Embed Size (px)
Citation preview

Surgical OverviewSURGICAL TECHNOLOGY INTERNATIONAL III
Antibiotic Update for theSurgeonROBERT S. BENNION, M.D.
ASSOCIATE PROFESSOR OF SURGERY,
UCLA SCHOOL OF MEDICINE
Los ANGELES, CA
All too often, it seems that the utilization of antibiotics by surgeons
for either prophylaxis or the treatment of established infections is
shrouded in a combination of mysticism and marketing. What
should be straight forward, frequently becomes confused by factors
such as superstition, habit, recent interaction with an industry repre-
sentative, and faulty information. The rational use of antibiotics is sur-
prising simply, and is based on the fact that these agents are, quite
simply, systemic chemotherapy against bacteria.' Once delivered to the
patient these agents act not only locally, but, more importantly, sistem-
ically against susceptible microorganisms. This demands that the prac-
titioner make an educated guess as to which bacteria are likely to be
present, as well as use an agent that both safe and effective in that spe-
cific patient. The types and variety of bacteria present in a surgical
infection, or likely to be present, can usually be deduced by the loca-
tion and/ or organ system involved. The safest and most effective agent
to be used against those organisms is primarily a function of the specif-
ic hospital that the patient in, and whether the infection is hospital-
acquired (nosocomial) or community-acquired. The susceptibility
patterns for bacteria vary from community to community (as noted by
local hospitals), as well as from hospital to hospital dependent on
whether it is a community hospital or a tertiary referral center. It is
illogical to assume that the same drug or drugs will be just as effective
in one setting as in another, regardless of whether they are used for
prophylaxis or an established infection.
69

Antibiotic Update for the SurpeonBENNION
In this chapter, we will explore therationale for the use of antibiotics inboth surgical prophylaxis and estab-lished infections, as well as discuss newdevelopments in antimicrobial therapysuch as the mechanisms of resistanceto ~-lactam antibiotics and the ratio-nale for ~-lactmase inhibitor combina-tions, changes in dosing regimens foraminoglycosides that may increaseboth efficacy and safety, new uses ofquinolone antibiotics for severe infec-tions, and use of vancomycin in theface of increasing resistance from ente-rococci.
SURGICAL ANTIBIOTIC PROPHYLAXIS
Although the scientific basis for theuse of prophylactic antibiotics insurgery was elucidated over thirty years
ago,2,3 it wasn't until the mid-seventiesthat good clinical trials began to provethe benefit of these agents as prophylax-is in surgical procedures.t' The objec-tive of antibiotic prophylaxis is simplyto prevent the establishment andgrowth of a microbial inoculum in asurgical site, and thus prevent postoper-ative infectious complications. Thereare, however, certain basic rules andprinciples which must be followedwhen administering prophylactic antibi-otics for a surgical procedure both tomaximize the efficiency of the agentsand minimize any possible problems.First, is the recognition that all theantibiotics in the world are not going tomake up for poor surgical judgment andtechnique. Second, the antibiotic cho-sen must be administered prior to thebacteriologic inoculation. As recently
EXPECTED POST-OPERATIVE WOUND INFECTION RATES BASED ON 1964 SURVEY
TYPE OF OPERATION
CLEAN
CLEAN-CONTAMINATED
CONTAMINATED
DIRTY / INFECTED
EXPECTED WOUND INFECTION RATE (%)
2-5
8-10
15 - 20
30 - 45
Table 1. (Adapted from Academy of Sciences National Research Councii"}
PERCENTAGE RISK OF WOUND INFECTION FOR SOME COMMON OPERATIONS BASED UPON RISK INDEX
TIME "X" RISK FACTORS PRESENTOPERATION (HOURS) 0 1 2 3
ABD.HYSTERECTOMY 2 1.4% 4.1% 5.1% *
AMPUTATION, MAJOR 1 3.9% 4.6% 5.5% 7%APPENDECTOMY 1 2.4% 2.3% 9.4% 9.7%CABG 5 1.1% 3.5% 6.7% 33.3%CHOLECYSTECTOMY 2 1.4% 2% 7.1% 11.5%COLONIC 3 3.2% 8.5% 16.1% 22.2%C-SECTION 1 4.2% 5.9% 11.4% *CRANIOTOMY 4 0.6% 2.5% 2.6% *
EXP. LAPAROTOMY 2 1.5% 4.1% 14% 14%GASTRIC 3 4.9% 6.9% 15% *
HERNIORRAPHY 2 1% 1.9% 5.2% *
HEAD AND HECK 4 1.3% 3.5% 9% *
JOINT PROSTHESIS 3 1.2% 2.6% 4.8% *
MASTECTOMY 2 0.8% 2.4% 5.2% *
ORIF 2 1% 1.8% 3.5% 3.7%SKIN 2 1 .3% 1 .8% 6.1% 1 1.1%SPINAL 3 0.7% 1.9% 4% *
VASCULAR 3 1.6% 2.1% 6.1% 14.8%* Numbers too small to analyze
Table 2. (Adapted and modified from Culver et sl "}
70
demonstrated by Classen and his co-workers, administration of an antibioticeither more than two hours before thesurgery or any time after the surgerybegins results in Significantly higherwound infection rates." In fact, adminis-tration of the antibiotic post-operativelyresulted in infection rates not dissimilarfrom administration of no antibiotic atall. The best time for administration ofthe agent is probably within an hourprior to the actual incision of the skin.
