Embed Size (px)
Citation preview
ANTIMICROBIAL STEWARDSHIP: TOOLS FOR PRACTICE & OVERCOMING BARRIERS
PAS Conference 2019 Justin Kosar BSc. BSP [email protected]
Disclaimer • No relevant conflicts of interest to disclose • Will be provided an honorarium for the content described
in this presentation by the Pharmacy Association of Saskatchewan (PAS)
Learning objectives 1. Understand the importance of antimicrobial stewardship
in everyday practice. – THE WHY 2. Recommend antibiotic management strategies that
reflect application of antibiotic stewardship principles. – THE WHAT
3. Recognize opportunities for stewardship intervention that are easy to implement in the community and hospital settings – THE WHEN
4. Highlight strategies to maximize antimicrobial stewardship impact in your practice. – THE HOW
Key findings from the Canadian Antimicrobial Resistance Surveillance System (CARSS)-Update 2018:
1) Increase in colonization by carbapenemase-producing organisms in both hospitals and the community setting…
2) The rate of methicillin-resistant Staphylococcus aureus (MRSA) infections coming from the community has nearly doubled;
3) Increasing rates of vancomycin-resistant enterococci infections are still being seen in hospitalized patients;
4) Azithromycin resistance in Neisseria gonorrhoea has doubled;
5) Prescriptions for adults 60 years and older have continued to increase over time and represent the age group with the greatest use of antimicrobials;
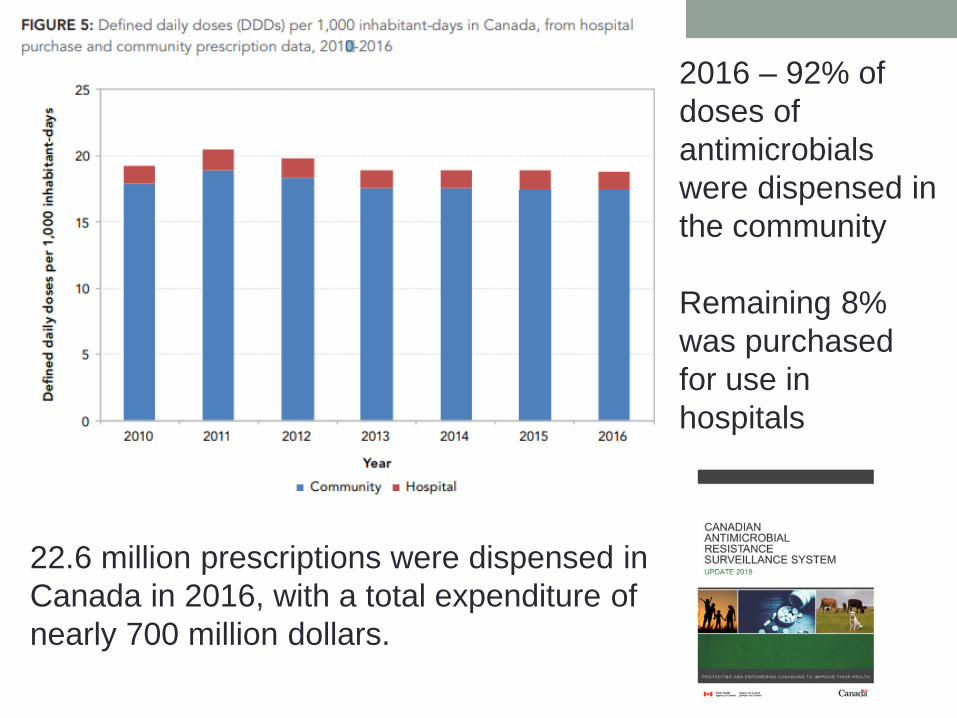
22.6 million prescriptions were dispensed in Canada in 2016, with a total expenditure of nearly 700 million dollars.
