Embed Size (px)
Citation preview

N E U R O L O G Y, P S Y C H I A T R Y A N D B R A I N R E S E A R C H 1 8 ( 2 0 1 2 ) 1 2 2 – 1 2 8
.sc iencedi rect .com
Avai lab le at wwwjournal homepage: www.elsev ier .com/ locate /npbr
Anxiety and depression in incident stroke survivors and theircarers in rural Tanzania: A case-control follow-up study overfive years
Matthew P. Jones a, Suzanne C. Howitt a, Ahmed Jusabani b, William K. Gray a,Eric Aris c, Ferdinand Mugusi c, Mark Swai b, Richard W. Walker a,*
a North Tyneside General Hospital, Rake Lane, North Shields, Tyne and Wear, NE29 8NH, UKb Kilimanjaro Christian Medical Centre, Moshi, United Republic of Tanzaniac Department of Neurology, Muhimbili University Hospital, Dar-es-Salaam, United Republic of Tanzania
A R T I C L E I N F O
Article history:
Received 21 September 2011
Accepted 17 January 2012
Available online 16 February 2012
Keywords:
Stroke
Tanzania
Anxiety
Depression
Africa
Cerebrovascular disease
0941-9500/$ - see front matter � 2012 Elsevidoi:10.1016/j.npbr.2012.01.003
* Corresponding author. Address: DepartmNE29 8NH, UK. Tel./fax: +44 0191 293 2709.
E-mail address: [email protected]
A B S T R A C T
Aims: To quantify the extent and nature of anxiety and depression in a representative
cohort of stroke survivors and their carers in rural Tanzania.
Design: A cross-sectional design was used and stroke cases were followed up at 6–60
months post-stroke. Levels of anxiety and depression in stroke survivors, their carers (for
physically dependent stroke survivors) and age- and sex-matched controls were assessed
using the hospital anxiety and depression (HAD) scale. Other data collected included age,
sex, time elapsed since stroke, quality of life, cognitive function, level of disability and
socioeconomic status.
Results: Levels of depression seen in our cohort of stroke survivors (53.0%) are high com-
pared to data from the developed and developing world. Anxiety levels (21.6%) are similar
to published data. Stroke survivors (n = 58, full data set n = 51) and carers (n = 27) were sig-
nificantly more anxious than controls (n = 58), whereas levels of depression were similar
across all three groups. High stroke survivor HAD scores correlated with lower scores in
physical health, psychological health and environment sections of the WHOQOL-Bref.
Increased carer anxiety and depression were associated with reduced informant-reported
levels of cognitive function in stroke survivors.
Conclusions: To our knowledge this is the first long term study of incident stroke cases in
sub-Saharan Africa which has investigated the psychological health of stroke survivors
and their carers. Our study highlights the growing need to develop community rehabilita-
tion services in the developing world, which address both physical and psychological
morbidity.
� 2012 Elsevier GmbH. All rights reserved.
1. Introduction
Although stroke has traditionally been viewed as a disease of
high-income countries, demographic and epidemiological
er GmbH. All rights reser
ent of Medicine, North Ty
.uk (R.W. Walker).
changes mean that it is becoming more common in other re-
gions, with 87% of stroke deaths now occurring in low to mid-
dle income countries.1 In addition to the serious physical
consequences that may be experienced after stroke, a large
ved.
neside General Hospital, Rake Lane, North Shields, Tyne and Wear,

N E U R O L O G Y, P S Y C H I A T R Y A N D B R A I N R E S E A R C H 1 8 ( 2 0 1 2 ) 1 2 2 – 1 2 8 123
proportion of patients also suffer from psychiatric sequelae
which may adversely affect quality of life and rehabilitation
outcomes.2 Such problems are not confined to stroke survi-
vors themselves, but are often experienced by their carers
who are under increased levels of emotional and physical
stress.3
Depression is common in stroke survivors, and has been
associated with reduced quality of life and poorer rehabilita-
tion outcomes.4,5 Patients with severe disability are at in-
creased risk of depression although this relationship is
likely to be bi-directional as depression may, in turn, hinder
physical recovery.6,7 A systematic review of 51 observational
studies showed that depressive symptoms were present in
33% of all stroke survivors at any time during follow-up.8 In
sub-Saharan Africa (SSA), the Ibadan stroke study in Nigeria
noted that negative feelings (including anxiety, fear and
depression) were present in 75% of 100 consecutive stroke pa-
tients presenting to hospital, although the spectrum of nega-
tive feelings assessed was wider than that of clinical
depression.9 Compared to symptoms of depression, post-
stroke anxiety has been much less well studied, despite the
considerable symptom overlap.10 A longitudinal community-
based Swedish study of 80 stroke survivors found that the
prevalence of generalised anxiety disorders after stroke was
28% in the acute stage, with no significant decrease through
3 years of follow-up.11 This Swedish study showed that gener-
alised anxiety disorders were strongly associated with depres-
sion, dependence in activities of daily living and stroke
survivors having a smaller social network.
