Today, CDC’s Office of Antibiotic Stewardship launched the first section of a four-part web-based training course on Antibiotic Stewardship. While this particular course is primarily for clinicians who prescribe antibiotics, CDC recognizes that everyone plays an important role in improving antibiotic use. Doctors, nurse practitioners, physician assistants, certified health education specialists, nurses, pharmacists, and public health practitioners with a master’s degree in public health are all eligible to receive up to eight hours of CE from this course, which is accessible in multiple modules offered in four sections. The first section is available now, with additional content releasing later this year.
Nicole M. Acquisto, Pharm.D., FCCP, BCCCP Emergency Medicine Clinical Pharmacy Specialist,
Department of Pharmacy Associate Professor, Department of Emergency Medicine
University of Rochester Medical Center Rochester, NY
Stewardship in the Emergency Department: Culture Surveillance and Follow-Up
Conflict of Interests
I have no actual or potential conflict of interest in relation to this presentation or program
Objectives
Describe differences in ED antimicrobial stewardship compared to traditional stewardship activities
Explain the development and implementation of an ED culture surveillance and follow-up program
Discuss associated metrics
Summarize additional ED stewardship quick wins
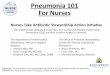
136 million
34.5 million
One-third
5-39%
142,500 ED visits annually
Antibiotics prescribed during ED
visits
Of antibiotics are
inappropriate
ED visits a year are due to antibiotic
ADEs
Of patients on
antibiotics develop AAD
Centers for Disease Control and Prevention. National Hospital Ambulatory Medical Care Survey: 2011 Emergency Department Summary. Available at: http://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2010_ed_web_tables.pdf. Accessed January 20, 2016. Haran et al. Am J Emerg Med. 2014;32:1195-1199.; May et al. Ann Emerg Med. 2013;62(1):69-77.
Why is ASP Important in the ED?
Presenter
Presentation Notes
130 million ED visits in 2010 103 million visits – At least 1 medication administered Average 2.1 medications/visit Total medication doses administered ~255 million Antibiotics were the second most common therapeutic drug class prescribed during ED visits 34,442,000 million drug mentions (13.5%) Estimated 142,500 ED visits/year – adverse effects associated with systemic antibiotic use 19.3% of all ED visits for drug related adverse effects 78.7% allergic reactions 136 million visits annually to the ED (2011 CDC) 5 of top 10 most common reasons for presentation were potentially infection related Fever 3rd, cough 4th, SOB 6th, throat 9th, vomiting 10th 160 million antibiotics are prescribed each year – 12.9% of all medications given in the ED or rx patients are d/c with are abx 1/3 of the 160 million rx for abx are inappropriate – inappropriate abx use has been described as the most important preventantable cause of drug resistance in the inpatient and outpatient setting 142,500 (0.1%) ED visits that occur each year are for an ED event 80% allergic reaction Between 5-39% of pts started on abx will go on to develop antibiotic associated diarrhea
Barriers of antimicrobial stewardship in ED setting
Provider liability
Variety in provider practice
Lack of patient info
Patient turnover
Lack of awareness
Quick decision making
Empiric therapy
Trinh TD, et al. Infect Dis Ther. 2015;4 (Suppl 1):S39–S50.; May et al. Ann Emerg Med. 2013;62(1):69-77.; Bishop BM. J Pharm Pract. 2015:1-8.
