Embed Size (px)
Citation preview

Pharmacology, Biochemistry and Behavior 124 (2014) 396–404
Contents lists available at ScienceDirect
Pharmacology, Biochemistry and Behavior
j ourna l homepage: www.e lsev ie r .com/ locate /pharmbiochembeh
Antinociceptive effect of3-(4-fluorophenyl)-5-trifluoromethyl-1H-1-tosylpyrazole.A Celecoxib structural analog in models of pathological pain
Sara Marchesan Oliveira a,b,⁎, Cássia Regina Silva a,1, Alexandre Pereira Wentz c,2, Gisele R. Paim c,2,Michele S. Correa c,2, Hélio G. Bonacorso c,2, Arthur S. Prudente d,3, Michel Fleith Otuki e,4, Juliano Ferreira a,f,1,5
a Laboratório de Neurotoxicidade e Psicofarmacologia, Programa de Pós-graduação em Ciências Biológicas: Bioquímica Toxicológica, Universidade Federal de Santa Maria,Santa Maria, RS 97.105-900, Brazilb Departamento de Bioquímica e Biologia Molecular, Universidade Federal de Santa Maria, Santa Maria, RS 97.105-900, Brazilc Núcleo de Química de Heterociclos (NUQUIMHE), Departamento de Química, Universidade Federal de Santa Maria, Santa Maria, RS 97.105-900, Brazild Departamento de Farmacologia, Universidade Federal do Paraná, Curitiba, PR, Brazile Departamento de Ciências Farmacêuticas, Universidade Estadual de Ponta Grossa, Ponta Grossa, PR, Brazilf Departamento de Farmacologia, Universidade Federal de Santa Catarina, Florianópolis, SC, Brazil
⁎ Corresponding author at: Programa de Pós-graduBioquímica Toxicológica, Centro de Ciências NatuFederal de Santa Maria, Cidade Universitária, CamoRS, Brazil. Tel.: +55 55 3220 8053; fax: +55 55 3220
E-mail address: [email protected] (S.M. Ol1 Tel.: +55 55 3220 8053; fax: +55 55 3220 8756.2 Tel.: +55 55 3220 8870; fax: +55 55 3220 8756.3 Tel.: +55 41 3361 1538; fax: +55 41 3266 2042.4 Tel.: +55 42 3220 3120; fax: +55 42 3220 3247.5 Tel.: +55 48 3721 9491; fax: +55 48 3337 5479.
http://dx.doi.org/10.1016/j.pbb.2014.07.0050091-3057/© 2014 Elsevier Inc. All rights reserved.
a b s t r a c t
a r t i c l e i n f oArticle history:Received 24 March 2014Received in revised form 11 June 2014Accepted 6 July 2014Available online 16 July 2014
Keywords:AntinociceptionArthritisHyperalgesiaNeuropathyPyrazoleSurgery
Pain is the most common complaint in the medical field and the identification of novel compounds that caneffectively treat painful states without causing side effects remains a major challenge in biomedical research.The aim of the present study is to investigate the antinociceptive effect of 3-(4-fluorophenyl)-5-trifluoromethyl-1H-1-tosylpyrazole (FTosPz) inmodels of pathological pain inmice and compare these effectswith those producedby Celecoxib. FTosPz (100–500 μmol/kg) or Celecoxib (26–260 μmol/kg)was administrated orally. The administra-tion of either FTosPz or Celecoxib reduced the hyperalgesia but not the edema or leukocyte infiltration that wascaused by Complete Freund's Adjuvant (CFA), used as an arthritis model. Oral administration of both FTosPz andCelecoxib also attenuated the postoperative hyperalgesia as well as the hyperalgesia caused by partial sciaticnerve ligation, used as a neuropathic pain model. FTosPz and Celecoxib produced antinociceptive effects withoutaltering the locomotor activity of animals. Furthermore, FTosPz neither altered AST/ALT enzyme activity nor theurea/creatinine levels. Still, the FTosPz did not alter the COX-1 and COX-2 enzyme activities. Thus, FTosPz is aninteresting prototype for the development of novel analgesic drugs.
ação em Ciências Biológicas:rais e Exatas, Universidadebi, 97105-900, Santa Maria,8756.iveira).
© 2014 Elsevier Inc. All rights reserved.
1. Introduction
Pain is themost common complaint in themedical field, dominatingand disrupting the quality of life of many patients. However, the arsenalof effective and safe analgesics is still relatively small (Williams et al.,1999;Woller and Hook, 2013).Many of the currently available pharma-cological treatments to alleviate pain (especially nonsteroidal anti-inflammatory drugs and opioids) are only partially effective and maybe accompanied by distressing side effects or have abuse potential(Chan, 2006; Graziottin et al., 2011; Scholz and Woolf, 2002).
Mechanical hyperalgesia is an increased pain sensitivity which canbe produced by mechanical stimuli and is characteristic of pathologicalpain. Both joint inflammation and surgical procedures are importantcauses of pathological inflammatory pain sensitivity to mechanicalstimulus. In arthritis, the joint nerves become sensitized, producingacute and chronic pain (von Banchet et al., 2007). The current therapiesto alleviate joint pain have limited effectiveness and certain drugs pro-duce unwanted negative side effects, thereby precluding their long-term use (McDougall, 2006). Moreover, in postoperative pain, approxi-mately half of all patients experience moderate to severe pain after sur-gery (Pogatzki-Zahn et al., 2007) and the treatments used to treat itcause side effects that often limit their use (Mercadante, 1999). In addi-tion, the pain related with the injury to peripheral nerves often resultsin a persistent neuropathic pain (Malmberg and Basbaum, 1998;Woolf and Mannion, 1999). Neuropathic pain is a major challenge inclinical medicine because it is largely resistant to the currently availableanalgesics (Dworkin et al., 2007; Woolf and Mannion, 1999). The iden-tification of compounds that can more effectively and safely treat bothacute and chronic pain states and, additionally, show a reduced
Fig. 1.Molecular structures of FTosPz and Celecoxib.
397S.M. Oliveira et al. / Pharmacology, Biochemistry and Behavior 124 (2014) 396–404
tendency to cause the side effects associated thereof, remains a majorunmet challenge in biomedical research.
In this context, pyrazole and its derivatives bearing a diversity offunctional groups have attracted a great deal of interest due to theirwide range of pharmacological properties (Bekhit and Abdel-Azien,2004; Cheng et al., 1986), mainly antinociceptive activities (Gürsoyet al., 2000; Matheus et al., 1991; Ochi and Goto, 2000). In recentyears, we have synthesized new pyrazole derivatives and reportedtheir antinociceptive and antipyretic effects in animal models of inflam-mation, fever, and pain (Milano et al., 2008a, 2008b; Milano et al.,2008a; Prokopp et al., 2006; Sauzem et al., 2007; Souza et al., 2001;Tomazetti et al., 2005). We have previously demonstrated that 3-(4-fluorophenyl)-5-trifluoromethyl-1H-1-tosylpyrazole (FTosPz) reducedthe inflammatory pain induced by carrageenan and the visceralnociception induced by acetic acid. Furthermore, FTosPz causes neithermotor impairment nor gastric ulcer or hypothermia in animals(Oliveira et al., 2009). However, the pain models used to evaluatethe antinociceptive effect of FTosPz have been considered not clinicallyrelevant.
Taking this into account, the purpose of the present study was toinvestigate the effects of FTosPz in three pathological pain models thatafflict millions of people worldwide. These models are the arthriticpain caused by CFA, the postoperative pain induced by surgical incision,and the neuropathic pain induced by partial ligation of the right sciaticnerve.
2. Materials and methods
2.1. Animals
Male Swiss mice (25–35 g) were kept in a temperature-controlledroom (22 ± 2 °C) under a 12 h light–dark cycle (lights on from6:00 a.m. to 6 p.m.) with standard lab chow and tap water ad libitum.Animalswere acclimatized to the laboratory for at least 2 h before the ex-periments and were used only once. All of the experiments were carriedout between 8:00 a.m. and 5:00 p.m. The data reported in this studywere carried out in accordancewith current ethical guidelines for the in-vestigation of experimental pain in conscious animals (Zimmermann,1983) and were approved by the Ethics Committee of the FederalUniversity of Santa Maria (30/2009). The number of animals andintensities of noxious stimuli used were the minimum necessary todemonstrate the consistent effects of the drug treatments.