Caring for a stroke survivor can prove burdensome, and re-
sult in stress and psychological morbidity for the caregiver.12
Several studies from high-income countries report adverse ef-
fects on health and well-being amongst carers for stroke sur-
vivors.12–15 In an Australian study investigating the impact of
caring for stroke survivors at one-year post stroke, almost
80% of caregivers reported a detrimental impact on their emo-
tional health, social activities and leisure time, and over half
reported negative effects on family relationships. The fear
and worry of leaving the stroke survivor alone was a central
theme.16 Increased psychological morbidity among caregivers
has been found to be associated with smaller social networks,
greater stroke severity and lower socio-economic status.12,14
Data are lacking on the psychiatric well-being of stroke sur-
vivors and their carers in low- and middle-income countries,
particularly SSA. Long-term follow-up studies in SSA have
been difficult to conduct due to poor infrastructure, limited pa-
tient records and other practical problems.17 Furthermore,
many studies have used hospital-based cohorts which may
lead to a selection bias, since results are only representative
of those who are able or willing to attend the hospital. Many
patients in the developing world do not present to hospital
due to limited financial resources, inadequate transport links
or because they seek alternative care from traditional healers.
Community-based research is therefore needed to assess the
psychiatric morbidity of the wider and more representative
population of stroke survivors and their carers.9,18–20
The aim of this study was to conduct a long term, commu-
nity-based study to investigate anxiety and depression among
a cohort of incident stroke survivors, carers and control
subjects in rural Tanzania.
2. Methods
A favourable ethical opinion was obtained from the National
Institute of Medical Research in Tanzania and from the New-
castle and North Tyneside Joint Ethics Committee.
2.1. Participants
Cases were recruited from survivors of a stroke incidence
study in the rural Hai district of northern Tanzania from June
2003 to June 2006, in addition to further cases identified in the
same region between June 2006 and December 2007.21 The
World Health Organization (WHO) criteria were used to clas-
sify stroke cases.22 Cases were assessed as part of the current
study between June and September 2008. A person was
deemed to be the primary carer of a stroke survivor if the
stroke survivor identified them as there carer and the stroke
survivor was physically dependent on the carer. If stroke sur-
vivors were physically independent then they were consid-
ered not to have a carer. The control subjects were selected
by local healthcare workers, by convenience sampling, from
within the Hai district. Relatives and carers of stoke patients
were not considered as potential controls. In total 58 stroke
patients and 58 controls were recruited to the follow-up study.
2.2. Assessment
Assessment was between 6 months and 5 years post-stroke,
depending on the date of their incident stroke. Assessment
and examination of stroke patients and carers were carried
out by research doctors (MPJ and SCH), with local healthcare
workers acting as translators and interpreters. Controls were
interviewed by either MPJ, SCH or one designated clinical
assistant who had been suitably trained.
2.2.1. Anxiety and depressionAnxiety and depression was measured in patients, controls
and carers of physically dependent patients using the hospi-
tal anxiety and depression scale (HAD).23 Physically depen-
dent patients were classified as patients with a Barthel ADL
index of less than the maximum score of 20. The HAD scale
asks seven questions relating to anxiety and a further seven
relating to depression. Responses are scored from 0 to 3. For
the purposes of this study, an anxiety or depression sub-score
of 0–7 was indicative of no symptoms, a score of 8–10 was
indicative of mild symptoms, a score of 11–15 moderate
symptoms and a score of 16–21 severe symptoms of anxiety
or depression. The HAD scale has been validated for use in
a hospital and community setting a Nigeria.24 The tool per-
formed well in both settings, although mis-classification rates
for both anxiety and depression were generally lower in the
community than in a hospital setting.
2.2.2. Other assessmentIn addition, each patient and control was assessed using a
series of well recognised scales and assessment tools during
a 1–2 h interview. A 10-item questionnaire, which covered
areas including housing and land ownership, was used to
determine the socio-economic status of patients and controls.

124 N E U R O L O G Y, P S Y C H I A T R Y A N D B R A I N R E S E A R C H 1 8 ( 2 0 1 2 ) 1 2 2 – 1 2 8
Quality of life was assessed using the WHOQOL-Bref.25 This
instrument measures overall QOL and satisfaction with
health. It provides summary scores in the domains of physical
health (domain 1), psychological health (domain 2), social
relationships (domain 3) and environment (domain 4). Further
details of its use by our study team have been described
previously.2 The CSI-D is a 34-item screening instrument for
dementia in developing countries, consisting of two parts;
one questionnaire directed at patients and the other at an
informant or carer.26 Scores from patients and informants
(carers) are weighted to give a global measure of dementia.
