Embed Size (px)
Citation preview

Antioxidant agents and physiological responses in
adult epileptic patients treated with lamotrigine
El¿bieta P³onka-Pó³torak1, Pawe³ Zagrodzki2,3, Fergus Nicol4, Jadwiga
Kryczyk2, Henryk Bartoñ2, Tuomas Westermarck5, Pekka Kaipainen5,
Sakaewan Ounjaijean5,6, Markus Kaski5, Faik Atroshi7
�Antiepileptic Outpatient Clinic, Provincial Hospital No. 2, Lwowska 60, PL 35-301 Rzeszów, Poland
�Department of Food Chemistry and Nutrition, Medical College, Jagiellonian University, Medyczna 9,
PL 30-688 Kraków, Poland
�Henryk Niewodniczañski Institute of Nuclear Physics, Radzikowskiego 152, PL 31-342 Kraków, Poland
�Vascular Health Division, Rowett Institute of Nutrition and Health, The University of Aberdeen, Bucksburn,
Aberdeen AB21 9SB, UK
�Rinnekoti Research Centre, FIN 02980 Espoo, Finland
�Faculty of Pharmacy, Payap University, Chiang Mai 50000, Thailand
�Department of Pharmacology and Toxicology, ELTDK, FIN 00014 University of Helsinki, Finland
Correspondence: El¿bieta P³onka-Pó³torak, e-mail: [email protected]
Abstract:
Background: The aim of our research was to evaluate some biochemical changes in blood during lamotrigine (LTG) monotherapy
of adult patients with epilepsy, and to check possible associations between typical selenium status parameters and the frequency of
seizures.
Methods: The study was performed by examining aspartate aminotransferase (AspAT), alanine aminotransferase (AlaAT), creati-
nine, ferric reducing ability of plasma (FRAP), serum uric acid (UA), uric-acid-independent FRAP (UAiFRAP), plasma glutathione
peroxidase (GPX3), selenoprotein P (SelP), plasma superoxide dismutase (pSOD), 8-hydroxy-2’-deoxyguanosine (8-OHdG) in se-
rum and urine, serum selenium (sSe) and zinc (sZn), in 22 adult patients with epilepsy and 22 healthy controls. Additionally, the lev-
els of LTG were determined in patients.
Results: pSOD activity was higher in the study group (5.32 ± 1.24 U/ml) compared with the controls (4.05 ± 0.92 U/ml, p = 0.008).
No other statistical difference between patients and controls was found.
Conclusion: Lack of difference in parameters other than SOD, particularly no difference in 8-OHdG concentrations between the pa-
tients treated with LTG compared to the control subjects suggests that these patients are at no particular risk of oxidative DNA dam-
age. In patients who are well or moderately well clinically controlled, selenium status parameters (sSe, GPX3, SelP) are not directly
connected with the frequency of seizures.
Key words:
epilepsy, lamotrigine, oxidative stress, selenium, superoxide dismutase
������������� �� ����� ����� ��� ����� 99
������������� �� ����
����� ��� �����
��� � �������
��������� � ����
�� �������� �� �!�"!#�$���
�$��� %#!&�"� �� �#���#��

Abbreviations: AEDs – antiepileptic drugs, AlaAT – alanine
aminotransferase, AspAT – aspartate aminotransferase, FRAP –
ferric reducing ability of plasma, GPX3 – plasma glutathione per-
oxidase, IGE – idiopathic generalized epilepsy, 8-OHdG – 8-
hydroxy-2’-deoxyguanosine, LTG – lamotrigine, pSOD – plasma
superoxide dismutase, ROS – reactive oxygen species, SelP –
selenoprotein P, sSe – serum selenium concentration, sZn – serum
zinc concentration, UA – uric acid, UAiFRAP – uric-acid-
independent ferric reducing ability of plasma, VPA – valproate
Introduction
It is now acknowledged, as demonstrated for animal
models, that reactive oxygen species (ROS) are gener-
ated in the epileptic processes [29, 34]. The neuronal
and glial cells are particularly susceptible to ROS-
induced oxidative damages. The predisposing condi-
tions for enhanced oxidative stress in brain may arise
from various biological phenomena, including high
oxygen consumption by neurons, low concentration of
endogenous antioxidants and concomitant accumula-
tion of reactive iron, the abundance of polyunsaturated
fatty acids comprising brain lipids, and excess of pre-
dominant neurotransmiter glutamate, inducing cell tox-
icity [20, 29, 37]. Pharmacotherapy of epilepsy is often
long life and may result, as epilepsy itself does, in an
increase of oxidative stress. For this reason the antioxi-
dative defense mechanisms can play an important role
in both seizure control and side effects of drugs taken
by epileptic patients [4]. There are evidences that nutri-
tionally essential element – selenium, in accord with
other trace elements, may alleviate the consequences of
lesions caused by excitotoxic conditions [22, 29], while
the deficiency of this element in humans was linked
with epileptic seizures [3, 28, 36]. However, the neuro-
protective effect may be mediated via different mecha-
nisms, not exclusively associated with its role in anti-
oxidant enzymes [29].
