Embed Size (px)
Citation preview
![Page 1: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/1.jpg)
![Page 2: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/2.jpg)
![Page 3: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/3.jpg)
Anticancer Therapeutics
![Page 4: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/4.jpg)
![Page 5: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/5.jpg)
Anticancer Therapeutics
From Drug Discovery to Clinical Applications
ADAM TODDNewcastle University, UK
PAUL W. GROUNDWATERUniversity of Sydney, Australia
JASON H. GILLNewcastle University, UK
![Page 6: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/6.jpg)
This edition first published 2018© 2018 John Wiley & Sons Ltd
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by law. Advice on how to obtain permission to reuse material from this title is available at http://www.wiley.com/go/permissions.
The right of Adam Todd, Paul W. Groundwater and Jason H. Gill to be identified as the authors of this work has been asserted in accordance with law.
Registered Office(s)John Wiley & Sons, Inc., 111 River Street, Hoboken, NJ 07030, USAJohn Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
Editorial OfficeThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
For details of our global editorial offices, customer services, and more information about Wiley products visit us at www.wiley.com.
Wiley also publishes its books in a variety of electronic formats and by print‐on‐demand. Some content that appears in standard print versions of this book may not be available in other formats.
Limit of Liability/Disclaimer of WarrantyIn view of ongoing research, equipment modifications, changes in governmental regulations, and the constant flow of information relating to the use of experimental reagents, equipment, and devices, the reader is urged to review and evaluate the information provided in the package insert or instructions for each chemical, piece of equipment, reagent, or device for, among other things, any changes in the instructions or indication of usage and for added warnings and precautions. While the publisher and authors have used their best efforts in preparing this work, they make no representations or warranties with respect to the accuracy or completeness of the contents of this work and specifically disclaim all warranties, including without limitation any implied warranties of merchantability or fitness for a particular purpose. No warranty may be created or extended by sales representatives, written sales materials or promotional statements for this work. The fact that an organization, website, or product is referred to in this work as a citation and/or potential source of further information does not mean that the publisher and authors endorse the information or services the organization, website, or product may provide or recommendations it may make. This work is sold with the understanding that the publisher is not engaged in rendering professional services. The advice and strategies contained herein may not be suitable for your situation. You should consult with a specialist where appropriate. Further, readers should be aware that websites listed in this work may have changed or disappeared between when this work was written and when it is read. Neither the publisher nor authors shall be liable for any loss of profit or any other commercial damages, including but not limited to special, incidental, consequential, or other damages.
Library of Congress Cataloging‐in‐Publication Data
Names: Todd, Adam, 1982– author. | Groundwater, Paul W., author. | Gill, Jason H., 1973– author.Title: Anticancer therapeutics : from drug discovery to clinical applications / Dr. Adam Todd, Professor Paul W. Groundwater, Dr. Jason H. Gill.Description: First edition. | Hoboken, NJ : Wiley, 2017. | Includes bibliographical references and index. | Identifiers: LCCN 2017024305 (print) | LCCN 2017025861 (ebook) | ISBN 9781118696217 (pdf) | ISBN 9781118696200 (epub) | ISBN 9781118622124 (cloth) Subjects: | MESH: Neoplasms–drug therapy | Neoplasms–physiopathology | Antineoplastic Agents | Drug DiscoveryClassification: LCC RC270.8 (ebook) | LCC RC270.8 (print) | NLM QZ 267 | DDC 616.99/4061–dc23LC record available at https://lccn.loc.gov/2017024305
Cover design by WileyCover image: (right) © Xray Computer/Shutterstock; (left top & left buttom) Courtesy of Adam Todd, Paul W. Groundwater & Jason H. Gill
Set in 10/12pt Warnock by SPi Global, Pondicherry, India
10 9 8 7 6 5 4 3 2 1
![Page 7: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/7.jpg)
FOR OUR CHILDREN
![Page 8: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/8.jpg)
![Page 9: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/9.jpg)
vii
Preface xi
Section 1: Introduction 1
1.1 The Global Burden of Cancer 3 References 11
1.2 Cancer Staging and Classification 131.2.1 Benign Tumour (or neoplasm) 131.2.2 Malignant Tumour (or cancer) 141.2.3 Tumour Nomenclature and Classification 141.2.4 Cellular Differentiation and Tumour Grade 211.2.5 Tumour Invasion and Metastasis 241.2.6 Clinical Staging of Cancer 26 References 36
1.3 Cellular and Molecular Basis of Cancer 391.3.1 Oncogenes 401.3.2 Tumour Suppressor Genes 451.3.3 Role of Epigenetics and Gene Promoter Regulation in Tumourigenesis 491.3.4 Multistage Tumourigenesis 531.3.5 Oncogene Addiction 541.3.6 Hallmarks of Cancer 551.3.7 Principles of Cancer Treatment 73 References 77
Section 2: The Anticancer Agents 81
2.1 Agents Which Act Directly on DNA 832.1.1 Nitrogen Mustards and Nitrosoureas 83 References 962.1.2 Temozolomide 98 References 106
Contents
![Page 10: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/10.jpg)
Contentsviii
2.1.3 Platinum‐containing Agents 108 References 1182.1.4 Gemcitabine 120 References 1282.1.5 Camptothecin and Its Analogues 128 References 1392.1.6 Podophyllotoxins 141 References 1502.1.7 Anthracyclines 151 References 1602.1.8 Epigenetic Targeting Agents 162 References 177
2.2 Antimetabolites 1812.2.1 Cytarabine 181 References 1832.2.2 Methotrexate 184 References 1952.2.3 5‐Fluorouracil 196 References 2052.2.4 6‐Mercaptopurine 206 References 210