Information concerning demographics (name, age, sex,
abode, highest level of education) and medical care was also
obtained. In cases where patients were unable to respond
due to dysphasia or aphasia, demographic and other back-
ground information was sought from a relative or carer.
The Barthel index27 was used to assess patients but not
carers or controls. The scale measures the functional inde-
pendence of an individual with regard to their ability to carry
out activities of daily living (ADL). Muscle power was also
measured in patients by using the Medical Research Council
Scale28 and a language, speech and swallowing screen was
performed.
2.3. Statistics
The data were analysed using statistical software, PASW-18
for windows (PASW, Chicago, IL, USA). All variables were
non-normally distributed and, therefore, the Mann–Whitney
U test was used to characterise differences. Spearman’s corre-
lation test was used to assess associations between scores for
ordinal data and the point biserial correlation test was used
for dichotomous data. Due to the significant deviation from
normality in the data obtained from the HAD scale mean
and median values are not quoted. The data were categorised
as described in Section 2.2.1 and the frequency of each score
given.
3. Results
The initial incidence study21 identified 132 incident stroke
cases and a 52 further cases were identified between the
end of the incidence study and 31st December 2007, giving
184 cases in total. By the start of the current study on 1st June
2008, 102 cases had died, 16 cases were unable to participate
in a follow-up assessment due to co-morbidity or illness and 8
had left the study area or could not be traced. Therefore, 58
patients were followed up.
Details of the cohort have been described previously and
are summarised here.2,21 There was no significant difference
in age at stroke (U = 3114.5, z = )1.608, p = 0.108) or gender
(v2(1) = 0.047, p = 0.828) between those who were followed-up
and those not followed-up. Patients were assessed at a median
of 36 months post-stroke (range 6–60) post-stroke. The mean
age of patients was 67.1 years (range 30–88) and 28 (48.3%) were
male. The mean age of controls was 61.7 years (range 27–86)
and 30 (51.7%) were male. Although controls were, on average,
younger than patients the difference was not significant
(U = 1368.0, z = )1.596, p = 0.111). There was no significant dif-
ference in gender (v2(1) = 0.138, p = 0.853).
Carer HAD scores are based on responses from the 27
carers of physically dependent patients. The remaining pa-
tients were physically independent and were therefore classi-
fied as not needing a carer for the purposes of this study. Of
the 27 carers, only 4 were male, 11 were a spouse of the stroke
survivor, 14 were a son or daughter (including in-laws) and 2