2.2. Drugs
The compound 3-(4-fluorophenyl)-5-trifluoromethyl-1H-1-tosylpyrazole (FTosPz, Fig. 1),was synthesized according to the literaturepreviously described by Bonacorso et al. (2006). Both the analytical andspectral data (1H and 13C NMR) of FTosPz are in full agreement with theassigned structure. Celecoxib (26–260 μmol/kg), a 3-trifluoromethyl-substituted pyrazole (Fig. 1) (Sigma Chemical Co., St. Louis, MO, USA),was used as a positive control. Both compounds (Fig. 1) were dilutedin dimethyl sulfoxide (DMSO) (10%), tween 80 (10%) and saline(0.9% NaCl, 80%) and were administered orally (10 ml/kg) by gavage(p.o.) in all in vivo experiments. The FTosPz (100–500 μmol/kg) wasadministered at the maximal possible dose in accordance with theirsolubility in vehicle and the doses of FTosPz and Celecoxibwere chosenbased on previous experiments (Oliveira et al., 2009). CompleteFreund's Adjuvant (CFA) (1 mg/ml of heat killed Mycobacteriumtuberculosis in 85% paraffin oil and 15% mannide monooleate) and allother reagents used in the experiments were obtained from Sigma(St. Louis, MO, USA). Enzyme-linked immunosorbent assay (ELISA)kits were purchased from R&D Systems Inc. (USA) and the COX(ovine) inhibitor screening assay kit was obtained from CaymanChemical Co. (USA).
2.3. Assessment of hyperalgesia
The measurement of mechanical paw withdrawal threshold wascarried out using the Up-and-Down paradigm as described previouslyby Chaplan et al. (1994), with minor modifications (Oliveira et al.,2011). The 50%mechanical paw withdrawal threshold (PWT) responsewas then calculated from the resulting scores as described previously byDixon (1980). The PWTwas expressed in grams (g) and was evaluatedseveral times before and after treatments or surgical procedures. Asignificant decrease in PWT compared to the baseline values wasconsidered as mechanical hyperalgesia.
2.4. Model of incisional pain
The incisional pain model was carried out as previously described(Oliveira et al., 2011). The animals were pretreated (0.5 h beforeincision) or post-treated (0.5 h after incision) with FTosPz, Celecoxib orvehicle and the mechanical hyperalgesia was measured from 0.5 up to6.0 h after the administration of compounds.
2.5. Model of arthritic pain
2.5.1. Induction of inflammation and hyperalgesia assessmentThe acute (early) and chronic (later) inflammatory responses caused
by CFA were assessed according to Ferreira et al. (2001). The acute re-sponse was assessed after the administration of CFA (starting at30 min), while the chronic response was evaluated only 48 h after theadministration of CFA, as describedbelow. Briefly,malemicewere light-ly anesthetized with 2% halothane via a nose cone and received a 20 μlsubcutaneous injection of CFA (1 mg/ml of heat killed M. tuberculosisin paraffin oil (85%) and mannide monoleate (15%)) on the plantarsurface (intraplantar, i.pl.) of the right hind paw. To evaluate earlyresponse, the mice were submitted to FTosPz, Celecoxib or vehicle ad-ministration 0.5 h before the administration of CFA and the hyperalgesiawas measured from 1.0 up to 6.5 h after the administration of the com-pounds. However, a later inflammatory response was observed 48 hafter CFA administration, where the hyperalgesia was measured intime 0 (B2; 48 h after CFA) before the administration of drugs andimmediately after the mice were treated with FTosPz, Celecoxib orvehicle. The hyperalgesia was measured from 1.0 up to 24 h after itsadministration.

398 S.M. Oliveira et al. / Pharmacology, Biochemistry and Behavior 124 (2014) 396–404
2.5.2. Edema assessmentBesides mechanical hyperalgesia, we also evaluated paw edema
development after CFA injection in the plantar tissue using a caliper(used to measure the thickness of the paw). The effect of the drugs onthe paw edema produced by CFA was assessed from 2.0 up to 3.5 h or1 up to 24h after the administration of drugs to the early or later inflam-matory response, respectively. Paw edema was expressed as theincrease in paw thickness (mm) in comparison to the baselinemeasure(Oliveira et al., 2009).
2.5.3. Assessment of leukocyte infiltration
2.5.3.1. Measurement of myeloperoxidase (MPO) and N-acetyl-β-D-glucosaminidase (NAGase) activities. To investigate the involvementof neutrophil and mononuclear cell infiltration in the inflammatoryresponse caused by CFA, we measured the MPO and NAGase enzymeactivities as previously described by Suzuki et al. (1983) and Lloretand Moreno (1995), respectively.
Forty eight hours after CFA injection in the paw and 2 h after theadministration of FTosPz, Celecoxib or vehicle, separate groups of micewere sacrificed by cervical dislocation and the plantar surface of thehind paw was harvested to determine MPO and NAGase activities.Samples were homogenized in acetate buffer (80 mM, pH 5.4) contain-ing 0.5% hexadecyltrimethylammonium bromide and kept at 4 °C.Immediately before the assay, the tissue homogenate was centrifugedat 11,000 ×g for 20 min and the supernatant was then collected forassay.
To determine the MPO enzyme activity, 10 μl of supernatantwas incubated with 200 μl of acetate buffer and 40 μl of 3,3′,5,5′-tetramethylbenzidine solution (18.4 mM) for 3 min at 37 °C. The reac-tion was stopped on ice by addiction of 30 μl acetic acid. The colorformed was analyzed by a spectrophotometer at 630 nm. Otherwise,in order to determine NAGase activity, 25 μl of supernatant was mixedwith sodium citrate buffer (50 mM, pH 4.5) and 25 μl of p-nitrofenil-2-acetamide-β-D-glucopyranoside (NAG 2.25 nM) and incubated for60 min at 37 °C. After this time, the reaction was stopped on ice byaddition of 100 μl glycine buffer (0.2 μM, pH 10.4). The color formedwas analyzed by a spectrophotometer at 405 nm. Both reactions wereread on a Fisher Biotech Microkinetics BT 2000 microplate reader.Values were expressed as optical densities and corrected by homoge-nized tissue grams (g).
2.5.3.2. Histology. Separate groups of mice were used to verify the histo-logical changes in mouse paw 48 h after the induction of inflammationby CFA and 2 h after administration of FTosPz, Celecoxib or vehicle; micewere euthanized by cervical dislocation and the plantar surface of thehind paw was removed and fixed in an alfac solution (16:2:1 mixtureof ethanol 80%, formaldehyde 40% and acetic acid). Each samplewas embedded in paraffin wax, sectioned at 5 μm and stained withhematoxylin–eosin. A representative area was selected for qualitativelight microscopic analysis of the inflammatory cellular response with a40× objective (Oliveira et al., 2011). To minimize a source of bias, theinvestigator did not know the group that they were analyzing.
2.6. Cyclooxygenase-1 and cyclooxygenase-2 activities in vitro
To investigate a possible mechanism of action of FTosPz, we verifiedwhether it was able to alter COX-1 and COX-2 enzyme activities. For theassay, a COX screening assay kit (Kit No. 560101, Cayman) was used ac-cording to the manufacturer's instructions and as previously described(Pasin et al., 2010) and the dose of FTosPz was chosen from pilot exper-iments. The results are reported as a percent inhibition of COX-1 andCOX-2 enzymes.
2.7. Model of neuropathic pain
For the induction of neuropathy, themicewere first anesthetized byintraperitoneal injection of 90 mg/kg of ketamine plus 3 mg/kg ofxylazine hydro-chloride. Then, a partial ligation of the right sciaticnerve was made by tying one-third to one-half of the dorsal portion ofthe sciatic nerve, as previously described (Malmberg and Basbaum,1998; Villarinho et al., 2012). In sham-operated mice, the nerve wasexposed without ligation. Seven days after the surgical procedure themechanical sensitivity was measured to confirm the development ofhyperalgesia. Then, mice were treated with FTosPz, Celecoxib or vehicleand mechanical sensitivity was assessed 0.5, 1, 2, 4, and 6 h aftertreatment.
