Embed Size (px)
Citation preview
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 1 -
Antibiotic guideline in Adult Cystic Fibrosis Choice of antibiotics in cystic fibrosis is based on several factors including organism sensitivity, history of adverse reactions or allergy and severity of symptoms. In most cases, at least two antibiotics are prescribed together in order to limit the emergence of superinfection with resistant strains or pathogens which may be present in sputum but not consistently present on culture. The incidence of Closdtridium difficile in CF is low, so the restriction on use of drugs which commonly cause C. difficile. diarrhoea in other patient groups is less critical. In patients colonised by multiple pathogens often a third (or more) antibiotic may be required. Specialist advice is required in complex cases. Individual antibiotic regimens should be based on sputum sensitivity results, however a response is often observed despite in vitro resistance. Synergy testing may be useful to guide antimicrobial choice where multi-resistant organisms are cultured. Where possible treatment regimens are designed to maximise patient adherence and minimise adverse effects. This is a guideline only and individual patient factors should be considered when selecting treatment, including:
Interactions should be checked, especially in post-transplant patients who will be taking immunosuppressant drugs
Low body weight patients under 50kg a dose reduction be required
Doses may need to be reduced in renal impairment
History of allergic reactions or documented intolerances Courses are generally given for two weeks. Response to treatment should be assessed at end of the first and second weeks. A third week of treatment should be considered if there has been a partial response. Poor response requires review of treatment. Several drugs also can cause photosensitivity on exposure to sunlight (e.g. quinilones and tetracyclines) and patients should be warned about this and how to avoid it.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 2 -
These guidelines have been produced by a working group including the Scottish Adult Cystic Fibrosis team, pharmacy and microbiology departments. They are intended to be used along side national guidance such as Antibiotic Treatment for Cystic Fibrosis, 3rd Edition, May 2009, Cystic Fibrosis Trust and local expertise. [http://www.cftrust.org.uk/aboutcf/publications/consensusdoc/Antibiotic_treatment_for_Cystic_Fibrosis.pdf] It is the intention of the group to carry out ongoing surveillance and regular audit of critical areas such as C difficile incidence, contamination of samples, patterns of infection and resistance and MRSA acquisition/colonisation/eradication and treatment outcomes. These guidelines will be regularly updated and reviewed in line with emerging evidence, change in practice and results of surveillance and audits. Date written: 08 June 2011 Written by: Douglas McCabe, Pharmacist, Cystic Fibrosis Approved by: Dr Ian Laurenson, Consultant Microbiologist
Dr Helen Rodgers, Clinical Director of Adult CF Service Professor Andrew Greening, Consultant Physician Dr Alastair Innes, Consultant Physician
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 3 -
Table of contents
Table Title Page
1
Common gram-positive infections Haemophilus influenzae, Staphylococcus aureus,
4
2 2a 2b
MRSA Eradication Exacerbation
5
3 3a 3b 3c
Pseudomonas aeruginosa Eradication Exacerbation Chronic infection
7
4 4a 4b 4c
Other gram-negative infections Burkholeria cepacia complex, Stenotrophomonas maltophillia, Achromobacter (Alcaligenes) xylosoxidans
9
5 5a 5b
Fungal infections Oral candidiasis ABPA
11
6 Non-tuberculous mycobacteria 12
7 Totally implantable intravenous access device (TIVAD) infections 12
8 Oral antimicrobials dosing 13
9 Intravenous antimicrobials dosing 14
10 Diluents and flushes 15
11 Desensitisation 16
12 Renal doses 17
13 Cost of commonly prescribed antimicrobials 20
14 Summary chart of antimicrobial choices 21
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 4 -
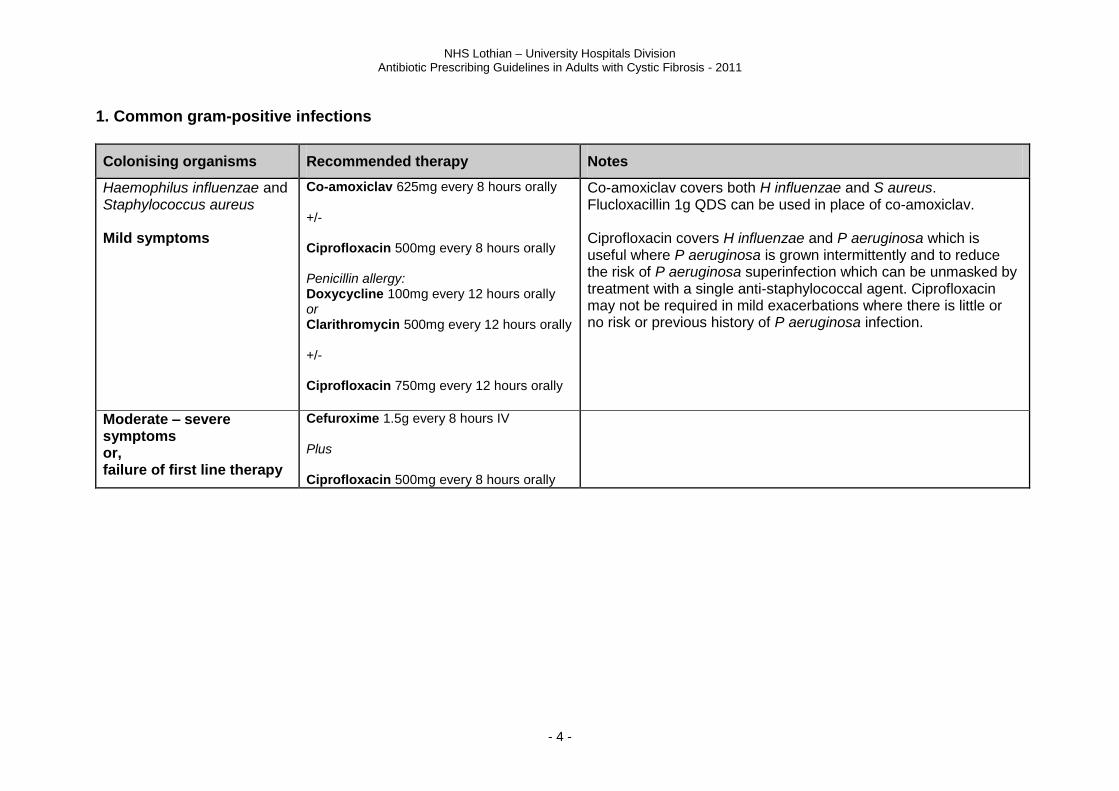
1. Common gram-positive infections
Colonising organisms Recommended therapy Notes
Haemophilus influenzae and Staphylococcus aureus Mild symptoms
Co-amoxiclav 625mg every 8 hours orally +/- Ciprofloxacin 500mg every 8 hours orally Penicillin allergy: Doxycycline 100mg every 12 hours orally or Clarithromycin 500mg every 12 hours orally +/- Ciprofloxacin 750mg every 12 hours orally
Co-amoxiclav covers both H influenzae and S aureus. Flucloxacillin 1g QDS can be used in place of co-amoxiclav. Ciprofloxacin covers H influenzae and P aeruginosa which is useful where P aeruginosa is grown intermittently and to reduce the risk of P aeruginosa superinfection which can be unmasked by treatment with a single anti-staphylococcal agent. Ciprofloxacin may not be required in mild exacerbations where there is little or no risk or previous history of P aeruginosa infection.