were a grand-daughter. The average age was 47 years old
although the range of ages was 16–73 (SD 15.989). Seventeen
were employed or self-employed which included selling fruit
or crops at the market, and 4 were subsistence farmers.
Six patients were unable to give responses to the HAD due
expressive dysphasia or complete aphasia and one patient did
not wish to answer the HAD questions. He was subjectively
noted by researchers to have a very low mood and only spoke
a few words. No patients were excluded due to dementia. A
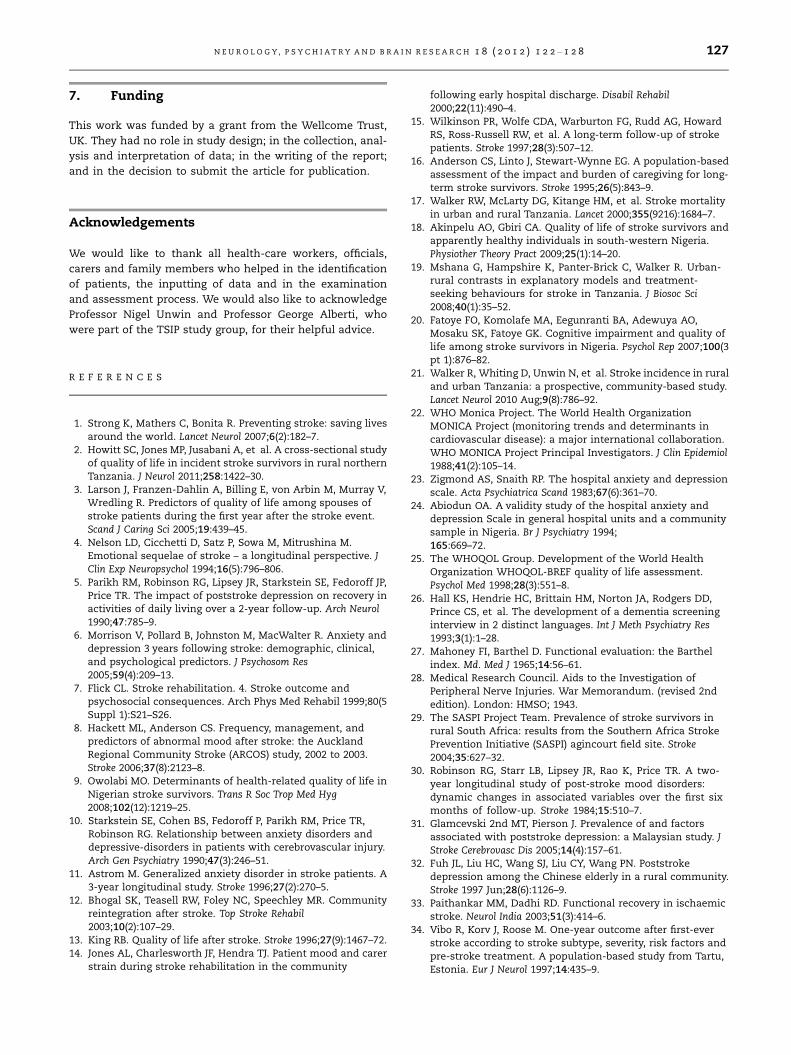
summary of patient and carer HAD scores are shown in Table
1. More patients (19.6%) and carers (22.2%) were classified as
having some form of anxiety, than controls (3.4%). Depression
was more common across all three groups, with 51.0% of pa-
tients and 40.7% of carers being depressed, compared to 53.4%
of controls. No patients and only one carer were defined as
having severe depression and anxiety.
3.1. Associations between predictors
Depression in stroke survivors, as measured on the HAD
scale, was associated with a number of tests of motor perfor-
mance in a number of functional tasks, see Table 2. Anxiety
was associated with WHOQOL-Bref domain 1 (physical
health) and domain 2 (psychological health) scores only. The
use of anti-hypertensive drugs post-stroke was associated
with lower anxiety (r = 0.284, p = 0.046) and depression
(r = 0.292, p = 0.040).
In patients, symptoms of anxiety and depression were not
associated with any of the 10 items measuring socio-eco-
nomic status. Reduced cognitive function (CSI-D patient inter-
view) was not associated with anxiety or depression, but a
lower informant ranked score of the patient’s cognitive func-
tion (CSI-D informant interview) was strongly associated with
anxiety in patients (r = 0.346, p = 0.016) and anxiety (r = 0.668,
p = 0.001) and depression in carers (r = 0.503, p = 0.017).
Patient age, sex, time elapsed since stroke, Barthel index
score, and speech, language and swallowing scores were not
associated with levels of anxiety or depression in patients or
carers.
4. Discussion
Although there has been considerable research from high-in-
come countries into psychiatric problems following stroke,
there have been few studies investigating these problems in
low and middle income countries, despite high levels of doc-
umented stroke related morbidity.29 The present study re-
veals that patients were significantly more anxious than
controls but had similar rates of depression. A weak associa-
tion was seen between levels of depression in patients and
their carers but no association in anxiety levels was found
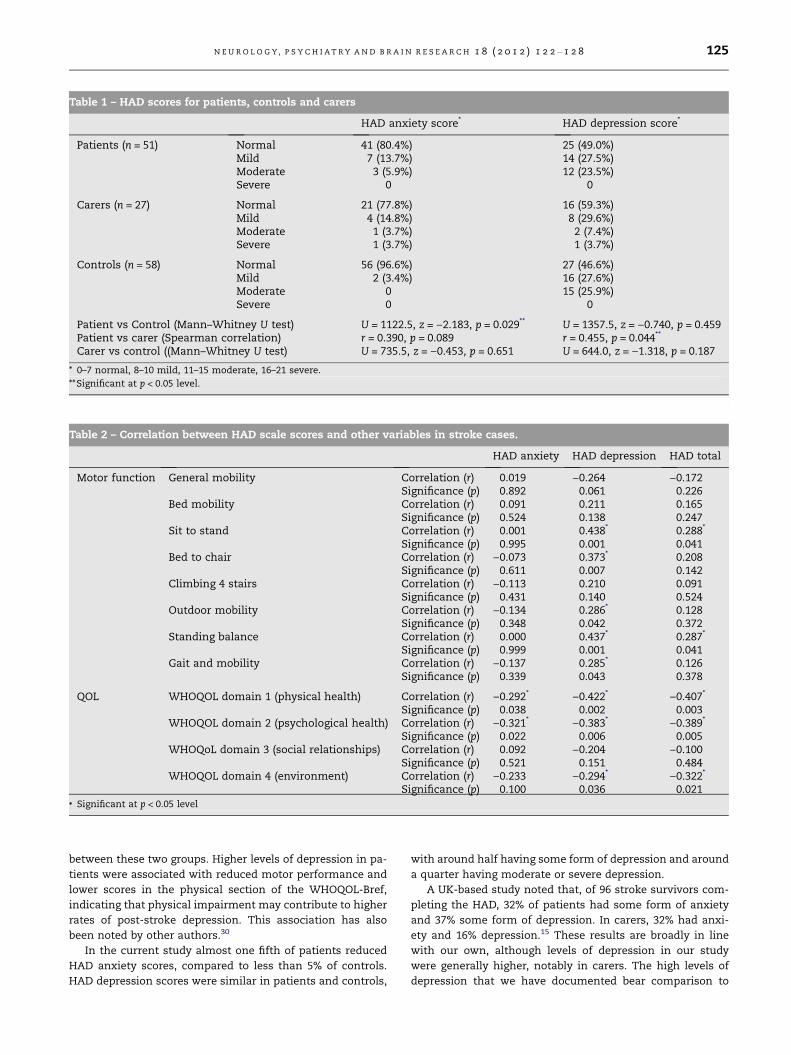
Table 2 – Correlation between HAD scale scores and other variables in stroke cases.