2016 – 92% of doses of antimicrobials were dispensed in the community Remaining 8% was purchased for use in hospitals
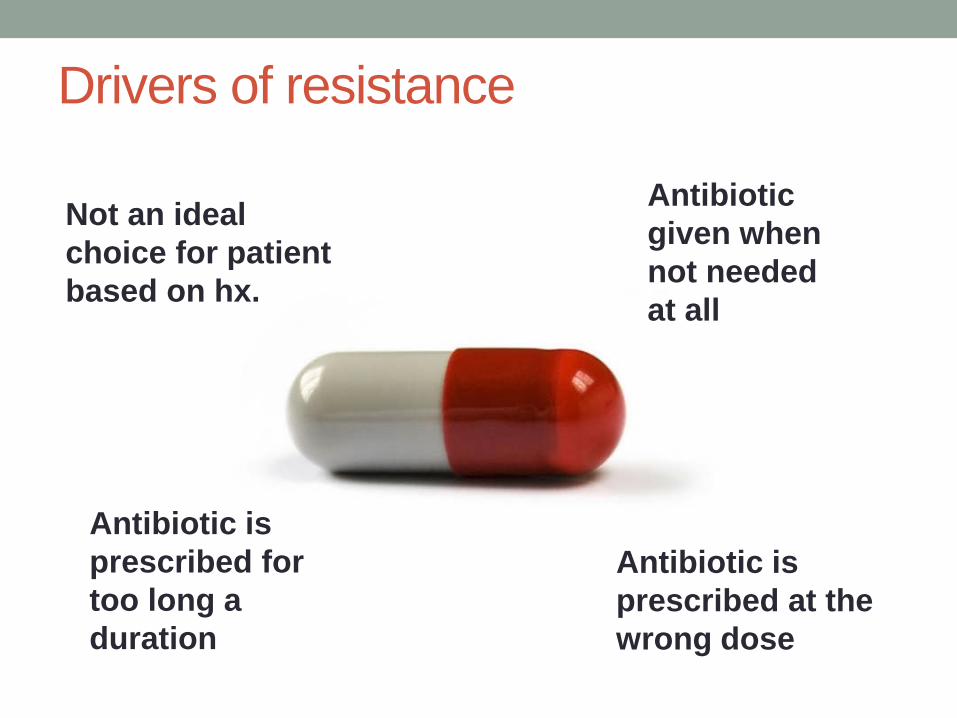
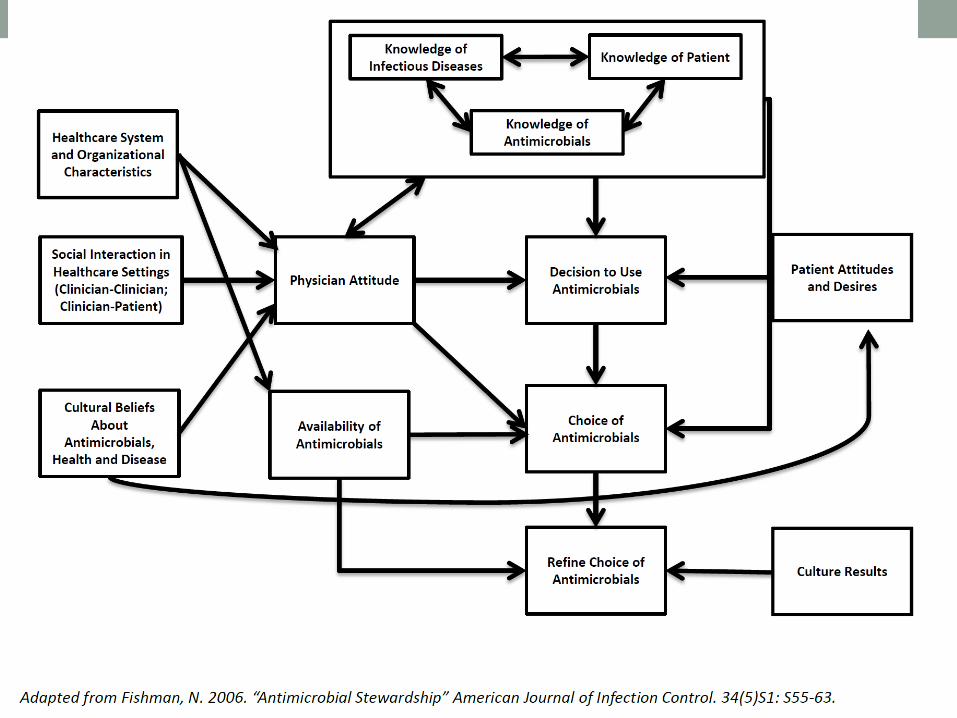
Drivers of resistance
Contribution of behavioural science to antibiotic stewardship
Antibiotic is prescribed for too long a duration
Not an ideal choice for patient based on hx.
