Embed Size (px)
Citation preview

Antioxidants for male subfertility (Review)
Showell MG, Brown J, Yazdani A, Stankiewicz MT, Hart RJ
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2011, Issue 6
http://www.thecochranelibrary.com
Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2SUMMARY OF FINDINGS FOR THE MAIN COMPARISON . . . . . . . . . . . . . . . . . . .
5BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Figure 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Figure 4. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Figure 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Figure 6. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Figure 7. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Figure 8. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Figure 9. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Figure 10. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Figure 11. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Figure 12. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Figure 13. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Figure 14. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Figure 15. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Figure 16. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Figure 17. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Figure 18. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Figure 19. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Figure 20. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Figure 21. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Figure 22. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Figure 23. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
38DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 24. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
Figure 25. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
41AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
41ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
42REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
46CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
91DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 Antioxidant(s) versus control, Outcome 1 Live Birth per couple randomised. . . . . 98
Analysis 1.2. Comparison 1 Antioxidant(s) versus control, Outcome 2 Pregnancy rate per couple randomised. . . . 99
Analysis 1.3. Comparison 1 Antioxidant(s) versus control, Outcome 3 Adverse event: Miscarriage rate per couple
randomised. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101
Analysis 1.4. Comparison 1 Antioxidant(s) versus control, Outcome 4 DNA fragmentation. . . . . . . . . . 102
Analysis 1.5. Comparison 1 Antioxidant(s) versus control, Outcome 5 Sperm total motility at 3 months or less. . . 102
Analysis 1.6. Comparison 1 Antioxidant(s) versus control, Outcome 6 Sperm total motility at 6 months. . . . . 105
Analysis 1.7. Comparison 1 Antioxidant(s) versus control, Outcome 7 Sperm total motility at 9 months or more. . 106
Analysis 1.8. Comparison 1 Antioxidant(s) versus control, Outcome 8 Sperm concentration at 3 months or less. . . 107
Analysis 1.9. Comparison 1 Antioxidant(s) versus control, Outcome 9 Sperm concentration at 6 months. . . . . 109
Analysis 1.10. Comparison 1 Antioxidant(s) versus control, Outcome 10 Sperm concentration at 9 months or more. 110
Analysis 1.11. Comparison 1 Antioxidant(s) versus control, Outcome 11 Total sperm motility over time. . . . . 111
iAntioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.12. Comparison 1 Antioxidant(s) versus control, Outcome 12 Sperm concentration over time. . . . . 113
Analysis 1.13. Comparison 1 Antioxidant(s) versus control, Outcome 13 Side effects. . . . . . . . . . . . 114
Analysis 1.18. Comparison 1 Antioxidant(s) versus control, Outcome 18 Pregnancy. . . . . . . . . . . . . 117
Analysis 2.1. Comparison 2 Live birth versus pregnancy, Outcome 1 Live birth. . . . . . . . . . . . . . 118
Analysis 3.1. Comparison 3 Head to head antioxidant(s), Outcome 1 Pregnancy per couple randomised. . . . . 119
Analysis 3.2. Comparison 3 Head to head antioxidant(s), Outcome 2 Sperm total motility at 3 months or less. . . 120
Analysis 3.3. Comparison 3 Head to head antioxidant(s), Outcome 3 Sperm total motility at 6 months. . . . . . 121
Analysis 3.4. Comparison 3 Head to head antioxidant(s), Outcome 4 Sperm total motility at 9 months or more. . . 122
Analysis 3.5. Comparison 3 Head to head antioxidant(s), Outcome 5 Sperm concentration at 3 months or less. . . 123
Analysis 3.6. Comparison 3 Head to head antioxidant(s), Outcome 6 Sperm concentration at 6 months. . . . . . 124
Analysis 3.7. Comparison 3 Head to head antioxidant(s), Outcome 7 Sperm concentration at 9 months or more. . . 125
Analysis 3.8. Comparison 3 Head to head antioxidant(s), Outcome 8 Side effects. . . . . . . . . . . . . 125
126APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
135WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
135HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
135CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
135DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
136SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
136DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .
136INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iiAntioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Antioxidants for male subfertility
Marian G Showell1, Julie Brown1 , Anusch Yazdani2, Marcin T Stankiewicz3 , Roger J Hart4
1Obstetrics and Gynaecology, University of Auckland, Auckland, New Zealand. 2Clinical Research and Development, Queensland
Fertility Group, Woolloongabba, Australia. 3Reproductive Medicine, Flinders Reproductive Medicine, Bedford Park, Australia. 4School
of Women’s and Infants Health, The University of Western Australia, King Edward Memorial Hospital and Fertility Specialists of
Western Australia, Subiaco, Australia
Contact address: Marian G Showell, Obstetrics and Gynaecology, University of Auckland, Park Road Grafton, Auckland, New Zealand.
Editorial group: Cochrane Menstrual Disorders and Subfertility Group.
Publication status and date: Edited (no change to conclusions), published in Issue 6, 2011.
Review content assessed as up-to-date: 21 August 2010.
Citation: Showell MG, Brown J, Yazdani A, Stankiewicz MT, Hart RJ. Antioxidants for male subfertility. Cochrane Database ofSystematic Reviews 2011, Issue 1. Art. No.: CD007411. DOI: 10.1002/14651858.CD007411.pub2.
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Between 30% to 80% of male subfertility cases are considered to be due to the damaging effects of oxidative stress on sperm. Oral
supplementation with antioxidants may improve sperm quality by reducing oxidative stress.
Objectives
This Cochrane review aimed to evaluate the effect of oral supplementation with antioxidants for male partners of couples undergoing
assisted reproduction techniques (ART).
Search strategy
We searched the Cochrane Menstrual Disorders and Subfertility Group Register, CENTRAL (The Cochrane Library), MEDLINE,
EMBASE, CINAHL, PsycINFO and AMED databases (from their inception until Febuary 2010), trial registers, sources of unpublished
literature, reference lists and we asked experts in the field.
Selection criteria
We included randomised controlled trials comparing any type or dose of antioxidant supplement (single or combined) taken by the
male partner of a couple seeking fertility assistance with placebo, no treatment or another antioxidant. The outcomes were live birth,
pregnancy, miscarriage, stillbirth, sperm DNA damage, sperm motility, sperm concentration and adverse effects.
Data collection and analysis
Two review authors independently assessed studies for inclusion and trial quality, and extracted data.
Main results
We included 34 trials with 2876 couples in total.
Live birth: three trials reported live birth. Men taking oral antioxidants had an associated statistically significant increase in live birth
rate (pooled odds ratio (OR) 4.85, 95% CI 1.92 to 12.24; P = 0.0008, I2 = 0%) when compared with the men taking the control.
This result was based on 20 live births from a total of 214 couples in only three studies.
1Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Pregnancy rate: there were 96 pregnancies in 15 trials including 964 couples. Antioxidant use was associated with a statistically significant
increased pregnancy rate compared to control (pooled OR 4.18, 95% CI 2.65 to 6.59; P < 0.00001, I2 = 0%).
Side effects: no studies reported evidence of harmful side effects of the antioxidant therapy used.
Authors’ conclusions
The evidence suggests that antioxidant supplementation in subfertile males may improve the outcomes of live birth and pregnancy
rate for subfertile couples undergoing ART cycles. Further head to head comparisons are necessary to identify the superiority of one
antioxidant over another.
P L A I N L A N G U A G E S U M M A R Y
Antioxidants for male subfertility
Oxidative stress may cause sperm cell damage. This damage can be reduced by the body’s own natural antioxidant defences. Antioxidants
can be part of our diet and taken as a supplement. It is believed that in many cases of unexplained subfertility, and also in instances
where there may be a sperm-related problem, taking an oral antioxidant supplement may increase a couple’s chance of conceiving when
undergoing fertility treatment. This review identified 34 randomised controlled trials involving 2876 couples. Pooled findings support
increases in live births and pregnancy rates with the use of antioxidants by the male partner. Further work is recommended to confirm
these findings.
2Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

S U M M A R Y O F F I N D I N G S F O R T H E M A I N C O M P A R I S O N [Explanation]
Antioxidant/s versus control for male subfertility
Patient or population: patients with male subfertility
Settings:
Intervention: Antioxidant/s versus control
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Control Antioxidant/s versus
control
Live Birth per couple
randomised
Follow-up: 6 - 24 months
20 per 1000 90 per 1000
(38 to 200)
OR 4.85
(1.92 to 12.24)
214
(3 studies)
⊕⊕©©
low1,2
Pregnancy rate per cou-
ple randomised
Follow-up: 3-24 months
31 per 1000 118 per 1000
(78 to 174)
OR 4.18
(2.65 to 6.59)
964
(15 studies)
⊕⊕⊕©
moderate3
Adverse event: Miscar-
riage rate per couple
randomised
Follow-up: 6-18 months
19 per 1000 29 per 1000
(6 to 124)
OR 1.54
(0.32 to 7.3)
242
(3 studies)
⊕⊕⊕©
moderate4
Total spermmotility over
time - Total sperm motil-
ity at 3 months or less
Follow-up: 4-24 weeks
The mean Total sperm
motility over time - To-
tal sperm motility at 3
months or less in the in-
tervention groups was
13.47 higher
(3.45 to 23.49 higher)
454
(10 studies)
⊕©©©
very low5,6
3A
ntio
xid
an
tsfo
rm
ale
sub
fertility
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

Sperm
concentration over time
- Sperm concentration at
3 months or less
Follow-up: 4-36 weeks
The mean Sperm con-
centration over time -
Sperm concentration at 3
months or less in the in-
tervention groups was
6.79 higher
(5.09 lower to 18.66
higher)
302
(7 studies)
⊕©©©
very low7,8
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; OR: Odds ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 The trials lacked adequate explanation for methods of randomisation, allocation concealment and blinding2 wide confidence intervals3 Only 6 trials gave adequate explanation for randomisation and allocation concealment4 Total number of events = 75 Very high heterogeneity and remained high after sensitivity analysis6 Wide confidence intervals7 Very high heterogeneity8 Wide confidence intervals
4A
ntio
xid
an
tsfo
rm
ale
sub
fertility
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

B A C K G R O U N D
Description of the condition
Eighty million people worldwide are affected by the inability to
have children (Tournaye 2006). Delayed conception affects 15%
of couples trying to conceive (Attia 2007) and male factor subfer-
tility accounts for up to 50% of these cases. A review by Tremellen
(Tremellen 2008) notes that one man in 20 will be affected by
subfertility.
Some 30% to 80% of male factor subfertility cases are said to be
due to the damaging effects of oxidative stress (Tremellen 2008).
Oxidative stress occurs when reactive oxygen species (ROS) over-
come the semen’s natural antioxidant defences and cause cellular
damage (Tremellen 2008). Some studies have suggested that sperm
production and quality has decreased over the past few decades
(Stankiewicz 2003). The increased levels of ROS are thought to be
due to environmental factors such as high temperatures, electro-
magnetic radiation, pesticides and pollution; and lifestyle factors
of advanced age, alcohol consumption, smoking, stress, obesity
and poor diet. Other factors include infections, autoimmunity and
chronic disease (Aitken 2007; Alvarez 2003; Tremellen 2008).
Spermatozoal membranes are rich in poly-unsaturated fatty acids
and are susceptible to oxygen damage from lipid peroxida-
tion (Sheweita 2005). Abnormal spermatozoa and contaminating
leukocytes generate ROS (Sikka 1995).
Antioxidants that are naturally found in semen include vitamins E
and C, superoxide dismutase, glutathione and thioredoxin (Omu
2008). These antioxidants act as free radical scavengers that help
to overcome ROS. Subfertile men have been identified as hav-
ing lower levels of antioxidants in their semen compared to fertile
men (Tremellen 2007). A study by Bykova (Bykova 2007) showed
that ROS levels were significantly higher in infertile sperm sam-
ples when compared with healthy controls and that the infertile
men who provided these samples may benefit from an antioxidant
supplement.
ROS are thought to cause fertility problems in two ways, firstly by
damaging the sperm membrane thus affecting the sperm motil-
ity and the ability of the spermatozoa to break down the oocyte
membrane; and secondly by altering the sperm DNA. Spermato-
zoal DNA integrity is one of the major determinants of normal
fertilisation and embryo growth in natural and assisted conception
(Agarwal 2003; Aitken 2004; Tarozzi 2007). Indeed, many men
with normal seminal parameters may have a high degree of sperm
DNA damage and this correlates with a poor chance of natural
conception (Boe-Hansen 2006).
Sperm DNA damage or integrity can be assessed in a number of
ways. These include sperm chromatin structural assay by flow cy-
tometry (SCSA); enzymatic labelling of broken DNA strands, the
terminal deoxynucleotide transferase-mediated nick end-labelling
assay (TUNEL); and microscopic observations of DNA fragments,
the Comet assay. The greatest experience with and standardisa-
tion of exists for the SCSA (Aitken 2007; Evenson 2007). Indeed
there are advocates who state that this should be part of a stan-
dard assessment of the male partner when a couple presents with
subfertility (Boe-Hansen 2006); although it is recognised that the
technique has its limitations and hence strict laboratory control
and standardisation is required (Boe-Hansen 2005).
Sperm DNA fragmentation does not appear to influence fertilisa-
tion in in vitro fertilisation (IVF), although a negative correlation
of sperm DNA damage with embryo or blastocyst development has
been described (Evenson 2006; Li 2006; Tarozzi 2007). Women
undergoing intrauterine insemination with a sperm DNA frag-
mentation index < 30%, as measured by the SCSA, are seven times
more likely to achieve a pregnancy than those couples where the
male partner had a higher degree of sperm DNA damage (Evenson
2006). The evidence for the effect of a high degree of sperm DNA
damage upon pregnancy outcome is less clear. A meta-analysis of
sperm DNA fragmentation assessed by the SCSA determined that
if the sperm DNA fragmentation was < 30% the couple were twice
as likely to conceive in an IVF cycle than if it was greater than 30%,
though the evidence for a benefit in women undergoing intra-
cytoplasmic sperm injection (ICSI) was unclear (Evenson 2006).
However, a meta-analysis of SCSA papers published in the same
year demonstrated conflicting results (Li 2006). This meta-analy-
sis found that there was no effect of sperm DNA damage assessed
by the SCSA assay upon the outcome of IVF or ICSI (Li 2006).
The meta-analysis also reviewed the effect of sperm DNA damage
as assessed by the TUNEL assay. This demonstrated a reduced
pregnancy rate in women undergoing IVF when the male partner
had a high degree of sperm DNA damage, but no difference if they
were undergoing ICSI (Li 2006). It also appears that miscarriage
is more likely in women undergoing assisted reproduction when
the sperm DNA damage is high (Borini 2006).
Description of the intervention
Antioxidants are both biological (enzymes) and chemical sub-
stances that reduce oxidative damage. The chemical antioxidants
are both natural and synthetic. These can be derived from nutri-
tional sources and from supplementation (Sikka 1995). The pre-
dominant supplementary antioxidants that are studied in male
subfertility clinical trials are vitamin E, vitamin C, carotenoids,
ubiquinol and the micronutrients folate and zinc (Eskenazi 2005).
A paper by Tremellen (Tremellen 2008) discussed the use of a
combination of vitamins and minerals to improve pregnancy rates
for subfertile men.
Polyunsaturated fatty acids (PUFAs) are sources of antioxidants
and are commonly taken in the community as nutritional supple-
ments. PUFAs have varying effects in male fertility. They provide
antioxidants and also increase the plasma fluidity of the sperm
membrane which acts to assist with conception, however this fluid-
ity makes the sperm susceptible to reactive oxygen species and lipid
peroxidation that can damage the sperm (Wathes 2007). Wathes
states that “It appears that PUFAs are a two edged sword - some
5Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

are essential, but too many are potentially harmful” (Wathes 2007,
page198). An open study by Comhaire attempted to overcome
the double edged sword of essential fatty acid supplements by also
treating the subfertile men in their study with antioxidant sup-
plements of acetyl cysteine or beta-carotene and alpha-tocopherol
(Comhaire 2000).
PUFAs are classified into omega-3, omega-6 and omega-9.
Omega-9 is synthesised by animals but omegas-3 and 6 need to be
supplemented in the diet. The main sources of omega-6 are veg-
etable oils. Sources of omega-3 are vegetable and fish oils (Wathes
2007).
Antioxidants are widely available and inexpensive when compared
to other fertility treatments however this review did not include
any cost benefit analysis.
How the intervention might work
Antioxidants are known to scavenge and dispose of ROS, suppress
their formation and also act to oppose the actions of ROS (Sikka
1995). The dietary intake of antioxidants has been shown to be
critically important for semen quality. Some clinical trials of an-
tioxidant supplementation have shown an associated increase in
fertilisation rates, possibly by reducing oxidative stress, lipid per-
oxidation potential and ROS levels (Eskenazi 2005).
Why it is important to do this review
Currently there is limited evidence that antioxidant supplemen-
tation improves outcomes for subfertile couples. Although some
clinical trials of supplemental antioxidants have suggested benefits
in treating male subfertility there are other trials that fail to demon-
strate the same benefit (Agarwal 2004). Tournaye (Tournaye 2006)
described the consensus on the treatment of unexplained male
subfertility with antioxidants as potentially beneficial but stated a
need for further evaluation. The purpose of this Cochrane review
was to assess the effects of antioxidants on men with documented
sperm DNA damage and men with impaired semen parameters
from appropriate clinical trials that use the clinically relevant pa-
rameters of live birth and pregnancy. The review also assessed the
effectiveness of different antioxidants and dosages on these out-
comes.
O B J E C T I V E S
The objective of this review was to determine whether supple-
mented oral antioxidants compared to placebo, no treatment or
another antioxidant improve outcomes for couples with a subfer-
tile male partner. Couples were undergoing assisted reproduction
technologies (ART) such as in vitro fertilisation (IVF), intrauterine
insemination (IUI) or intracytoplasmic sperm injection (ICSI).
The main questions asked in this review were whether:
1. supplemented oral antioxidants improve outcomes for couples
with male factor infertility or unexplained infertility who are un-
dergoing ART;
2. different types of antioxidants given to men have varying effects
in this setting.
M E T H O D S
Criteria for considering studies for this review
Types of studies
Inclusion criteria
• Only randomised controlled trials were eligible for
inclusion. The participants were randomised to antioxidant
versus placebo, an alternative antioxidant, or no treatment.
• Only pre-crossover data were used from randomised
crossover trials, as achieving outcomes such as pregnancy and live
birth precluded couples entering the next trial phase (Dias 2006).
Exclusion criteria
• Any quasi-randomised trials
Types of participants
Inclusion criteria
• Trials that included men who were part of a couple with
male factor subfertility or unexplained subfertility and who were
undergoing ART using their own gametes.
In situations where individuals were randomised again following
failed cycles the data would not be pooled in a meta-analysis unless
individual data could be excluded.
Exclusion criteria
• Trials that included men taking any other fertility
enhancing drugs
• Trials that included men who had had chemotherapy
treatment
6Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Types of interventions
• Trials were included if they investigated any type of
chemical supplementary antioxidant
• Trials were included if they investigated individual or
combined antioxidants (including head to head comparisons)
• Any dose of antioxidant was included
• Trials using only the oral route of administration were
included
Types of outcome measures
Primary outcomes
• Live birth rate per couple randomised
Secondary outcomes
• Pregnancy rate per couple
• Miscarriage rate per couple, or spontaneous abortion
• Stillbirth rate per couple
• Level of sperm DNA damage after treatment
• Sperm concentration
• Sperm motility
• Adverse effects or side effects associated with antioxidant
supplementation, or as was reported by the trial. Withdrawal
numbers due to individual adverse effects were reported
Search methods for identification of studies
See the Cochrane Menstrual Disorders and Subfertility
Group (MDSG) for methods used in reviews, as stated in
their Module (http://www.mrw.interscience.wiley.com/cochrane/
clabout/articles/MENSTR/frame.html).
All reports that described randomised controlled trials of oral an-
tioxidant supplementation for subfertile men were to be found
using the following strategy.
Electronic searches
(1) The Menstrual Disorders and Subfertility Group Specialised
Register of controlled trials was searched by the Group’s Trial
Search Coordinator using the terms ’male subfertility’ or ’In vitro
fertilisation’ or ’IVF’ or ’Intracytoplasmic sperm injection’ or
’ICSI’ AND ’antioxidants’ or ’vitamin e’ or ’vitamin’ or ’ascorbic
acid’ or ’zinc’ or ’folate’ or ’selenium’ or ’glutathione’ or ’ubiquinol’
or ’carnitine’ or ’astaxanthin’ or ’coenzyme Q10’ or ’lycopene’ or
’Menevit’ or “carnitine” or “carnitine” or “ascorbic acid” or “zinc”
or “fatty acids” or “oil” or “fish oils” or “plant extracts” in the titles,
abstracts and keywords (from inception to 22.08.10) (Appendix
7).
This register also contains unpublished trial abstracts. These were
found by handsearching 20 relevant journals and conference pro-
ceedings.
(2) The following databases were searched using the Ovid plat-
form:
• Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library 2010, Issue 3) (Appendix 3);
• MEDLINE (inception to 22.08.10) (Appendix 1);
• EMBASE (2008 to 22.08.10) (Appendix 2);
• CINAHL (Cumulative Index to Nursing and Allied Health
Literature) (1980 to 22 August 2010) (Appendix 4);
• PsycINFO (inception to 22.08.10) (Appendix 5);
• AMED (Allied and Complementary Medicine) (inception
to 22 August 2010) (Appendix 6).
Both indexed and free text terms were used.
The MEDLINE search was combined with the Cochrane highly
sensitive search strategy for identifying randomised trials, which
appears in the Cochrane Handbook of Systematic Reviews of In-
terventions (Version 5.0.1 chapter 6, 6.4.11).
The EMBASE and CINAHL searches were combined with trial fil-
ters developed by the Scottish Intercollegiate Guidelines Network
(SIGN) (www.sign.ac.uk/mehodology/filters.html#random).
Searches were not limited to any one language.
Searching other resources
Appropriate journals were handsearched for trial conference ab-
stracts. These journals included ’Human Reproduction’ which
contains abstract supplements for the European Society of Hu-
man Reproduction and Embryology (ESHRE) and ’Fertility and
Sterility’ which contains abstract supplements for the ’American
Society for Reproductive Medicine’ (ASRM). Lists of journals
handsearched by the Menstrual Disorders and Subfertility Group
(MDSG) are found in the MDSG Module.
Research registers were searched for ongoing and recently com-
pleted trials:
• ’ClinicalTrials.gov’, a service of the US national Institutes of
Health (http://clinicaltrials.gov/ct2/home) (last searched 6
August 2010);
• ’The World Health Organization International Trials
Registry Platform search portal’ (www.who.int/trialsearch/
Default.aspx) (last searched August 2010).
Conference abstracts were found on the ISI Web of Knowledge:
http://isiwebofknowledge.com/ (last searched 6 August 2010).
OpenSIGLE database was searched for European grey literature:
http://opensigle.inist.fr/ (last searched 6 August 2010).
Citation lists from review articles and other relevant publications
were searched.
Personal communication with manufacturers, experts and special-
ists in the field.
7Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Data collection and analysis
Selection of studies
Two people were responsible for independently selecting the tri-
als. Titles and abstracts from the searches were scanned. We ob-
tained the full text of those articles that appeared to be eligible
for inclusion. On assessment they were then placed in included
(Characteristics of included studies), excluded (Characteristics of
excluded studies), ongoing (Characteristics of ongoing studies)
studies or studies awaiting assessment (Characteristics of studies
awaiting classification). One of these individuals is a content ex-
pert. Any disagreements were resolved through consensus or by a
third party.
Studies were appraised in an unblinded fashion, as recommended
by the Cochrane Menstrual and Fertility Disorders Group. Further
information, where required, was sought from the authors
Data extraction and management
The studies that appeared to meet the inclusion criteria were in-
dependently assessed by the two review authors (MS and JB) us-
ing data extraction forms. Any discrepancies were resolved with
discussion.
The data extraction forms included methodological quality and al-
location information. This information was included in the review
and presented in the characteristics of included and excluded stud-
ies tables (see Characteristics of included studies; Characteristics of
excluded studies) following the guidance of the Cochrane Hand-
book for Systematic Reviews of Interventions (Higgins 2006).
Assessment of risk of bias in included studies
The included studies were assessed for risk of bias using the
Cochrane risk of bias assessment tool to assess: sequence genera-
tion; allocation concealment; blinding of participants, providers
and outcome assessors; completeness of outcome data; selective
outcome reporting; and other potential sources of bias. MS and JB
assessed these six criteria; any disagreements were resolved by con-
sensus or by discussion with a third author. The conclusions were
presented in the ’Risk of bias’ table (Characteristics of included
studies) and incorporated into the interpretation of review findings
by means of sensitivity analyses. Where identified studies failed to
report the primary outcome of live birth, but did report interim
outcomes such as pregnancy, informal assessment was undertaken
on whether those reporting the primary outcomes had typical val-
ues for the interim outcomes.
If other potential sources of bias were identified in advance, these
were specified and the number of criteria increased accordingly.
Sensitivity analyses were specified later, under the appropriate
heading.
The authors aimed to minimise reporting bias, publication bias,
within trial reporting bias and their potential impact by ensuring
that a comprehensive search for eligible studies was carried out.
Authors were also alert to duplication of data. As there were 10
or more studies in the analysis, a funnel plot was used to explore
the possibility of small study effects (a tendency for estimates of
the intervention effect to be more beneficial in smaller studies).
Care was taken to search for within study reporting bias, such
as trials failing to report obvious outcomes or reporting them in
insufficient detail to allow inclusion.
Measures of treatment effect
The dichotomous data for live birth, pregnancy rate, miscarriage,
stillbirth, and adverse events were expressed as odds ratios (OR)
with 95% confidence intervals (95% CI) and combined in a meta-
analysis with Rev Man software using the Peto method and a fixed-
effect model (Higgins 2006). The OR has mathematically sound
properties that are consistent with benefit or harm and work well in
small samples with rare events. This effect measure is appropriate
when considering subfertility. For continuous data (for example
sperm quality measurements) mean differences between treatment
groups were calculated with associated standard deviations and
95% confidence intervals. These were displayed on forest plots, if
possible.
Attempts were made to contact all authors of the included trials
that reported data in a form that was not suitable for meta-analysis,
for example data reported in medians or ranges. Where additional
data were not forthcoming the data were reported under ’other
data’ and not included in the meta-analysis.
Unit of analysis issues
The outcomes of live birth and pregnancy were analysed as per
couple randomised. The sperm outcomes analyses were per man
randomised. We included both parallel and crossover trials, using
only the first phase of the crossover trial.
Dealing with missing data
We attempted to contact the authors of the trials with any missing
data by email or post. If there was no reply, and if possible, we
reported the data in terms of intention to treat. If this was not
possible the trials were placed in ’studies awaiting assessment’.
Assessment of heterogeneity
The authors considered whether the clinical and methodological
characteristics of the included studies were sufficiently similar to
provide a meaningful summary in a meta-analysis.
Heterogeneity between the treatment effects of different studies
were studied by looking at the points on the forest plot, the overlap
of confidence intervals (a poor overlap indicates heterogeneity),
and the Chi2 statistical test for heterogeneity. A low P value (or a
8Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

large Chi2 statistic relative to its degree of freedom) shows evidence
of heterogeneity of treatment effects, or that the differences were
not likely to be by chance (Higgins 2006). If there was only a small
number of trials or they had small sample sizes then a P value of
0.10 rather than 0.05 was used to show heterogeneity. To more
formally quantify the variations between the studies the I2 statistic
was used (Higgins 2006). This statistic describes the variation in
effect estimates due to heterogeneity rather than by chance, as a
percentage. If a value over 50% was found we assumed that there
was large heterogeneity.
Assessment of reporting biases
If there was a question of publication bias, a funnel plot was drawn.
A gap on either side of the graph would have given a visual indi-
cation that some trials have not been identified (Higgins 2006).
This is often due to the difficulties in locating unpublished trials.
If there were outcomes with no data the review included empty
data tables. This indicates that further clinical trials need to be
conducted in this area. It also allows for updating, when new data
may be found.
Data synthesis
Statistical analysis of the data was carried out using Review Man-
ager 5 (RevMan 5). Pregnancy outcomes are considered positive
and higher numbers of pregnancy rates are considered a benefit.
The outcomes of miscarriage and adverse events are negative ef-
fects and higher numbers would be considered harmful. These
aspects have to be considered when assessing the summary graphs
(Attia 2007).
The data from primary studies were combined using a fixed-effect
model in the following comparisons.
1. Antioxidants versus control (placebo or no treatment), stratified
by type of antioxidant. Further analyses of sperm motility and
concentration were carried out by sub grouping trials over time: at
three, six and nine months. Subgrouping was also performed on
the outcomes of live birth and pregnancy. Trials that reported both
of these outcomes were subgrouped into live birth and pregnancy
in order to assess any overestimation of effect in the pregnancy
outcome. Subgrouping was also performed on those trials that
reported both live birth and pregnancy and trials that only reported
pregnancy in order to assess any reporting bias in the pregnancy
outcome.
2. Antioxidants versus antioxidants or head to head stratification
by type of antioxidant. An increase in the odds of a particular out-
come, which may be beneficial (for example live birth) or detri-
mental (for example adverse effects), were displayed graphically in
the meta-analyses to the right of the centre line and a decrease in
the odds of an outcome to the left of the centre line.
The aim here was to define analyses that were comprehensive and
mutually exclusive so that all eligible study results could be be
slotted into one stratum only. Comparisons were specified so that
any trials falling within each stratum could sensibly be pooled for
meta-analysis. Stratification allowed for consideration of effects
within each stratum as well as, or instead of, an overall estimate
for the comparison.
Subgroup analysis and investigation of heterogeneity
Subgroup analysis was performed on the following.
• Trials that reported antioxidants (individual and combined)
given to men with documented elevated levels of sperm DNA
damage, as defined by the trials, who were undergoing fertility
treatment (ART). A minimum of 80% of participants in the
trials had to satisfy this criterion for inclusion. If individual data
were available these were used in preference.
• Trials that reported antioxidants (individual and combined)
given to men with impaired semen parameters who were
undergoing fertility treatment (ART). A minimum of 80% of
participants in the trials had to satisfy this criterion for inclusion.
If individual data were available these were used in preference.
• Treatment was divided into the subgroups of individual and
combined antioxidants for live birth and pregnancy outcomes.
• Subgroup analysis was also performed on those studies that
reported live birth and pregnancy in order to assess any
overestimation of effect and reporting bias.
• Subgroup analysis was also used in the sperm outcomes of
motility and concentration over time, at: three, six and nine
months.
Sensitivity analysis
We performed sensitivity analysis (using the random-effects model
in RevMan software) for the primary outcomes to assess whether
the findings from the analysis were robust. Sensitivity analysis
considered whether conclusions were any different if eligibility was
restricted to studies without high risk of bias.
We also stated that sensitivity analysis would be performed on un-
published studies. These studies may not have been peer reviewed
and thus could be of lower quality. However there were no un-
published trials in this review.
Initially trials were subgrouped according to placebo or no treat-
ment, however after statistical advice all the trials comparing an-
tioxidants to placebo and no treatment were grouped as one then
a sensitivity analysis was performed to assess any evidence of dif-
ference in effect between the placebo and the no-treatment group.
These results are described in the ’Risk of bias in included studies’
section of the review.
R E S U L T S
9Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Description of studies
See: Characteristics of included studies; Characteristics of
excluded studies; Characteristics of studies awaiting classification;
Characteristics of ongoing studies.
Results of the search
Two review authors (MS and RH) scanned the abstracts and titles
of the results of the search strings. The MEDLINE search pro-
duced 406 abstracts; there were six abstracts from CENTRAL,
three from CINAHL, 62 from EMBASE, 107 from the MSDG
database and three from PsycINFO. Two conference abstracts
were found from handsearching the conference proceedings of
the European Society for Human Reproduction and Embryology
(ESHRE) and the American Society for Reproductive Medicine
(ASRM). One title was found from reference lists in reviews.
Five non-English trials were assessed for inclusion: two Chinese,
one Bulgarian, one Japanese and one Iranian. The two Chinese
trials (Li 2005a; Li 2005 ), the Japanese trial (Akiyama 1999) and
the Iranian trial (Peivandi 2010) were included in the analysis.
The Bulgarian study (Nikolova 2007) was excluded as it did not
have random allocation (see Characteristics of excluded studies).
After removal of inappropriate and duplicate studies 53 trials re-
mained: 34 trials were included, 15 were excluded and four trials
were ongoing.
Included studies
There were 34 included trials in this review. Full details of these
trials can be seen in the table of included studies (Characteristics of
included studies). The trials came from 19 different countries and
randomised 2876 couples. Eight trials were based in Italy (Balercia
2005; Balercia 2009; Biagiotti 2003; Cavallini 2004; Galatioto
2008; Lenzi 2003; Lenzi 2004; Lombardo 2002). Three trials were
from Iran (Safarinejad 2009; Safarinejad 2009a; Peivandi 2010).
Two trials each were from USA (Dawson 1990; Sigman 2006),
Tunisia (Keskes-Ammar 2003; Nozha 2001), United Kingdom
(Kessopoulou 1995; Scott 1998), Hungary (Micic 1988; Zavaczki
2003), Kuwait (Omu 1998; Omu 2008) and China (Li 2005; Li
2005a). The remaining trials were from single countries: Japan
(Akiyama 1999), Turkey (Ciftci 2009), Canada (Conquer 2000),
France (Greco 2005), Mexico (Merino 1997), Germany (Rolf
1999), Saudi Arabia (Suleiman 1996), Australia (Tremellen 2007),
Hong Kong (Wang 1983), Netherlands (Wong 2002) and Belgium
(Zalata 1998).
Data were able to be extracted from 28 of these included trials.
The six remaining trials either did not report any data or the
continuous data were reported in medians or ranges (Biagiotti
2003; Lombardo 2002; Merino 1997; Nozha 2001; Wong 2002;
Zalata 1998), see Characteristics of included studies and the anal-
yses (Analysis 1.14; Analysis 1.15; Analysis 1.16; Analysis 1.17;
Analysis 3.9; Analysis 3.10). Attempts were made to contact all
authors of the included trials for further details and clarification.
The duration of treatment period ranged from three weeks with
three weeks follow up (Dawson 1990) to 26 weeks treatment and a
24-month follow up (Wong 2002). The longest follow-up period
was in the trial by Kessopoulou (Kessopoulou 1995), with a three-
week treatment period and a two-year follow-up period.
Three trials (Kessopoulou 1995; Sigman 2006; Tremellen 2007)
enrolled men who, as a couple, were undergoing IVF or ICSI.
There were no trials that enrolled men who were part of a couple
undergoing intrauterine insemination (IUI).
Participants
Most trials included couples who had attended a fertility clinic,
with a fertile partner and had been trying to conceive with regular
intercourse for over one year.
The mean age of the participants ranged from 20 to 52 years. Most
men in the included trials had a deficient level of spermatozoa
in the seminal fluid (oligospermia) or a low motility of sperm
in the seminal fluid (asthenospermia). Trials excluded men with
any inflammatory disease, antibody problems or chromosomal
problems and most trials stated that they did not enrol men who
smoked, took any additional medication or drank alcohol.
Details of inclusion and exclusion criteria are found in
Characteristics of included studies.
Interventions
A wide variety of antioxidants were used in the included trials. The
three comparisons were: antioxidants versus placebo, antioxidants
versus no treatment and antioxidants versus antioxidants (or head
to head).
The comparison ’antioxidants versus placebo’ included the antiox-
idants: vitamin E, combined antioxidants plus minerals, L-acetyl-
carnitine, L-carnitine, L-acetyl carnitine plus L-carnitine, pentox-
ifylline and magnesium.
The comparison ’antioxidants versus no treatment’ included: zinc,
combined antioxidants plus minerals, pentoxifylline, zinc plus vi-
tamin E, zinc plus vitamin E plus vitamin C.
In the analysis placebo and no treatment groups were grouped as
one and the comparison labelled ’antioxidants versus control’.
The third comparison, head to head, was implemented in an at-
tempt to assess whether one antioxidant may be more effective
than another, as stated in the protocol. However in some cases they
may have countered each other as the treatment was also included
in the control (Balercia 2005; Omu 2008; Safarinejad 2009; Scott
1998). The antioxidants used were: L-acetyl carnitine, L-carni-
tine, L-acetyl carnitine plus L-carnitine, ethyl cysteine, vitamin E,
docosahexaenoic acid, vitamin C, selenium, vitamin B, combined
antioxidants plus minerals and N-acetyl cysteine.
Outcomes
The primary outcome for this review was as follows.
10Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