2.3 Antimicrotubule Agents 2112.3.1 Taxanes 211 References 2242.3.2 Vinca Alkaloids 225 References 231
2.4 Anti‐hormonal Agents 2332.4.1 Bicalutamide 233 References 2392.4.2 Tamoxifen 240 References 2472.4.3 Anastrozole 248 References 254
2.5 Kinase Inhibitors 2572.5.1 Discovery 2572.5.2 Synthesis 2622.5.3 Mode of Action 2672.5.4 Mechanism of Resistance 2682.5.5 Adverse Drug Reactions 268 References 271
![Page 11: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/11.jpg)
Contents ix
Section 3: The Cancers 275
3.1 Breast Cancer 277 Key points 2773.1.1 Epidemiology 2773.1.2 Presentation 2793.1.3 Diagnosis 2823.1.4 Staging 2833.1.5 Treatments 285 References 289
3.2 Colorectal Cancer 293 Key points 2933.2.1 Epidemiology 2933.2.2 Presentation 2943.2.3 Diagnosis 2963.2.4 Staging 2983.2.5 Treatments 299 References 303
3.3 Leukaemia 307 Key points 3073.3.1 Epidemiology 3073.3.2 Presentation 3103.3.3 Diagnosis 3113.3.4 Staging 3133.3.5 Treatments 314 References 319
3.4 Lung Cancer 323 Key points 3233.4.1 Epidemiology 3233.4.2 Presentation 3273.4.3 Diagnosis 3273.4.4 Staging 3303.4.5 Treatments 330 References 337
3.5 Oesophageal Cancer 339 Key points 3393.5.1 Epidemiology 3393.5.2 Presentation 3403.5.3 Diagnosis 3413.5.4 Staging 3443.5.5 Treatments 346 References 350
![Page 12: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/12.jpg)
Contentsx
3.6 Ovarian Cancer 353 Key points 3533.6.1 Epidemiology 3533.6.2 Presentation 3543.6.3 Diagnosis 3563.6.4 Staging 3573.6.5 Treatments 357 References 363
3.7 Pancreatic Cancer 367 Key points 3673.7.1 Epidemiology 3673.7.2 Presentation 3683.7.3 Diagnosis 3703.7.4 Staging 3713.7.5 Treatments 373 References 375
3.8 Prostate Cancer 379 Key points 3793.8.1 Epidemiology 3793.8.2 Presentation 3813.8.3 Diagnosis 3823.8.4 Staging 3843.8.5 Treatments 387 References 391
3.9 Skin Cancers 393 Key points 3933.9.1 Epidemiology 3933.9.2 Presentation 3943.9.3 Diagnosis 3953.9.4 Staging 3963.9.5 Treatments 399 References 403
3.10 Testicular Cancer 405 Key points 4053.10.1 Epidemiology 4053.10.2 Presentation 4073.10.3 Diagnosis 4073.10.4 Staging 4093.10.5 Treatments 409 References 414
Index 417
![Page 13: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/13.jpg)
xi
By the year 2020 estimates suggest that almost one in two of us will suffer from cancer at some stage in our lives [1]. This is an understandably frightening statistic, especially when we consider that, globally, cancer results in more deaths than HIV/AIDS, tuber-culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3 million by 2025) and 8.2 million people died from cancer [3]. On a more positive note, however, increasing numbers of people are now surviving cancer; in 2012 an estimated 32.5 million people were alive 5 (or more) years after their original diagnosis and by 2020, it is thought almost 40% of people suffering from cancer will not die from the disease, but from another cause, such as cardiovascular disease [1,3].
These days, one of the greatest temptations for any patient who has just been diag-nosed with cancer must be to search the internet for information relating to survival rates. There are many excellent resources for people who have cancer, but until a patient’s cancer has been fully classified, statistics are meaningless and, even after stag-ing, median survival rates are the best which can be offered. In addition, an internet search for news items on cancer cures will result in many hits, but these should be tem-pered by the knowledge that cancer refers to a diverse group of diseases, affecting dif-ferent organs and systems of the body, and a single cure (or even one for more than one group of related cancers) is, therefore, extremely unlikely.
Since its use was first described over 74 years ago, chemotherapy has contributed to significant improvements in survival rates for patients suffering from a range of differ-ent cancers, with a number of cancers now considered, and even managed, as long‐term conditions as opposed to acute illnesses. A good example of this is prostate cancer; through the use of chemotherapy, men now live with this condition for many years without the cancer affecting their quality of life. Unfortunately, however, this progress is not evident for all cancers and, as we shall see, the survival rates for pancreatic cancer, to take one example, have remained roughly the same for many years and the prognosis for patients with this disease is still incredibly poor.
The complexity of cancer mirrors the complexity of the human body itself. The improvement in survival rates (which are required to address the increasing numbers of us who will get cancer) relies on advances in our understanding of normal cellular func-tioning and how these processes can go wrong in the development of cancer. It is these types of advances that have informed the treatment regimens (comprising combina-tions of surgery, radiotherapy, and chemotherapy) and resulted in increased survival
Preface
![Page 14: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/14.jpg)
Prefacexii
rates for many different cancers. For example, in the UK, in 1992, 21% of patients diagnosed with cancer died from another cause; by 2010 this figure had risen to 35%, and by 2020 it is projected to reach 38% [1]. These statistics are very encouraging and show the progress we have made against this hugely challenging and complex disease. A vast array of people, including medicinal chemists, molecular biologists, clinical trialists, health economists, and oncologists, are working to continue this significant progress. It is quite unusual to make a one‐off landmark discovery that significantly changes the way cancer is managed overnight (although this can happen and a good example is the discovery of platinum therapy in the treatment of testicular cancer). What is more common is that, through high‐quality research and robustly designed clinical trials, we make small, but important steps in our understanding of how to best manage this disease.