Antibiotic given when not needed at all
Antibiotic is prescribed at the wrong dose
Your pressures as I see them • Financial success of your/the pharmacy • Time factors for antibiotic adjudication • Workload • Priority vs. other important pharmacy activities • Other DRP’s • Coverage • Counselling • “bigger fish to fry”
Prescriber concerns & influences • Diagnostic uncertainty • Perspectives on AMR • Pharmacological considerations/clinical factors • Influencers • Policies and guidelines • Context – time and expectation
• Patients expectation for therapy • Perceived duration and severity reported to physicians • Potential for loss of patients
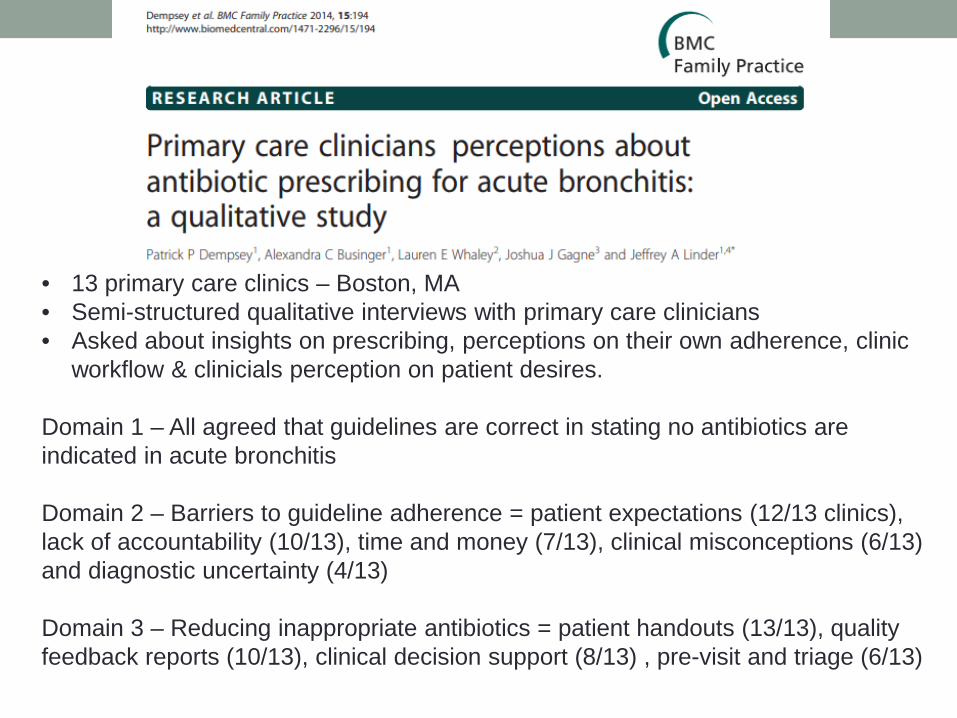
• 13 primary care clinics – Boston, MA • Semi-structured qualitative interviews with primary care clinicians • Asked about insights on prescribing, perceptions on their own adherence, clinic
workflow & clinicials perception on patient desires.
Domain 1 – All agreed that guidelines are correct in stating no antibiotics are indicated in acute bronchitis Domain 2 – Barriers to guideline adherence = patient expectations (12/13 clinics), lack of accountability (10/13), time and money (7/13), clinical misconceptions (6/13) and diagnostic uncertainty (4/13) Domain 3 – Reducing inappropriate antibiotics = patient handouts (13/13), quality feedback reports (10/13), clinical decision support (8/13) , pre-visit and triage (6/13)
Perspectives on AMR • OVERALL - Prescribers widely agree that AMR is important
and a current healthcare issue deserving attention
BUT • Less likely to perceive their own practice as the problem (e.g.
believing resistance comes into the hospital from the community)
In other words “It’s a problem, I’m NOT the problem, other people and other places are the problem.
https://www.safetyandquality.gov.au/wp-content/uploads/2018/04/Chapter10-Role-of-prescribers-in-antimicrobial-stewardship.pdf
CASE EXAMPLE
Ms. Kranberry
A 23 year old woman with well-controlled T2DM presents to your pharmacy with signs and symptoms suggestive of a UTI Upon quick consultation she reports: two days of increased frequency, painful urination and suprapubic tenderness. She has not received antibiotics recently. She is not sexually active. She has not any prior urinary tract infections.