Moderate – severe symptoms or, failure of first line therapy
Cefuroxime 1.5g every 8 hours IV Plus Ciprofloxacin 500mg every 8 hours orally
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 5 -
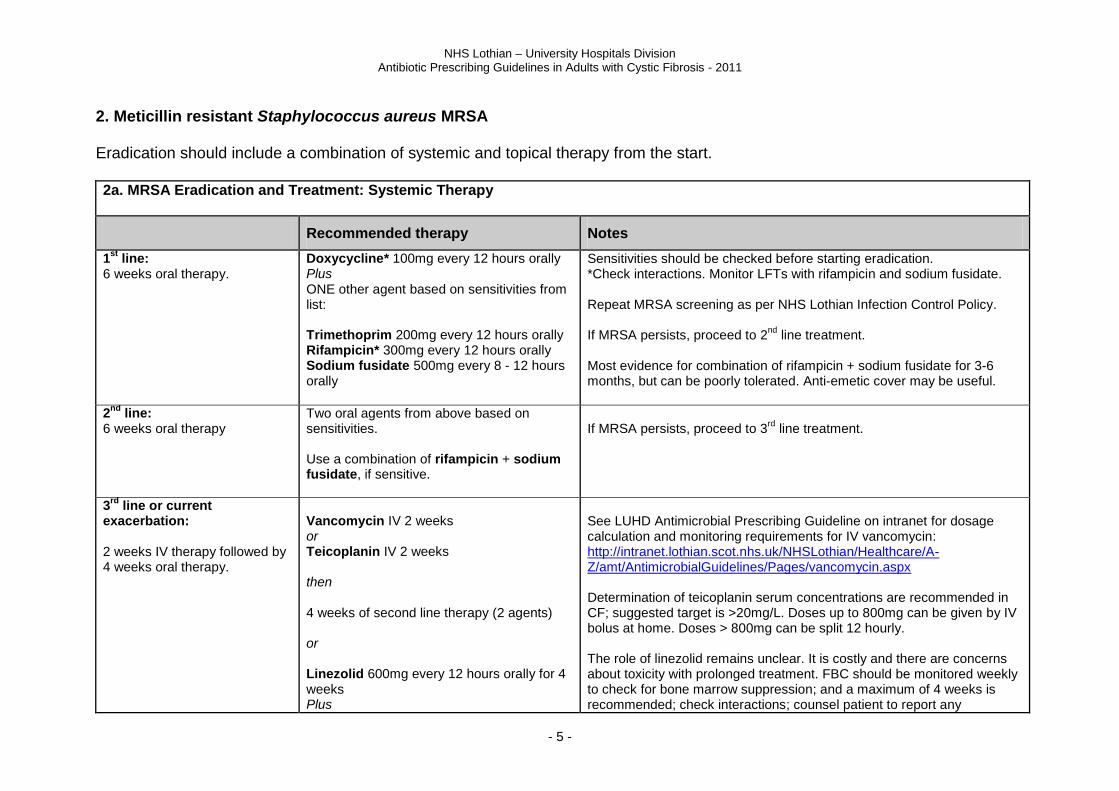
2. Meticillin resistant Staphylococcus aureus MRSA Eradication should include a combination of systemic and topical therapy from the start. 2a. MRSA Eradication and Treatment: Systemic Therapy
Recommended therapy Notes
1st
line: 6 weeks oral therapy.
Doxycycline* 100mg every 12 hours orally Plus ONE other agent based on sensitivities from list: Trimethoprim 200mg every 12 hours orally Rifampicin* 300mg every 12 hours orally Sodium fusidate 500mg every 8 - 12 hours orally
Sensitivities should be checked before starting eradication. *Check interactions. Monitor LFTs with rifampicin and sodium fusidate. Repeat MRSA screening as per NHS Lothian Infection Control Policy. If MRSA persists, proceed to 2
nd line treatment.
Most evidence for combination of rifampicin + sodium fusidate for 3-6 months, but can be poorly tolerated. Anti-emetic cover may be useful.
2nd
line: 6 weeks oral therapy
Two oral agents from above based on sensitivities. Use a combination of rifampicin + sodium fusidate, if sensitive.
If MRSA persists, proceed to 3
rd line treatment.
3rd
line or current exacerbation: 2 weeks IV therapy followed by 4 weeks oral therapy.
Vancomycin IV 2 weeks or Teicoplanin IV 2 weeks then 4 weeks of second line therapy (2 agents) or Linezolid 600mg every 12 hours orally for 4 weeks Plus
See LUHD Antimicrobial Prescribing Guideline on intranet for dosage calculation and monitoring requirements for IV vancomycin: http://intranet.lothian.scot.nhs.uk/NHSLothian/Healthcare/A-Z/amt/AntimicrobialGuidelines/Pages/vancomycin.aspx Determination of teicoplanin serum concentrations are recommended in CF; suggested target is >20mg/L. Doses up to 800mg can be given by IV bolus at home. Doses > 800mg can be split 12 hourly. The role of linezolid remains unclear. It is costly and there are concerns about toxicity with prolonged treatment. FBC should be monitored weekly to check for bone marrow suppression; and a maximum of 4 weeks is recommended; check interactions; counsel patient to report any
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 6 -
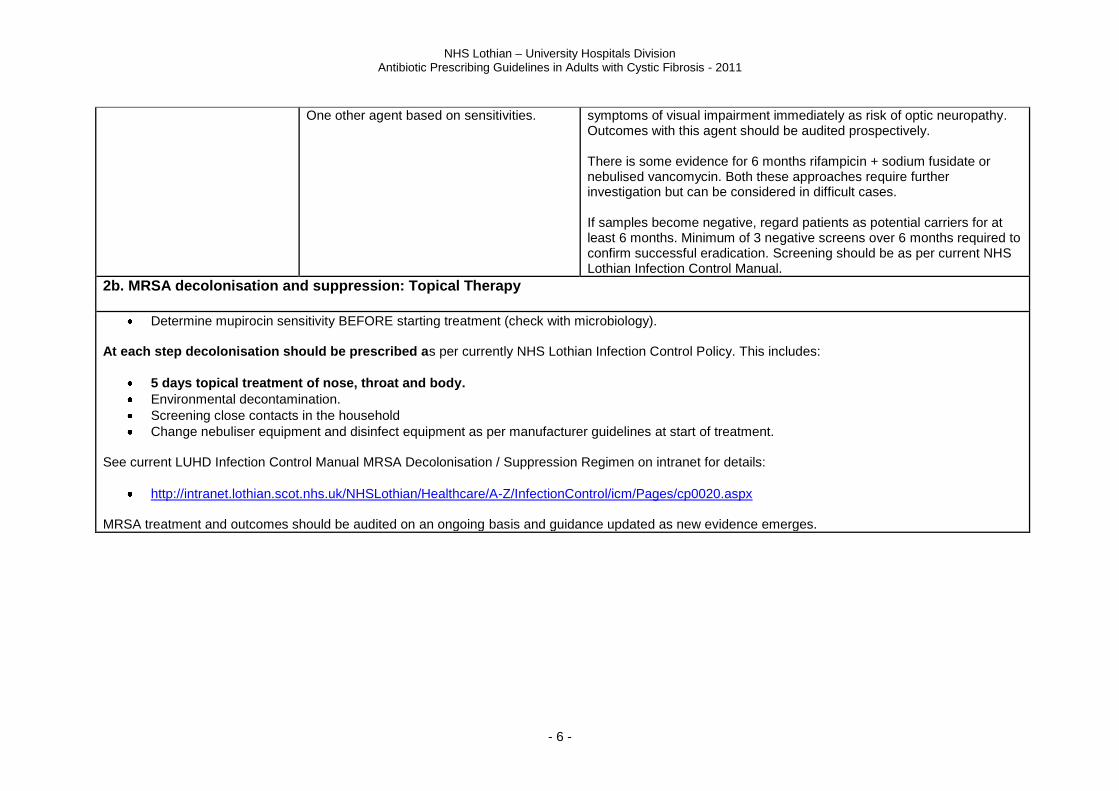
One other agent based on sensitivities.
symptoms of visual impairment immediately as risk of optic neuropathy. Outcomes with this agent should be audited prospectively. There is some evidence for 6 months rifampicin + sodium fusidate or nebulised vancomycin. Both these approaches require further investigation but can be considered in difficult cases. If samples become negative, regard patients as potential carriers for at least 6 months. Minimum of 3 negative screens over 6 months required to confirm successful eradication. Screening should be as per current NHS Lothian Infection Control Manual.
