Embed Size (px)
Citation preview

Antibiotics- A Quick Overview
Ged Hawthorn Jan 2014

Ben P
en
Flu
clo
x
Am
p/ a
mox
Am
ox-C
lav
Tic
-Cla
v
Pip
- Taz
Cephazolin
Cefa
clo
r/
cefu
roxim
e
Ceftria
xone
Cefta
zid
ime
Gram Positive Strep A,B,C,G
Strep Pneumonia
MSSA
MRSA
CA-MRSA
enterrococcus faecalis
s
Listeria monocytogenes
Gram Negative
H. Influenzae
E. Coli
Klebsiella
Kleb/ Ecoli ESBL
Pseudomonas
legionella
ESCAPPM
MISC
m. Pneumoniae
Anaerobes
Baceroides Fragilis
C. Diff
usually effective or >60% susceptible
S synergy
trials lacking or 30-60% susceptible
Sensitive but resistance develops rapidly

Ben P
en
Flu
clo
x
Am
p/ a
mox
Am
ox-C
lav
Tic
-Cla
v
Pip
- Taz
Cephazolin
Cefa
clo
r/
cefu
roxim
e
Ceftria
xone
Cefta
zid
ime
Gram Positive Strep A,B,C,G
Strep Pneumonia
MSSA
MRSA
CA-MRSA
enterrococcus faecalis
s
Listeria monocytogenes
Gram Negative
H. Influenzae
E. Coli
Klebsiella
Kleb/ Ecoli ESBL
Pseudomonas
legionella
ESCAPPM
MISC
m. Pneumoniae
Anaerobes
Baceroides Fragilis
C. Diff
usually effective or >60% susceptible
S synergy
trials lacking or 30-60% susceptible
Sensitive but resistance develops rapidly

Genta
mic
in
Azith
rom
ycin
Doxycyclin
e
Metro
nid
azole
Clin
dam
ycin
Vancom
ycin
Cip
roflo
acin
Moxiflo
xacin
Mero
penem
Lin
ezolid
Gram Positive Strep A,B,C,G
Strep Pneumonia
MSSA
MRSA
CA-MRSA
enterrococcus faecalis s
Listeria monocytogenes s
Gram Negative
H. Influenzae
E. Coli
Klebsiella
Kleb/ Ecoli ESBL
Pseudomonas
Legionella
ESCAPPM
MISC
m. Pneumoniae
Anaerobes
Baceroides Fragilis
C. Diff
orally
usually effective or >60% susceptible
trials lacking or 30-60% susceptible
s used synergistically

Genta
mic
in
Azith
rom
ycin
Doxycyclin
e
Metro
nid
azole
Clin
dam
ycin
Vancom
ycin
Cip
roflo
acin
Moxiflo
xacin
Mero
penem
Lin
ezolid
Gram Positive Strep A,B,C,G
Strep Pneumonia
MSSA
MRSA
CA-MRSA
enterrococcus faecalis s
Listeria monocytogenes s
Gram Negative
H. Influenzae
E. Coli
Klebsiella
Kleb/ Ecoli ESBL
Pseudomonas
Legionella
ESCAPPM
MISC
m. Pneumoniae
Anaerobes
Baceroides Fragilis
C. Diff
orally
usually effective or >60% susceptible
trials lacking or 30-60% susceptible
s used synergistically

Pharmacodynamics of
Antibacterials BACTERIAL KILLING/PERSISTENT
EFFECT
DRUGS THERAPY GOAL-
PK/PD Parameter
Concentration-dependent/Prolonged
persistent effect
Aminoglycosides; daptomycin;;
quinolones; metronidazole
High peak serum concentration
Peak/MIC
Time-dependent/No persistent effect Penicillins; cephalosporins;
carbapenems; monobactams
Long duration of exposure
Time above MIC
Time-dependent/Moderate to long
persistent effect
Clindamycin; erythro/azithro/clarithro;
linezolid; tetracyclines; vancomycin
Enhanced amount of drug
24-hr AUC1/MIC

