Embed Size (px)
DESCRIPTION
A short presentation on antidiabetic drugs.
Citation preview

DRUGS ACTING ON AUTONOMIC NERVOUS
SYSTEM(REVIEW ON IT’S ANATOMY AND
PHYSIOLOGY)(GROUP 2)

AUTONOMIC NERVOUS SYSTEM
• Peripheral nervous system located outside the brain and spinal cord is made of 2 divisions the autonomic nervous system and somatic.
• Autonomic nervous system is also called visceral system.
• Its function include control and regulation of the heart,respiratory system,GI tract,bladder,eyes and glands.

• Involuntary nervous system.• 2 sets of neuron in ANS are: AFFERENT
(sensory neurons) and EFFERENT (motor neurons).
• Afferent neurons send impulses to the central nervous system where they are interpreted.
• Efferent neurons receives impulses from the brain and transmit those impulses through spinal cord to the effectors organ cells.

• Efferent pathway is divided into 2 branches :• -Sympathetic• -Parasympathetic• Sympathetic nervous system is also called the
adrenergic system • Adrenaline was the neurotransmitter that
innervated the smooth muscle.


• Adrenergic receptor organ cells are:• -Alpha₁• -Alpha₂• -Beta₁• -Beta₂• Norepinephrine is released from the
terminal nerve ending and stimulate the cell receptors release response.

Parasympathetic nervous system
• Also called the cholinergic system because the neurotransmitter at the end of the neuron that innervates the muscle is called acetylcholine.
• Cholinergic receptors are organ cells that are either nicotinic or muscarinic.

• Acetylcholine stimulates the receptor cells to produce a response ,but the enzyme acetylcholine sterase may inactivate acetylcholine before it reaches the receptor cells.
• Drugs that mimic the neurotransmitter noepinephrine and acetylcholine produce a response opposite to each other in same organ.

CHOLINERGIC SYSTEM
and DRUGS
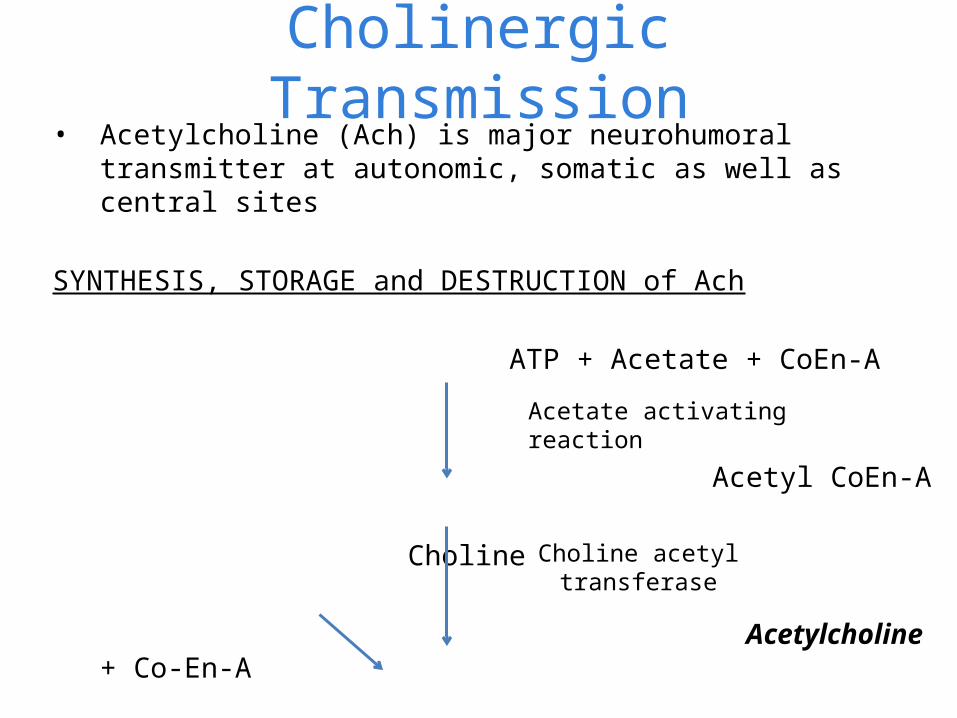
Cholinergic Transmission• Acetylcholine (Ach) is major neurohumoral transmitter at
autonomic, somatic as well as central sites
SYNTHESIS, STORAGE and DESTRUCTION of Ach ATP + Acetate + CoEn-A
Acetyl CoEn-A
Choline Acetylcholine + Co-En-A
Acetate activating reaction
Choline acetyl transferase

CHOLINOCEPTORS
Two types:1. Muscarinic (G-protein coupled
receptors)
2. Nicotinic (Ligand gated cation channel)

MUSCARINIC RECEPTORS
• Selectively stimulated by muscarine and blocked by atropine
• Located on autonomic effector cells in heart, blood vessels, eyes, smooth muscles, and glands of GIT, respiratory and urinary tracts, sweat glands and in CNS

Subtypes of muscarinic receptors
• 5 subtypes: M1, M2, M3, M4, M5
• M1, M2, M3 are present on effector cells, prejunctional nerve endings
• Expressed both in both peripheral organs and in CNS
• M4, M5 are present mainly on nerve endings in areas of brain, ; regulate release of other NTs
• Functionally, M1, M3 and M5 are in one class and M2
and M4 in one class
M1
• neuronal receptor located on ganglion cells and central neurons, esp. in cortex, hippocampus and corpus striatum
• Plays a major role in gastric secretion, relaxation of esophageal sphincter on vagal stimulation, learning, memory, motor functions, etc.
• Agonist: oxotremorine• Antagonist: pirenzipine, telenzipine