2b. MRSA decolonisation and suppression: Topical Therapy
Determine mupirocin sensitivity BEFORE starting treatment (check with microbiology). At each step decolonisation should be prescribed as per currently NHS Lothian Infection Control Policy. This includes:
5 days topical treatment of nose, throat and body.
Environmental decontamination.
Screening close contacts in the household
Change nebuliser equipment and disinfect equipment as per manufacturer guidelines at start of treatment. See current LUHD Infection Control Manual MRSA Decolonisation / Suppression Regimen on intranet for details:
http://intranet.lothian.scot.nhs.uk/NHSLothian/Healthcare/A-Z/InfectionControl/icm/Pages/cp0020.aspx MRSA treatment and outcomes should be audited on an ongoing basis and guidance updated as new evidence emerges.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 7 -
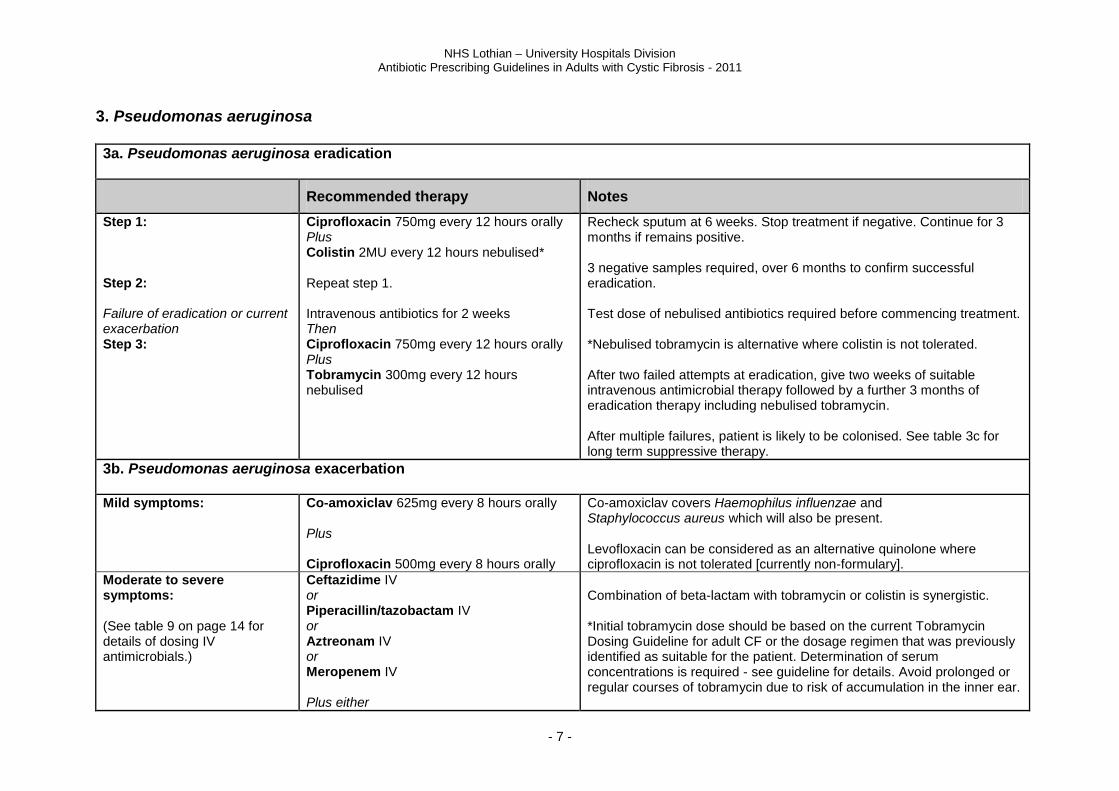
3. Pseudomonas aeruginosa 3a. Pseudomonas aeruginosa eradication
Recommended therapy Notes
Step 1: Step 2: Failure of eradication or current exacerbation Step 3:
Ciprofloxacin 750mg every 12 hours orally Plus Colistin 2MU every 12 hours nebulised* Repeat step 1. Intravenous antibiotics for 2 weeks Then Ciprofloxacin 750mg every 12 hours orally Plus Tobramycin 300mg every 12 hours nebulised
Recheck sputum at 6 weeks. Stop treatment if negative. Continue for 3 months if remains positive. 3 negative samples required, over 6 months to confirm successful eradication. Test dose of nebulised antibiotics required before commencing treatment. *Nebulised tobramycin is alternative where colistin is not tolerated. After two failed attempts at eradication, give two weeks of suitable intravenous antimicrobial therapy followed by a further 3 months of eradication therapy including nebulised tobramycin. After multiple failures, patient is likely to be colonised. See table 3c for long term suppressive therapy.
3b. Pseudomonas aeruginosa exacerbation Mild symptoms:
Co-amoxiclav 625mg every 8 hours orally Plus Ciprofloxacin 500mg every 8 hours orally
Co-amoxiclav covers Haemophilus influenzae and Staphylococcus aureus which will also be present. Levofloxacin can be considered as an alternative quinolone where ciprofloxacin is not tolerated [currently non-formulary].
Moderate to severe symptoms: (See table 9 on page 14 for details of dosing IV antimicrobials.)
