Embed Size (px)
Citation preview
Antibiotics
Slackers Facts by Mike Ori
Disclaimer
The information represents my understanding only so errors and omissions are probably rampant. It has not been vetted or reviewed by faculty. The source is our class notes.
The document can mostly be used forward and backward. I tried to mark questionable stuff with (?).
If you want it to look pretty, steal some crayons and go to town.
Finally…
If you’re a gunner, buck up and do your own work.
What are the types of beta lactam antibiotics
PenicillinsCephalosporinsCarbapenemsMonobactams
Name the classes of penicillins
StandardAntistaphylococcal
AminoAntipseudomonal
What are the anti-staph penicillins and their routes
Nafcillin - IVDicloxacillin - PO
What are the standard penicillins and routes
Penicillin V – POPenicillin G - IV
Which bacteria are exquisitely sensitive to standard penicillins
Group A strep (pyogenes)
Amino penicillins names and routes
Ampicillin – PO,IVAmoxicillin – PO
What is typically coadministered with the aminopenicillins
Beta lactamase inhibitorsAmoxicillin – clavulanate
Ampicillin - sulbactam
What is the CSF action of aminopenicillins
Can reach CSF if the meninges are inflamed
What side effect can happen when giving aminopenicillins to pt with infectious
mononucleosis, chronic lymphocitic leukemia, allopurinol
RashLowest incidence with allopurinol, others are
very high.
Cephalosporins names, generation, routes, and gram positive/negative effectiveness
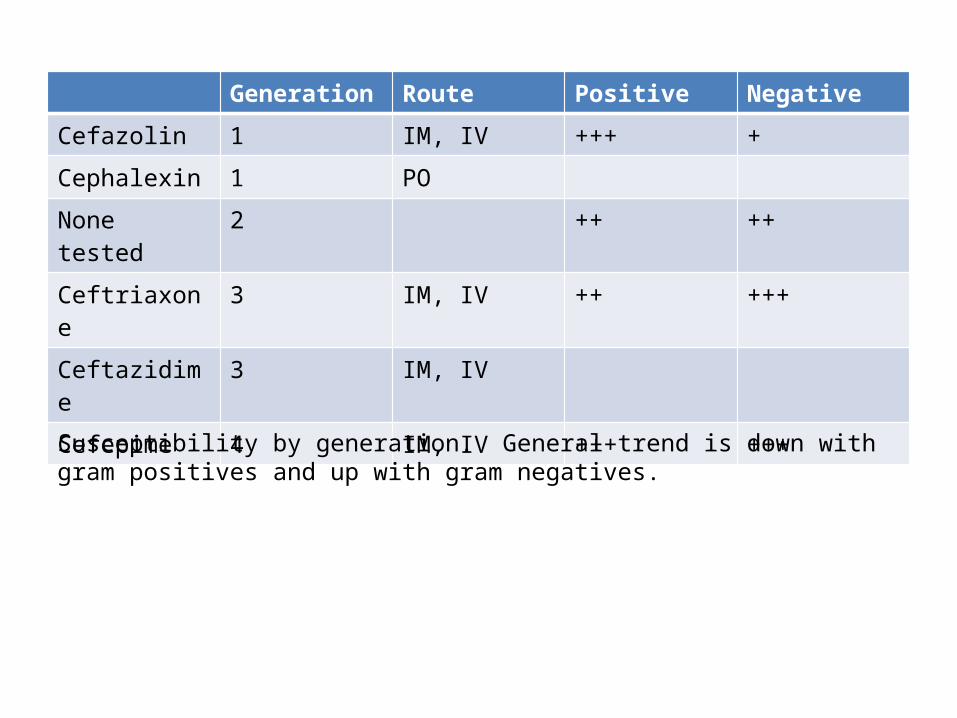
Generation Route Positive Negative
Cefazolin 1 IM, IV +++ +
Cephalexin 1 PO
None tested 2 ++ ++
Ceftriaxone 3 IM, IV ++ +++
Ceftazidime 3 IM, IV
Cefepime 4 IM, IV +++ +++
Susceptibility by generation. General trend is down with gram positives and up with gram negatives.
Which generation reaches effective levels in the CSF
Third gen
Your patient has an allergy to penicillin G can you administer cephalosporins
Maybe. Contraindicated if the pt experienced an IgE mediated rash. Caution with other
penicillin type reaction.
Carbapenems names, routes, and spectrum
Imipenem, IVBroadest range of all available antibiotics.
Excellent penetration through porins into gram negative periplasmic space
What is cilastin
A drug coadministered with imipenem to inhibit kidney ezymes that breakdown imipenem into
nephrotoxic metabolites
Imipenem ADR
Seizures
Monbactam names, routes, spectrum
Aztreonam, IVgram negatives including P aeruginosa.
Ineffective against gram positives or anaerobes
Glycopeptides name, route, spectrum
Vancomycin, IV, Gram positives only
Vanco has poor oral availability so why do the dosing instructions include oral
administration?
Vanco is useful for treatment of gram positive anaerobic infections of the GI tract such as C.
difficile infections.