Initial serum
peak level Died Survived
< 5mcg/ml 21% 79%
>= 5mcg/ml 2% 98%
Aminoglycoside response rate
Beta Lactam Pharmacodynamics
24h-AUC/MIC ratio Satisfactory Unsatisfactory
< 125 4 (50%) 4
> 125 71 (97%) 2
Vancomycin Outcome vs 24h-AUC/MIC ratio
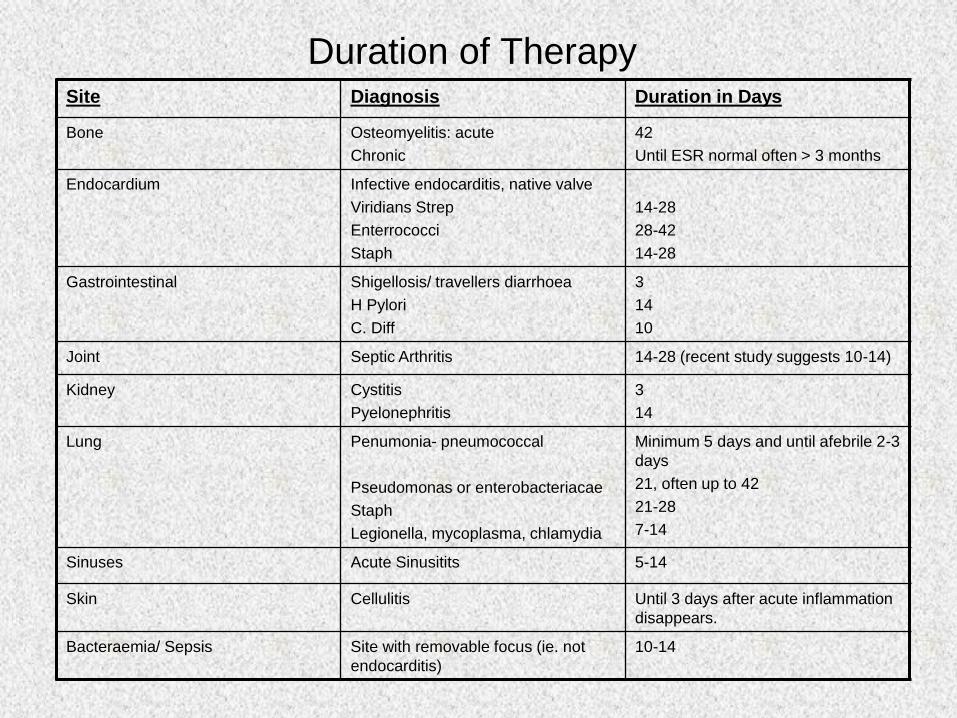
Duration of Therapy Site Diagnosis Duration in Days
Bone Osteomyelitis: acute
Chronic
42
Until ESR normal often > 3 months
Endocardium Infective endocarditis, native valve
Viridians Strep
Enterrococci
Staph
14-28
28-42
14-28
Gastrointestinal Shigellosis/ travellers diarrhoea
H Pylori
C. Diff
3
14
10
Joint Septic Arthritis 14-28 (recent study suggests 10-14)
Kidney Cystitis
Pyelonephritis
3
14
Lung Penumonia- pneumococcal
Pseudomonas or enterobacteriacae
Staph
Legionella, mycoplasma, chlamydia
Minimum 5 days and until afebrile 2-3
days
21, often up to 42
21-28
7-14
Sinuses Acute Sinusitits 5-14
Skin Cellulitis Until 3 days after acute inflammation
disappears.
Bacteraemia/ Sepsis Site with removable focus (ie. not
endocarditis)
10-14
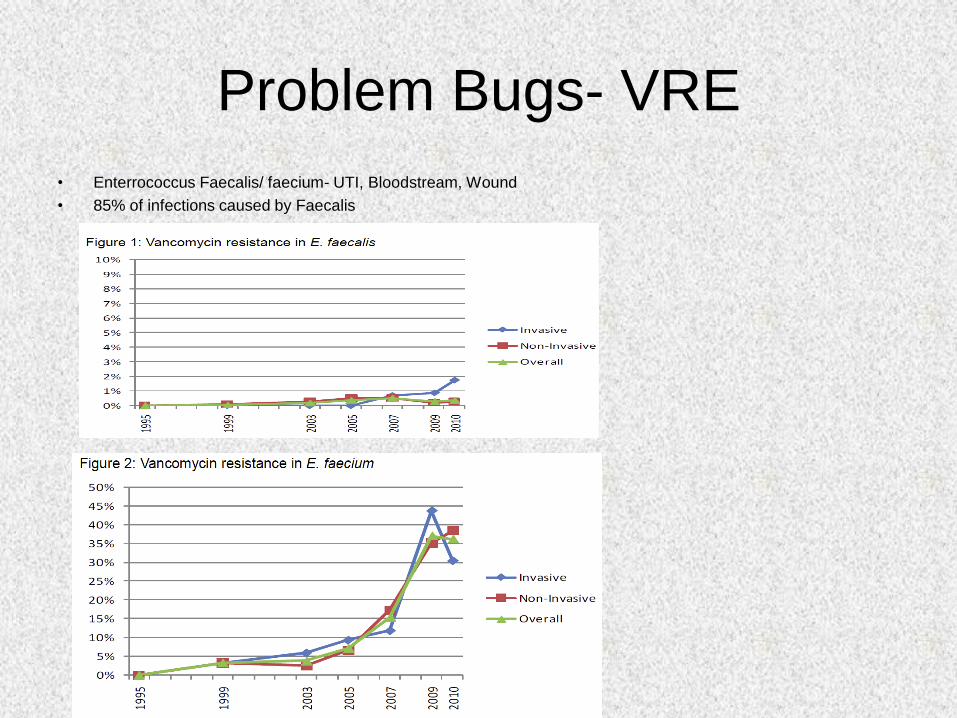
Problem Bugs- VRE
• Enterrococcus Faecalis/ faecium- UTI, Bloodstream, Wound
• 85% of infections caused by Faecalis