Ceftazidime IV or Piperacillin/tazobactam IV or Aztreonam IV or Meropenem IV
Plus either
Combination of beta-lactam with tobramycin or colistin is synergistic. *Initial tobramycin dose should be based on the current Tobramycin Dosing Guideline for adult CF or the dosage regimen that was previously identified as suitable for the patient. Determination of serum concentrations is required - see guideline for details. Avoid prolonged or regular courses of tobramycin due to risk of accumulation in the inner ear.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 8 -
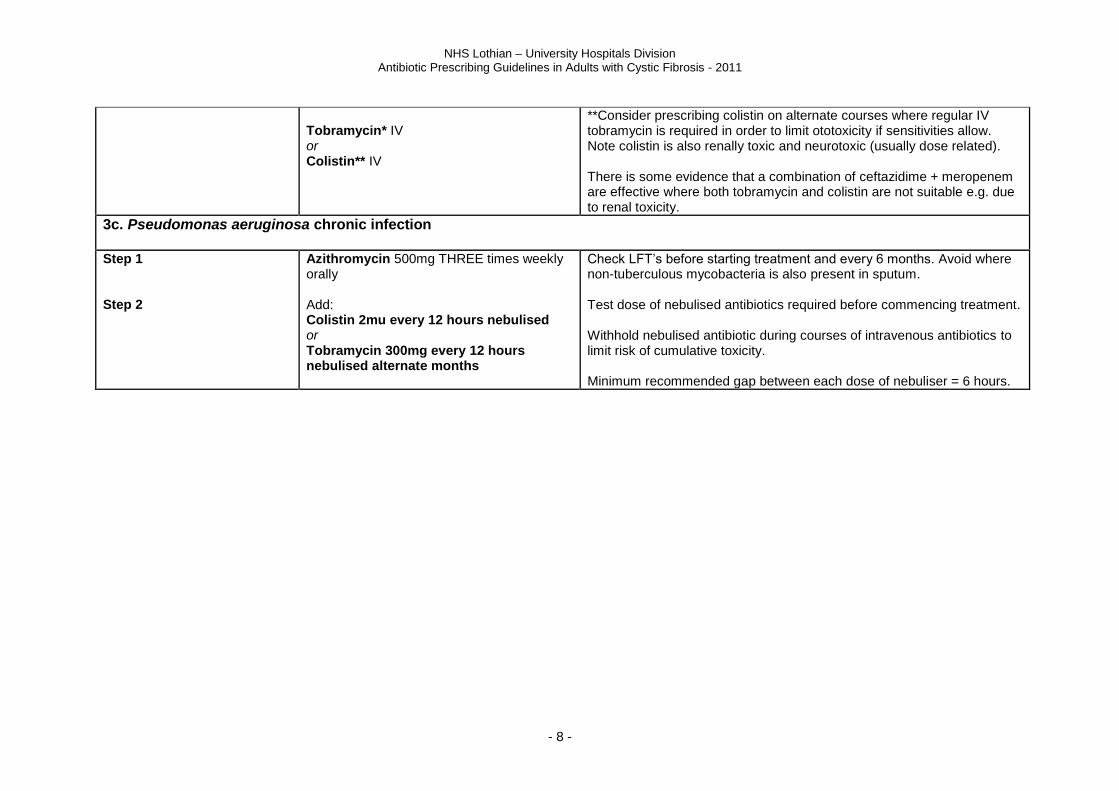
Tobramycin* IV or Colistin** IV
**Consider prescribing colistin on alternate courses where regular IV tobramycin is required in order to limit ototoxicity if sensitivities allow. Note colistin is also renally toxic and neurotoxic (usually dose related). There is some evidence that a combination of ceftazidime + meropenem are effective where both tobramycin and colistin are not suitable e.g. due to renal toxicity.
3c. Pseudomonas aeruginosa chronic infection Step 1 Step 2
Azithromycin 500mg THREE times weekly orally Add: Colistin 2mu every 12 hours nebulised or Tobramycin 300mg every 12 hours nebulised alternate months
Check LFT’s before starting treatment and every 6 months. Avoid where non-tuberculous mycobacteria is also present in sputum. Test dose of nebulised antibiotics required before commencing treatment. Withhold nebulised antibiotic during courses of intravenous antibiotics to limit risk of cumulative toxicity. Minimum recommended gap between each dose of nebuliser = 6 hours.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 9 -
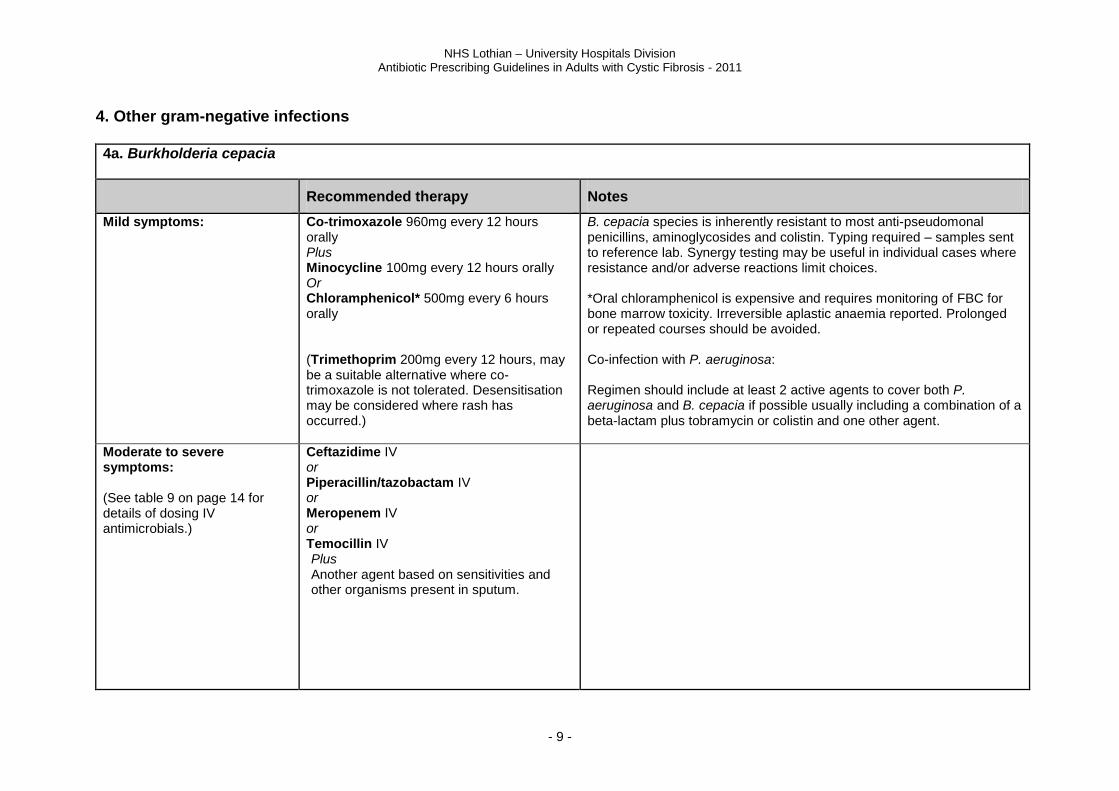
4. Other gram-negative infections 4a. Burkholderia cepacia
Recommended therapy Notes
Mild symptoms:
Co-trimoxazole 960mg every 12 hours orally Plus Minocycline 100mg every 12 hours orally Or Chloramphenicol* 500mg every 6 hours orally (Trimethoprim 200mg every 12 hours, may be a suitable alternative where co-trimoxazole is not tolerated. Desensitisation may be considered where rash has occurred.)
B. cepacia species is inherently resistant to most anti-pseudomonal penicillins, aminoglycosides and colistin. Typing required – samples sent to reference lab. Synergy testing may be useful in individual cases where resistance and/or adverse reactions limit choices. *Oral chloramphenicol is expensive and requires monitoring of FBC for bone marrow toxicity. Irreversible aplastic anaemia reported. Prolonged or repeated courses should be avoided. Co-infection with P. aeruginosa: Regimen should include at least 2 active agents to cover both P. aeruginosa and B. cepacia if possible usually including a combination of a beta-lactam plus tobramycin or colistin and one other agent.
Moderate to severe symptoms: (See table 9 on page 14 for details of dosing IV antimicrobials.)