• Live birth per couple. Three trials reported live birth
(Kessopoulou 1995; Omu 1998; Suleiman 1996) in the
antioxidant versus control groups.
Secondary outcomes for this review were as follows.
• Pregnancy rate per couple, as reported by 16 trials (Balercia
2005; Balercia 2009; Cavallini 2004; Galatioto 2008; Lenzi
2003; Lenzi 2004; Li 2005; Omu 1998; Peivandi 2010; Rolf
1999; Safarinejad 2009a; Sigman 2006; Suleiman 1996;
Tremellen 2007; Wang 1983; Zavaczki 2003). Li 2005 (Li 2005)
used head to head comparisons. Balercia 2005 (Balercia 2005)
was multi-armed and used both head to head and a control while
the remaining trials investigated antioxidant versus control.
• Miscarriage rate, as reported by three trials (Omu 1998;
Suleiman 1996; Tremellen 2007) in the antioxidant versus
control comparison.
• DNA fragmentation, as reported by one trial (Greco 2005).
This trial compared antioxidant versus control.
The sperm motility and concentration outcomes were divided into
three groups: measurement at three, six and nine months or more;
the included trials measured motility and concentration at these
different points in time. This analysis was only useful in directly
comparing the same trials reporting at the three time points and
not in comparing results of meta analyses that included different
subsets of trials.
• Sperm motility at three months or less was reported by 13
trials (Akiyama 1999; Ciftci 2009; Conquer 2000; Dawson
1990; Greco 2005; Keskes-Ammar 2003; Li 2005; Micic 1988;
Omu 2008; Peivandi 2010; Scott 1998; Sigman 2006; Zavaczki
2003).
• Sperm motility at six months was measured by four trials
(Balercia 2005; Balercia 2009; Safarinejad 2009; Suleiman
1996).
• Sperm motility at nine months or more was reported by
three trials (Balercia 2005; Balercia 2009; Safarinejad 2009a).
• Sperm concentration at three months or less was reported
by nine trials in total (Akiyama 1999; Conquer 2000; Ciftci
2009; Greco 2005; Peivandi 2010; Rolf 1999; Wang 1983;
Zavaczki 2003).
• Sperm concentration at six months was reported as an
outcome by a total of five trials (Balercia 2005; Balercia 2009;
Lenzi 2004; Li 2005a; Safarinejad 2009; Wang 1983).
• Sperm concentration at nine months or more was reported
on by three trials (Balercia 2005; Balercia 2009; Safarinejad
2009a).
• Side effects were subgrouped according to the type of side
effect, as described by the trials. There were only seven trials that
reported side effects. Failure by the remaining included studies to
report adverse effects could be construed as selective reporting.
The side effects reported were mainly gastrointestinal upsets
(Cavallini 2004; Kessopoulou 1995; Safarinejad 2009a; Sigman
2006; Tremellen 2007; Zavaczki 2003). These were reported as
mild epigastria, nausea, gastric acidity, gastro-oesophageal reflux,
constipation and diarrhoea. One of the six trials (Cavallini 2004)
also reported on the side effect of euphoria. The trial by Li (Li
2005) reported that no side effects were found in either the
treatment or control groups. It should also be noted that the trial
by Cavallini (Cavallini 2004) had unexplained differences in
randomisation and analysis numbers for this outcome, and
therefore introduced some reporting bias.
Excluded studies
In total 15 trials were excluded. Six trials (Cavallini 2004a; Ebisch
2006; Pryor 2003; Rolf 1998; Tremellen 2006; Zalata 1998a) were
excluded as they reported the initial analysis or were a conference
proceeding of a later, included trial. Five trials (Comhaire 2005;
Micic 2001; Nikolova 2007; Pawlowicz 2001; Stanislavov 2009)
were excluded because they did not use a randomised sequence to
allocate the participants to the treatment and control groups. Four
trials (Ebisch 2003; Elgindy 2008; Vicari 2001; Vicari 2001a) did
not have appropriate inclusion criteria for population, outcomes
or controls. Refer to the table Characteristics of excluded studies.
Studies awaiting classification
There is one trial (Wang 2010) awaiting classification. It has not
yet been assessed.
Ongoing studies
Four trials were ongoing (Revel 2006; Sadeghi 2008; Tsafrir 2010;
Gonzalez 2009).
Risk of bias in included studies
Adequate sequence generation
All included trials were randomised. Four trials (Akiyama 1999;
Kessopoulou 1995; Lenzi 2003; Peivandi 2010) had a randomised
crossover design. In the meta-analysis only the first phase data were
used as all trials reported first and second phase data separately.
Including crossover data may introduce reporting bias due to the
fact that it is unusual for a trial to report usable data at each phase.
The remaining 30 trials had a randomised parallel group de-
sign. Only 10 trials described their methods of randomisation
(Biagiotti 2003; Galatioto 2008; Keskes-Ammar 2003; Rolf 1999;
Safarinejad 2009; Safarinejad 2009a; Scott 1998; Sigman 2006;
Tremellen 2007; Wong 2002). The predominant method was by
computer generated blocks. Some degree of selection bias may
11Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

have been present in the trials due to the high numbers of included
trials that did not describe their method of randomisation (24 out
of 34 trials).
One study (Li 2005) had a large imbalance between the interven-
tion and control groups at the randomisation stage; 150 men were
randomised: 90 into the treatment group and 60 into the control
group. This imbalance was not explained in the report. Attempts
were made to contact the author but as yet there has been no reply.
Allocation
The methods of allocation concealment were generally quite
poorly described in the included studies. Therefore there was
some risk of selection bias in the trials under review. Nine tri-
als (Cavallini 2004; Ciftci 2009; Galatioto 2008; Rolf 1999;
Safarinejad 2009; Sigman 2006; Tremellen 2007; Wong 2002;
Peivandi 2010) described their method of allocation. These meth-
ods included anonymous coloured boxes, sealed opaque envelopes
and numbered bottles.
Blinding
Seventeen trials (Balercia 2005; Balercia 2009; Cavallini 2004;
Kessopoulou 1995; Lenzi 2003; Lenzi 2004; Li 2005; Lombardo
2002; Peivandi 2010; Rolf 1999; Safarinejad 2009; Safarinejad
2009a; Scott 1998; Sigman 2006; Suleiman 1996; Tremellen
2007; Wong 2002) were described as randomised, double blind
controlled trials. The researchers and patients were blinded. Two
trials (Ciftci 2009; Dawson 1990) stated that a placebo was used
as the control but only the patients were blinded. Other trials
(Conquer 2000; Greco 2005; Merino 1997; Wang 1983; Zavaczki
2003) used a placebo as the control but did not discuss blinding.
One trial (Galatioto 2008) was open label but stated that the
pharmacy was blinded during the randomisation process. One trial
(Keskes-Ammar 2003) was described as open label however the
numeric code was withheld from the investigators and patients.
Suleiman 1996 reported that if a couple became pregnant then
the treatment was stopped; however they did not appear to stop
the placebo. This suggests that the investigators had knowledge of
whether the patients were in the placebo or antioxidant.
Incomplete outcome data
Only two trials (Balercia 2009; Galatioto 2008) actually stated
that they used intention to treat in their analysis, however most
of the included trials accounted for the participants that withdrew
from their trials and then analysed the groups in an intention-to-
treat fashion.
Four trials had over 20% withdrawal from their trials. One trial (
Keskes-Ammar 2003) had over 50% drop out rate; these men were
accounted for and the main reason given was non-compliance.
Cavallini 2004 had 30% dropout rate and reasons were provided
for 53 out of the 55 drop outs; these reasons included refusal
due to the chance of taking a placebo and preference for assisted
reproduction techniques. There also remained some confusion in
this trial on the total numbers randomised and analysed. Li 2005a
and Suleiman 1996 had slightly over 20% withdrawal from their
trials.
One trial (Suleiman 1996) had a large imbalance in numbers.
There were found to be 52 in the treatment group and 35 in the
placebo once the code had been broken at the end of the trial.
There was no indication of how the randomisation was performed
therefore the trial did not perform intention to treat. The dropouts
were however accounted for: many couples had left the region and
some simply failed to continue.
Selective reporting
There was great potential for reporting bias throughout this review
as no outcome had been consistently reported by all studies and
the key outcomes were reported by a minority of studies.
The trial by Cavallini (Cavallini 2004) had unexplained differences
in randomisation and analysis numbers and therefore may have
introduced some reporting bias.
Four trials (Balercia 2005; Balercia 2009; Scott 1998; Sigman
2006) gave pregnancy data although pregnancy as an outcome was
not stated a priori in the protocols. Li 2005a stated that pregnancy
was an outcome but did not provide the data. One trial (Wang
1983) gave follow-up data on the treatment group but no data
were supplied on the control group.
Three trials reported on the adverse event of miscarriage (
Tremellen 2007; Suleiman 1996; Omu 1998).
Six trials reported on side effects, which were mainly gas-
trointestinal (Cavallini 2004; Kessopoulou 1995; Safarinejad
2009a; Sigman 2006; Tremellen 2007; Zavaczki 2003). Cavallini
(Cavallini 2004) also reported euphoria as a side effect. The ma-
jority of included trials did not report side effects and this could
be construed as a reporting bias.
Other potential sources of bias
Funding sources were stated by nine trials (Conquer 2000;
Kessopoulou 1995; Lenzi 2003; Lombardo 2002; Omu 1998;
Peivandi 2010; Rolf 1999; Wang 1983; Zavaczki 2003). Two trials
(Conquer 2000; Wang 1983) stated that funding was from a com-
mercial source and the remaining seven obtained funding through
non-commercial avenues or university grants. However three of
these non-commercially funded trials (Kessopoulou 1995; Lenzi
2003; Zavaczki 2003) received the medication from commercial
interests.
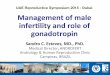
Publication bias was assessed using a funnel plot (Figure 1). Preg-
nancy outcome was used for the funnel plot as there were only two
studies in the primary outcome of live birth. The plot appeared
to be symmetrical and therefore we assumed that there was little
publication bias.
12Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 1. Funnel plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.2 Pregnancy rate per
couple randomised.
Trials comparing an antioxidant to a placebo or to no treatment
were grouped together and compared in the subgroups. Sensitivity
analysis was performed on the outcomes whereby the placebo data
were removed in order to assess whether the ’no treatment’ trials
were biasing the results. This was only possible for the outcome of
sperm motility at three months and the result remained statistically
significant. The other outcomes either contained only placebo
trials or contained only one no-treatment trial, therefore sensitivity
analysis could not be performed.
Effects of interventions
See: Summary of findings for the main comparison
Antioxidant/s versus control for male subfertility
Antioxidant(s) versus control
Live birth per couple randomised
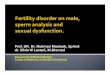
Overall there was a statistically significant difference in favour of
the antioxidant treated group compared with the control group
for live birth (pooled OR 4.85, 95% CI 1.92 to 12.24; P = 0.0008,
I2 = 0%) (Analysis 1.1). Three trials reported on this outcome
(Kessopoulou 1995; Omu 1998; Suleiman 1996). In total there
were 20 live births from a total of 214 couples randomised, 18
(15%) in the antioxidant group (n = 116) and two (2%) in the
control group (n = 98) (Figure 2). The I2 statistic in the analysis
was 0% however sensitivity analysis was performed on the trial by
Suleiman 1996 as this trial had more than 20% of participants
drop out of the trial. There remained a statistically significant
difference in favour of the antioxidant-treated group compared
with the control group for live birth (pooled OR 3.94, 95% CI
1.14 to 13.55; P = 0.03, I2 = 0%).
13Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 2. Forest plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.1 Live birth per couple
randomised.
Two trials (Kessopoulou 1995; Suleiman 1996) reported on this
outcome comparing the intervention of vitamin E versus placebo.
Kessopoulou 1995 included couples undergoing IVF or ICSI.
There was a statistically significant difference (pooled OR 6.44,
95% CI 1.72 to 24.04; P = 0.006, I2 = 0%) in the number of live
births between the antioxidant and placebo groups that favoured
the antioxidant over the placebo.
One trial (Omu 1998) reported on live births per couple ran-
domised and compared zinc versus no treatment. In total there
were 10 live births from 97 couples randomised, eight in the an-
tioxidant group (n = 49) and two in the no treatment group (n =
48). There was a statistically significant difference (OR 3.67, 95%
CI 1.00 to 13.51; P = 0.05) in the number of live births between
the antioxidant and no treatment, in favour of the antioxidant.
Pregnancy rate per couple randomised
Fifteen trials reported the outcome of pregnancy rate per cou-
ple randomised (Balercia 2005; Balercia 2009; Cavallini 2004;
Galatioto 2008; Lenzi 2003; Lenzi 2004; Omu 1998; Peivandi
2010; Rolf 1999; Sigman 2006; Safarinejad 2009a; Suleiman
1996; Tremellen 2007; Wang 1983; Zavaczki 2003). There were
964 couples in total, 515 in the antioxidant group and 449 in the
control group. In total there were 96 pregnancies, 82 (16%) in the
antioxidant group and 14 (3%) in the control group.
There was a statistically significant difference (pooled OR 4.18,
95% CI 2.65 to 6.59; P < 0.00001, I2 = 0%) (Analysis 1.2) in
the number of pregnancies between the antioxidant and control
groups in favour of the antioxidant group over the control group
(Figure 3).
14Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 3. Forest plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.2 Pregnancy rate per
couple randomised.
15Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

The trial by Cavallini 2004 included men with variocoele associ-
ated oligoasthenospermia whereas many of the other included tri-
als excluded men with variocoele (see Characteristics of included
studies). Heterogeneity was however low in this analysis and there-
fore sensitivity analysis was not performed.
Sensitivity analysis was performed on those trials (Cavallini 2004;
Suleiman 1996; Wang 1983) that reported over 20% dropouts.
There was a statistically significant difference (pooled OR 3.52,
95% CI 2.08 to 5.95; P < 0.00001, I2 = 0%) in favour of the
antioxidant group over the control group.
Two of the 15 trials included couples undergoing IVF or ICSI.
When these two trials (Sigman 2006; Tremellen 2007) were re-
moved the effect of antioxidants over control remained as a statis-
tically significant difference for the remaining trials (pooled OR
4.52, 95% CI 2.71 to 7.53; P < 0.00001, I2 = 0%), in favour
of the antioxidant over control. When these two trials (Tremellen
2007; Sigman 2006) were subgrouped together there was also a
statistically significant difference in favour of the antioxidant over
the control (pooled OR 3.06, 95% CI 1.10 to 8.47; P = 0.03, I2
= 7%).
After removing those trials that used a placebo as a control, as
opposed to no treatment, there remained a statistically significant
difference (pooled OR 4.97, 95% CI 1.63 to 15.14; P = 0.005, I2 = 0%) although the confidence intervals widened, in favour of
the antioxidant group over the no-treatment group.
Two trials (Rolf 1999; Wang 1983) were not estimable due to no
pregnancies in either the treatment or control group.
Two trials (Galatioto 2008; Omu 1998) reported on pregnancy
rate per couple randomised, comparing antioxidants versus no
treatment. In total there were 14 pregnancies from 130 couples
randomised, 12 in the treatment group (n = 69) and two in the
no-treatment group (n = 70). There was a statistically significant
difference (pooled OR 4.97, 95% CI 1.63 to 15.14; P = 0.005)
in the number of pregnancies between the antioxidant group and
the no-treatment group, in favour of the antioxidant group. No
heterogeneity was seen in this analysis (Chi2 = 0.07, I2 = 0%).
Two further comparisons were created to assess any overestimate of
benefit or reporting bias that may exist in the pregnancy analysis.
• Live birth versus pregnancy: two (Omu 1998; Suleiman
1996) out of three trials that reported on live birth and also
reported on pregnancy rate were analysed (see Figure 4). The live
birth analysis showed a statistically significant difference in
favour of the antioxidants (pooled OR 4.73, 95% CI 1.82 to
12.27; P = 0.001, I2 = 0%). This analysis had slightly lower
evidence of effect than when these same trials were analysed in
terms of the pregnancy outcome (pooled OR 5.53, 95% CI 2.34
to 13.08; P < 0.0001, I2 = 0%) (see Analysis 2.1). The results for
the two analyses appear similar therefore there is no clear
evidence of overestimation of benefit in the the full (all studies)
pregnancy analysis. If the results for pregnancy suggested a larger
effect than the corresponding result for live birth then we would
have assumed that the full pregnancy analysis overestimated the
benefit of antioxidants. In the trials that reported on both live
birth and pregnancy 22% of the treatment group became
pregnant and 17% had a live birth, while 2% of the control
became pregnant and 2% had a live birth.
Figure 4. Forest plot of comparison: 2 Live birth versus pregnancy, outcome: 2.1 Live birth.
16Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

• Pregnancy: the trials (Omu 1998; Suleiman 1996) that
reported on both live birth and pregnancy (pooled OR 5.53,
95% CI 2.34 to 13.08; P < 0.0001, I2 = 0%) (Analysis 1.18;
Figure 5) were compared to all other trials reporting pregnancy
(Balercia 2005; Galatioto 2008; Lenzi 2003; Lenzi 2004;
Peivandi 2010; Rolf 1999; Safarinejad 2009a; Sigman 2006;
Tremellen 2007; Wang 1983; Zavaczki 2003) (pooled OR 4.40,
95% CI 2.78 to 6.97; P < 0.00001, I2 = 0%). The results for the
two analyses appear similar thus giving us some confidence that
the reporting bias in this outcome was low. In the trials that
reported both live birth and pregnancy 22% became pregnant in
the antioxidant group and 2% in the control, while in the
pregnancy-only reported trials 15% of the antioxidant group
became pregnant while 3% became pregnant in the control group
Figure 5. Forest plot of comparison: 1 Antioxidant(s) versus control, outcome: 1.16 Live birth and
pregnancy.
17Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Two trials (Galatioto 2008; Tremellen 2007) compared combined
antioxidants. There were 25 pregnancies in total, 21 in the antiox-
idant group (n = 58) and 4 in the control (n = 42). There was a
statistically significant difference in pregnancy rates (pooled OR
3.97, 95% CI 1.39 to 11.33; P = 0.01, I2 = 0%) in favour of the
combined antioxidants over the control.
One trial (Balercia 2005) compared L-acetyl carnitine to placebo.
There were three pregnancies in total, two in the antioxidant group
(n = 15) and one in the placebo group (n = 5). The placebo group
was divided by three as this trial had multiple arms and the placebo
data appeared three times in the analysis. The analysis showed no
statistically significant difference (OR 0.61, 95% CI 0.04 to 9.64;
P = 0.72) in pregnancy rates between the antioxidant and placebo
groups.
Three trials (Balercia 2005; Lenzi 2003; Peivandi 2010) compared
L-carnitine to control. There were 12 pregnancies in total, 11 in
the antioxidant group (n = 73) and 1 in the control group (n =
63). There was a statistically significant difference in pregnancy
rates (pooled OR 5.08, 95% CI 1.51 to 17.09; P = 0.009, I2 =
29%) in favour of the antioxidant group over the control group.
Four trials (Balercia 2005; Cavallini 2004; Lenzi 2004; Sigman
2006) assessed L-acetyl carnitine + L-carnitine versus placebo.
There were 21 pregnancies in total, 19 (n = 96) in the antioxi-
dant group and 3 in the placebo (n = 87). There was a statistically
significant difference significance in pregnancy rates (pooled OR
4.48, 95% CI 1.77 to 11.36; P = 0.002, I2 = 0%) in favour of the
antioxidant group over the placebo group.
Two trials (Balercia 2009; Safarinejad 2009a) reported on coen-
zyme versus placebo. There were nine pregnancies in total (n =
272). All pregnancies occurred in the Balercia 2009 trial and none
in the Safarinejad 2009a trial. Balercia 2009 was the only trial to
be considered for this outcome as there were no pregnancies in
the second trial. Balercia 2009 showed no statistically significant
difference (pooled OR 2.16, 95% CI 0.53 to 8.82; P = 0.28) in
pregnancy rates between the antioxidant and placebo groups.
Only one trial (Wang 1983) reported on pentoxifylline versus
placebo and there were no pregnancies in either group, therefore
the results were not estimable.
One trial (Zavaczki 2003) reported on magnesium versus placebo.
There was one pregnancy in the antioxidant group (n = 10) and
none in the placebo (n = 10). The results showed no statistically
significant difference in pregnancy rates between the antioxidant
group and the placebo group (OR 7.39, 95% CI 0.15 to 372.38;
P = 0.32).
One trial (Suleiman 1996) reported on vitamin E versus placebo.
There were 11 pregnancies in the antioxidant group (n = 52)
and none in the placebo group (n = 35). There was a statistically
significant difference (OR 6.64, 95% CI 1.84 to 23.93; P = 0.004)
in the pregnancy rate in favour of the antioxidant group over the
placebo group. However this trial had a large degree of attrition
due to drop outs leading to an imbalance between the groups; the
confidence intervals were quite large.
One trial (Rolf 1999) reported on vitamin C + vitamin E versus
placebo. There were no pregnancies in either group therefore the
results were not estimable.
One trial (Omu 1998) reported on pregnancy rate with the com-
parison of zinc versus no treatment. A statistically significant dif-
ference was seen (OR 4.75, 95% CI 1.49 to 15.20; P = 0.009) in
favour of the antioxidant group over the no-treatment group.
Adverse event: miscarriage rate per couple randomised
Three trials (Omu 1998; Suleiman 1996; Tremellen 2007) re-
ported on miscarriage per couple randomised. In total there were
five miscarriages in the antioxidant group (n = 139) and two in
the control group (n = 103). There was no statistically significant
difference (pooled OR 1.54, 95% CI 0.32 to 7.30; P = 0.59, I2
= 20%) (Analysis 1.3) in miscarriage rate per couple randomised
between the antioxidant and placebo groups. The confidence in-
tervals of the three trials overlapped the line of no effect (Figure
6).
18Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 6. Forest plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.3 Adverse event:
miscarriage rate per couple randomised.
Stillbirth rate per couple randomised
There were no trials of antioxidants versus control that reported
on stillbirths per couple randomised.
Level of sperm DNA fragmentation
There was only one trial (Greco 2005) that reported on the out-
come of sperm fragmentation levels. There was a statistically sig-
nificant difference (MD -13.80, 95% CI -17.50 to -10.10; P ≤
0.00001) (Analysis 1.4) in favour of the antioxidant group (vita-
min C + vitamin E) over the placebo group (Figure 7).
Figure 7. Forest plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.10 DNA fragmentation.
19Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Total sperm motility at three months or less
Ten trials (Ciftci 2009; Conquer 2000; Dawson 1990; Greco
2005; Micic 1988; Omu 2008; Peivandi 2010; Scott 1998; Sigman
2006; Zavaczki 2003) reported on total sperm motility at three
months or less. In total there were 514 participants, 302 in the an-
tioxidant group and 212 in the control group. There was a statis-
tically significant difference (MD 31.26, 95% CI 31.17 to 31.35;
P < 0.00001, I2 = 96%) (Analysis 1.5) in favour of the antioxidant
group over the control group (Figure 8). The heterogeneity with
the I2 statistic at 96% was very high. Sensitivity analysis was per-
formed on the trial of Peivandi 2010 as the data in this trial were
outlying. The standard deviations had unusually low values when
compared to other trials. The trial by Peivandi also carried 99.8%
of the weight in the analysis. A random-effects model was used
and after sensitivity analysis the statistically significant difference
remained, in favour of the antioxidant group over the control (MD
11.72, 95%CI 6.94 to 16.49; P < 0.00001) and the I2 dropped
to 56%. As heterogeneity remained high we were unable to pool
these data and only subtotals were used in the analysis.
20Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 8. Forest plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.5 Sperm total motility at
3 months or less.
21Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Total sperm motility at six months
Seven trials (Balercia 2005; Balercia 2009; Lenzi 2004; Safarinejad
2009; Safarinejad 2009a; Sigman 2006; Suleiman 1996) reported
on total sperm motility at six months. In total there were 963
participants, 625 in the antioxidant group and 338 in the con-
trol group. This difference in numbers between the treatment and
control groups was due to the splitting of the control arm of the
three or four-arm trials. There was a statistically significant differ-
ence (MD 4.19, 95% CI 3.81 to 4.56; P < 0.00001) (Analysis 1.6)
in favour of the antioxidant group over the control group (Figure
9). Substantial heterogeneity was found in this analysis (Chi2 =
90.87, I2 = 89%). As heterogeneity was large, a sensitivity anal-
ysis was performed by removing the study with over 20% drop
out (Suleiman 1996) but there was little change to the I2 statis-
tic. Therefore, due to unexplained heterogeneity, the totals were
removed in this analysis and only subtotals used.
22Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 9. Forest plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.6 Sperm total motility at
6 months.
23Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Only one comparison (Balercia 2005; Lenzi 2004; Sigman 2006),
L-carnitine + L-acetyl carnitine versus placebo at six months, had
confidence intervals that crossed the line of no effect. One com-
parison, (Balercia 2009; Safarinejad 2009a) coenzyme Q10 versus
placebo at six months, carried 42.9% of the weight of this analysis
and was in favour of the antioxidant group over the placebo group
(MD 4.50, 95% CI 3.93 to 5.07; P < 0.00001, I2 = 0%).
Three trials (Balercia 2005; Lenzi 2004; Sigman 2006) reported
on total sperm motility with the comparison of L-carnitine + L-
acetyl carnitine versus placebo at six months. In total there were
97 participants, 57 in the antioxidant group and 40 in the placebo
group. There was a statistically significant difference in the total
sperm motility in favour of the antioxidant over the placebo group
(MD 5.48, 95% CI 0.44 to 10.52; P = 0.03). Substantial hetero-
geneity was found in this analysis (Chi2 = 8.61, I2 = 77%).
Total sperm motility at nine months or more
Three trials (Balercia 2005; Balercia 2009; Safarinejad 2009a) re-
ported on total sperm motility at nine months or more. In total
there were 332 participants, 181 in the antioxidant and 151 in
the placebo group. There was a statistically significant difference
in treatment effect in favour of the antioxidant over the control
group (MD 1.38, 95% CI 0.81 to 1.95; P < 0.00001) (Analysis
1.7; Figure 10). Heterogeneity was found in this analysis (Chi2
= 10.98, I2 = 64%). Three comparisons had confidence intervals
that crossed the line of no effect. One comparison, coenzyme Q10
(Balercia 2005; Safarinejad 2009a) versus control at 56 weeks, car-
ried 98.9% of the weight of this analysis and was in favour of
the antioxidant group over the control group (MD 1.31, 95% CI
0.74 to 1.88; P < 0.00001). Heterogeneity was moderate in the
analysis, probably due to the variation of antioxidants, therefore
a random-effects model was used. Only subtotals were able to be
used in the analysis.
Figure 10. Forest plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.7 Sperm total motility at
9 months or more.
24Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Sperm concentration at three months or less
Seven trials ( Ciftci 2009; Conquer 2000; Greco 2005; Peivandi
2010; Rolf 1999; Wang 1983; Zavaczki 2003) reported on sperm
concentration at three months or less. In total there were 320
participants, 162 in the antioxidant and 158 in the placebo group.
There was no statistically significant difference (MD 6.04, 95% CI
-5.42 to 17.50; P = 0.30) (Analysis 1.8) between the antioxidant
and the placebo groups (Figure 11). Heterogeneity was high (I2
= 93%) in this analysis. A random-effects model was used and a
sensitivity analysis performed for the trial Peivandi 2010. This trial
had outlying data as the standard deviations were much lower than
for the other studies. When this trial was removed from analysis
the I2 statistic became 0% and there was no statistically significant
difference between the groups (MD 2.64, 95% CI -0.52 to 5.81;
P = 0.10, I2 = 0%).
Figure 11. Forest plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.8 Sperm concentration
at 3 months or less.
25Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Two trials (Greco 2005; Rolf 1999) reported on sperm concentra-
tion with the comparison of vitamin C + vitamin E versus placebo
at two months. In total there were 95 participants, 47 in the an-
tioxidant group and 48 in the placebo group. A statistically signif-
icant difference between the antioxidant and placebo group could
not be found (MD 1.36, 95% CI -10.01 to 12.72; P = 0.82).
Moderate heterogeneity was found in this analysis (Chi2 = 2.07, I2 = 52%).
Sperm concentration at six months
Six trials (Balercia 2005; Balercia 2009; Lenzi 2004; Safarinejad
2009; Safarinejad 2009a; Wang 1983) reported on sperm con-
centration at six months in eight different comparisons. In total
there were 825 participants, 536 in the antioxidant and 289 in
the placebo group. There was a statistically significant difference
in treatment effect in favour of the antioxidant over the placebo
group (MD 5.25, 95% CI 4.43 to 6.08; P < 0.00001) (Analysis
1.9; Figure 12). Heterogeneity was moderate in this analysis (Chi2= 19.05, I2= 53%). The raised heterogeneity was probably due
to the variation in antioxidants. Five comparisons had confidence
intervals that crossed the line of no effect. Due to the heterogene-
ity a random-effects model was applied and subtotals were used in
the analysis.
26Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 12. Forest plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.9 Sperm concentration
at 6 months.
27Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Two trials (Balercia 2005; Lenzi 2004) reported on sperm concen-
tration with the comparison L-carnitine + L-acetyl carnitine versus
placebo at six months. In total there were 76 participants, 45 in
the antioxidant group and 31 in the placebo group. A statistically
significant difference between the antioxidant and placebo group
could not be found (MD 0.63, 95% CI -5.93 to 7.18; P = 0.85).
There was no heterogeneity in this analysis (Chi2 = 0.19, I2 = 0%).
Two trials (Balercia 2009, Safarinejad 2009a) reported on sperm
concentration with the comparison of coenzyme Q10 versus
placebo at six months. In total there were 272 participants, 136 in
the antioxidant group and 136 in the placebo group. There was
statistically significant difference in favour of the antioxidant over
the placebo (MD 5.50, 95% CI 4.34 to 6.67; P < 0.00001). Het-
erogeneity was moderate (Chi2 = 1.92, I2 = 48%) in this analysis.
Sperm concentration at nine months or more
Three trials (Balercia 2005; Balercia 2009; Safarinejad 2009a) re-
ported on sperm concentration at nine months or more in five
different comparisons. In total there were 332 participants, 181 in
the antioxidant group and 151 in the placebo group. There was a
statistically significant difference in favour of the antioxidant over
the placebo (MD 1.61, 95% CI 0.61 to 2.61; P = 0.002) (Analysis
1.10), see Figure 13. Heterogeneity could not be found in this
analysis (Chi2 = 3.79, I2 = 0%). One trial (Safarinejad 2009a) car-
ried 96.1% of the weight of this pooled analysis as it had a larger
sample size and tighter confidence intervals.
Figure 13. Forest plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.10 Sperm concentration
at 9 months or more.
Two trials (Balercia 2009; Safarinejad 2009a) reported on sperm
concentration with the comparison coenzyme Q10 versus placebo
at nine months or more. A statistically significant difference was
seen in favour of the the antioxidant over the placebo group (MD
1.53, 95% CI 0.51 to 2.55; P = 0.003). One trial (Safarinejad
2009a) carried 96.1% of the weight of this analysis.
28Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Total sperm motility and sperm concentration over time
Trials were also subgrouped according to sperm motility over time.
A random-effects model was used due to high heterogeneity in the
following analyses.
• At three months or less (MD 31.26, 95% CI 31.17 to
31.36; P < 0.00001) (Analysis 1.11; Figure 14) a statistically
significant difference in favour of the antioxidant, however the I2
statistic was 97%. When sensitivity analysis was performed for
Peivandi 2009 (Peivandi 2010) due to outlying data the
heterogeneity remained high at 71%.
Figure 14. Forest plot of comparison: 1 Antioxidant(s) versus control, outcome: 1.17 Total sperm motility
over time.
29Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

• At six months there was a statistically significant difference
in treatment effect in favour of the antioxidant over the control
group (MD 5.34, 95% CI 4.91 to 5.77; P < 0.00001) and the I2
statistic was 84%. Sensitivity analysis was performed for
Sulieman (Suleiman 1996) due to >20% drop outs however
there was only a slight decrease in heterogeneity.
• At nine months there was also a statistically significant
difference in treatment effect in favour of the antioxidant over
the placebo (MD 1.35, 95% CI 0.78 to 1.92; P<0.00001, I2 =
68%).
Sperm concentration over time:
• at three months or less (MD 12.74, 95% CI 10.23 to
15.26; P < 0.00001) (Analysis 1.12; Figure 15) a statistically
significant difference in favour of the antioxidant over the
control however the I2 statistic was 94%. When sensitivity
analysis was performed for Peivandi 2009 (Peivandi 2010) due to
outlying data the I2 statistic became 0% and the result changed
to become not statistically significant (MD 2.70, 95% CI -0.47
to 5.88; P = 0.10);
Figure 15. Forest plot of comparison: 1 Antioxidant(s) versus control, outcome: 1.18 Sperm concentration
over time.
• at six months (MD 6.32, 95% CI 5.40 to 7.24; P <
0.00001) a statistically significant difference of the antioxidant
over the control however the I2 statistic = 69%;
• at nine months or more (MD 1.56, 95% CI 0.55 to 2.57; P
30Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