M2
Are predominantly as cardiac muscarinic receptors and as autoceptors on cholinergic nerve endings and in smooth muscles
Mediate vagal bradycardia Agonist: methacholine antagonist: triptamine,
methoctramine
M3
Mediate smooth muscle contractions and glandular secretions Mediate vasodilation through EDRF release Agonist: bethanechol antagonist: darifenacin
MOA through M1, M3. M5
1. Function through Gq protein
• Activate membrane bound phospholipase C (PLc)
• Generate inositol triphosphate (IP3) and diacylglycerol (DAG)
• Release Ca++ intracellularly
• Cause deploarization, glandular secretion, raise smooth muscle tone

Also
2. Also activate phopholipase A2
Enhanced release and synthesis of PGs, LTs

MOA through M2, M4
1. Function through Gi protein
• Open K+ channel
2. Inhibit adenylyl cyclase
hyperpolarization, reduced pacemaker activity, slowing of conduction and decreased force of contractions in the heart
Nicotinic receptors • Selectively activated by nicotine• Blocked by tubocurarine or hexamethonium• Enclose ligand activated ion channel: their activation causes
opening of channel
• rapid flow of cations
• Depolarization
• Generation of action potential
• Two subtypes: NM and NN
NN
• Present at ganglionic cells (sympathetic and parasympathetic), adrenal medullary cells and in spinal cord and certain areas of brain
• Selectively stimulated by dimethyl phenyl piperazinium (DMPP)
• Blocked by hexamethonium
• mediate primary pathway of transmission in ganglia
CHOLINERGIC DRUGS or Cholinomimetics
or Parasympathomimetics
• Drugs that produce actions similar to ACh
• Act either by directly interacting with cholinergic receptors (cholinergic agonists) or by increasing availability of ACh at these sites (anticholinesterases)
Cholinergic agonists
CHOLINE ESTERS
AcetylcholineMethacholine
CarbacholBethnechol
ALKALOIDS
MuscarinePilocarpineArecoline

Actions (of ACh as prototype)
Depending on which receptors Ach is binding to, peripheral actions can be either muscarinic or nicotinic;
central actions described differently
A. Muscarinic
1. HEART (M2) ACh hyperpolarizes SA nodal cells; ↓ rate of diastolic
depolarization therefore, ↓ rate of impulse generation bradycardia or even cardiac arrest may occur
HEART At AV node and His-Purkinje fibres, ↑ refractory period;
↓ conduction; partial AV blockade ↓ force of atrial contraction - ventricular contractility is reduced

2. BLOOD VESSELS (M3) All blood vessels are dilated Fall in B.P. and flushing occurReasons M3 receptors are present on vascular endothelial cells
vasodilatation is mediated through release of EDRF (NO)Due to inhibitory action of ACh on NA release from
vasoconstrictor nerve endings
Stimulation of cholinergic nerves to penis cause erection - by releasing NO - dilating cavernosal vessels through M3 receptors

3. SMOOTH MUSCLES (M3) In most organs, are contracted ↑ Tone and peristalsis in GIT Sphincters relax Abdominal cramps and evaculation of bowel
↑ peristalsis in ureter Detruser muscle contracts, sphincter relax Voiding of bladder
Bronchial muscle constrict dysponea, precipitation of bronchial asthma

4. GLANDS (M3 and M2) ↑ secretion from all glands sweating, salivation, lacrimation, gastric secretion
5. EYE contraction of circular muscles of iris miosis contraction of ciliary muscles spasm of
accomodation; reduction in intraoccular tension

B. NICOTINIC
1. AUTONOMIC GANGLIA Both sympathetic and parasympathetic ganglia are
stimulated
2. SKELETAL MUSCLES contraction of fibre May cause twitching and fasciculations

C. CNS
Produce a complex pattern of stimulation followed by depression
USES Bethanechol is used in post-operative or post-partum
urinary retention Neurogenic bladder atony, congenital megacolon,
gastroesophageal reflux
Side effects are prominent: belching, colic, involuntary urination, defecation, flushing, sweating, fall in BP, bronchospasm

CHOLINOMIMETIC ALKALOIDS
PILOCARPINE• Obtained from leaves of Pilocarpus microphyllus• Has prominent muscarinic actions• Stimulate ganglia• Cause marked sweating, salivation, ↑ other body
secretions • Small doses cause fall in BP (through muscarinic
receptors)• Higher doses elicit rise in BP and tachycardia (due to
ganglionic stimulation)• It penetrates cornea; cause miosis, ciliary muscle
contraction, fall in intraocular tension

• Used only in the eyes as 0.5-4% drops in open angle glaucoma
- Side effects: stinging sensation in eye, painful spasm of accomodation
• Used as miotic

MUSCARINE• Occur in poisonous mushroom Amanita muscaria
• Mushroom poisoning: 3 types1. Muscarine type (early mushroom poisoning)- Symptoms appear within an hour of eating mushroom; promptly reversed
by atropine
2. Anticholinergic/hallucinogenic type- Central manifestations occur; no specific treatment; atropine is
contraindicated
3. Phalloidin type (late mushroom poisoning)- Inhibit RNA and protein synthesis- Symptoms appear after many hours and due to damage to GIT mucosa,
liver, kidney- Treatment consists of supportive measures, thiotic acid

ANTICHOLINESTERASES (antiChEs)
AntiChEs are agents which inhibit ChE; protect Ach from hydrolysis
REVERSIBLECarbamates AcridinePhysostigmine (eserine) TacrineNeostigminePyridostimineEdrophoniumRivastigmine, Donepezil
IRREVERSIBLECarbamates OrganophosphatesCarbaryl DyflosPropoxur Echothiophate Parathion, Malathion Diazinon, tabun, sarin, soman
MOA• Anti-ChEs (carbamates and phosphates) carbamylate or
phosphorylate the esteratic site of the enzyme
• Acetylated enzyme reacts with water rapidly and esteratic site is freed in few milisec.;
• carbamylated enzyme (reversible inhibitors) react slowly
• Phosphorylated enzyme (irreversible inhibitors) react extremely slowly or not at all
PHARMACOLOGICAL ACTIONS1. Ganglia anti-ChEs stimulate ganglia through muscarinic receptors High doses causes persistent depolarization of nicotinic receptors and
cause transmission blockade
2. CVS muscarinic action produce bradycardia and hypotension; ganglionic
stimulation ↑ heart and B.P. Overall effects are unpredictable and depend on agent and dose
3. Skeletal muscles Repetitive firing of muscles twitchings and facsiculations Higher doses cause persistent depolarization of endplates blockade
of neuromuscular transmission muscle weakness and paralysis
4. Other effects Stimulation of smooth muscles and glands of GIT, respiratory, urinary