Current medications: • OCP • Metformin Allergies: Penicillin – rash She is not in any acute distress.
She hands you a prescription for Ciprofloxacin 500 mg po BID x 7 days . Thoughts?
Uncomplicated Cystitis • Acute uncomplicated cystitis is one of the most common
indications for prescribing antimicrobials in the community setting
• By the age of 24, 1 in 3 women has experienced > 1 episode • As many as 60% of women report having had a UTI in their lifetime
• Women presenting to outpatient clinics with at least 2
symptoms of UTI (dysuria, urgency or frequency) and the absence of vaginal discharge have a greater than 90% probability of having acute cystitis
Bent S, Nallamothu BK, Simel DL, et al. Does this woman have an acute uncomplicated urinary tract infection? JAMA. 2002; 287:2701-10. Hooton TM, Besser R, Foxman B, et al. Acute uncomplicated cystitis in an era of increasing antibiotic resistance: a proposed approach to empirical therapy. Clin Infect Dis. 2004; 39:75-80.
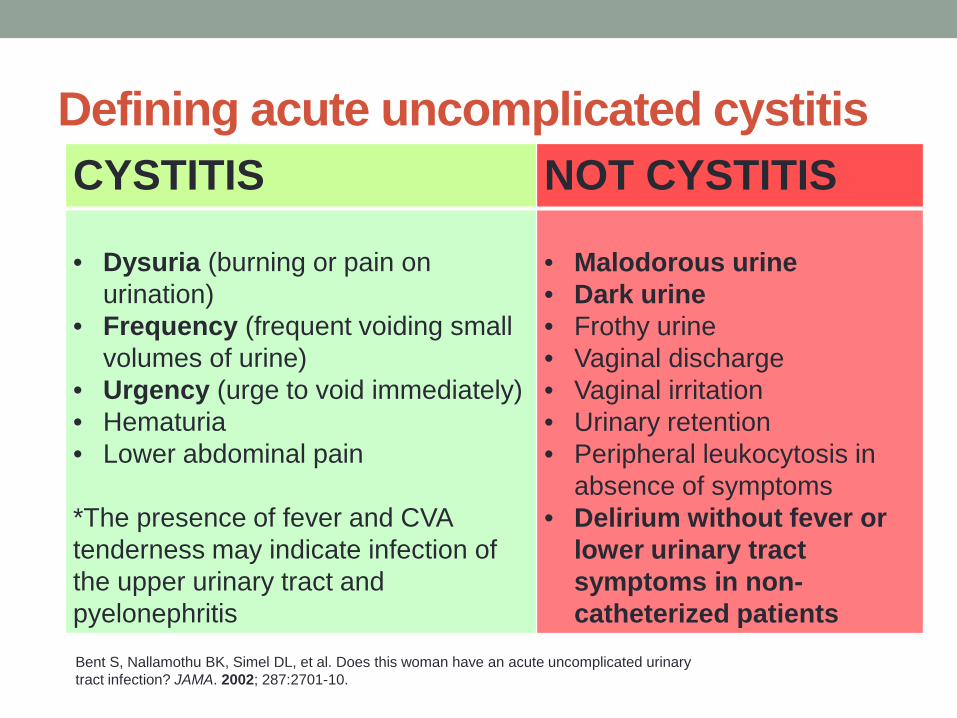
Defining acute uncomplicated cystitis CYSTITIS NOT CYSTITIS
• Dysuria (burning or pain on
urination) • Frequency (frequent voiding small
volumes of urine) • Urgency (urge to void immediately) • Hematuria • Lower abdominal pain
*The presence of fever and CVA tenderness may indicate infection of the upper urinary tract and pyelonephritis
• Malodorous urine • Dark urine • Frothy urine • Vaginal discharge • Vaginal irritation • Urinary retention • Peripheral leukocytosis in
absence of symptoms • Delirium without fever or
lower urinary tract symptoms in non-catheterized patients
Bent S, Nallamothu BK, Simel DL, et al. Does this woman have an acute uncomplicated urinary tract infection? JAMA. 2002; 287:2701-10.
Pharmacist adjudication • Check your resources • Check your patient history
• DOES THIS MAKE A FAIR AMOUNT OF SENSE

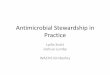
Example of an antibiogram
• https://saskhealthauthority.libguides.com/mobile/antibiograms
How are antibiograms useful?