In our previous study [26], we demonstrated sig-
nificant changes in antioxidant status in blood during
valproate (VPA) monotherapy of adult epileptic pa-
tients. We also revealed that the frequency of seizures
and duration of VPA therapy were associated with
changes of oxidative/antioxidative balance. Obvi-
ously, the underlying mechanisms of complex interac-
tions between pathological conditions, antiepileptic
drugs (AEDs), and neuroprotective mechanisms in
patients with epilepsy are still far from being fully dis-
cerned. Thus, focus in the present study was on the po-
tential clinical relevance of parameters characterizing
biochemical and antioxidant status in blood during la-
motrigine (LTG) monotherapy of adult patients with
epilepsy. Lamotrigine is a triazine compound [3,5-
diamino-6-(2,3-dichlorophenyl)-1,2,4-triazine] with broad
spectrum of antiepileptic activity indicated for pri-
mary or secondarily generalized and partial seizures,
and Lennox-Gastaut syndrome [24]. LTG has multi-
ple mechanisms of actions, which are not fully eluci-
dated. It blocks voltage-gated sodium channels to sta-
bilize neuronal membranes, and inhibits release of the
excitatory amino acids [18]. LTG enhances cation
currents and alters dendritic h-channels, reducing the
excitability of neurons [17, 27]. The major metabolic
pathway for LTG is glucuronidation in the liver mi-
crosomes. LTG also undergoes hepatic and nonhe-
patic bioactivation to a reactive aryl epoxide interme-
diate, which can be related to the idiosyncratic cuta-
neous reactions or leucopenia associated with LTG
therapy [7]. Inactive metabolites are eliminated
mainly by renal excretion. Low protein binding
(55%), an absence of enzyme induction, and linear
pharmacokinetics are beneficial pharmacologic prop-
erties of LTG [23]. It has proven by numerous clinical
studies to be effective in the treatment of epilepsy
with a relatively low risk of side effects [33].
The information regarding the interactions between
lamotrigine and oxidative stress is scarce. In epileptic
patients treated either with VPA or LTG monothera-
pies, oxidative stress parameter – thiobarbituric acid
reactive substances – was elevated in VPA treated pa-
tients while it was normal in LTG group [8]. In line
with these results, treatment with lamotrigine was more
protective against oxidative stress in the cortex of the
brain and plasma in rats with experimentally induced
depression than the treatment with other medicines i.e.,
aripiprazole and escitalopram [10]. Similarly, Pavone
and Cardile proved that LTG at low concentrations, did
significantly change neither ROS production nor
lipoperoxidation level in antiepileptic drug treated pri-
mary rat astrocyte cultures [25]. Also in the study of
Agarwal et al. [1] LTG did not show significant altera-
tion in oxidative stress parameters during pentylenete-
trazole-kindling in mice. LTG treatment itself exerted
no significant effect on the levels of malondialdehyde,
reduced glutathione, superoxide dismutase and catalase
in non-kindled rats. The putative mild antioxidative LTG
activity was attributed to its inhibition of glutamate-
mediated excitotoxity through N-malondialdehde recep-
tors, which leads subsequently to lowering of ROS gen-
eration [2].
100 ������������� �� ����� ����� ��� �����

The current study was evaluated for detection of
possible changes, mainly in oxidant/antioxidant bal-
ance and selenium status, in the course of disease and
medical treatment with LTG, and to compare them (if
any) with those previously obtained for epileptic pa-
tients cured with VPA. The practical aspect of the
study was to indicate an antiepileptic drug which is
more advantageous in terms of oxidative stress pro-
tection. Plasma superoxide dismutase (pSOD), serum
zinc (sZn) concentration, and uric-acid-independent
ferric reducing ability of plasma (UAiFRAP) were de-
rived from our previous studies as the most sensitive
and relevant parameters (amid those studied) for char-
acterizing antioxidative defence mechanism, while
ferric reducing ability of plasma (FRAP) and serum
uric acid (UA) are auxiliary parameters for calculating
UAiFRAP values (see Methods section). Serum sele-
nium (sSe), selenoprotein P (SelP), and plasma glu-
tathione peroxidase (GPX3) are commonly acknowl-
edged as reliable selenium status parameters. The lat-
ter is also a major enzymatic antioxidant in plasma.