Ceftazidime IV or Piperacillin/tazobactam IV or Meropenem IV or Temocillin IV Plus Another agent based on sensitivities and other organisms present in sputum.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 10 -
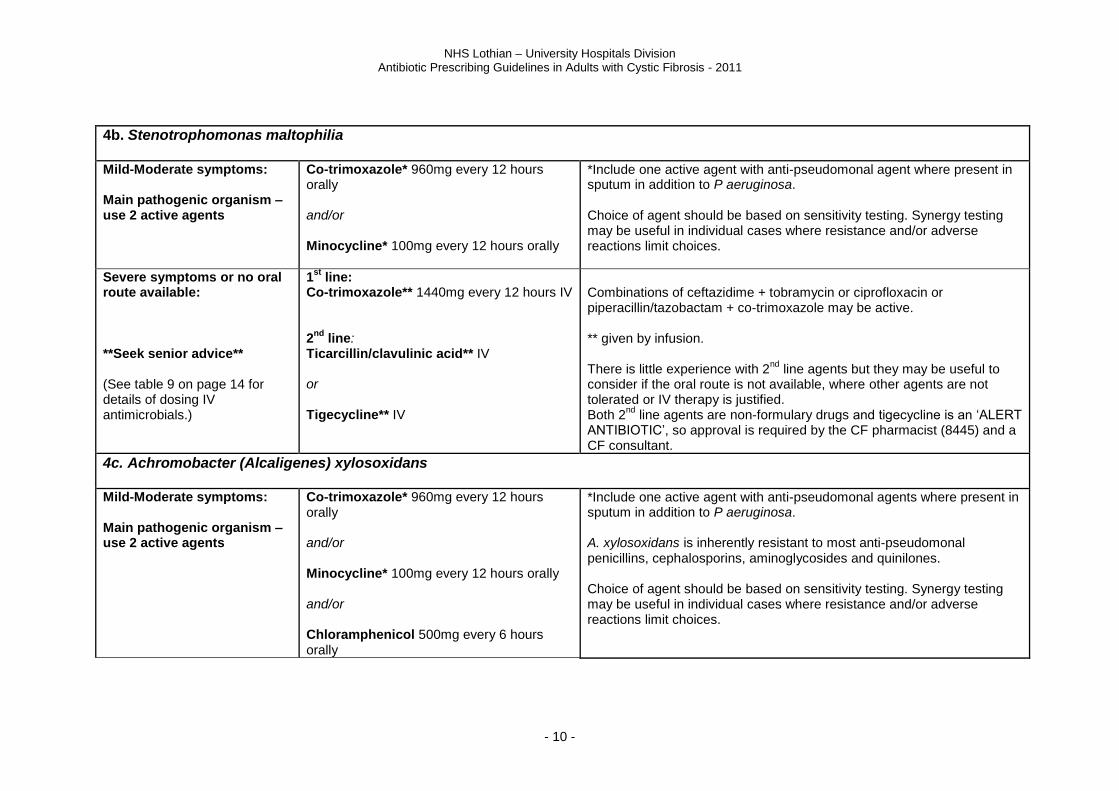
4b. Stenotrophomonas maltophilia Mild-Moderate symptoms: Main pathogenic organism – use 2 active agents
Co-trimoxazole* 960mg every 12 hours orally and/or Minocycline* 100mg every 12 hours orally
*Include one active agent with anti-pseudomonal agent where present in sputum in addition to P aeruginosa. Choice of agent should be based on sensitivity testing. Synergy testing may be useful in individual cases where resistance and/or adverse reactions limit choices.
Severe symptoms or no oral route available: **Seek senior advice** (See table 9 on page 14 for details of dosing IV antimicrobials.)
1st
line: Co-trimoxazole** 1440mg every 12 hours IV 2
nd line:
Ticarcillin/clavulinic acid** IV or Tigecycline** IV
Combinations of ceftazidime + tobramycin or ciprofloxacin or piperacillin/tazobactam + co-trimoxazole may be active. ** given by infusion. There is little experience with 2
nd line agents but they may be useful to
consider if the oral route is not available, where other agents are not tolerated or IV therapy is justified. Both 2
nd line agents are non-formulary drugs and tigecycline is an ‘ALERT
ANTIBIOTIC’, so approval is required by the CF pharmacist (8445) and a CF consultant.
4c. Achromobacter (Alcaligenes) xylosoxidans Mild-Moderate symptoms: Main pathogenic organism – use 2 active agents
Co-trimoxazole* 960mg every 12 hours orally and/or Minocycline* 100mg every 12 hours orally and/or Chloramphenicol 500mg every 6 hours orally
*Include one active agent with anti-pseudomonal agents where present in sputum in addition to P aeruginosa. A. xylosoxidans is inherently resistant to most anti-pseudomonal penicillins, cephalosporins, aminoglycosides and quinilones. Choice of agent should be based on sensitivity testing. Synergy testing may be useful in individual cases where resistance and/or adverse reactions limit choices.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 11 -
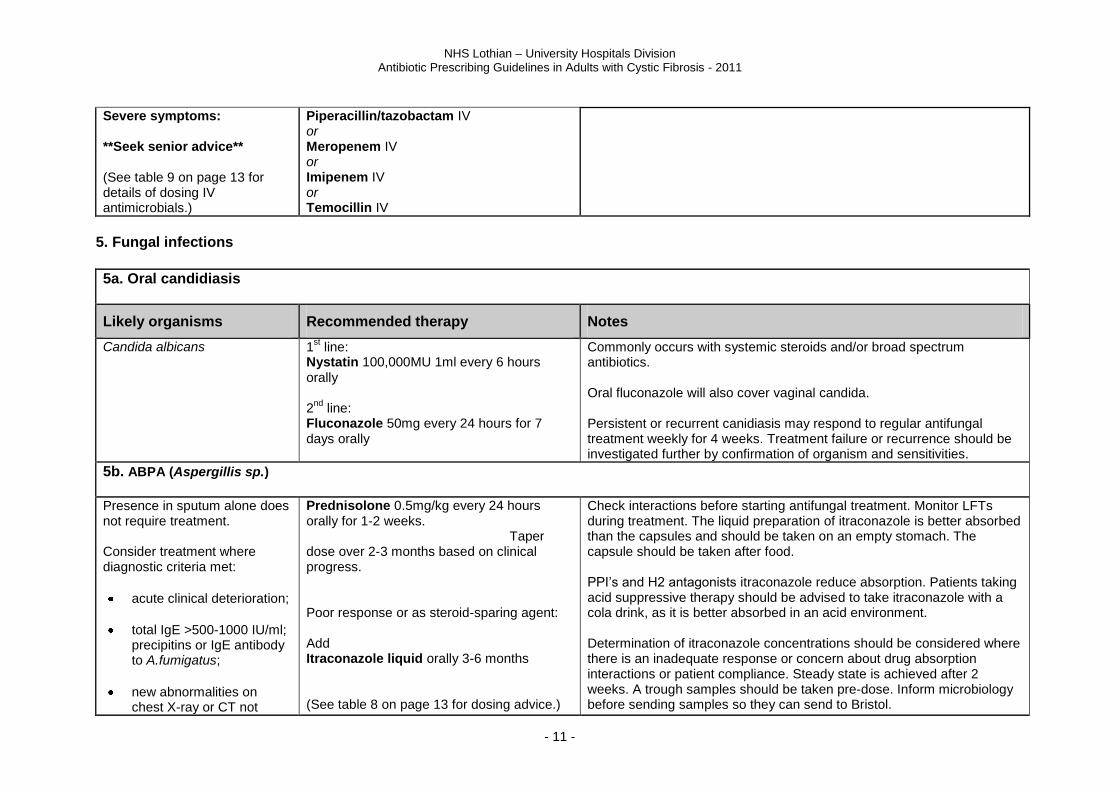
Severe symptoms: **Seek senior advice** (See table 9 on page 13 for details of dosing IV antimicrobials.)
Piperacillin/tazobactam IV or Meropenem IV or Imipenem IV or Temocillin IV
5. Fungal infections
5a. Oral candidiasis
Likely organisms Recommended therapy Notes
Candida albicans
1st line:
Nystatin 100,000MU 1ml every 6 hours orally 2
nd line:
Fluconazole 50mg every 24 hours for 7 days orally
Commonly occurs with systemic steroids and/or broad spectrum antibiotics. Oral fluconazole will also cover vaginal candida. Persistent or recurrent canidiasis may respond to regular antifungal treatment weekly for 4 weeks. Treatment failure or recurrence should be investigated further by confirmation of organism and sensitivities.