= 0. 003, I2 = 0%) a statistically significant difference in favour
of the antioxidant over the control.
Side effects
Gastrointestinal side effects
Six trials (Cavallini 2004; Kessopoulou 1995; Safarinejad 2009a;
Sigman 2006; Tremellen 2007; Zavaczki 2003) reported on gas-
trointestinal side effects with the comparison of antioxidants ver-
sus placebo. In total there were 426 participants, 219 in the an-
tioxidant group and 207 in the placebo group. A statistically sig-
nificant difference between the antioxidant and placebo groups
could not be found (pooled OR 1.63, 95% CI 0.48 to 5.58; P =
0.44) (Analysis 1.13; Figure 16). There was no heterogeneity (Chi2 = 2.49, I2 = 0%).
Figure 16. Forest plot of comparison: 1 Antioxidant(s) versus placebo, outcome: 1.11 Side effects.
Euphoria
One trial (Cavallini 2004) reported on euphoria as a side effect
with the comparison of antioxidants versus placebo. A statistically
significant difference between the antioxidant and placebo group
could not be found (OR 1.21, 95% CI 0.16 to 9.01; P = 0.85) (
Analysis 1.13; Figure 16).
Antioxidant(s) versus antioxidant(s) - head to head
The total summary statistic was disabled for this analysis as there
was no reason to pool direct comparisons.
Pregnancy rate per couple randomised
Two trials (Balercia 2005; Li 2005 ) reported on pregnancy rates
with three different comparisons (see Analysis 3.1; Figure 17). All
three comparisons crossed the line of no effect. There were 10
pregnancies form 90 couples (11%) in the L-acetyl carnitine + L-
carnitine group and 2 pregnancies from 60 couples in the control
group (3%). The controls were L-acetyl carnitine, carnitine and
vitamin E + vitamin C.
31Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 17. Forest plot of comparison: 3 Antioxidant(s) versus antioxidant(s), outcome: 3.1 Pregnancy per
couple randomised.
One trial (Balercia 2005) reported on the outcome of pregnancy
rates with the comparison of L-acetyl carnitine + L-carnitine (treat-
ment) versus L-acetyl carnitine (control). There were two preg-
nancies in the L-acetyl carnitine + L carnitine group and two in
the L-acetyl carnitine. .
Balercia (Balercia 2005) also reported on the outcome of preg-
nancy rate with the comparison of L-acetyl carnitine + L-carnitine
versus L-carnitine. There were three pregnancies in the treatment
group and two in the control group.
Sperm total motility at three months or less
Seven trials (Akiyama 1999; Conquer 2000; Dawson 1990;
Keskes-Ammar 2003; Li 2005; Omu 2008; Scott 1998) reported
on sperm motility at three months or less in nine different com-
parisons (Analysis 3.2) and (Figure 18).
32Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 18. Forest plot of comparison: 3 Antioxidant(s) versus antioxidant(s), outcome: 3.2 Sperm total
motility at 3 months or less.
33Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Only one trial (Dawson 1990) showed a statistically significant
difference in measure of effect. This study compared ascorbic acid
(vitamin C) 200 mg/day versus vitamin C 1000 mg/day. There
was a statistically significant difference (MD -43.00, 95% CI -
67.10 to -18.90; P = 0.0005) in favour of the 1000 mg/day in
sperm motility.
Sperm total motility at six months
Two trials (Balercia 2005, Safarinejad 2009) reported on five dif-
ferent comparisons of antioxidants versus antioxidants (Analysis
3.3; Figure 19).
Figure 19. Forest plot of comparison: 3 Antioxidant(s) versus antioxidant(s), outcome: 3.3 Sperm total
motility at 6 months.
The comparisons of L-acetyl carnitine + L-carnitine versus L-car-
nitine (Balercia 2005) (MD -3.46, 95% CI -11.41 to 4.49; P =
0.39) and L-acetyl carnitine + L-carnitine versus L-acetyl carni-
tine (Balercia 2005) (MD 0.64, 95% CI -7.58 to 8.86; P = 0.88)
showed no statistically significant difference in effect between these
two different antioxidants.
Safarinejad (Safarinejad 2009) also reported on three other com-
parisons.
Selenium versus N-acetyl cysteine, with a statistically significant
34Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

difference in favour of selenium (MD 1.30, 95% CI 0.39 to 2.21;
P = 0.005).
Selenium versus selenium + N-acetyl cysteine with a statistically
significant difference in favour of selenium + N-acetyl cysteine over
selenium alone (MD -3.10, 95% CI -4.16 to -2.04; P < 0.00001).
N-acetyl cysteine versus selenium + N-acetyl cysteine with a sta-
tistically significant difference in favour of selenium plus N-acetyl
cysteine (MD -4.40, 95% CI -5.31 to -3.49; P < 0.00001).
Sperm total motility at nine months
Only one trial (Balercia 2005) reported on sperm motility at nine
months using the two comparisons of L-acetyl carnitine + L-car-
nitine versus L-carnitine (MD -5.27, 95% CI -12.61 to 2.07; P =
0.16) and L-acetyl carnitine + L-carnitine versus L-acetyl carnitine
(MD -1.57, 95% CI -7.70 to 4.56; P = 0.62) with no evidence of
effect in either of these comparisons (Analysis 3.4; Figure 20).
Figure 20. Forest plot of comparison: 3 Antioxidant(s) versus antioxidant(s), outcome: 3.4 Sperm total
motility at 9 months or more.
Sperm concentration at three months
Three trials (Akiyama 1999; Conquer 2000; Li 2005a) reported
on sperm concentration at three months (Analysis 3.5; Figure 21).
The trial by Akiyama showed no statistically significant difference
in effect between the antioxidant ethyl cysteine versus vitamin E
(MD 2.20, 95% CI -16.65 to 21.05; P = 0.82). The trial by Con-
quer compared docosahexaenoic acid (DHA) 400g/day and DHA
800 g/day also with no statistically significant difference in effect
(MD -6.80, 95% CI -41.87 to 28.27; P = 0.70). The trial by Li
2005a reported on sperm concentration at three months compar-
ing L-carnitine versus vitamin E + vitamin C with a statistically
significant difference (MD 15.50, 95% CI 12.49 to 18.51; P <
0.00001) in favour of vitamin E + vitamin C over L-carnitine.
35Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 21. Forest plot of comparison: 3 Antioxidant(s) versus antioxidant(s), outcome: 3.5 Sperm
concentration at 3 months or less.
Sperm concentration at six months
Two trials (Balercia 2005; Safarinejad 2009) reported on sperm
concentration at six months using five comparisons (Analysis 3.6;
Figure 22).
36Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 22. Forest plot of comparison: 3 Antioxidant(s) versus antioxidant(s), outcome: 3.6 Sperm
concentration at 6 months.
The trial by Balercia reported on two comparisons for this out-
come: L-acetyl carnitine + L-carnitine versus L-carnitine (MD -
8.13, 95% CI -24.42 to 8.16; P = 0.33) and L-acetyl carnitine +
L-carnitine versus L-acetyl carnitine (MD -2.17, 95% CI -17.40
to 13.06; P = 0.78). Neither of these comparisons showed any sta-
tistically significant difference in effect between the antioxidants.
Safarinejad 2009 reported on three comparisons. Selenium versus
N-acetyl cysteine showed no statistically significant difference in
effect. Selenium versus selenium + N-acetyl cysteine showed a
statistically significant difference favouring selenium + N-acetyl
cysteine (MD -4.50, 95%CI -6.90 to -2.10; P < 0.0002).
Safarinejad 2009 also reported on N-acetyl cysteine versus sele-
nium + N-acetyl cysteine. There was a statistically significant dif-
ference (MD -5.30, 95% CI -7.29 to -3.31; P < 0.00001) in favour
of selenium + N-acetyl cysteine.
Sperm concentration at nine months
Balercia (Balercia 2005) reported on the outcome of sperm con-
centration at nine months with two comparisons (Analysis 3.7;
Figure 23).
37Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 23. Forest plot of comparison: 3 Antioxidant(s) versus antioxidant(s), outcome: 3.7 Sperm
concentration at 9 months or more.
L-acetyl carnitine + L-carnitine versus L-carnitine showed no sta-
tistically significant difference in effect between the two antioxi-
dants (MD -6.13, 95% CI -18.44 to 6.18; P = 0.33).
L-acetyl carnitine + L-carnitine versus L-acetyl carnitine also
showed no statistically significant difference in effect between the
two antioxidants (MD 2.06, 95% CI -8.33 to 12.45; P = 0.70).
D I S C U S S I O N
Summary of main results
This systematic review and meta analysis aimed to investigate
whether supplemental antioxidants given to subfertile men made a
difference to the outcomes of live birth, pregnancy and the adverse
events of miscarriage or stillbirth. Seminal parameters were also
analysed. The comparisons used were antioxidants versus control
and head to head antioxidants.
In the antioxidant versus control comparison there was a statisti-
cally significant difference in effect in favour of antioxidants in the
live birth and pregnancy outcomes. These antioxidants did not ap-
pear to be associated with any increase in miscarriage. There were
however only three trials (Omu 1998; Suleiman 1996; Tremellen
2007) in the outcome of live birth. One of these trials Suleiman
1996 had drop outs. The reasons were explained but we were un-
aware of how many of the drop outs were from the treatment or
control group. Therefore we could not use intention-to-treat anal-
ysis for this trial.
Fifteen trials reported on pregnancy rate (Balercia 2005; Balercia
2009; Cavallini 2004; Galatioto 2008; Lenzi 2003; Lenzi 2004;
Omu 1998; Peivandi 2010; Rolf 1999; Safarinejad 2009a; Sigman
2006; Suleiman 1996; Tremellen 2007; Wang 1983; Zavaczki
2003) in the antioxidant versus control comparison and two (
Balercia 2005; Li 2005) in the head to head comparisons. Balercia
2005 was multi-armed and also reported pregnancy rate per couple
using the antioxidant versus control comparison.
There were no trials reporting on the outcome of stillbirth.
The data for the outcomes of total sperm motility at three, six and
nine months were unable to be pooled due to heterogeneity. A
random-effects model was used and sensitivity analysis was per-
formed. Heterogeneity remained moderate therefore we were not
able to pool this data and subtotals were used.
Sperm concentration at three months or less had high heterogene-
ity and did not show a statistically significant difference in effect
after sensitivity analysis was performed. The I2 statistic became
0% in the sensitivity analysis and therefore the data were able to
be pooled. The analysis of the outcome of sperm concentration
at six months also showed high heterogeneity. A random-effects
model was used and subtotals were used as the data were unable
to be pooled. The analysis of sperm concentration at nine months
showed a statistically significant difference in effect in favour of
the antioxidants over the control group. No heterogeneity was ev-
ident in this analysis. The high heterogeneity in the analysis of the
sperm parameters may in some way be due to the variations of the
types of antioxidants.
The main side effects reported were gastrointestinal and there
was no evidence that the antioxidant was more harmful than the
placebo.
It is difficult to draw conclusions from the head to head compar-
isons until there are more randomised trials that compare the same
antioxidants against controls. One antioxidant did not appear to
have any effect on pregnancy rate per couple or sperm parameters
over those of another antioxidant.
Overall completeness and applicability ofevidence
38Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

The live birth analysis in the antioxidant versus control group
was based on only three trials (Kessopoulou 1995; Omu 1998;
Suleiman 1996). The Suleiman trial had some imbalance in par-
ticipant numbers due to loss to follow up. The analysis remained
statistically significant when sensitivity analysis was performed on
the Suleiman trial.
Pregnancy rate evidence between antioxidants and control is in-
complete. Only 15 of 34 trials reported this outcome. Several of
these trials had high and selective losses to follow up. However
heterogeneity between the trials is low. The outcomes of sperm
motility and concentration also appear to be incomplete and not
applicable. Only 15 of 34 trials reported on sperm motility and
16 reported on sperm concentration
Two trials (Galatioto 2008; Tremellen 2007) used combined an-
tioxidants (three or more antioxidants) versus control.
Only one trial (Greco 2005) reported DNA fragmentation in the
comparison of antioxidants versus control therefore there were no
pooled data available for this outcome.
The adverse events of stillbirth, miscarriage and side effects appear
to be poorly reported.
The head to head comparison does not provide constructive in-
formation as there was no reason to pool direct comparisons. Sub-
grouping of antioxidants or different doses of antioxidants was un-
able to be performed in the treatment versus treatment groups as
there were only single trials analysing these differences. Therefore
this review was unable to show any difference in effect between
different antioxidants or different doses of the same antioxidant.
Quality of the evidence
All three studies reporting live birth (Kessopoulou 1995; Omu
1998; Suleiman 1996) had unclear methods of sequence genera-
tion and allocation concealment; one trial (Suleiman 1996) also
had some imbalance in numbers at analysis due to drop outs and
in another (Omu 1998) the comparison was no treatment and not
placebo.
Figure 23 (Figure 24) shows the review authors’ judgements about
the methodological quality of the trials included in this review.
All included trials were described as randomised however only
30% gave information on how the randomisation was achieved.
Allocation concealment was described in only 24% of the trials.
Blinding was better described with over 50% of the trials being
double and occasionally single blinded; 10% of trials stated that
there was no blinding. Incomplete outcome data were addressed
by most of the studies but selective reporting of outcomes was
unclear in the majority of trials.
Figure 24. Methodological quality graph: review authors’ judgements about each methodological quality
item presented as percentages across all included studies.
The seven trials that described their methods more thoroughly
(Galatioto 2008; Greco 2005; Peivandi 2010; Rolf 1999;
Safarinejad 2009; Sigman 2006; Tremellen 2007) can be seen
graphically in figure 24 (Figure 25).
39Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 25. Methodological quality summary: review authors’ judgements about each methodological
quality item for each included study.
40Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Potential biases in the review process
Some bias in the review process may have arisen due to the inclu-
sion of trials that have had drop outs of participants of > 20% and
imbalances between the treatment and control groups.
Agreements and disagreements with otherstudies or reviews
Two reviews described the effects of L-carnitine and L-acetylcar-
nitine on subfertile men. The systematic review and meta-analysis
by Zhou (Zhou 2007) compared L-carnitine and L-acetylcarni-
tine therapy to placebo treatment and found significant improve-
ments in pregnancy rate and total sperm motility. No significant
difference was found in the outcome of sperm concentration. The
descriptive review by Patel (Patel 2008) discusses the improvement
in pregnancy rates with oral intake of antioxidants, however Patel
states that randomised controlled trials (RCTs) have not shown an
effect on sperm motility and that there is a need for more RCTs in
men with oxidative stress. These results were similar for the trials
reporting on L-carnitine and acetyl carnitine interventions in this
review.
Agarwal (Agarwal 2004) in an overview of the literature discusses
a range of antioxidants, and combinations of these, and their effect
on male subfertility. Agarwal notes that vitamin E and a combina-
tion of vitamin E with other antioxidants such as N-acetylcysteine,
vitamin A and fatty acids appears to improve pregnancy rates in
asthenozoospermic men. Carntines also appear to have an effect
on pregnancy rates. This review agrees with the carnitine discus-
sion but there were only single trials in the vitamin E interventions
versus placebo so a summary statistic for the outcome was unable
to be obtained.
Another review that was published recently (Ross 2010) also
showed improvement in pregnancy rate after antioxidant therapy.
A Cochrane review of antioxidants for female subfertility has been
published concurrently (Clarke 2009). The findings of both re-
views are consistent in that combined antioxidants improved preg-
nancy rate.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
When trying to conceive as part of an assisted reproductive pro-
gram, it may be advisable to encourage the male partner to take
an oral antioxidant supplement to improve his partner’s chance of
conceiving. More research is required to further substantiate these
conclusions.
Implications for research
In this review there were only three trials (two comparing antiox-
idant versus placebo and one versus no treatment) reporting on
live birth, the most important outcome from the perspective of
the couple experiencing difficulty with conception. Only one trial
reported on DNA fragmentation. A low degree of DNA fragmen-
tation is thought to increase a the likelihood of achieving a preg-
nancy. More well designed randomised controlled trials that report
on the outcomes of live birth, pregnancy, DNA fragmentation and
adverse events are needed.
Only two trials (Galatioto 2008; Tremellen 2007) used combined
antioxidants (three or more antioxidants) versus control. The re-
sults were in favour of the antioxidant over the control however
there is a need for more randomised controlled trials on this in-
tervention in order to make any conclusions on whether a combi-
nation of antioxidants would have statistical significant difference
over a single antioxidant versus placebo.
Further randomised controlled trials are needed to assess whether
one antioxidant is more effective than another by head to head
comparisons.
There is also a gap in the evidence for the assessment of different
doses of an antioxidant having differing effects. This review was
only able to include single trials measuring different doses and
therefore meta analysis of this comparison was unable to be per-
formed.
Evidence to date suggests that the side effect profile is low however,
as there were few studies, more data are required to determine any
adverse events and the side effect profile of these supplements.
A C K N O W L E D G E M E N T S
Cochrane Menstrual Disorders and Subfertility Group (MDSG).
I would like to make special mention of the MDSG editors who
were very thorough and helpful in editing this review.
Many thanks to the translators of the non-English trials - Ichiro
Omori (Japanese paper), Shaofu Li (two Chinese papers), Ivan
Sola (Bulgarian paper) and Pawel Kanturski (Polish paper) and Dr
Peviandi (Iranian paper).
Thanks also to Stephan Bontekoe who kindly helped with some
of the text.
41Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

R E F E R E N C E S
References to studies included in this review
Akiyama 1999 {published data only}
Akiyama M. In vivo scavenging effect of ethylcysteine on
reactive oxygen species in human semen. Japanese Journal
of Urology 1999; Vol. 90, issue 3:421–8.
Balercia 2005 {published data only}
Balercia G, Regoli F, Armeni T, Koverech A, Mantero F,
Boscaro M. Placebo-controlled double-blind randomized
trial on the use of L-carnitine, L-acetylcarnitine, or
combined L-carnitine and L-acetylcarnitine in men with
idiopathic asthenozoospermia. Fertility and Sterility 2005;
Vol. 84, issue 3:662–71.
Balercia 2009 {published data only}
Balercia G, Buldreghini E, et al.Coenzyme Q10 treatment
in infertile men with idiopathic asthenozoospermia: a
placebo-controlled, double-blind randomized trial. Fertility
and Sterility 2009;91(5):1785–92.
Biagiotti 2003 {published data only}
Biagiotti G, Cavallini G, Modenini F, Vitali G, Magli
C, Ferraretti A. Prostaglanadins pulsed down-regulation
enhances carnitine therapy performance in severe idiopathic
oligoasthenospermia. Human Reproduction 2003; Vol. 18
Suppl 1:202.
Cavallini 2004 {published data only}
Cavallini G, Ferraretti AP, Gianaroli L, Biagiotti G, Vitali G.
Cinnoxicam and L-carnitine/acetyl-L-carnitine treatment
for idiopathic and varicocele-associated oligoasthenospermia
[see comment]. Journal of Andrology 2004; Vol. 25, issue
5:761–70.
Ciftci 2009 {published data only}
Ciftci H, Verit A, Savas M, Yeni E, Erel O. Effects of
N-acetylcysteine on semen parameters and oxidative/
antioxidant status. Urology 2009;74(1):73–6.
Conquer 2000 {published data only}
Conquer JA, Martin JB, Tummon I, Watson L, Tekpetey F.
Effect of DHA supplementation on DHA status and sperm
motility in asthenozoospermic males. Lipids 2000;35(2):
149–54.
Dawson 1990 {published data only}
Dawson EB, Harris WA, Powell LC. Relationship between
ascorbic acid and male fertility. World Review of Nutrition
and Dietetics 1990; Vol. 62:1–26.
Galatioto 2008 {published data only}
Galatioto GP, Gravina GL, Angelozzi G, Sacchetti A,
Innominato PF, Pace G, et al.May antioxidant therapy
improve sperm parameters of men with persistent
oligospermia after retrograde embolization for varicocele?.
World Journal of Urology 2008; Vol. 26, issue 1:97–102.
Greco 2005 {published data only}
Greco E, Iacobelli M, Rienzi L, Ubaldi F, Ferrero S, Tesarik
J. Reduction of the incidence of sperm DNA fragmentation
by oral antioxidant treatment. Journal of Andrology 2005;
Vol. 26, issue 3:349–53.
Keskes-Ammar 2003 {published data only}
Keskes-Ammar L, Feki-Chakroun N, Rebai T, Sahnoun Z,
Ghozzi H, Hammami S, et al.Sperm oxidative stress and
the effect of an oral vitamin E and selenium supplement
on semen quality in infertile men. Archives of Andrology
2003; Vol. 49, issue 2:83–94.
Kessopoulou 1995 {published data only}
Kessopoulou E, Powers HJ, Sharma KK, Pearson MJ,
Russell JM, Cooke ID, et al.A double-blind randomized
placebo cross-over controlled trial using the antioxidant
vitamin E to treat reactive oxygen species associated male
infertility. Fertility and Sterility 1995; Vol. 64, issue 4:
825–31.
Lenzi 2003 {published data only}
Lenzi A, Lombardo F, Sgro P, Salacone P, Caponecchia L,
Dondero F, et al.Use of carnitine therapy in selected cases
of male factor infertility: a double-blind crossover trial [see
comment]. Fertility and Sterility 2003; Vol. 79, issue 2:
292–300.
Lenzi 2004 {published data only}
Lenzi A, Sgro P, Salacone P, Paoli D, Gilio B, Lombardo F,
et al.A placebo-controlled double-blind randomized trial
of the use of combined l-carnitine and l-acetyl-carnitine
treatment in men with asthenozoospermia [see comment].
Fertility and Sterility 2004; Vol. 81, issue 6:1578–84.
Li 2005 {published data only}
Li Z, Chen GW, Shang XJ, Bai WJ, Han YF, Chen B, et
al.A controlled randomized trial of the use of combined
L-carnitine and acetyl-L-carnitine treatment in men with
oligoasthenozoospermia. Zhong Hua Nan Ke Xue 2005;
Vol. 11, issue 10:761–4.
Li 2005a {published data only}
Li Z, Gu R, Liu Y, Xiang Z, Cao X, Han Y, et al.Curative
effect of L-carnitine supplementation in the treatment of
male infertility. Academic Journal of Shanghai Second
Medical University 2005; Vol. 25, issue 3:292–4.
Lombardo 2002 {published data only}
Lombardo F, Gandini L, Agarwal A, Sgro P, Dondero F,
Lenzi A. A prospective double blind placebo controlled
cross over trial of carnitine therapy in selected cases of male
infertility. Fertility and Sterility 2002; Vol. 78 Suppl 1:
68–9.
Merino 1997 {published data only}
Merino G, Martinez Chequer JC, Barahona E, Bermudez
JA, Moran C, Carranza-Lira S. Effects of pentoxifylline on
sperm motility in normogonadotropic asthenozoospermic
men. Archives of Andrology 1997; Vol. 39, issue 1:65–9.
Micic 1988 {published data only}
Micic S, Hadzi-Djokic J, Dotlic R, Tulic C. Pentoxifyllin
treatment of oligoasthenospermic men. Acta Europaea
Fertilitatis 1988; Vol. 19, issue 3:135–7.
Nozha 2001 {published data only}
Nozha CF, Leila AK, Zouhir S, Hanen G, Khled Z, Tarek
R. Oxidative stress and male infertility: comparative study
42Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