In Section 1 of this book we give an introduction to the global burden of cancer, can-cer classification, and the cellular and molecular basis of cancer. In Section 2 we describe the different classes of anticancer agents and include chapters on the discovery, synthe-sis, mechanism of action, and resistance for each class. In Section 3 we bring everything together and explore the clinical management of ten different cancers; importantly in this section, we consider the various screening approaches that may, or may not, be taken to help improve survival. We hope that the organisation of the book helps you to appreciate the sheer complexity of anticancer therapeutics and that cancer treatment is not – and never will be – a one size fits all approach. Like any book on anticancer agents, this text presents a snapshot of the agents used clinically at the time. There is no doubt that with the rapid progress being made in large‐scale data‐rich biology, yet more significant advances will be made against this disease, and that future texts (not necessarily further editions of this one) will have many more new anticancer agents (and targets) to discuss.
References
1 https://www.macmillan.org.uk/_images/cancer-statistics-factsheet_tcm9-260514.pdf (last accessed 21.8.2017).
2 Moten A, Schafer D, Ferrari M. Rededefining global health priorities: Improving cancer care in developing settings. J Glob Health. 2014, 4, 010304.
3 https://publications.cancerresearchuk.org/downloads/product/CS_REPORT_WORLD.pdf (last accessed 21.8.2017).
![Page 15: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/15.jpg)
1
Section 1
Introduction
![Page 16: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/16.jpg)
![Page 17: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/17.jpg)
3
Anticancer Therapeutics: From Drug Discovery to Clinical Applications, First Edition. Adam Todd, Paul W. Groundwater and Jason H. Gill. © 2018 John Wiley & Sons Ltd. Published 2018 by John Wiley & Sons Ltd.
1.1
In order for us to understand cancer and its treatment it is obviously important to define what is meant by the term ‘cancer’. The word is credited to Hippocrates, the Greek physician (460–370 BC), who used the words carcinos and carcinoma to describe non‐ulcer and ulcer‐forming growths. These words in Greek derive from the word for crab, and their use is believed to be due to the fact that the spreading nature and cellular projections of the growths observed were reminiscent of the shape of a crab. Later changes resulted in the use of the words cancer (Latin for crab) and oncos (Greek for swelling) to describe tumours, terms attributed to the Roman physicians, Celsus (28–50 BC) and Galen (130–200 AD), respectively. Interestingly, we still use all of these words to define malignancy, to discuss a tumour’s histological appearance, and as a descrip-tion for medical specialists in this area (oncologists).
Although described as a single condition, cancer is actually a family of hundreds of different diseases. The distinction between the different types of cancer is extremely important since their treatment, management, and outcomes for the patient are very diverse (as we shall see in the later sections). Additionally, even within a single cancer ‘type’ there are significant issues with regards to treatment options and patient progno-sis, as individual cancers of the same type can behave very differently from one another. The same can be said for the global distribution of cancer; there are different profiles of cancer types in different geographical regions, with different causative factors, different treatment options and successes, and different prognostic and survival rates. Invariably, across the globe, some cancer types and some patients will achieve some degree of remission, and some will be cured, but others will not, with treatment in their case focusing on extending life expectancy.
Cancer is a major worldwide public health problem, as indicated by the World Health Organization (WHO) identifying cancer as one of four leading threats to human health and development (the others being cardiovascular disease, chronic respiratory diseases, and diabetes) in 2008 [1]. In 2012, cancer incidence1 was estimated at 14.1 million people, cancer mortality2 was predicted at 8.2 million deaths, and cancer
The Global Burden of Cancer
1 Incidence is the number of new cases arising in a given time period in a specified population, presented as the absolute number of cases annually or the ‘age‐standardised’ rate per 100,000.2 Mortality is the number of deaths in a given time period in a specified population, presented as absolute number of deaths annually or the ‘age‐standardised’ rate per 100,000.
![Page 18: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/18.jpg)
1 Introduction4
prevalence3 was estimated at 32.6 million people [2]. When we just consider these numbers it is difficult to appreciate the scale of the problem, and it is therefore impor-tant to put this into context. For instance, in 2012 the estimated population of the world was 7.05 billion people, and the risk of dying4 from cancer before age 75 was 10.5% [2].
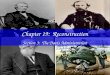
Cancer is not a modern disease, being first identified and described around 5,000 years ago. What may be unexpected is that the frequency and occurrence of cancer are higher nowadays than about a century ago despite significant advances in cancer diag-nosis, treatment, and management over this period. So how can that be? Are we seeing an increase in cancer cases? Are we really making progress with the treatment of these diseases? The answers to these questions relate to the way we consider and view cancer, and have a direct relationship to factors and successes outside of the cancer field. A major contributory factor in cancer appearing to become an increasing cause of mor-tality over the past century is our achievements in the treatment of other life‐threaten-ing diseases. In the early 1900s cancer accounted for a small proportion of deaths, with the majority of deaths being due to infectious diseases such as pneumonia, tuberculosis, and polio. Since this time, medical progress and improvements in public health and hygiene have led to the significant reduction and elimination of infection as a major cause of death. This effect can be observed if we compare differences in cancer inci-dence and mortality in different regions of the world, particularly developed versus developing countries. In the developed countries of Europe, treatment for infectious diseases is highly successful and cancer appears to be a major mortality factor, for exam-ple mortality rates are greater than 150 per 100,000 and incidence rates are greater than 300 per 100,000 in Northern and Western Europe. We can compare this to the develop-ing countries of Middle and Northern Africa, where infectious diseases are a major factor and treatment success is poor; here cancer mortality rates are below 90 per 100,000 and incidence rates are below 130 per 100,000 (Figure 1.1.1).