2.8. Evaluation of locomotor activity
To evaluate the possible nonspecific muscle-relaxant or sedativeeffects we examined the locomotor activity of the animals by usingthe open-field test as previously reported by Trevisan et al. (2012).The apparatus consisted of a wooden box measuring 40 × 60 × 50 cmwherein the floor of the arena was divided into 12 equal squares.The mice were treated with FTosPz (500 μmol/kg, p.o.), Celecoxib(260 μmol/kg, p.o.) or vehicle (10 ml/kg, p.o.) and the number ofareas crossed and the number of rearings with all paws were recordedfor 5 min at 1 h after treatments.
2.9. Biochemical markers of toxicity
We also evaluated the activities of alanine aminotransferase(ALT), aspartate aminotransferase (AST), and the urea and creat-inine levels, which are sensitive indicators of liver and kidneyinjury, respectively. To biochemically evaluate the occurrenceof liver or kidney toxicity, the animals were treated with FTosPz(500 μmol/kg, p.o.), Celecoxib (260 μmol/kg, p.o.) or vehicle(10 ml/kg, p.o.) and 1 h after treatment they were euthanized.The activities of ALT and AST, and the urea and creatinineserum levels were assessed spectrophotometrically usingLabtest® kits according to the manufacturer's specifications(Labtest Diagnostica, Brazil).
2.10. Statistical analyses
The results are expressed as means ± standard error of the mean(S.E.M.), except for the ID50 values (i.e., the FTosPz or Celecoxib dosethat reduces nociceptive responses to the order of 50% relative to thecontrol value),whichwere expressed as geometricmeans accompaniedby their respective 95% confidence limits. Statistical analyses werecarried out using GraphPad Prism 5.0 software. The significance of thedifferences between the groups was evaluated with one-way analysisof variance (ANOVA) followed by a Student–Newman–Keuls test or atwo-way analysis of variance followed by Bonferroni's post hoc testwhen appropriate. P values less than 0.05 (P b 0.05) were consideredas indicative of significance and F values are presented in the text onlywhen P b 0.05.
3. Results
3.1. Effects of FTosPz or Celecoxib on the incisional pain model
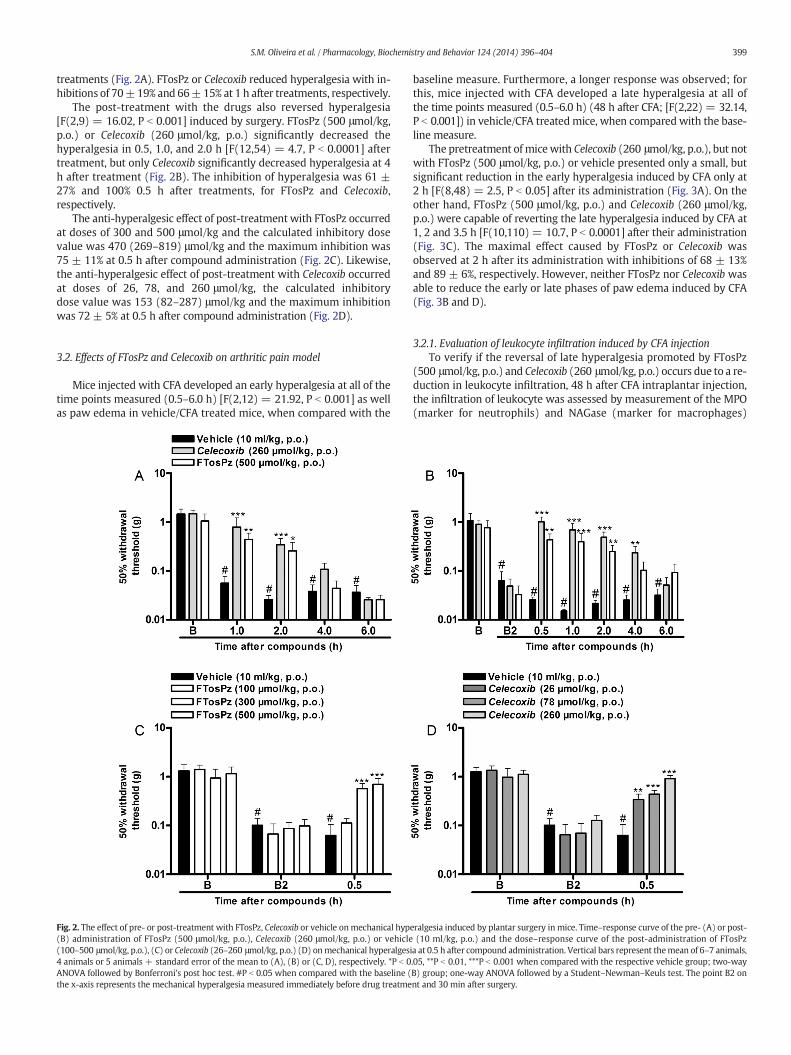
In this model, we evaluated the preemptive and curativeantinociceptive effects of FTosPz and Celecoxib in the postoperativepain model. The plantar incision produced a marked hyperalgesia inthe injured paw at all of the time points measured (0.5–6 h) in vehicletreated mice when compared with the baseline (B) [F(2,16) = 32.93,P b 0.001]. The pretreatment with FTosPz or Celecoxib significantlydecreased hyperalgesia at 1 and 2 h [F(8,64) = 3.6, P b 0.01] after the
399S.M. Oliveira et al. / Pharmacology, Biochemistry and Behavior 124 (2014) 396–404
treatments (Fig. 2A). FTosPz or Celecoxib reduced hyperalgesia with in-hibitions of 70±19% and 66±15% at 1 h after treatments, respectively.
The post-treatment with the drugs also reversed hyperalgesia[F(2,9) = 16.02, P b 0.001] induced by surgery. FTosPz (500 μmol/kg,p.o.) or Celecoxib (260 μmol/kg, p.o.) significantly decreased thehyperalgesia in 0.5, 1.0, and 2.0 h [F(12,54) = 4.7, P b 0.0001] aftertreatment, but only Celecoxib significantly decreased hyperalgesia at 4h after treatment (Fig. 2B). The inhibition of hyperalgesia was 61 ±27% and 100% 0.5 h after treatments, for FTosPz and Celecoxib,respectively.
The anti-hyperalgesic effect of post-treatment with FTosPz occurredat doses of 300 and 500 μmol/kg and the calculated inhibitory dosevalue was 470 (269–819) μmol/kg and the maximum inhibition was75 ± 11% at 0.5 h after compound administration (Fig. 2C). Likewise,the anti-hyperalgesic effect of post-treatment with Celecoxib occurredat doses of 26, 78, and 260 μmol/kg, the calculated inhibitorydose value was 153 (82–287) μmol/kg and the maximum inhibitionwas 72 ± 5% at 0.5 h after compound administration (Fig. 2D).