of combined vitamin E/selenium treatment versus vitamin
B. Human Reproduction 2001; Vol. 17, issue Abstract
book 1:111–2.
Omu 1998 {published data only}
Omu AE, Dashti H, Al-Othman S. Treatment of
asthenozoospermia with zinc sulphate: andrological,
immunological and obstetric outcome. European Journal of
Obstetrics, Gynecology, and Reproductive Biology 1998;
Vol. 79, issue 2:179–84.
Omu 2008 {published data only}
Omu AE, Al-Azemi MK, Kehinde EO, Anim JT, Oriowo
MA, Mathew TC. Indications of the mechanisms involved
in improved sperm parameters by zinc therapy. Medical
Principles and Practice 2008; Vol. 17, issue 2:108–16.
Peivandi 2010 {published data only}
Peivandi S, Abasali K, Narges M. Effects of L-carnitine on
infertile men’s spermogram; a randomised clinical trial.
Journal of Reproduction and Infertility 2010;10(4):331.
Rolf 1999 {published data only}
Rolf C, Cooper TG, Yeung CH, Nieschlag E. Antioxidant
treatment of patients with asthenozoospermia or moderate
oligoasthenozoospermia with high-dose vitamin C and
vitamin E: a randomized, placebo-controlled, double-blind
study [see comment]. Human Reproduction 1999; Vol. 14,
issue 4:1028–33.
Safarinejad 2009 {published data only}
Safarinejad MR, Safarinejad S. Efficacy of selenium and/
or N-acetyl-cysteine for improving semen parameters
in infertile men: a double-blind, placebo controlled,
randomized study. The Journal of Urology 2009;181(2):
741–51.
Safarinejad 2009a {published data only}
Safarinejad ME. Efficiacy of coenzyme Q10 on semen
parameters, sperm function and reproductive hormones in
infertile men. The Journal of Urology 2009;182:237–48.
Scott 1998 {published data only}
Scott R, MacPherson A, Yates RW, Hussain B, Dixon J. The
effect of oral selenium supplementation on human sperm
motility. British Journal of Urology 1998; Vol. 82, issue 1:
76–80.
Sigman 2006 {published data only}
Sigman M, Glass S, Campagnone J, Pryor JL. Carnitine for
the treatment of idiopathic asthenospermia: a randomized,
double-blind, placebo-controlled trial. Fertility and Sterility
2006; Vol. 85, issue 5:1409–14.
Suleiman 1996 {published data only}
Suleiman SA, Ali ME, Zaki ZM, el-Malik EM, Nasr MA.
Lipid peroxidation and human sperm motility: protective
role of vitamin E. Journal of Andrology 1996; Vol. 17, issue
5:530–7.
Tremellen 2007 {published data only}
Tremellen K, Miari G, Froiland D, Thompson J. A
randomised control trial examining the effect of an
antioxidant (Menevit) on pregnancy outcome during IVF-
ICSI treatment. The Australian & New Zealand Journal of
Obstetrics & Gynaecology 2007;47:216–21.
Wang 1983 {published data only}
Wang C, Chan CW, Wong KK, Yeung KK. Comparison
of the effectiveness of placebo, clomiphene citrate,
mesterolone, pentoxifylline, and testosterone rebound
therapy for the treatment of idiopathic oligospermia.
Fertility and Sterility 1983;40(3):358–65.
Wong 2002 {published data only}
Wong WY, Merkus HM, Thomas CM, Menkveld R,
Zielhuis GA, Steegers-Theunissen RP. Effects of folic acid
and zinc sulfate on male factor subfertility: a double-blind,
randomized, placebo-controlled trial. Fertility and Sterility
2002; Vol. 77, issue 3:491–8.
Zalata 1998 {published data only}
Zalata A, Christophe A, Horrobin D, Dhooge W, Comhaire
F. Effect of essential fatty acids and antioxidants dietary
supplementation on the oxidative DNA damage of the
human spermatozoa. ESHRE 14th annual meeting.
Goteborg, 1998:270–1.
Zavaczki 2003 {published data only}
Zavaczki Z, Szollosi J, Kiss S, Koloszar S, Fejes I, Kovacs L,
Pal A. Magnesium-orotate supplementation for idiopathic
infertile male patients: a randomized, placebo-controlled
clinical pilot study. Magnesium Research 2003;16(2):131–6.
References to studies excluded from this review
Cavallini 2004a {published data only}
Cavallini G, Ferraretti AP, Gianaroli L, Magli MC, Biagiotti
G, Vitali G. Cinnoxicam + carnitines for idiopathic
dyspermia. The 20th Annual Meeting of the European
Society of Human Reproduction and Embryology 2004:
i23–4.
Comhaire 2005 {published data only}
Comhaire FH, El Garem Y, Mahmoud A, Eertmans
F, Schoonjans F. Combined conventional/antioxidant
“Astaxanthin” treatment for male infertility: a double blind,
randomized trial. Asian Journal of Andrology 2005; Vol. 7,
issue 3:257–62.
Ebisch 2003 {published data only}
Ebisch IM, van Heerde WL, Thomas CM, van der
Put N, Wong WY, Steegers-Theunissen RP. C677T
methylenetetrahydrofolate reductase polymorphism
interferes with the effects of folic acid and zinc sulfate on
sperm concentration. Fertility and Sterility 2003; Vol. 80,
issue 5:1190–4.
Ebisch 2006 {published data only}
Ebisch IM, Pierik FH, DE Jong FH, Thomas CM,
Steegers-Theunissen RP. Does folic acid and zinc sulphate
intervention affect endocrine parameters and sperm
characteristics in men?. International Journal of Andrology
2006; Vol. 29, issue 2:339–45.
Elgindy 2008 {published data only}
Elgindy EA, El-Huseiny AM, Mostafa MI, Gaballah AM,
Amed TA. N-Acetylcysteine: Could it be an effective
adjuvant therapy in ICSI cycles. Fertility and Sterility
2008;90 Suppl 1(American Society for Reproductive
43Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Medicine 64th Annual Meeting. November 8-12, 2008,
San Francisco CA):356 Abstract no: P738.
Micic 2001 {published data only}
Micic S, Lalic N, Bojanic N, Nale DJ. Oligospermic men
treated by carnitine. 17th World Congress on Fertility and
Sterility. Melbourne, 2001:38.
Nikolova 2007 {published data only}
Nikolova V, Stanislavov R, Vatev I, Nalbanski B, Punevska
M. Sperm parameters in male idiopathic infertility after
treatment with prelox. Akusherstvo i Ginekologiia 2007;
Vol. 46, issue 5:7–12.
Pawlowicz 2001 {published data only}
Pawlowicz P, Stachowiak G, Bielak A, Wilczynski J.
Administration of natural anthocyanins derived from
chokeberry (aronia melanocarpa) extract in the treatment
of oligospermia in males with enhanced autoantibodies to
oxidized low density lipoproteins (oLAB). The impact on
fructose levels. Ginekologia Polska 2001;72(12):983–8.
Pryor 2003 {published data only}
Pryor JL, Stacy L, Glass S, Campagnone J, Sigman M.
Randomized double blind placebo controlled trial of
carnitine for the treatment of idiopathic asthenospermia.
Fertility and Sterility 2003; Vol. 80 Suppl 3:48.
Rolf 1998 {published data only}
Rolf C. Antioxidant treatment with high dose vitamin
C and vitamin E of patients with asthenozoospermia a
randomized placebo controlled double blind study. ESHRE
14th annual meeting. Goteborg, 1998:72.
Stanislavov 2009 {published data only}
Stanislavov R, Nikolova V, Rohdewald P. Improvement of
seminal parameters with Prelox® : a randomized, double-
blind, placebo controlled, cross over trial. Phytotherapy
Research 2009;23:297–302. [DOI: 10.1002]
Tremellen 2006 {published data only}
Tremellen K, Froiland D, Miari G, Thompson J. A
randomised control trial examining the effect of an
antioxidant on sperm function pregnancy outcome during
IVF treatment. The Fertility Society of Australia 25th
Annual scientific meeting 2006 2006; Vol. 46 Suppl 2:A2.
Vicari 2001 {published data only}
Vicari E, Calogero AE. Effects of treatment with carnitines
in infertile patients with prostatovesiculoepididymitis and
elevated sperm oxidative stress. ESHRE 17th Annual
Meeting. Lausanne: Human Reproduction, 2001; Vol. 16
Suppl 1:106–7.
Vicari 2001a {published data only}
Vicari E, Rubino C, De Palma A, Longo G, Lauretta M,
Consoli S, Arancio A. Antioxidant therapeutic efficiency
after the use of carnitine in infertile patients with bacterial
or non bacterial prostato-vesiculo-epididymitis. Archivio
Italiano di Urologia, Andrologia 2001;73(1):15–25.
Zalata 1998a {published data only}
Zalata A, Christophe A, Horrbin D, Dhooge W, Comhaire
F. Protection of sperm function and DNA by essential fatty
acids and antioxidants dietary supplementation. Fertility
and Sterility 1998;70(3 Abstracts of 1998 Meetings):287.
References to studies awaiting assessment
Dimitriadis 2010 {published data only}
Dimitriadis F, Tsambalas S, Tsounapi P, Kawamura H,
Vlachopoulou E, Haliasos N, Gratsias S, Watanabe T, Saito
M, Miyagawa I, Sofikitis N. Effects of phosphodiesterase-
5 inhibitors on Leydig cell secretory function in
oligoasthenospermic infertile men: A randomized trial.
BJU International 2010;106(8):1181–1185.
Wang 2010 {published data only}
Wang YW, Yang SW, Qu CB, Huo HX, Li W, Li JD,
Chang XL, Cai GZ. L- carnitine: safe and effective for
asthenozoospermia. National Journal of Andrology 2010;16
(5):420–2.
References to ongoing studies
Gonzalez 2009 {unpublished data only}
Gonzalez Sanchez R. Assessment of the efficacy of dietary
supplement spermotrend in the treatment of male infertility.
ClinicalTrials.gov.
Kumar 2010 {unpublished data only}
Kumar R. Evaluation of oxidative stress as a cause for
idiopathic male infertility and the role of addyzoa.
ClinicalTrials.gov.
Revel 2006 {published data only}
Revel A. A preliminary study on effect of omega-3 on
human sperm. ClinicalTrials.gov. [CTG: NCT00479960]
Sadeghi 2008 {published data only}
Sadeghi M. Effects of coenzyme Q10 (CoQ10)
supplementation on semen quality and seminal oxidative
stress of idiopathic oligoasthenoteratozoospermic (iOAT)
infertile men. World Health Organization International
Clinical Trials Registry Platform Search Portal 2008.
[ISRCTN: ISRCTN29954277]
Tsafrir 2010 {published data only}
Tsafrir A. Is a carnitine based food supplement
(PorimoreTM) for infertile men superior to folate and zinc
with regard to pregnancy rates in intrauterine insemination
cycles?. Information obtained from ClinicalTrials.gov on
March 01, 2010.
Additional references
Agarwal 2003
Agarwal A, Said T. Role of sperm chromatin abnormalities
and DNA damage in male infertility. Human Reproduction
Update 2003;9(4):331–45.
Agarwal 2004
Agarwal A, Nallella K, Allamaneni S, Said T. Role of
antioxidants in treatment of male infertility: an overview of
the literature. Reproductive Biomedicine Online 2004;8(6):
616–27.
44Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Aitken 2004
Aitken RJ, Koopman P, Lewis SE. Seeds of concern. Nature
2004;432(7013):48–52.
Aitken 2007
Aitken RJ, De Iuliis GN. Origins and consequences of
DNA damage in male germ cells. Reproductive Biomedicine
Online 2007;14(6):727–33.
Alvarez 2003
Alvarez 2003. Nuture vs nature: How can we optimise
sperm quality?. Journal of Andrology 2003;24(5):640–8.
Attia 2007
Attia AM, Al-Inany HG, Farquar C, Proctor M.
Gonatrophins for idiopathic male factor male subfertility.
Cochrane Database of Systematic Reviews 2004, Issue 4.
[DOI: 10.1002/14651858.CD005071.pub3; : ]
Boe-Hansen 2005
Boe-Hansen GB, Ersboll AK, Christensen P. Variability and
laboratory factors affecting the sperm chromatin structure
assay in human semen. Journal of Andrology 2005;26(3):
360–8.
Boe-Hansen 2006
Boe-Hansen GB, Fedder J, Ersboll AK, Christensen P. The
sperm chromatin structure assay as a diagnostic tool in the
human fertility clinic. Human Reproduction 2006;21(6):
1576–82.
Borini 2006
Borini A, Tarozzi N, Bizzaro D, Bonu MA, Fava L, Flamigni
C, Coticchio G. Sperm DNA fragmentation: paternal effect
on early post-implantation embryo development in ART.
Human Reproduction 2006;21(11):2876–81.
Bykova 2007
Bykova M, Athayde K, Sharma R, Jha R, Sabanegh E,
Agarwal A. Defining the reference value of seminal reactive
oxygen species in a population of infertile men and normal
healthy volunteers. Fertility and Sterility 2007;88 Suppl 1
(P-597):305.
Clarke 2009
Clarke J, Showell MG, Hart RJ, Agarwal A, Gupta S.
Antioxidants for female subfertility. Cochrane Database
of Systematic Reviews 2009, Issue 2. [DOI: 10.1002/
146518858]
Comhaire 2000
Comhaire FH, Christophe AB, Zalata AA, Dhooge WS,
Mahmoud AM, Depuydt CE. The effects of combined
conventional treatment, oral antioxidants and essential fatty
acids on sperm biology in subfertile men. Prostaglandins,
Leukotrienes, and Essential Fatty Acids 2000;63(3):159–65.
Dias 2006
Dias S, McNamee R, Vail A. Evidence of improving quality
of reporting of randomised controlled trials in subfertility.
Human Reproduction 2006;21(10):2617–27.
El-Taieb 2009
El-Taieb MAA, Herwig R, Nada EA, Greilberger J,
Marberger M. Oxidative stress and epididymal sperm
transport, motility and morphological defects. European
Journal of Obstetrics, Gynecology, and Reproductive Biology
2009;144 Suppl 1:199–203.
Eskenazi 2005
Eskanazi B, Kidd SA, Marks AR, Sloter E, Block G,
Wyrobeck AJ. Antioxidant intake is associated with semen
quality in healthy men. Human Reproduction 2005;20(4):
1006–12.
Evenson 2006
Evenson D, Wixon R. Meta-analysis of sperm DNA
fragmentation using the sperm chromatin structure assay.
Reproductive Biomedicine Online 2006;12(4):466–72.
Evenson 2007
Evenson DP, Kasperson K, Wixon RL. Analysis of sperm
DNA fragmentation using flow cytometry and other
techniques. Society for Reproduction and Fertility 2007;65
Suppl:93–113.
Higgins 2006
Higgins JPT, Green S, editors. Cochrane Handbook for
Systematic Reviews of Interventions 4.2.6 (updated Sept
2006). The Cochrane Library Issue 4 Sept 2006. Chichester
UK: John Wiley and Sons Ltd, 2006.
Li 2006
Li Z, Wang L, Cai J, Huang H. Correlation of sperm DNA
damage with IVF and ICSI outcomes: a systematic review
and meta-analysis. Journal of Assisted Reproduction and
Genetics 2006;23(9-10):367–76.
Omu 2008
Omu AE, Al-Azemi MK, Kehinde EO, Anim JT, Oriowo
MA, Mathew TC. Indications of the mechanisms involved
in improved sperm parameters by zinc therapy. Medical
Principles and Practice 2008;17:108–16.
Patel 2008
Patel SR, Sigman M. Antioxidant therapy in male infertility.
Urologic Clinics of North America. 2008;35(2):319–30.
[MEDLINE: 18423251]
Ross 2010
Ross C, Morriss A, Khairy M, Khalaf Y, Braude P,
Coomarasamy A, El-Toukhy T. A systematic review of the
effect of oral antioxidants on male infertility. Reproductive
Biomedicine Online 2010;20(6):711–23. [PUBMED:
20378409]
Sheweita 2005
Sheweita S, Tilmisany A, Al-Sawaf H. Mechanisms of male
infertility: Role of antioxidants. Current Drug Metabolism
2005;6(5):495–501.
Sikka 1995
Sikka S, Rajasekaran M, Hellstrom W. Role of oxidative
stress and antioxidants in male infertility. Journal of
Andrology 1995;16(6):464–8.
Stankiewicz 2003
Stankiewicz M, Norman R. Zinc for male infertility.
Cochrane Database of Systematic Reviews 2003, Issue 4.
[DOI: 10.1002/14651858.CD004633]
45Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Tarozzi 2007
Tarozzi N, Bizzaro D, Flamigni C, Borini A. Clinical
relevance of sperm DNA damage in assisted reproduction.
Reproductive Biomedicine Online 2007;14(6):746–57.
Tournaye 2006
Tournaye H. Evidence-based management of male
subfertility. Current Opinion in Obstetrics & Gynecology
2006;18:253–9.
Tremellen 2008
Tremellen K. Oxidative stress and male infertility - a clinical
perspective. Human Reproduction Update 2008;14(3):
243–58.
Wathes 2007
Wathes DC, Abayasekara DR, Aitken RJ. Polyunsaturated
fatty acids in male and female reproduction. Biology of
Reproduction 2007;77(2):190–201.
Zhou 2007
Zhou X, Liu F, Zhai S. Effect of L-carnitine and/or L-
acetyl-carnitine in nutrition treatment for male infertility: a
systematic review. Asia Pacific Journal of Clinical Nutrition
2007;16 Suppl 1:383–90. [MEDLINE: 17392136]∗ Indicates the major publication for the study
46Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Akiyama 1999
Methods Randomised crossover trial. Single centre
Participants Country: Japan
Male infertility
Mean age: 36 years (treatment group age range 24-49, control 30-37)
n=10 recruited
Inclusion criteria: Male infertility (ROS >5*10000 counts/10000000 viable spermato-
zoa)
Exclusion criteria: Azoospermia, pyospermia
Duration of study: 8 months
Interventions Ethylcysteine 600mg/day for 3 months (n=5)
versus
Vitamin E 600mg/day (n=5)
With a one month wash out, then crossover for another 3 months. Only data from the
first phase was used in data analysis
Outcomes Semen parameters
Notes In Japanese. Data extraction translated by Ichiro, a colleague of Samantha Roberts, 29/
01/09
Author contacted ’no further information is available’.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “Patients were divided randomly”
Allocation concealment (selection bias) Unclear risk No details
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk No details
Incomplete outcome data (attrition bias)
All outcomes
Low risk No incomplete outcome data
Selective reporting (reporting bias) Low risk No statement regarding funding
Other bias Unclear risk Can not definitively assess other bias
47Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Balercia 2005
Methods Randomised trial, double blind. No details of randomisation or concealment
Participants Country: Italy
Infertile men recruited from an andrology clinic
mean age 30 (range 24-38 years)
n=60 recruited
Inclusion criteria: Primary infertility > 2 years after regular intercourse with a fertile
woman; 20-40 years of age; normal rheologic characteristics; sperm count >20 x 106/ml; sperm motility < 50%; normal sperm morphological features > 30%; seminal
WBC <1x106/ml; negative sperm culture and chlamydia and mycoplasma urealyticum;
normal serum gonadotropins; T, E2 and PRL; absence of infectious or genital disease;
no anatomic abnormalities of the genital tract; absence of systemic diseases or treatment
with other drugs within the 3 months before enrolment in the study. Absence of smoking,
alcohol or recreational drug use or of occupational chemical exposure.
Total duration of study 9 months
Interventions L carnitine 3g/day orally (n=15)
versus
L-acetyl carnitine 3g/day orally (n=15)
versus
L carnitine 2g/day + L-acetyl carnitine 1g/day (n=15)
versus
placebo (n=15)
Duration of treatment: 6 months
Outcomes Semen parameters
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “Placebo controlled double blind ran-
domised trial” No methods of randomisa-
tion mentioned
Allocation concealment (selection bias) Unclear risk No details
Blinding (performance bias and detection
bias)
All outcomes
Low risk “double blind” study. Patients blinded but
no details as to who else, assume it is the
clinician
Incomplete outcome data (attrition bias)
All outcomes
Low risk 1 withdrawal from the L carnitine 2g/day
+ L-acetyl carnitine 1g/day group
Selective reporting (reporting bias) High risk Pregnancy was not in the original list of
outcomes but was reported in the results
48Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Balercia 2005 (Continued)
Other bias Unclear risk Can not definitively assess other bias
Balercia 2009
Methods Double blind, placebo controlled randomised trial
Participants Country: Italy (University of Marche, Ancona)
Infertile men recruited from andrology clinic
Mean age: 32 (range 27-32 years)
N= 60 men recruited
Inclusion criteria: Age 20-40 years, infertility >2 years, regular sexual intercourse with
a potentially fertile female; Normal rheologic characteristics (appearance, consistency
and liquefaction) of semen and volume and pH in normal range, sperm count >20 x 106/mL, sperm motility <50% (WHO 1999), normal morphology >30%, seminal white
blood cells <1 x 106/mL and a negative sperm culture and chlamydia and M.urealyticum
detection. Normal levels of gonadotropins absence of genital disease and anatomical
abnormalities of the genital tract including variocoele and antibodies. Absence of systemic
disease or treatment with other drugs within 3 months of being enrolled in the study.
Absence of smoking, alcohol and drug addiction and exposure to occupational chemicals.
Exclusion criteria: Transient decrease in semen quality during run in and those who had
sudden improvement in semen parameters during run in.
Interventions Coenzyme Q10 100mg 2x/day (n=30)
versus
placebo (n=30)
Duration of study: 9 months
Outcomes Primary: Semen parameters
Secondary: Pregnancy rate
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “randomised” - no details. At end of trial
the paper mentions - “after opening ran-
domisation list” page 1789
Allocation concealment (selection bias) Unclear risk No details
Blinding (performance bias and detection
bias)
All outcomes
Low risk “Double blind” - no details
49Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Balercia 2009 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Low risk “5 patients dropped out of the study” 2
from the treatment group and 3 from the
placebo group this was discovered after
opening the randomisation list at the end
of the study. Intention to treat was carried
out.
Selective reporting (reporting bias) High risk Pregnancy was not in the original list of out-
comes but was reported in the results, “al-
though pregnancy was not an end point for
this controlled study, because of many pos-
sible interferences, it is interesting to note
that six pregnancies occurred with patients
given CoQ10”
Other bias Unclear risk Can not definitively assess other bias
Biagiotti 2003
Methods Randomised study - conference proceeding
Participants Country: Italy, Andrology clinic in Bologna
Population: severe idiopathic oligoasthenospermia (sperm concentration >5000/µl)
Mean age: Group a and b 35 (range 30-40 years), Group c 31 (range 24-34)
N= 42
Inclusion criteria: severe idiopathic oligoasthenospermia (sperm concentration >5000/
µl)
Exclusion criteria: Genomic, hormonal or inflammatory diseases
Duration of study: ?
Interventions a-Acetyl-carnitine 1 gr/day + L-carnitine 2gr/day + cinnoxicam (n=14)
versus
b-ALC + LC (n=14)
versus
c-no therapy (n=14)
Duration of treatment: ?
Outcomes Semen parameters
Notes Conference abstract - no data given. Contacted authors but no reply re questions as yet.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk “randomised (1patient = 1 block) analy-
sis of variance” Was this at the time of se-
50Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Biagiotti 2003 (Continued)
quence generation or at data analysis?
Allocation concealment (selection bias) Unclear risk Not mentioned
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Not mentioned
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Unclear
Selective reporting (reporting bias) Unclear risk Unclear
Other bias Unclear risk Can not definitively assess other bias
Cavallini 2004
Methods Randomised controlled trial.
Allocation concealment: anonymous colour coded boxes
Participants Country: Italy
Population: Idiopathic plus variocoele associated oligoasthenospermia (OAT)
Mean age: 34 years (range 27-40)
N= 325
Inclusion criteria: OAT men with deficiencies in all sperm patterns whose chief complaint
was primary couple infertility >12 months with regular intercourse. Normal sperm ap-
pearance, consistency, liquefaction, volume, pH. Female partner without fertility prob-
lems.
Exclusion criteria: Azoospermia, seminal white blood cell concentration more than
1000,000/mL, positive urethral chlamydia swab test, oligospermia < 5000,000mL, hor-
monal alterations, age >40 yrs, presence of anti sperm antibodies, drug, tobacco or alco-
hol abuse, ongoing medical treatments, presence of hydrocoele, diabetes,hypertension,
x ray exposure in previous 8 months, peptic ulcer, unexplained gastric pain, previous
hypersensitivity to NSAIDS or carnitines, carnitine metabolism deficiency, bilateral var-
iocoele, prostate abnormalities, previous or current testicular pathology, testicle echo-
graphic abnormalities.
Duration of study: 9 months
Interventions Group 1: Placebo, starch tablets 2x/day + glycerine suppository (1 every 4 days) (n=47)
Group 2: L-carnitine 1x 2g/day plus acetyl-L-carnitine 500 x 2mg/day plus glycerine
suppository (n=39)
Group 3: L-carnitine 1x 2g/day plus acetyl-L-carnitine 500 x 2mg/day plus glycerine
suppository plus cinnoxicam suppository 1 x 30mg (every 4 days) n=(44). Cinnoxicam
is a non steroidal antiinflammatory therefore this arm (Group 3) was not included in
meta analysis as per protocol.
Duration of treatment: 6 months
51Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Cavallini 2004 (Continued)
Outcomes Primary: Sperm parameters
Secondary: Pregnancy, side effects
Notes Continuous data taken from Cavallini 2004a ’excluded conference abstract’ no data for
placebo group
unit of analysis variocoele’s therefore cannot extract data that were presented as median
(interquartile range)
Author contacted regarding uneven numbers and missing placebo and continuous data
Author replied that raw data were not available due to computer crash
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “the patients were randomised into 3
groups” no details of how randomisation
was carried out
Allocation concealment (selection bias) Low risk “drug placebos identical in appearance”,
“anonymized carnitine and cinnoxicam
and glycerine suppository containers; and
filled and sealed anonymous color coded
boxes”, “the color code was disclosed to
physicians by pharmacists and by IRB at
the end of the research”
Blinding (performance bias and detection
bias)
All outcomes
Low risk “All study personnel and participants were
blinded to treatment assignment for the du-
ration of the study”
Incomplete outcome data (attrition bias)
All outcomes
High risk 325 randomised but only 185 accounted
for. 55 drop outs from 185 i.e. 42%, 53
reasons given for the drop outs
Selective reporting (reporting bias) Unclear risk Unclear
Other bias Unclear risk Can not definitively assess other bias
Ciftci 2009
Methods Randomised controlled trial
Allocation concealment: Sealed envelopes
Participants Country: Turkey
Population: Men attending fertility clinic with idiopathic infertility. Normal sperm pa-
rameters
Mean age: Treatment group 33.1±4.5, Control 32.8±3.7 years
N=120 recruited
52Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Ciftci 2009 (Continued)
Inclusion criteria: Men attending fertility clinic with idiopathic infertility. Normal sperm
parameters
Exclusion criteria: Cryptorchidism, vasectomy, abnormal liver functioning, smoking,
alcohol consumption
Duration of study: 3 months
Interventions N-acetylcysteine 600mg/day (n=60)
versus
placebo (n=60)
Duration of treatment: 3 months
Outcomes Primary outcomes: Total antioxidant capacity, peroxide levels, oxidative stress
Secondary outcomes: Other semen parameters
Notes Attempt made to contact author regarding data reported in SD’s or SE’s email sent
24.09.10
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “patients were randomly allocated to the
study group (60 men) or control group (60
men)”
No mention of how the randomisation was
carried out.
Allocation concealment (selection bias) Low risk “Using sealed envelopes, these patients
were randomly allocated...”
Blinding (performance bias and detection
bias)
All outcomes
Low risk “The patients in the study and control
groups were unaware of whether they were
receiving the drug or placebo.”
? researchers blinded
Incomplete outcome data (attrition bias)
All outcomes
Low risk All men recruited were analysed. No with-
drawals
Selective reporting (reporting bias) Unclear risk No statement of funding
Report includes all expected outcomes
Baseline data were similar for both groups
Other bias Unclear risk Can not definitively assess other bias
53Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Conquer 2000
Methods Randomised placebo controlled trial. 3 arms
Participants Country: Canada
Population: healthy asthenozoospermic individuals who were patients of an infertility
clinic
Mean age: placebo=35.2, DHA 400mg=38.3, DHA 800mg=34.4
N=28
Inclusion criteria: Asthenozoospermic, sperm motility <50% of total sperm
Exclusion criteria: Not stated
Duration of study: Not stated
Interventions Fatty acid omega 3
Docosahexaenoic acid (DHA) 400mg/day (n=9)
versus
DHA 800mg/day (n=10)
versus
placebo (n=9)
Duration of treatment: 3 months
Outcomes Sperm parameters
Notes Data with SEMs converted to SDs
Placebo arms split
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “The 28 subjects were randomly assigned
to ...”
Allocation concealment (selection bias) Unclear risk Not stated
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Placebo capsules made with “corn oil/soy
oil” however blinding not stated.
Incomplete outcome data (attrition bias)
All outcomes
Low risk All men randomised were in the analysis,
no drop outs. All specified outcomes were
reported
Selective reporting (reporting bias) Unclear risk Outcomes reported
Other bias Unclear risk Funding from Martek Bioscience corpora-
tion (also provided the placebo capsules)
54Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Dawson 1990
Methods Randomised controlled trial
Participants Country: USA
Population: males with sperm agglutination
Mean age: age range 25-45 years
N=30
Inclusion criteria: sperm agglutination over 25%, negative sperm antibodies, physically
normal, no inflammatory disease
Exclusion criteria: unclear
Duration of study: 4 weeks
Interventions Ascorbic acid (AA)1000mg (n=10)
versus
AA 200mg (n=10)
versus
placebo (n=10)
Duration of treatment: 3 weeks
Outcomes Seminal parameters
Notes Placebo numbers split by 2
Data were given in standard error converted to standard deviation
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “By random selection, three groups of 10 subjects each..”
Allocation concealment (selection bias) Unclear risk Not stated
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk “Each subject was told he was receiving AA and expected
improvement in sperm quality”
Incomplete outcome data (attrition bias)
All outcomes
Low risk No drop outs
Selective reporting (reporting bias) Unclear risk All specified outcomes were reported
Other bias Unclear risk “supplement and placebo were provided by Hoffmann-
La Roche, Inc, Nutley, NJ.”
55Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Galatioto 2008
Methods Randomised controlled, intention to treat, single centre study. Central allocation - phar-
macy, blinded
Power calculation performed
Participants Country: Italy
Population: Men with persistent oligospermia (5-20m/ml)
Mean age:Treatment group=32 years (27.5-35.5), Control=33(23-36)
N=42
Inclusion criteria: having performed a retrograde embolization with concomitant
oligospermia, persistent oligospermia and infertility > 12 months
Exclusion criteria: smoking, alcohol consumption, taking any fertility drugs within 3
months prior to the study, serious medical or psychiatric condition, abnormal hormonal
profile, sperm infection
Interventions N-acetylcysteine (NAC) 600mg and vitamins-minerals (Vit C, Vit E, Vit A, thiamine,
riboflavin, piridoxin, nicotinamide, pantothenate, biotin, cyanocobalamin, ergocalcif-
erol, calcium, magnesium, phosphate, iron, manganese, copper, zinc. (n= 20)
versus
no treatment (n=22)
Duration: 12 months after end of study which ran for 90 days
Outcomes Primary: seminal parameters
Secondary: pregnancy and adverse effects
Notes Attempted to contact author regarding median data. No response as yet.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk “Subjects were randomly assigned to either
antioxidant therapy or no medical therapy.
Randomisation number was assigned by
random allocation software using a block
randomisation design”
Allocation concealment (selection bias) Low risk ’All steps of randomisation process were
performed blindly in the pharmacy of our
hospital.’
Blinding (performance bias and detection
bias)
All outcomes
High risk Control is no treatment
Incomplete outcome data (attrition bias)
All outcomes
Low risk “intention to treat”
Selective reporting (reporting bias) Low risk Does not appear to be any selective report-
ing
56Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Galatioto 2008 (Continued)
Other bias Unclear risk Can not definitively assess other bias
Greco 2005
Methods Double blind randomised controlled trial. Trialists and patients blinded. Methods were
unclear
Participants Country: France
Population: infertile males
Mean age: ?
N=64
Inclusion criteria: Tunel assay showed a presence of fragmented DNA≥15%of ejaculated
spermatozoa
Exclusion criteria: Variocele, genitourinary inflammation, infection, smoking
Duration of study: ?
Interventions Vitamin C 500mg 2x/day + vitamin E 500mg 2x/day (n=32)
versus
placebo (n=32)
Duration of treatment: 2 months
Outcomes Sperm parameters
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk “The study participants were randomised
into 2 groups”
Allocation concealment (selection bias) Unclear risk No mention of allocation concealment
Blinding (performance bias and detection
bias)
All outcomes
Low risk “The study was double-blinded with both
the authors and the patients unaware of
which of the patients was in the treatment
or control arm of the study”
Incomplete outcome data (attrition bias)
All outcomes
Low risk All specified outcomes are assessed. No
drop outs
Selective reporting (reporting bias) Low risk Does not appear to be any selective report-
ing
Other bias Unclear risk Can not definitively assess other bias
57Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Keskes-Ammar 2003
Methods Randomised controlled trial - open labelled
Participants Country: Tunisia
Population: Infertile men
Mean Age: 35.5±6.8 (SD)
Recruited: N=78
Randomised: N=54
Inclusion criteria: Infertile men who had been married one year
Exclusion criteria: ?
Duration of study: 10 months
Interventions Vitamin E (400mg/day) + selenium (225mg/day) for 3 months (n=12)
versus
vitamin B (4.5g/day) (n=8)
Duration of treatment: 3 months
Outcomes Semen parameters
Notes Attempted to contact authors regarding high attrition rate >50% ?78 men randomised or
78 recruited then only 54 (28 in intervention and 26 in control) Then only 20 analysed
due to non-compliance.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk ”Randomisation was performed with ran-
dom numbers“ and the numeric code was
withheld from researchers and patients”
Allocation concealment (selection bias) Unclear risk open label
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk “The trial was randomised and open” How-
ever “the numeric code was withheld from
researchers and patients”
Incomplete outcome data (attrition bias)
All outcomes
Low risk High attrition rate was due to non-compli-
ance, no intention to treat.
Selective reporting (reporting bias) Unclear risk MDA post treatment has no SD no expla-
nation
Other bias Unclear risk Can not definitively assess other bias
58Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kessopoulou 1995
Methods Double blinded randomised placebo cross over trial
Power calculation performed
Participants Country: UK, Sheffield
Population: Men with high levels of reactive oxygen species (ROS) attending Obstetrics
and Gynecology department for infertility
Couples were undergoing IVF
Mean Age: ? Median age: 32 years
Recruited: N= 30
Inclusion criteria: Attending fertility clinic, high levels of ROS in semen. Female partner
has tubal patency and is ovulating
Exclusion criteria: Men with antisperm antibodies, >20% spermatozoa with Ig (immuno
globin A) and/or IgG antibodies and sperm concentration <5x 06 mL
Duration of study: 2 years
Interventions Vitamin E 300mg 2x/day (n=15)
versus
identical placebo (n=15)
Duration of treatment: 3 months
Outcomes Primary outcomes: Semen parameters
Secondary outcomes: Adverse effects. Live birth
Notes Attempted to contact author regarding median data, no response as yet
Only first phase data used in analysis
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “The study was a randomised double blind
placebo controlled trial”. “The randomisa-
tion was performed by the manufacturer”
Allocation concealment (selection bias) Unclear risk “The randomisation was performed by the
manufacturer”
Blinding (performance bias and detection
bias)
All outcomes
Low risk “the code was blind for the researcher and
patients. The code was broken at the end
of the trial”
Incomplete outcome data (attrition bias)
All outcomes
Low risk All outcomes are reported
Selective reporting (reporting bias) Low risk Does not appear to be any selective report-
ing
Other bias Unclear risk Funding grant by EEC. Tablets provided
by pharmaceutical company
59Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lenzi 2003
Methods Randomised placebo controlled, double blind crossover trial.
Power calculation performed
Participants Country: Italy
Population: Male factor infertility - oligoasthenoteratozoospermia (OAT).
Mean age: ? Range: 20-40 years
N=100
Inclusion criteria: Men are aged between 20-40 years with infertility lasting longer than
2 years. Regular sexual intercourse with a gynaecologically normal female partner with
no female infertility. Absence of endocrine disease, genital infections, obstructive cryp-
torchism, antisperm antibodies, normal sperm parameters with no significant differences
after 3 tests. Mild oligospermia. Sperm concentration 10-20 x 106/mL and motility 10-
30%
Exclusion criteria: Not mentioned
Duration of study:10 months
Interventions L-carnitine 2g/day (n=43)
Versus
placebo (n=43)
Duration of treatment: 6 months
Outcomes Semen parameters and pregnancy rate
Notes First phase data only used in analysis
Attempted to contact author regarding standard deviations, how many were in each
group for the 1st phase and how many of the 4 who went to assisted reproduction did
so in the 1st phase and what do they mean by 172 cycles. No response yet.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “we report on a randomised placebo con-
trolled cross over trial”. No mention of
method of randomisation
Allocation concealment (selection bias) Unclear risk No mention
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Double blinded. “seemingly identical
placebo”
Incomplete outcome data (attrition bias)
All outcomes
Low risk 14 withdrew - 4 went onto assisted re-
production, 6 did not return for 2nd pe-
riod and 4 due to pregnancy in first phase.
Therefore should only be ?4 at the most lost
from 1st phase. No intention to treat
All withdrawals accounted for for whole
trial however how many were lost in the
60Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lenzi 2003 (Continued)
first phase in first phase
Selective reporting (reporting bias) Unclear risk Although all outcomes are reported but no
standard deviations given
Other bias Unclear risk Funding stated - University grant. Tablets
from Sigma Tau SRL
Lenzi 2004
Methods Placebo controlled, double blind randomised trial. No mention of method of randomi-
sation or allocation concealment
“When codes were broken at the end of the study”
Power calculation performed
Participants Country: Italy
Population: Infertile males with oligoasthenoteratozoospermia
Mean age: Not stated. Age range 20-40 years
N=60
Duration of study: 8 months
Inclusion criteria: oligoasthenoteratospermia, age between 20-40 years, infertility >2years
with regular intercourse. No endocrine disease, cryptorchidism, genital infections/ob-
structions, variocoele or testicular hypertrophy, antisperm antibodies
Exclusion criteria: None
Duration of study: 8 months
Interventions L-carnitine 2g/day + L-acetyl-carnitine 500mg 2x/day (n=30)
versus
placebo (n=26)
Duration of treatment: 6 months
Outcomes Semen parameters and pregnancy rate
Notes Attempted to contact author regarding 8 month follow up data. No reply as yet.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “placebo controlled double blind ran-
domised trial”
Allocation concealment (selection bias) Unclear risk Mentions coding - “When codes were bro-
ken at the end of the study”
Blinding (performance bias and detection
bias)
All outcomes
Low risk Double
61Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lenzi 2004 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk 4 men withdrew from the placebo group.
60 randomised 56 analysed. No intention
to treat
Selective reporting (reporting bias) Unclear risk Unclear
Other bias Unclear risk Can not definitively assess other bias
Li 2005
Methods Double blinded randomised parallel trial
Participants Country: Eastern China
Population: infertile men with oligoasthenospermia
Mean Age: Treatment 30±5.5 (23-45 years), Control 32±3.5 (24-46 years)
N=150
Inclusion criteria: No smoking or alcohol. Any fertility medication needed to be stopped
2 weeks before
Exclusion criteria: Nil
Duration: 3 months
Interventions L-carnitine 2g/day + acetyl-L-carnitine 1g/day (n=85) (90 with intention to treat)
versus
vitamin E (100 mg tid) + vitamin C (100mg tid) (n=53) (60 with intention to treat)
Duration of treatment: 3 months
Outcomes Seminal parameters and pregnancy rate per couple
Notes Withdrawal: 5 from treatment group and 7 from control
Query whether randomised as there is imbalance between the groups. Contact author
re methods of randomisation (large imbalance of numbers), concealment and whether
SD or SE’s used and query that this is the same trial as Li 2005a
Translated by Shaofu Li 10/11/08
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Randomised controlled trial. Methods not
described. Unexplained differences in the
number of men in the treatment and con-
trol groups
Allocation concealment (selection bias) Unclear risk Allocation concealment not described
Blinding (performance bias and detection
bias)
All outcomes
Low risk Double
62Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Li 2005 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
High risk Unexplained imbalance between the num-
ber of men randomised into the treatment
and control groups
Selective reporting (reporting bias) Unclear risk Unclear whether data given in standard de-
viations or standard errors
Other bias Unclear risk Unexplained imbalance between the num-
ber of men randomised into the treatment
(n90) and control groups (n60)
Li 2005a
Methods Randomised trial. No information on concealment
Participants Country: Eastern China
Population: Infertile men with oligoasthenospermia
Mean age: 29±3.5 (23-40 years)
N=80
Inclusion criteria: No smoking or alcohol. Any fertility medication needed to be stopped
2 weeks before
Exclusion criteria: Nil
Duration: Not stated
Interventions L-carnitine 2g/day (n=40)
versus
vitamin E 100mg + vitamin C 100mg tid (n=40)
Duration of treatment: 3 months
Outcomes Seminal parameters and pregnancy
Notes Attempted to contact author re methods of randomisation, concealment and whether
SD or SE’s used and whether this is the same trial as Li 2005. Also asked whether there
were any data on pregnancy rate. Translator replied 22.09.09 no pregnancy data were
available in the text of the trial.
Translated by Shaofu Li 10/11/08
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk No mention of methods of randomisation
Allocation concealment (selection bias) Unclear risk No mention of allocation concealment
63Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Li 2005a (Continued)
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk No mention of blinding
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Withdrawal: 8 from treatment (n=32) and
9 from control (n=31). 21% loss to follow
up. No intention to treat
Selective reporting (reporting bias) High risk No data on pregnancy outcome
Other bias Unclear risk Can not definitively assess other bias
Lombardo 2002
Methods Randomised controlled crossover trial
Participants Country: Italy
Population: male infertility, oligoasthenospermia
Mean age: Not stated
N=100
Inclusion criteria: Age 20-40 years. Infertility > 2 years. 3 baseline semen analysis demon-
strating concentration 10-20 106/mL , %motility 10-30%, forward progression <15%,
abnormal morphological forms <70%, curvilinear velocity 10-30/second + linearity <4
Exclusion criteria: not mentioned
Duration: 10 months
Interventions L-carnitine 2g/day (n=?)
versus
placebo (n=?)
Duration of treatment: 2 months
Outcomes Semen parameters
Notes Abstract only
Attempted to contact author re 1st phase data, outcomes, randomisation, concealment
and whether there was a full publication of the trial.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk randomised -“all patients had an initial 2
months run in period and then randomised to
2 months of carnitine or placebo.”
Allocation concealment (selection bias) Unclear risk No mention of allocation concealment
64Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lombardo 2002 (Continued)
Blinding (performance bias and detection
bias)
All outcomes
Low risk “double blind crossover trial”
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk 86 patients completed the trial out of 100.
Need to see full trial for the reasons for with-
drawals and intention to treat
Selective reporting (reporting bias) Unclear risk Unclear
Other bias Unclear risk Funding stated - “support: None”
Merino 1997
Methods Randomised controlled trial
Participants Country: Mexico
Population: Male idiopathic asthenozoospermia attending a fertility clinic
Mean age: 30.8±6 (20-40 years)
N=47
Inclusion criteria: Free of urogenital symptoms, idiopathic asthenozoospermia, not re-
ceived drugs in prior 6 months and healthy
Exclusion criteria: Variocoele, inflammatory diseases, endocrine disorders
Duration of study: 6 months
Interventions Pentoxifylline 1200mg - 400mg/3xday (n=25)
versus
placebo (n=22)
Duration of intervention: 6 months
Outcomes Seminal parameters and hormonal assays
Notes Attempted to contact author to ask if had data in means + SD and not medians + range
as published. Letter sent 15.09.09. Letter returned to sender.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “The 47 men were divided at random”
Allocation concealment (selection bias) Unclear risk No mention of allocation concealment
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk No mention of blinding however the trial is placebo con-
trolled
65Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Merino 1997 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk No withdrawals
Selective reporting (reporting bias) Unclear risk ?all outcomes reported however seminal outcomes re-
ported in medians
Other bias Unclear risk Can not definitively assess other bias
Micic 1988
Methods Randomised controlled trial
Methods not stated. No mention on methods of concealment
Participants Country: Belgrade, Hungary
Population: idiopathic oligoasthenospermia
Mean age:29±2 in treatment group, 26±3 in control group
N=90
Inclusion criteria: idiopathic oligoasthenospermia and no pregnancy for 2 years
Exclusion criteria: Variocoele, inflammatory diseases, endocrine disorders
Duration of study: 3 months
Interventions Pentoxifylline 1200mg/day (n=51)
versus
no treatment (n=39)
Duration of treatment: 3 months
Outcomes Seminal parameters
Notes Attempted to contact author regarding extractable data for pregnancy rate plus methods
of of randomisation and concealment also don’t know if adverse events are single or
multiple events. No reply as yet.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “A randomised group of 90 men”
Allocation concealment (selection bias) Unclear risk No mention of allocation concealment
Blinding (performance bias and detection
bias)
All outcomes
High risk No mention of blinding
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Don’t know if adverse events are single or
multiple. Pregnancy data not extractable
66Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Micic 1988 (Continued)
Selective reporting (reporting bias) Unclear risk All randomised were analysed
Other bias Unclear risk Can not definitively assess other bias
Nozha 2001
Methods Randomised comparative study
No mention of allocation concealment
Abstract only
Participants Country: Tunisia
Population: Infertile males with oligoasthenoteratozoospermia
Mean age: not stated
N=?
Inclusion criteria: males with oligoasthenoteratozoospermia.
Exclusion criteria: none mentioned
Duration of study: not stated
Interventions Vitamin E (400mg) + selenium (200mµg)/day (n=12)
versus
vitamin B (B2, B6 and B12) (n=8)
Duration of treatment: 3 months
Outcomes Seminal parameters
Notes Attempted to contact authors regarding methods of randomisation and data - no ex-
tractable data from the abstract. No reply as yet.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “In a prospective randomised comparative
study”
Allocation concealment (selection bias) Unclear risk No mention of allocation concealment
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk No mention of blinding
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Unclear
Selective reporting (reporting bias) Unclear risk Unclear
Other bias Unclear risk Can not definitively assess other bias
67Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Omu 1998
Methods Randomised controlled trial
Open trial - control is no treatment
Participants Country: Kuwait
Population: Men with asthenozoospermia attending infertility and andrology clinic
Mean age: 37.8±7.9 in treatment group, 38.1±8.2 in control
N= 100
Inclusion criteria: Men with asthenozoospermia. Spermatozoal motility impaired with
>40% non mobile sperm. Have been trying to conceive for at least one year. Plus no
obvious female factor
Exclusion criteria: None mentioned
Duration of study: 12 months
Interventions Zinc 250mg 2xday (n=49)
versus
no treatment (n=48)
Duration of treatment: 3 months
Outcomes Seminal parameters
Notes Attempted to contact authors regarding methods randomisation and concealment ques-
tioned. No reply as yet.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Randomised. “100 men with Astheno-
zoospermia were randomised into two
groups”
Allocation concealment (selection bias) Unclear risk No mention of allocation concealment
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk No mention of blinding
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk 100 men randomised, 97 analysed, drop
outs are accounted for
Other bias Unclear risk Funding - Kuwait University
68Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Omu 2008
Methods Randomised controlled 4 armed trial, open as one arm of the trial is no therapy
Participants Country: Kuwait
Population: Men with Asthenozoospermia attending infertility clinic in Kuwait
Mean age: 35±1
N= 45
Inclusion criteria: Asthenozoospermia with normal sperm concentration (20-250mill/
ml) but with 40% or more immotile sperm
Exclusion criteria: Asthenozoospermia but sperm concentration of <20 mill/ml
Duration of study: No stated
Interventions Zinc 200mg 2x/day (n=11)
versus
zinc 200mg + vitamin E 10mg 2x/day (n=12)
versus
zinc 200mg + vitamin E 10mg + vitamin C 5mg 2x/day (n=14)
versus
no therapy (n=8)
Duration of intervention: 3 months
Outcomes Seminal parameters
Notes Attempted to contact author re methods of randomisation - states that “8 men served as
non- therapy control”. No reply as yet.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “the 45 asthenozoospermic men were ran-
domised into four groups”
Allocation concealment (selection bias) Unclear risk No mention of allocation concealment
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk No mention of blinding
Incomplete outcome data (attrition bias)
All outcomes
Low risk All outcomes are reported. No drop outs
Selective reporting (reporting bias) Unclear risk Appears to be free of selective reporting
Other bias Unclear risk Can not definitively assess other bias
69Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Peivandi 2010
Methods Double blind randomised crossover trial
Participants Country: Iran
Population: Infertile men with at least two abnormal spermiograms
N=30
Exclusion criteria: variocoele, testicular atrophy, ejaculatory disorders, use of medications,
azoospermia, endocrinological disorders, ICSI candidacy or other causes of infertility
Duration of 1st phase: 8 weeks
Interventions L-carnitine (2g/day)
versus
placebo
Outcomes Sperm parameters
Notes Abstract in English, full text in Arabic. Contacted the author and he is filling out the data
extraction sheets. Author responded but data queries remain contacted again re SD’s and
pregnancies in 1st phase of cross over. Author responded saying that the data was given
in SD’s and there were 3 pregnancies in the 1st phase.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk ”patients were randomly allocated to two
groups of A and B“
Allocation concealment (selection bias) Low risk ”sealed opaque envelopes“
Blinding (performance bias and detection
bias)
All outcomes
Low risk ”Double blind“ ”outcome assessor was
blinded“
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk ’loss to follow up was not accounted for”
Selective reporting (reporting bias) Unclear risk “Pregnancy was not our major goal but when
we found a positive pregnancy test after treat-
ment with carnitine, we reported the results”
Standard deviations appear to be unusual
Other bias Unclear risk Can not definitively assess other bias
70Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Rolf 1999
Methods Randomised placebo controlled double blind study
No mention of allocation concealment
Power calculation performed
Participants Country: Munster Germany
Population: men with infertility for over one year.
Mean age: treatment 36.1±5.0, placebo 35.2±4.8
N= 33
Inclusion criteria: Asthenozoospermia (<50% motile) diagnosed after 2 examinations,
normal or reduced sperm concentration (>20 x 106 per ejaculate) and without infection
of access glands
Exclusion criteria: None mentioned
Duration of study: 8 weeks
Interventions Vitamin C 1000mg + vitamin E 800mg/day (n=15)
versus
placebo (n=16)
Duration of treatment: 8 weeks
Outcomes Primary: Semen parameters
Secondary: Pregnancy rate and adverse effects
Notes Contacted author about the allocation concealment and pregnancy and adverse effects
were outcomes in their protocol. Rolf replied saying that pregnancy and adverse effects
were stated in the protocol.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk “Randomisation was performed with ran-
dom numbers without further stratification
by the pharmacist and the code was with-
held from researchers and patients”
Allocation concealment (selection bias) Unclear risk Pharmacist performing randomisation and
code withheld from patients and re-
searchers. However no mention of type of
containers or envelopes
Blinding (performance bias and detection
bias)
All outcomes
Low risk Double - patients and researchers
Incomplete outcome data (attrition bias)
All outcomes
Low risk All data reported. 2 patients withdrew form
the trial - “results from two patients were
rejected from analysis.” 1 from the treat-
ment group due to poor compliance and 1
from the placebo group due to genital tract
71Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Rolf 1999 (Continued)
infection. Intention to treat
Selective reporting (reporting bias) Low risk All semen outcomes reported and author
states (email 22.09.09) that pregnancy and
adverse effects were set a priori in the pro-
tocol
Other bias Unclear risk Funding stated - Health Ministry
Safarinejad 2009
Methods Double blind placebo controlled randomised study. Randomised using permuted blocks
Allocation concealment: Sealed envelopes
Blinding: Double, identical coating of tablets
Power calculation performed
Participants Country: Iran
Population: Idiopathic oligoasthenoteratospermia, asthenospermia or teratospermia of
2 years duration
Mean age: 31 years (25-48 years)
Recruited: N= 548
Randomised: N= 468
Inclusion criteria: Sperm count >5 x 106/ml, over 2 years of failed conception, no female
fertility problems, no history of possible cause for male infertility
Exclusion criteria: Abnormal testes, history of cancer or chemotherapy, testosterone or
antiandrogen use, use of selenium or N-acetyl-cystine supplements, abnormal hormone
levels, genital disease, genital inflammation or variocoele, history of genital surgery, major
surgery, central nervous system injury, a known sperm defect or retrograde ejaculation. Y
chromosome abnormalities, sexually transmitted disease, genitourinary infection, leuko-
cytospermia, smoking, any environmental exposures to reproductive toxins. Medical,
neurological or psychological problems. A history of drug or alcohol abuse, hepatobil-
iary disease or significant renal insufficiency. Any endocrine abnormality, a body mass
index (BMI) of 30kg/m2 or over, participation in another investigational study and a
likelihood of being unavailable for follow up.
Duration of study: 56 weeks
Interventions Selenium 200 µg/day (n=116)
versus
N-acetylcysteine 600mg/day (n=118)
versus
selenium 200 µg/day + N-acetylcysteine 600mg/day (n=116)
versus
placebo (n=118)
Duration of treatment: 26 weeks or 6.5 weeks
Analysed: n= 105 in selenium group (loss 11), n= 106 in placebo group (loss 12), n=105
in N-acetylcysteine group (loss 13) and n= 104 in selenium + N-acetylcysteine group
(loss 12)
72Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Safarinejad 2009 (Continued)
Outcomes Primary outcome: Semen parameters
Secondary outcomes: adverse events
Notes Attempted to contact authors regarding side effect data that had not yet been added to
the review due to the query of multiple comparisons. Also to ask whether data is in SD
or SE as requested by statistician 24.09.10.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk “randomisation table generated by the
method of random permuted blocks. Pa-
tient randomisation numbers were allo-
cated to each site in ascending sequence in
blocks.”
Allocation concealment (selection bias) Low risk “Assignment to treatment groups was per-
formed using a sealed envelope technique.”
Blinding (performance bias and detection
bias)
All outcomes
Low risk “Eligible patients were randomly assigned
to double blind..”
“Placebo pills were coated with titanium
oxide to ensure an identical appearance and
smell.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk All withdrawals were accounted for in each
treatment group. Withdrawal was mainly
due to withdrawal of consent followed by
lost to follow up and lastly for reasons of
missing data. No intention to treat
Selective reporting (reporting bias) Low risk The published report includes all expected
outcomes
Other bias Unclear risk Can not definitively assess other bias
Safarinejad 2009a
Methods Randomised controlled trial, double blind
Allocation concealment: Not mentioned
Power calculation performed
Participants Country: Tehran, Iran
Population: Infertile males between 21 and 42 years with idiopathic oligoasthenoter-
atospermia.
Mean age: Treatment group 28±9, Placebo 28±10. (Range 21-42 years)
Recruited: N= 268
73Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Safarinejad 2009a (Continued)
Randomised: N=212
Inclusion criteria: Minimum 2 years unprotected intercourse with 2 years unwilling
childlessness. male infertility diagnosed if 1 or more standard semen parameters were
below cutoff levels accepted by World Health Organisation (WHO). A fertile female
partner. No known medical condition that could account for infertility, testicular volume
12 ml or greater. No medical therapy for at least 12 weeks before the study begins. Only
patients seeking medical attention for infertility were included.
Exclusion criteria: Azoospermia or severe oligospermia (sperm count less than 5 million/
ml. An history of epypidymo-orchitis, prostatitis, genital trauma, testicular torsion, in-
guinal or genital surgery. Any genital or central nervous system disease, endocrinopathy,
cytotoxic drugs, immunosuppressants, anticonvulsives, androgens, antiandrogens, a re-
cent history of Sexually transmitted disease. Psychological or physiological abnormalities
that would impair sexual functioning or ability to produce sperm samples. Drug, alco-
hol or substance abuse. Liver disease, renal insufficiency or chromosome abnormalities.
occupational and environmental exposures to reproductive toxins. A body mass index
(BMI) of 30kg/m2 or over, participation in another investigational study and a likelihood
of being unavailable for follow up.
Duratoin of study: 20 months, from February 2005 until October 2006
Interventions Coenzyme Q10 (CoQ10) 300mg/day (n=106)
versus
placebo (n=106)
Duration of treatment: 26 weeks or 6.5 weeks
Analysed n= 98, 8 withdrawals in treatment group, analysed n=96, 10 withdrawals in
the placebo group
Outcomes Primary outcomes: semen parameters and testicular volume
Secondary outcomes: adverse effects and hormone levels
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk “Each eligible patient received a randomi-
sation number, which was determined by a
computer generated schedule. Therafter a
randomisation table was generated by the
method of random permuted blocks. Indi-
viduals who were geographically and oper-
ationally independent of the study investi-
gator performed the study randomisation”
Allocation concealment (selection bias) Unclear risk Allocation concealment: not mentioned
Blinding (performance bias and detection
bias)
All outcomes
Low risk “The clinician prescriber and the patients
were blinded to the treatment condi-
tion. To maintain and guarantee blinding
74Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Safarinejad 2009a (Continued)
CoQ10 and placebo were identical in ap-
pearance. Participant data collected dur-
ing this trial were kept confidential and
locked in a secure office area. Randomisa-
tion codes were opened only after all pa-
tients had completed the whole study pro-
tocol.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk All patients who dropped out of the trial
were accounted for - 8 from treatment
group and 10 from placebo group for rea-
sons such as withdrawal of consent, miss-
ing data and loss to follow up
Selective reporting (reporting bias) Unclear risk All semen, hormone and adverse effects
outcomes reported. Pregnancy outcome
not stated as an outcome initially but it was
reported on in the discussion
Other bias Unclear risk Funding source not stated. Can not defini-
tively assess other bias
Scott 1998
Methods Double blind randomised trial
Allocation concealment: no mention
Participants Country: Glasgow, UK
Population: Men attending subfertility clinic with low sperm motility
Mean age: 33.3 years±0.64
Recruited: N=69
Analysed: N=64
Inclusion criteria: Low sperm motility
Exclusion criteria: Not mentioned
Duration of study: 3 months and two weeks
Interventions Selenium 100µg/day (n=16)
versus
selenium 100µg + vitamin A 1mg + vitamin C 10mg + vitamin E 15mg/day (n=30)
versus
placebo (n=18)
Duration of treatment: 3 months
Analysed = 64, 5 withdrew 1 from selenium group, 4 from selenium + vit A, C and E
group. All withdrawals were due to non-compliance
Outcomes Primary outcome: semen parameters
Secondary outcome: Pregnancy rates given although not stated as an initial outcome
75Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Scott 1998 (Continued)
Notes Uneven numbers, multivitamin numbers are double the other groups
Need to ask author if they have separate numbers for pregnancy data. Currently have 5
pregnancies in the 2 treatment groups and none in placebo
Who was blinded, was the placebo identical when group 2 contained so many different
vitamins
Was there any allocation concealment?
Author has retired and is not contactable
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “As the patients entered the trial they were
randomly allocated to one of three treat-
ments, which had in turn been randomised
within each block of four numbers and
’blinded’ using a numeric code.”
Unclear as to why the uneven nature of the
numbers in the groups i.e. 30 in multivi-
tamin group and 16 in Selenium, 18 in
placebo
Allocation concealment (selection bias) Unclear risk Not mentioned
Blinding (performance bias and detection
bias)
All outcomes
Low risk Double blind
Incomplete outcome data (attrition bias)
All outcomes
Low risk Numbers of withdrawals and reasons (non
compliance) were reported
Selective reporting (reporting bias) Unclear risk Sperm counts and motility were reported
as per trial methods. Pregnancy rates were
given in the results of the trial, these had not
been specified in the methods. The preg-
nancy results given as a combination of the
2 vitamin groups. There were no pregnan-
cies in the placebo group
Other bias Unclear risk Can not definitively assess other bias
76Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Sigman 2006
Methods Randomised double blind trial
Allocation concealment: adequate
Participants Country: Minneapolis, USA
Population: Males aged 18-65 years
IVF
Mean age: 36.2±5.8 (SD), 35.3±7.5 (SD)
Recruited: N=26
Analysed: N=21, 5 withdrawals
Inclusion criteria: Males 18-65 years with infertility of at least six months duration,
sperm concentration of at least five million sperm/mL, motility of 10%-50%, absent
pyospermia and normal FSH and testosterone levels.
Exclusion criteria: History of post pubertal mumps, cryptorchism, vasal or epididymal
surgery, history of medication or chemotherapy. recent alcohol, chronic marijuana. Use
of testosterone or steroids. Exposure to environmental toxins. Recent history of fever or
diabetes, liver failure, renal failure, endocrine disorder, untreated variocoele, urogenital
infection, or prior vasectomy reversal.
Duration of study: 24 weeks
Interventions Carnitine (L-carnitine 2000mg +L-acetylcarnitine 1000mg/day) (n=12)
versus
placebo (n=9)
Outcomes Primary outcome: semen parameters
Secondary outcomes: Pregnancy - 2 pregnancies, 1 in the treatment arm after IVF and
one in placebo through intercourse
Notes Author replied 21.09.09 saying ’The published 2006 trial is the published version of
the 2003 abstract (Pryor 2003)’ and giving details of randomisation and concealment.
Author says he will try and find out about the 5 patients that dropped out.
Why did - ”5 additional patients entered the study but dropped out before completion“
- when did these patients enter and were they randomised? ”One of these 5 dropped out
because of pregnancy three months after starting carnitine“ Pryor paper excluded as it
is the same study as Sigman, author also gave details of randomisation and allocation
concealment, author will try to find info on 5 patients who dropped out.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk ”Patients were randomised to receive carni-
tine or placebo“
”The randomisation was done by a 3rd
party a company that oversaw the trial. We
sent the patient number of new recruited
patients in to them, they assigned them a
study number that was associated with a
collection of medication/placebo.“
The author replied to randomisation query
77Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Sigman 2006 (Continued)
23.09.09 saying that the protocol stated
that - ”treatments will be assigned ran-
domly to a subject number. The numbers
will range from 1-84 for study centre 1 and
85-168 for study centre 2. Randomisation
of treatments for each centre will be done
independently. One half of subject num-
bers will be placebo, the other half, active
ingredient.“
Allocation concealment (selection bias) Low risk ”The investigators and study sites had the
study medication/placebo packets identi-
fied by number only. They were blinded to
what was in the medication/placebo pack-
ets. We were sent the code at the con-
clusion of the trial.“ The author replied
to a query on allocation concealment on
23.09.09 saying that the protocol stated
that - ” Integrated Data Solutions, Inc. will
keep the randomisation code in a separate
sealed envelope for each site until the end
of the study. The randomisation lists will
be provided to the packaging company for
packaging of the packets into patient med-
ication boxes.”
Blinding (performance bias and detection
bias)
All outcomes
Low risk “Both the investigators and the patient were
blinded to the treatment arm assignment.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk “5 additional patients entered the study
but dropped out before completion. One
of these dropped out because of pregnancy
three months after starting carnitine.” Au-
thor replied to query re drop outs - “I have
data on one drop out at my site - the drop
out occurred after randomisation to carni-
tine. The drop out occurred before the first
follow-up study visit. The other four drop
outs were from the other study site - I am
trying to get that data for you” (23.09.09)
Selective reporting (reporting bias) Unclear risk Baseline data were similar
Pregnancy data were not an outcome but is
reported in the paper
All outcomes of interest were reported
Other bias Unclear risk Can not definitively assess other bias
78Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Suleiman 1996
Methods Double blind randomised controlled trial
No mention of allocation concealment
Participants Country: Saudi Arabia
Population: Men attending a fertility centre
Mean age: 34.8 (27-52 years), placebo 33.2 (22-45 years)
N=110
Inclusion criteria: Asthenospermic (>/=20 x 106/ml). sperm motility </= 40%, normal
sperm count, leucocyte concentration <5%, normal fructose concentration. Normal
female
Exclusion criteria: None mentioned
Duration of study: 6 months
Interventions Vitamin E 100mg 3x/day (n=52)
versus
placebo 3x/day (n=35)
Duration of treatment: 6 months
Outcomes Primary outcome: motility and MDA concentration
Secondary outcome: live birth, pregnancy, miscarriage
Notes Method of randomisation not stated. Large imbalance between the treatment (n=52)
and placebo group (n=35) at analysis. Drop outs were accounted for in text.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “ Either 100mg vitamin E or a placebo was
prescribed in a random double blind fash-
ion”. Method of randomisation not stated.
Large imbalance between the treatment (n=
52) and placebo group (n=35) at analysis
Allocation concealment (selection bias) Unclear risk Not mentioned
Blinding (performance bias and detection
bias)
All outcomes
Low risk “Double blinded”. Does not report on who
was blinded
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk All men who dropped out the trial were ac-
counted for. Although the exact figures for
each group is unclear - “A total of 110 pa-
tients were enrolled in the study, but some
of the patients dropped out and some left
the region and failed to continue. When
the experiment was terminated, 52 patients
were found to have taken vitamin E and 35
patients to have taken the placebo.”
79Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Suleiman 1996 (Continued)
Selective reporting (reporting bias) Unclear risk All outcomes stated in the methods were
reported in results
Other bias Unclear risk Unequal reporting bias “If the semen sam-
ple improved and the patient’s spouse be-
came pregnant, the treatment was stopped;
otherwise it was continued for 6 months.
The placebo was given for 6 months” Un-
equal reporting ?? incomplete outcome data
addressed
Tremellen 2007
Methods Randomised double blind controlled trial. randomisation by computer generated blocks.
Using a 2:1 ratio (treatment 2: placebo 1)
Allocation concealment: numbered bottles delivered to the site with all members of the
trial blinded to sequence, identical placebo
Power calculation performed
Participants Country: Australia
Population:male factor infertility undergoing IVF
Mean age: treatment group - 37.1±5.1, placebo group - 35.5±4.3
Recruited: N= 82
Randomised: N= 60
Inclusion criteria: men with sperm samples showing oxidative stress and a significant
level of DNA fragmentation (>25% Tunel positive)
Exclusion criteria: Female partner with diminished ovarian reserve or if the female partner
is aged over 39 years
Duration of study: 1.5 years
Interventions Menevit (folate 0.5mg, garlic 1000mg, lycopene 6mg, vitamin E 400 IU, vitamin C
100mg, zinc 25mg, selenium 26 µgm, palm oil). One capsule per day
versus
placebo (identical in appearance and taste - containing palm oil)
Duraton of treatment: 3 months prior to IVF cycle
Outcomes Primary outcome: embryo quality
Secondary outcomes: pregnancy, fertilization rate, side effects
Notes The study reports only on 37 men in the treatment group and not 38. There is no
explanation of the one man missing from this analysis.
Risk of bias
Bias Authors’ judgement Support for judgement
80Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Tremellen 2007 (Continued)
Random sequence generation (selection
bias)
Low risk “The randomisation schedule was com-
puter generated in blocks of six by Bayer
Consumer Care Australia”. Using a 2:1 ra-
tio
“There were no significant differences be-
tween the active and the placebo group
in terms of important baseline prognostic
characteristics...”
Allocation concealment (selection bias) Low risk “the appropriately numbered bottles of
capsules delivered to the clinical site with-
out any participant knowing the treatment
sequence. Patients were allocated the next
numerical treatment package (one to sixty
as they became eligible for enrolment”
Blinding (performance bias and detection
bias)
All outcomes
Low risk “double blind placebo controlled trial”
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk All withdrawals were accounted for, 2 from
the intervention group, 4 from placebo all
due to the couples not going through to
embryo transfer
The study reports only on 37 men in the
treatment group and not 38 (page 219 ?
typo). There is no explanation of the one
man missing from this analysis Intention
to treat stated
Selective reporting (reporting bias) Low risk All specified outcomes are reported
Pregnancy only followed to 13 weeks
Other bias Unclear risk Can not definitively assess other bias
Wang 1983
Methods Randomised placebo controlled trial
Participants Country: Hong Kong
Population: New patients attending infertility clinic
Mean age: 33.7±4.4 years (28-45 years)
N=46
Inclusion criteria: Men with Idiopathic oligospermia attending fertility clinic with nor-
mal hormones. They had not received treatment with pharmacologic agents for 1 year
prior to entry into the trial. None of the female partners had irreversible causes of female
infertility
Exclusion criteria: Not mentioned
81Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Wang 1983 (Continued)
Duration of study: 6-9 months
Interventions Pentoxifylline 400mg 3 x/day (n=11)
versus
placebo (n=7)
Duration of treatment: 6 months
Other interventions not included in meta analysis were clomiphene citrate, mesterolone
and testosterone enanthate
Outcomes Primary outcome: Semen parameters and pregnancy
Notes Pentoxifylline supplied by Hoechst Aktiengesellshaft
Attempted to contact the author re motility data as it was stated in the paper that this
was an outcome. Also asked about control data for post treatment period and methods
of randomisation + allocation concealment. Author replied saying she no longer has the
data.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “the subjects were randomly assigned to one of
the therapy groups..”
No mention of methods of randomisation
Allocation concealment (selection bias) Unclear risk No mention of allocation concealment
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding - one of the interventions was an
intra muscular injection while the others were
oral
Incomplete outcome data (attrition bias)
All outcomes
High risk Sperm motility data not given when motility was
discussed as an outcome of interest
Selective reporting (reporting bias) High risk No post-treatment control data given however
there is post-treatment given for treatment group
No intention to treat reported
Side effects reported in the results but this was
not stated as an initial outcome
Other bias Unclear risk Funding - Hoechst Aktiengesellshaft
82Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Wong 2002
Methods Double blind randomised placebo controlled interventional study. Computer generated
randomisation
Allocation concealment: central pharmacy coding
Participants Country: Netherlands
Population: Fertile and subfertile men
Mean age: 34.3±3.9 years
Recruited: N=258 subfertile
Randomised: N=103
Inclusion criteria for subfertile group: failure to conceive after 1 year regular unprotected
intercourse and sperm concentration of 5 - 20 million/ml
Exclusion criteria for subfertile group: chromosomal disorders, cryptorchidism, vasec-
tomy, use of folic acid or zinc supplements in the previous 3 months, vitamin B defi-
ciency
Duration of study: 1 year
Interventions Folic acid 5mg/day (n=22)
versus
placebo (n=25)
Zinc sulphate 66 mg/day (n=23)
versus
placebo (n=25)
Zinc sulphate 66 mg/day + folic acid 5 mg/day (n=24)
versus
placebo (n=25)
Duration of treatment: 26 weeks
Outcomes Semen parameters
Notes Data in median and range. Attempted to contact authors regarding means and standard
deviations. Letter returned to sender.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk “eligible fertile and subfertile men were
randomly assigned according to a simple
computer-generated randomisation sched-
ule in four blocks to receive folic acid
and placebo, zinc sulphate and placebo,
zinc sulphate and folic acid, or placebo
and placebo, which resulted in eight sub-
groups.” “At the end of the trial, the re-
search fellow received the randomisation
list that matched the codes from the hospi-
tal pharmacy.”
83Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Wong 2002 (Continued)
Allocation concealment (selection bias) Unclear risk “capsules were coded by the hospital phar-
macy according to the randomisation list.”
Blinding (performance bias and detection
bias)
All outcomes
Low risk Double blind
“Neither the research fellow and the par-
ticipants knew whether the participants re-
ceived folic acid, zinc sulphate or placebo
capsules”
“Folic acid and placebo capsules were yel-
low and identical in appearance. Zinc sul-
phate and placebo capsules were white and
identical in appearance”
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk 9 men withdrew from the subfertile arm of
the trial, 1 due to side effects (gastrointesti-
nal) and 8 due to lack of motivation. It is
unclear which treatment groups these men
were randomised to
Selective reporting (reporting bias) Low risk All outcomes except for semen volume is
given as medians
The protocol is given in methods section -
main outcomes are semen parameters and
these are presented in the report - “ Our
main goal was to investigate the effects of
the interventions on semen variables in fer-
tile and subfertile men.”
Other bias Unclear risk Can not definitively assess other bias
Zalata 1998
Methods A randomised pilot study
Allocation concealment not mentioned
Participants Country: Belgium
Population: Men attending andrology clinic
Mean age: Not given
N=22
Inclusion criteria: None given
Exclusion criteria: None given
Duration of study: ?4-6 months
Interventions Acetylcysteine 600mg/day (n=5)
versus
EFA (DHA 1g, y-linolenic acid, arachidonic acid 100mg) 100mg/day + antioxidant oil
mixture and tocopherol + B-carotene (n=12)
versus
84Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Zalata 1998 (Continued)
Acetylcysteine + EFA + antioxidants (n=5)
Duration of treatment: 4-6 months
Outcomes Sperm parameters
Notes Abstract only. No extractable data. Attempted to contact authors re availability of data
as means, if published?, methods of randomisation and allocation concealment.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “A prospective randomised pilot study”
No details of randomisation given
Allocation concealment (selection bias) Unclear risk No details of allocation concealment
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk No details
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk No details
Selective reporting (reporting bias) Unclear risk Unclear, abstract only
Other bias Unclear risk Unclear
Zavaczki 2003
Methods Randomised placebo controlled clinical study
Allocation concealment not mentioned
Participants Country: Hungary
Population: Subfertile men attending andrology Department of Obstetrics and Gynae-
cology, University of Szeged
Mean age: Treatment group 29.6, placebo group 28.3 years
Recruited: N =26
Randomised: N=20
Inclusion criteria: Unsuccessful attempt at pregnancy for over one year. A healthy female
partner examined by a gynaecologist. Sperm volume < 2ml and/or sperm concentration
<20mill/ml and/or morphology ratio <30% and/or motility <50%. No genital tract
infection, no bacteria or fungi in urine or semen. Hormones are within physiological
range. Intact renal function. No excessive magnesium intake
Exclusion criteria: None mentioned
Duration of study: 3 months
85Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Zavaczki 2003 (Continued)
Interventions Magnesium 3000mg/day (n=10)
versus
placebo (n=10)
Number analysed: N=14
Duration of treatment: 90 days
Outcomes Primary: Semen parameters
Secondary: pregnancy and side effects
Notes Attempted to contact authors regarding methods of randomisation and allocation con-
cealment
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “Patients were randomised and divided
into Magnesium or Placebo groups”
Methods of randomisation are not men-
tioned
Allocation concealment (selection bias) Unclear risk Not mentioned
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk “The members of Group P received the
same number of placebo tablets which
closely resembled the Magnerot tablets.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk 20 were randomised and 14 were analysed.
“To date 26 patients have participated in
the study and 20 men (10 in both groups)
have completed the program of treatment.
Six patients (2 in group M and 4 in group P
were excluded from the program, including
five cases for poor compliance, since they
did not attend the control meeting at the
end of treatment. One patient from Group
M experienced severe diarrhoea and so his
treatment was halted.”
Selective reporting (reporting bias) Unclear risk All data for outcomes in the trial were given,
unsure if these were prespecified
Other bias Unclear risk Funding - OKTA program. Tablets sup-
plied by pharmaceutical company
86Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Cavallini 2004a Superceded by full paper of the trial - Cavallini 2004. Continuous data were used in Cavallini 2004 analysis.
Comhaire 2005 Used non randomised controls recruited from another unrelated trial.
Ebisch 2003 Inappropriate outcomes. Polymorphisms.
Ebisch 2006 This study is part of included study Wong 2002.
Elgindy 2008 Antioxidant given to the women and not to the men.
Micic 2001 Not randomised. 105 men in the treatment group and 35 in control. Abstract only.
Nikolova 2007 Trial is not randomised, allocation method is by alternation. Translated from Bulgarian by Ivan Sola. “50 of them
were randomly invited to participate depending on their order of attendance to the clinic”.
Pawlowicz 2001 Not a randomised controlled trial.
Pryor 2003 Conference proceeding superceded by Sigman 2006.
Rolf 1998 Conference proceeding superceded by Rolfe 1999.
Stanislavov 2009 Trial design is not random. The trial uses alternate allocation, odd and even numbers. Appears to be a report of
the trial Nikolova 2007.
Tremellen 2006 Conference proceeding superceded by Tremellen 2007.
Vicari 2001 Inapproriate control (anti-inflammatory). Treatment is not compared to placebo or another antioxidant.
Vicari 2001a Inappropriate comparison. The same antioxidant is compared at different times - L-carnitine +acetyl-carnitine
versus L-carnitine +acetyl-carnitine.
Zalata 1998a Same study as included trial Zalata 1998.
Characteristics of studies awaiting assessment [ordered by study ID]
Dimitriadis 2010
Methods Randomised controlled trial
Participants 75 “infertile men with oligioasthenospermia”
Interventions Vardenafil (10mg/day)- Group A, sildenafil (50mg/day)- Group B, L-carnitine (1000mg/day)- Group C, no treat-
ment- Group D
87Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Dimitriadis 2010 (Continued)
Outcomes sperm motility, sperm concentration
Notes
Wang 2010
Methods Random controlled trial
Participants 135 men with asthenozoospermia
Interventions L-carnitine + vitamin E vs vitamin E
Outcomes Pregnancy, adverse events, motile sperm.
Notes In Chinese - paper will need translation
Characteristics of ongoing studies [ordered by study ID]
Gonzalez 2009
Trial name or title Assessment of the efficacy of dietary supplement Spermotrend in the treatment of male infertility
Methods Randomised, double blind (subject, caregiver, investigator), placebo control, parallel assignment, efficacy
study
Participants Subfertile men
Interventions Spermotrend (vitamins plus other antioxidants) versus placebo
Outcomes Parameters of seminal analysis at weeks 24
Fertilisation achievement
Presence of mild or severe adverse effects
Starting date September 2009
Contact information Rogelio Gonzalez Sanchez, MD
53 7 838 2626 ext 277
Gynecologic and Obstetric Hospital
Havana, Cuba, 10400
Notes Havana, Cuba, 10400
88Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kumar 2010
Trial name or title Kumar R. Evaluation of oxidative stress as a cause for idiopathic male infertility and the role of Addyzoa in
its treatment
Methods Randomised, parallel group, placebo controlled trial. Method of generating randomisation sequence: Random
number table method of allocation concealment: Pre-numbered or coded identical containers. Blinding and
masking: participant, investigator,outcome assessor and data-entry operator/statistician blinded.
Participants Inclusion criteria: Infertile male, normal semen volume with either oligospermia (sperm density between 5
and 20 million/mL) or asthenospermia or teratospermia by WHO criteria
Exclusion criteria: Identifiable cause for semen abnormality (varicocele, cryptorchidism, orchitis, radiation,
chemotherapy, recent febrile illness, hormonal abnormality etc)
Interventions Intervention1: Addyzoa capsules: 2 BD for 3 months
Control Intervention1: placebo: 2 BD for 3 months
Outcomes Improvement in semen parameters timepoint: 3 months and 6 months
Pregnancy timepoint: Upto 12 months
Starting date 15-03-2009
Contact information Name: Dr Rajeev Kumar
Address: Department of Urology,AIIMS, Ansari Nagar 110029, New Delhi, India
Telephone: 01126594884
Email: [email protected]
Notes Main ID:CTRI/2009/091/000551. In WHO International Clinical trials Registry Platform.
Revel 2006
Trial name or title Revel A. A preliminary study on effect of omega-3 on human sperm. ClinicalTrials.gov. [ClinicalTrials.gov:
NCT00479960]
Methods Double blind randomised crossover trial
Participants Men with oligospermia, asthenoospermia or teratozoospermia
Interventions Omega 3 fatty acids
Outcomes Sperm count, sperm lipid transition determination
Starting date Enrollment due to be June 2007
Contact information Ariel Revel: [email protected]
Abraham Benchetrit: [email protected]
Notes Email sent to Drs Revel and Benchetrit 17.09.09 asking whether they have any data ready for their trial
89Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Sadeghi 2008
Trial name or title Sadeghi M. Effects of coenzymeQ10 (CoQ10) supplementation on semen quality and seminal oxidative stress
of idiopathic oligoasthenoteratozoospermic (iOAT) infertile men. World Health Organization International
Clinical Trials Registry Platform Search Portal 2008. [ISRCTN: ISRCTN29954277]
Methods Randomised double blind placebo controlled trial
Participants Men with idiopathic oligoasthenoteratozoospermia with at least one year infertility
Interventions Coenzyme10 (Ubiquinone) 200mg 2x/day for 3 months
Outcomes Sperm morphology, motility and sperm DNA fragmentation
Starting date 1.10.08
Contact information [email protected]
Notes letter sent to author regarding data 17.09.09
Tsafrir 2010
Trial name or title Is a carnitine based food supplement (PorimoreTM) for infertile men superior to folate and zinc with regard
to pregnancy rates in intrauterine insemination cycles?
Methods Randomised, open label, active control, parallel assignment, efficacy study
Participants Infertile men aged 18-50 years
Interventions Carnitine supplement versus zinc and folate supplement
Outcomes Pregnancy rate and sperm quality parameters
Starting date February 2010 - expected completion December 2012
Contact information Avi Tsafrir, MD
tel: 972-6555111
Shaare-Zedek IVF and Infertility Unit
Jerusalem
91031
Notes
90Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. Antioxidant(s) versus control
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Live Birth per couple randomised 3 214 Peto Odds Ratio (Peto, Fixed, 95% CI) 4.85 [1.92, 12.24]
1.1 Vitamin E versus placebo 2 117 Peto Odds Ratio (Peto, Fixed, 95% CI) 6.44 [1.72, 24.04]
1.2 Zinc versus no treatment 1 97 Peto Odds Ratio (Peto, Fixed, 95% CI) 3.67 [1.00, 13.51]
2 Pregnancy rate per couple
randomised
15 964 Peto Odds Ratio (Peto, Fixed, 95% CI) 4.18 [2.65, 6.59]
2.1 Combined antioxidants
versus placebo/no treatment
2 100 Peto Odds Ratio (Peto, Fixed, 95% CI) 3.97 [1.39, 11.33]
2.2 L acetyl carnitine versus
placebo
1 20 Peto Odds Ratio (Peto, Fixed, 95% CI) 0.61 [0.04, 9.64]
2.3 L carnitine versus placebo 3 136 Peto Odds Ratio (Peto, Fixed, 95% CI) 5.08 [1.51, 17.09]
2.4 L acetyl carnitine + L
carnitine versus placebo
4 183 Peto Odds Ratio (Peto, Fixed, 95% CI) 4.48 [1.77, 11.36]
2.5 Coenzyme Q10 versus
placebo
2 272 Peto Odds Ratio (Peto, Fixed, 95% CI) 2.16 [0.53, 8.82]
2.6 Pentoxifylline versus
placebo
1 18 Peto Odds Ratio (Peto, Fixed, 95% CI) 0.0 [0.0, 0.0]
2.7 Magnesium versus placebo 1 20 Peto Odds Ratio (Peto, Fixed, 95% CI) 7.39 [0.15, 372.38]
2.8 Vitamin E versus placebo 1 87 Peto Odds Ratio (Peto, Fixed, 95% CI) 6.64 [1.84, 23.93]
2.9 Vitamin C plus Vitamin E
versus placebo
1 31 Peto Odds Ratio (Peto, Fixed, 95% CI) 0.0 [0.0, 0.0]
2.10 Zinc versus no treatment 1 97 Peto Odds Ratio (Peto, Fixed, 95% CI) 4.75 [1.49, 15.20]
3 Adverse event: Miscarriage rate
per couple randomised
3 242 Peto Odds Ratio (Peto, Fixed, 95% CI) 1.54 [0.32, 7.30]
3.1 Combined antioxidants
versus placebo
1 58 Peto Odds Ratio (Peto, Fixed, 95% CI) 0.48 [0.06, 4.03]
3.2 Vitamin E versus placebo 1 87 Peto Odds Ratio (Peto, Fixed, 95% CI) 5.43 [0.32, 93.28]
3.3 Zinc versus no treatment 1 97 Peto Odds Ratio (Peto, Fixed, 95% CI) 7.24 [0.14, 364.94]
4 DNA fragmentation 1 Mean Difference (IV, Fixed, 95% CI) Subtotals only
4.1 Vitamin C + vitamin E
versus placebo at 2 months
1 64 Mean Difference (IV, Fixed, 95% CI) -13.80 [-17.50, -
10.10]
5 Sperm total motility at 3 months
or less
10 Mean Difference (IV, Random, 95% CI) Subtotals only
5.1 Docosahexaenoic acid
(DHA) 400g/day versus
placebo
1 14 Mean Difference (IV, Random, 95% CI) -7.80 [-30.56,
14.96]
5.2 Docosahexaenoic acid
(DHA) 800mg/day vs placebo
1 15 Mean Difference (IV, Random, 95% CI) -15.20 [-34.31,
3.91]
5.3 Ascorbic acid (Vitamin C)
200mg/day versus placebo
1 15 Mean Difference (IV, Random, 95% CI) 2.0 [-24.07, 28.07]
5.4 Ascorbic acid (Vitamin
C)1000mg/day versus placebo
1 15 Mean Difference (IV, Random, 95% CI) 45.0 [15.25, 74.75]
91Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