5b. ABPA (Aspergillis sp.)
Presence in sputum alone does not require treatment. Consider treatment where diagnostic criteria met:
acute clinical deterioration;
total IgE >500-1000 IU/ml; precipitins or IgE antibody to A.fumigatus;
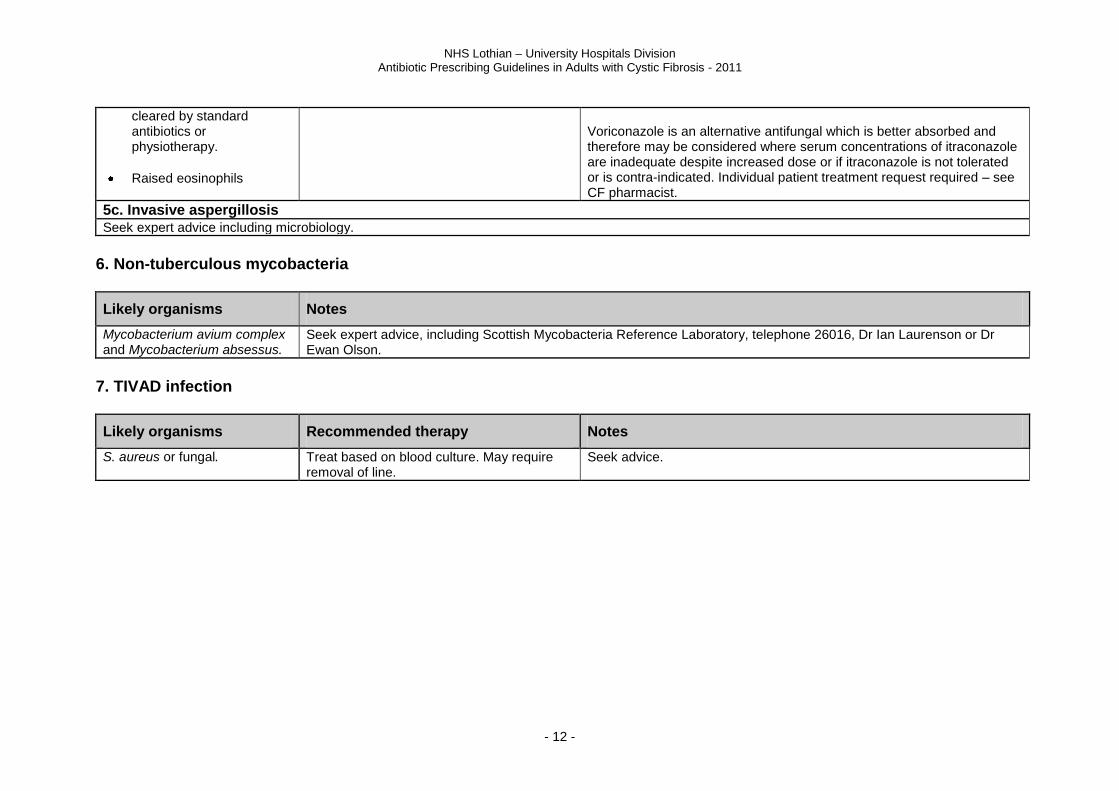
new abnormalities on chest X-ray or CT not
Prednisolone 0.5mg/kg every 24 hours orally for 1-2 weeks. Taper dose over 2-3 months based on clinical progress. Poor response or as steroid-sparing agent: Add Itraconazole liquid orally 3-6 months (See table 8 on page 13 for dosing advice.)
Check interactions before starting antifungal treatment. Monitor LFTs during treatment. The liquid preparation of itraconazole is better absorbed than the capsules and should be taken on an empty stomach. The capsule should be taken after food. PPI’s and H2 antagonists itraconazole reduce absorption. Patients taking acid suppressive therapy should be advised to take itraconazole with a cola drink, as it is better absorbed in an acid environment. Determination of itraconazole concentrations should be considered where there is an inadequate response or concern about drug absorption interactions or patient compliance. Steady state is achieved after 2 weeks. A trough samples should be taken pre-dose. Inform microbiology before sending samples so they can send to Bristol.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 12 -
cleared by standard antibiotics or physiotherapy.
Raised eosinophils
Voriconazole is an alternative antifungal which is better absorbed and therefore may be considered where serum concentrations of itraconazole are inadequate despite increased dose or if itraconazole is not tolerated or is contra-indicated. Individual patient treatment request required – see CF pharmacist.
5c. Invasive aspergillosis Seek expert advice including microbiology.
6. Non-tuberculous mycobacteria
Likely organisms Notes
Mycobacterium avium complex and Mycobacterium absessus.
Seek expert advice, including Scottish Mycobacteria Reference Laboratory, telephone 26016, Dr Ian Laurenson or Dr Ewan Olson.
7. TIVAD infection
Likely organisms Recommended therapy Notes
S. aureus or fungal. Treat based on blood culture. May require removal of line.
Seek advice.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 13 -
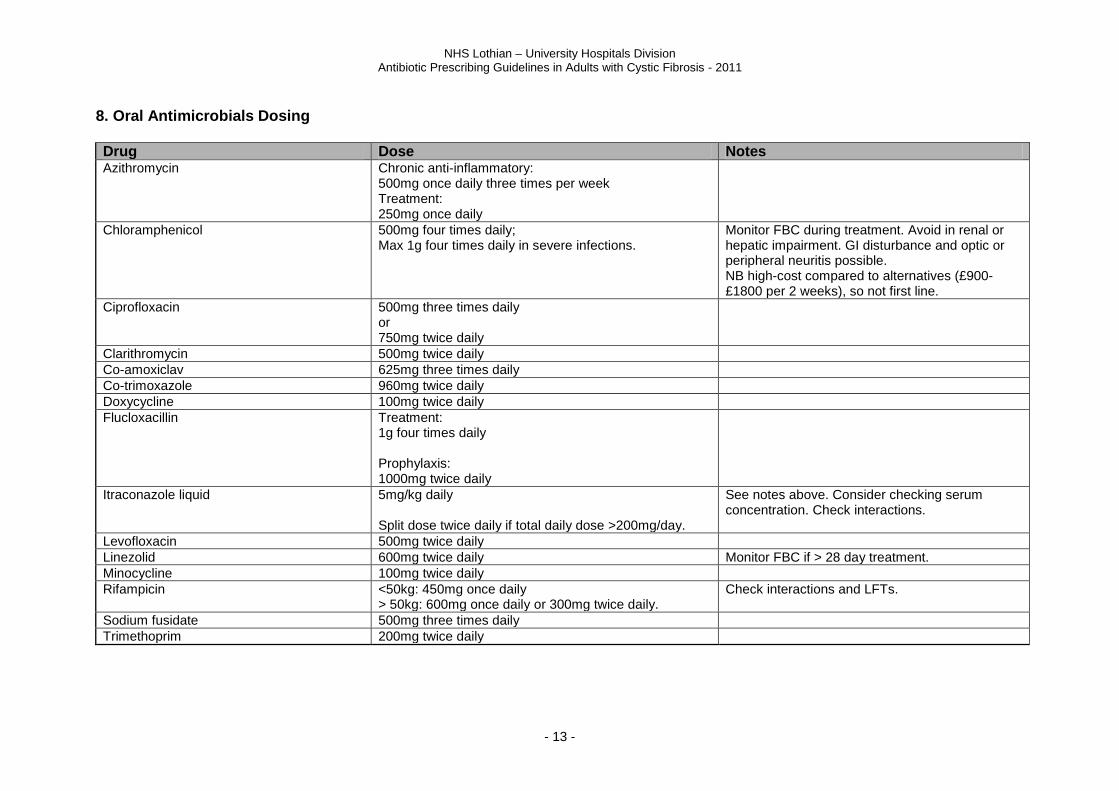
8. Oral Antimicrobials Dosing Drug Dose Notes Azithromycin Chronic anti-inflammatory:
500mg once daily three times per week Treatment: 250mg once daily
Chloramphenicol 500mg four times daily; Max 1g four times daily in severe infections.