The levels of 8-hydroxy-2’-deoxyguanosine (8-OHdG)
in serum or urine provide information on systemic
oxidant/antioxidant status [12, 19]. The biochemical
parameters: aspartate aminotransferase (AspAT), al-
anine aminotransferase (AlaAT) and creatinine were
chosen to assess liver and renal functions in patients.
Patients
Fasting blood antioxidant status and diagnostic pa-
rameters’ levels were evaluated in 22 adult epileptic
patients (15 women and 7 men) receiving LTG anti-
convulsant monotherapy for at least 6 months (up to
������������� �� ����� ����� ��� ����� 101
Antioxidant agents in epileptic patients�������� �� ������� �� ���
Tab. 1. Demographic and clinical characteristics of the patients and controls (data shown as the mean values ± standard deviations; n –number of subjects in each group)
Parameter
Groups of patients
Whole study group (n = 22)Mean ± SD (Min-Max)
Male (n = 7)Mean ± SD (Min-Max)
Female (n = 15)Mean ± SD (Min-Max)
Age (years) 27.9 ± 5.4 (20-43) 25 ± 4.5 (20-34) 28.2 ± 3.9 (23-43)
Body Mass Index (kg/m2) 22.5 ± 2.8 (19.3-25.5) 21.6 ± 2.8 (20.4-25.5) 22.8 ± 2.9 (19.3-28.9)
Time of LTG
monotherapy (years)
5.0 ± 2.2 (0.5-8) 5.4 ± 2.2 (0.5-8) 4.9 ± 23 (1-8)
Daily dose of LTG
(mg/d)
210 ± 98 (50-400) 207 ± 107 (75-400) 212 ± 98 (50-400)
Serum LTG
(μmol/l)
20.6 ± 12.8 (5.0-47.2) 20.3 ± 9.4 (11.5-39.8) 21.7 ± 14.4 (5.0-47.2)
Epilepsy diagnosis IGE, n (%) 10 (45%) 4 (57%) 6 (40%)
MRI/CT findings, n (%) 3 (14%) 2 (28%) 1 (7%)
EEG normal, n (%)
GED
Others
3 (14%)
7 (32%)
12 (54%)
1 (14%)
3 (43%)
3 (43%)
2 (13%)
4 (27%)
9 (60%)
Patients with seizures inyear/month before study, n (%)
13/5 (59% / 23%) 3/0 (43% / 0%) 10/5 (67% / 33%)
Parameter Groups of controls
Whole control group (n = 22)
Mean ± SD (Min-Max)
Male (n = 8)
Mean ± SD (Min-Max)
Female (n = 14)
Mean ± SD (Min-Max)
Age (years) 28 ± 6 (21-43) 26 ± 4 (21-34) 29 ± 6 (22-43)
Body Mass Index (kg/m2) 24.0 ± 3.7 (19.8-33.2) 25.7 ± 3.1 (21.1-30.4) 23.0 ± 3.8 (19.8-33.2)
n – number of cases, SD – standard deviation, IGE – idiopathic generalised epilepsy, MRI – magnetic resonance imaging, CT – computer tomo-graphy, EEG – electroencephalography, GED – generalized epileptiform discharges, Others – focal or/and background abnormalities

8 years). All of them were treated in the antiepileptic
outpatient clinic of the Provincial Hospital in Rzeszów
(Poland). Exclusion criteria were pregnancy, breast-
feeding, and progressive brain pathology. No restric-
tions were imposed on diet habits during the sampling
period. Demographic and clinical characteristics of the
patients and controls are shown in Table 1.
The patients were not treated with any medication
other than LTG and they did not suffer from any con-
comitant disease. They were clinically either well
(seizure free in the year preceding the current study,
n = 9), or moderately controlled (one to more than ten
seizures in the last year, but not more than ten fits per
month, n = 13). Among the patients with general
tonic-clonic seizures the number of fits per year was
not more than three, and they had not seizure in the
month of the study). No signs of overdosage or seri-
ous adverse events were observed. The differences in
daily dose of LTG between male and female patients
were not statistically significant. The types of epi-
lepsy were identified according to International
League Against Epilepsy classification [9]. The sub-
jects comprised of 10 cases with idiopathic general-
ized epilepsy (IGE), and 12 patients with other types
(non-IGE), including localization-related sympto-
matic or cryptogenic epilepsies, and undetermined, ei-
ther focal or generalized. The control group consisted
of 22 sex- and age-matched subjects. They were re-
cruited from the hospital staff and students.
The local Ethical Committee of Regional Chamber
of Physicians approved the plan of the study. The in-
formed consent was obtained from all the participants.
Methods
Plasma and serum samples were obtained as described
previously [26]. The morning, casual urine samples
were collected from all the patients and controls on the
same day, and kept frozen (–20°C) until analysis.