Quality measures
Presenter
Presentation Notes
Unique environment Quick decision making Limited patient information Difficult to sustain knowledge ED as a unique environment High patient volume and turnover Need for quick decision making High rates of staff turnover compared to other clinical areas Difficult for sustained knowledge Limited information No culture information or susceptibilities for that presentation Institution antibiograms often include the ED with inpatient isolates Also, may not be employed by the hospital – ED contract groups Goals are to: Decrease Overall and inappropriate use Costs Treatment duration Adverse effects and collateral damage Local resistance Representation/readmission Improve Healthcare outcomes Overall antibiotic utilization Overall strategies: Surveillance Data evaluation Policies/guidelines Education 1. Empiric therapy - Lack of information about the patient (cannot determine risk factors, recent hospitalizations or abx use, etc.) – come in alone or with EMS transporters that have incomplete stories Unclear source of infection – Altered, but CXR hazy infiltrate (meningitis, PNA, UTI) Culture history 2. Provider obstacles Pressure to see as many patients as possible Limits amount of time they can spend investigating patient’s previous hospitalizations Rapid turnover quick decision making (usually don’t have time to wait for consultation) Medical liability – concern for failure to diagnose and treat Pressure from local and/or national quality measures – inappropriate use of vanco/zosyn for HCAP criteria Patient satisfaction rates linked directly with prescribing of abx
Traditional ASP
Selection/Dose/Formulary restriction Drug monitoring Review of culture data and susceptibilities De-escalation or discontinuation of therapy IV to PO interchange Scheduled evaluation at 72 hours Duration Cost reduction
All ASPs Aren’t Created Equal
Trinh TD, et al. Infect Dis Ther. 2015;4 (Suppl 1):S39–S50.; May et al. Ann Emerg Med. 2013;62(1):69-77.; Bishop BM. J Pharm Pract. 2015:1-8.
Presenter
Presentation Notes
Maximize the appropriateness of BROAD SPECTRUM abx and Traditional activities: Selection Dose Rapid initiation De-escalation of therapy IV to oral interchange Scheduled evaluation at 72 hrs Duration
Right empiric drug/dose/duration Prompt administration Preventing re-presentations/re-admissions Guidelines- interdisiplinary development, consider national recommendations, institution factors, availability to providers (available on intranet) Disease specific order sets – Empiric regimens and also to direct length of treatment, direct important laboratory and culture data, auto-selected and linked, direct treatment as outlined in the guideline (lab and medication direction) Computer based decision support – direct appropriate selection, direct appropriate dose, limitations (does not take into consideration patient specific factors (drug and dose selection) Education - Identify the need based on practice trends or pointed medication DUE Focused UTI/SSTI education program Interactive lecture at weekly EM attending/resident conference Pocket guides and ID badge cards were prepared and distributed to EM providers with brief education Educational e-mail Evaluate education program – review of appropriate vs. inappropriate prescribing practices (before and after education program) Re-education and Feedback Barriers to prospective order review Availability of medications on override in the medication cabinets Limited time for review of the order and intervention Orders may not be seen by a pharmacist at all Centralized pharmacist location Paper orders “Autoverify” Retrospective order review and pointed education Focused on disease state management, selection, optimal dose, not “tweeking” Reference to the guidelines or reference tools
Widely recognized as an important component of any comprehensive antimicrobial stewardship program
Facilitates appropriate antibiotic selection and dose
Improve time to antibiotic administration
Point person to identify problem areas, implement improvement strategies, and follow-up on the results
Ability to monitor all ED patients simultaneously
Identify and triage any medication misadventures
May L, et al. Ann Emerg Med 2013;62:69-77
Emergency Medicine Clinical Pharmacist
Presenter
Presentation Notes
Medication misadventures: Medication errors, adverse effects, adverse drug reactions, drug interactions
American College of Emergency Physicians. Clinical Pharmacist Services in the Emergency Department . Available at : https://www.acep.org/Clinical---Practice-Management/Clinical-Pharmacist-Services-in-the-Emergency-Department/. Accessed June 13, 2016.
Getting Started: Identify the current process at your institution
Routine and immediate review Are there areas of breakdown in the current system? Differences in weekdays vs. weekends
Presenter
Presentation Notes
to determine appropriateness of empiric therapy Areas of breakdown: Ex: Delays to review due to direct patient care activities
Interdisciplinary group
Determine: How will you be notified of results (routine and immediate)? Paper or electronic process? Who will be available to discuss cases? Where will follow-up and outcome be documented? Who else will be involved to provide consistent coverage?