HAD anxiety HAD depression HAD total
Motor function General mobility Correlation (r) 0.019 )0.264 )0.172Significance (p) 0.892 0.061 0.226
Bed mobility Correlation (r) 0.091 0.211 0.165Significance (p) 0.524 0.138 0.247
Sit to stand Correlation (r) 0.001 0.438* 0.288*
Significance (p) 0.995 0.001 0.041Bed to chair Correlation (r) )0.073 0.373* 0.208
Significance (p) 0.611 0.007 0.142Climbing 4 stairs Correlation (r) )0.113 0.210 0.091
Significance (p) 0.431 0.140 0.524Outdoor mobility Correlation (r) )0.134 0.286* 0.128
Significance (p) 0.348 0.042 0.372Standing balance Correlation (r) 0.000 0.437* 0.287*
Significance (p) 0.999 0.001 0.041Gait and mobility Correlation (r) )0.137 0.285* 0.126
Significance (p) 0.339 0.043 0.378
QOL WHOQOL domain 1 (physical health) Correlation (r) )0.292* )0.422* )0.407*
Significance (p) 0.038 0.002 0.003WHOQOL domain 2 (psychological health) Correlation (r) )0.321* )0.383* )0.389*
Significance (p) 0.022 0.006 0.005WHOQoL domain 3 (social relationships) Correlation (r) 0.092 )0.204 )0.100
Significance (p) 0.521 0.151 0.484WHOQOL domain 4 (environment) Correlation (r) )0.233 )0.294* )0.322*
Significance (p) 0.100 0.036 0.021
* Significant at p < 0.05 level
Table 1 – HAD scores for patients, controls and carers
HAD anxiety score* HAD depression score*
Patients (n = 51) Normal 41 (80.4%) 25 (49.0%)Mild 7 (13.7%) 14 (27.5%)Moderate 3 (5.9%) 12 (23.5%)Severe 0 0
Carers (n = 27) Normal 21 (77.8%) 16 (59.3%)Mild 4 (14.8%) 8 (29.6%)Moderate 1 (3.7%) 2 (7.4%)Severe 1 (3.7%) 1 (3.7%)
Controls (n = 58) Normal 56 (96.6%) 27 (46.6%)Mild 2 (3.4%) 16 (27.6%)Moderate 0 15 (25.9%)Severe 0 0
Patient vs Control (Mann–Whitney U test) U = 1122.5, z = )2.183, p = 0.029** U = 1357.5, z = )0.740, p = 0.459Patient vs carer (Spearman correlation) r = 0.390, p = 0.089 r = 0.455, p = 0.044**
Carer vs control ((Mann–Whitney U test) U = 735.5, z = )0.453, p = 0.651 U = 644.0, z = )1.318, p = 0.187
* 0–7 normal, 8–10 mild, 11–15 moderate, 16–21 severe.
**Significant at p < 0.05 level.
N E U R O L O G Y, P S Y C H I A T R Y A N D B R A I N R E S E A R C H 1 8 ( 2 0 1 2 ) 1 2 2 – 1 2 8 125
between these two groups. Higher levels of depression in pa-
tients were associated with reduced motor performance and
lower scores in the physical section of the WHOQOL-Bref,
indicating that physical impairment may contribute to higher
rates of post-stroke depression. This association has also
been noted by other authors.30
In the current study almost one fifth of patients reduced
HAD anxiety scores, compared to less than 5% of controls.