MRSA by Region
Coombs et al., Australian Group for Antimicrobial Resistance (AGAR), Staphylococcus aureus Program 2008 (SAP 2008)
Community Survey MRSA Epidemiology and Typing Report, 2009

ESBL
Gram Negative Survey 2011 Antimicrobial Susceptibility Report: Report from the Australian Group on Antimicrobial Resistance
•E.Coli, Klebsiella spp, other Enterobacteracaie
•E coli ESBL 5-10% in Aus
•Klebsiella ESBL 10-15% in Aus
•Much higher overseas
•Associated with use of 3rd gen cephalosporin
•In vitro appear to be sensitive to cephalosporins, but have resistance in vivo
•Plasmid mediated resistance to penicillins and cephalosporins and…
Species Category Ciprofloxacin Gentamicin Trimethoprim
E Coli %I 1.7% 0.9% -
%R 51.1% 42.6% 55.1%
Klebsiella %I 27.1% 0% -
%R 29.2% 66.7% 79.2%
Co-resistance Percentages in Strains With Confirmed ESBLs

Antibiotic E Coli Aus 2011
Cat
%
Ampicillin %I 0.9
%R 50.5
Amox-clav %I 16.1
%R 7.7
Tic- Clav %R 8
Cephazolin %R 22.3
Ceftriaxone %NS 9.6
Ceftazidime %NS 5.8
Cefepime %NS 1.8
Meropenem %NS 0.1
Ciprofloxacin %NS 10.6
Gentamicin %R 8.2
Trimethoprim %R 23.4
Source AGAR 2012
2006 2006
Antibiotic Kleb spp Aus 2011
Cat
%
Ampicillin %R Intrinsic
Amox-clav %I 7.6
%R 7.1
Tic-Clav %R 9.7
Cephazolin %R 31.1
Ceftriaxone %NS 11.4
Ceftazidime %NS 8.2
Cefepime %NS 1.7
Meropenem %NS 0.4
Ciprofloxacin %NS 6.1
Gentamicin %R 8.4
Trimethoprim %R 14.9
Source AGAR 2012

