Embed Size (px)
Citation preview

Antithrombotic therapy for stroke prevention in patients with newly diagnosed atrial fibrillation and a history of acute coronary syndrome: the Global Anticoagulant Registry in the FIELD (GARFIELD)
Freek WA Verheugt,1 Jean-Pierre Bassand,2 Alexander GG Turpie,3 David A Fitzmaurice,4 Sylvia Haas,5 Shinya Goto,6 Gregory YH Lip,7 Iris Mueller,8 Sophie K Rushton-Smith,8 Ajay K Kakkar,8 for the GARFIELD Investigators
PURPOSE
METHODS
RESULTS
1Onze Lieve Vrouwe Gasthuis (OLVG), Amsterdam, Netherlands; 2University Hospital Jean-Minjoz, Besançon, France; 3McMaster University, Hamilton, Canada; 4Primary Care Clinical Sciences, The University of Birmingham, Birmingham, UK; 5Technical University of Munich, Munich, Germany; 6Tokai University, Kanagawa, Japan; 7University of Birmingham Centre for Cardiovascular Sciences, City Hospital, Birmingham, UK; 8Thrombosis Research Institute, London, UK
TABLE. Patient baseline characteristics: Cohort 1 of the GARFIELD Registry
DECLARATION OF INTEREST
The GARFIELD Registry is supported by an unrestricted research grant from Bayer Pharma AG.
ACKNOWLEDGEMENTS
We thank the physicians, nurses, and patients involved in the GARFIELD Registry. Peter Wilkinson(Wilkinson Associates) performed the statistical analyses.
REFERENCES
CONCLUSIONS ◆ Patients with a history of myocardial infarction have a three- to
fourfold increased risk of stroke or transient ischaemic attack.1
◆ Little is known about stroke incidence and outcomes in patients with non-valvular atrial fibrillation (AF) and a history of acute coronary syndrome (ACS).
◆ We describe the baseline characteristics and use of antithrom-botics in ACS patients with non-valvular AF from the Global Anticoagulant Registry in the FIELD (GARFIELD).
◆ Data collected at baseline included patient demographics, medical history, nature of AF, and antithrombotic treatments at diagnosis.
◆ The GARFIELD Registry is an ongoing, observational, multicentre, worldwide study of adult patients newly diagnosed with AF and at risk of stroke.3
◆ Prospectively enrolled patients were ≥18 years of age, newly diagnosed (≤6 weeks previously) with non-valvular AF, with ≥1 additional investigator-determined stroke risk factor (not limited to risk factors included in existing risk scores). For adult patients with established AF (diagnosed 6–24 months before enrolment) and ≥1 additional stroke risk factor, baseline data were collected retrospectively from the time of their diagnosis.
◆ Of 10,537 AF patients in the study population, 1048 (9.9%) had a history of ACS.
◆ In such patients, triple therapy (vitamin K antagonist [VKA], aspirin and clopidogrel) should be considered for 3–6 months (or for longer in selected patients at low bleeding risk).2
◆ This analysis from Cohort 1 describes the use of antithrombotic agents in AF patients with a history of ACS.
◆ Consecutive patients were recruited into cohort 1 (the first of 5) of the GARFIELD Registry between December 2009 and October 2011 at 543 randomly selected sites in 19 countries:◆ Asia-Pacific (n=2931, 27.8%; Australia, China, Korea, Japan);◆ Canada (n=228, 2.2%);
◆ Central/South America (n=843, 8.0%; Brazil, Mexico).
◆ Europe (n=6535, 62.0%; Austria, Denmark, Finland, France, Germany, Italy, Netherlands, Norway, Poland, Spain, Sweden, UK);
◆ Baseline characteristics for patients with a history of ACS and for the total population are given in the Table. Compared with the overall group, patients with an ACS were less likely to be female but more likely to have other risk factors.
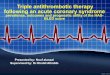
◆ Patients with an ACS history were most likely to receive a VKA alone (29.4%), VKA plus one antiplatelet (AP) (23.8%), or one AP alone (23.7%) (Figure 1).
◆ ACS patients with stenting were more likely to receive VKA plus one or more AP than those without stenting (31.0% vs 24.1%; Figure 1).
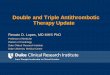
◆ Compared with the overall population, ACS patients were more likely to receive antiplatelet therapy, with or without a VKA (Figure 2).
Data are n (%) or mean (SD).BMI=body mass index. BP=blood pressure. DVT=deep vein thrombosis. GFR=glomerular filtra-tion rate. LVEF=left ventricular ejection fraction. NSAID=non-steroidal anti-inflammatory drug. PE=pulmonary embolism. TIA=transient ischaemic attack.*First-degree relative with premature cardiac history (age <55 years [male], <65 years [female]). †Data not available for 2907 patients.‡For example, central venous thrombosis, retinal occlusion. §Investigator defined.