Individual compoundsPhysostigmine Neostigmine
1. Natural alkaloid fron Physostigma venonsum 1. synthetic
2. Good oral absorption 2. Poor oral absorption
3. CNS actions present 3. CNS actions absent
4. Penetrate cornea in eye 4. Poor penetration
5. No direct effects on NM cholinoceptors 5. direct action on NM cholinoceptors
6. Prominent effect on autonomic effectors 6. Prominent effect on skeletal muscles
7. Used as miotic in glaucoma 7. Used in myasthenia gravis
8. Dose: 0.5-1 mg oral/parentral 0.1-1% eye drops
8. dose: 0.5-2.5 mg i.m./s.c. 15-30 mg orally
9. Duration of action: systemic: 4-6 hrs in eye: 6-24 hrs
9. DOA: 3-4 hrs

** anti-ChEs are to be used cautiously in peptic ulcer, asthma, COPD and seizure patients
USES1. As miotic
a) In glaucoma: miotics ↑ tone of ciliary muscles and sphincter pupillae which pull on and improve outflow facility i.o.t. falls in open angle glaucoma
• Pilocarpine is most preferred in glaucoma. Sideeffects: spasm of accomodation, brow pain; systemic sideeffects: nausea, diarrhoea, sweating, bronchospasm
• Physostigmine is used only to supplement pilocarpine
b) To reverse the effect of mydriatics after refraction testing
c) To prevent formation of adhesions between iris and lens or iris and cornea in iritis, corneal ulcers etc.
In GLAUCOMA
Group of diseases characterised by a progressive form of optic nerve damage associated with raised i.o.t. (> 21mmHg)
Therapeutic measure: 1. lower i.o.t. either by reducing aqueous humor secretion or by promoting its drainage
OPEN ANGLE GLAUCOMA (wide angle, chronic simple) It is genetically predisposed degenerative disease affecting patency
of the trabecular meshwork which is lost with age i.o.t. rise progressively,, ocular hypotensive drugs are used
1. β adrenergic blockers: (timolol, betaxolol, levobunolol) lower i.o.t. by reducing aqueous formation (by downregulation of
adenylyl cyclase) Doesnot affect pupil size, tone of ciliary muscle or outflow facility

2. Miotics• They increase tone of ciliary muscles; and pull on and improve
alignment of trabeculae increase outflow facility i.o.t. falls
PILOCARPINE• Preferred as miotic• Therapy is started with lowest effective concentration (0.5%)• Action is rapid and short lasting (4-6 hrs)
3. α Adrenergic agonists • Adrenaline, dipivefrine, brimonidine
4. Carbonic anhydrase inhibitors• Acetazolamide, dorzolamide
ANGLE CLOSURE (narrow angle, acute, congestive) glaucoma• Occur in individuals with a narrow iridocorneal angle and
shallow anterior chamber• i.o.t. remains normal (until attack is precipitated)• i.o.t. risese rapidly to very high values• Emergency condition; failure to lower i.o.t. causes loss of sight
Therapy measures1. Topical β blocker: timolol 0.5% is instilled 6-8 hourly2. Miotic: pilocarpine 1-2%3. Hypertonic mannitol 20% or glycerol 10%4. Acetazolamide 0.5 g i.v. or oral twice daily
USES2. In myasthenia gravis
• Autoimmune disorder due to development of antibodies for nicotinic receptors at muscle end plate
• Treatment: 1. Neostigmine (15mg orally 6 hourly;;; dose adjusted as per response
2. corticosteroids

Anticholinesterase poisoning
• Local muscarinic manifestations at site of exposure occur immediately complex systemic effects due to muscarinic, nicotinic and central effects
• Irritation of eye, lacrymation, salivation, sweating, blurring of vision, defecation, urination
• Fall in B.P., tachycardia, arrythmias, vascular collapse• Muscular weakness, fasciculations, respiratory paralysis• Excitement, ataxia, convulsions, coma, death• Death is due to respiratory failure
• Treatment: 1. termination of exposure 2. supportive measures 3. specific antidotes: atropine, cholinesterase
reactivators (pralidoxime (2-PAM))
Anticholinergic Drugs (muscarinic receptor antagonists, Atropinic, Parasympatholytic)
• Anticholinergic drugs are those which block actions of ACh on autonomic effectors and in CNS exerted through muscarinic receptors
• Generally, called as Neuromuscular blockers
• Atropine is prototype of this class

CLASSIFICATION
1. Natural alkaloids: atropine, hyoscine (scopolamine)
2. Semisynthetic derivatives: homatropine , atropine methonitrate, hyoscine bromide, ipratropium bromide, tiotropium bromide
3. Synthetic compounds:a) mydriatics: cyclopentolate, tropicamideb) Antisecretory, antispasmodics: (i) quaternary compounds eg. Propantheline, oxyphenonium,
clidinium, pipenzolate, isopropamide, glycopyrolate (ii) tertiary amines eg. Dicyclomine, oxybutynin, flevoxate,
pirenzipine, telenzipinec) Antiparkinsonians trihexyphenidyl, procyclidine, biperiden,
benztropine, cycrimine, ethopropazine