3.2. Effects of FTosPz and Celecoxib on arthritic pain model
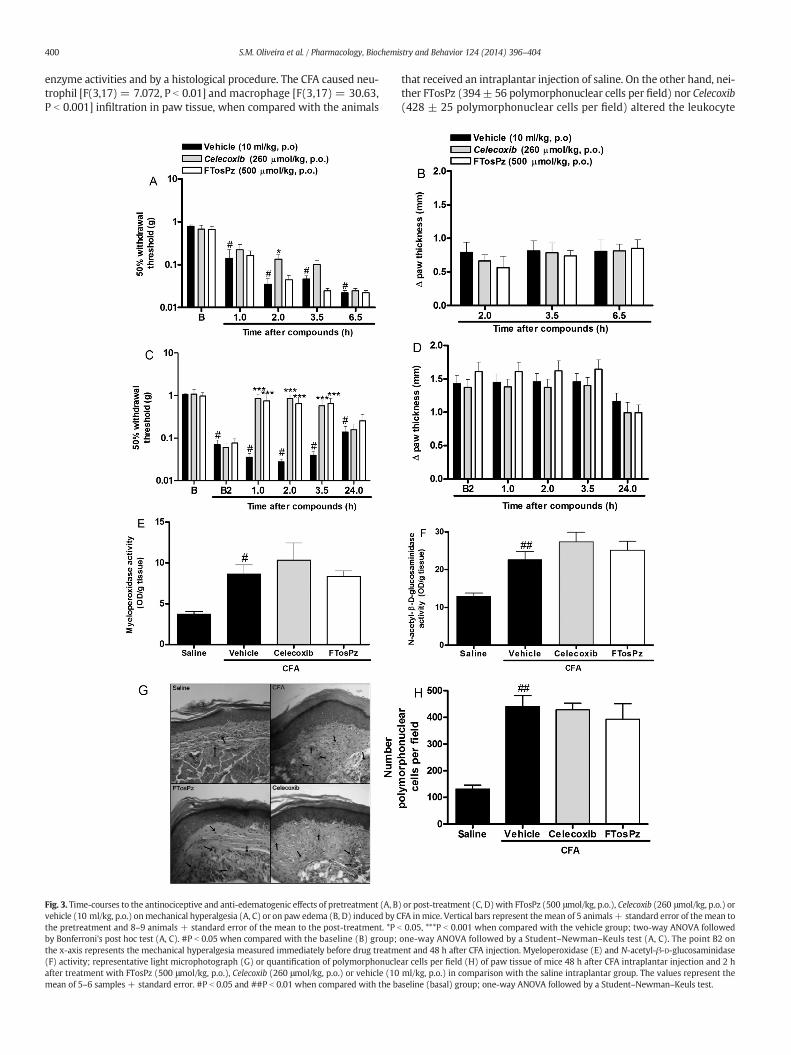
Mice injected with CFA developed an early hyperalgesia at all of thetime points measured (0.5–6.0 h) [F(2,12) = 21.92, P b 0.001] as wellas paw edema in vehicle/CFA treated mice, when compared with the
Fig. 2. The effect of pre- or post-treatment with FTosPz, Celecoxib or vehicle onmechanical hyp(B) administration of FTosPz (500 μmol/kg, p.o.), Celecoxib (260 μmol/kg, p.o.) or vehicle(100–500 μmol/kg, p.o.), (C) or Celecoxib (26–260 μmol/kg, p.o.) (D) onmechanical hyperalges4 animals or 5 animals + standard error of the mean to (A), (B) or (C, D), respectively. *P b 0ANOVA followed by Bonferroni's post hoc test. #P b 0.05 when compared with the baseline (the x-axis represents the mechanical hyperalgesia measured immediately before drug treatme
baseline measure. Furthermore, a longer response was observed; forthis, mice injected with CFA developed a late hyperalgesia at all ofthe time points measured (0.5–6.0 h) (48 h after CFA; [F(2,22) = 32.14,P b 0.001]) in vehicle/CFA treatedmice, when compared with the base-line measure.
The pretreatment of micewith Celecoxib (260 μmol/kg, p.o.), but notwith FTosPz (500 μmol/kg, p.o.) or vehicle presented only a small, butsignificant reduction in the early hyperalgesia induced by CFA only at2 h [F(8,48) = 2.5, P b 0.05] after its administration (Fig. 3A). On theother hand, FTosPz (500 μmol/kg, p.o.) and Celecoxib (260 μmol/kg,p.o.) were capable of reverting the late hyperalgesia induced by CFA at1, 2 and 3.5 h [F(10,110) = 10.7, P b 0.0001] after their administration(Fig. 3C). The maximal effect caused by FTosPz or Celecoxib wasobserved at 2 h after its administration with inhibitions of 68 ± 13%and 89 ± 6%, respectively. However, neither FTosPz nor Celecoxib wasable to reduce the early or late phases of paw edema induced by CFA(Fig. 3B and D).
3.2.1. Evaluation of leukocyte infiltration induced by CFA injectionTo verify if the reversal of late hyperalgesia promoted by FTosPz
(500 μmol/kg, p.o.) and Celecoxib (260 μmol/kg, p.o.) occurs due to a re-duction in leukocyte infiltration, 48 h after CFA intraplantar injection,the infiltration of leukocyte was assessed by measurement of the MPO(marker for neutrophils) and NAGase (marker for macrophages)
eralgesia induced by plantar surgery in mice. Time–response curve of the pre- (A) or post-(10 ml/kg, p.o.) and the dose–response curve of the post-administration of FTosPz
ia at 0.5 h after compound administration. Vertical bars represent themean of 6–7 animals,.05, **P b 0.01, ***P b 0.001 when compared with the respective vehicle group; two-wayB) group; one-way ANOVA followed by a Student–Newman–Keuls test. The point B2 onnt and 30 min after surgery.
400 S.M. Oliveira et al. / Pharmacology, Biochemistry and Behavior 124 (2014) 396–404
enzyme activities and by a histological procedure. The CFA caused neu-trophil [F(3,17) = 7.072, P b 0.01] and macrophage [F(3,17) = 30.63,P b 0.001] infiltration in paw tissue, when compared with the animals
Fig. 3. Time-courses to the antinociceptive and anti-edematogenic effects of pretreatment (A, Bvehicle (10 ml/kg, p.o.) onmechanical hyperalgesia (A, C) or on paw edema (B, D) induced by Cthe pretreatment and 8–9 animals + standard error of the mean to the post-treatment. *P b
by Bonferroni's post hoc test (A, C). #P b 0.05 when compared with the baseline (B) group;the x-axis represents the mechanical hyperalgesia measured immediately before drug treatm(F) activity; representative light microphotograph (G) or quantification of polymorphonucleafter treatment with FTosPz (500 μmol/kg, p.o.), Celecoxib (260 μmol/kg, p.o.) or vehicle (10mean of 5–6 samples + standard error. #P b 0.05 and ##P b 0.01 when compared with the b
that received an intraplantar injection of saline. On the other hand, nei-ther FTosPz (394± 56 polymorphonuclear cells per field) nor Celecoxib(428 ± 25 polymorphonuclear cells per field) altered the leukocyte
) or post-treatment (C, D)with FTosPz (500 μmol/kg, p.o.), Celecoxib (260 μmol/kg, p.o.) orFA inmice. Vertical bars represent themean of 5 animals+ standard error of themean to0.05, ***P b 0.001 when compared with the vehicle group; two-way ANOVA followed
one-way ANOVA followed by a Student–Newman–Keuls test (A, C). The point B2 onent and 48 h after CFA injection. Myeloperoxidase (E) and N-acetyl-β-D-glucosaminidasear cells per field (H) of paw tissue of mice 48 h after CFA intraplantar injection and 2 hml/kg, p.o.) in comparison with the saline intraplantar group. The values represent theaseline (basal) group; one-way ANOVA followed by a Student–Newman–Keuls test.

401S.M. Oliveira et al. / Pharmacology, Biochemistry and Behavior 124 (2014) 396–404
infiltration that was caused by CFA (440± 41 polymorphonuclear cellsper field) when compared to the saline group (132 ± 14 polymorpho-nuclear cells per field) (Fig. 3E, F, G and H).
3.3. Effects of FTosPz or Celecoxib on the neuropathic pain model
Mechanical nociceptive thresholds were stable before and afterthe sham procedure in all of the groups [F(12,90) = 0.8, P = 0.61](Fig. 4A). Partial sciatic nerve ligation produced a significant decreasein the mechanical sensitivity average 7 days after surgery when com-pared with the mean baseline mechanical sensitivity, characterizingthe development of neuropathic pain [F(2,23) = 8.313, P b 0.001](Fig. 4B). The mechanical hyperalgesia produced by nerve injurypersisted throughout the experiment period in the saline treated mice,but it was reverted by FTosPz (500 μmol/kg, p.o.) and Celecoxib(260 μmol/kg, p.o.) at 1 and 2 h [F(12,144) = 2.5, P b 0.01] aftertreatment (Fig. 4B). The inhibitions of hyperalgesia were 73 ±12% and 92 ± 13% at 2 h after treatments, for FTosPz and Celecoxib,respectively.