• Periodic summary of susceptibilities of local isolates submitted to that hospital’s local microbiology lab
• Watch resistance patterns and monitoring trends over time
• Aid in selection of appropriate empirical therapy
• Aids in the development of local guidelines and clinical pathways
• Tool for any clinician when treated an infection empirically
• Can be an alternative to a C&S report until the results of a C&S are available OR alternative to a C&S report if no organism is grown where infection is still suspected.
Antibiogram does not provide • Organism sensitivity to an antibiotic based on site of infection
• Average MIC – antibiotic activity at various doses/concentrations
• Trend data over time
• Does not consider the source, nature of infection, possible complications and relevant drug PK and PD factors that go into each prescribing decision. • Some antibiotics and bacteria are purposefully left out.
• Eg. Macrolides are represented solely by erythro
Antibiotic cascade and how the antibiogram helps
• Urine – E. coli • “Primary Report” --- kept in house / in lab
• AMPICILLIN - S • CEFAZOLIN – S • CEPHALEXIN - S • CIPROFLOXACIN - S • NITROFURANTOIN - S • TRIMETHOPRIM/SULFAMETHOXAZOLE (TMP/SMX) - S • CEFTRIAXONE - S • IMIPENEM - S • CEFEPIME - S • PIPERACILLIN/CLAVULANATE – S • GENTAMICIN - S • TOBRAMYCIN – S