As we can clearly see from Figure 1.1.1, the incidence of cancer is highest in Australia/New Zealand, but is also higher than the global rate (World) in Europe and North America. The mortality rates (which are dictated by the most prevalent can-cers found in each of the regions) partly reflect the incidence rates, but notable exceptions are Melanesia (Western Pacific), which has an incidence rate below the global average, but a mortality rate near the top, and its near neighbours Australia/New Zealand, which have the highest incidence per 100,000 but are below global average mortality. The most common cancer‐related death in Australia is lung can-cer (19%), followed by bowel cancer (11%); in Melanesia, cervical, breast, liver and lip/oral cavity cancers are the most common causes of cancer‐related death (10%). Another significant factor which is related to the apparent increase in the rates of cancer in modern times is the fact that, as a population, we are living longer, with a subsequent steady increase in the global population; better lifestyles and disease management have resulted in improved life expectancy. In 1970 the median age5 of the global population was 22 years, which increased to 29 years by 2010 and is predicted
3 The number of people diagnosed with cancer in the preceding 5 years who were still alive in 2008.4 In other words, at current cancer rates, just over 10 in every 100 newborn babies would be expected to die from cancer by the age 75.5 The age that divides a population into equal halves.
![Page 19: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/19.jpg)
1.1 The Global Burden of Cancer 5
to reach 38 years by 2050. Additionally, the number of people aged 60 years and over in 2050 is predicted to increase threefold, to 2 billion. With respect to cancer, by 2030 it is predicted that, annually, there could be 27 million new cancer cases and 17 million cancer‐related deaths worldwide. Our extended life expectancy and improved can-cer survival prevalence rates are thus an indirect consequence of the elimination of other life‐threatening diseases, which has propelled cancer into the top four major health concerns.
0 50 100 150 200 250 300 350
Australia/New Zealand
North America
Western Europe
Northern Europe
Eastern Asia
World
Southern Africa
Melanesia
South-Eastern Asia
Central America
South-Central Asia
Western Africa
Incidence per 100,000
(a)
0 20 40 60 80 100 120 140
Eastern Asia
Melanesia
Southern Africa
Northern Europe
North America
Western Europe
World
Australia /New Zealand
South-Eastern Asia
Central America
Western Africa
South-Central Asia
Mortality per 100,000
(b)
Figure 1.1.1 Estimated age‐standardised (a) cancer incidence and (b) cancer‐related mortality rates per 100,000 population in regions of the world in 2012 [3]. Northern Europe incorporates the UK and Scandinavia; South‐Central Asia incorporates Iran, Iraq, Afghanistan, Pakistan, and India; Eastern Asia incorporates China, Taiwan, Japan, North Korea, South Korea, and Mongolia; South‐eastern Asia incorporates Laos, Myanmar, Philippines, Thailand, Vietnam, Malaysia, Singapore, and Indonesia. Source: Torre 2012 [3].
![Page 20: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/20.jpg)
1 Introduction6
But why are the number of cancer cases apparently rising? If we accept that the increased percentage of deaths attributable to cancer is due to a shift in the dynamic balance because of significantly reduced figures for other diseases, such as infec-tion, then should we not just see a reduced number of total deaths reported, but with approximately the same number of cancer‐related deaths? Although in prin-ciple this point should be true, what it fails to account for is the fact that, as a population, we are living longer. We know that there is a significant correlation between increasing age and the number of cancer cases, for which the underlying principles will be discussed later. Put simply, the continued growth and ageing of the World population means that people are around longer and so there is a greater opportunity for cancer to develop. Taken together, we can appreciate that these underlying factors have propelled cancer to become a major health concern glob-ally. Nevertheless, recent studies have begun to indicate improvements in combat-ing cancer as a consequence of improved lifestyle, earlier detection, or better treatments. For instance, the overall risk in Europe for being diagnosed with can-cer has now reportedly stabilised relative to previous years (estimated at an age‐standardised rate of 356 people per 100,000), and the overall risk of dying from cancer has shown a decline (estimated to be 168 per 100,000, with variations dependent on tumour type and country) [4].
We now know that cancer is a major disease, with clear global differences in terms of incidence, survival, and related‐deaths. However, it is worthwhile at this point to fly a flag of caution in relation to this data, with particular reference to evaluation and inter-pretation. In the previous section it was identified that cancer incidence is stabilising and cancer deaths are declining in Europe, which is true based on the data presented. While this overarching change is positive, it does not identify data for specific cancers or European countries, and does not report the degree by which the risk of cancer‐related mortality varies between these factors. This highlights a major consideration when evaluating or analysing cancer data, particularly in the extraction of the specific information you require. As with all things, the quality and utility of the information gained is only as good as the data entered into the system. We are by no means suggest-ing that this data is uninformative, misleading, or indeed incorrect, but merely indicat-ing the caution that should be adopted when considering this task. Careful thought and consideration must be applied when drawing conclusions from these observations because of inter‐country differences in data reporting, documentation, reporting practices, and pathological evaluations. It should be no surprise that the majority of reported studies concentrate on developed areas, such as Europe and the USA, where there are dedicated and well‐developed cancer registries and standardised reporting structures for cancer. Therefore, in order to make valid conclusions and comparisons, it is important to confirm data reliability and that appropriate analyses and statistical evaluation have been applied, to ensure the figures are not skewed by confounding factors. Incomplete documentation, such as the description of ‘lung cancer’ without specification of histological type, has significant implications for reporting and conse-quent analyses. Similarly, there can be a lack of follow‐up data or inconsistencies in reporting structures between one area and the next. Nevertheless, when used correctly, this data is invaluable in assessing the causative and progressive factors associated with a particular cancer type, and more importantly from a pharmaceutical perspective, for evaluating treatment options and successes.