PHARMACOLOGICAL ACTIONS (of atropine as prototype)
1. CNS: overall stimulant actions
Hyoscine produces central (depressant) effects at low doses
Atropine stimulates medullary centres: vagal, respiratory, vasomotor
Depresses vestibular excitation; has anti-motion sickness property
By blocking anti-cholinergic activity in basal ganglia, it suppresses tremor and rigidity in parkinsonism
High doses cause cortical excitation, restlessness, disorientation, hallucinations, delirium, followed by respiratory depression and coma

2. CVS: overall stimulant actions
1. HEART : atropine cause tachycardia (due to blockade of M2 receptors on SA node, through which vagal tone ↓ heart rate)
• Atropine facilatates A-V conduction
2. B.P.: atropine dosenot have any marked effect on B.P.• Tachycardia and vasomotor centre stimulation raise B.P. • Histamine release and direct vasodilator action lower B.P.• Atropine blocks vasodepressor actions of cholinergic agonists

3. EYE Topical instillation of atropine causes mydriasis, abolition of light
reflex, cycloplegia lasting 7-10 days photophobia, blurring of near vision
i.o.t. rise
4. SMOOTH MUSCLES All smooth muscles that receive parasympathetic innervation, are
relaxed by atropine ↓ Tone and amplitude of contractions of stomach, intestine
passage of chyme ↓ constipation occur Atropine cause bronchodilation and ↓ airway resistance Atropine attenuate the action of histamine, PGs, by antagonising
the reflex vagal component Has relaxant action on ureter and urinary bladder
5. GLANDS Atropine ↓ sweat, salivary, lacrimal secretion Skin and eyes become dry; talking and swallowing becomes difficult Atropine ↓ secretion of acid, pepsin and mucus in stomach Bicarbonate secretino in stomach is ↓ed
4. SMOOTH MUSCLES All smooth muscles that receive parasympathetic innervation, are
relaxed by atropine ↓ Tone and amplitude of contractions of stomach, intestine passage
of chyme ↓ constipation occur Atropine cause bronchodilation and ↓ airway resistance Atropine attenuate the action of histamine, PGs, by antagonising the
reflex vagal component Has relaxant action on ureter and urinary bladder
USES1. As antisecretorya) Preanaesthetic medication b) Peptic ulcer (because it reduce gastric secretion)c) Pulmonary embolism (reducing reflex secretions)d) To check excess sweating or swelling
2. As spasmodica) Intestinal and renal colic, abdominal crampsb) Nervous and drug induced diarrhoeac) Spastic constipation, irritable colond) Gastric hypermotility, gastritis, nervous dyspepsiae) To relieve urinary frequency and urgencyf) dynmenorrhoea
USES3. Bronchial asthma, asthmatic bronchitis, COPD Reflex vagal activity causes vasoconstriction and
increased secretion
4. As mydriatic and cycloplegic
5. As cardiac vagolytic
6. For central action i) parkinsonism ii) motion sickness iii) hyoscine is used as a ‘lie detector’
7. To antagonise muscarinic effects of drugs and poisons
SIDE EFFECTS AND TOXICITY Dry mouth, difficulty in swallowing and talking Dry, flushed and hot skin, fever, difficulty in micturition Dilated pupil, photophobia, blurred vision, palpitation Excitement, ataxia, delirium, hallucinations Hypotension, weak and rapid pulse, cardiovascular
collapse with respiratory depression
Treatment: gastric lavage with Tannic acid supportive measures Physostigmine 1-3 mg s.c. or i.v.,
repeated 4-6 hourly

Adrenergic blockers (antagonist)
•Drugs that block the effect of adrenergic neurotransmitter
•drugs that selectively inhibit specific receptor sites from sympathetic stimulation.
effects of adrenergic blockers at receptors
Receptors
• Alpha
• Βeta 1
• Beta 2
Responses
Vasodilation: decrease blood pressure, reflex tachycardia might result miosis, occurs; suppresses ejaculation; reduces contraction of the smooth muscles in the bladder neck and prostate gland
Decrease heart rate; reduces force of contraction.
Constrict bronchioles contract uterus; inhibits glycogenolysis.
Alpha adrenergic blockers• Drugs that block or inhibit a response at the alpha
adrenergic receptor site...eg,. Prazosin and analogs - terazosin,
doxazosin, trimazosin
• These are used to treat hypertension by relaxing arterial and venous smooth muscle, decreasing vascular resistance and venous return, and decreasing blood pressure without a significant increase in heart rate.
• Orthostatic hypotension and reflex tachychardia
Beta-adrenergic blockers
• Hormones known as catecholamines (norepinephrine, epinephrine) activate or stimulate specific receptors on cell surfaces, known as adrenergic receptors. A receptor has a specific structure that allows a drug or hormone to bind to it, similar to a key fitting in a lock.
What Side Effects Can I Expect?
• some patients notice muscle fatigue, especially with vigorous physical activity.
• Patients with asthma should not take β-blockers because they can interfere with the passage of air into the lungs.
• In some patients, heart rate and blood pressure may be reduced too much, causing lightheadedness and fainting.
• The drugs should be used with caution in diabetic patients taking insulin who have problems with excessive blood-sugar lowering and lightheadedness.
• The drugs should not be used if a patient has severe mental depression.
What Precautions Do I Need to Take?
• Never stop taking your prescribed β-blockers abruptly without informing your healthcare provider. Try not to miss any doses.
• If you develop excessive fatigue, mental depression, lightheadedness, fainting, or excessive shortness of breath, inform your healthcare provider.
• If you are prescribed new medicines or herbal remedies, inform your healthcare provider.

Adrenergic neuron blockers
* Potent drugs that block norepi. form sympathetic nerve endings a dec. in norepi. dec. in BP
• * Decrease in both cardiac output & peripheral vascular resistance
• * Common SE = Orthostatic Hypotension*

ANTIDIABETIC DRUGS

Diabetes Mellitus
third leading cause of death antidiabetic drugs are used to control this

Two Groups
• Insulin – a protein secreted from the beta cells of pancreas which is necessary for carbohydrate metabolism and plays an important role in protein and fat metabolism. The beta cells make up 75% of the pancreas and the alpha cells that secrete glucagon, a hyperglycemic substance, occupy approximately 20% of pancreas.