• Plus 10 MORE
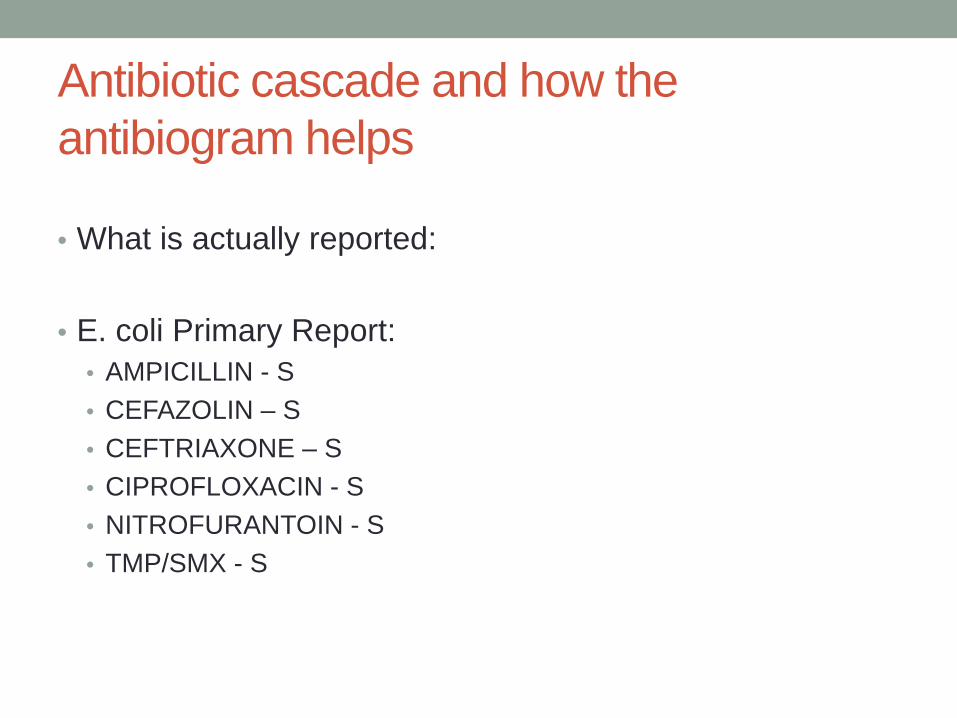
Antibiotic cascade and how the antibiogram helps
• What is actually reported:
• E. coli Primary Report:
• AMPICILLIN - S • CEFAZOLIN – S • CEFTRIAXONE – S • CIPROFLOXACIN - S • NITROFURANTOIN - S • TMP/SMX - S


Clinical Pathways Pathogens Antimicrobials
• Local, evidence-based guidelines • Use patient-specific factors • Interactive algorithmic format
tailored to your patient
• Includes local resistance data • Includes infection prevention and
control recommendations
• Local formulary data with dosing recommendations
• Local antibiogram data
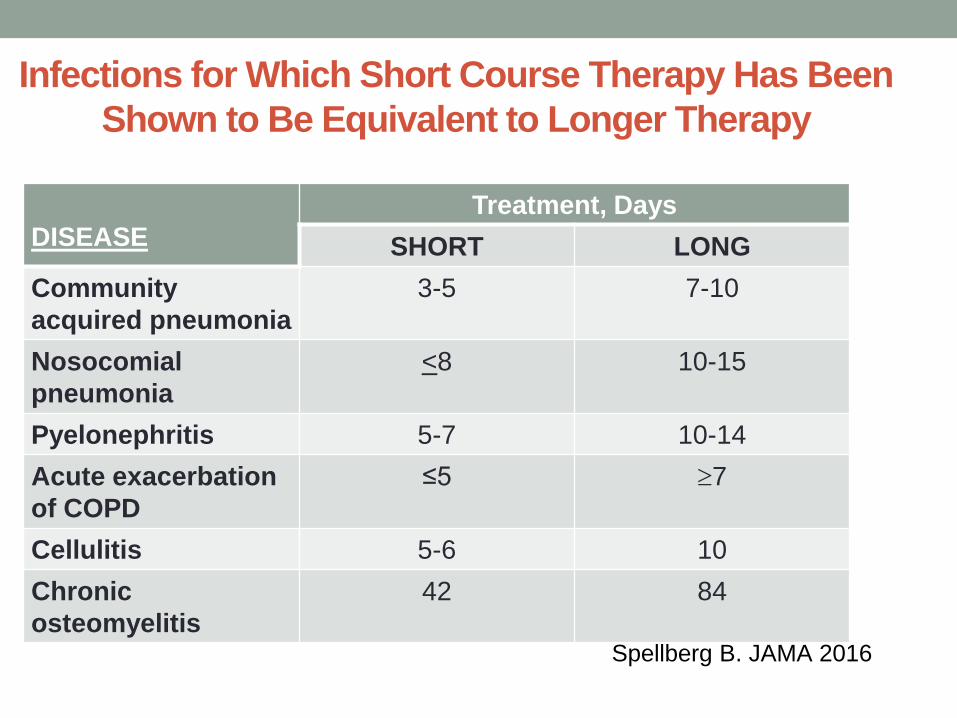
Infections for Which Short Course Therapy Has Been Shown to Be Equivalent to Longer Therapy
DISEASE
Treatment, Days SHORT LONG
Community acquired pneumonia
3-5 7-10
Nosocomial pneumonia
<8 10-15
Pyelonephritis 5-7 10-14 Acute exacerbation of COPD
≤5 ≥7
Cellulitis 5-6 10 Chronic osteomyelitis
42 84
Spellberg B. JAMA 2016
“I’M ALLERGIC TO PENICILLIN”
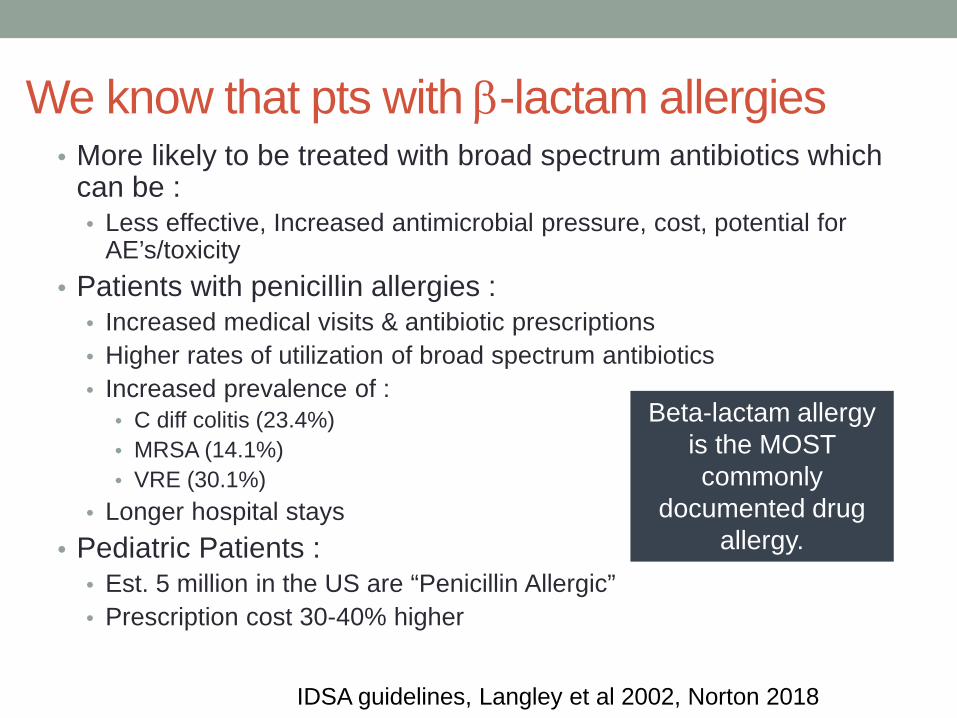
We know that pts with β-lactam allergies • More likely to be treated with broad spectrum antibiotics which
can be : • Less effective, Increased antimicrobial pressure, cost, potential for
AE’s/toxicity • Patients with penicillin allergies :