Another principle of antibiotic pro-phylaxis in surgery is that there must bemaintenance of adequate tissue levels ofthe antibiotic throughout the period ofcontamination risk. This means that ifthe antibiotic has a short half-life or ifthe surgery is especially prolonged,redo sing of the agent will be necessary.This redosing can be eliminated byusing an agent with a prolonged half-life(dosing interval of every eight or twelvehours). Also, it is important that theprophylactic therapy be of brief dura-tion. It has never been shown that a sin-gle dose of a single long-actingantibiotic is any less effective thaneither the use of multiple agents forprophylaxis or multiple postoperativedoses for prophvlaxis.j Finally, if anestablished infection is encountered,then it is no longer a prophylactic situa-tion but rather a therapeutic one. Inthat case, the agent which was chosenfor prophylaxis should simply be con-tinued post-operatively in a therapeuticfashion. One should always employ fulltherapeutic dosing of an antibioticappropriate to the type of bacteriaanticipated when choosing a prophylac-tic antibiotic. This facilitates transitionfrom a prophylactic to a therapeutic sit-uation if the need arises.
All surgeons are familiar with the tradi-tional wound classification system whichwas developed in 1964 by the Academy ofSciences National Research Council." Bythis classification, surgical procedures aredivided into clean, clean contaminated,contaminated, dirty/infected based onlyon the type of procedure and organ sys-tem involved. The expected woundinfection rates derived from this classifi-cation is noted in Table 1. Using this data,specific antibiotic prophylaxis was rec-ommended only for clean-contaminatedoperations, because the available datafrom the late sixties and early seventiessuggested that antibiotics reduced thewound infection rates of these operationsdown to that of a clean operation whichwas the desired goal and endpoint.

However, about 15 years ago reportsbegan to emerge suggesting that theseaccepted wound infection rates wereprobably too high. A report on woundsurveillance in a single institution for theyears 1977 and 1981 demonstrated thatthe post-operative wound infection ratesfor clean-contaminated cases were con-sistently less that five percent (and there-fore not significantly different from theclean wound rate), and that the infectionrates for contaminated wounds were onlyten percent." Findings such as thes~resulted in investigators looking at factorsother than just the type of 'operation per-formed as being important determinantsof post-operative infection rates.
Haley, in 1985, reported that morepatient specific factors such as abdominaloperation, an operation lasting greaterthan two hours, the patient having threeor more diagnoses on the discharge sum-mary, or a contaminated/ dirty opera-tion, were significant determinants ofpost-operative wound infection rate, 10
and were probably more realistic indica-tors of actual risk. Based upon the pres-ence or absence of these four factors, heproposed a simple wound infection riskindex. This showed wound infectionrates of 1. 0% if none of the factorsoccurred, 3.6% if one factor was pre-sent, 8.9% if two factors were present,17.2% if three factors were present, and27% if all four factors were present. Itwas suggested that antibiotic prophylaxisonly be used in those cases with two ormore risk factors present.