URMC program development
Acquisto NM and Baker SN. J Pharm Pract 2011;24:196-202
Culture Surveillance and Follow-up
Presenter
Presentation Notes
Collaboration with physicians, advanced practice providers, nurses, and microbiology staff to streamline the system for follow-up on all microbiologic cultures for patients discharged from the ED Collaborative practice agreement vs. face to face conversation
Barriers • Advanced practice providers responsible for weekend coverage • Time requirement • Paper system • Sterile site culture review (pager system)
Baker SN, Acquisto NM, et al. J Pharm Pract 2012;25:190-94
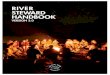
Previous Program 11/2007-1/2008
EPh Program 11/2008-1/2009
Median Time to Positive Culture Review, Days (range)
3 (1-15) n = 104
2 (0-4) n = 73
Median Time to Patient or PCP Notification, Days (range)
3 (1-9) n = 74
2 (0-4) n = 36
Evaluate the Impact/Evolve
Presenter
Presentation Notes
Call schedule pager coverage consistent APP phone coverage Limitation – currently not deescalating therapy (Glowacki RC, et al. Antibiotics combinations with redundant antimicrobial specta: clinical epidemiology and pilot intervention of computer-assisted surveillance. Clin Infec Dis. 2003;37:59-64. Target those discharged on multiple medication regimens, concern for community antibiotics availability of unused antibiotics
Electronic system 7 days/week – 365 days Sterile site review Culture hotline (telephone) Expanded cultures/serology Regional coverage (off-campus ED, urgent care) Electronic vs. phone call notification De-escalation
Optimization
Presenter
Presentation Notes
Collaboration with physicians, advanced practice providers, nurses, and microbiology staff to streamline the system for follow-up on all microbiologic cultures for patients discharged from the ED Collaborative practice agreement vs. face to face conversation
Evaluate the Impact
Retrospective chart review (n = 4639) 12 months before and after implementation
*Treatment failure, noncompliance due to cost or other reason, allergy, ADE
Randolf TC, et al. Am J Health-Syst Pharm 2011;68:916-9
Physician (n = 2278)
Pharmacist (n = 2361)
Modified regimen, n (%) 275 (12) 355 (15)
Unplanned readmissions at 96 hrs, n (%)*
432 (19) 165 (7)
Other Metrics
Davis LC:1270-1274.; Dumkow LE, et al. Infect Dis Ther 2014;3:45-53.; Miller K, et al. Am J Emerg Med 2014;32:1270-1274; Dumkow LE, et al. Infect Dis Ther 2014;3:45-53.
Pharmacist-driven antimicrobial optimization in the ED 30% increase in interventions for inappropriate antimicrobial
therapy based on culture data Pharmacist addition to the post-ED visit review of discharge
antimicrobial regimens 31.9% reduction of inappropriate revision of antibiotics after
culture review Impact of a multidisciplinary culture follow-up program of antimicrobial
therapy in the ED 12.9% reduction in return ED visits among uninsured
after culture review
Education Opportunities
Retrospective discharge prescription review for routine cultures Provide feedback based on drug, dose, duration, prescription writing
errors Reference to guidelines or institution tools during re-education
Retrospective blood culture review and education Review decision making process – gram stain data, patient clinical
information, oral vs. IV antibiotics Contamination vs. infectious
Presenter
Presentation Notes
Pharmacist involvement likely decreases overall use of antimicrobials and re-presentation to the ED for contaminated cultures (ex: blood, urine, vaginal) Barriers to prospective order review Availability of medications on override in the medication cabinets Limited time for review of the order and intervention Orders may not be seen by a pharmacist at all Centralized pharmacist location Paper orders “Autoverify” Retrospective order review and pointed education Focused on disease state management, selection, optimal dose, not “tweeking” Reference to the guidelines or reference tools
Education/Reference Tools Identify needs based on practice trends and DUEs
Focused UTI/SSTI education program
Presenter
Presentation Notes
Discuss the process for development – National and institution guidelines, local susceptibility patterns, approval by antimicrobial subcommittee. Already had SSTI guidelines, provided education and a new format for reference