• Oral hypoglycemic dugs or oral antidiabetic drugs – are synthetic preparations that stimulate insulin increase otherwise alter the metabolic response to hyperglycemia.
Diabetes Mellitus
• A chronic disease resulting from deficient glucose metabolism
• Caused by insufficient insulin secretion from the beta cells. This results in high blood sugar or hyperglycemia
• Characterized by 3 p’s: Polyuria ( increased urine output), Polydipsia (increased thirst), and polyphagia (increased hunger)

Types of Diabetes Mellitus
1. Type 1 DM (Insulin Dependent DM or IDDM) 10%-12% caused by viral infections, environmental sanitations, and genetic factors
2. Type 2 DM (Non- Insulin Dependent or NIDDM) 85%-90% caused by heredity or obesity some beta cell function with varying amounts of
insulin secretion

3. Gestational DM < 1% ( 2%-5% of all pregnancies) during the 2nd and 3rd trimesters of pregnancy, the levels of the hormones, progesterone, cortisol, and human placental lactogen (HPL), are increased Glucose is then mabiuzed (?) from the tissue
Insulin
• Released from the beta cells of the islets of Langerhans in response to an increase in blood glucose
• Promote the uptake of glucose, amino acids, and fatty acids and converts them to substances that are stored in the body cells
• Normal Range : 60-100mg/dl (blood glucose) and 70-110mg/dl (serum glucose)
Beta Cells Secretion of Insulin
• Beta Cells in the pancreas secrete insulin approximately 0.2-0.5 units/kg/daily
• A client with DM may require 0.2-1.0 units/kg/daily

Commercially Prepared Insulin
• Parenteral (injectable) Insulin is obtained from pork and beef pancreas when the animals re slaughtered1. Pork Insulin- related to human insulin having
only one amino acid; weaker allergen2. Beef Insulin- for different amino acids
Human Insulin (Humulin)Introduced in 1983 and is produced by two
methods: 1. Changing the direfferent amino acid of prok insulin2. Using DNA technology
Humulin produced by DNA technology is made more pure which results in fewer side effects. It is administered via SubQ and is absorbed faster and have a shorter duration than animal insulin.

• The concentration of insulin is 100 units/ml or 500 U/ml and the insulin is packaged in a 10 ml vial.

Administration of Insulin
• Insulin is a protein and cannot be administered daily because GI secretions destroy the insulin structure.
• Administered via SubQ at 45o-90o • Regular insulin is the only type that can administered
IV• Insulin absorption is greater when given in the
deltoid and abdominal areas than when given in the thigh and buttocks areas. Heat and massage can increase subQ absorption.

• Insulin injection sites should be rotated to prevent lipodystrophy (tissue atrophy or hypertrophy) which can interfere with insulin absorption
Lipoatrophy a depression under the skin surface that primarily occurs in females & children
caused by the use of animal insulin (beef &pork)

Lipohypertrophy is a raised lump or knot on the skin surface that is more common in males
caused by repeated injection in the SubQ sites

Types of InsulinA. Rapid Acting Insulins
clear in solution with no added substance to prolong the insulin action
1. Lispro Insulin (Humalog) approved for use in 1996 the action begins in 5-15 minutes and the duration of action is 2-4 hoursActs faster than regular insulin must not be administered more than 5 mins before mealtime formed by reversing 2 amino acids in human regular insulin

2. Regular Insulin unmodified , crystalline any type of insulin that can be administered IV and SubQ given 30 minutes before meals
B. Short Acting Insulin clear in solution with ni added substance to prolong the insulin action has an onset of action in 30 minutes to 1 hour the peak action occurs in 2-4 hours and the duration of action is 6-8 hours

C. Intermediate Acting Insulins cloudy and may contain protamine, a protein that prolongs the action of insulin or zinc which also slows the onset of action and prolongs the duration of action.
the onset is 1-2 hours, peak action occurs in 6-12 hours and the duration of action 18-24 hours
include neutral –protamine-Hagedorn (NPH) , Lerute, humulinV and Humulin L.
Lerute and humulin L contain zinc which aslo prolongs the insulin action time

D. Long Acting Insulin acts in 4-8 hours, peaks in 14-20 hours and lasts for 24-36 hours1. Humulin V Ultralente absorbed slower than other insulins because of its; large crystals which dissolve slowly and prolong the duration time2. Lantus newer long acting insulin an insulin glargine that is an analogue of human insulin first long aching recombinant DNA (rDNA) human insulin approved by FDA has 24 hr duration

E. Combination Insulins- commercially premixed1. Humulin 70/30 it’s vials or prefilled disposable pens contain 70% of human isophane (intermediate-acting insulin NPH) and 30% regular (fast acting) insulin
2. Humulin 50/50 -it’s vial or pen contains 50% of isophane (NPH) insulin and 50% insulin
3. Humalog 75/25- available as a prefilled disposable pen only and contains 75% Lispro prostamine insulin and 25% Lispro “rapid” insulin
- helps prevent hypoglycemia , which could occur with the 70/30 or 50/50 combinations insulin and helps control hyperglycemia more effectively
4. Novalin 70/30