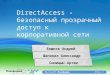
More recently, this same group hasmodified this post-operative woundinfection risk index. 11 With informationon nearly 85,000 operations, theyaltered the risk factors to be: 1) apatient having an American Society ofAnesthesiologist (ASA) pre-operativeassessment score of three, four, or five;2) an operation classified as either cont-aminated or dirty/infected; and 3) anoperation where the duration on thesurgery exceeds X hours (where X isdependent upon the operative proce-dure being performed). For all opera-tions, this index reveals that if no riskfactors were present, the infection ratewas 1.5%, for one risk factor present2.9%, for two risk factors present6.8%, and if all three risk factors pre-sent, the infection rate was 13%. Table2 shows the infection risk for somecommon operations, based upon thissystem, and Table 3 gives some specificantibiotic recommendations for surgicalprophylaxis based upon type of opera-
Surqical OverviewSURGICAL TECHNOLOGY INTERNATIONAL III
aspect of the global care of the patient'sdisease process. As with the use ofantibiotics in surgical prophylaxis, theusage of antibiotics in the treatment ofestablished infections is also governed bycertain principles. As with prophylaxis,the first principle that must thoroughlyunderstood is that antibiotics by them-selves will not substitute for adherence
tion performed or area being operatedupon.
ANTIBIOTIC USAGE IN ESTABLISHEDINFECTIONS
The use of antibiotics as adjunctivetherapy for the established infectionsencountered by surgeons is an important
ANTIBIOTIC1st generation cephalosporin
orvancomycin*
SUGGESTED AGENTS FOR SURGICAL PROPHYLAXIS FOR ELECTIVE OPERATIONS
Table 3.
71
1st generation cephalosporinor
vancomycin*
vancomycin
1st generation cephalosporinor
vancomycin*
1st generation cephalosporinor
~-Iactamase inhibitor comb.
1st generation cephalosporinor vancomycin*
1st generation cephalosporinor vancomycin*
Topical aminoglycosideor
Topical triple antibiotics
2nd generation cephalosporinor
~-Iactamase inhibitor comb.
2nd generation cephalosporinor ~-Iactamase inhibitor comb.
Oral:neomycin + erythromycinplus
IV: 3rd generationcephalosporin or
~-Iactamase inhibitor comb.
1st generation cephalosporinor
~-Iactamase inhibitor comb.
OPERATION PATHOGEN(S)SKIN Staph.epi., Staph. aureusLong operation (>2 hrs),use of prosthetic material
VASCULAR Staph. epi., Staph. aureus,Abd. aorta, prosthesis,groin incision enteric gram - bacilli
VASCULAR ACCESS FOR Staph. epi., Staph. aureusHEMODIALYSIS
CARDIAC Staph. epi., Staph, aureus,Corynbacterium,enterie gram-bacilli
HEAD AND NECK Staph. aureus, streptococci,Enter oral eavity orpharynx,ORIF oral anaerobes
NEUROSURGERY Staph. epi., Staph. aureus
ORTHOPEDICS Staph. epi., Staph. aureusTotal oint ORIF
OPHTHALMOLOGIC Staph. epi., Staph. aureus,streptococci,
enteric gram-bacilli
GASTRODUODENAL Enteric gram - bacilli,gram + coeci
BILIARY TRACT Enteric gram - bacilli,enterococci, anaerobes
COLORECTAL Enteric gram- bacilli,anaerobes
GYNECOLOGIC Enteric gram - bacilli,anaerobes, streptococci,
enterococci
*where MRSA or MRSE is a problem.

Antibiotic Update for the SurqeonBENNION
to good surgical technique and judg-ment. Second, one should match theantibiotic used to the type of bacteriafound either on a previous culture speci-men or on the flora which might beexpected to be present. Also, the use ofa single antibiotic agent for all infectionsin all locations and circumstances is bothdangerous and foolish. Since each antibi-otic has more or less a specific anti-microbial spectrum of action, it isillogical to assume that one specific agentcan be effective in every infection a sur-geon might encounter. Such inappropri-ate use of antibiotics is one of the leadingcauses of the emergent of resistantorganisms. As a corollary, the choice ofthe drug should be made based uponknown bacterial sensitivity data. If possi-ble, this data should be institutionallyspecific. Each hospital should publish atleast quarterly an antibiogram listing thespecific antibiotic susceptibilities basedupon the bacteria seen in that institution.This is probably the best guide to boththe pool of community microflora andthe expected nosocomial pathogens inthat institution.