Apart from LTG in serum of patients, the following
parameters were determined: aspartate aminotransfe-
rase (AspAT), alanine aminotransferase, creatinine,
FRAP, UA, UAiFRAP, GPX3, SelP, pSOD, 8-OHdG
in serum and urine, sSe and sZn. AspAT, AlaAT, and
creatinine were determined on routine basis using ma-
terials from Thermo Fisher Scientific Oy Clinical Di-
agnostics, Finland, and according to the manufactur-
er’s instructions. The assays for FRAP, uric acid,
pSOD and GPX3 were performed as previously de-
scribed [26]. UAiFRAP was calculated by subtracting
doubled UA molar concentration from FRAP [5].
Electrothermal atomic absorption spectrometric meas-
urements of sSe concentrations were performed on
a Perkin Elmer Model 5100 ZL. Serum zinc was de-
termined by electrothermal atomic absorption spec-
trometry by means of AAS-30 spectrometer (Carl-
Zeiss, Germany). The validity and accuracy of the se-
lenium and zinc determination were checked by a cer-
tified reference material SeronormTM Trace Ele-
ments Serum. The results indicated that analytical
procedures were reliable. For SelP determination
high-binding, 96 well plates (Greiner) were coated
with 100 μl antibody diluted in PBS (raised against
peptides by Eurogentec, and purified at RINH) and
incubated for 2 h at 37°C. The antibody solutions
were discarded and the plates washed with PBS con-
taining 0.05% Tween-20 and blocked overnight at
room temperature with 0.5% casein in PBS. Sixty μl
of samples or standards were mixed with 60 μl of
mouse monoclonal antibody (clone 37A1 AbFrontier,
Korea; diluted 1 : 1500) in round bottomed, 96 well
plates and stored overnight at 4°C. The next day, the
blocker in the high-binding plates was discarded and
they were washed 3 times with PBS containing 0.05%
Tween-20. A hundred μl of sample or standard was
transferred to the respective high-binding plate and
incubated at 37°C. After 2 h, the samples and stan-
dards were discarded and the plates washed again
3 times with PBS/Tween-20. A hundred μl of anti-
mouse HRP-linked antibody #7076 (1 : 5000) was
added and incubated at 37°C with shaking for 1 h.
The anti mouse HRP was discarded and the plates
washed 3 times with PBS/Tween-20. A hundred μl
TMB (KPL, USA) was added to each well and incu-
bated at room temperature for up to 30 min. Each
sample was analyzed in duplicate at two different di-
lutions (0.5 μl and 1 μl of plasma/well). Standards of
pure SelP were incubated alongside the samples
(range 0.25–16 ng/well) and a pooled plasma from the
previous study was used as a quality control. The lev-
els of LTG in serum of patients were evaluated by
high-performance liquid chromatography [11]. Uri-
nary and serum 8-OHdG concentrations were deter-
mined using an ELISA kit (Cayman Chemical, USA),
according to the method of Kikuchi et al. [16].
The set of parameters was completed by weight,
height, age, the type of epilepsy, the frequency of sei-
zures, magnetic resonance imaging (MRI) or com-
102 ������������� �� ����� ����� ��� �����

puter tomography (CT) and electroencephalography
(EEG) findings, duration of LTG monotherapy, level
and daily dose of LTG. The daily selenium intake (I��)
was evaluated using equation:
ISe [μg/d] = (sSe [μg/l] – 3.1)/1.62 [35].
Statistical approach
All the data were presented as the mean ± SD and
within a minimum-maximum range. Comparisons be-
tween groups were performed using either Student
t-test for parameters with normal distributions and ho-
mogenous variances, or Mann-Whitney test for un-
paired samples in all other cases and when the median
values were compared. The differences of p values <
0.05 were considered statistically significant. For sele-
nium status parameters, the Spearman rank correlation
coefficients (R�) were calculated. Statistical evaluations
were done with the commercially available package
STATISTICA PL v.10 (StatSoft, Tulsa, USA).
Results
Descriptive statistics of clinical and biochemical pa-
rameters are shown in Table 2. The only parameter
that differed between the patients and controls was
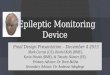
pSOD. Overall activity of pSOD was higher in the
study group compared with controls (p = 0.008; me-
dian values: 5.46 vs. 4.06 U/ml, Fig. 1). When both
groups (the study group and controls) were subdi-
vided according to sex, the difference did not reach
statistical significance. There was also no difference
in this parameter between the patients with or without
seizures in the last year and controls, as well as be-
tween overweight (n = 4, BMI > 25 kg/m�) and those
with normal BMI. The uncontrolled patients (i.e., pa-
tients with seizures) did not differ with the controlled
patients or control subjects in respect to any bio-
chemical parameter studied.