Insulins
DRUG CLASSAntidiabetic InsulinsHumalog (Lispro) – rapid actingRegular Humulin R – short actingHumulin N- intermediate actingGlargine (Lantus) – long actingPregnancy Category – BCONTRAINDICATIONSHypersensitivity to beef, prk, zimc, protamine insulinsCaution: Hypersensitivity
DOSAGEVaries according to client’s blood sugar
DRUG-LAB-FOOD INTERACTIONSDrugs: Increased hypoglycemic effect with aspirin, o: Increased oral anticoagulant, alcohol, oral hypoglycemics, beta-blockers, tricyclic antidepressants, MAOIs, tetracycline;Decreased hypoglycemic effect with thiazides, glucocorticoids, oral contraceptives, thyroid drugs, smoking
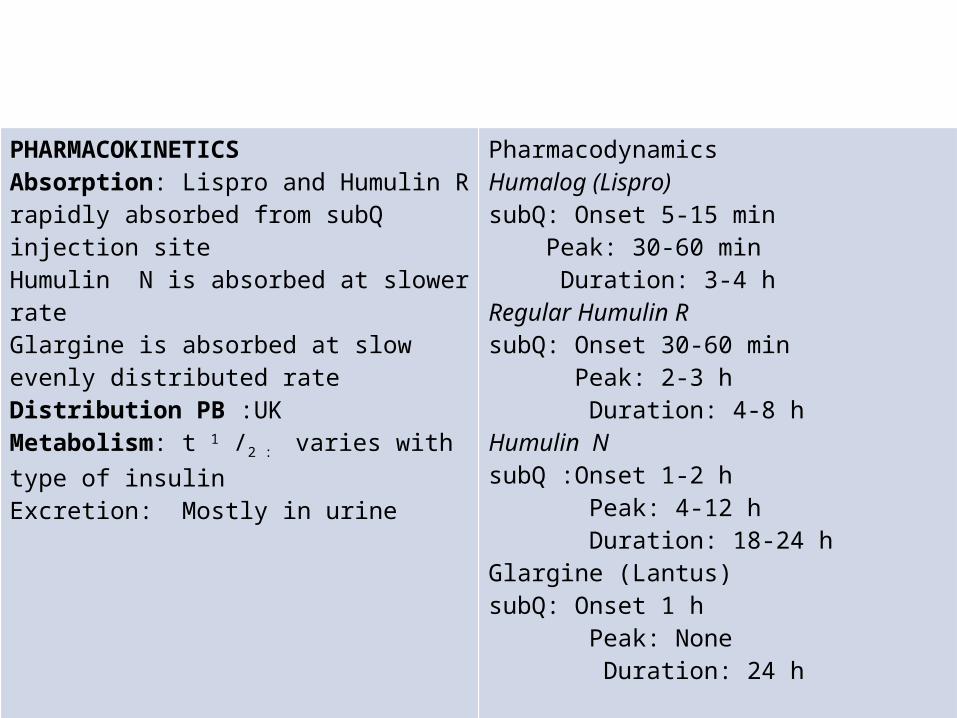
PHARMACOKINETICSAbsorption: Lispro and Humulin R rapidly absorbed from subQ injection siteHumulin N is absorbed at slower rateGlargine is absorbed at slow evenly distributed rateDistribution PB :UKMetabolism: t 1 /2 : varies with type of insulinExcretion: Mostly in urine
PharmacodynamicsHumalog (Lispro)subQ: Onset 5-15 min Peak: 30-60 min Duration: 3-4 hRegular Humulin R subQ: Onset 30-60 min Peak: 2-3 h Duration: 4-8 hHumulin NsubQ :Onset 1-2 h Peak: 4-12 h Duration: 18-24 h Glargine (Lantus)subQ: Onset 1 h Peak: None Duration: 24 h

Therapeutics EffectsTo control DM; to lower blood sugar
Mode of Action: Insulin promotes use of glucose by body cells
Side Effects: Confusion, agitation, tremors, headache, flushing, hunger, weakness, lethargy, fatigue, urticaria, redness, irritation or swelling at insulin injection site
Adverse Effects Tachycardia, palpitations, hypoglycemic reaction, rebound hypergylcemia (somogyi effect), lipodystrophyLife Threatening: Shock, anaphylaxis

Insulin Resistance
• antibodies develop over time in persons taking animal insulin
• Antibody development can cause insulin resistance and insulin allergy. This can slow the onset of insulin action and extend it’s duration action.
• Obesity can also be a causative factor of insulin resistance

Storage of Insulin
• Unopened insulin vials are refrigerated until needed• An open insulin vial may be kept at room temperature
for 1 month or in the refrigerator for 3 months• Opened insulin vials lose their strength after
approximately 3 months• Insulin vials should not be put in the freezer or places
in direct sunlight or in high temperature area• Refilled syringes should be stored in the refrigerator
and should be used within 1-2 wks
Sliding Scale Insulin Coverage
• Insulin may be administered in adjusted doses that depend an individual blood glucose test results
• When the diabetic client has extreme variances in insulin requirements( e.g. stress from nebulization, surgery illness, infection), adjusted dosing or sliding scale insulin coverage provides a more constant.

Insulin Pen Injection
• An insulin pen resembles a fountain pen. The pen contains a disposable needle and disposable insulin-filled cartridge
• The insulin filled pens are considered to deliver an insulin dose more accurate than the traditional 100 unit syringe and vial
• The capacity of these prefilled and reusable pens is 150-300 units.

Insulin Pumps1. Implantable Insulin Pumps
-is surgically implanted in the abdomen-it delivers basal insulin infusion and bolus with meals, administered either intraperitoneally or IV- With use of this, fewer hypoglycemic reactions occur and blood glucoses levels are controlled

2. Portable or External Insulin Pumps a.k.a Continous SubQ insulin infusion (CSII)-keeps the blood glucose levels as close to normal as possible- insulin pump is a battery-operated device that uses regular insulin, which is stored in a reservoir syringe placed inside the device. The syringe is the size of a pager and weighs about 3.5 oz

Intranasal Insulin -Administration of this is in experimental stage-causes a rapid onset and has a short duration of action-It’s dose is 10 times greater than a subQ dose

Insulin Jet Injection• Directly through
the skin in the fatty tissue
• Insulin is delivered in a high pressure
• Not indicated for children or older adults

Oral Antidiabetic Drugs ( Oral Hypoglycemic Drugs)
• A.k.a. hypoglycemics were discovered in 1950s• Persons with type 2 DM are indicated
Sulfonylureas- antidiabetics are chemically related to sulfonamides but lacking antibacterial activyt
- increases the insulin cell receptors