Describe the ADR from rapid infusion of vancomycin
Rapid infusion results in histamine release that cause flushing of the skin of the neck and
upper trunk that can result in hypotension. AKA red man or red neck syndome
List the protein inhibitory antibiotic classes and their action
Aminoglycosides – 30sMacrolides – 50s
Lincosamides – 50sTetracyclines – 30s
Chloramphenicol – 50sStreptogramins – 50s
Oxazolidinones – ribosome assembly
Aminoglycoside names, routes, spectrum
Gentamicin, IVTobramycin, IV
Both are effective against aerobic gram negative and mycobacterium
Aminoglycoside toxicity characteristics
Nephrotoxic and ototoxic above an patient variable threshold in time dependent manner
Aminoglycoside dosing characteristics
Concentration dependent killing with significant post antibiotic effect allows for once daily
dosing.
Note: This contrasts to most others that are both time and concentration dependent.
Why are aminoglycosides ineffective against anaerobic bacteria?
Entry into the cell is mediated by oxygen dependent transport.
Aminoglycoside resistance basis
Transferase enzymes inactive them. Unlike penicillins, there are variations in the
resistance enzymes.
Aminoglycoside toxic trough threshold
Trough concentrations above 2 mcg/mL are predictive of toxicity
Macrolide names, route
Azithromycin, PO (Z pack), IV
Azithromycin indications
Treatment of out of hospital community acquired respiratory infection and in hospital
pneumonia in combination.STD’s
Macrolide CSF penetration characteristics
Poor
Azithromycin volume of distribution
Extremely high volume of distribution with tissue concentration 10-100x plasma.
Azithromycin half life
2-4 days
Primary azithromycin caution
Caution in PT with prolonged QT interval due to risk of torsades des pointes
Lincosamides name, route, spectrum
Clindamycin, PO,IV, strep, staph, anaerobes
Clindamycin indications
Anaerobes above the diaphragm
Clindamycin associated disease
C-diff enteritis
Tetracycline name, route, spectrum
Doxycycline, PO, IV, Chlamydia, mycoplasma, spirochetes
Tetracyclines contraindication
Children and pregnant or breastfeeding women due to staining of developing teeth
Tetracycline food cautions
Do not take with meals, supplements, or vitamins due to cation chelation
Your PT is a lifeguard with chlamydia, should you prescribe doxycycline?
No, photosensitivity is a common side effect.
Chloramphenicol indication and route
Given IV as second line therapy for CSF infections
What is the basis of chloramphenicol’s black box warning
Causes dose dependent myelosuppression that can lead to aplastic anemia.
Fluroquniolones names, route, spectrum
CiprofloxacinLevofloxacinMoxifloxacin
Excellent oral availability. IV forms exist.Active against gram negative bacilli
Fluroquniolones CSF therapeutic role
Unknown. Not recommended for meningitis.
What are common ADR to fluoroquinolones
CNS: hallucinations, delerium, seizuresBone: Cartilage damage, tendonitis
Pregnancy class C
Ok Smarty, what is pregnancy class C
C = don’t give it to them cause it jacks up animal fetuses and the IRB won’t give you the go
ahead to test it on humans.
What are the respiratory fluoroquinolones?
LevifloxacinMoxifloxacin
Fluoroquniolones food cautions
Do not take with meals, supplements, vitamins as chelation occurs.
Metronidazole route and spectrum
Obligate anaerobes, PO and IV
Metronidazole function
Creates reactive intermediates and free radicals that damage cellular components.
Your patient has an anaerobic bacterial infection. He has a small firm micronodular
liver. What are the issues for metronidazole?
Hepatic metabolism with renal excretion. Disulfiram like effects with alcohol use.
Rifmycin antibiotic mechanism
Inhibits RNA polymerase
Rifampin metabolism
Hepatic. Induces microsomal system which increases metabolism of other drugs.
Sulfonamide action
Inhibits PABA conversion to dihydrofolate by dihydropteroate synthetase
Trimethoprim action
Inhibits DHF conversion to THF by DHR reductase
What is TMP-SMX and why is it given?
TMP = trimethoprimSMX = sulfamethoxazole (a sulfonamide)
Given in combination to increase their effectiveness by 20-100 times over SMX alone.
TMP-SMX indication
UTI and pneumocystis jiroveci pneumonia
Your patient complains of a rash after starting UTI treatment. What did you prescribe. Are
you worried about the rash?
You prescribed TMP-SMX. You would be very worried about this rash and would advise your
PT to stop taking the drug immediately.
Your patient does not stop taking the drug even though you called back later and re-iterated
the importance. A few days later you receive a courtesy call from an ER doc advising you that they are admitting your pt. What is a
potential admitting diagnosis?
Stevens-Johnson syndrome or toxic epidermal necrolysis.
Which of the drugs (TMP/SMX) most likely caused the reaction and what is its general
class.
Sulfamethoxazole. It is a sulfa drug.












![[Salesforce] Perforce - Enablers of Rampant Growth](https://img.pdfslide.us/doc/110x75/546d6a48b4af9f8e2c8b54d7/salesforce-perforce-enablers-of-rampant-growth.jpg)