There was a significant correlation between sSe
and SelP in patients (R� = 0.438, p < 0.05).
Discussion
The patients in the present study received LTG in
monotherapy as the second or next line AED due to
intolerance or lack of efficacy of classic AEDs. Ac-
cording to the health care rules in Poland, LTG is re-
funded only in cases of drug resistance epilepsy, so its
availability to many patients is restricted. Thus, the
number of patients who fulfilled all the enrolling cri-
teria to this study was limited.
Every patient underwent a routine EEG examina-
tion in the year of the study for classification of epi-
lepsy and selection of its proper control. As none of
the patients had general tonic-clonic seizure in the
month preceding the study, the influence of this kind
of seizures on the tested parameters can be neglected.
However, as carrying out EEG examination exactly
on the day of the study was not possible for technical
reasons, we cannot exclude the influence of subclini-
cal EEG discharges on the results.
Most of the patients and controls appeared well
nourished, as 95% of patients and 100% of controls
had BMI above lower limit. They had correct liver
and renal function with normal levels of AspAT,
AlaAT and creatinine, respectively. It should be also
noted that although GPX3 activity was limited by se-
rum selenium concentration (Tab. 2), considerably
lower than required for optimal synthesis and activity
of this enzyme, the patients had no clinical evidence
of any selenium responsive disorder.
������������� �� ����� ����� ��� ����� 103
Antioxidant agents in epileptic patients�������� �� ������� �� ���
Study group Controls1
2
3
4
5
6
7
8
pS
OD
acti
vit
y[U
/ml]
Median
25%-75%
Min-Max
Fig. 1. Plasma SOD activity in study group (n = 22) and controls(n = 22) (two outlying healthy subject were excluded). Median values,25�� and 75�� centiles, minimal and maximal values were depicted.The difference between groups was evaluated by means of Mann-Whitney test, p = 0.008

SOD is a major antioxidant enzyme in the brain
[32]. In the current study we found increased level of
pSOD in LTG treated patients (Tab. 2). When we com-
pared (using Mann-Whitney test) our current results
with those previously obtained for the group of patients
(11 women and 10 men) receiving valproate monother-
apy (cf. [26], see also the whole set of corresponding
results) we found significantly higher pSOD activity in
patients treated with LTG (median value: 5.46 U/ml vs.
4.22 U/ml, p = 0.002). The patients in LTG group had
also higher UAiFRAP (median values: 121 μM Fe/l vs.
75 μM Fe/l, p = 0.043), which confirms our previous
hypothesis that VPA treatment per se induces oxidative
stress. This is manifested by lowering the levels of the
low molecular plasma antioxidants e.g., ascorbates and
tocopherols mainly responsible for changes in UAi-
FRAP values in such patients [26].
In the current study, we tested whether the 8-OHdG
levels would be useful in evaluating oxidative stress
in epileptic patients, and could discriminate between
them and healthy subjects. However, the values of 8-
OHdG did not allow distinguishing the LTG treated
epileptic patients from the controls. This suggests that
such patients are at no particular risk of oxidative
DNA damage. This could be reconciled with clinical
and epidemiological data about increased risk of ma-
lignancy, and cancer morbidity among epileptic pa-
tients treated with different medicines. The other pos-
sibility is that the rise in DNA damage can be attenu-
ated by the induction of repair systems. Of relevance
to our findings is the fact that the values of 8-OHdG
in an individual depend on a variety of other con-
founding effects (e.g., variation between different tis-
sues in rates of oxidative DNA damage and repair)
[12], which were not evaluated in the present study. It
is worth noting that 8-OHdG concentration in serum
was significantly higher in the VPA group (median
values: 3.72 vs. 2.73 pg/ml, p = 0.014) [26]. Similarly,
Schulpis et al. [31], who evaluated oxidative status in
epileptic children treated with VPA, found that pa-
tients with higher VPA serum levels had enhanced se-
rum 8-OHdG as compared with those with lower VPA
levels and healthy controls. They concluded that 8-
OHdG evaluations might be a useful procedure to fol-
low up the increased risk of degeneration processes
in patients treated with VPA. Our results indicate that
104 ������������� �� ����� ����� ��� �����
Tab. 2. The main descriptive statistics of all clinical and biochemical parameters in the study group and in healthy volunteers (data shown asthe mean values ± standard deviations)