Another principle of antibiotic usagein established infection, is that wherepossible a single agent should beemployed. Although the treatment ofnosocomial infections may require mul-tiple agents because of drug resistance,there has never been a good random-ized, prospective trial which hasdemonstrated the superior efficacy ofmulti-antibiotic therapy over a single-agent therapy for a mixed community-acquired infection. It goes withoutsaying that when there are multiple
choices of equivalent therapeuticagents, the safest should be employed.Also, once treatment has been startedwith a specific antibiotic, that agentshould only be changed if there is atrue therapeutic failure. Mid-coursechanging of antibiotics based solelyupon culture and sensitivity data in apatient otherwise doing well should bediscouraged since this increases thelikelihood of the emergence of resistantorganisms. Finally, the antibioticsshould be discontinued when there ispatient-specific evidence that the infec-tion has been controlled, such as returnof the white blood cell count to normallimits, lack of a fever, etc. The use ofan arbitrary number of days of treat-ment (whether strictly parenteral orcombined parenteral! oral) is an exam-ple of the physician treating him orherself rather than treatment of theindividual patient.
Although there have not been manynew antibiotics approved by the FDAover the last five years, there are severalnew agents which may soon becomeavailable over the couple of years. These.include new parenteral quinalones,cephalospor ins , and carbapenems. Inthe following section, some of thesenew agents will be discussed as well asnewer dosing regimens of currentlyaccepted antibiotics such as amino-glyeosides will be explored.
~-LACTAMS
The ~-Iactam group of antibiotics isthe single largest group of antimicrobialcompounds currently available, and com-
~-LACTAMASE GROUPS AND THEIR CHARACTERISTICS AS DEFINEDBY BLACTAMASE INHIBITOR ACTIVITY
~-Lactamase Group Bush Class Clavulanate Sulbactam Tazobactam
2a +++ +++ +++Staphylococcal Peniciiiinases(e.g. PCI)
Transferable, ~-Lactamases(e.q. TEM-I, SHV-I)
Chromosomal Cephalosporinases(e.g. P99, S2)
Extended-Spectrum ~-Lactamases(e.g. TEM-3 TEM- 10)
Metaiio-BLactamases(e.g. CerA, L1)
2b'
2b +++ ++ +++
+ ++
+++ +++++
3
Table 4. (Adapted and modified from Bush et aP')
72
prises the penicillins, eephalosporins,monobaetams, and earbapenems. Duringthe 1980's, a large number of ~-Iactamantibiotics, especially cephalosporins,were released by the pharmaceuticalindustry. Aided by their general effective-ness against a wide range of mixed aero-bic and anaerobic infections, this groupof agents also benefits from 'an excellentsafety profile when compared with themore traditional aminoglyeoside-basedtherapy. However, all ~-lactam drugs (toa greater or lesser degree) were quicklynoted to be vulnerable to resistancemediated by beta-lactamases,
~-lactamases are ubiquitous enzymesthat occur in almost all bacteria. All ~-lactam antibiotics share a four-mem-bered ring with a nitrogen in one cornerand a carbon with a double-bonded oxy-gen adjacent to it as part of their basicstructure. ~-lactamases are able to non-covalently bond to this ring between thenitrogen and the carbon with the dou-ble-bonded oxygen, and through hydrol-ysis open it up. This destroys the drug'sactivity. In general, gram-positive bacte-ria produce large amounts of ~-Iacta-mases that are excreted extra-cellularly.So much so that in some gram-positivebacteria, the ~-Iactamases expressed canactually constitute up to 1% of the dryweight of the bacterium. In gram nega-tive bacteria, ~-lactamases are found inlesser amounts, but are located in theperiplasmic spaces between the innerand outer cell membranes. Table 4 liststhe commonly accepted classes of the ~-lactamases. Some bacteria, especiallymembers of the Enterobacteriaceae,have the ability to synthesis largeamounts of, ~-lactamases if challengedwith a ~-lactam drug (induction). Somedrugs, such as cefamandole, are potentinducers of these enzymes with resultanttreatment failure. Some evidence isreported suggesting that Enterobacteria-ceae species, especially Enterobacter, areable to rapidly develop resistance tosome ~-lactam drugs (especiallycephalospor ins) with an increase inmortality rate." Two new third-genera-tion cephalosporins (cefepime and cef-pirome) are in the FDA approvalpipeline and appear to demonstratesome enhanced activity, which may bedue to increased resistance to the actionof these induced, ~-lactamases.14Whether this is intrinsic to the drugs oris simply a matter of their being newcompounds to which resistance willeventually occur is unknown at thistime.