Pan Resistant Bugs
• Klebsiella Pneumonia Carbapenemase (KPC).
• KPC-producing bacteria are often misidentified by routine microbiological
susceptibility testing and incorrectly reported as sensitive to carbapenems
• Organisms with detected KPC enzyme- Citrobacter,Pseudomonas, Escherichia coli,
Enterobacter, aerogenes, Acinetobacter spp Klebsiella pneumoniae, Klebsiella
oxytoca, Proteus mirabilis, Salmonella, Serratia marcescens
• Treatment- Colistin and Tigecycline
• New Delhi metallo-Clactamase 1 (NDM-1)
• An enzyme that produces resistance to a broad-range of beta-lactam antibiotics
• Produces a carbapenease
• Bacteria involved: E. coli, Klebsiella pneumoniae, Acinetobacter baumanni
• Can spread to other bacteria through horizontal gene transfer (via plasmids)
• Treatment: tigecycline and colistin
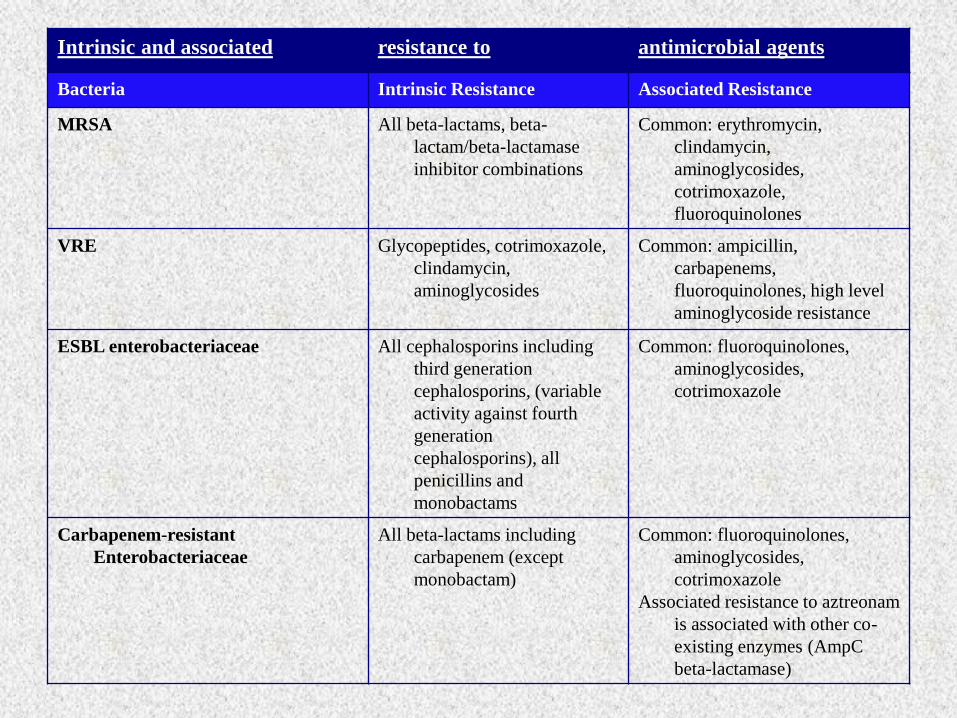
Intrinsic and associated resistance to antimicrobial agents
Bacteria Intrinsic Resistance Associated Resistance
MRSA All beta-lactams, beta-
lactam/beta-lactamase
inhibitor combinations
Common: erythromycin,
clindamycin,
aminoglycosides,
cotrimoxazole,
fluoroquinolones
VRE Glycopeptides, cotrimoxazole,
clindamycin,
aminoglycosides
Common: ampicillin,
carbapenems,
fluoroquinolones, high level
aminoglycoside resistance
ESBL enterobacteriaceae
All cephalosporins including
third generation
cephalosporins, (variable
activity against fourth
generation
cephalosporins), all
penicillins and
monobactams
Common: fluoroquinolones,
aminoglycosides,
cotrimoxazole
Carbapenem-resistant
Enterobacteriaceae
All beta-lactams including
carbapenem (except
monobactam)
Common: fluoroquinolones,
aminoglycosides,
cotrimoxazole
Associated resistance to aztreonam
is associated with other co-
existing enzymes (AmpC
beta-lactamase)

Strep Pneumoniae
• 2005 AGAR data
• 28.0% penicillin resistant
• 22.7% erythromycin resistant
• 15.6% clindamycin resistant
• 18.4% tetracycline resistant
• 31.0% trimethoprim-sulphamethoxazole resistant
• Seventeen point three per cent of isolates were multi-resistant (acquired resistance to more than 2 drug classes).
• North American data: may be between 40-80% penicillin resistant
• normal resistance: penicillin MIC < 0.1microgram/mL
• intermediate resistance: MIC 0.1-1microgram/mL (treat with high dose penicillin)
• high resistance: MIC > 2.0micrograms/mL