ParameterStudy group Healthy volunteers
Unit Mean ± SD Min Max Mean ± SD Min Max p
Age year 27 ± 5 20 43 28 ± 6 21 43 NS1
BMI kg/m2 22.5 ± 2.8 16.6 28.9 24.0 ± 3.7 19.8 33.2 NS2
AspAT IU/l 24 ± 8 15 49 20 ± 4 13 31 NS2
AlaAT IU/l 23 ± 15 1 66 20 ± 11 10 58 NS2
Creatinine mg/dl 0.76 ± 0.13 0.50 1.10 0.76 ± 0.12 0.60 1.00 NS2
FRAP μM Fe/l 691 ± 100 508 878 712 ± 126 491 945 NS1
UA μM/l 294 ± 61 178 422 306 ± 66 202 452 NS1
UAiFRAP μM Fe/l 123 ± 56 33 232 124 ± 67 19 280 NS1
GPX3 U/ml 0.406 ± 0.109 0.218 0.652 0.448 ± 0.172 0.164 0.823 NS2
SelP μg/ml 4.72 ± 0.86 2.70 6.02 5.08 ± 1.14 3.39 8.13 NS2
pSOD U/ml 5.32 ± 1.24 2.82 6.95 4.05 ± 0.92 2.17 5.84 0.0082,3
8-OHdGin serum pg/ml 3.03 ± 0.99 1.82 5.43 3.10 ± 1.22 0.60 6.57 NS2
8-OHdGin urine pg/ml 29.5 ± 18.5 8.8 76.4 37.3 ± 20.1 11.2 101.0 NS1
sSe μmol/l 0.77 ± 0.16 0.40 1.05 0.84 ± 0.14 0.57 1.10 NS1
sZn μmol/l 11.7 ± 2.5 8.6 16.8 12.9 ± 4.0 8.9 25.1 NS2
� – Result of Student t-test; � – result of Mann-Whitney test, � – two outlying healthy volunteers with pSOD = 26.79 U/ml and 19.02 U/ml, respec-tively, were rejected from calculations

8-OHdG is not a useful biomarker of oxidative dam-
age of DNA or oxidant induced base modifications in
patients with LTG monotherapy.
Two selenium nutritional status parameters, sSe and
SelP correlated with each other in patients but with nei-
ther “antioxidant” parameters. Liver-derived, a sele-
nium-rich plasma SelP is mainly regarded as a sele-
nium storage and transport protein, though possessing
also detoxifying and antioxidant properties. The latter
ones are possibly by reducing phospholipid hydroper-
oxides in a glutathione peroxidase type 4 like manner
[6]. In our study, age, gender and taking LTG pills had
no effect on SelP concentration (data not shown). Lack
of influence of demographic factors on SelP is consis-
tent with results reported by Hill et al. [14].
Using the equation after Wasowicz [35], mean daily
selenium intake in LTG patients was 35.6 ± 8.0 μg/d
(the difference between LTG and VPA groups was not
significant) and the intake range was 17.4–49.1 μg/d.
This indicates that selenium status of the study group
was borderline, with some cases of mild selenium
deficiency, and concurrent large inter-individual
variation within the whole group. At present, such se-
lenium levels should be considered inadequate in rela-
tion to the Recommended Dietary Allowances for se-
lenium of 55 μg/d [15]. However, statistical analysis
for patients whose selenium status parameters (sSe,
GPX3 or SelP) were in the bottom quartile did not re-
veal any significant differences in the frequency of
seizures compared with respective top quartiles of pa-
tients. This finding indicates that typical selenium
status parameters are not directly associated with
a neuroprotective effect of selenium, at least in pa-
tients who are well or moderately well clinically con-
trolled. The protective potential of selenium in normal
brain functioning and ageing, as well as against neu-
rodegenerative disorders, e.g., excitotoxic brain dam-
age in epileptic patients, is provided by high brain Se
pool and putative involvement of selenium-containing
proteins [29]. It appears that SelP specific expression
in the brain renders it largely independent from
plasma selenium supply and bioavailability, including
contribution from circulating plasma SelP [30].
In several papers reviewed by Naziroglu [21], sele-
nium levels and blood glutathione peroxidase activi-
ties were lower in epileptic patients than in healthy
controls, although other authors did not confirm the
existence of such differences [13]. Our study provides
indirect evidence that the vital role of selenium me-
tabolism in the brain is apparently not hampered by
relatively low level of plasma indices of this element.
This obviously raises the question of which approach
for assessing selenium status should be adopted for
neuropreventive strategies and antiepileptic therapies.
Further studies are needed to address this problem.
Conclusions
We found significant increase only in pSOD activity
in the LTG treated patients compared with the con-
trols. The values of 8-OHdG did not distinguish be-
tween the LTG treated epileptic patients and the con-
trols, which suggests that such patients are at no par-
ticular risk of oxidative DNA damage.
Typical selenium status parameters (sSe, GPX3,
SelP) were not directly associated with the frequency
of seizures, at least in patients who are well or moder-
ately well clinically controlled.