3.4. Effects of FTosPz and Celecoxib on COX activity
Since the FTosPz has a molecular structure similar to the structureof Celecoxib (a selective COX-2 inhibitor) and both have similarantinociceptive effects, we tested the possible action of FTosPz on theactivity of the enzymes COX-1 and COX-2. We verified that FTosPz(5 μM) had an effect neither on COX-1 activity (0% of inhibition) noron COX-2 activity (0% of inhibition). On the other hand, Celecoxib(0.001 μM) was used as an internal standard in the assay inhibitedCOX-2 activity by 94% but did not inhibit COX-1 activity (0% ofinhibition).
3.5. Assessment of the side effects of drugs on the locomotor andbiochemical parameters
The treatment of animals with FTosPz (500 μmol/kg, p.o.) orCelecoxib (260 μmol/kg, p.o.) did not alter its locomotor activities com-paredwith the vehicle treated animals, as evaluated by the total numberof both crossings and rearings in the open-field test (Table 1). Still,FTosPz (500 μmol/kg, p.o.) or Celecoxib (260 μmol/kg, p.o.) caused nochanges in the serum AST or ALT enzyme activities, or in the creatinineor urea concentrationswhen comparedwith the vehicle treated animals(Table 1).
Fig. 4. Effects of FTosPz (500 μmol/kg, p.o.), Celecoxib (260 μmol/kg, p.o.) or vehicle (10 ml/kg(A) Time-course curve of pawwithdrawal threshold in sham-operatedmice. (B) Time-course cbars represent themean of 6 animals + standard error of themean to the sham-operatedmicemice. *P b 0.05, **P b 0.01, ***P b 0.001 when compared with the respective vehicle group; twbaseline (B) group; one-way ANOVA followed by a Student–Newman–Keuls test. The point B2treatment.
4. Discussion
Pathological painful states are difficult to treat and pain is the mostcommon complaint in the medical field; it produces severe distress formany patients, dominating and disrupting the quality of their lives(Kloppenburg and Kwok, 2011; Woller and Hook, 2013). However,the arsenal of effective and safe analgesics is still relatively small(Scholz and Woolf, 2002; Williams et al., 1999). Despite the grantadvances in the last decade, the discovery and development of a safe,effective, and economical therapy for treating pain conditions still pre-sents a major challenge. In this scenario, different tools have beenused to study different pathological pain states. One of them is the useof the Complete Freund's Adjuvant used to induce a chronic inflamma-tory condition in rodents. This model is used as a laboratory model inthe study of arthritic pain once M. tuberculosis produces arthritis inhumans (Hogan, 2002; Nagakura et al., 2003). Previous studies demon-strated that classical NSAIDs or selective COX-2 inhibitors reduce thedevelopment of hyperalgesia induced by the injection of adjuvantarthritis in rats and mice (Attal et al., 1988; Ochi and Goto, 2000;Vardeh et al., 2009); furthermore, Celecoxib is effective in reducingarthritic pain in humans (Essex et al., 2012; McCormack, 2011). The lit-erature data showed that 5-trifluoromethyl and 4-trifluoromethyl-substituted pyrazoles are able to inhibit mechanical allodynia and theseverity of collagen and collagen antibody-induced arthritis in mice,respectively (Chiba et al., 2012; Milano et al., 2008a, 2008b). Likethese compounds, FTosPz also contains in its molecular structure thetrifluoromethyl group attached at the C-5 position of the pyrazolering, and this fact makes it an important biological agent for the treat-ment of arthritic pain. According to such evidence, we demonstratedin the current study that the acute oral administration of FTosPz waseffective and reverses the late persistent inflammatory hyperalgesiacaused by intraplantar CFA injection in mice. This result reinforces thefact that the presence of the trifluoromethyl substituent group is of fun-damental importance for the analgesic activity of FTosPz in this painmodel. Furthermore, the ability of FTosPz to reverse mechanicalhyperalgesia caused by CFA is clinically relevant since patients seekmedical care for the treatment of painful symptoms after they start.Consequently, analgesic agents that are capable of reversing arthriticpain are most important than agents that prevent it. Despite FTosPz re-ducing mechanical hyperalgesia, it was not able to reduce the edemaformation induced by early or late CFA injection.
We demonstrated that, similar to FTosPz, Celecoxib was able toprevent and revert the development of hyperalgesia induced byCFA injection, without altering the edema. These data are in goodagreement with the results previously described by Milano et al.(2008a) and Sauzem et al. (2009) whose studies demonstrated that
, p.o.) treatment on mechanical nociceptive threshold in a mice neuropathic pain model.urve of pawwithdrawal threshold in partial sciatic nerve ligation submittedmice. Verticaland 9 animals+ standard error of themean to the partial sciatic nerve ligation submittedo-way ANOVA followed by Bonferroni's post hoc test. #P b 0.05 when compared with theon the x-axis represents the mechanical hyperalgesia measured immediately before drug

Table 1Effect of FTosPz (500 μmol/kg, p.o.), Celecoxib (260 μmol/kg, p.o.) or vehicle (10 ml/kg, p.o.) on spontaneous (open-field test) locomotor activity and on biochemical parameters in mice1 h after treatments.
Treatment Motor function Biochemical parameters
Crossing (n.) Rearing (n.) AST (U/L) ALT (U/l) Urea (mg/dl) Creatinine (mg/dl)
Vehicle (10 ml/kg) 64.1 ± 7.6 45.7 ± 4.2 62.4 ± 5.67 54.7 ± 6.8 71.6 ± 3.8 0.58 ± 0.12FTosPz (500 umol/kg, p.o.) 79.4 ± 4.6 46.2 ± 6.7 72.2 ± 4.3 54.4 ± 6.7 61.2 ± 3.1 0.44 ± 0.06Celecoxib (260 umol/kg, p.o.) 76.3 ± 3.8 52.6 ± 3.4 70.6 ± 9.1 58.9 ± 5.6 70.3 ± 1.9 0.32 ± 0.07
Significant differences were not observed between most groups (one-way ANOVA followed by Dunnett's test). Data represent the mean ± S.E.M. of 6–8 animals.
402 S.M. Oliveira et al. / Pharmacology, Biochemistry and Behavior 124 (2014) 396–404
5-trifluoromethyl-substituted pyrazole reverted the hyperalgesia in-duced by CFA injection in mice and rats without altering the edema.Furthermore, the mice that received the intraplantar CFA injectionpresented a marked increase in myeloperoxidase and N-acetyl-β-D-glucosaminidase activities (indirect evidence for neutrophil andmacro-phages influx, respectively) in the inflamed paw tissue 48 h after injec-tion. However, the administration of FTosPz or Celecoxib did not reducetheMPOandNAGactivities in the paws thatwere CFA injected, possiblybecause they did not alter the recruitment of immune cells at the lesionsite. In accordance with our MPO or NAG activity findings, cell infiltra-tion was also confirmed by histological analysis, demonstrating leuko-cyte infiltration, at least up to 48 h after CFA injection. These resultsare consistent with those reported by Vardeh et al. (2009) andSauzem et al. (2009), where the injection of intraplantar CFA in miceor rats, respectively, causes edema and leukocyte infiltration. Thus, theantinociceptive action of FTosPz does not appear to be associated witha local anti-inflammatory action.