![Page 21: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/21.jpg)
1.1 The Global Burden of Cancer 7
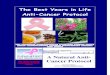
Over the past 40 years cancers affecting the lung, breast, bowel, stomach, and prostate were the types most commonly diagnosed, with varying levels of treatment success and prognostic outcomes. This has not changed significantly, with the most common can-cers globally being lung, female breast, colorectal, and prostate, accounting for close to four in ten cancers (Figure 1.1.2) [2,5]. If we consider Europe alone, the situation is slightly different, with cancers of the female breast, colorectal region, prostate, and lung representing almost half of the overall burden of cancer in this region [4]. The differ-ences in cancer types are a reflection of the different geographical and environmental factors across the World, with stomach being a top‐four cancer type globally, but not in Europe, probably reflecting dietary factors in Asia. The higher incidence of prostate cancer in Europe, as opposed to the global picture, may also reflect dietary and lifestyle factors in developed versus developing regions of the World. This gender‐specific can-cer also feeds into differences reported globally, wherein the incidence of cancer per se is more than a fifth higher in males than females, with male and female incidence rates varying by three‐ to four‐fold across different regions of the globe. In a similar pattern to that observed globally for cancer incidence there are also marked differences with respect to cancer deaths. The four most common cancer types in relation to cancer‐related deaths globally are lung, stomach, liver, and colorectal, which are responsible for 45% of global cancer mortality. This pattern is again different when analysed specifically for the UK, where lung, colorectal, breast, and prostate cancers account for almost half of the total number of cancer‐related deaths.
0 500,000 1,000,000 1,500,000 2,000,000
Lung (13.0%)Breast (11.9%)
Colorectum (9.7%)Prostate (7.8%)Stomach (6.8%)
Liver (5.6%)Cervix (3.8%)
Oesophagus (3.2%)Bladder (3.1%)
Non-Hodgkin lymphoma (2.7%)Leukaemia (2.5%)
Pancreas (2.4%)Kidney (2.4%)Uterus (2.3%)
Lip/Oral cavity (2.1%)Thyroid (2.1%)
Brain/CNS (1.8%)Ovary (1.7%)
Malignant melanoma (1.7%)Gallbladder (1.3%)
Number of new cases
Figure 1.1.2 Estimates of the 20 most commonly diagnosed cancers Worldwide in 2012 (http://globocan.iarc.fr/Pages/fact_sheets_population.aspx). CNS, central nervous system.
![Page 22: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/22.jpg)
1 Introduction8
The incidence of cancer in a particular region, country, or culture can be used to indicate or outline potential underlying contributory factors to those specific cancers. In simple terms, we could attribute variations in cancer incidence between different populations or geographical regions purely on genetic differences between these varying populations. However, we now know that this viewpoint is too simplis-tic and there is a second contributory dimension involving the variation in environ-mental factors and subsequent exposure profiles of the inhabitants. There is now a clear argument to directly link specific environmental, dietary, recreational and industrial factors to the development or promotion of cancer based upon compari-sons of cancer incidence in different geographical regions. For instance, a high inci-dence of liver cancer was previously identified in Mozambique, which was suggested to be due to a dietary factor of some sort. One possible cause identified related to the way in which peanuts were stored, which permitted growth of aflatoxin mould. In the years and decades following a change in practise for peanut storage, the incidence of liver cancer declined in this region, strongly supporting a link between these fac-tors. This example provides a straightforward indication of the existence of cancer‐causing (carcinogenic) factors, but pessimistically could also indicate a genetic link related to food intolerances or other risk factors specific to this population.
A stronger validation for the co‐existence of genetic and environmental risk fac-tors for cancer development is provided through studies of migrant populations. This is easily evaluated through the study of cancer incidence in immigrants who have settled with a new lifestyle in a new country. One such example, in support of the promotion of cancer development by environmental factors, is the fact that Japanese immigrants in the USA were shown to have a similar incidence of colon cancer to Americans, but five times that of those still living in Japan, indicating an environmental driver for colon cancer development over that provided by the genetic background. Conversely, stomach (gastric) cancer is reportedly higher in Japan than the UK or USA. At face value it could be claimed this is due to the differ-ent genetic profiles of these populations. However, in reality, studies of the inci-dence of gastric cancer of Japanese individuals relocated from Japan to the USA supported the environmental contribution to cancer development. Within one to two generations, the incidence of gastric cancer in the Japanese‐American popula-tion shifted towards that of America. In this case, the carcinogenic factor was believed to be due to a change in salt preservation of food, which was high in Japan in comparison to the USA.
Whereas (unfortunately) it is not within the scope of this particular section to describe a multitude of risk factors, it is pertinent to briefly discuss tobacco smoking and its clear links to the development of cancer, particularly lung cancer. Tobacco smoking is unquestionably a major environmental and carcinogenic risk factor for lung cancer, both directly to the smoker and indirectly to bystanders in the form of passive smoke. The global frequency of lung cancer has increased more than tenfold since 1930, making this cancer the leading cause of cancer death in Europe in 2012 and the most common malignant disease in the World for several decades. This rise in lung cancer incidence is directly attributable to increased use of tobacco, particu-larly cigarettes [4]. However, an important criterion when comparing the effect of an agent upon cancer development is the time taken for the effect to be observed. In this case, there is an approximately 20‐year lag in the relationship between incidence
![Page 23: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/23.jpg)
1.1 The Global Burden of Cancer 9
of people smoking and the development of lung cancer. This lag‐time is a reflection of the cellular basis of cancer development (which we will discuss later), involving a multistep developmental process and the requirement for specific hallmarks of can-cer to be satisfied. The existence of a lag‐time is evident through studies of differ-ences in smoking habits within a specific population, which in the case of smoking and lung cancer can be evaluated via comparison of males and females. Whereas tobacco smoking in males began to increase around the First World War (1910s to 1920s), it only really became popular in females during and after the Second World War (1940s). Whereas the incidence of lung cancer in males began to increase in the 1930s to the 1940s, that in females increased around the 1960s, reinforcing an approximately 20‐year lag period.