HAD depression scores were similar in patients and controls,
with around half having some form of depression and around
a quarter having moderate or severe depression.
A UK-based study noted that, of 96 stroke survivors com-
pleting the HAD, 32% of patients had some form of anxiety
and 37% some form of depression. In carers, 32% had anxi-
ety and 16% depression.15 These results are broadly in line
with our own, although levels of depression in our study
were generally higher, notably in carers. The high levels of
depression that we have documented bear comparison to

126 N E U R O L O G Y, P S Y C H I A T R Y A N D B R A I N R E S E A R C H 1 8 ( 2 0 1 2 ) 1 2 2 – 1 2 8
data from other world regions. A hospital-based study
which followed up 80 patients at 3–6 months after their
stroke in Malaysia found that 51% were mildly depressed
and 15% were severely depressed.31 The authors found the
presence of depression to be associated with greater age
and poorer performance in functional activities of daily liv-
ing. However, the cohort had a mean age of only 56.8 years
and therefore may not be representative of the wider stroke
community. A door-to-door survey of 45 stroke survivors in
rural China found that 62.2% were depressed, at a mean
interval of 5.7 years post-stroke32. Furthermore, 33.4% of
1471 people from the background population were also
depressed.
In our study, the use of regular antihypertensive medica-
tion was associated with reduced levels of anxiety and
depression. Hypertension is a risk factor for stroke and has
been associated with poor outcomes.33 Research has also
shown that patients diagnosed with hypertension who
regularly use antihypertensive drugs prior to stroke have less
severe strokes and more favourable outcomes.34 Our results
indicate that the benefits of antihypertensive medication
may extend beyond physical effects and may improve psy-
chological wellbeing, possibly by helping to reassure patients
that they are taking positive action to reduce their risk of
further stroke.
Amongst carers, rates of anxiety and depression were
similar to those noted by Wilkinson et al.15 and lower than
levels noted in an Australian study by Anderson et al.35 The
Australian study looked at factors affecting distress in carers
for stroke survivors at one year post-stroke and found high
levels of anxiety (58%) and depression (50%) using the HAD
scale.35
Although very little research has been conducted in low-
income countries, a hospital-based Nigerian study noted that
22.3% of stroke caregivers had clinically significant anxiety
symptoms compared with 11.7% of controls.36 Moreover,
24.3% of caregivers reported depressive symptoms in compar-
ison with 13.6% of controls.
Interestingly, in our study increased carer anxiety and
depression levels were associated with lower informant-re-
ported cognitive function of patients, suggesting poor cogni-
tive function in patients may cause symptoms of anxiety and
depression in carers. This relationship has been noted by other
authors.35
This study has certain limitations. Firstly, the medical
care received by the cohort may not be truly representative
of the wider population of stroke survivors in SSA, as they
were involved in an incidence study and transport to hospi-
tal for assessment at the time of stroke was paid for by the
study. Secondly, people in both the case and control groups
struggled to grade their emotions and physical and mental
health status on a rating scale (HAD and WHOQOL-Bref
scores). A large number of participants had never been
asked to do this before and the reason for doing so was
not always clear to them. However, both of these scales
have previously been used to assess post stroke survivors
in SSA and the HAD has been validated in Nigeria.24 Six pa-
tients did not complete the HAD due to aphasia or dysphasia
and one patient, who was noted to have a very low mood re-
fused to complete it. It may be that these patients, who were
more severely affected by their strokes, had higher levels of
anxiety and depression but were unable to express their emo-
tions. This missing data could have influenced the signifi-
cance of our results and conclusions. However, it is likely
that all studies on the psychiatric sequelae of stroke would
have a similar limitation. Interestingly, no patients were ex-
cluded due to having dementia. We feel this may reflect the
fact that many stroke cases who had dementia may have died
prematurely prior to follow-up. This observation requires fur-
ther investigation. Finally, we recognise that there was a large
variation between cases in time since stroke. Although this is
far from ideal, and may have lowered the degree of homoge-
neity in our data, it is interesting that nether anxiety of
depression score were associated with the time elapsed since
stroke.
5. Conclusions
Low- and middle-income countries endure more than two
thirds of the worldwide stroke burden which means that a
greater understanding of stroke and its wider impact on psy-
chological health is needed to allow the planning of effective
stroke services.37 To our knowledge this is the first long-term
follow-up study of incident stroke cases in SSA which has
examined the psychological health of stroke survivors and
their carers. This research helps to characterise the impact
of post stroke anxiety and depression among a representa-
tive cohort of stroke survivors and their carers in rural
Tanzania.