Another type of inflammatory pain is postoperative pain, which is acommon form of acute pain. In response to surgical intervention, blood-borne immune cells are recruited to the site of injury and resident im-mune cells are activated and release multiple inflammatory mediators.These immune cells contribute to peripheral nociceptive sensitizationby releasing soluble factors and interacting directly with nociceptors(Julius and Basbaum, 2001; Ren and Dubner, 2010). Unfortunately,surveys have demonstrated that approximately half of all patientsexperience moderate to severe pain after surgery, indicating that de-spite the development of new drugs the postoperative pain remainspoorly treated (Pogatzki-Zahn et al., 2007). The main drugs that areclinically used to produce postoperative analgesia are nonsteroidalanti-inflammatory drugs (NSAIDs), opioids, ketamine, peripheral localanesthetics and gabapentin. However, it is known that these drugscan cause side effects that often limit their use (Dahl and Kehlet,2006). Once patients who have controlled the pain well have improvedhealth-related quality of life and an overall greater satisfaction withtheir experience (Gandhi et al., 2011), we seek compounds that aremore effective and have fewer side effects for the treatment of postop-erative pain. Firstly, we demonstrated that the oral administration ofFTosPz presented a preventive and curative effect on the hyperalgesiainduced by plantar incision. These results are according with the datafound by Milano et al. (2008a), where a 5-trifluoromethyl-substitutedpyrazole prevented and reversed the hyperalgesia induced by surgicalincision in mice. In addition to pyrazoles containing the trifluoromethylsubstituent group, pyrazoles with difluoromethyl or trichloromethylsubstituent groups also present an anti-hyperalgesic effect in a postop-erative pain model in rat and mice, respectively (Ochi et al., 2003;Trevisan et al., 2013). Like FTosPz, Celecoxib, a 3-trifluoromethyl-substituted pyrazole, also reduced postoperative pain behavior in thispain model, which is in agreement with the pre-clinical and clinicaldata (Senard et al., 2010; White et al., 2011; Whiteside et al., 2004).These results reinforce the importance of pyrazoles with different sub-stituent groups especially di or trifluoromethyl-substituted pyrazoleon hyperalgesia induced by surgical procedures. Thus, FTosPz could bea useful tool in the treatment of postoperative pain, since it is devoidof ulcerogenic effects when tested pre-clinically, which is a commonside effect of the current NSAIDs (Oliveira et al., 2009).
We also evaluated the effects of FTosPz on a neuropathic painmodelin mice. Neuropathic pain is a debilitating condition that frequentlyresults from injury to a peripheral nerve causing spontaneous pain(ongoing, paroxysms) and painful hypersensitivity to mechanical andthermal (hyperalgesia) or innocuous (allodynia) stimuli (Baron, 2009).The current approaches for neuropathic pain treatment include the useofmorphine-like opioids. However, thesemedications are partially effec-tive, and neuropathic pain is usually not responsive to NSAID analgesics(de Leon-Casasola, 2013; Dworkin et al., 2007; Woolf and Mannion,1999). Preclinical data show that only high doses of morphine adminis-tered by systemic route in rats are able to partially reduce neuropathicpain. Furthermore, the doses used are higher than those used therapeu-tically in this model, which is consistent with the clinical results (Suzukiet al., 1999; Lee et al., 1995). Moreover, a randomized clinical trial dem-onstrated that morphine did not differ from placebo in the treatment ofchronic neuropathic pain (Khoromi et al., 2007). Thus, preclinical andclinical studies report a wide range in the effectiveness of morphine,ranging from inadequate to potent analgesia (Dworkin et al., 2007). Sim-ilar to opioids, preclinical results demonstrate the lack of an analgesic ef-fect of NSAIDs on neuropathic pain. Systemic diclofenac, a potent NSAID,did not attenuate mechanical hyperalgesia in a neuropathic pain modelinduced by the ligation of the L5/L6 sciatic nerve in mice (Kiso et al.,2008). In addition, the subcutaneous injection of indomethacin (a classicinhibitor of cyclooxygenase) into the contralateral paw or abdomen ofrats had no effect in a neuropathic pain model induced by partial sciaticnerve ligation (Syriatowicz et al., 1999). On the other hand, Celecoxib andother COX-2 selective inhibitors are effective in reducing neuropathichyperalgesia (Guindon and Beaulieu, 2006; Hefferan et al., 2003; Lauet al., 2010; Syriatowicz et al., 1999). Here, we demonstrated that themice submitted to partial sciatic nerve ligation presented hyperalgesiaseven days after surgery, which was reverted by FTosPz or Celecoxib.Our results have great relevance, since the pathological pain modelsstudied here are difficult to treat clinically and the currently avail-able drugs are ineffective or cause adverse effects that limit theiruse (Labianca et al., 2012). Furthermore, the fact that FTosPz whenadministered orally presented similar efficacy to Celecoxib seemsto be relevant because the oral administration of drugs is more clin-ically usable due to its safety, easy administration and low cost(Buxton, 2006).
In our previous results (Oliveira et al., 2009), we demonstrated thatFTosPz neither reduced the body temperature of the animals, a commoneffect caused by some opioids and cyclooxygenase-3 inhibitors (such asacetaminophen or dypirone) nor produced gastric lesions, which is amajor side-effect of NSAIDs (Brune, 2007; Hayes and Tyers, 1983;Tomazetti et al., 2005). Here, we have demonstrated that oral treatmentwith FTosPz or Celecoxib did not alter the motor activity of mice, a sideeffect that is often caused by opioids (Li et al., 2004; Listos et al.,2011). In addition, neither FTosPz nor Celecoxib caused alterations inthe activity of enzymes ALT/AST or in the creatinine/urea levelsthat would indicate liver or renal injury, respectively, which is a sideeffect of NSAIDs (Dinchuk et al., 1995; Unzueta and Vargas, 2013).Furthermore, FTosPzwas not able to alter the COX-1 and COX-2 enzymeactivities. Thus, the antinociceptive action of FTosPz after its systemicadministration seems to be different from classical analgesic drugs,such as opioids and selective or non-selective cyclooxygenase inhibitors.

403S.M. Oliveira et al. / Pharmacology, Biochemistry and Behavior 124 (2014) 396–404
4.1. Conclusions
Many studies have shown that COX-2 selective inhibitors cause car-diovascular damage and life-threatening side effects that appear fromlong-term use (Baron et al., 2008; Grosser et al., 2006; Nussmeieret al., 2005; Scheiman, 2009). Therefore, there is an urgent need forthe further development of new analgesic drugs that are more effectivefor the treatment of pathological pain and with fewer undesired effects.We developed our study in an attempt to find a compound that was aseffective as Celecoxib in the treatment of different pain models, withoutcausing locomotor alterations, gastric lesions or liver and renal toxicity,which are commoneffects experienced in some clinically used analgesicdrugs to treat various pathological pain. As expected, our preclinicalresults showed that FTosPz presents an anti-hyperalgesic effect that isas good as Celecoxib in pathological pain models. However, further in-vestigations are necessary to elucidate the exact mechanism of actionof this compound, since it was not able to alter COX enzyme activities.Although FTosPz did not show superior efficacy to Celecoxib, our resultssuggest that it is an interesting prototype of mild analgesic drugs forthe treatment of acute and chronic painful conditions such as arthritic,postoperative, and neuropathic pain.
Acknowledgments
This study was supported by the Programa de Apoio aos Núcleos deExcelência (PRONEX) (GrantNº 0408660) (Brazil).We also acknowledgefellowships from Conselho Nacional de Desenvolvimento Científico(CNPq) and Coordenação de Aperfeiçoamento de Pessoal de EnsinoSuperior (CAPES).
References
Attal N, Kayser V, Eschalier A, Benoist JM, Guilbaud G. Behavioural and electrophysiolog-ical evidence for an analgesic effect of a non-steroidal anti-inflammatory agent,sodium diclofenac. Pain 1988;35:341–8.
Baron R. Neuropathic pain: a clinical perspective. Handb Exp Pharmacol 2009;194:3–30.Baron JA, Sandler RS, Bresalier RS, Lanas A, Morton DG, Riddell R, et al. Cardiovascular
events associated with rofecoxib: final analysis of the APPROVe trial. Lancet 2008;372:1756–64.
Bekhit A, Abdel-Azien T. Design, synthesis and biological evaluation of some pyrazolederivatives as anti-inflammatory-antimicrobial agents. Bioorg Med Chem 2004;12:1935–45.
Bonacorso HG,Wentz A, Lourega VR, Cechinel CA, Moraes TS, Coelho HS. Trifluoromethyl-containing pyrazolinyl (p-tolyl) sulfones: the synthesis and structure of promisingantimicrobial agents. J Fluor Chem 2006;127:1066–72.