In recent years a clear shift has been made in many populations from the smoking of cigarettes towards the use of electronic cigarettes, primarily on the communicated improved health benefits of the latter over the former, and improved awareness of can-cer risk factors associated with smoking. It will be interesting to see if this manifests in a reduction in lung (and other smoking‐related) cancers over time.
As you will now appreciate, there is a huge level of complexity and uncertainty about the factors contributing to cancer, and widespread differences in the prevalence and aetiology of specific cancer types. However, based upon the information discussed above, we now understand there are multiple external factors driving the development of cancer. On face value this would strongly imply a direct causative relationship between these carcinogenic (cancer‐causing) factors and the development of cancer. Is this not true? It is without doubt that there is an environmental link in cancer develop-ment, with many epidemiological studies providing strong evidence in support. The remaining pieces in the puzzle are, therefore, whether these carcinogenic factors are actually causative, catalysts of the disease process, central and indispensable factors, or purely coincidental to the whole process. Second, it remains to be shown how these carcinogenic factors actually manifest themselves in the alteration of cell behaviour (how they become tumourigenic and malignant). The answer is actually fairly straight-forward (now many studies over many years have been conducted): cancer is a conse-quence of genetic change and reprogramming of cell behaviour, and these carcinogenic factors drive and/or promote these changes. This, therefore, implies that the environ-mental and carcinogenic contributors are predominantly catalysts and promoters for cancer development.
Although it is clear that environment and lifestyle are major contributors and risk factors for cancer development, it is all too easy to describe many practices, activities, and environmental parameters as being tumourigenic or carcinogenic. Consequently, we must be realistic about these causative factors for cancer. Cancer of the colon, for example, showed a rise in developed countries in the later part of the 20th century. This has been linked to a decline in healthy diets, an increase in take‐away and convenience foods, and a subsequent increase in obesity. In support of this, it is now well reported that diets low in fruit and vegetables, and high in red meat, processed food, and fat result in an increased risk of colorectal cancer [4]. However, the rise in colorectal cancer over the same time period would also support a relationship between this cancer to the invention and use of the personal computer and electronic games machines. Whereas a clear link can be seen between colon cancer and diet, it is unlikely that the use of the per-sonal computer is the major causative factor for this disease (although a lack of exercise,
![Page 24: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/24.jpg)
1 Introduction10
parallel consumption of unhealthy snacks, and computer‐related dormancy could be contributory factors!). Consequently, risk factors and carcinogenic stimuli have also to be biologically (or scientifically) plausible. The caveat, as can be drawn from the colorectal‐electronic gaming relationship, is that the risk–disease link is commonly not linear or straightforward, with several additional contributory or supporting factors also playing a role in the complex intertwined pathogenic networks. In this particular case, there is a lot to be said for exercise and physical activity, a balanced diet, fresh fruit and vegetables, and weight management. In reality, this is not a new concept, reflecting normal practices from the earlier parts of the 20th century. The underlying culprit could thus be assumed to be changes in lifestyle, social environment, retail convenience, and attitudes over the past 50 or so years.
As well as linking particular risk factors to specific cancer types, a change in the inci-dence of cancer in a particular population also provides clues to its aetiology. This is especially so for ‘rare’ cancers which may appear in greater numbers in a particular place or sub‐population. An example would be several cases of acute leukaemia occur-ring in close proximity in a particular town within a short space of time, indicating a strong environmental or personal exposure factor, such as radiation.
The important message from these epidemiological studies (and several thousand more) is the relationships between human cancers and environmental risk factors, suggesting that many cancers could, in principle, be prevented through identification, elimination, and modification of causative carcinogenic factors. This ‘preventative’ approach to cancer has probably become the highest priority initiative in the cancer research field over the past couple of decades, and remains so to this date. Based on this, can we therefore prevent cancer developing in the first place? Before answering this question it is important to consider the role environmental factors play in the process. Based on the assumption that environmental factors play a major role in approximately 75% of all cancers, a baseline intrinsic (genetic) cause of cancer must indeed exist. This would suggest that we can, at least, reduce the rate of cancer devel-opment through control of risk factors, potentially to a rate wherein an individual dies of another factor before the cancer is detectable or problematic. However, there is strong evidence to suggest environmental factors primarily promote and accelerate cancer development rather than cause the initiating event, especially when we remember cancer is a genetic disease. This latter concept would thereby support the hypothesis that the multistep nature of carcinogenesis is merely fuelled by environmental factors, with the cancer developing eventually (albeit potentially beyond the lifetime of the individual). So to address the question ‘Can we completely prevent cancer formation?’ we need to consider the ‘cancer initiating’ genetic event, the pre‐existence of genetic changes, and the contribution of environmental carcinogenic factors, but in essence the answer is a combination of yes and no.
Cancer awareness and prevention is also now becoming a major initiative through health‐promotion campaigns, improved education of public health practitioners, and the changing role of the health practitioner within the community setting.