5.5 Ascorbic acid (vitamin C)
+ Vitamin E versus placebo at 2
months
1 64 Mean Difference (IV, Random, 95% CI) 2.90 [-7.76, 13.56]
5.6 L-carnitine +l-acetyl
carnitine versus placebo at 3
months
1 21 Mean Difference (IV, Random, 95% CI) -9.0 [-39.49, 21.49]
5.7 Selenium versus placebo
at 3 months
1 25 Mean Difference (IV, Random, 95% CI) 14.90 [-1.04, 30.84]
5.8 Combined antioxidants
versus placebo at 3 months
1 39 Mean Difference (IV, Random, 95% CI) 11.7 [-1.79, 25.19]
5.9 N-acetylcysteine versus
placebo at 3 months
1 120 Mean Difference (IV, Random, 95% CI) 10.96 [7.91, 14.01]
5.10 Magnesium versus
placebo at 90 days
1 20 Mean Difference (IV, Random, 95% CI) 14.5 [-6.01, 35.01]
5.11 L-carnitine versus
placebo
1 30 Mean Difference (IV, Random, 95% CI) 31.30 [31.21, 31.39]
5.12 Pentoxifyllin versus no
treatment at 3 months
1 90 Mean Difference (IV, Random, 95% CI) 12.77 [9.23, 16.31]
5.13 Zinc versus no treatment
at 3 months
1 14 Mean Difference (IV, Random, 95% CI) 25.0 [9.68, 40.32]
5.14 Zinc + Vitamin E versus
no treatment at 3 months
1 15 Mean Difference (IV, Random, 95% CI) 26.0 [9.03, 42.97]
5.15 Zinc + Vitamin E +
Vitamin C versus no treatment
at 3 months
1 17 Mean Difference (IV, Random, 95% CI) 26.0 [8.85, 43.15]
6 Sperm total motility at 6 months 7 Mean Difference (IV, Random, 95% CI) Subtotals only
6.1 L-carnitine versus placebo
at 6 months
1 20 Mean Difference (IV, Random, 95% CI) 21.13 [11.50, 30.76]
6.2 L-acetyl carnitine versus
placebo at 6 months
1 20 Mean Difference (IV, Random, 95% CI) 17.03 [6.90, 27.16]
6.3 L-carnitine + L-acetyl
carnitine versus placebo at 6
months
3 97 Mean Difference (IV, Random, 95% CI) 6.12 [-7.37, 19.60]
6.4 Selenium versus placebo
at 26 weeks (6 months)
1 155 Mean Difference (IV, Random, 95% CI) 3.20 [2.33, 4.07]
6.5 N-acetyl-cysteine versus
placebo at 26 weeks (6months)
1 157 Mean Difference (IV, Random, 95% CI) 1.90 [1.03, 2.77]
6.6 Selenium plus
N-acetyl-cysteine versus
placebo at 26 weeks (6months)
1 155 Mean Difference (IV, Random, 95% CI) 6.3 [5.43, 7.17]
6.7 Coenzyme Q10 versus
placebo at 6 months.
Safarinejad trial =26 weeks
2 272 Mean Difference (IV, Random, 95% CI) 4.50 [3.93, 5.07]
6.8 Vitamin E versus placebo
at 6 months
1 87 Mean Difference (IV, Random, 95% CI) 13.0 [7.02, 18.98]
7 Sperm total motility at 9 months
or more
3 Mean Difference (IV, Random, 95% CI) Subtotals only
7.1 L-carnitine versus placebo
at 9 months
1 20 Mean Difference (IV, Random, 95% CI) 11.54 [1.66, 21.42]
7.2 L-acetyl carnitine versus
placebo at 9 months
1 20 Mean Difference (IV, Random, 95% CI) 7.84 [-1.41, 17.09]
92Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7.3 L-carnitine + L-acetyl
carnitine versus placebo at 9
months
1 20 Mean Difference (IV, Random, 95% CI) 6.27 [-3.36, 15.90]
7.4 Coenzyme Q10 versus
placebo at 9 months
2 272 Mean Difference (IV, Random, 95% CI) -0.04 [-3.62, 3.55]
8 Sperm concentration at 3
months or less
7 320 Mean Difference (IV, Random, 95% CI) 6.04 [-5.42, 17.50]
8.1 Docosahexaenoic acid
(DHA) 400g/day versus
placebo
1 18 Mean Difference (IV, Random, 95% CI) -5.30 [-41.09,
30.49]
8.2 Docosahexaenoic acid
(DHA) 800g/day versus
placebo
1 19 Mean Difference (IV, Random, 95% CI) 1.50 [-35.23, 38.23]
8.3 Magnesium versus placebo
at 90 days
1 20 Mean Difference (IV, Random, 95% CI) 5.20 [-2.61, 13.01]
8.4 Vitamin C + Vitamin E
versus placebo at 2 months
2 95 Mean Difference (IV, Random, 95% CI) 1.36 [-10.01, 12.72]
8.5 N-acetylcysteine versus
placebo at 3 months
1 120 Mean Difference (IV, Random, 95% CI) -0.47 [-6.70, 5.76]
8.6 Pentoxifylline versus
placebo at 3 months
1 18 Mean Difference (IV, Random, 95% CI) 4.30 [-0.69, 9.29]
8.7 L-carnitine versus placebo 1 30 Mean Difference (IV, Random, 95% CI) 29.5 [25.39, 33.61]
9 Sperm concentration at 6
months
6 Mean Difference (IV, Random, 95% CI) Subtotals only
9.1 L-carnitine versus placebo
at 6 months
1 20 Mean Difference (IV, Random, 95% CI) 11.80 [-4.81, 28.41]
9.2 L-acetyl carnitine versus
placebo at 6 months
1 20 Mean Difference (IV, Random, 95% CI) 5.84 [-10.31, 21.99]
9.3 L-carnitine + L-acetyl
carnitine versus placebo at 6
months
2 76 Mean Difference (IV, Random, 95% CI) 0.63 [-5.93, 7.18]
9.4 Selenium versus placebo
at 26 weeks (6 months)
1 155 Mean Difference (IV, Random, 95% CI) 4.10 [1.94, 6.26]
9.5 N-acetyl-cysteine versus
placebo at 26 weeks (6months)
1 157 Mean Difference (IV, Random, 95% CI) 3.30 [1.24, 5.36]
9.6 Selenium plus
N-acetyl-cysteine versus
placebo at 26 weeks (6months)
1 155 Mean Difference (IV, Random, 95% CI) 8.60 [6.40, 10.80]
9.7 Coenzyme Q10 versus
placebo at 6 months
2 272 Mean Difference (IV, Random, 95% CI) 3.86 [-2.09, 9.81]
9.8 Pentoxifylline versus
placebo up to 6 months
1 18 Mean Difference (IV, Random, 95% CI) 2.80 [-2.58, 8.18]
10 Sperm concentration at 9
months or more
3 332 Mean Difference (IV, Fixed, 95% CI) 1.61 [0.61, 2.61]
10.1 L-carnitine versus
placebo at 9 months
1 20 Mean Difference (IV, Fixed, 95% CI) 9.27 [-1.51, 20.05]
10.2 L-acetyl carnitine versus
placebo at 9 months
1 20 Mean Difference (IV, Fixed, 95% CI) 1.08 [-8.16, 10.32]
10.3 L-carnitine + L-acetyl
carnitine versus placebo at 9
months
1 20 Mean Difference (IV, Fixed, 95% CI) 3.14 [-7.54, 13.82]
93Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