B-lactamase inhibitor combina-tions are a group of B-lactam antibioticswhich were specifically designed toattempt to deal with B-lactamaseinduced resistance. The members of thisgroup of drugs include ampicillin/ sul-bactam (Unisyn'"), ticarcillin/ clavulanate(Tirncntin'f}, and a third compound,which was just gained FDA approval thisyear, piperacillin/tazobactam (Zosyn ®).This group of drugs works by suicideinhibition of the B-lactamases, where thesulbactam, clavulanate, and tazobactamall bind to the B-lactamases in a high-affinity, non-covalent complex which isnot hydrolyzed. Table 4 shows the rela-tive activity of these B-lactamaseinhibitors against the commonly occur-ring B-lactamase groups. As is shown,none of the current B-lactamaseinhibitors are highly effective against thechromosomally mediated B-lactamasesproduced by many of the more resistantvarieties of Enterobacteriaceae (such asEnterobacter, Citrobacter, Pseudomonas,etc.), although tazobactam and sulbac-tam appear to be more active against thisgroup of enzymes than clavulanate.
Zo svn'" (the new piperacillin/tazobactam combination) appears to bea particularly potent broad spectrumantibiotic, although this may be a reflec-tion of its newness. In mixed floraintra-abdominal infections, it was sig-nificantly more effective at eradicatingpathogens than the combination therapyof gentamicin and clindamycin (90% vs.80%, p<O.OI), and demonstrated anequivalent clinical cure rate (88% vs.77%, p=0.08).15 Similarly, equivalentclinical cure rates have been reportedfor Zosyn'" versus Timentin® in severeskin and soft tissue infections."
There is another mechanism foracquired bacterial resistance to B-lac-tam antibiotics that has become increas-ingly important. The ultimate targets ofB-lactam antibiotics are cell wall-syn-thesizing enzymes (penicillin-sensitiveenzymes or penicillin-binding proteins).These enzymes are present in essentiallyall bacteria, but vary from species tospecies in numbers, size, amount, andaffinity for B-lactam antibiotics.!" Theycontrol such fundamental processes ascell growth and division, and thereforewhen inhibited by B-lactam antibioticsresult in cell lysis, death, or growtharrest. The mechanism of resistance isan alteration of the B-lactam antibioticbinding site which decreases the abilityof the drug to bind to the enzyme.Alteration of the enzymes are more
commonly found in gram-positive thanin gram-negative bacteria.!" This is themethod by which Staphylococcus aureusand Staphylococcus epidermidis have devel-oped the resistance to methacillin thatnow plagues us. It is also the mecha-nism by which Streptococcus pneumoniae,veridans group streptococci, andEnterococcus species have increased sig-nificantly their resistance to essentiallythe entire group of B-lactam antibioticsduring the last 10-15 years (especiallyEnterococcus) .
AMINOGLYCOSIDES
For the last two decades, aminogly-cosides have remained major work hors-es in the treatment of severe infections.However, because of the availability ofnew broad spectrum antibiotics withwider safety margins (B-lactams andquinolones), aminoglycosides are beingreserved with increasing frequency foruse in severe/life-threatening or noso-comial infections. The great fear, ofcourse, has always been the toxicityproblems (nephrotoxicity and ototoxici-ty) for which amino,glycosides have beenknown. Unlike the ~-lactams, the effica-cy of aminoglycosides depends primarilyon the maximal concentration which isachieved in serum. There is a directrelationship between how much higherthe serum concentration of the amino-glycoside is than the minimum inhibito-ry concentration and the rate and extentof bacterial killing. IS
Unfortunately, fear of the toxic sideeffects of the aminoglyeosides has fre-quently resulted in the underdosing ofthese agents. More attention is typicallyplaced on the antibiotic trough levelthan on the peak serum concentration ofth~ antibiotic. A recent example of theeffect of this fear on clinical outcomedemonstrated a significant difference inthe occurrence of post-operative infec-tious complications in abdominal traumapatients treated with a beta-lactamantibiotic combination (aztreonam +clindamycin) versus patients treatedwith the combination of gentamiein andclindamycin.!" In this study, patients inthe aztreonam group had a significantlylower incidence of post-operative infec-tious complications than those in thegentamicin group (3% versus 19%,p<0.03). In reviewing their data theauthors felt that the reason for this dif-ference was due to chronic underdosingof the aminoglycoside.