• Increased medical visits & antibiotic prescriptions • Higher rates of utilization of broad spectrum antibiotics • Increased prevalence of :
• C diff colitis (23.4%) • MRSA (14.1%) • VRE (30.1%)
• Longer hospital stays • Pediatric Patients :
• Est. 5 million in the US are “Penicillin Allergic” • Prescription cost 30-40% higher
IDSA guidelines, Langley et al 2002, Norton 2018
Beta-lactam allergy is the MOST commonly
documented drug allergy.
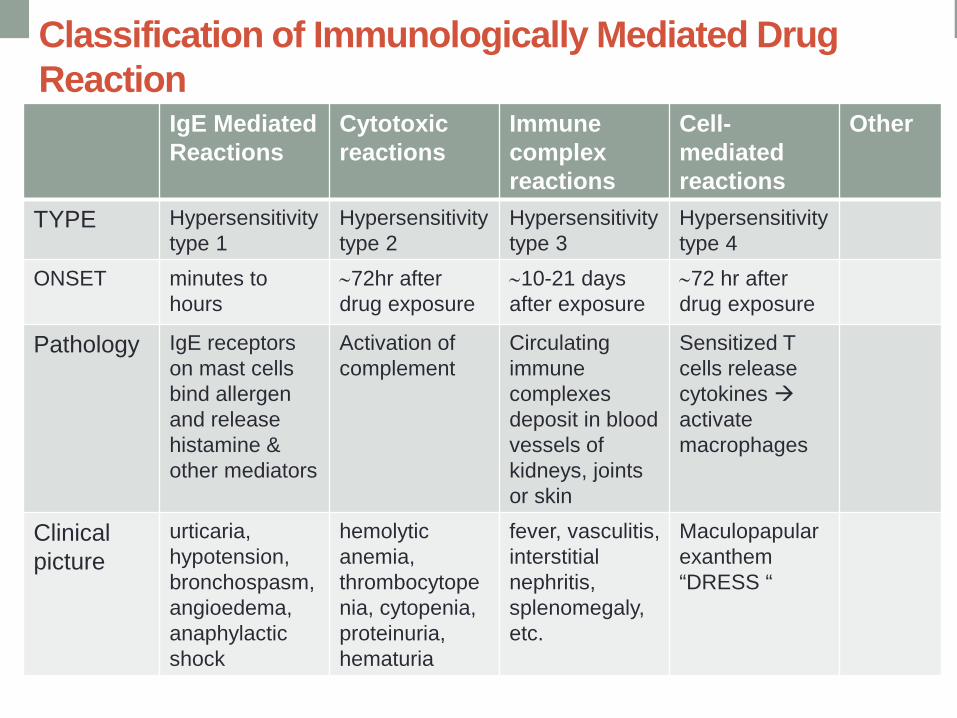
Classification of Immunologically Mediated Drug Reaction
IgE Mediated Reactions
Cytotoxic reactions
Immune complex reactions
Cell-mediated reactions
Other
TYPE Hypersensitivity type 1
Hypersensitivity type 2
Hypersensitivity type 3
Hypersensitivity type 4
ONSET minutes to hours
∼72hr after drug exposure
∼10-21 days after exposure
∼72 hr after drug exposure
Pathology IgE receptors on mast cells bind allergen and release histamine & other mediators
Activation of complement
Circulating immune complexes deposit in blood vessels of kidneys, joints or skin
Sensitized T cells release cytokines activate macrophages
Clinical picture
urticaria, hypotension, bronchospasm, angioedema, anaphylactic shock
hemolytic anemia, thrombocytopenia, cytopenia, proteinuria, hematuria
fever, vasculitis, interstitial nephritis, splenomegaly, etc.