Acknowledgments:
This study was partly supported by grant from Rinnekoti Research
Foundation. Dr. E. P³onka-Pó³torak has received support for her
attendance in congresses in epilepsy and neurology and speaker’s
honoraria from UCB-Pharma and Sanofi-Aventis. None of these
relations is related to the current submission. The remaining
authors confirm that there are no conflicts of interest.
References:
1. Agarwal NB, Agarwal NK, Mediratta PK, Sharma KK:
Effect of lamotrigine, oxcarbazepine and topiramate on
cognitive functions and oxidative stress in PTZ-kindled
mice. Seizure, 2011, 20, 257–262.
2. Arora T, Mehta AK, Sharma KK, Mediratta PK, Baner-
jee BD, Garg GR, Sharma AK: Effect of carbamazepine
and lamotrigine on cognitive function and oxidative
stress in brain during chemical epileptogenesis in rats.
Basic Clin Pharmacol Toxicol, 2010, 106, 372–377.
3. Ashrafi MR, Shams S, Nouri M, Mohseni M, Shabanian
R, Yekaninejad MS, Chegini N et al.: A probable causa-
tive factor for an old problem: selenium and glutathione
peroxidase appear to play important roles in epilepsy
pathogenesis. Epilepsia, 2007, 48, 1750–1755.
4. Ayçiçek A, Iºcan A: The effects of carbamazepine, val-
proic acid and phenobarbital on the oxidative and anti-
oxidative balance in epileptic children. Eur Neurol,
2007, 57, 65–69.
5. Benzie IF, Strain JJ: The ferric reducing ability of plasma
(FRAP) as a measure of “antioxidant power”: The FRAP
assay. Anal Biochem, 1996, 239, 70–76.
������������� �� ����� ����� ��� ����� 105
Antioxidant agents in epileptic patients�������� �� ������� �� ���

6. Burk RF, Hill KE: Selenoprotein P: an extracellular pro-
tein with unique physical characteristics and a role in se-
lenium homeostasis. Annu Rev Nutr, 2005, 25, 215–235.
7. Chen H, Grover S, Yu L, Walker G and Abdul Mutlib A:
Bioactivation of lamotrigine in vivo in rat and in vitro in
human liver microsomes, hepatocytes, and epidermal
keratinocytes: characterization of thioether conjugates by
liquid chromatography/mass spectrometry and high field
nuclear magnetic resonance spectroscopy. Chem Res
Toxicol, 2010, 23, 159–170.
8. Chuang YC, Chuang HY, Lin TK, Chang CC, Lu CH,
Chang WN, Chen SD et al.: Effects of long-term antiepi-
leptic drug monotherapy on vascular risk factors and
atherosclerosis. Epilepsia, 2012, 53, 120–128.
9. Commission on Classification and Terminology of the
International League Against Epilepsy. Proposal for re-
vised classification of epilepsies and epileptic syn-
dromes. Epilepsia, 1989, 30, 389–399.
10. Eren I, Nazýroðlu M, Demirdaº A: Protective effects of
lamotrigine, aripiprazole and escitalopram on
depression-induced oxidative stress in rat brain. Neuro-
chem Res, 2007, 32, 1188–1195.
11. Fraser AD. MacNeil W, Isner AF, Camfield PR: Lamo-
trigine analysis in serum by high-performance liquid
chromatography. Ther Drug Monit, 1995, 17, 174–178.
12. Halliwell B: Oxidative stress and neurodegeneration:
where are we now? J Neurochem, 2006, 97, 1634–1658.
13. Hamed SA, Abdellah MM, El-Melegy N: Blood levels
of trace elements, electrolytes, and oxidative stress/anti-
oxidant systems in epileptic patients. J Pharmacol, 2004,
96, 465–473.
14. Hill KE, Xia Y, Akesson B, Boeglin ME, Burk RF: Seleno-
protein P concentration in plasma is an index of selenium
status in selenium-deficient and selenium-supplemented
Chinese subjects. J Nutr, 1996, 126, 138–145.
15. Institute of Medicine, Food and Nutrition Board. Dietary
Reference Intakes: Vitamin C, Vitamin E, Selenium, and
Carotenoids. National Academy Press, Washington, DC,
2000, 284–324.
16. Kikuchi Y, Yasuhara T, Agari T, Kondo A, Kuramoto S,
Kameda M, Kadota T et al.: Urinary 8-OHdG elevations
in a partial lesion rat model of Parkinson’s disease corre-
late with behavioral symptoms and nigrostriatal dopamin-
ergic depletion. J Cell Physiol, 2011, 226, 1390–1398.