Most all antibiotics, aminoglycosides
73
Surqical OverviewSURGICAL TECHNOLOGY INTERNATIONAL III
in particular, possess another mecha-nism to kill bacteria, called the post-antibiotic effect (PAE). This mechanismis the ability to continue suppression ofbacterial growth after exposure to thedrug at concentrations well below thedrug's minimum inhibitory concentra-tion for the infecting organism. Some ofthe manifestations of PAE includedelayed recovery of enzyme and non-enzyme protein activities; prolongedchanges in cell morphology, metabo-lism, growth, and generation times;changes in cell receptors and suscepti-bility to phagocytosis; and altered sus-ceptibility to an antibiotic followingr e-e xp o sur e.Y'' Although not wellunderstood, it is PAE which helpsexplain many of the inconsistenciesfound in antibiotic dosing, such as giv-ing gentamicin every eight hours andamikacin every twelve hours despitetheir serum half-lives being essentiallythe same. What this means for amino-glycosides is that the ability to continuebacterial growth suppression by PAEcan allow for a prolonged drug wash-out period. This allows for lower serumtrough levels of the drug, which shouldlead to decreased toxicity.
Gilbert" has suggested that becauseaminoglycosides demonstrate both signif-icant PAE and have such a direct correla-tion between serum concentration andbacterial killing, once daily dosing is notonly possible, but advantageous as well.Instead of the usual dosing of the patientevery 8 or 12 hours (3-5 mg/kg/ day forgentamicin and tobramycin, 15mg/kg/day for amikacin), the drug isadministered as a larger single dose oncea day (5-9 mg/kg/ day for gentamicin andtobramycin, 15-20 mg/kg/day foramikacin). Because of the higher initialpeak drug concentrations, both morerapid killing of bacteria as well as adecrease in the emergent of resistantpopulations can be achievecl.F Clinicaltrials in both intra-abdominal and otherserious mixed infections have demon-strated the efficacy of this approach.P:"Patients who are severely neutropenic,however, may not benefit from once dailydosing of aminoglycoside because of thepotential for rapid regrowth of bacteriaduring the last twelve hours of the dosinginterval is frequently seen in thesepatients. 25
In addition to providing higher peakserum levels, the other benefit of oncedaily aminoglycoside dosing appears tobe a decreased risk of nephrotoxicity.In individuals with normal renal func-

Antibiotic Update for the SurqeonBENNION
tion, once daily dosing results in serumtrough levels of less than 0.5 mg/dl.Clinical trials evaluating the efficacy ofonce daily aminoglycoside dosing ascompared to multiple dosing do notshow any significant therapeutic differ-ences,23,26,27and other studies indicate adefinite safety advantage for less fre-quent or once daily dosing of theseagents. 28,29
Another potential benefit to oncedaily aminoglycoside dosing is that itlessens the possibility of adaptive resis-tance. Closely related to PAE, adaptiveresistance is a short lived (less than twoto five hour) effect which causesreduced bactericidal activity followinga second antibiotic exposure. Seen pri-marily with aminoglycosides and somequinolones, it is probably due toreduced transport of the antibiotic intothe cell and is of finite duration. 30Increasing the dosing intervals negatesthe effect.
QUiNOLONES
The quinolones constitute an unusu-al group of antibiotics in that they arecompletely man-made. This is in con-tradistinction to essentially all othergroups of antibiotics which are variantsof chemical compounds isolated frombacteria. Because of this, it is possiblethat as a group, quinolones may growto have the largest number of distinctcompounds of all antibiotics (morethan even the ~-lactams). Actingdirectly on the bacteria's DNA,quinolones are potent bacterial killingagents that are very effective against awide variety of gram negative and grampositive bacteria. Although currentlylicensed quinolones (e.g., ciprofloxacinand ofloxacin) are primarily effectiveonly against aerobic organisms, thereare newer experimental quinolones(e.g. clinafloxacin) which appear to beeffective against not only gram positiveand gram negative bacteria but bothaerobes and anaerobes as well." Such aquinolone would offer true single-agent therapeutics similar to many ofthe ~-lactam antibiotics, which currentquinolones lack.