Monitor FBC during treatment. Avoid in renal or hepatic impairment. GI disturbance and optic or peripheral neuritis possible. NB high-cost compared to alternatives (£900-£1800 per 2 weeks), so not first line.
Ciprofloxacin 500mg three times daily or 750mg twice daily
Clarithromycin 500mg twice daily
Co-amoxiclav 625mg three times daily
Co-trimoxazole 960mg twice daily
Doxycycline 100mg twice daily
Flucloxacillin Treatment: 1g four times daily Prophylaxis: 1000mg twice daily
Itraconazole liquid 5mg/kg daily Split dose twice daily if total daily dose >200mg/day.
See notes above. Consider checking serum concentration. Check interactions.
Levofloxacin 500mg twice daily
Linezolid 600mg twice daily Monitor FBC if > 28 day treatment.
Minocycline 100mg twice daily
Rifampicin <50kg: 450mg once daily > 50kg: 600mg once daily or 300mg twice daily.
Check interactions and LFTs.
Sodium fusidate 500mg three times daily
Trimethoprim 200mg twice daily
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 14 -
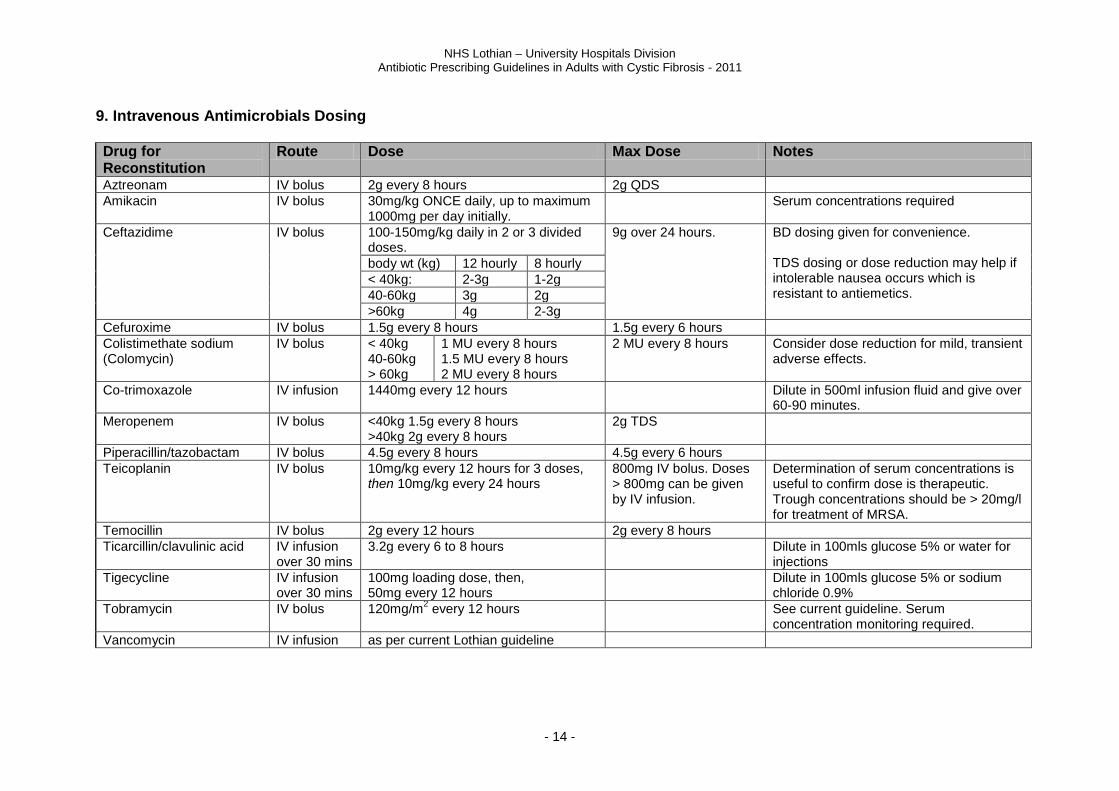
9. Intravenous Antimicrobials Dosing Drug for Reconstitution
Route Dose Max Dose Notes
Aztreonam IV bolus 2g every 8 hours 2g QDS
Amikacin IV bolus 30mg/kg ONCE daily, up to maximum 1000mg per day initially.
Serum concentrations required
Ceftazidime IV bolus 100-150mg/kg daily in 2 or 3 divided doses.
9g over 24 hours. BD dosing given for convenience. TDS dosing or dose reduction may help if intolerable nausea occurs which is resistant to antiemetics.
body wt (kg) 12 hourly 8 hourly
< 40kg: 2-3g 1-2g
40-60kg 3g 2g
>60kg 4g 2-3g
Cefuroxime IV bolus 1.5g every 8 hours 1.5g every 6 hours
Colistimethate sodium (Colomycin)
IV bolus < 40kg 40-60kg > 60kg
1 MU every 8 hours 1.5 MU every 8 hours 2 MU every 8 hours
2 MU every 8 hours Consider dose reduction for mild, transient adverse effects.
Co-trimoxazole IV infusion 1440mg every 12 hours Dilute in 500ml infusion fluid and give over 60-90 minutes.
Meropenem
IV bolus
<40kg 1.5g every 8 hours >40kg 2g every 8 hours
2g TDS
Piperacillin/tazobactam IV bolus 4.5g every 8 hours 4.5g every 6 hours
Teicoplanin IV bolus 10mg/kg every 12 hours for 3 doses, then 10mg/kg every 24 hours
800mg IV bolus. Doses > 800mg can be given by IV infusion.
Determination of serum concentrations is useful to confirm dose is therapeutic. Trough concentrations should be > 20mg/l for treatment of MRSA.
Temocillin IV bolus 2g every 12 hours 2g every 8 hours
Ticarcillin/clavulinic acid IV infusion over 30 mins
3.2g every 6 to 8 hours Dilute in 100mls glucose 5% or water for injections
Tigecycline IV infusion over 30 mins
100mg loading dose, then, 50mg every 12 hours
Dilute in 100mls glucose 5% or sodium chloride 0.9%
Tobramycin IV bolus 120mg/m2 every 12 hours See current guideline. Serum
concentration monitoring required.