1. First Generation- short acting, intermediate-acting and long acting antidiabetics
2. 2ND Generation- have a greater hypoglycemic potency- have larger duration and cause fewer side effects- have less displacement potential from protein binding sites by other highly protein-bound proteins such as salicylates and warfarin - should not be used when there is liver or kidney dysfunction

Oral Antidiabetics
Generic Route and Dosage Uses and Considerations
First-Generation: Short Actingtobultamide(Orinase)
A: PO: 500-3000 mg/d in 2-3 divided doses
For managing type 2 Diabetes. Drug is chemically related to sulfonamides with no antiinfective effect. Hypoglycemic reaction may occur if overdosed. Pregnancy category: C; PB: >90%; ½; 4-7 h
First-Generation: Intermediate Actingacetohexamide (Dymelor)
tolazamide (Tolinase)
A: PO: 500-3000 mg/d before breakfast; max: 1.5 g/d
A: PO: 100-250 mg/d in 1-2 divided doses; max 1 g/d
For managing mild to moderately severe type 2 DM. Pregnancy Category : C ; PB:UK ;t1/2: 5-6 h
Same as acetohexamide. Diet and exercise should be a part of diabetic therapy. Duration of action is 10 to 20 hours.Pregnancy Category : C ; PB:90% ;t1/2: 7 h

First Generation: Long Actingchlorpropamide (Diabinase)
A: PO: Initially :100-250 mg/dMaint.: 100-500 mg/d in ½ divided doses; max: 750 mg/d
Second Generationglipzide (Glucotrol)
glyburide nonmicronized (Diabeta, Micronase)
A: PO: Initially|: 1.25-5 mg/d; maint. : 1.25-20 mg q.i.d./b.i.d.Max. : 20 mg/d
For managing type 2 DM: May be given to selected type1 clients for reducing insulin. Diet and Exercis should be a part of diabetic therapy. Duration of action is 24 h. May cause water and sodium retention.Pregnancy Category : C ; PB:95% ; t1/2: 36h
glyburide micronized (Glynase)
A: PO: Initially: 1.5-3 mg/d in AM; maint. : 3-4.5 mg/dMax. : 12 mg/d in 1 or 2 divided doses
For type 2 Diabetes. Same as glyburide nonmicronized

glimepiride (Amaryl) A: PO: Initially :1-2 mg a.c.Maint.: 1-4 mg/d a.c.; max: 8 mg/d a.c.
To treat clients with type 2 DM. Maybe used in combination with insulin. Can lower the 2 hour post-prandial glucose levels significantly. GI disturbance may occur.Pregnancy Category : C ; PB:99.5% ; t1/2: 5-9h
NonsulfonylureaseBiguanidesmetformin (Glucophage)
Inhibitorsacarbose (Precose)
A: PO: Initially :25 mg 1-3x daily with mealsmax: 150 mg/d<60 kg, 300 mg/d if > 60 kg
For managing hyperglycemia in type 2DM. Used as monotherapy or in combination with sulfonylurea.Pregnancy category: B; PB: UK;t½; 2 h
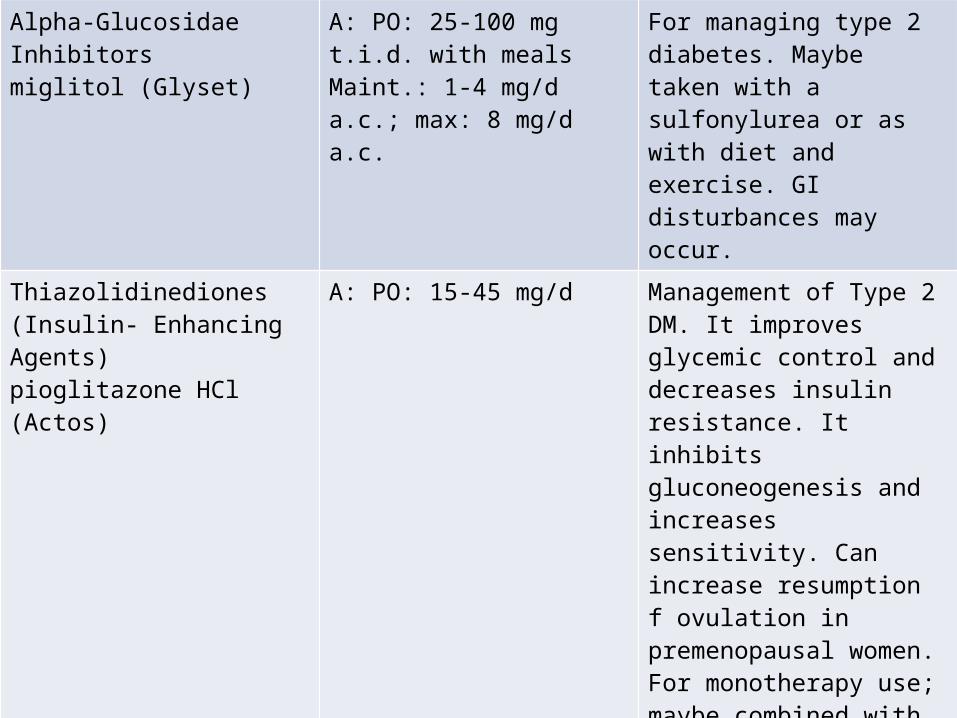
Alpha-GlucosidaeInhibitorsmiglitol (Glyset)
A: PO: 25-100 mg t.i.d. with mealsMaint.: 1-4 mg/d a.c.; max: 8 mg/d a.c.
For managing type 2 diabetes. Maybe taken with a sulfonylurea or as with diet and exercise. GI disturbances may occur.
Thiazolidinediones (Insulin- Enhancing Agents)pioglitazone HCl (Actos)
A: PO: 15-45 mg/d Management of Type 2 DM. It improves glycemic control and decreases insulin resistance. It inhibits gluconeogenesis and increases sensitivity. Can increase resumption f ovulation in premenopausal women. For monotherapy use; maybe combined with metformin. Diet and exercise and monitoring liver enzymes are suggested. Replaced troglitazone (Rezulin), which was removed from the market because it caused severe liver problems. Pregnancy Category : C ; PB:99.8% ; t1/2:3-4 h
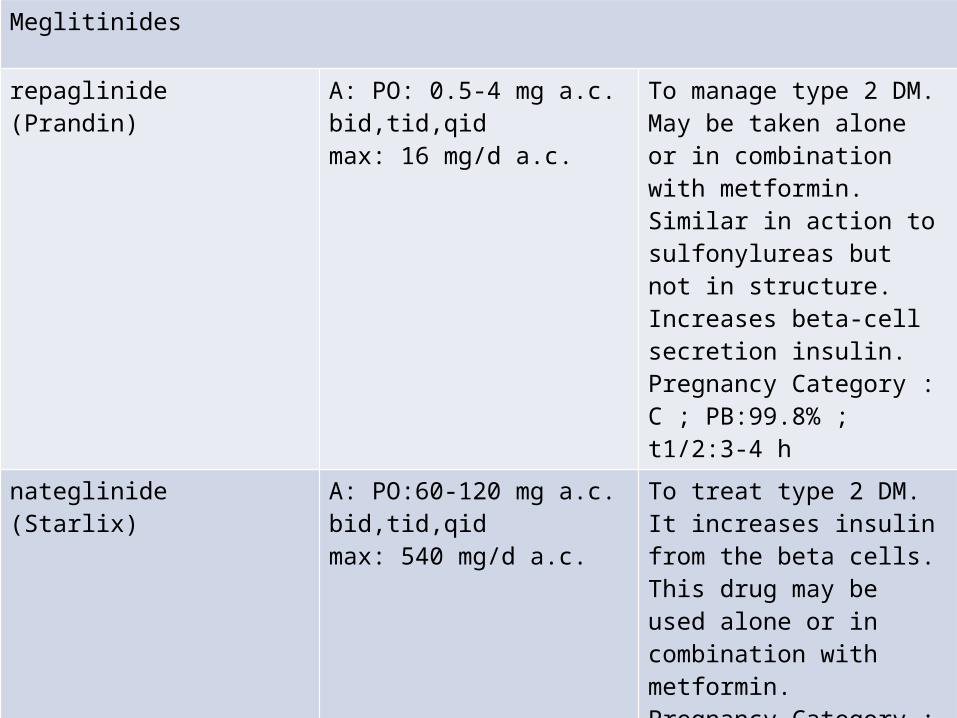
Meglitinides
repaglinide (Prandin) A: PO: 0.5-4 mg a.c. bid,tid,qidmax: 16 mg/d a.c.
To manage type 2 DM. May be taken alone or in combination with metformin. Similar in action to sulfonylureas but not in structure. Increases beta-cell secretion insulin.Pregnancy Category : C ; PB:99.8% ; t1/2:3-4 h
nateglinide (Starlix) A: PO:60-120 mg a.c. bid,tid,qidmax: 540 mg/d a.c.
To treat type 2 DM. It increases insulin from the beta cells. This drug may be used alone or in combination with metformin.Pregnancy Category : UK ; PB:98% ; t1/2:1.5 h