Although not yet approved for thetreatment of intra-abdominal infections(the indication application has been sub-mitted to the FDA), parenteralquinolones have been approved for, andare very effective in, the treatment ofother severe mixed infections in thelower respiratory tract, urinary tract,
and skin and soft tissues. These agentshave the distinct advantage that th<J notsubject to the actions of inducible [j-Iac-tamases, especially those of the chro-mosomal group found in the gramnegative bacilli, which is becoming aproblem with the ~-lactam antibiotics.Another advantage is the possibility ofswitching a patient with a serious gramnegative infection from parenteral tooral therapy using the same agent.Considered by some the Holy Grail oftreatment options for its potential costand hospitalization savings, it has neverbeen properly studied in a randomized,prospective clinical trial (though thatmay change very soon). However, thereare groups who have been employingthis form of treatment in patients withnormal gut function and who haveresponded to initial parenteral treat-ment if cultures showed quinolone-sen-sitive organisms with success. 32
6LYCOPEPTIDES
Effective only against gram positiveorganisms, the glycopeptide group ofantibiotics is made up of vancomycinand teicoplanin (which is not yet com-mercially available in the US). Becauseof the emergence of Significant resis-tance by Enterococcus sp., and to a lesserextent Staphylococcus sp., to ~-lactarns,arninoglycosides, and even quinolones,glycopeptides have emerged over theyears as the primary agents for thetreatment of sepsis from gram positivebacteria, eSfecially in the immunocom-promised. 3 However, over the lastcouple of years enterococci resistant tovancomycin have been reported withdisturbing frequency in both Europeand North American. 34,35Caused byinducible enzymes which alter peptido-glycan precursors so as >todecrease thebinding ability of glycopeptide antibi-otics, this resistance has forced a re-evaluation of the empiric use of theseagents. Vancomycin, specifically,should not be used in a frivolous man-ner for either prophylaxis or treat-ment, but rather should be employedonly when there is either a significantrisk for an infectious complication dueto methicillin-resistant staphylococci orfor treatment of an established infec-tion resistant to other agents but sus-ceptible to vancomycin. Too frequentuse of vancomycin, particularly in theICU environment, may well be themajor determinant of development ofresistant organisms (especially entcro-
74
cocci) that has plagued many largeteaching centers recently. Em
REFERENCES
1. Sande MA, Kapusnik-Uner ]E, MandellGL: Antimicrobial agents. General considera-tions, in Gilman AG, Rall TW, Nies AS,Taylor P (eds): Goodman and Gilman's ThePharmacoloqical Basis rj Therapeutics (8th ed).New York:Pergamon Press, 1990, pp. 1018-1046.2. Burke ]F: The effective period of preven-tive antibiotic action in experimental incisionsand dermal lesions. SurBer'y 1961; 50:161-168.3. Alexander ]W, Altemeier WA: Penicillinprophylaxis of experimental staphylococcalwound infections. SurB G'ynecol Obstet 1965;120: 243-254.4. Berger SA, Nagar H, Weitzman S:Prophylactic antibiotics in surgical proce-dures. Surq Gynecol Obstet 1978; 146:469-475.5. Hirschman]V, Invi TS: Antimicrobial pro-phylaxis: a critique of recent trials. Rev InfectDis 1980; 2:1-23.6. Classen DC, Evans RS, Pestotnik SL, et al:The timing of prophylactic administration ofantibiotics and the risk of surgical-woundinfection. NEnal)Med 1992; 326:281-286.7. Antimicrobial prophylaxis in surgery. MedLetter 1993; 35:91-94.8. Academy of Sciences National ResearchCouncil: Postoperative wound infections: theinfluence of ultraviolet irradiation of the oper-ating room and of various other factors. AnnSura 1964; 160(Suppl 2): 1-192.9. Olson M, O'Connor M, Schwartz ML:Surgical wound infections: a 5-year prospec-tive study of 20,193 wounds at theMinneapolis VA Medical Center. Ann Sura1984; 199:253-260.10. Haley RW, Culver DH, Morgan WM, etal: Identifying patients at high- risk of surgicalwound infection: a simple multivariate indexof patient susceptibility and wound contami-nation. Am) Epidemiol1985; 121:206-213.11. Culver DH, Horan TC, Gaynes RP, et al:Surgical wound infection rates by woundclass, operative procedure, and patient riskindex. Am )Med 1991; 91 (Suppl 3B): 15 2S-157S.12. Bush K, Macalintal C, Rasmussen