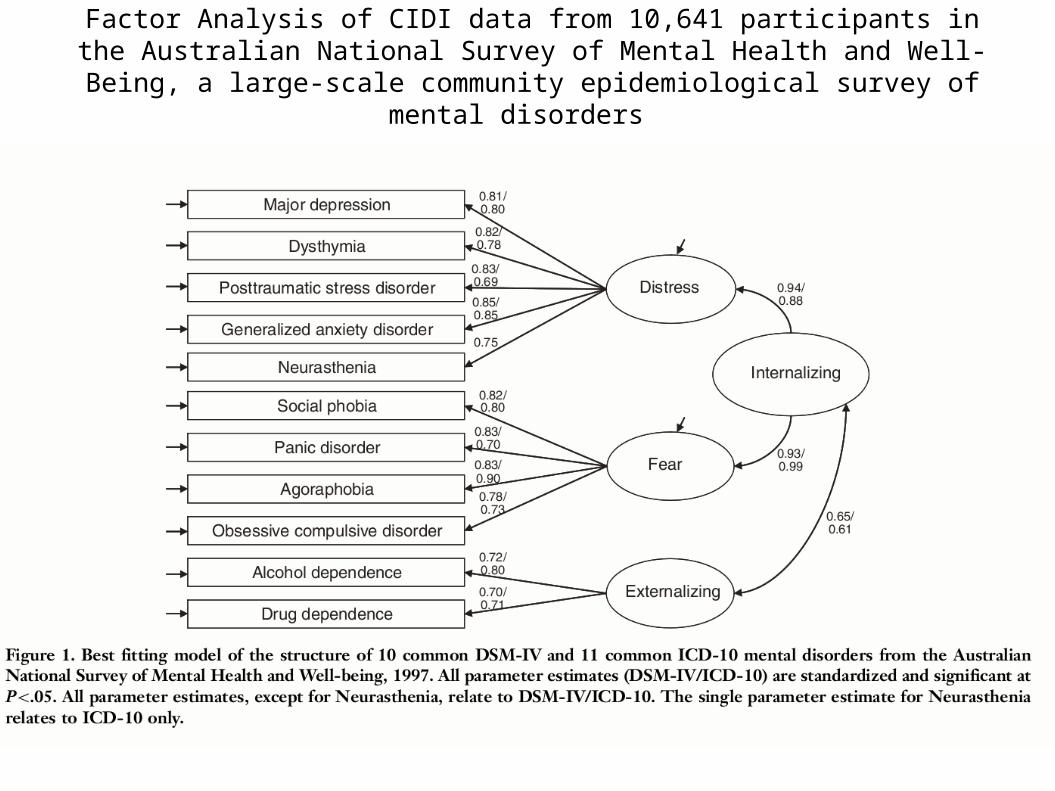
Factor Analysis of CIDI data from 10,641 participants in the Australian National Survey of Mental Health and Well-Being, a large-scale community
epidemiological survey of mental disorders
General
Think of diagnoses, not diagnosis. Consider priority of treatment.
Timing for treatment. Use of others – practice nurse, primary mental
health. Consider referral
Opinion Management
Positive approach: can minimize disability.
Treatment
General techniques. Talking therapies Medication
Behaviour therapies
Applied relaxation. Education about anxiety. Activity Scheduling. Befriending. Exercise Relaxation technique & practice.
Bibliotherapy “Anxiety and Neurosis handbook” etc. Internet therapy – via CrufAD (in Australia) and now
integrated in most GP practices (in New Zealand)
Graded exposure.
Phobias. List of stimuli and programmed increase in anxiety List of stimuli and programmed increase in anxiety
provoking triggers.provoking triggers. Can expose symptoms panic (exercise, antihistamines).Can expose symptoms panic (exercise, antihistamines).
OCD add response prevention (expose and no ritual).add response prevention (expose and no ritual).
Cognitive therapy.
More effective in GAD Very useful in depression, which is quite co-morbid. Common distortions.
Over responsibleOver responsible Perfectionism (“All or nothing”)Perfectionism (“All or nothing”) Catastrophization (“Mountains out of molehills”).Catastrophization (“Mountains out of molehills”).
USE MANUAL.
Comments medications.
Generally do not control all symptoms. Take six to ten weeks to work. Need higher doses SSRI than in depression: 20 –
60 for GAD, 40 – 100 for OCD.
Medications.
Antidepressants.
SSRI, TCA, MAOISSRI, TCA, MAOI Anticonvulsants
Gabapentin, Pregabalin, TigiabatineGabapentin, Pregabalin, Tigiabatine Aziopirones.
Buspirone, Gepirone.Buspirone, Gepirone. Benzodiazepines. (dependancy) Hyoscine & Kava (side effects) Low dose antipsychotics esp Quetiapine (side effects ++)