17. Lasoñ W, Dudra-Jastrzêbska M, Rejdak K, Czuczwar SJ:
Basic mechanisms of antiepileptic drugs and their phar-
macokinetic/pharmacodynamic interactions: an update.
Pharmacol Rep, 2011, 63, 271–292.
18. Leach MJ, Marden CM, Miller AA: Pharmacological
studies on lamotrigine, a novel potential antiepileptic
drug: II. Neurochemical studies on the mechanism of ac-
tion. Epilepsia, 1986, 27, 490–497.
19. Loft S, Paulsen HE: Cancer risk and oxidative DNA
damage in man. J Mol Med, 1996, 74, 297–312.
20. Nazýroðlu M: New molecular mechanisms on the activa-
tion of TRPM2 channels by oxidative stress and ADP-
ribose. Neurochem Res, 2007, 32, 1990–2001.
21. Nazýroðlu M: Role of selenium on calcium signaling and
oxidative stress-induced molecular pathways in epilepsy.
Neurochem Res, 2009, 34, 2181–2191.
22. Nazýroðlu M, Kutluhan S, Yilmaz M: Selenium and topi-
ramate modulates brain microsomal oxidative stress val-
ues, Ca��-ATPase activity, and EEG records in
pentylentetrazol-induced seizures in rats. J Membr Biol,
2008, 225, 39–49.
23. Messenheimer JA: Lamotrigine. Epilepsia, 1996, 36
Suppl 2, S87–S294.
24. Panayiotopoulos CP: Pharmacopoeia of prophylactic an-
tiepileptic drugs. In: The epilepsies: seizures, syndromes
and management. Bladon Medical Publishing, Oxford-
shire (UK), 2005, 504–506.
25. Pavone A, Cardile V: An in vitro study of new antiepi-
leptic drugs and astrocytes. Epilepsia, 2003, 44, 34–39.
26. P³onka-Pó³torak E, Zagrodzki P, Ch³opicka J, Bartoñ H,
Westermarck T, Kaipainen P, Kaski M, Atroshi F: Val-
proic acid modulates superoxide dismutase, uric acid-
independent FRAP and zinc in blood of adult epileptic
patients. Biol Trace Elem Res, 2011, 143, 1424–1434.
27. Poolos NP, Migliore M, Johnston D: Pharmacological
upregulation of h-channels reduces the excitability of py-
ramidal neuron dendrites. Nat Neurosci, 2002, 5, 767–774.
28. Ramaekers VT, Calomme M, Vanden Berghe D, Makro-
poulos W: Selenium deficiency triggering intractable sei-
zures. Neuropediatrics, 1994, 25, 217–223.
29. Savaskan NE, Bräuer AU, Kühbacher M, Eyüpoglu IY,
Kyriakopoulos A, Ninnemann O, Behne D, Nitsch R:
Selenium deficiency increases susceptibility to
glutamate-induced excitotoxicity. FASEB J, 2003, 17,
112–114.
30. Scharpf M, Schweizer U, Arzberger T, Roggendorf W,
Schomburg L, Köhrle J: Neuronal and ependymal ex-
pression of selenoprotein P in the human brain. J Neural
Transm, 2007, 114, 877–884.
31. Schulpis KH, Lazaropoulou C, Regoutas S, Karikas GA,
Margeli A, Tsakiris S, Papassotiriou I: Valproic acid
monotherapy induces DNA oxidative damage. Toxicol-
ogy, 2006, 217, 228–232.
32. Sudha K, Rao AV, Rao A: Oxidative stress and anti-
oxidants in epilepsy. Clin Chim Acta, 2001, 303, 19–24.
33. Tatum WO, French JA: Lamotrigine and side effects:
Another headache. Neurology, 2012, 78, 849–850.
34. Torbati D, Church DF, Keller JM, Pryor WA: Free radical
generation in the brain precedes hyperbaric oxygen induced
convulsions. Free Radic Biol Med, 1992, 13, 101–106.
35. Wasowicz W: Selenium in eastern European countries.
Poland as an example. In: Proceedings of the fifth interna-
tional symposium on uses of selenium and tellurium. Eds.
Carapella SC, Oldfield JE, Palmieri Y, Brussels, 1994,
163–170.
36. Weber GF, Maertens P, Meng X, Pippenger CE: Glu-
tathione peroxidase deficiency and childhood seizures.
Lancet, 1991, 337, 1443–1444.
37. Zecca L, Youdim MB, Riederer P, Connor JR, Crichton
RR: Iron, brain ageing and neurodegenerative disorders.
Nat Rev Neurosci, 2004, 5, 863–873.
Received: June 2, 2012; in the revised form: August 14, 2012;
accepted: September 25, 2012.
106 ������������� �� ����� ����� ��� �����