Brune K. Persistence of NSAIDs at effect sites and rapid disappearance from side-effectcompartments contributes to tolerability. Curr Med Res Opin 2007;23:2985–95.
Buxton ILO. Pharmacokinetics and pharmacodynamics: the dynamics of drug absorption,distribution, action and elimination. In: Brunton L, Lazo JS, Parker KLP, editors. Good-man and Gilman’s The Pharmacological Basis of Therapeutics. New York: McGraw-Hill; 2006. p. 1–40.
Chan FK. Primer: managing NSAID-induced ulcer complications—balancing gastrointesti-nal and cardiovascular risks. Nat Clin Pract Gastroenterol Hepatol 2006;3:563–73.
Chaplan SR, Bach FW, Pogrel JW, Chung JM, Yaksh TL. Quantitative assessment of tactilehyperalgesia in the rat paw. J Neurosci Methods 1994;53:55–63.
Cheng CC, Elslager EF, Werbel LM, Priebe SR, Leopold WR. Pyrazole derivatives. Synthesisand antineoplastic activity of 3-(2 chloroethyl)-3,4-dihydro-4-oxopyrazolo{5,1-d}-1,2,3,5-tetrazine-8 carboxamide and related compounds. J Med Chem 1986;29:1544–7.
Chiba A, Mizuno M, Tomi C, Tajima R, Alloza I, di Penta A, et al. A 4-trifluoromethylanalogue of Celecoxib inhibits arthritis by suppressing innate immune cell activation.Arthritis Res Ther 2012;14(1):R9.
Dahl JB, Kehlet H. Postoperative pain and its management. In: Mc. Mahon SB, KlotzenburgM, editors. Textbook of pain. Londres: Wall/Melzack´s; 2006. p. 635–51.
de Leon-Casasola OA. Opioids for chronic pain: new evidence, new strategies, safeprescribing. Am J Med 2013;126(3 Suppl. 1):S3–S11.
Dinchuk JE, Car BD, Focht RJ, Johnston JJ, Jaffee BD, CovingtonMB, et al. Renal abnormalitiesand an altered inflammatory response in mice lacking cyclooxygenase II. Nature 1995;378:406–9.
Dixon WJ. Efficient analysis of experimental observations. Annu Rev Pharmacol Toxicol1980;20:441–62.
Dworkin RH, O'Connor AB, Backonja M, Farrar JT, Finnerup NB, Jensen TS, et al. Pharma-cologic management of neuropathic pain: evidence-based recommendations. Pain2007;132:237–51.
Essex MN, Bhadra P, Sands GH. Efficacy and tolerability of Celecoxib versus naproxen inpatients with osteoarthritis of the knee: a randomized, double-blind, double-dummy trial. J Int Med Res 2012;40:1357–70.
Ferreira J, Campos MM, Pesquero JB, Araújo RC, Bader M, Calixto JB. Evidence for theparticipation of kinins in Freund's adjuvant-induced inflammatory and nociceptiveresponses in kinin B1 and B2 receptor knockout mice. Neuropharmacology 2001;41:1006–12.
Gandhi K, Heitz JW, Viscusi ER. Challenges in acute pain management. Anesthesiol Clin2011;29:291–9.
Graziottin A, Gardner-Nix J, Stumpf M, Berliner MN. Opioids: how to improve complianceand adherence. Pain Pract 2011;11:574–81.
Grosser T, Fries S, FitzGerald GA. Biological basis for the cardiovascular consequences of COX-2 inhibition: therapeutic challenges and opportunities. J Clin Invest 2006;116:4–15.
Guindon J, Beaulieu P. Antihyperalgesic effects of local injections of anandamide,ibuprofen, rofecoxib and their combinations in a model of neuropathic pain.Neuropharmacology 2006;50:814–23.
Gürsoy A, Demirayak S, Capan G, Erol K, Vural K. Synthesis and preliminary evaluation ofnew 5-pyrazolinone derivatives as analgesic agents. Eur J Med Chem 2000;35:359–64.
Hayes AG, Tyers MB. Determination of receptors that mediate opiate side effects in themouse. Br J Pharmacol 1983;79:731–6.
Hefferan MP, Carter P, Haley M, Loomis CW. Spinal nerve injury activates prostaglandinsynthesis in the spinal cord that contributes to early maintenance of tactile allodynia.Pain 2003;101:139–47.
Hogan Q. Animal pain model. Reg Anesth Pain Med 2002;27:385–401.Julius D, Basbaum AI. Molecular mechanisms of nociception. Nature 2001;413:203–10.Khoromi S, Cui L, Nackers L, Max MB. Morphine, nortriptyline and their combination vs.
placebo in patients with chronic lumbar root pain. Pain 2007;130:65–75.Kiso T, Watabiki T, Tsukamoto M, Okabe M, Kagami M, Nishimura K, et al. Pharmacolog-
ical characterization and gene expression profiling of an L5/L6 spinal nerve ligationmodel for neuropathic pain in mice. Neuroscience 2008;153:492–500.
Kloppenburg M, Kwok WY. Hand osteoarthritis—a heterogeneous disorder. Nat RevRheumatol 2011;8:22–31.
Labianca R1, Sarzi-Puttini P, Zuccaro SM, Cherubino P, Vellucci R, Fornasari D. Adverseeffects associated with non-opioid and opioid treatment in patients with chronicpain. Clin Drug Investig 2012;32(Suppl. 1):53–63.
Lau WK, Lau YM, Zhang HQ, Wong SC, Bian ZX. Electroacupuncture versus Celecoxib forneuropathic pain in rat SNL model. Neuroscience 2010;170:655–61.
Lee YW, Chaplan SR, Yaksh TL. Systemic and supraspinal, but not spinal, opiates suppresshyperalgesia in a rat neuropathic pain model. Neurosci Lett 1995;199:111–4.
Li JX, Zhang Q, Liang JH. Valproate prevents the induction, but not the expression ofmorphine sensitization in mice. Behav Brain Res 2004;152:251–7.
Listos J, Talarek S, Poleszak E, Wrobel A, Fidecka S. Attenuating effect of adenosinereceptor agonists on the development of behavioral sensitization induced by sporadictreatment with morphine. Pharmacol Biochem Behav 2011;98:356–61.
Lloret S, Moreno JJ. Effects of an anti-inflammatory peptide (antiflammin 2) on cell influx,eicosanoid biosynthesis and oedema formation by arachidonic acid and tetradecanoylphorbol dermal application. Biochem Pharmacol 1995;50:347–53.
Malmberg AB, Basbaum AI. Partial sciatic nerve injury in the mouse as a model ofneuropathic pain: behavioral and neuroanatomical correlates. Pain 1998;76:215–22.
Matheus ME, Oliveira FL, Freitas CC. Antinociceptive property of new 4-acyl-arylhydrazonepyrazole compounds. Braz J Med Biol Res 1991;24:1219–22.
McCormack PL. Celecoxib: a review of its use for symptomatic relief in the treatment ofosteoarthritis, rheumatoid arthritis and ankylosing spondylitis. Drugs 2011;71:2457–89.
McDougall JJ. Arthritis and pain. Neurogenic origin of joint pain. Arthritis Res Ther 2006;8:220–6.
Mercadante S. Problems of long-term spinal opioid treatment in advanced cancerpatients. Pain 1999;79:1–13.
Milano J, Oliveira SM, Rossato MF, Sauzem PD, Machado P, Beck P, et al. Antinociceptiveeffect of novel trihalomethyl-substituted pyrazoline methyl esters in formalin andhot-plate tests in mice. Eur J Pharmacol 2008a;581:86–96.
Milano J, Rossato MF, Oliveira SM, Drewes C, Machado P, Beck P, et al. Antinociceptiveaction of 4-methyl-5-trifluoromethyl-5-hydroxy-4,5-dihydro-1H-pyrazole methylester in models of inflammatory pain in mice. Life Sci 2008b;83:739–46.