Our results, together with those from other world regions,
emphasise the need for community-based rehabilitation ser-
vices. Such services should not only consider the stroke sur-
vivor but also the caregiver’s medical, social and emotional
needs. Local health workers could receive training to allow
them to identify stroke patients and carers with psychological
morbidity. This might be achieved through community-based
screening for mental health problems. Appropriate interven-
tions and treatment could then be offered to the relevant
stroke survivors and carers, including self-help guides, coun-
selling and pharmacological therapy. Additional support
through community organisations and the patient’s wider
family might also be developed to help reduce the stress
and burden on the main caregiver and allow time for leisure
and social activities.
As SSA continues to undergo demographic transition,
stroke is emerging as a leading cause of death and disability
and there is a need to develop effective rehabilitation services
in both the hospital and the community.38 These services
should not only address the physical effects of stroke but
must also tackle psychological morbidity among patients
and their carers. National and international bodies should
encourage the development of these services in order to
offset the high social and economic cost which is likely to re-
sult from the rising prevalence of stroke in the developing
world.
6. Conflicting interests
None.
N E U R O L O G Y, P S Y C H I A T R Y A N D B R A I N R E S E A R C H 1 8 ( 2 0 1 2 ) 1 2 2 – 1 2 8 127
7. Funding
This work was funded by a grant from the Wellcome Trust,
UK. They had no role in study design; in the collection, anal-
ysis and interpretation of data; in the writing of the report;
and in the decision to submit the article for publication.
Acknowledgements
We would like to thank all health-care workers, officials,
carers and family members who helped in the identification
of patients, the inputting of data and in the examination
and assessment process. We would also like to acknowledge
Professor Nigel Unwin and Professor George Alberti, who
were part of the TSIP study group, for their helpful advice.
R E F E R E N C E S
1. Strong K, Mathers C, Bonita R. Preventing stroke: saving livesaround the world. Lancet Neurol 2007;6(2):182–7.
2. Howitt SC, Jones MP, Jusabani A, et al. A cross-sectional studyof quality of life in incident stroke survivors in rural northernTanzania. J Neurol 2011;258:1422–30.
3. Larson J, Franzen-Dahlin A, Billing E, von Arbin M, Murray V,Wredling R. Predictors of quality of life among spouses ofstroke patients during the first year after the stroke event.Scand J Caring Sci 2005;19:439–45.
4. Nelson LD, Cicchetti D, Satz P, Sowa M, Mitrushina M.Emotional sequelae of stroke – a longitudinal perspective. JClin Exp Neuropsychol 1994;16(5):796–806.
5. Parikh RM, Robinson RG, Lipsey JR, Starkstein SE, Fedoroff JP,Price TR. The impact of poststroke depression on recovery inactivities of daily living over a 2-year follow-up. Arch Neurol1990;47:785–9.
6. Morrison V, Pollard B, Johnston M, MacWalter R. Anxiety anddepression 3 years following stroke: demographic, clinical,and psychological predictors. J Psychosom Res2005;59(4):209–13.
7. Flick CL. Stroke rehabilitation. 4. Stroke outcome andpsychosocial consequences. Arch Phys Med Rehabil 1999;80(5Suppl 1):S21–S26.
8. Hackett ML, Anderson CS. Frequency, management, andpredictors of abnormal mood after stroke: the AucklandRegional Community Stroke (ARCOS) study, 2002 to 2003.Stroke 2006;37(8):2123–8.
9. Owolabi MO. Determinants of health-related quality of life inNigerian stroke survivors. Trans R Soc Trop Med Hyg2008;102(12):1219–25.
10. Starkstein SE, Cohen BS, Fedoroff P, Parikh RM, Price TR,Robinson RG. Relationship between anxiety disorders anddepressive-disorders in patients with cerebrovascular injury.Arch Gen Psychiatry 1990;47(3):246–51.
11. Astrom M. Generalized anxiety disorder in stroke patients. A3-year longitudinal study. Stroke 1996;27(2):270–5.
12. Bhogal SK, Teasell RW, Foley NC, Speechley MR. Communityreintegration after stroke. Top Stroke Rehabil2003;10(2):107–29.
13. King RB. Quality of life after stroke. Stroke 1996;27(9):1467–72.14. Jones AL, Charlesworth JF, Hendra TJ. Patient mood and carer
strain during stroke rehabilitation in the community
following early hospital discharge. Disabil Rehabil2000;22(11):490–4.
15. Wilkinson PR, Wolfe CDA, Warburton FG, Rudd AG, HowardRS, Ross-Russell RW, et al. A long-term follow-up of strokepatients. Stroke 1997;28(3):507–12.