BA, etal: Kinetic interactions of azobactam with p-lactamases from all major structural classes.Antimicrob Aqents Chemother 1993; 37:851-858.13.Chow ]W, Fine MJ, Shlaes DM, et al:Enterobacter bacteremia: clinical features andemergence of antibiotic resistance duringtherapy. Ann Intern Med 1991; 115:5B5-590.14.Sanders CC, Sanders WE: Beta-lactamresistance in gram-negative bacteria: globaltrends and clinical impact. Clin Inject Dis1992; 15:824-B39.15.Polk HC, Fink MP, Laverdiere M, et al:Prospective randomized study ofpiperacillin/ tazobactam therapy of surgicallytreated intra-abdominal infections. Am Sura1993; 59:598-605.16. Tan ]S, Wishnow RM, Talan DA, et al:Treatment of hospitalized patients with com-plicated skin and skin structure infections: a

double-blind, randomized, multicenter studyof piperacillin-tazobactam versus ticarcillin-clavulanate. Antimicrob Agents Chemother 1993;37:1580-1586.17. Georgopapadakou NH: Penicillin-bindingproteins and bacterial resistance to ~-Iactams.Antimicrob Agents Chemother 1993; 37:2045-2053.18.Moore RD, Smith CR, Lietman PS:Association of aminoglycoside plasma levelswith therapeutic outcome in gram-negativepneumonia. Am]Med 1984; 77:657-662.19. Fabian TC, Hess MM, Croce MA, et al:Superiority of aztreonam/ clindamycin com-pared with gentamicin/ clindamycin inpatients with penetrating abdominal trauma.Am]Surg1994; 167:291-296.20.MacKenzie FM, Gould 1M: The post-antibiotic effect.] Antimicrob Chetnother 1993;32:519-537.21. Gilbert DN: Once-daily aminoglycosidetherapy. Antimicrob Agents Chemother 1991;35:399-405.22.Blazer J, Stone BB, Groner MC, et al:Comparative study with enoxacin andnetilmicin in a pharmacodynamic model todetermine importance of ratio of antibioticpeak concentration to MIC for bactericidalactivity and emergence of resistance.Antimicrob Agents Chemother 1987;31: 1054-1060.23. Hollender LF, Bahnini LFJ, DeManzini N,
et al: A multicentric study of netilmicin oncedaily versus thrice daily in patients withappendicitis and other intra-abdominal infec-tions.] Antimicrob Cbemother 1989; 23:773-783.24. Nordstrom LH, Ringbcrg S, Cromberg 0,et al: Does administration of an aminoglyco-side in a single daily dose affect its efficacy andtoxicity? ] Antimicrob Chemother 1990; 25: 159-173.25.Kapusnik JR, Hackbarth C], ChambersHF, ct al: Single large daily dosing versusintermittent dosing of tobramvcin for treatingexperimental Pseudomonas pneumonia. ] lifectDis 1988;158:7-12.26.Fan ST, Lau WY, Teoh-Chan CH, ct al:Oncc daily administration of nctilmicin com-pared with thrice daily, both in combinationwith metronidazole, in gangrenous and perfo-rated appendicitis. ] Antimicrob Chemother1988; 22:69-74.27.Maller R, Isaksson B, Nilsson K, et al: Astudy of amikacin given once versus twicedaily in serious infections. ] AntimicrobCbemother 1988; 22:75-79.28. Powell SH, Thompson WL, Luthe MA, ctal: Once-daily vs continuous aminoglycosidedosing: efficacy and toxicity in animal andclinical studies of gentamicin, netilmicin, andtobramycin.] IifectDis 1983; 147:918-932.29.Wood CA, Norton DR, Kohlhcpp SI, etal: The influence of tobramycin dosage regi-
Surgical OverviewSURGICAL TECHNOLOGY INTERNATIONAL III
mens on nephrotoxicity, ototoxicity, andantibacterial efficacy in a rat model of subcu-taneous abscess.] Iifect Dis 1988; 158:13-22.30.Gould 1M, Milne K, Jason C:Concentration-depcndent bacterial killing,adaptive resistance and post-antibiotic effectof ciprofloxacin alonc and in combinationwith gentamicin. Drugs Esp Clin Res 1990;16:621-628.31.Ford AS, Baltch AL, Smith RP, et al: In-vitro susceptibilities of Pseudomonas aeruginosaand Pseudomonas spp. to the new fluoro-quinolones clinafloxacin and PD 131628 andnine other antimicrobial agents. ] AntimicrobChemother 1993; 31 :523-532.32. Solomkin JS, Miyagawa CI: Principles ofantibiotic therapy. Surg Clin North Am 1994;74:497 -517.33.Rolston KVI, Hieu N, Amos G, et al: Arandomized double-blind trial of vancomycinversus teicoplanin for the treatment of gram-positive bacteremia in patients with cancer. ]lifect Dis 1994; 169:350-355.34. Livornese LL, Dias S, Samel C, et al:Hospital-acquired infection with vancomycin-resistant Enterococcus faecium transmitted byelectronic thermometers. Ann Intern Med19;92; 11 7:1121 16.35. Rubin LG, Tucci V, Cercenado E, et al:Vancomycin-resistant Enterococcus Jaecium inhospitalized children. Inject Control HospEpidemio11992; 13:700-705.
75