Nagakura Y, Okada M, Kohara A, Kiso T, Toya T, Iwai A, et al. Hyperalgesia andhyperalgesia in adjuvant-induced arthritic rats: time course of progression andefficacy of analgesics. J Pharmacol Exp Ther 2003;306:490–7.
Nussmeier NA, Whelton AA, Brown MT, Langford RM, Hoeft A, Parlow JL, et al. Complica-tions of the COX-2 inhibitors parecoxib and valdecoxib after cardiac surgery. N Engl JMed 2005;352:1081–91.
Ochi T, Goto T. Anti-inflammatory effect of FR 140423, a novel selective cyclooxygenase-2inhibitor, in rat adjuvant arthritis without gastrointestinal side effects. J PharmPharmacol 2000;52:553–60.
Ochi T, Ohkubo Y, Mutoh S. Effect of systemic FR140423, a new analgesic compound, in arat model of postoperative pain: contribution of delta-opioid receptors. Neurosci Lett2003;350:29–32.
Oliveira SM, Gewehr C, Dalmolin GD, Cechinel CA, Wentz A, Lourega RV, et al.Antinociceptive effect of a novel tosylpyrazole FTosPzn mice. Basic Clin PharmacolToxicol 2009;104:122–9.
Oliveira SM, Drewes CC, Silva CR, Trevisan G, Boschen SL, Moreira CG, et al. Involvementof mast cells in a mouse model of postoperative pain. Eur J Pharmacol 2011;672:88–95.
Pasin JS, Ferreira AP, Saraiva AL, Ratzlaff V, Andrighetto R, Machado P, et al. Antipyreticand antioxidant activities of 5-trifluoromethyl-4,5-dihydro-1H-pyrazoles in rats.Braz J Med Biol Res 2010;43. [1193-02].
Pogatzki-Zahn EM, Zahn PK, Brennan TJ. Postoperative pain—clinical implications of basicresearch. Best Pract Res Clin Anaesthesiol 2007;21:3–13.
404 S.M. Oliveira et al. / Pharmacology, Biochemistry and Behavior 124 (2014) 396–404
Prokopp CR, Rubin MA, Sauzem PD, Souza AH, Berlese DB, Lourega RV, et al. A pyrazolyl-thiazole derivative causes antinociception in mice. Braz J Med Biol Res 2006;39:795–9.
Ren K, Dubner R. Interactions between the immune and nervous systems in pain. NatMed 2010;16:1267–76.
Sauzem PD, Machado P, Rubin MA, Sant'Anna GS, Faber HB, Souza AH, et al. Design andmicrowave-assisted synthesis of 5-trifluoromethyl-4,5-dihydro-1H-pyrazoles: novelagents with analgesic and anti-inflammatory properties. Eur J Med Chem 2007;43:1237–47.
SauzemPD, Sant'Anna Gda S,Machado P, DuarteMM, Ferreira J, Mello CF, et al. Effect of 5-trifluoromethyl-4,5-dihydro-1H-pyrazoles on chronic inflammatory pain model inrats. Eur J Pharmacol 2009;616:91–100.
Scheiman JM. Balancing risks and benefits of cyclooxygenase-2 selective nonsteroidalanti-inflammatory drugs. Gastroenterol Clin North Am 2009;38:305–14.
Scholz J, Woolf CJ. Can we conquer pain? Nat Neurosci 2002;5:1062–7.Senard M, Deflandre EP, Ledoux D, Roediger L, Hubert BM, Radermecker M, et al. Effect of
Celecoxib combined with thoracic epidural analgesia on pain after thoracotomy. Br JAnaesth 2010;105:196–200.
Souza FR, Fighera MR, Lima TTF, Bastiani J, Barcellos IB, Almeida CE, et al. 3-Methyl-5-hydroxy-5-trichloromethyl-1H-1-pyrazolcarboxyamide induces antinociception.Pharmacol Biochem Behav 2001;68:525–30.
Suzuki K, Ota H, Sasagawa S, Sakatani T, Fujikura T. Assay method for myeloperoxidase inhuman polymorphonuclear leukocytes. Anal Biochem 1983;132:345–52.
Suzuki R, Chapman V, Dickenson AH. The effectiveness of spinal and systemic morphineon rat dorsal horn neuronal responses in the spinal nerve ligation model of neuro-pathic pain. Pain 1999;80:215–28.
Syriatowicz JP, Hu D, Walker JS, Tracey DJ. Hyperalgesia due to nerve injury: role ofprostaglandins. Neuroscience 1999;94:587–94.
Tomazetti J, Ávila DS, Ferreira APO, Martins JS, Souza FR, Royer C, et al. Baker yeast-induced fever in young rats: characterization and validation of an animal model forantipyretics screening. J Neurosci Methods 2005;147:29–35.
Trevisan G, Rossato MF, Walker CI, Klafke JZ, Rosa F, Oliveira SM, et al. Identification of theplant steroid α-spinasterol as a novel transient receptor potential vanilloid 1 antago-nist with antinociceptive properties. J Pharmacol Exp Ther 2012;343:258–69.
Trevisan G, Rossato MF, Walker CI, Oliveira SM, Rosa F, Tonello R, et al. A novel, potent,oral active and safe antinociceptive pyrazole targeting kappa opioid receptors. Neuro-pharmacology 2013;73:261–73.
Unzueta A, Vargas HE. Nonsteroidal anti-inflammatory drug-induced hepatoxicity. ClinLiver Dis 2013;17:643–56.
Vardeh D, Wang D, Costigan M, Lazarus M, Saper CB, Woolf CJ, et al. COX2 in CNS neuralcells mediates mechanical inflammatory pain hypersensitivity in mice. J Clin Invest2009;119:287–94.
Villarinho JG, Oliveira SM, Silva CR, Cabreira TN, Ferreira J. Involvement of monoamineoxidase B on models of postoperative and neuropathic pain in mice. Eur J Pharmacol2012;690:107–14.
von Banchet GS, Richter J, HückelM, Rose C, Bräuer R, SchaibleHG. Fibroblast-like synovialcells from normal and inflamed knee joints differently affect the expression of pain-related receptors in sensory neurones: a co-culture study. Arthritis Res Ther 2007;9(1):R6.
White PF, Tang J, Wender RH, Zhao M, Time M, Zaentz A, et al. The effects of oral ibupro-fen and Celecoxib in preventing pain, improving recovery outcomes and patientsatisfaction after ambulatory surgery. Anesth Analg 2011;112:323–9.
Whiteside GT, Harrison J, Boulet J, Mark L, Pearson M, Gottshall S, et al. Pharmacologicalcharacterisation of a rat model of incisional pain. Br J Pharmacol 2004;141:85–91.
Williams M, Kowaluk EA, Arneric SP. Emerging molecular approaches to pain therapy. JMed Chem 1999;42:1481–500.
Woller SA, Hook MA. Opioid administration following spinal cord injury: implications forpain and locomotor recovery. Exp Neurol 2013;247:328–41.
Woolf CJ, Mannion RJ. Neuropathic pain: aetiology, symptoms,mechanisms, andmanage-ment. Lancet 1999;353:1959–64.
Zimmermann M. Ethical guidelines for investigations of experimental pain in consciousanimals. Pain 1983;16:109–10.











![Identification of 2-[2-nitro-4-(trifluoromethyl)benzoyl ... · Regular paper Identification of 2-[2-nitro-4-(trifluoromethyl)benzoyl]- cyclohexane-1,3-dione metabolites in urine of](https://img.pdfslide.us/doc/110x75/5ad096377f8b9ae2138dec36/identification-of-2-2-nitro-4-trifluoromethylbenzoyl-paper-identification.jpg)

![Index [application.wiley-vch.de] · alkyl trifluoromethyl (or perfluoroalkyl) sulfoximines 681 alkyl trifluoromethyl sulfoxides [(Alk) S(O)CF 3] applications 491–492 preparation](https://img.pdfslide.us/doc/110x75/6064b9f559fa9f231e4ca32d/index-alkyl-trifluoromethyl-or-perfluoroalkyl-sulfoximines-681-alkyl-trifluoromethyl.jpg)