While it is clear that tackling cancer worldwide will remain one of the major chal-lenges in the 21st century, in addition to preventative strategies, advances in diagnosis and treatment will also hopefully significantly reduce the impact of these diseases.
![Page 25: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/25.jpg)
1.1 The Global Burden of Cancer 11
References
1 WHO. 2008–2013 action plan for the global strategy for the prevention and control of noncommunicable diseases:prevent and control cardiovascular diseases, cancer, chronic respiratory diseases and diabetes, edited by WHO, Switzerland, 2008.
2 Ferlay J, Shin HR, Bray F, Forman D, Mathers C, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010, 127, 2893–917. doi: 10.1002/ijc.25516.
3 Torre LA, Bray F, Siegel RL, Ferlay J, Lorete‐Tieulent, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015, 65, 87–108.
4 Ferlay J, Steliarova‐Foucher E, Lortet‐Tieulent J, Rosso S, Coebergh JW, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013, 49, 1374–1403.
5 Bray F, Ren JS, Masuyer E, Ferlay J. Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Intnl J Cancer. 2013, 132, 1133–1145.
![Page 26: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/26.jpg)
![Page 27: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/27.jpg)
13
Anticancer Therapeutics: From Drug Discovery to Clinical Applications, First Edition. Adam Todd, Paul W. Groundwater and Jason H. Gill. © 2018 John Wiley & Sons Ltd. Published 2018 by John Wiley & Sons Ltd.
1.2
There are now believed to be more than 200 different types of cancer, with the potential for the disease to develop in any body organ; this is further complicated by the fact that each organ and tissue is composed of a number of different cell types, each with the potential to develop into a tumour. As you can imagine, the different activities and functions of these ‘normal’ cells directly affects the growth rate, mobility, and lethality of any developing cancer. Consequently, despite the cancer development process being fundamentally similar across different cancer types, vast differences exist in response to treatment, cellular ‘behaviour’ characteristics, and overall disease prognosis.
So, what actually is the difference between a tumour, a cancer, and a malignancy? The answer is contextual, with several of these terms (incorrectly) used interchangeably nowadays. In clinical terms, it is the distinction between benign and malignant which is actually most important, with their use alongside ‘tumour’ to define a particular growth. However, in reality, ‘tumour’ is often used when the term ‘neoplasm’ (which literally means ‘new growth’) would be more appropriate. Presumably for ease more than accu-racy we now often use ‘tumour’ as opposed to ‘neoplasm’. However, whether ‘neoplasm’ or ‘tumour’, they can be either benign or malignant – a difference that is critical and fundamental in interpreting or treating the disease.
1.2.1 Benign Tumour (or neoplasm)
This type of growth is confined to its original location and lacks the ability to invade into surrounding normal tissue, or to dissociate from neighbouring cells and spread to other parts of the body. In general, benign tumours are genetically stable, with very little change in their genotype (genetic composition) over time. Any genetic perturbation within a benign tumour does not provide it with a selective cellular growth advantage over neighbouring cells, with the cells retaining normal growth regulatory mechanisms and defined morphology and functions. As an example, the common skin wart is a benign growth caused by a viral infection, the human papillomavirus (HPV).
The restriction of benign tumours to their site of origin normally means that they can be completely removed via surgery so they are often not life‐threatening. However, excep-tions do exist, wherein the benign tumour is in an inoperable location and its presence disrupts and retards the normal function of its ‘home tissue’, such as some brain tumours.
Cancer Staging and Classification
![Page 28: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/28.jpg)
1 Introduction14
1.2.2 Malignant Tumour (or cancer)
Although in the minority of cases benign tumours can be problematic to a person’s health (and so necessitate curative treatment), this very rarely involves the use of medi-cation (commonly termed cancer chemotherapy). However, ‘cancer’ is the complete opposite and commonly requires chemotherapeutic intervention, as described in detail throughout this book.
We will now focus on what cancer actually is, how it differs to a benign tumour, and why we need to administer therapies systemically, rather than just introduce them exclusively to the site of the cancerous tumour.
There are a number of characteristic distinctions between a benign and a cancerous tumour, including cellular differentiation, growth rate, and genetic stability, and the fact that benign tumours histologically resemble their normal tissue of origin. However, the critical and defining difference between a benign tumour and a cancerous tumour is the capability of the latter to invade adjacent tissues and spread to other tissues and organs, a characteristic termed ‘malignancy’. In this context, malignant tumours (malignant neoplasms) are synonymous with cancer, with their ability to move from their origin into neighbouring tissues, and spread and disseminate throughout the body (a process defined as ‘metastasis’). This invasive and metastatic capability of malignancy is exactly what makes cancer so dangerous and life‐threatening, as once it has spread it can no longer be successfully dealt with by localised treatments and surgery.
In general, benign tumours grow slowly and malignant tumours grow at an accelerated rate, spreading to neighbouring and subsequently distant sites. However, there are several exceptions to this concept, with several benign tumour types growing more rap-idly than some cancers because of their resident environment or the presence of endog-enous growth‐inducing factors etc. Despite these exemptions, it is true to say that most benign tumours develop and expand slowly over the span of months to years.
It is also important to note that not all cancerous tumours are life‐threatening or lethal, and some of the most aggressive cancers are also some of the most curable. Similarly, as mentioned previously, benign tumours, although fairly innocent in nature, can in them-selves cause lethality as a consequence of their location. Therefore, the risk and fate of both benign and malignant tumours is neither clear‐cut nor straightforward.
1.2.3 Tumour Nomenclature and Classification
An important concept when discussing the presence and location of a tumour (and its treatment) is its classification. The descriptive and defining name for a tumour allows us to know where it is, how it associates with the surrounding tissue environment, whether it is predicted to be life‐threatening, its likely prognosis, and when and how we treat it.