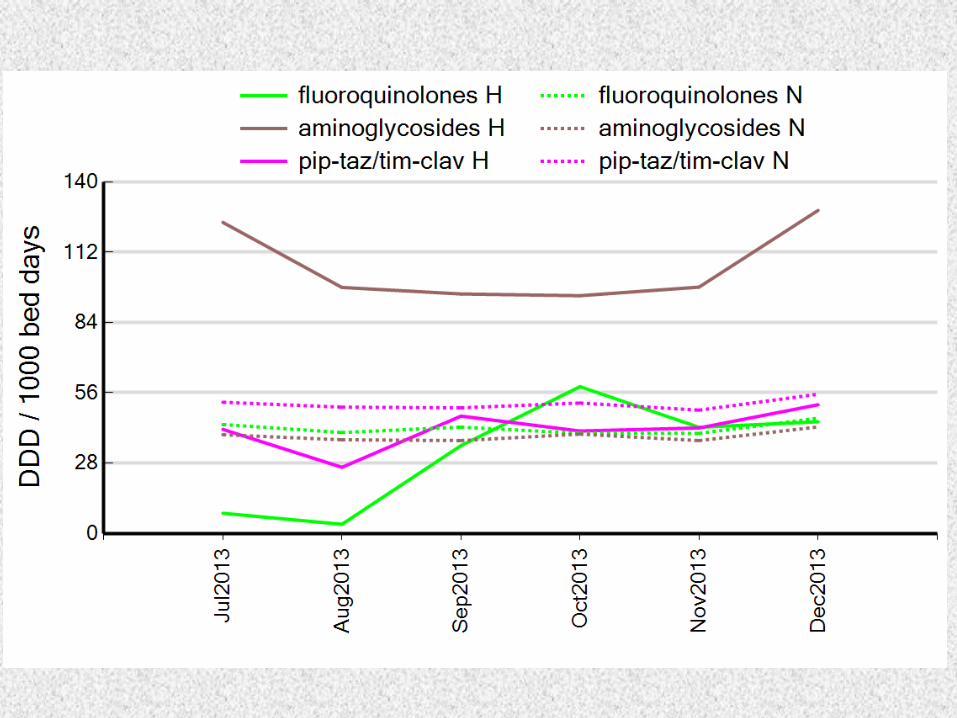
How do we compare?

Vancomycin Dosing and Monitoring
Loading dose and subsequent doses •Maximum infusion rate is 10 mg/minute to avoid Red Man syndrome (e.g., for 1.5 g, at least 2.5 hrs)
•Initial dose is a loading dose of 25 mg/kg of actual body weight
•Subsequent dosing and monitoring is based on the GFR calculated by the Cockroft Gault equation
Following the loading dose of 25 mg/kg (all patients):
Monitoring of target levels:
Timing of first level is per the table above
Target trough level is 15-20 mg/L
Only measure trough levels; peak levels aren’t measured
Do not delay regular dosing while waiting for a level
If levels are therapeutic and renal function stable, then repeat ~ weekly
Repeat more frequently with changing renal function, hemodynamic instability or concurrent nephrotoxins
Adjusting dosing and repeating levels:
Ensure that the trough level taken was a “true trough” taken pre-dose
Adjustment of vancomycin dosing is directly linear
e.g., for a trough of 12 and an existing dose of 1 g: 18/12 x 1 = 1.5 g
Re-check at same intervals as per table above if an adjustment is made

Indications
Empiric o <48 hours with investigations
pending, there is no need for levels
if use is less than 48 hrs o Gram negative pathogens
Directed o Infections when resistance to other
microbials shown o Combo therapy for Pseudomonas
aeruginosa and brucellois o Low doses as synergistic treatment
for streptococcal and enterococcal
endocarditis
Contraindications
Previous vestibular or auditory toxicity
due to an aminoglycoside
Hypersensitivity reaction to an
aminoglycoside
Precautions
Hearing problems
Vestibular problems
Neuromuscular disorders
Chronic liver disease, severe cholestasis
(serum bili >90)
Chronic renal failure or deteriorating
renal function
10-29 years 30-60 years >60 years
6mg/kg STAT
(up to 560mg)
5mg/kg STAT
(up to 480mg)
4mg/kg STAT
(up to 400mg)
Creatinine
Clearance
<30mL/min 30-40mL/min 40-60mL/min >60mL/min
Approach Seek expert
advice –
contact
Infectious
Diseases
Repeat same
dose in 48
hours
Repeat same
dose in 36
hours
Repeat same
dose in 24 hours
(can have a total
of 3 doses at
0,24 & 48 hrs)
Empirical or
Directed Therapy
Severe Sepsis Intermittent Dosing (only
when used synergistically)
7mg/kg STAT
(up to 640mg)
1mg/kg every 8 hours
(monitor trough levels
and UEC daily)
Single/Initial
Dose
Continued dosing for 48 hours without
need for drug monitoring (if indicated)
Gentamicin Dosing and Monitoring