16. Anderson CS, Linto J, Stewart-Wynne EG. A population-basedassessment of the impact and burden of caregiving for long-term stroke survivors. Stroke 1995;26(5):843–9.
17. Walker RW, McLarty DG, Kitange HM, et al. Stroke mortalityin urban and rural Tanzania. Lancet 2000;355(9216):1684–7.
18. Akinpelu AO, Gbiri CA. Quality of life of stroke survivors andapparently healthy individuals in south-western Nigeria.Physiother Theory Pract 2009;25(1):14–20.
19. Mshana G, Hampshire K, Panter-Brick C, Walker R. Urban-rural contrasts in explanatory models and treatment-seeking behaviours for stroke in Tanzania. J Biosoc Sci2008;40(1):35–52.
20. Fatoye FO, Komolafe MA, Eegunranti BA, Adewuya AO,Mosaku SK, Fatoye GK. Cognitive impairment and quality oflife among stroke survivors in Nigeria. Psychol Rep 2007;100(3pt 1):876–82.
21. Walker R, Whiting D, Unwin N, et al. Stroke incidence in ruraland urban Tanzania: a prospective, community-based study.Lancet Neurol 2010 Aug;9(8):786–92.
22. WHO Monica Project. The World Health OrganizationMONICA Project (monitoring trends and determinants incardiovascular disease): a major international collaboration.WHO MONICA Project Principal Investigators. J Clin Epidemiol1988;41(2):105–14.
23. Zigmond AS, Snaith RP. The hospital anxiety and depressionscale. Acta Psychiatrica Scand 1983;67(6):361–70.
24. Abiodun OA. A validity study of the hospital anxiety anddepression Scale in general hospital units and a communitysample in Nigeria. Br J Psychiatry 1994;165:669–72.
25. The WHOQOL Group. Development of the World HealthOrganization WHOQOL-BREF quality of life assessment.Psychol Med 1998;28(3):551–8.
26. Hall KS, Hendrie HC, Brittain HM, Norton JA, Rodgers DD,Prince CS, et al. The development of a dementia screeninginterview in 2 distinct languages. Int J Meth Psychiatry Res1993;3(1):1–28.
27. Mahoney FI, Barthel D. Functional evaluation: the Barthelindex. Md. Med J 1965;14:56–61.
28. Medical Research Council. Aids to the Investigation ofPeripheral Nerve Injuries. War Memorandum. (revised 2ndedition). London: HMSO; 1943.
29. The SASPI Project Team. Prevalence of stroke survivors inrural South Africa: results from the Southern Africa StrokePrevention Initiative (SASPI) agincourt field site. Stroke2004;35:627–32.
30. Robinson RG, Starr LB, Lipsey JR, Rao K, Price TR. A two-year longitudinal study of post-stroke mood disorders:dynamic changes in associated variables over the first sixmonths of follow-up. Stroke 1984;15:510–7.
31. Glamcevski 2nd MT, Pierson J. Prevalence of and factorsassociated with poststroke depression: a Malaysian study. JStroke Cerebrovasc Dis 2005;14(4):157–61.
32. Fuh JL, Liu HC, Wang SJ, Liu CY, Wang PN. Poststrokedepression among the Chinese elderly in a rural community.Stroke 1997 Jun;28(6):1126–9.
33. Paithankar MM, Dadhi RD. Functional recovery in ischaemicstroke. Neurol India 2003;51(3):414–6.
34. Vibo R, Korv J, Roose M. One-year outcome after first-everstroke according to stroke subtype, severity, risk factors andpre-stroke treatment. A population-based study from Tartu,Estonia. Eur J Neurol 1997;14:435–9.

128 N E U R O L O G Y, P S Y C H I A T R Y A N D B R A I N R E S E A R C H 1 8 ( 2 0 1 2 ) 1 2 2 – 1 2 8
35. Anderson CS, Linto J, Stewart-Wynne EG. A population-basedassessment of the impact and burden of caregiving for long-term stroke survivors. Stroke 1995 May;26(5):843–9.
36. Fatoye FO, Komolafe MA, Adewuya AO, Fatoye GK. Emotionaldistress and self-reported quality of life among primarycaregivers of stroke survivors in Nigeria. East Afr Med J2006;83(5):271–9.
37. Fitzgerald SM, Srikanth VK, Evans RG, Thrift AG. Benefits andchallenges in stroke research in developing countries. BrainImpairment 2008;9(2):198–204.
38. Walker RW, Jusabani A, Aris E, et al. Post-stroke case fatalitywithin an incident population in rural Tanzania. NeurolNeurosurg Psychiatry. 2011;82(9):1001–5.