From a histological and anatomical standpoint, all benign and malignant tumours are composed of two cellular elements: (1) the tumour mass, composed of the neoplastic cells, and (2) the surrounding and supportive host‐derived, non‐neoplastic cells, comprising stromal support cells, connective tissues, blood vessels, inflammatory cells, and the extracellular protein matrix network. It is now clear that both of these cellular elements are essential for the growth, survival, and support of the tumour, involving a
![Page 29: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/29.jpg)
1.2 Cancer Staging and Classification 15
bi‐directional interaction and communication between the tumour and surrounding cells. This realisation was a turning‐point in the management of malignant tumours, with a new wave of chemotherapies targeted towards the genetically‐stable tumour microenvironment, as opposed to historical chemotherapeutics focused exclusively on the genetically unstable and often drug‐resistant malignant tumour mass. This treat-ment concept is exemplified by several new ‘molecular‐targeted’ chemotherapeutics, as discussed later in the book.
The nomenclature of both benign and malignant tumours involves three components:
i) location (e.g. brain, breast, lung, prostate),ii) type of cell and tissue from which they arose (e.g. epithelial, mesenchymal), and
iii) the growth behaviour of the tumour (e.g. benign or malignant).
The location is easy to define in terms of nomenclature for the majority of tumours (with the exception of metastatic tumours, as described later). Although informative, this alone is insufficient to provide details regarding the type, characteristics, prognosis, and, importantly, the treatment of the particular tumour. These factors rely upon the identification and description of whether the tumour is benign or malignant, the embry-onic origin of the tissue from which the tumour has developed, the functional basis of the originating cell type, the level to which the tumour cells resemble their cellular ori-gin (i.e. their degree of cellular differentiation), their cellular growth pattern, and ulti-mately the microscopic and macroscopic histological features of the tumour. The use of a ‘common language’ when describing and defining tumours is thus essential for com-parison, characterisation and classification, for diagnosis and prognosis, and ultimately in identifying the most appropriate treatment options for the particular case.
The classification of tumours, whether benign or malignant, is initially correlated with the embryonic origin from which the cell type derived. In this context, in the early stages of embryonic development there are three defined cellular layers, termed germ layers: the ectoderm, the mesoderm, and the endoderm. Of these germ layers, the ecto-derm gives rise to the brain, nervous system, and epidermis (outer layer) of the skin, amongst others; the mesoderm produces supporting tissues, including bone, muscle, and blood; and the endoderm develops into internal organs, such as the pancreas, uri-nary bladder and liver, and the epithelial linings of the gastrointestinal tract (except the oral and anal cavities) and respiratory tract. Interestingly, the epithelial linings of the urogenital tracts (i.e. ovaries and kidneys) are derived from the mesodermal rather than the endodermal layers. An important point in the context of development is the defined nature and function of these cells originating from the different germ layers, with some specialising (or differentiating) as pancreatic cells capable of secreting hormones, oth-ers as nerve cells capable of transmitting an electrical impulse, and others differentiat-ing into specialised acid‐secreting cells within the stomach. In all cases, a balance between coordination of cellular division and focused differentiation is essential for these specialisations to be achieved, and the respective organs to develop and function. The importance and relevance of this developmental origin for tumour classification will hopefully become evident in the upcoming parts of this section, and in later chap-ters when discussing tumour development, malignant and metastatic potential, and response to therapy.
Although both benign and malignant tumours can develop from the same cell type (Figures 1.2.1 and 1.2.2), it is vitally important that the classification and name associated
![Page 30: Anticancer Therapeutics - Startseite · culosis, and malaria combined [2]. In 2012, around 14.1 million new cases of cancer were diagnosed (with this figure expected to rise to 19.3](https://reader035.pdfslide.us/reader035/viewer/2022070806/5f04933b7e708231d40ea609/html5/thumbnails/30.jpg)
1 Introduction16
with these distinct tumour types are clearly articulated (Table 1.2.1). In this context, benign tumours are designated by attaching the suffix –oma to the cell type from which the tumour arises. For instance, a benign tumour arising in mesodermal‐derived fibrous connective tissue is termed a fibroma, and a benign tumour of fatty tissue is termed a lipoma (Table 1.2.1). The nomenclature of benign tumours of epithelial origin (endo-dermal and a few mesodermal‐derived tissues) is slightly less straightforward, with clas-sification commonly associated with their histology and constituent epithelial cell characteristics, for example glandular, squamous, or transitional epithelium. For
Figure 1.2.1 Nomenclature of mesenchymal‐derived tumours.
Mesenchymal-derived
Malignant
Fibrous tissue:
Adipose tissue:
Cartilage:
Bone:
Muscle:
Fibrous tissue:
Adipose tissue:
Cartilage:
Bone:
Muscle:
Leiomyoma, Rhabdomyoma
Leiomyosarcoma, Rhabdomyosarcoma
Osteoma
Osteosarcoma, Ewing’s sarcoma
Chondroma
Chondrosarcoma
Lipoma
Liposarcoma
Fibroma
Fibrosarcoma
Benign
Epithelial-derived
Epithelia
Benign Tumour:
Benign Tumour:
Benign Tumour:
Benign Tumour:
carcinoma
Adenocarcinoma
Squamous cell carcinoma
Transitional cell carcinoma
Malignant Tumour:
Malignant Tumour:
Malignant Tumour:
Malignant Tumour:
-oma
Adenoma
Papilloma
Urothelial papilloma
GlandularEpithelia
SquamousEpithelia
TransitionalEpithelia
Figure 1.2.2 Nomenclature of epithelial tumours.