ACS=acute coronary syndrome; AP=antiplatelet; DAPT=dual antiplatelet therapy (aspirin + adenosine diphosphate [ADP] receptor/P2Y12 receptorinhibitor); VKA=vitamin K antagonist.
◆ These contemporary observational data suggest that AF patients with a history of ACS and stenting are more likely to receive combined VKA+AP(s) therapy than VKA alone; whilst in patients without a stent, rates of VKA mono-therapy and combined use of VKA+AP(s) were similar to AF patients without an ACS.
◆ These data suggest that ESC guidelines2 for patients with AF and a history of ACS – which recommend combined use of VKAs and APs regardless of percutaneous coronary intervention for at least 3–6 months post ACS – are more frequently adopted in ACS patients with a stent than in those without.
◆ GARFIELD is the largest ongoing international academic observational study in patients newly diagnosed with non-valvular AF. The data from this initiative will provide a benchmark against which subsequent data, incorporating new therapies for AF, can be compared.
1.
2.
3..
Kannel WB. Risk factors for atherosclerotic cardiovascular outcomes in different arterial territories. J Cardiovasc Risk 1994;1:333-9.Camm AJ, Kirchhof P, Lip GY, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J 2010;31:2369-429.Kakkar AK, Mueller I, Bassand JP, et al. International longitudinal registry of patients with atrial fibrillation at risk of stroke: Global Anticoagulant Registry in the FIELD (GARFIELD). Am Heart J 2012;163:13-19 e1.
Overall population
(n=10,537)
70.2 (11.2)
4550 (43.2%)
27.5 (5.3)
3475 (35.2%)
86.7 (25.1)
2211 (21.0%)
4122 (39.1%)
8184 (77.7%)
7313 (69.4%)
3642 (34.6%)
3798 (36.0%)
2018 (19.2%)
1925 (18.3%)
2317 (22.0%)
1010 (9.6%)
1506 (14.3%)
586 (9.6%)
864 (11.3%)
155 (2.0%)
54 (0.5%)
738 (7.0%)
363 (3.4%)
149 (1.4%)
80 (0.8%)
362 (3.4%)
214 (2.3%)
297 (2.8%)
1.8 (1.2)
2.9 (1.5)
ACS patients
(n=1048)
72.1 (9.5)
292 (27.9%)
27.9 (5.0)
474 (47.5%)
86.7 (25.1)
342 (32.6%)
681 (65.0%)
864 (82.4%)
801 (76.4%)
413 (39.4%)
388 (37.0%)
1041 (99.3%)
299 (28.5%)
3516 (34.0%)
121 (11.5%)
183 (17.5%)
118 (17.3%)
135 (16.4%)
19 (2.3%)
4 (0.4%)
155 (14.8%)
76 (7.3%)
19 (1.8%)
9 (0.9%)
64 (6.1%)
15 (1.6%)
33 (3.1%)
Variable
Age (years)
Women
BMI (kg/m2)
Smoking status (current/previous)
Pulse (beats per minute)
Medical history
Congestive heart failure
Hypercholesterolaemia
Hypertension
Age >65 years
Age ≥75 years
Age 65–74 years
Coronary artery disease
Family history of cardiac disease*
Diabetes mellitus
Stroke history (with or without prior TIA)
Stroke or TIA history
LVEF ≤40%
Chronic renal disease (n=7630)†
Moderate renal dysfunction
(GFR 30–59 mL/min)
Severe renal dysfunction
(GFR <30 mL/min)
Cirrhosis
Peripheral artery disease
Carotid occlusive disease
Other thromboembolism‡
Systemic embolism
History of bleeding
Heavy alcohol consumption§
PE or DVT history
Risk scores
CHADS2
CHA2DS2-VASc
FIGURE 2 Use of antithrombotic therapies in AF patients with versus withoutan ACS
FIGURE 1 Antithrombotic use among all patients with a history of ACS, and by previous stenting
*P values are for ACS patients with vs without a stent
100
All ACS patients(n=1048)
80
60
Ra
te (
%)
40
20
0ACS with previous stent
(n=429)ACS with no previous stent
(n=619)
29.4
23.8
24.2
33.0
22.3
24.9
9.9
8.2
21.9
5.1
25.9
15.4
7.5
23.7
3.1
12.1
7.9
1.8
None(P = 0.64)*
DAPT(P = 0.008)
1 AP(P = 0.27)*
VKA + DAPT(P = 0.003)*
VKA + 1 AP(P = 0.18)*
VKA only(P = 0.002)*
50
40
30
Ra
te (
%)
20
10
0VKA + ≥1 APVKA only ≥1 AP None
ACS patients with AF (n=1048)All AF patients (n=10,537)
29.4
46.0
26.9
11.4
35.8
27.0
7.9
15.6