Maculopapular exanthem “DRESS “
Other Reactions to consider • Virus Driven Reactions
• Cutaneous reactions to ampicillin in EBV infections
• Drug Side effect • 10% of patients taking penicillin can develop a non-
allergic, non-pruritic, non-urticarial rashes • 1-3 % of patients taking cephalosporins can develop
non-allergic rash
AAAAI Practice Parameter
Approach to patient with “Antibiotic Allergy” • Pragmatically - Not ALL Penicillin Allergies are real :
• 10% of patient reported penicillin allergies • 90% of those allergies are not real
1. Take a history 2. Confirmation
• Skin prick testing • Intradermal testing • Oral Challenge
3. Change patient records 4. Patient education on drug allergies Pichichero et al 2014
How you can help • Commit your site to a Pledge for antibiotic stewardship • Manage expectations
• MUCH OF WHAT PROPER ANTIBIOTIC STEWARDSHIP IS ENDS UP DOING A LITTLE BIT OF SOMETHING AND A LOT OF DOING NOTHING
Communication cues for pharmacists
• After listening carefully to the patients concerns, specifically re-state your understanding and validate their feelings – sympathize
• State a goal that you share in common with patients – “I too want to see you get better”
• Provide clear recommendations in lay language without jargon
• Explain why no antibiotic was provided and is not useful and may be in fact harmful
• Check to see understanding and re-iterate concerns being heard.
Steps involved in explaining that an antibiotic or test may not be necessary
Talking it over with prescribers • Find out what your key pressures from prescribers are or
better yet – pre-emptively acknowledge them.
• “You must be seeing a lot of respiratory tract infections lately” – vs. “sorry to bother you ….”
Talking it over with prescribers • Examine/audit and openly present common prescribing
trends? • If doc A is a large prescriber for FQ’s in UTI but good with using
amoxicillin for CAP – only focus on the antibiotic behavior you want to change
• BUT – use your records to highlight success
• Ask your prescribers what information they think would
inform their practice the most before you present it. • “I’d like to come and talk with your group about how we can tackle
our upcoming respiratory tract infection season together – what information about your previous prescribing do you think would help? “
Talking it over with prescribers • What other stuff is on their minds?
• Tell them about your concerns – FQ usage, antibiotic side
effects, • Use your records to your advantage
• Do you find a lot of pressure to provide antibiotics?
• If so – would you be interested in getting some common signage • Signing the pledge together?
• 49 primary care practices in 3 health systems using 3 different EHR’s • Primary outcome – antibiotic prescribing rate for antibiotic-inappropriate
acute RTI’s (e.g. URTIs, AB & Influenza) • 3 behavioural interventions implemented:
• A) suggested alternatives, • B) accountable justification • C) peer comparison
• Mean antibiotic prescribing rates decreased with accountable justification (23.2 5.2%) and peer comparison (19.9 3.7%)
• BOTTOM LINE: social comparison methods result in lower inappropriate prescribing.
Example script – Providers • Shortened therapies with plans
• Requires both practitioner and patient buy in • Must be logical and succinct in communication
• Example: I see you’ve prescribed azithromycin for this patients rhinitis – usually these infections are viral – after talking it over with our patient I was wondering your thoughts on delayed prescribing – if she/he doesn’t get better within then next 10-14 days can I instruct them to return? I’ve spoken to them about this and they are also ok with my plan. What do you think?
OR
• Check e-health for common diagnostics (e.g. NP swab)
Other strategies – rx filling • Check those resources again
• Previously filled rx history – might have been a different
doctor
• How would the previous UTI example change if she had 1 episode 7 months ago? • Check PIP or your Rx software to see what was prescribed • Check E-health to see if sampling done --- is this needed or
relevant ?
In the end • Getting buy-in from both patients and prescribers at the
same time is essential. • Remember downstream effects of your actions now with
antibiotics. • In speaking with prescribers – make the diagnosis less of
the emphasis and spend more time on getting a common plan.
• Ensure communication remains about the situation and patient NOT interpersonal
• Do not let a “no” this time become a “no” every time. • Celebrate your successes and feedback to everyone.