Fixed Combination of Oral Antidiabetic Drugs
glyburide/ metformin ( Glucovance)
A: PO: Initially:1.25/250 mg (glyburide/ metformin)daily or bid with meals. Increase dose at 2-wk intervals; maint: 2.5/500 mg or 5/500mg/d or bid with meals; max: 20/2000 mg/d
For managing type 2 DM. May be used when glucose or not controlled with either drug alone. Contraindicated for clients with renal insufficiency because of the risk of developing lactic acidosis. Pregnancy Category : B-D ; PB: UK ; t1/2: UK
Hyperglycemic Drugs
• Glucagon– A hyperglycemic hormone secreted by the alpha cells
of the islets of Langerhans– Increases blood sugar by stimulating glycogenolysis
(glycogen breakdown) in the liver– It protects the body cells (esp. in brain and retina), by
providing the nutrients and energy needed to maintain body function
– Available for parenteral use (subQ,IM, and IV)– Used to treat insulin-induced hypoglycemia

Diazoxide1. Oral Diazoxide (Proglycem)
-increases blood sugar by inhibiting insulin release from the beta cells and stimulating release of epinephrine (adrenaline) from adrenal medulla- not indicated for hypoglycemic reactions- used to treat chronic hypoglycemia caused by hyperinsulin because of islet cell cancer or hyperplasia-the parenteral form of diazoxide is prescribed for malignant hypertension- has a long half life and is highly CHIN bound.-it’s onset of action is 1 hr and the duration of action is 18 hrs

Other Agents
• Exenatide (Byetta)- under new classification of drugs known as mimetic that improves beta-cell responsiveness, which improves glucose control in people with type 2 DM
Enhance insulin secretion, increase beta cell responsiveness, suppress glucagon secretion, slow gastric emptying and reduce food intake
A/E: headache, dizziness, nausea, vomiting and diarrhea

Pramtintide acetate (Symlin)
• For adults with type 1 and 2 DM• Improve postprandial glucose control in diabetic
patients who are using insulin but unable to achieve and maintain glucose control
• Suppress glucagon secretion, slow gastric emptying and modulate appetite by including satiety
• A/E : dizziness, anorexia, nausea, vomiting and fatigue• Administered via subQ before meals in the abdomen
or thigh.


![Mechanism of antidiabetic effects of Plicosepalus Acaciae ......their efficacy as antidiabetic drugs [6]. Bamane et al. [7] reported that methanolic extracts of Plicosepalus acacia](https://img.pdfslide.us/doc/110x75/60db669939dd7a66f77f8583/mechanism-of-antidiabetic-effects-of-plicosepalus-acaciae-their-efficacy.jpg)