10.4 Coenzyme Q10 versus
placebo at 9 months or more
2 272 Mean Difference (IV, Fixed, 95% CI) 1.53 [0.51, 2.55]
11 Total sperm motility over time 16 Mean Difference (IV, Random, 95% CI) Subtotals only
11.1 Total sperm motility at 3
months or less
10 454 Mean Difference (IV, Random, 95% CI) 13.47 [3.45, 23.49]
11.2 Total sperm motility at 6
months
7 700 Mean Difference (IV, Random, 95% CI) 6.28 [4.36, 8.21]
11.3 Total sperm motility at 9
months or more
3 302 Mean Difference (IV, Random, 95% CI) 1.07 [-2.29, 4.43]
12 Sperm concentration over time 12 Mean Difference (IV, Random, 95% CI) Subtotals only
12.1 Sperm concentration at
3 months or less
7 302 Mean Difference (IV, Random, 95% CI) 6.79 [-5.09, 18.66]
12.2 Sperm concentration 6
months
6 610 Mean Difference (IV, Random, 95% CI) 5.12 [2.53, 7.72]
12.3 Sperm concentration at
9 months or more
3 302 Mean Difference (IV, Random, 95% CI) 1.56 [0.55, 2.57]
13 Side effects 6 Peto Odds Ratio (Peto, Fixed, 95% CI) Subtotals only
13.1 gastrointestinal 6 426 Peto Odds Ratio (Peto, Fixed, 95% CI) 1.63 [0.48, 5.58]
13.2 euphoria 1 86 Peto Odds Ratio (Peto, Fixed, 95% CI) 1.21 [0.16, 9.01]
14 Sperm motility at 3 months or
less
Other data No numeric data
14.1 L-carnitine +
Acetyl-carnitine versus placebo
(median and interquartile
range)
Other data No numeric data
14.2 Combined antioxidants
versus no treatment
Other data No numeric data
14.3 Vitamin E versus placebo Other data No numeric data
14.4 L-carnitine versus
placebo
Other data No numeric data
14.5 Pentoxifylline versus
Placebo
Other data No numeric data
15 Sperm motility at 6 months Other data No numeric data
15.1 L-carnitine +
Acetyl-carnitine versus placebo
(median and interquartile
range)
Other data No numeric data
15.2 Pentoxifylline versus
placebo
Other data No numeric data
15.3 Folic acid versus placebo Other data No numeric data
15.4 Zinc versus placebo Other data No numeric data
15.5 Zinc + folic acid versus
placebo
Other data No numeric data
16 Sperm concentration at 3
months or less
Other data No numeric data
16.1 L-carnitine +
Acetyl-carnitine versus placebo
(median and interquartile
range)
Other data No numeric data
16.2 Vitamin E versus placebo Other data No numeric data
94Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

16.3 L-carnitine versus
placebo
Other data No numeric data
17 Sperm concentration at 6
months
Other data No numeric data
17.1 L-carnitine +
acetyl-carnitine versus placebo
Other data No numeric data
17.2 Folic acid versus Placebo Other data No numeric data
17.3 Zinc versus Placebo Other data No numeric data
18 Pregnancy 15 963 Peto Odds Ratio (Peto, Fixed, 95% CI) 4.40 [2.78, 6.97]
18.1 Pregnancy rate of trials
that also report live birth
2 184 Peto Odds Ratio (Peto, Fixed, 95% CI) 5.53 [2.34, 13.08]
18.2 Pregnancy rate only
reported
13 779 Peto Odds Ratio (Peto, Fixed, 95% CI) 4.02 [2.34, 6.92]
Comparison 2. Live birth versus pregnancy
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Live birth 2 Peto Odds Ratio (Peto, Fixed, 95% CI) Subtotals only
1.1 live birth 2 184 Peto Odds Ratio (Peto, Fixed, 95% CI) 4.73 [1.82, 12.27]
1.2 pregnancy 2 184 Peto Odds Ratio (Peto, Fixed, 95% CI) 5.53 [2.34, 13.08]
Comparison 3. Head to head antioxidant(s)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pregnancy per couple
randomised
2 Peto Odds Ratio (Peto, Fixed, 95% CI) Subtotals only
1.1 L acetyl carnitine +
L carnitine versus L acetyl
carnitine
1 22 Peto Odds Ratio (Peto, Fixed, 95% CI) 2.66 [0.27, 25.80]
1.2 L acetyl carnitine + L
carnitine versus L- carnitine
1 23 Peto Odds Ratio (Peto, Fixed, 95% CI) 3.89 [0.51, 29.76]
1.3 L acetyl carnitine + L
carnitine versus Vitamin E +
Vitamin C
1 150 Peto Odds Ratio (Peto, Fixed, 95% CI) 2.86 [0.86, 9.49]
2 Sperm total motility at 3 months
or less
7 Mean Difference (IV, Fixed, 95% CI) Subtotals only
2.1 Ethylcysteine 600mg/day
vs Vitamin E
1 10 Mean Difference (IV, Fixed, 95% CI) -1.90 [-41.97,
38.17]
2.2 Docosahexaenoic
acid (DHA) 400g/day
vs Docosahexaenoic acid
800mg/day
1 19 Mean Difference (IV, Fixed, 95% CI) 7.40 [-11.35, 26.15]
95Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2.3 Ascorbic Acid 200mg/day
versus Ascorbic Acid
1000mg/day
1 20 Mean Difference (IV, Fixed, 95% CI) -43.0 [-67.10, -
18.90]
2.4 Vitamin E + Selenium
versus Vitamin B at 3 months
1 54 Mean Difference (IV, Fixed, 95% CI) 0.0 [-10.71, 10.71]
2.5 Zinc versus Zinc +
Vitamin E at 3 months
1 18 Mean Difference (IV, Fixed, 95% CI) -1.0 [-13.00, 13.00]
2.6 Zinc versus Zinc +
Vitamin E + Vitamin C at 3
months
1 12 Mean Difference (IV, Fixed, 95% CI) -1.0 [-19.66, 17.66]
2.7 Zinc + Vitamin E versus
Zinc + Vitamin E + Vitamin C
at 3 months
1 18 Mean Difference (IV, Fixed, 95% CI) 0.0 [-18.97, 18.97]
2.8 Selenium versus combined
antioxidants
1 46 Mean Difference (IV, Fixed, 95% CI) 3.20 [-10.13, 16.53]
2.9 L acetyl carnitine + L
carnitine versus Vitamin E +
Vitamin C
1 150 Mean Difference (IV, Fixed, 95% CI) 23.05 [20.23, 25.87]
3 Sperm total motility at 6 months 2 Mean Difference (IV, Fixed, 95% CI) Subtotals only
3.1 L-aceytl carnitine
+L-carnitine versus L-carnitine
at 6 months
1 22 Mean Difference (IV, Fixed, 95% CI) -3.46 [-11.41, 4.49]
3.2 L-acetyl carnitine +
L-carnitine versus L-acetyl
carnitine at 6 months
1 23 Mean Difference (IV, Fixed, 95% CI) 0.64 [-7.58, 8.86]
3.3 Selenium versus
N-acetyl-cysteine at 26 weeks
(6 months)
1 176 Mean Difference (IV, Fixed, 95% CI) 1.30 [0.39, 2.21]
3.4 Selenium versus selenium
plus N-acetyl-cysteine at 26
weeks (6 months)
1 116 Mean Difference (IV, Fixed, 95% CI) -3.10 [-4.16, -2.04]
3.5 N-acetyl-cysteine vs
selenium plus N-acetyl-cysteine
at 26 weeks
1 176 Mean Difference (IV, Fixed, 95% CI) -4.40 [-5.31, -3.49]
4 Sperm total motility at 9 months
or more
1 Mean Difference (IV, Fixed, 95% CI) Subtotals only
4.1 L-aceytl carnitine
+L-carnitine versus L-carnitine
at 9 months
1 22 Mean Difference (IV, Fixed, 95% CI) -5.27 [-12.61, 2.07]
4.2 L-acetyl carnitine +
L-carnitine versus L-acetyl
carnitine at 9 months
1 23 Mean Difference (IV, Fixed, 95% CI) -1.57 [-7.70, 4.56]
5 Sperm concentration at 3
months or less
3 Mean Difference (IV, Fixed, 95% CI) Subtotals only
5.1 Ethylcysteine 600mg/day
vs Vitamin E
1 10 Mean Difference (IV, Fixed, 95% CI) 2.20 [-16.65, 21.05]
5.2 Docosahexaenoic acid
(DHA) 400g/day versus
Docosahexaenoic acid (DHA)
800g/day
1 19 Mean Difference (IV, Fixed, 95% CI) -6.80 [-41.87,
28.27]
96Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