IV to Oral Antibiotic Step Down
Inclusion Criteria:
Tolerating oral medications
Has received 2 days of IV therapy
Temperature <38 C over 24 hours
Respiratory Rate <20 or at baseline
Mental Status at baseline
Decreased WBC Count
Oxygenation >90% at room air or at
baseline
Exclusion Criteria:
In critical care area
Bone and joint infections
Endocarditis
Meningitis or other CNS infections
Bacteremia
Neutropenia
Legionella pneumonia
Malabsorption/Short Bowel syndrome
Severe diarrhoea
Uncontrolled nausea and vomiting
Patient on Total Parenteral Nutrition
When and when not to switch from IV to PO
antibiotics

IV ORAL
Antimicrobial Standard Dose* Antimicrobial Standard Dose*
Ampicillin 1-2g q6h Amoxycillin 500mg-1g TDS
Azithromycin 500mg daily Roxithromycin 300mg daily
Benzylpenicillin 1.2g q4-6h Amoxycillin 500mg-1g TDS
Ceftriaxone 1g daily
Cephazolin 1g q8h Cephalexin 500mg QID
Ciprofloxacin 200-400mg q12h Ciprofloxacin 250-500mg BD
Flucloxacillin 1g q6h Flucloxacillin 500mg QID
Lincomycin 600mg q8h Clindamycin 450mg TDS
Fluconazole 200-400mg daily Fluconazole 200-400mg daily
Metronidazole 500mg q12h Metronidazole 400mg TDS
Moxifloxacin 400mg daily Moxifloxacin 400mg daily
Piperacillin + Tazobactam^ 4.5g q8h Amoxycillin + Clavulanate 875/125mg BD
Ticarcillin + Clavulanate^ 3.1g q6h Amoxycillin + Clavulanate 875/125mg BD
Antimicrobial Oral Bioavailability
Ciprofloxacin 70-90%
Clindamycin 90%
Fluconazole >90%
Metronidazole 80%
Moxifloxacin 90%
Trimethoprim +
Sulfamethoxazole 98%
IV TO ORAL SWITCH Suggested Conversion Regimens *Dose adjustments may be required in renal impairment
^Consult ID Physician if pseudomonas or resistant negative Gram bacteria

Surgical Prophylaxis

Common Ups
• Timentin and Tazocin are penicillin based antibiotics- check allergies
• Give decent doses of gentamicin 4-7mg/kg
• Can give 48 hrs of gentamicin without needing to take a level (ie. 3 doses in normal renal function).
• Don’t use ceftriaxone 1st line for everything, has no enterrococcus or pseudo cover for UTI.
• Rate pneumonia severity using SMART COP or CORB and dose according to therapeutic guidelines (consider benzylpenicillin + doxycycline/ roxithromycin)

Common Ups
• Check sensitivites and choose a narrower spectrum antibiotic once known.
• Don’t give gentamicin/ other antibiotics for catheter changes.
• There is no evidence for using benpen plus fluclox to treat cellulitis.
• Bilateral cellulitits rarely exists.
• Don’t forget to dose adjust renally excreted drugs (check eTG)

Common Ups
• Investigate penicillin allergies before jumping to using moxifloxacin, vanc etc, around 10% of reported penicillin allergies are true.
• As a general rule remember to convert to oral therapy once afebrile for 48 hrs.
• For most surgical procedures a stat dose at time of induction is all the prophylaxis that is needed. Guidelines do not list any need for gentamicin prophylaxis in orthopaedic surgery.

An estimated 70 percent of all U.S. antibiotics are used nontherapeutically
in animal agriculture. (Image credit: Keep Antibiotics Working Coalition)

Remember M icrobiology guides therapy wherever possible
I ndications should be evidence based
N arrowest spectrum required
D osage appropriate to the site and type of infection
M inimise duration of therapy
E nsure monotherapy in most cases





