ED Discharge Panels
Presenter
Presentation Notes
Pharmacist involvement likely decreases overall use of antimicrobials and re-presentation to the ED for contaminated cultures (ex: blood, urine, vaginal) Barriers to prospective order review Availability of medications on override in the medication cabinets Limited time for review of the order and intervention Orders may not be seen by a pharmacist at all Centralized pharmacist location Paper orders “Autoverify” Retrospective order review and pointed education Focused on disease state management, selection, optimal dose, not “tweeking” Reference to the guidelines or reference tools
ED Discharge Panels
Presenter
Presentation Notes
Pharmacist involvement likely decreases overall use of antimicrobials and re-presentation to the ED for contaminated cultures (ex: blood, urine, vaginal) Barriers to prospective order review Availability of medications on override in the medication cabinets Limited time for review of the order and intervention Orders may not be seen by a pharmacist at all Centralized pharmacist location Paper orders “Autoverify” Retrospective order review and pointed education Focused on disease state management, selection, optimal dose, not “tweeking” Reference to the guidelines or reference tools
Conners GP and Hays DP. Ann Emerg Med 2007;50:414-18
Does drug storage in the ED change prescribing practices?
Presenter
Presentation Notes
Hypothesized that adding medications previously only available from the hospital central pharmacy to the ED medication cabinets would alter the frequency with which they were ordered 4 medications that were not previously available and were not subject to prescribing practice changes over the study period were included Not available in the ED < 5 orders per month Available in the ED increase in order volume Pantoprazole IV – 25-fold Azithromycin IV – 6.5-fold Moxifloxacin PO – 7.2 fold Moxifloxacin IV – 4-fold Does drug storage in the ED change prescribing practices?
Batch if possible Vancomycin Ceftriaxone/lidocaine IM syringes
Optimizing Medication Storage in ED
Presenter
Presentation Notes
Talk about pyxis Talk about how to identify what meds have longest TAT and how batching may be helpful
Drive Use of Meds Readily Available
Presenter
Presentation Notes
Measure the impact by Evaluate order set utilization and compare to ICD9 admission codes Review medication cabinet pulls compared to central pharmacy dispense Direct prescribing practices Built based on medication cabinet availability Details location for specific ED areas (PEDS)
4014) Re-presentation 2.5% vs. 5.9%, p = 0.026 Cellulitis 2/122 (1.6%) vs. 71/ 1072 (6.9%), p = 0.024
Return visit avoidance 136
UTI 0/29 (0%) vs. 40/692 (5.8%), p = 0.18 318 medication courses = $1122.80
Hayes BD, et al. Am J Emerg Med 2012;30:2011-4
Presenter
Presentation Notes
Obj: If patients with a complete course of Abx for select conditions would decrease the rate of 7 days representation To-Go med or prescription for UTI, pyelonephritis, cellulitis, or dental infection Jan-Dec 2010; limited health insurance or discharged off hours when nearby pharmacies were closed Prepresentation captured if within 7 days for similar diagnosis Meds were PCN, clindamycin, Bactrim, nitrofurantoin Of 1149, 122 were given Go-To meds 318 medication courses in 243 patients Helps to standardize practice of medications used an duration of therapy
Conclusions Pharmacist-managed culture surveillance and
follow-up is associated with: Decreased ED re-presentation Faster time to follow-up and intervention Improvement in appropriate interventions
Several different opportunities for ASP in the ED Right empiric drug/dose/duration Prompt administration Preventing re-presentations/re-admissions
Presenter
Presentation Notes
Prompt administration for sick patients and ED throughput
Thank You!
Next Steps
• Next Call – October 9 at 2pm Eastern/1pm Central Time – Staphylococcus aureus Bacteremia Care Bundles
• Opportunities for involvement
– Speaker or Topic for future call – Antibiotic Use Reporting into NHSN and TDH AU Point