5.3 L-carnitine versus Vitamin
E + Vitamin C
1 63 Mean Difference (IV, Fixed, 95% CI) 15.5 [12.49, 18.51]
6 Sperm concentration at 6
months
2 Mean Difference (IV, Fixed, 95% CI) Subtotals only
6.1 L-aceytl carnitine
+L-carnitine versus L-carnitine
at 6 months
1 22 Mean Difference (IV, Fixed, 95% CI) -8.13 [-24.42, 8.16]
6.2 L-acetyl carnitine +
L-carnitine versus L-acetyl
carnitine at 6 months
1 23 Mean Difference (IV, Fixed, 95% CI) -2.17 [-17.40,
13.06]
6.3 Selenium versus
N-acetyl-cysteine at 26 weeks
(6 months)
1 176 Mean Difference (IV, Fixed, 95% CI) 0.80 [-1.10, 2.70]
6.4 Selenium versus selenium
plus N-acetyl-cysteine at 26
weeks (6 months)
1 116 Mean Difference (IV, Fixed, 95% CI) -4.5 [-6.90, -2.10]
6.5 N-acetyl-cysteine vs
selenium plus N-acetyl-cysteine
at 26 weeks
1 176 Mean Difference (IV, Fixed, 95% CI) -5.3 [-7.29, -3.31]
7 Sperm concentration at 9
months or more
1 Mean Difference (IV, Fixed, 95% CI) Subtotals only
7.1 L-aceytl carnitine
+L-carnitine versus L-carnitine
at 9 months
1 22 Mean Difference (IV, Fixed, 95% CI) -6.13 [-18.44, 6.18]
7.2 L-acetyl carnitine +
L-carnitine versus L-acetyl
carnitine at 9 months
1 23 Mean Difference (IV, Fixed, 95% CI) 2.06 [-8.33, 12.45]
8 Side effects 1 150 Odds Ratio (M-H, Fixed, 95% CI) 0.0 [0.0, 0.0]
8.1 L acetyl carnitine + L
carnitine versus Vitamin E +
Vitamin C
1 150 Odds Ratio (M-H, Fixed, 95% CI) 0.0 [0.0, 0.0]
9 Sperm concentration at 6
months
Other data No numeric data
9.1 Zinc versus Folic acid Other data No numeric data
9.2 Zinc versus Zinc + Folic
acid
Other data No numeric data
10 Sperm motility at 6 months Other data No numeric data
10.1 Zinc versus Folic acid Other data No numeric data
97Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.1. Comparison 1 Antioxidant(s) versus control, Outcome 1 Live Birth per couple randomised.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 1 Live Birth per couple randomised
Study or subgroup Experimental Control Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
1 Vitamin E versus placebo
Kessopoulou 1995 1/15 0/15 5.6 % 7.39 [ 0.15, 372.38 ]
Suleiman 1996 9/52 0/35 43.8 % 6.33 [ 1.56, 25.63 ]
Subtotal (95% CI) 67 50 49.4 % 6.44 [ 1.72, 24.04 ]
Total events: 10 (Experimental), 0 (Control)
Heterogeneity: Chi2 = 0.01, df = 1 (P = 0.94); I2 =0.0%
Test for overall effect: Z = 2.77 (P = 0.0056)
2 Zinc versus no treatment
Omu 1998 8/49 2/48 50.6 % 3.67 [ 1.00, 13.51 ]
Subtotal (95% CI) 49 48 50.6 % 3.67 [ 1.00, 13.51 ]
Total events: 8 (Experimental), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.96 (P = 0.050)
Total (95% CI) 116 98 100.0 % 4.85 [ 1.92, 12.24 ]
Total events: 18 (Experimental), 2 (Control)
Heterogeneity: Chi2 = 0.36, df = 2 (P = 0.84); I2 =0.0%
Test for overall effect: Z = 3.34 (P = 0.00084)
Test for subgroup differences: Chi2 = 0.35, df = 1 (P = 0.55), I2 =0.0%
0.001 0.01 0.1 1 10 100 1000
Favours control Favours antioxidant
98Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.2. Comparison 1 Antioxidant(s) versus control, Outcome 2 Pregnancy rate per couple
randomised.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 2 Pregnancy rate per couple randomised
Study or subgroup Experimental Control Peto Odds Ratio Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
1 Combined antioxidants versus placebo/no treatment
Galatioto 2008 1/20 0/22 8.17 [ 0.16, 413.39 ]
Tremellen 2007 20/38 4/20 3.75 [ 1.26, 11.16 ]
Subtotal (95% CI) 58 42 3.97 [ 1.39, 11.33 ]
Total events: 21 (Experimental), 4 (Control)
Heterogeneity: Chi2 = 0.14, df = 1 (P = 0.71); I2 =0.0%
Test for overall effect: Z = 2.57 (P = 0.010)
2 L acetyl carnitine versus placebo
Balercia 2005 2/15 1/5 0.61 [ 0.04, 9.64 ]
Subtotal (95% CI) 15 5 0.61 [ 0.04, 9.64 ]
Total events: 2 (Experimental), 1 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.35 (P = 0.72)
3 L carnitine versus placebo
Balercia 2005 2/15 1/5 0.61 [ 0.04, 9.64 ]
Lenzi 2003 6/43 0/43 8.37 [ 1.61, 43.58 ]
Peivandi 2010 3/15 0/15 8.57 [ 0.82, 89.45 ]
Subtotal (95% CI) 73 63 5.08 [ 1.51, 17.09 ]
Total events: 11 (Experimental), 1 (Control)
Heterogeneity: Chi2 = 2.81, df = 2 (P = 0.25); I2 =29%
Test for overall effect: Z = 2.63 (P = 0.0086)
4 L acetyl carnitine + L carnitine versus placebo
Balercia 2005 5/15 1/5 1.83 [ 0.21, 15.73 ]
Cavallini 2004 9/39 1/47 7.50 [ 2.01, 27.98 ]
Lenzi 2004 4/30 0/26 7.20 [ 0.95, 54.34 ]
Sigman 2006 1/12 1/9 0.74 [ 0.04, 13.02 ]
Subtotal (95% CI) 96 87 4.48 [ 1.77, 11.36 ]
Total events: 19 (Experimental), 3 (Control)
Heterogeneity: Chi2 = 2.99, df = 3 (P = 0.39); I2 =0.0%
Test for overall effect: Z = 3.17 (P = 0.0015)
5 Coenzyme Q10 versus placebo
0.002 0.1 1 10 500
Favours control Favours antioxidant
(Continued . . . )
99Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Peto Odds Ratio Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
Balercia 2009 6/30 3/30 2.16 [ 0.53, 8.82 ]
Safarinejad 2009a 0/106 0/106 0.0 [ 0.0, 0.0 ]
Subtotal (95% CI) 136 136 2.16 [ 0.53, 8.82 ]
Total events: 6 (Experimental), 3 (Control)
Heterogeneity: Chi2 = 0.0, df = 0 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 1.08 (P = 0.28)
6 Pentoxifylline versus placebo
Wang 1983 0/11 0/7 0.0 [ 0.0, 0.0 ]
Subtotal (95% CI) 11 7 0.0 [ 0.0, 0.0 ]
Total events: 0 (Experimental), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P < 0.00001)
7 Magnesium versus placebo
Zavaczki 2003 1/10 0/10 7.39 [ 0.15, 372.38 ]
Subtotal (95% CI) 10 10 7.39 [ 0.15, 372.38 ]
Total events: 1 (Experimental), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.00 (P = 0.32)
8 Vitamin E versus placebo
Suleiman 1996 11/52 0/35 6.64 [ 1.84, 23.93 ]
Subtotal (95% CI) 52 35 6.64 [ 1.84, 23.93 ]
Total events: 11 (Experimental), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 2.89 (P = 0.0038)
9 Vitamin C plus Vitamin E versus placebo
Rolf 1999 0/15 0/16 0.0 [ 0.0, 0.0 ]
Subtotal (95% CI) 15 16 0.0 [ 0.0, 0.0 ]
Total events: 0 (Experimental), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P < 0.00001)
10 Zinc versus no treatment
Omu 1998 11/49 2/48 4.75 [ 1.49, 15.20 ]
Subtotal (95% CI) 49 48 4.75 [ 1.49, 15.20 ]
Total events: 11 (Experimental), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 2.63 (P = 0.0086)
Total (95% CI) 515 449 4.18 [ 2.65, 6.59 ]
Total events: 82 (Experimental), 14 (Control)
Heterogeneity: Chi2 = 9.41, df = 13 (P = 0.74); I2 =0.0%
Test for overall effect: Z = 6.14 (P < 0.00001)
Test for subgroup differences: Chi2 = 3.47, df = 7 (P = 0.84), I2 =0.0%
0.002 0.1 1 10 500
Favours control Favours antioxidant
100Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.3. Comparison 1 Antioxidant(s) versus control, Outcome 3 Adverse event: Miscarriage rate per
couple randomised.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 3 Adverse event: Miscarriage rate per couple randomised
Study or subgroup Experimental Control Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
1 Combined antioxidants versus placebo
Tremellen 2007 2/38 2/20 54.1 % 0.48 [ 0.06, 4.03 ]
Subtotal (95% CI) 38 20 54.1 % 0.48 [ 0.06, 4.03 ]
Total events: 2 (Experimental), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.67 (P = 0.50)
2 Vitamin E versus placebo
Suleiman 1996 2/52 0/35 30.1 % 5.43 [ 0.32, 93.28 ]
Subtotal (95% CI) 52 35 30.1 % 5.43 [ 0.32, 93.28 ]
Total events: 2 (Experimental), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.17 (P = 0.24)
3 Zinc versus no treatment
Omu 1998 1/49 0/48 15.8 % 7.24 [ 0.14, 364.94 ]
Subtotal (95% CI) 49 48 15.8 % 7.24 [ 0.14, 364.94 ]
Total events: 1 (Experimental), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.99 (P = 0.32)
Total (95% CI) 139 103 100.0 % 1.54 [ 0.32, 7.30 ]
Total events: 5 (Experimental), 2 (Control)
Heterogeneity: Chi2 = 2.50, df = 2 (P = 0.29); I2 =20%
Test for overall effect: Z = 0.54 (P = 0.59)
Test for subgroup differences: Chi2 = 2.50, df = 2 (P = 0.29), I2 =20%
0.01 0.1 1 10 100
Favours antioxidant Favours control
101Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.4. Comparison 1 Antioxidant(s) versus control, Outcome 4 DNA fragmentation.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 4 DNA fragmentation
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Vitamin C + vitamin E versus placebo at 2 months
Greco 2005 32 9.1 (7.2) 32 22.9 (7.9) 100.0 % -13.80 [ -17.50, -10.10 ]
-50 -25 0 25 50
Favours antioxidant Favours control
Analysis 1.5. Comparison 1 Antioxidant(s) versus control, Outcome 5 Sperm total motility at 3 months or
less.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 5 Sperm total motility at 3 months or less
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
1 Docosahexaenoic acid (DHA) 400g/day versus placebo
Conquer 2000 9 39.4 (24.3) 5 47.2 (18.6) 100.0 % -7.80 [ -30.56, 14.96 ]
Subtotal (95% CI) 9 5 100.0 % -7.80 [ -30.56, 14.96 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.67 (P = 0.50)
2 Docosahexaenoic acid (DHA) 800mg/day vs placebo
Conquer 2000 10 32 (16.1) 5 47.2 (18.6) 100.0 % -15.20 [ -34.31, 3.91 ]
Subtotal (95% CI) 10 5 100.0 % -15.20 [ -34.31, 3.91 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.56 (P = 0.12)
3 Ascorbic acid (Vitamin C) 200mg/day versus placebo
Dawson 1990 10 51 (22.1) 5 49 (25.3) 100.0 % 2.00 [ -24.07, 28.07 ]
Subtotal (95% CI) 10 5 100.0 % 2.00 [ -24.07, 28.07 ]
Heterogeneity: not applicable
-50 -25 0 25 50
Favours control Favours antioxidant
(Continued . . . )
102Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Test for overall effect: Z = 0.15 (P = 0.88)
4 Ascorbic acid (Vitamin C)1000mg/day versus placebo
Dawson 1990 10 94 (32) 5 49 (25.3) 100.0 % 45.00 [ 15.25, 74.75 ]
Subtotal (95% CI) 10 5 100.0 % 45.00 [ 15.25, 74.75 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.96 (P = 0.0030)
5 Ascorbic acid (vitamin C) + Vitamin E versus placebo at 2 months
Greco 2005 32 41.6 (22) 32 38.7 (21.5) 100.0 % 2.90 [ -7.76, 13.56 ]
Subtotal (95% CI) 32 32 100.0 % 2.90 [ -7.76, 13.56 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.53 (P = 0.59)
6 L-carnitine +l-acetyl carnitine versus placebo at 3 months
Sigman 2006 12 28.6 (38.1) 9 37.6 (33) 100.0 % -9.00 [ -39.49, 21.49 ]
Subtotal (95% CI) 12 9 100.0 % -9.00 [ -39.49, 21.49 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.58 (P = 0.56)
7 Selenium versus placebo at 3 months
Scott 1998 16 30.2 (22.8) 9 15.3 (17.4) 100.0 % 14.90 [ -1.04, 30.84 ]
Subtotal (95% CI) 16 9 100.0 % 14.90 [ -1.04, 30.84 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.83 (P = 0.067)
8 Combined antioxidants versus placebo at 3 months
Scott 1998 30 27 (20.3) 9 15.3 (17.4) 100.0 % 11.70 [ -1.79, 25.19 ]
Subtotal (95% CI) 30 9 100.0 % 11.70 [ -1.79, 25.19 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.70 (P = 0.089)
9 N-acetylcysteine versus placebo at 3 months
Ciftci 2009 60 31.29 (8.62) 60 20.33 (8.43) 100.0 % 10.96 [ 7.91, 14.01 ]
Subtotal (95% CI) 60 60 100.0 % 10.96 [ 7.91, 14.01 ]
Heterogeneity: not applicable
Test for overall effect: Z = 7.04 (P < 0.00001)
10 Magnesium versus placebo at 90 days
Zavaczki 2003 10 33.5 (29.8) 10 19 (14.4) 100.0 % 14.50 [ -6.01, 35.01 ]
Subtotal (95% CI) 10 10 100.0 % 14.50 [ -6.01, 35.01 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.39 (P = 0.17)
11 L-carnitine versus placebo
Peivandi 2010 15 48.3 (0.16) 15 17 (0.09) 100.0 % 31.30 [ 31.21, 31.39 ]
Subtotal (95% CI) 15 15 100.0 % 31.30 [ 31.21, 31.39 ]
Heterogeneity: not applicable
-50 -25 0 25 50
Favours control Favours antioxidant
(Continued . . . )
103Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Test for overall effect: Z = 660.35 (P < 0.00001)
12 Pentoxifyllin versus no treatment at 3 months
Micic 1988 51 31.21 (10.66) 39 18.44 (6.35) 100.0 % 12.77 [ 9.23, 16.31 ]
Subtotal (95% CI) 51 39 100.0 % 12.77 [ 9.23, 16.31 ]
Heterogeneity: not applicable
Test for overall effect: Z = 7.07 (P < 0.00001)
13 Zinc versus no treatment at 3 months
Omu 2008 11 49 (12) 3 24 (12) 100.0 % 25.00 [ 9.68, 40.32 ]
Subtotal (95% CI) 11 3 100.0 % 25.00 [ 9.68, 40.32 ]
Heterogeneity: not applicable
Test for overall effect: Z = 3.20 (P = 0.0014)
14 Zinc + Vitamin E versus no treatment at 3 months
Omu 2008 12 50 (18) 3 24 (12) 100.0 % 26.00 [ 9.03, 42.97 ]
Subtotal (95% CI) 12 3 100.0 % 26.00 [ 9.03, 42.97 ]
Heterogeneity: not applicable
Test for overall effect: Z = 3.00 (P = 0.0027)
15 Zinc + Vitamin E + Vitamin C versus no treatment at 3 months
Omu 2008 14 50 (20) 3 24 (12) 100.0 % 26.00 [ 8.85, 43.15 ]
Subtotal (95% CI) 14 3 100.0 % 26.00 [ 8.85, 43.15 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.97 (P = 0.0030)
-50 -25 0 25 50
Favours control Favours antioxidant
104Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.6. Comparison 1 Antioxidant(s) versus control, Outcome 6 Sperm total motility at 6 months.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 6 Sperm total motility at 6 months
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
1 L-carnitine versus placebo at 6 months
Balercia 2005 15 64.53 (8.41) 5 43.4 (9.85) 100.0 % 21.13 [ 11.50, 30.76 ]
Subtotal (95% CI) 15 5 100.0 % 21.13 [ 11.50, 30.76 ]
Heterogeneity: not applicable
Test for overall effect: Z = 4.30 (P = 0.000017)
2 L-acetyl carnitine versus placebo at 6 months
Balercia 2005 15 60.43 (10.46) 5 43.4 (9.85) 100.0 % 17.03 [ 6.90, 27.16 ]
Subtotal (95% CI) 15 5 100.0 % 17.03 [ 6.90, 27.16 ]
Heterogeneity: not applicable
Test for overall effect: Z = 3.30 (P = 0.00098)
3 L-carnitine + L-acetyl carnitine versus placebo at 6 months
Balercia 2005 15 61.07 (9.07) 5 43.4 (9.85) 38.4 % 17.67 [ 7.89, 27.45 ]
Lenzi 2004 30 31.11 (13.46) 26 29.55 (9.5) 43.9 % 1.56 [ -4.48, 7.60 ]
Sigman 2006 12 32.3 (24.2) 9 40 (33) 17.7 % -7.70 [ -33.24, 17.84 ]
Subtotal (95% CI) 57 40 100.0 % 6.12 [ -7.37, 19.60 ]
Heterogeneity: Tau2 = 98.36; Chi2 = 8.61, df = 2 (P = 0.01); I2 =77%
Test for overall effect: Z = 0.89 (P = 0.37)
4 Selenium versus placebo at 26 weeks (6 months)
Safarinejad 2009 116 26.1 (2.9) 39 22.9 (2.2) 100.0 % 3.20 [ 2.33, 4.07 ]
Subtotal (95% CI) 116 39 100.0 % 3.20 [ 2.33, 4.07 ]
Heterogeneity: not applicable
Test for overall effect: Z = 7.22 (P < 0.00001)
5 N-acetyl-cysteine versus placebo at 26 weeks (6months)
Safarinejad 2009 118 24.8 (2.9) 39 22.9 (2.2) 100.0 % 1.90 [ 1.03, 2.77 ]
Subtotal (95% CI) 118 39 100.0 % 1.90 [ 1.03, 2.77 ]
Heterogeneity: not applicable
Test for overall effect: Z = 4.30 (P = 0.000017)
6 Selenium plus N-acetyl-cysteine versus placebo at 26 weeks (6months)
Safarinejad 2009 116 29.2 (2.9) 39 22.9 (2.2) 100.0 % 6.30 [ 5.43, 7.17 ]
Subtotal (95% CI) 116 39 100.0 % 6.30 [ 5.43, 7.17 ]
Heterogeneity: not applicable
Test for overall effect: Z = 14.21 (P < 0.00001)
7 Coenzyme Q10 versus placebo at 6 months. Safarinejad trial =26 weeks
-20 -10 0 10 20
Favours control Favours antioxidant
(Continued . . . )
105Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Balercia 2009 30 39.41 (6.8) 30 34.93 (8.04) 2.3 % 4.48 [ 0.71, 8.25 ]
Safarinejad 2009a 106 27.6 (2.2) 106 23.1 (2.1) 97.7 % 4.50 [ 3.92, 5.08 ]
Subtotal (95% CI) 136 136 100.0 % 4.50 [ 3.93, 5.07 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 0.00, df = 1 (P = 0.99); I2 =0.0%
Test for overall effect: Z = 15.41 (P < 0.00001)
8 Vitamin E versus placebo at 6 months
Suleiman 1996 52 48.9 (15.5) 35 35.9 (12.8) 100.0 % 13.00 [ 7.02, 18.98 ]
Subtotal (95% CI) 52 35 100.0 % 13.00 [ 7.02, 18.98 ]
Heterogeneity: not applicable
Test for overall effect: Z = 4.26 (P = 0.000020)
-20 -10 0 10 20
Favours control Favours antioxidant
Analysis 1.7. Comparison 1 Antioxidant(s) versus control, Outcome 7 Sperm total motility at 9 months or
more.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 7 Sperm total motility at 9 months or more
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
1 L-carnitine versus placebo at 9 months
Balercia 2005 15 54.27 (8.96) 5 42.73 (10.02) 100.0 % 11.54 [ 1.66, 21.42 ]
Subtotal (95% CI) 15 5 100.0 % 11.54 [ 1.66, 21.42 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.29 (P = 0.022)
2 L-acetyl carnitine versus placebo at 9 months
Balercia 2005 15 50.57 (5.71) 5 42.73 (10.02) 100.0 % 7.84 [ -1.41, 17.09 ]
Subtotal (95% CI) 15 5 100.0 % 7.84 [ -1.41, 17.09 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.66 (P = 0.097)
3 L-carnitine + L-acetyl carnitine versus placebo at 9 months
Balercia 2005 15 49 (7.8) 5 42.73 (10.02) 100.0 % 6.27 [ -3.36, 15.90 ]
-20 -10 0 10 20
Favours control Favours antioxidant
(Continued . . . )
106Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Subtotal (95% CI) 15 5 100.0 % 6.27 [ -3.36, 15.90 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.28 (P = 0.20)
4 Coenzyme Q10 versus placebo at 9 months
Balercia 2009 30 32.93 (6.33) 30 35.3 (8) 38.1 % -2.37 [ -6.02, 1.28 ]
Safarinejad 2009a 106 24.2 (2.1) 106 22.8 (2.2) 61.9 % 1.40 [ 0.82, 1.98 ]
Subtotal (95% CI) 136 136 100.0 % -0.04 [ -3.62, 3.55 ]
Heterogeneity: Tau2 = 5.33; Chi2 = 4.00, df = 1 (P = 0.05); I2 =75%
Test for overall effect: Z = 0.02 (P = 0.98)
-20 -10 0 10 20
Favours control Favours antioxidant
Analysis 1.8. Comparison 1 Antioxidant(s) versus control, Outcome 8 Sperm concentration at 3 months or
less.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 8 Sperm concentration at 3 months or less
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
1 Docosahexaenoic acid (DHA) 400g/day versus placebo
Conquer 2000 9 37.8 (36.9) 9 43.1 (40.5) 6.2 % -5.30 [ -41.09, 30.49 ]
Subtotal (95% CI) 9 9 6.2 % -5.30 [ -41.09, 30.49 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.29 (P = 0.77)
2 Docosahexaenoic acid (DHA) 800g/day versus placebo
Conquer 2000 10 44.6 (41.1) 9 43.1 (40.5) 6.0 % 1.50 [ -35.23, 38.23 ]
Subtotal (95% CI) 10 9 6.0 % 1.50 [ -35.23, 38.23 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.08 (P = 0.94)
3 Magnesium versus placebo at 90 days
Zavaczki 2003 10 16.1 (10.2) 10 10.9 (7.4) 14.7 % 5.20 [ -2.61, 13.01 ]
Subtotal (95% CI) 10 10 14.7 % 5.20 [ -2.61, 13.01 ]
-50 -25 0 25 50
Favours control Favours antioxidant
(Continued . . . )
107Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Heterogeneity: not applicable
Test for overall effect: Z = 1.30 (P = 0.19)
4 Vitamin C + Vitamin E versus placebo at 2 months
Greco 2005 32 27.5 (24.6) 32 20.3 (21.2) 13.7 % 7.20 [ -4.05, 18.45 ]
Rolf 1999 15 20.6 (13.5) 16 25 (17.8) 13.7 % -4.40 [ -15.48, 6.68 ]
Subtotal (95% CI) 47 48 27.4 % 1.36 [ -10.01, 12.72 ]
Heterogeneity: Tau2 = 34.83; Chi2 = 2.07, df = 1 (P = 0.15); I2 =52%
Test for overall effect: Z = 0.23 (P = 0.82)
5 N-acetylcysteine versus placebo at 3 months
Ciftci 2009 60 21.85 (11.08) 60 22.32 (22) 15.0 % -0.47 [ -6.70, 5.76 ]
Subtotal (95% CI) 60 60 15.0 % -0.47 [ -6.70, 5.76 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.15 (P = 0.88)
6 Pentoxifylline versus placebo at 3 months
Wang 1983 11 12.8 (4.7) 7 8.5 (5.6) 15.3 % 4.30 [ -0.69, 9.29 ]
Subtotal (95% CI) 11 7 15.3 % 4.30 [ -0.69, 9.29 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.69 (P = 0.091)
7 L-carnitine versus placebo
Peivandi 2010 15 46 (3.62) 15 16.5 (7.26) 15.4 % 29.50 [ 25.39, 33.61 ]
Subtotal (95% CI) 15 15 15.4 % 29.50 [ 25.39, 33.61 ]
Heterogeneity: not applicable
Test for overall effect: Z = 14.08 (P < 0.00001)
Total (95% CI) 162 158 100.0 % 6.04 [ -5.42, 17.50 ]
Heterogeneity: Tau2 = 217.11; Chi2 = 107.29, df = 7 (P<0.00001); I2 =93%
Test for overall effect: Z = 1.03 (P = 0.30)
Test for subgroup differences: Chi2 = 100.86, df = 6 (P = 0.0), I2 =94%
-50 -25 0 25 50
Favours control Favours antioxidant
108Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.9. Comparison 1 Antioxidant(s) versus control, Outcome 9 Sperm concentration at 6 months.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 9 Sperm concentration at 6 months
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
1 L-carnitine versus placebo at 6 months
Balercia 2005 15 45.53 (21.42) 5 33.73 (14.36) 100.0 % 11.80 [ -4.81, 28.41 ]
Subtotal (95% CI) 15 5 100.0 % 11.80 [ -4.81, 28.41 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.39 (P = 0.16)
2 L-acetyl carnitine versus placebo at 6 months
Balercia 2005 15 39.57 (19.99) 5 33.73 (14.36) 100.0 % 5.84 [ -10.31, 21.99 ]
Subtotal (95% CI) 15 5 100.0 % 5.84 [ -10.31, 21.99 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.71 (P = 0.48)
3 L-carnitine + L-acetyl carnitine versus placebo at 6 months
Balercia 2005 15 37.4 (16.42) 5 33.73 (14.36) 18.9 % 3.67 [ -11.41, 18.75 ]
Lenzi 2004 30 22.09 (9.05) 26 22.17 (16.95) 81.1 % -0.08 [ -7.36, 7.20 ]
Subtotal (95% CI) 45 31 100.0 % 0.63 [ -5.93, 7.18 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 0.19, df = 1 (P = 0.66); I2 =0.0%
Test for overall effect: Z = 0.19 (P = 0.85)
4 Selenium versus placebo at 26 weeks (6 months)
Safarinejad 2009 116 27.6 (6.4) 39 23.5 (5.8) 100.0 % 4.10 [ 1.94, 6.26 ]
Subtotal (95% CI) 116 39 100.0 % 4.10 [ 1.94, 6.26 ]
Heterogeneity: not applicable
Test for overall effect: Z = 3.72 (P = 0.00020)
5 N-acetyl-cysteine versus placebo at 26 weeks (6months)
Safarinejad 2009 118 26.8 (5.3) 39 23.5 (5.8) 100.0 % 3.30 [ 1.24, 5.36 ]
Subtotal (95% CI) 118 39 100.0 % 3.30 [ 1.24, 5.36 ]
Heterogeneity: not applicable
Test for overall effect: Z = 3.15 (P = 0.0017)
6 Selenium plus N-acetyl-cysteine versus placebo at 26 weeks (6months)
Safarinejad 2009 116 32.1 (6.8) 39 23.5 (5.8) 100.0 % 8.60 [ 6.40, 10.80 ]
Subtotal (95% CI) 116 39 100.0 % 8.60 [ 6.40, 10.80 ]
Heterogeneity: not applicable
Test for overall effect: Z = 7.66 (P < 0.00001)
7 Coenzyme Q10 versus placebo at 6 months
Balercia 2009 30 44.93 (19.3) 30 46.37 (19.77) 24.7 % -1.44 [ -11.33, 8.45 ]
-20 -10 0 10 20
Favours control Favours antioxidant
(Continued . . . )
109Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Safarinejad 2009a 106 26.4 (4.4) 106 20.8 (4.3) 75.3 % 5.60 [ 4.43, 6.77 ]
Subtotal (95% CI) 136 136 100.0 % 3.86 [ -2.09, 9.81 ]
Heterogeneity: Tau2 = 11.88; Chi2 = 1.92, df = 1 (P = 0.17); I2 =48%
Test for overall effect: Z = 1.27 (P = 0.20)
8 Pentoxifylline versus placebo up to 6 months
Wang 1983 11 11.1 (5.8) 7 8.3 (5.6) 100.0 % 2.80 [ -2.58, 8.18 ]
Subtotal (95% CI) 11 7 100.0 % 2.80 [ -2.58, 8.18 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.02 (P = 0.31)
-20 -10 0 10 20
Favours control Favours antioxidant
Analysis 1.10. Comparison 1 Antioxidant(s) versus control, Outcome 10 Sperm concentration at 9 months
or more.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 10 Sperm concentration at 9 months or more
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 L-carnitine versus placebo at 9 months
Balercia 2005 15 39.4 (13.93) 5 30.13 (9.3) 0.9 % 9.27 [ -1.51, 20.05 ]
Subtotal (95% CI) 15 5 0.9 % 9.27 [ -1.51, 20.05 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.69 (P = 0.092)
2 L-acetyl carnitine versus placebo at 9 months
Balercia 2005 15 31.21 (8.6) 5 30.13 (9.3) 1.2 % 1.08 [ -8.16, 10.32 ]
Subtotal (95% CI) 15 5 1.2 % 1.08 [ -8.16, 10.32 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.23 (P = 0.82)
3 L-carnitine + L-acetyl carnitine versus placebo at 9 months
Balercia 2005 15 33.27 (13.62) 5 30.13 (9.3) 0.9 % 3.14 [ -7.54, 13.82 ]
Subtotal (95% CI) 15 5 0.9 % 3.14 [ -7.54, 13.82 ]
-20 -10 0 10 20
Favours control Favours antioxidant
(Continued . . . )
110Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Heterogeneity: not applicable
Test for overall effect: Z = 0.58 (P = 0.56)
4 Coenzyme Q10 versus placebo at 9 months or more
Balercia 2009 30 44.18 (20.43) 30 49.56 (20.47) 0.9 % -5.38 [ -15.73, 4.97 ]
Safarinejad 2009a 106 22.8 (3.8) 106 21.2 (3.8) 96.1 % 1.60 [ 0.58, 2.62 ]
Subtotal (95% CI) 136 136 97.1 % 1.53 [ 0.51, 2.55 ]
Heterogeneity: Chi2 = 1.73, df = 1 (P = 0.19); I2 =42%
Test for overall effect: Z = 2.95 (P = 0.0032)
Total (95% CI) 181 151 100.0 % 1.61 [ 0.61, 2.61 ]
Heterogeneity: Chi2 = 3.79, df = 4 (P = 0.44); I2 =0.0%
Test for overall effect: Z = 3.14 (P = 0.0017)
Test for subgroup differences: Chi2 = 2.05, df = 3 (P = 0.56), I2 =0.0%
-20 -10 0 10 20
Favours control Favours antioxidant
Analysis 1.11. Comparison 1 Antioxidant(s) versus control, Outcome 11 Total sperm motility over time.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 11 Total sperm motility over time
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
1 Total sperm motility at 3 months or less
Ciftci 2009 60 31.29 (8.62) 60 20.33 (8.43) 12.4 % 10.96 [ 7.91, 14.01 ]
Conquer 2000 10 32 (16.1) 9 47.2 (18.6) 9.6 % -15.20 [ -30.92, 0.52 ]
Dawson 1990 10 94 (32) 10 49 (25.3) 7.0 % 45.00 [ 19.72, 70.28 ]
Greco 2005 32 41.6 (22) 32 38.7 (21.5) 11.0 % 2.90 [ -7.76, 13.56 ]
Micic 1988 51 31.21 (10.66) 39 18.44 (6.35) 12.3 % 12.77 [ 9.23, 16.31 ]
Omu 2008 14 50 (20) 8 24 (12) 10.2 % 26.00 [ 12.62, 39.38 ]
Peivandi 2010 15 48.3 (0.16) 15 17 (0.09) 12.5 % 31.30 [ 31.21, 31.39 ]
Scott 1998 30 27 (20.3) 18 15.3 (17.4) 10.9 % 11.70 [ 0.87, 22.53 ]
-50 -25 0 25 50
Favours control Favours antioxidant
(Continued . . . )
111Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Sigman 2006 12 28.6 (38.1) 9 37.6 (33) 5.8 % -9.00 [ -39.49, 21.49 ]
Zavaczki 2003 10 33.5 (29.8) 10 19 (14.4) 8.2 % 14.50 [ -6.01, 35.01 ]
Subtotal (95% CI) 244 210 100.0 % 13.47 [ 3.45, 23.49 ]
Heterogeneity: Tau2 = 208.58; Chi2 = 359.85, df = 9 (P<0.00001); I2 =97%
Test for overall effect: Z = 2.63 (P = 0.0084)
2 Total sperm motility at 6 months
Balercia 2005 15 61.07 (9.07) 15 43.4 (9.85) 6.5 % 17.67 [ 10.89, 24.45 ]
Balercia 2009 30 39.41 (6.8) 30 34.93 (8.04) 14.5 % 4.48 [ 0.71, 8.25 ]
Lenzi 2004 30 31.11 (13.46) 26 29.55 (9.5) 7.7 % 1.56 [ -4.48, 7.60 ]
Safarinejad 2009 116 29.2 (2.9) 118 22.9 (2.2) 31.4 % 6.30 [ 5.64, 6.96 ]
Safarinejad 2009a 106 27.6 (2.2) 106 23.1 (2.1) 31.6 % 4.50 [ 3.92, 5.08 ]
Sigman 2006 12 32.3 (24.2) 9 40 (33) 0.6 % -7.70 [ -33.24, 17.84 ]
Suleiman 1996 52 48.9 (15.5) 35 35.9 (12.8) 7.8 % 13.00 [ 7.02, 18.98 ]
Subtotal (95% CI) 361 339 100.0 % 6.28 [ 4.36, 8.21 ]
Heterogeneity: Tau2 = 2.95; Chi2 = 37.94, df = 6 (P<0.00001); I2 =84%
Test for overall effect: Z = 6.41 (P < 0.00001)
3 Total sperm motility at 9 months or more
Balercia 2005 15 49 (7.8) 15 42.73 (10.02) 17.8 % 6.27 [ -0.16, 12.70 ]
Balercia 2009 30 32.93 (6.33) 30 35.3 (8) 31.9 % -2.37 [ -6.02, 1.28 ]
Safarinejad 2009a 106 24.2 (2.1) 106 22.8 (2.2) 50.3 % 1.40 [ 0.82, 1.98 ]
Subtotal (95% CI) 151 151 100.0 % 1.07 [ -2.29, 4.43 ]
Heterogeneity: Tau2 = 5.75; Chi2 = 6.27, df = 2 (P = 0.04); I2 =68%
Test for overall effect: Z = 0.62 (P = 0.53)
-50 -25 0 25 50
Favours control Favours antioxidant
112Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.12. Comparison 1 Antioxidant(s) versus control, Outcome 12 Sperm concentration over time.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 12 Sperm concentration over time
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
1 Sperm concentration at 3 months or less
Ciftci 2009 60 21.85 (11.08) 60 22.32 (22) 16.0 % -0.47 [ -6.70, 5.76 ]
Conquer 2000 10 44.6 (41.1) 9 43.1 (40.5) 6.4 % 1.50 [ -35.23, 38.23 ]
Greco 2005 32 27.5 (24.6) 32 20.3 (21.2) 14.6 % 7.20 [ -4.05, 18.45 ]
Peivandi 2010 15 46 (3.62) 15 16.5 (7.26) 16.4 % 29.50 [ 25.39, 33.61 ]
Rolf 1999 15 20.6 (13.5) 16 25 (17.8) 14.6 % -4.40 [ -15.48, 6.68 ]
Wang 1983 11 12.8 (4.7) 7 8.5 (5.6) 16.3 % 4.30 [ -0.69, 9.29 ]
Zavaczki 2003 10 16.1 (10.2) 10 10.9 (7.4) 15.6 % 5.20 [ -2.61, 13.01 ]
Subtotal (95% CI) 153 149 100.0 % 6.79 [ -5.09, 18.66 ]
Heterogeneity: Tau2 = 218.93; Chi2 = 106.32, df = 6 (P<0.00001); I2 =94%
Test for overall effect: Z = 1.12 (P = 0.26)
2 Sperm concentration 6 months
Balercia 2005 15 37.4 (16.42) 15 33.73 (14.36) 4.8 % 3.67 [ -7.37, 14.71 ]
Balercia 2009 30 44.93 (19.3) 30 46.37 (19.77) 5.8 % -1.44 [ -11.33, 8.45 ]
Lenzi 2004 30 22.09 (9.05) 26 22.17 (16.95) 9.4 % -0.08 [ -7.36, 7.20 ]
Safarinejad 2009 116 32.1 (6.8) 118 23.5 (5.8) 31.9 % 8.60 [ 6.98, 10.22 ]
Safarinejad 2009a 106 26.4 (4.4) 106 20.8 (4.3) 33.9 % 5.60 [ 4.43, 6.77 ]
Wang 1983 11 11.1 (5.8) 7 8.3 (5.6) 14.2 % 2.80 [ -2.58, 8.18 ]
Subtotal (95% CI) 308 302 100.0 % 5.12 [ 2.53, 7.72 ]
Heterogeneity: Tau2 = 4.82; Chi2 = 16.26, df = 5 (P = 0.01); I2 =69%
Test for overall effect: Z = 3.87 (P = 0.00011)
3 Sperm concentration at 9 months or more
Balercia 2005 15 33.27 (13.62) 15 30.13 (9.3) 1.5 % 3.14 [ -5.21, 11.49 ]
Balercia 2009 30 44.18 (20.43) 30 49.56 (20.47) 1.0 % -5.38 [ -15.73, 4.97 ]
Safarinejad 2009a 106 22.8 (3.8) 106 21.2 (3.8) 97.6 % 1.60 [ 0.58, 2.62 ]
Subtotal (95% CI) 151 151 100.0 % 1.56 [ 0.55, 2.57 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 1.87, df = 2 (P = 0.39); I2 =0.0%
Test for overall effect: Z = 3.02 (P = 0.0025)
-20 -10 0 10 20
Favours control Favours antioxidant
113Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.13. Comparison 1 Antioxidant(s) versus control, Outcome 13 Side effects.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 13 Side effects
Study or subgroup Experimental Control Peto Odds Ratio Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
1 gastrointestinal
Cavallini 2004 2/39 2/47 1.21 [ 0.16, 9.01 ]
Kessopoulou 1995 0/15 1/15 0.14 [ 0.00, 6.82 ]
Safarinejad 2009a 0/106 0/106 0.0 [ 0.0, 0.0 ]
Sigman 2006 0/12 0/9 0.0 [ 0.0, 0.0 ]
Tremellen 2007 3/37 0/20 4.94 [ 0.44, 55.27 ]
Zavaczki 2003 2/10 1/10 2.11 [ 0.19, 23.05 ]
Subtotal (95% CI) 219 207 1.63 [ 0.48, 5.58 ]
Total events: 7 (Experimental), 4 (Control)
Heterogeneity: Chi2 = 2.49, df = 3 (P = 0.48); I2 =0.0%
Test for overall effect: Z = 0.78 (P = 0.44)
2 euphoria
Cavallini 2004 2/39 2/47 1.21 [ 0.16, 9.01 ]
Subtotal (95% CI) 39 47 1.21 [ 0.16, 9.01 ]
Total events: 2 (Experimental), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.19 (P = 0.85)
Test for subgroup differences: Chi2 = 0.06, df = 1 (P = 0.81), I2 =0.0%
0.002 0.1 1 10 500
Favours antioxidant Favours control
Analysis 1.14. Comparison 1 Antioxidant(s) versus control, Outcome 14 Sperm motility at 3 months or less.
Sperm motility at 3 months or less
Study Heading one Heading two
L-carnitine + Acetyl-carnitine versus placebo (median and interquartile range)
Cavallini 2004 L-carnitine + Acetyl-carnitine
Median=22.3 (n=39)
Interquartile range =28.4-15.2
Placebo
Median= 14.0 (n=47)
Interquartile range=17.4-5.1
Combined antioxidants versus no treatment
Galatioto 2008 Combined antioxidants
% of motile sperm =58% (n=20)
No treatment
% of motile sperm =51% (n=22)
114Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Sperm motility at 3 months or less (Continued)
Vitamin E versus placebo
Kessopoulou 1995 Vitamin E
Median=7 (n=15)
min/max= -27-34
Placebo
Median=7 (n=15)
min/max= -33-36
L-carnitine versus placebo
Lenzi 2003 L-carnitine
Mean=11(n=43)
no sd given
Placebo
Mean=8.8 (n=43)
no sd given
Pentoxifylline versus Placebo
Merino 1997 Pentoxifylline
Median=35.5 (n=25)
Range=31.5-39.5
Placebo
Median=33.5 (n=22)
Range=28.5-37.5
Analysis 1.15. Comparison 1 Antioxidant(s) versus control, Outcome 15 Sperm motility at 6 months.
Sperm motility at 6 months
Study Heading one Heading two
L-carnitine + Acetyl-carnitine versus placebo (median and interquartile range)
Cavallini 2004 L-carnitine + acetyl-carnitine
Median=23.6 (n=39)
Interquartile range=28.9-16.0
Placebo
Median=13.2 (n=47)
Interquartile range=18.6-9.0
Pentoxifylline versus placebo
Merino 1997 Pentoxifylline
Median=42 (n=25)
Range=38-46
Placebo
Median=31.5 (22)
Range=28-35
Folic acid versus placebo
Wong 2002 Folic acid
Median=35 (n=22)
Range=5-65
Placebo
Median=30 (n=25)
Range=5-80
Zinc versus placebo
Wong 2002 Zinc
Median=35 (n=23)
Range=10-65
Placebo
Median=30 (n=25)
115Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Sperm motility at 6 months (Continued)
Range=5-80
Zinc + folic acid versus placebo
Wong 2002 Zinc + folic acid
Median=35 (n=24)
Range 5-70
Placebo
Median=30 (n=25)
Range=5-80
Analysis 1.16. Comparison 1 Antioxidant(s) versus control, Outcome 16 Sperm concentration at 3 months
or less.
Sperm concentration at 3 months or less
Study Heading one Heading two
L-carnitine + Acetyl-carnitine versus placebo (median and interquartile range)
Cavallini 2004 L-carnitine + acetyl-carnitine
Median=20.9 (n=39)
Interquartile range=25.6-14.8
Placebo
Median=12.3 (n=47)
Interquartile range=16.0-9.1
Vitamin E versus placebo
Kessopoulou 1995 Vitamin E
Median= -15 (n=15)
min/max= -58-59
Placebo
Median=0 (n=15)
min/max= -37-160
L-carnitine versus placebo
Lenzi 2003 L-carnitine
Mean= 9 (1st phase data) (n=43)
no sd given
Placebo
Mean=5.3 (n=43)
no sd given
Analysis 1.17. Comparison 1 Antioxidant(s) versus control, Outcome 17 Sperm concentration at 6 months.
Sperm concentration at 6 months
Study Heading one Heading two
L-carnitine + acetyl-carnitine versus placebo
Cavallini 2004 L-carnitine + acetyl-carniitne
Median=20.6 (n=39)
Interquartile range=24.9-15.1
Placebo
Median=10.9 (n=47)
Interquartile range=15.1-9.0
Folic acid versus Placebo
116Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Sperm concentration at 6 months (Continued)
Wong 2002 Folic acid
Median=14 (n=22)
Range=0.9-130
Placebo
Median=9 (n=25)
Range=0.8-80
Zinc versus Placebo
Wong 2002 Zinc
Median=16 (n= 23)
Range=0.6-80
Placebo
Median=9 (n= 25)
Range=0.8-80
Analysis 1.18. Comparison 1 Antioxidant(s) versus control, Outcome 18 Pregnancy.
Review: Antioxidants for male subfertility
Comparison: 1 Antioxidant(s) versus control
Outcome: 18 Pregnancy
Study or subgroup Experimental Control Peto Odds Ratio Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
1 Pregnancy rate of trials that also report live birth
Omu 1998 11/49 2/48 4.75 [ 1.49, 15.20 ]
Suleiman 1996 11/52 0/35 6.64 [ 1.84, 23.93 ]
Subtotal (95% CI) 101 83 5.53 [ 2.34, 13.08 ]
Total events: 22 (Experimental), 2 (Control)
Heterogeneity: Chi2 = 0.14, df = 1 (P = 0.71); I2 =0.0%
Test for overall effect: Z = 3.89 (P = 0.00010)
2 Pregnancy rate only reported
Balercia 2005 9/45 3/15 1.00 [ 0.23, 4.26 ]
Balercia 2009 6/30 3/30 2.16 [ 0.53, 8.82 ]
Cavallini 2004 9/39 1/47 7.50 [ 2.01, 27.98 ]
Galatioto 2008 1/20 0/22 8.17 [ 0.16, 413.39 ]
Lenzi 2003 6/43 0/43 8.37 [ 1.61, 43.58 ]
Lenzi 2004 4/30 0/26 7.20 [ 0.95, 54.34 ]
Peivandi 2010 3/15 0/15 8.57 [ 0.82, 89.45 ]
Rolf 1999 0/15 0/16 0.0 [ 0.0, 0.0 ]
Safarinejad 2009a 0/106 0/106 0.0 [ 0.0, 0.0 ]
0.005 0.1 1 10 200
Favours control Favours antioxidant
(Continued . . . )
117Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Peto Odds Ratio Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
Sigman 2006 1/10 0/10 7.39 [ 0.15, 372.38 ]
Tremellen 2007 20/38 4/20 3.75 [ 1.26, 11.16 ]
Wang 1983 0/11 0/7 0.0 [ 0.0, 0.0 ]
Zavaczki 2003 1/10 0/10 7.39 [ 0.15, 372.38 ]
Subtotal (95% CI) 412 367 4.02 [ 2.34, 6.92 ]
Total events: 60 (Experimental), 11 (Control)
Heterogeneity: Chi2 = 6.96, df = 9 (P = 0.64); I2 =0.0%
Test for overall effect: Z = 5.02 (P < 0.00001)
Total (95% CI) 513 450 4.40 [ 2.78, 6.97 ]
Total events: 82 (Experimental), 13 (Control)
Heterogeneity: Chi2 = 7.48, df = 11 (P = 0.76); I2 =0.0%
Test for overall effect: Z = 6.32 (P < 0.00001)
Test for subgroup differences: Chi2 = 0.38, df = 1 (P = 0.54), I2 =0.0%
0.005 0.1 1 10 200
Favours control Favours antioxidant
Analysis 2.1. Comparison 2 Live birth versus pregnancy, Outcome 1 Live birth.
Review: Antioxidants for male subfertility
Comparison: 2 Live birth versus pregnancy
Outcome: 1 Live birth
Study or subgroup Experimental Control Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
1 live birth
Omu 1998 8/49 2/48 53.6 % 3.67 [ 1.00, 13.51 ]
Suleiman 1996 9/52 0/35 46.4 % 6.33 [ 1.56, 25.63 ]
Subtotal (95% CI) 101 83 100.0 % 4.73 [ 1.82, 12.27 ]
Total events: 17 (Experimental), 2 (Control)
Heterogeneity: Chi2 = 0.31, df = 1 (P = 0.58); I2 =0.0%
Test for overall effect: Z = 3.19 (P = 0.0014)
2 pregnancy
Omu 1998 11/49 2/48 54.9 % 4.75 [ 1.49, 15.20 ]
Suleiman 1996 11/52 0/35 45.1 % 6.64 [ 1.84, 23.93 ]
Subtotal (95% CI) 101 83 100.0 % 5.53 [ 2.34, 13.08 ]
0.005 0.1 1 10 200
Favours control Favours antioxidant
(Continued . . . )
118Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
Total events: 22 (Experimental), 2 (Control)
Heterogeneity: Chi2 = 0.14, df = 1 (P = 0.71); I2 =0.0%
Test for overall effect: Z = 3.89 (P = 0.00010)
0.005 0.1 1 10 200
Favours control Favours antioxidant
Analysis 3.1. Comparison 3 Head to head antioxidant(s), Outcome 1 Pregnancy per couple randomised.
Review: Antioxidants for male subfertility
Comparison: 3 Head to head antioxidant(s)
Outcome: 1 Pregnancy per couple randomised
Study or subgroup Antioxidant ’a’ Antioxidant ’b’ Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
1 L acetyl carnitine + L carnitine versus L acetyl carnitine
Balercia 2005 2/7 2/15 100.0 % 2.66 [ 0.27, 25.80 ]
Subtotal (95% CI) 7 15 100.0 % 2.66 [ 0.27, 25.80 ]
Total events: 2 (Antioxidant ’a’), 2 (Antioxidant ’b’)
Heterogeneity: not applicable
Test for overall effect: Z = 0.84 (P = 0.40)
2 L acetyl carnitine + L carnitine versus L- carnitine
Balercia 2005 3/8 2/15 100.0 % 3.89 [ 0.51, 29.76 ]
Subtotal (95% CI) 8 15 100.0 % 3.89 [ 0.51, 29.76 ]
Total events: 3 (Antioxidant ’a’), 2 (Antioxidant ’b’)
Heterogeneity: not applicable
Test for overall effect: Z = 1.31 (P = 0.19)
3 L acetyl carnitine + L carnitine versus Vitamin E + Vitamin C
Li 2005 10/90 2/60 100.0 % 2.86 [ 0.86, 9.49 ]
Subtotal (95% CI) 90 60 100.0 % 2.86 [ 0.86, 9.49 ]
Total events: 10 (Antioxidant ’a’), 2 (Antioxidant ’b’)
Heterogeneity: not applicable
Test for overall effect: Z = 1.71 (P = 0.086)
Test for subgroup differences: Chi2 = 0.08, df = 2 (P = 0.96), I2 =0.0%
0.01 0.1 1 10 100
Favours antioxidant ’b’ Favours antioxidant ’a’
119Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.2. Comparison 3 Head to head antioxidant(s), Outcome 2 Sperm total motility at 3 months or
less.
Review: Antioxidants for male subfertility
Comparison: 3 Head to head antioxidant(s)
Outcome: 2 Sperm total motility at 3 months or less
Study or subgroup Antioxidant b Antioxidant b Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Ethylcysteine 600mg/day vs Vitamin E
Akiyama 1999 5 40.9 (30.1) 5 42.8 (34.4) 100.0 % -1.90 [ -41.97, 38.17 ]
Subtotal (95% CI) 5 5 100.0 % -1.90 [ -41.97, 38.17 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.09 (P = 0.93)
2 Docosahexaenoic acid (DHA) 400g/day vs Docosahexaenoic acid 800mg/day
Conquer 2000 9 39.4 (24.3) 10 32 (16.1) 100.0 % 7.40 [ -11.35, 26.15 ]
Subtotal (95% CI) 9 10 100.0 % 7.40 [ -11.35, 26.15 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.77 (P = 0.44)
3 Ascorbic Acid 200mg/day versus Ascorbic Acid 1000mg/day
Dawson 1990 10 51 (22.1) 10 94 (32) 100.0 % -43.00 [ -67.10, -18.90 ]
Subtotal (95% CI) 10 10 100.0 % -43.00 [ -67.10, -18.90 ]
Heterogeneity: not applicable
Test for overall effect: Z = 3.50 (P = 0.00047)
4 Vitamin E + Selenium versus Vitamin B at 3 months
Keskes-Ammar 2003 28 39 (19) 26 39 (21) 100.0 % 0.0 [ -10.71, 10.71 ]
Subtotal (95% CI) 28 26 100.0 % 0.0 [ -10.71, 10.71 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P = 1.0)
5 Zinc versus Zinc + Vitamin E at 3 months
Omu 2008 6 49 (12) 12 50 (18) 100.0 % -1.00 [ -15.00, 13.00 ]
Subtotal (95% CI) 6 12 100.0 % -1.00 [ -15.00, 13.00 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.14 (P = 0.89)
6 Zinc versus Zinc + Vitamin E + Vitamin C at 3 months
Omu 2008 6 49 (12) 6 50 (20) 100.0 % -1.00 [ -19.66, 17.66 ]
Subtotal (95% CI) 6 6 100.0 % -1.00 [ -19.66, 17.66 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.11 (P = 0.92)
7 Zinc + Vitamin E versus Zinc + Vitamin E + Vitamin C at 3 months
Omu 2008 12 50 (18) 6 50 (20) 100.0 % 0.0 [ -18.97, 18.97 ]
Subtotal (95% CI) 12 6 100.0 % 0.0 [ -18.97, 18.97 ]
-50 -25 0 25 50
Antioxidant b Antioxidant a
(Continued . . . )
120Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Antioxidant b Antioxidant b Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P = 1.0)
8 Selenium versus combined antioxidants
Scott 1998 16 30.2 (22.8) 30 27 (20.3) 100.0 % 3.20 [ -10.13, 16.53 ]
Subtotal (95% CI) 16 30 100.0 % 3.20 [ -10.13, 16.53 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.47 (P = 0.64)
9 L acetyl carnitine + L carnitine versus Vitamin E + Vitamin C
Li 2005 90 38.29 (9.67) 60 15.24 (7.89) 100.0 % 23.05 [ 20.23, 25.87 ]
Subtotal (95% CI) 90 60 100.0 % 23.05 [ 20.23, 25.87 ]
Heterogeneity: not applicable
Test for overall effect: Z = 16.00 (P < 0.00001)
-50 -25 0 25 50
Antioxidant b Antioxidant a
Analysis 3.3. Comparison 3 Head to head antioxidant(s), Outcome 3 Sperm total motility at 6 months.
Review: Antioxidants for male subfertility
Comparison: 3 Head to head antioxidant(s)
Outcome: 3 Sperm total motility at 6 months
Study or subgroup Antioxidant ’a’ Antioxidant ’b’ Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 L-aceytl carnitine +L-carnitine versus L-carnitine at 6 months
Balercia 2005 7 61.07 (9.07) 15 64.53 (8.41) 100.0 % -3.46 [ -11.41, 4.49 ]
Subtotal (95% CI) 7 15 100.0 % -3.46 [ -11.41, 4.49 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.85 (P = 0.39)
2 L-acetyl carnitine + L-carnitine versus L-acetyl carnitine at 6 months
Balercia 2005 8 61.07 (9.07) 15 60.43 (10.46) 100.0 % 0.64 [ -7.58, 8.86 ]
Subtotal (95% CI) 8 15 100.0 % 0.64 [ -7.58, 8.86 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.15 (P = 0.88)
3 Selenium versus N-acetyl-cysteine at 26 weeks (6 months)
Safarinejad 2009 58 26.1 (2.9) 118 24.8 (2.9) 100.0 % 1.30 [ 0.39, 2.21 ]
Subtotal (95% CI) 58 118 100.0 % 1.30 [ 0.39, 2.21 ]
-10 -5 0 5 10
Favours antioxidant b Favours antioxidant a
(Continued . . . )
121Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Antioxidant ’a’ Antioxidant ’b’ Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Heterogeneity: not applicable
Test for overall effect: Z = 2.80 (P = 0.0052)
4 Selenium versus selenium plus N-acetyl-cysteine at 26 weeks (6 months)
Safarinejad 2009 58 26.1 (2.9) 58 29.2 (2.9) 100.0 % -3.10 [ -4.16, -2.04 ]
Subtotal (95% CI) 58 58 100.0 % -3.10 [ -4.16, -2.04 ]
Heterogeneity: not applicable
Test for overall effect: Z = 5.76 (P < 0.00001)
5 N-acetyl-cysteine vs selenium plus N-acetyl-cysteine at 26 weeks
Safarinejad 2009 118 24.8 (2.9) 58 29.2 (2.9) 100.0 % -4.40 [ -5.31, -3.49 ]
Subtotal (95% CI) 118 58 100.0 % -4.40 [ -5.31, -3.49 ]
Heterogeneity: not applicable
Test for overall effect: Z = 9.46 (P < 0.00001)
Test for subgroup differences: Chi2 = 81.67, df = 4 (P = 0.00), I2 =95%
-10 -5 0 5 10
Favours antioxidant b Favours antioxidant a
Analysis 3.4. Comparison 3 Head to head antioxidant(s), Outcome 4 Sperm total motility at 9 months or
more.
Review: Antioxidants for male subfertility
Comparison: 3 Head to head antioxidant(s)
Outcome: 4 Sperm total motility at 9 months or more
Study or subgroup Antioxidant ’a’ Antioxidant ’b’ Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 L-aceytl carnitine +L-carnitine versus L-carnitine at 9 months
Balercia 2005 7 49 (7.8) 15 54.27 (8.96) 100.0 % -5.27 [ -12.61, 2.07 ]
Subtotal (95% CI) 7 15 100.0 % -5.27 [ -12.61, 2.07 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.41 (P = 0.16)
2 L-acetyl carnitine + L-carnitine versus L-acetyl carnitine at 9 months
Balercia 2005 8 49 (7.8) 15 50.57 (5.71) 100.0 % -1.57 [ -7.70, 4.56 ]
Subtotal (95% CI) 8 15 100.0 % -1.57 [ -7.70, 4.56 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.50 (P = 0.62)
Test for subgroup differences: Chi2 = 0.57, df = 1 (P = 0.45), I2 =0.0%
-20 -10 0 10 20
Favours antioxidant ’b’ Favours antioxidant ’a’
122Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.5. Comparison 3 Head to head antioxidant(s), Outcome 5 Sperm concentration at 3 months or
less.
Review: Antioxidants for male subfertility
Comparison: 3 Head to head antioxidant(s)
Outcome: 5 Sperm concentration at 3 months or less
Study or subgroup Antioxidant ’a’ Antioxidant ’b’ Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Ethylcysteine 600mg/day vs Vitamin E
Akiyama 1999 5 20.1 (14.8) 5 17.9 (15.6) 100.0 % 2.20 [ -16.65, 21.05 ]
Subtotal (95% CI) 5 5 100.0 % 2.20 [ -16.65, 21.05 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.23 (P = 0.82)
2 Docosahexaenoic acid (DHA) 400g/day versus Docosahexaenoic acid (DHA) 800g/day
Conquer 2000 9 37.8 (36.9) 10 44.6 (41.1) 100.0 % -6.80 [ -41.87, 28.27 ]
Subtotal (95% CI) 9 10 100.0 % -6.80 [ -41.87, 28.27 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.38 (P = 0.70)
3 L-carnitine versus Vitamin E + Vitamin C
Li 2005a 32 34.6 (7.4) 31 19.1 (4.5) 100.0 % 15.50 [ 12.49, 18.51 ]
Subtotal (95% CI) 32 31 100.0 % 15.50 [ 12.49, 18.51 ]
Heterogeneity: not applicable
Test for overall effect: Z = 10.08 (P < 0.00001)
Test for subgroup differences: Chi2 = 3.36, df = 2 (P = 0.19), I2 =41%
-100 -50 0 50 100
Favours antioxidant ’b’ Favours antioxidant ’a’
123Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.6. Comparison 3 Head to head antioxidant(s), Outcome 6 Sperm concentration at 6 months.
Review: Antioxidants for male subfertility
Comparison: 3 Head to head antioxidant(s)
Outcome: 6 Sperm concentration at 6 months
Study or subgroup Antioxidant ’a’ Antioxidant ’b’ Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 L-aceytl carnitine +L-carnitine versus L-carnitine at 6 months
Balercia 2005 7 37.4 (16.42) 15 45.53 (21.42) 100.0 % -8.13 [ -24.42, 8.16 ]
Subtotal (95% CI) 7 15 100.0 % -8.13 [ -24.42, 8.16 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.98 (P = 0.33)
2 L-acetyl carnitine + L-carnitine versus L-acetyl carnitine at 6 months
Balercia 2005 8 37.4 (16.42) 15 39.57 (19.99) 100.0 % -2.17 [ -17.40, 13.06 ]
Subtotal (95% CI) 8 15 100.0 % -2.17 [ -17.40, 13.06 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.28 (P = 0.78)
3 Selenium versus N-acetyl-cysteine at 26 weeks (6 months)
Safarinejad 2009 58 27.6 (6.4) 118 26.8 (5.3) 100.0 % 0.80 [ -1.10, 2.70 ]
Subtotal (95% CI) 58 118 100.0 % 0.80 [ -1.10, 2.70 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.82 (P = 0.41)
4 Selenium versus selenium plus N-acetyl-cysteine at 26 weeks (6 months)
Safarinejad 2009 58 27.6 (6.4) 58 32.1 (6.8) 100.0 % -4.50 [ -6.90, -2.10 ]
Subtotal (95% CI) 58 58 100.0 % -4.50 [ -6.90, -2.10 ]
Heterogeneity: not applicable
Test for overall effect: Z = 3.67 (P = 0.00024)
5 N-acetyl-cysteine vs selenium plus N-acetyl-cysteine at 26 weeks
Safarinejad 2009 118 26.8 (5.3) 58 32.1 (6.8) 100.0 % -5.30 [ -7.29, -3.31 ]
Subtotal (95% CI) 118 58 100.0 % -5.30 [ -7.29, -3.31 ]
Heterogeneity: not applicable
Test for overall effect: Z = 5.21 (P < 0.00001)
Test for subgroup differences: Chi2 = 22.09, df = 4 (P = 0.00), I2 =82%
-20 -10 0 10 20
Favours antioxidant ’b’ Favours antioxidant ’a’
124Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.7. Comparison 3 Head to head antioxidant(s), Outcome 7 Sperm concentration at 9 months or
more.
Review: Antioxidants for male subfertility
Comparison: 3 Head to head antioxidant(s)
Outcome: 7 Sperm concentration at 9 months or more
Study or subgroup Antioxidant ’a’ Antioxidant ’b’ Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 L-aceytl carnitine +L-carnitine versus L-carnitine at 9 months
Balercia 2005 7 33.27 (13.62) 15 39.4 (13.93) 100.0 % -6.13 [ -18.44, 6.18 ]
Subtotal (95% CI) 7 15 100.0 % -6.13 [ -18.44, 6.18 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.98 (P = 0.33)
2 L-acetyl carnitine + L-carnitine versus L-acetyl carnitine at 9 months
Balercia 2005 8 33.27 (13.62) 15 31.21 (8.6) 100.0 % 2.06 [ -8.33, 12.45 ]
Subtotal (95% CI) 8 15 100.0 % 2.06 [ -8.33, 12.45 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.39 (P = 0.70)
Test for subgroup differences: Chi2 = 0.99, df = 1 (P = 0.32), I2 =0.0%
-20 -10 0 10 20
Favours antioxidant ’b’ Favours antioxidant ’a’
Analysis 3.8. Comparison 3 Head to head antioxidant(s), Outcome 8 Side effects.
Review: Antioxidants for male subfertility
Comparison: 3 Head to head antioxidant(s)
Outcome: 8 Side effects
Study or subgroup Experimental Control Odds Ratio Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 L acetyl carnitine + L carnitine versus Vitamin E + Vitamin C
Li 2005 0/90 0/60 0.0 [ 0.0, 0.0 ]
Total (95% CI) 90 60 0.0 [ 0.0, 0.0 ]
Total events: 0 (Experimental), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P < 0.00001)
0.01 0.1 1 10 100
Favours antioxidant ’a’ Favours antioxidant ’b’
125Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.9. Comparison 3 Head to head antioxidant(s), Outcome 9 Sperm concentration at 6 months.
Sperm concentration at 6 months
Study Heading one Heading two
Zinc versus Folic acid
Wong 2002 Zinc
Median=16
Range=0.6-80
Folic acid
Median=14
Range=0.9-130
Zinc versus Zinc + Folic acid
Wong 2002 Zinc
Median= 16
Range=0.6-80
Zinc + Folic acid
Median=12
Range=0.5-180
Analysis 3.10. Comparison 3 Head to head antioxidant(s), Outcome 10 Sperm motility at 6 months.
Sperm motility at 6 months
Study Heading one Heading two
Zinc versus Folic acid
Wong 2002 Zinc
Median=35
Range=10-65
Folic acid
Median=35
Range=5-65
A P P E N D I C E S
Appendix 1. MEDLINE search strategy
1 exp male infertility/ (19113)
2 (asthenozoospermia or oligospermia or azoospermia).tw. (4464)
3 exp Spermatozoa/ (48125)
4 Sperm$.tw. (85274)
5 (male$ adj2 subfertil$).tw. (484)
6 (male$ adj2 infertil$).tw. (5719)
7 (subfertil$ adj2 men).tw. (356)
8 (infertil$ adj2 men).tw. (2400)
9 (male$ adj2 fertility).tw. (2706)
10 semen.tw. (16927)
11 oligoasthenoteratozoospermi$.tw. (185)
12 or/1-11 (108373)
126Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

13 exp antioxidants/ or free radical scavengers/ (280006)
14 (antioxidant$ or radical scavengers).tw. (69599)
15 exp vitamins/ or exp ascorbic acid/ or exp dehydroascorbic acid/ or exp vitamin a/ or exp vitamin e/ or exp vitamin u/ or exp alpha-
tocopherol/ or exp beta carotene/ or exp beta-tocopherol/ or exp gamma-tocopherol/ (234713)
16 vitamin$.tw. (111181)
17 exp Zinc/ (41085)
18 exp Selenium/ (13920)
19 (Glutathione$ or folate).tw. (81376)
20 exp Ubiquinone/ (5352)
21 ubiquin$.tw. (5228)
22 coenzyme q10.tw. (1462)
23 exp Carnitine/ (6812)
24 (carnitine$ or carotenoid$).tw. (17142)
25 (astaxanthin$ or lycopene$).tw. (2711)
26 menevit.tw. (1)
27 multivitamin$.tw. (1967)
28 (betacarotene$ or beta carotene$).tw. (7738)
29 ascorbic acid.tw. (18104)
30 n-acetylcysteine.tw. (5514)
31 alpha-tocopherol$.tw. (10653)
32 exp Pentoxifylline/ (3302)
33 Pentoxifylline$.tw. (3079)
34 (fish adj2 oil$).tw. (5536)
35 omega$.tw. (23211)
36 exp fatty acids/ or exp fish oils/ or exp cod liver oil/ or exp fatty acids, omega-3/ or exp plant oils/ (321518)
37 fatty acid$.tw. (109608)
38 (plant adj4 oil$).tw. (899)
39 l-arginine$.tw. (25627)
40 flavonoid$.tw. (11562)
41 carotenoid$.tw. (8425)
42 riboflavin$.tw. (5897)
43 pycnogenol$.tw. (177)
44 lutein$.tw. (27811)
45 lipoic acid$.tw. (1986)
46 or/13-45 (968481)
47 46 and 12 (8395)
48 randomized controlled trial.pt. (280587)
49 controlled clinical trial.pt. (80011)
50 randomized.ab. (190341)
51 placebo.tw. (118552)
52 clinical trials as topic.sh. (146404)
53 randomly.ab. (138335)
54 trial.ti. (82364)
55 (crossover or cross-over or cross over).tw. (43907)
56 or/48-55 (666167)
57 (animals not (humans and animals)).sh. (3345663)
58 56 not 57 (615399)
59 47 and 58 (247)
60 from 59 keep 1-247 (247)
127Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Appendix 2. EMBASE search strategy
1 exp male infertility/ (17017)
2 (asthenozoospermia or oligospermia or azoospermia).tw. (3803)
3 exp Spermatozoa/ (10504)
4 Sperm$.tw. (62512)
5 (male$ adj2 subfertil$).tw. (451)
6 (male$ adj2 infertil$).tw. (5173)
7 (subfertil$ adj2 men).tw. (302)
8 (infertil$ adj2 men).tw. (2207)
9 (male$ adj2 fertility).tw. (2138)
10 semen.tw. (11264)
11 oligoasthenoteratozoospermi$.tw. (192)
12 or/1-11 (74872)
13 vitamin$.tw. (83637)
14 exp Zinc/ (44487)
15 exp Selenium/ (15822)
16 (Glutathione$ or folate).tw. (72891)
17 exp Ubiquinone/ (3388)
18 ubiquin$.tw. (4120)
19 coenzyme q10.tw. (1640)
20 exp Carnitine/ (6361)
21 (carnitine$ or carotenoid$).tw. (14110)
22 (astaxanthin$ or lycopene$).tw. (2452)
23 menevit.tw. (6)
24 multivitamin$.tw. (1730)
25 (betacarotene$ or beta carotene$).tw. (6736)
26 ascorbic acid.tw. (13434)
27 n-acetylcysteine.tw. (5536)
28 alpha-tocopherol$.tw. (9008)
29 exp Pentoxifylline/ (8389)
30 Pentoxifylline$.tw. (3181)
31 (fish adj2 oil$).tw. (5366)
32 omega$.tw. (19649)
33 fatty acid$.tw. (85842)
34 (plant adj4 oil$).tw. (937)
35 l-arginine$.tw. (24461)
36 flavonoid$.tw. (11342)
37 carotenoid$.tw. (6265)
38 riboflavin$.tw. (3601)
39 pycnogenol$.tw. (202)
40 lutein$.tw. (21048)
41 lipoic acid$.tw. (1791)
42 exp antioxidant/ (46224)
43 exp vitamin/ or exp ascorbic acid/ or exp carotenoid/ or exp multivitamin/ or vitamin b group/ (246879)
44 exp fatty acid/ (244186)
45 exp vegetable oil/ (25806)
46 exp fish oil/ (7175)
47 exp cod liver oil/ (573)
48 exp omega 3 fatty acid/ (8974)
49 or/13-48 (735430)
50 12 and 49 (5848)
51 Clinical Trial/ (579096)
128Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

52 Randomized Controlled Trial/ (181492)
53 exp randomization/ (27531)
54 Single Blind Procedure/ (9051)
55 Double Blind Procedure/ (76202)
56 Crossover Procedure/ (22447)
57 Placebo/ (138119)
58 Randomi?ed controlled trial$.tw. (37822)
59 Rct.tw. (3250)
60 random allocation.tw. (669)
61 randomly allocated.tw. (10813)
62 allocated randomly.tw. (1393)
63 (allocated adj2 random).tw. (573)
64 Single blind$.tw. (7937)
65 Double blind$.tw. (88810)
66 ((treble or triple) adj blind$).tw. (149)
67 placebo$.tw. (116382)
68 prospective study/ (90830)
69 or/51-68 (760080)
70 case study/ (6847)
71 case report.tw. (127165)
72 abstract report/ or letter/ (526689)
73 or/70-72 (658112)
74 69 not 73 (733696)
75 50 and 74 (544)
76 (2009$ or 2010$).em. (774638)
77 75 and 76 (59)
78 from 77 keep 1-59 (59)
Appendix 3. CENTRAL search strategy
1 exp male infertility/ (433)
2 (asthenozoospermia or oligospermia or azoospermia).tw. (180)
3 exp Spermatozoa/ (315)
4 Sperm$.tw. (1726)
5 (male$ adj2 subfertil$).tw. (52)
6 (male$ adj2 infertil$).tw. (266)
7 (subfertil$ adj2 men).tw. (19)
8 (infertil$ adj2 men).tw. (91)
9 (male$ adj2 fertility).tw. (42)
10 semen.tw. (510)
11 oligoasthenoteratozoospermi$.tw. (6)
12 or/1-11 (2087)
13 exp antioxidants/ or free radical scavengers/ (8109)
14 (antioxidant$ or radical scavengers).tw. (2829)
15 exp vitamins/ or exp ascorbic acid/ or exp dehydroascorbic acid/ or exp vitamin a/ or exp vitamin e/ or exp vitamin u/ or exp alpha-
tocopherol/ or exp beta carotene/ or exp beta-tocopherol/ or exp gamma-tocopherol/ (9080)
16 vitamin$.tw. (7367)
17 exp Zinc/ (930)
18 exp Selenium/ (345)
19 (Glutathione$ or folate).tw. (1838)
20 exp Ubiquinone/ (200)
21 ubiquin$.tw. (70)
22 coenzyme q10.tw. (189)
129Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

23 exp Carnitine/ (358)
24 (carnitine$ or carotenoid$).tw. (955)
25 (astaxanthin$ or lycopene$).tw. (231)
26 menevit.tw. (1)
27 multivitamin$.tw. (392)
28 (betacarotene$ or beta carotene$).tw. (959)
29 ascorbic acid.tw. (747)
30 n-acetylcysteine.tw. (444)
31 alpha-tocopherol$.tw. (850)
32 exp Pentoxifylline/ (356)
33 Pentoxifylline$.tw. (589)
34 (fish adj2 oil$).tw. (998)
35 omega$.tw. (885)
36 exp fatty acids/ or exp fish oils/ or exp cod liver oil/ or exp fatty acids, omega-3/ or exp plant oils/ (13281)
37 fatty acid$.tw. (4996)
38 (plant adj4 oil$).tw. (48)
39 l-arginine$.tw. (775)
40 flavonoid$.tw. (221)
41 carotenoid$.tw. (380)
42 riboflavin$.tw. (242)
43 pycnogenol$.tw. (50)
44 lutein$.tw. (1402)
45 lipoic acid$.tw. (108)
46 or/13-45 (36854)
47 46 and 12 (253)
48 from 47 keep 1-253 (253)
Appendix 4. CINAHL search strategy
CINAHL search from inception until 13.08.08
1 exp male infertility/ (0)
2 (asthenozoospermia or oligospermia or azoospermia).tw. (35)
3 (male$ or men or man).tw. (60126)
4 exp Spermatozoa/ (269)
5 Sperm$.tw. (585)
6 or/1-5 (60531)
7 exp antioxidants/ or free radical scavengers/ (3528)
8 (antioxidant$ or radical scavengers).tw. (2606)
9 exp vitamins/ or exp ascorbic acid/ or exp dehydroascorbic acid/ or exp vitamin a/ or exp vitamin e/ or exp vitamin u/ or exp alpha-
tocopherol/ or exp beta carotene/ or exp beta-tocopherol/ or exp gamma-tocopherol/ (11605)
10 vitamin$.tw. (6740)
11 exp Zinc/ (1056)
12 (zinc or selenium).tw. (1529)
13 exp Selenium/ (524)
14 exp Glutathione Peroxidase/ or exp folic acid/ (2362)
15 (Glutathione$ or folate).tw. (1745)
16 exp Ubiquinone/ (328)
17 (ubiquin$ or folic acid).tw. (988)
18 coenzyme q10.tw. (149)
19 exp Carnitine/ (271)
20 (carnitine$ or carotenoid$).tw. (609)
21 (astaxanthin$ or lycopene$).tw. (223)
22 menevit.tw. (2)
130Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

23 or/7-22 (18483)
24 6 and 23 (1359)
25 exp fertilization in vitro/ or exp sperm injections, intracytoplasmic/ or exp Insemination, Artificial, Homologous/ (947)
26 (in vitro fertilisation or intracytoplasmic sperm injection$).tw. (148)
27 (intrauterine adj3 insemination$).tw. (45)
28 (ivf or icsi or iui).tw. (332)
29 in-vitro fertilisation.tw. (90)
30 in vitro fertilization.tw. (287)
31 ART.tw. (5558)
32 Artificial reproduc$ technique$.tw. (1)
33 or/25-32 (6666)
34 24 and 33 (8)
35 exp clinical trials/ (61758)
36 Clinical trial.pt. (32434)
37 (clinic$ adj trial$1).tw. (14019)
38 ((singl$ or doubl$ or trebl$ or tripl$) adj (blind$3 or mask$3)).tw. (8276)
39 Randomi?ed control$ trial$.tw. (12024)
40 Random assignment/ (18434)
41 Random$ allocat$.tw. (1272)
42 Placebo$.tw. (11470)
43 Placebos/ (4474)
44 Quantitative studies/ (4044)
45 Allocat$ random$.tw. (74)
46 or/35-45 (85043)
47 34 and 46 (3)
48 from 47 keep 1-3 (3)
CINAHL search from 13.08.08 until 22.02.10
# Query Limiters/Expanders Last Run Via Results
S5 S1 and S4 Search modes
- Boolean/Phrase
Interface
- EBSCOhost
Search Screen
- Advanced Search
Database
- CINAHL Plus
31
S4 S2 or S3 Search modes
- Boolean/Phrase
Interface
- EBSCOhost
Search Screen
- Advanced Search
Database
- CINAHL Plus
1167
S3 (“sperm”) or (MH “Sperm
Count”) or (MH “Spermato-
zoa”)
Search modes
- Boolean/Phrase
Interface
- EBSCOhost
Search Screen
- Advanced Search
Database
- CINAHL Plus
1074
131Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
S2 “male infertility” Search modes
- Boolean/Phrase
Interface
- EBSCOhost
Search Screen
- Advanced Search
Database
- CINAHL Plus
168
S1 (MH “Antioxidants+”) or
(MH “Berries+”) or
(MH “Chlorophyll”) or (MH
“Flavonoids+”) or (MH “Ly-
copene”) or (MH “Polyphe-
nols+”)
Search modes
- Boolean/Phrase
Interface
- EBSCOhost
Search Screen
- Advanced Search
Database
- CINAHL Plus
8581
Appendix 5. PsycINFO search strategy
1 exp male infertility/ (0)
2 (asthenozoospermia or oligospermia or azoospermia).tw. (26)
3 exp Spermatozoa/ (0)
4 Sperm$.tw. (1871)
5 (male$ adj2 subfertil$).tw. (6)
6 (male$ adj2 infertil$).tw. (114)
7 (subfertil$ adj2 men).tw. (0)
8 (infertil$ adj2 men).tw. (46)
9 (male$ adj2 fertility).tw. (89)
10 semen.tw. (268)
11 oligoasthenoteratozoospermi$.tw. (1)
12 or/1-11 (2254)
13 exp antioxidants/ or free radical scavengers/ (736)
14 (antioxidant$ or radical scavengers).tw. (1433)
15 exp vitamins/ or exp ascorbic acid/ or exp dehydroascorbic acid/ or exp vitamin a/ or exp vitamin e/ or exp vitamin u/ or exp alpha-
tocopherol/ or exp beta carotene/ or exp beta-tocopherol/ or exp gamma-tocopherol/ (2281)
16 vitamin$.tw. (3287)
17 exp Zinc/ (317)
18 exp Selenium/ (0)
19 (Glutathione$ or folate).tw. (1280)
20 exp Ubiquinone/ (0)
21 ubiquin$.tw. (52)
22 coenzyme q10.tw. (49)
23 exp Carnitine/ (0)
24 (carnitine$ or carotenoid$).tw. (310)
25 (astaxanthin$ or lycopene$).tw. (16)
26 menevit.tw. (0)
27 multivitamin$.tw. (115)
28 (betacarotene$ or beta carotene$).tw. (64)
29 ascorbic acid.tw. (264)
30 n-acetylcysteine.tw. (65)
31 alpha-tocopherol$.tw. (127)
132Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

32 exp Pentoxifylline/ (0)
33 Pentoxifylline$.tw. (40)
34 (fish adj2 oil$).tw. (87)
35 omega$.tw. (908)
36 exp fatty acids/ or exp fish oils/ or exp cod liver oil/ or exp fatty acids, omega-3/ or exp plant oils/ (1906)
37 fatty acid$.tw. (1589)
38 (plant adj4 oil$).tw. (18)
39 l-arginine$.tw. (555)
40 flavonoid$.tw. (87)
41 carotenoid$.tw. (153)
42 riboflavin$.tw. (92)
43 pycnogenol$.tw. (9)
44 lutein$.tw. (1034)
45 lipoic acid$.tw. (52)
46 or/13-45 (11595)
47 46 and 12 (29)
48 from 47 keep 1-29 (29)
Appendix 6. AMED search strategy
1 exp male infertility/ (0)
2 (asthenozoospermia or oligospermia or azoospermia).tw. (12)
3 exp Spermatozoa/ (32)
4 Sperm$.tw. (151)
5 (male$ adj2 subfertil$).tw. (4)
6 (male$ adj2 infertil$).tw. (107)
7 (subfertil$ adj2 men).tw. (2)
8 (infertil$ adj2 men).tw. (7)
9 (male$ adj2 fertility).tw. (24)
10 semen.tw. (82)
11 oligoasthenoteratozoospermi$.tw. (0)
12 or/1-11 (285)
13 exp antioxidants/ or free radical scavengers/ (1009)
14 (antioxidant$ or radical scavengers).tw. (1775)
15 exp vitamins/ or exp ascorbic acid/ or exp dehydroascorbic acid/ or exp vitamin a/ or exp vitamin e/ or exp vitamin u/ or exp alpha-
tocopherol/ or exp beta carotene/ or exp beta-tocopherol/ or exp gamma-tocopherol/ (2001)
16 vitamin$.tw. (1947)
17 exp Zinc/ (92)
18 exp Selenium/ (83)
19 (Glutathione$ or folate).tw. (574)
20 exp Ubiquinone/ (0)
21 ubiquin$.tw. (28)
22 coenzyme q10.tw. (62)
23 exp Carnitine/ (14)
24 (carnitine$ or carotenoid$).tw. (157)
25 (astaxanthin$ or lycopene$).tw. (36)
26 menevit.tw. (0)
27 multivitamin$.tw. (52)
28 (betacarotene$ or beta carotene$).tw. (91)
29 ascorbic acid.tw. (374)
30 n-acetylcysteine.tw. (25)
31 alpha-tocopherol$.tw. (73)
32 exp Pentoxifylline/ (0)
133Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

33 Pentoxifylline$.tw. (7)
34 (fish adj2 oil$).tw. (142)
35 omega$.tw. (173)
36 exp fatty acids/ or exp fish oils/ or exp cod liver oil/ or exp fatty acids, omega-3/ or exp plant oils/ (1076)
37 fatty acid$.tw. (588)
38 (plant adj4 oil$).tw. (689)
39 l-arginine$.tw. (101)
40 flavonoid$.tw. (903)
41 carotenoid$.tw. (91)
42 riboflavin$.tw. (16)
43 pycnogenol$.tw. (15)
44 lutein$.tw. (47)
45 lipoic acid$.tw. (35)
46 or/13-45 (6342)
47 46 and 12 (24)
48 from 47 keep 1-24 (24)
Appendix 7. MDSG Specialised Register search strategy
Keywords CONTAINS “antioxidants” or “antioxidant levels” or “vitamin” or “vitamin A” or “vitamin B” or “Vitamin-B-12” or
“Vitamin-B-12-Therapeutic-Use” or “vitamin B6” or “vitamin C” or “Vitamin D” or “vitamin E” or “vitamins” or “selenium” or
“folic acid” or “glutathione” or “Menevit anti-oxidant” or “carnitene” or “carnitine” or “ascorbic acid” or “zinc” or “fatty acids” or
“oil” or “fish oils” or “plant extracts” or Title CONTAINS “fatty acids” or “oil” or “fish oils” or “plant extracts or ”antioxidants“ or
”antioxidant levels“ or ”vitamin“ or ”vitamin A“ or ”vitamin B“ or ”Vitamin-B-12“ or ”Vitamin-B-12-Therapeutic-Use“ or ”vitamin
B6“ or ”vitamin C“ or ”Vitamin D“ or ”vitamin E“ or ”vitamins“ or ”selenium“ or ”folic acid“ or ”glutathione“ or ”Menevit anti-
oxidant“ or ”carnitene“ or ”carnitine“ or ”ascorbic acid“ or ”zinc“
AND
Keywords CONTAINS ”IVF“ or ”ICSI“ or ”idiopathic asthenospermia“ or ”idiopathic oligozoospermia“ or ”in-vitro fertilisation “ or
”in-vitro fertilisation procedure“ or ”in vitro fertilization“ or ”intracytoplasmic sperm injection“ or ”intracytoplasmic morphologically
selected sperm injection“ or ”superovulation“ or ”superovulation induction“ or ”IUI“ or ”insemination, intrauterine “ or ”Intrauterine
Insemination“ or ”ART“ or ”artificial insemination“ or ”Sperm“ or ”sperm DNA integrity“ or ”sperm damage“ or ”sperm quality“ or
”sperm parameters“ or ”oligo-asthenozoospermia“ or ”Oligoasthenospermia“ or ”oligoasthenoteratozoospermia“ or ”oligospermia“ or
”oligozoospermia“ or ”asthenospermia“ or ”asthenozoospermia“ or ”assisted reproduction techniques“ or ”azoospermia“
Appendix 8. ’The World Health Organization International Trials Registry Platform’ search portal
1) Antioxidants AND men
2) Vitamins AND men
3) Antioxidant* AND male
4) Vitamin* AND male
5) Infertiltiy AND men
Appendix 9. ’ClinicalTrials.gov’ trials register
1) Antixidants AND men
2) Vitamins AND men
134Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Appendix 10. OpenSigle
1) Antioxidant*
2) Vitamin*
3) Infertility AND Men
W H A T ’ S N E W
Last assessed as up-to-date: 21 August 2010.
Date Event Description
3 May 2011 Amended 2.1 Analysis edited to fixed effect Peto. The conclusions remain the same.
H I S T O R Y
Protocol first published: Issue 4, 2008
Review first published: Issue 1, 2011
Date Event Description
8 March 2011 Amended Changed summary of findings table to reflect quality of studies
21 December 2010 Amended Minor edits made - no changes to conclusions
4 May 2007 New citation required and major changes Substantive amendment
C O N T R I B U T I O N S O F A U T H O R S
MGS: initiated, conceptualised and wrote the protocol. Performed the searches, selected trials for inclusion, assessed quality, performed
data extraction, entered data and wrote the final review.
RH: advised and supervised both the protocol and review, helped select trials for inclusion and wrote the implications for practice and
research and assisted with the abstract.
JB: co-drafted the protocol. Selected trials for inclusion, assessed quality and performed data extraction. Julie also provided advice on
the data analysis and helped with incorporating the editorial comments into the review.
AY: co-drafted the protocol and provided Word document concerning sperm DNA for background and provided technical advice.
MS: co-drafted the protocol and provided technical advice.
135Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D E C L A R A T I O N S O F I N T E R E S T
None known
S O U R C E S O F S U P P O R T
Internal sources
• Cochrane Menstrual Disorders and Subfertility Group, Not specified.
External sources
• No sources of support supplied
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
Sperm outcomes of concentration and motility were added as these two sperm outcomes are thought to reflect the oxidative process.
A study by El-Taieb (El-Taieb 2009) states that ”increased ROS generation and reduced antioxidant capacity is negatively correlated
with sperm concentration and motility in infertile men“.
The comparisons ’antioxidant versus placebo’ and ’antioxidants versus no treatment’ were combined as one comparison ’antioxidants
versus control’ and then it was stated under sensitivity analysis whether exclusion of those that failed to use placebo would have altered
the conclusions - as per statistical advice in editorial comments.
Subgrouping and sensitivity analysis were performed on the outcomes of live birth and pregnancy in order to assess the potential of
overestimation of benefit and reporting bias.
Sensitivity analysis was performed on trials that enrolled couples undergoing IVF or ICSI or IUI.
I N D E X T E R M S
Medical Subject Headings (MeSH)
Antioxidants [∗therapeutic use]; DNA Damage; Infertility, Male [∗drug therapy; etiology]; Live Birth; Oxidative Stress [∗drug effects];
Pregnancy Rate; Sperm Count; Sperm Motility [drug effects]; Spermatozoa [drug effects]
MeSH check words
Female; Humans; Male; Pregnancy
136Antioxidants for male subfertility (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.