Vancomycin IV infusion as per current Lothian guideline
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 15 -
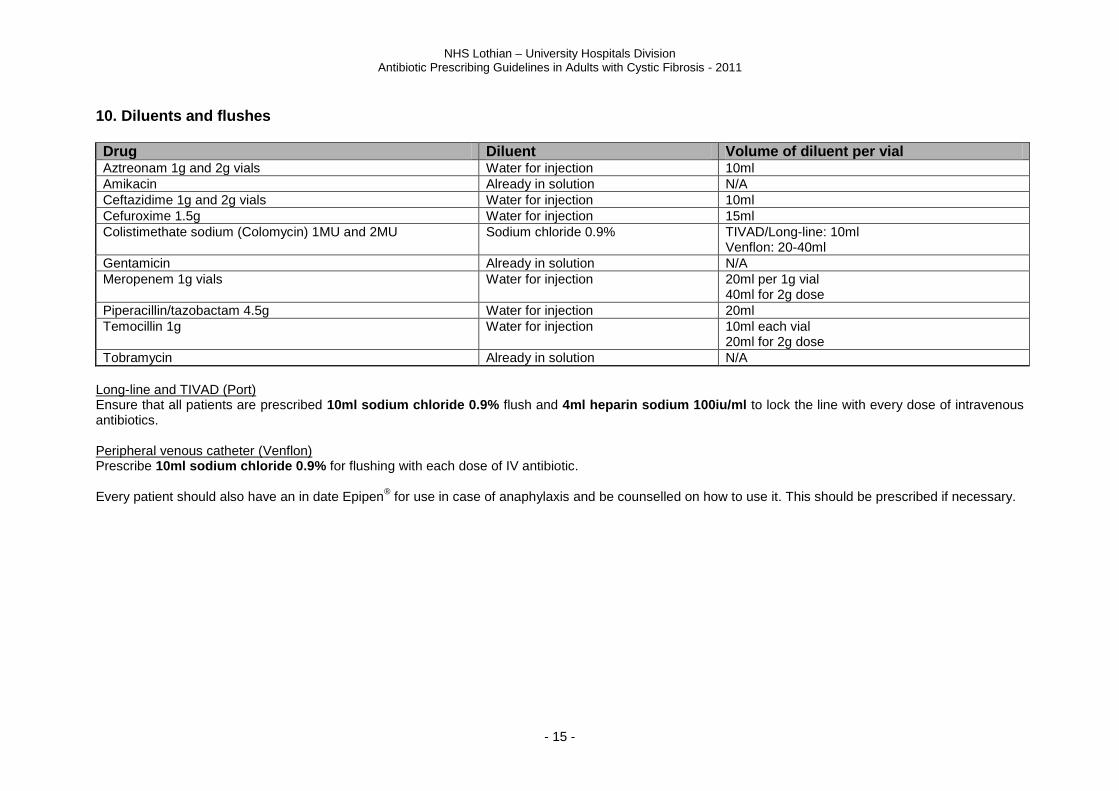
10. Diluents and flushes Drug Diluent Volume of diluent per vial Aztreonam 1g and 2g vials Water for injection 10ml
Amikacin Already in solution N/A
Ceftazidime 1g and 2g vials Water for injection 10ml
Cefuroxime 1.5g Water for injection 15ml
Colistimethate sodium (Colomycin) 1MU and 2MU Sodium chloride 0.9% TIVAD/Long-line: 10ml Venflon: 20-40ml
Gentamicin Already in solution N/A
Meropenem 1g vials
Water for injection 20ml per 1g vial 40ml for 2g dose
Piperacillin/tazobactam 4.5g Water for injection 20ml
Temocillin 1g
Water for injection 10ml each vial 20ml for 2g dose
Tobramycin Already in solution N/A
Long-line and TIVAD (Port) Ensure that all patients are prescribed 10ml sodium chloride 0.9% flush and 4ml heparin sodium 100iu/ml to lock the line with every dose of intravenous antibiotics. Peripheral venous catheter (Venflon) Prescribe 10ml sodium chloride 0.9% for flushing with each dose of IV antibiotic. Every patient should also have an in date Epipen
® for use in case of anaphylaxis and be counselled on how to use it. This should be prescribed if necessary.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 16 -
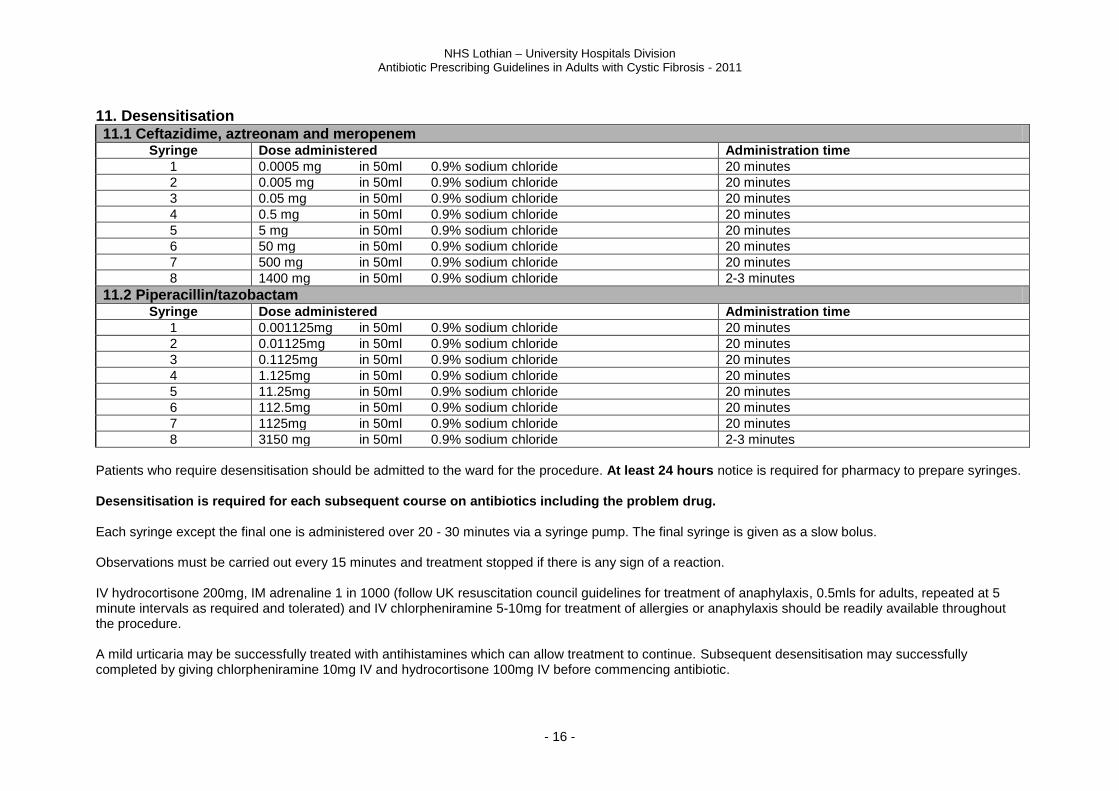
11. Desensitisation 11.1 Ceftazidime, aztreonam and meropenem
Syringe Dose administered Administration time
1 0.0005 mg in 50ml 0.9% sodium chloride 20 minutes
2 0.005 mg in 50ml 0.9% sodium chloride 20 minutes
3 0.05 mg in 50ml 0.9% sodium chloride 20 minutes
4 0.5 mg in 50ml 0.9% sodium chloride 20 minutes
5 5 mg in 50ml 0.9% sodium chloride 20 minutes
6 50 mg in 50ml 0.9% sodium chloride 20 minutes
7 500 mg in 50ml 0.9% sodium chloride 20 minutes
8 1400 mg in 50ml 0.9% sodium chloride 2-3 minutes
11.2 Piperacillin/tazobactam Syringe Dose administered Administration time
1 0.001125mg in 50ml 0.9% sodium chloride 20 minutes
2 0.01125mg in 50ml 0.9% sodium chloride 20 minutes
3 0.1125mg in 50ml 0.9% sodium chloride 20 minutes
4 1.125mg in 50ml 0.9% sodium chloride 20 minutes
5 11.25mg in 50ml 0.9% sodium chloride 20 minutes
6 112.5mg in 50ml 0.9% sodium chloride 20 minutes
7 1125mg in 50ml 0.9% sodium chloride 20 minutes
8 3150 mg in 50ml 0.9% sodium chloride 2-3 minutes
Patients who require desensitisation should be admitted to the ward for the procedure. At least 24 hours notice is required for pharmacy to prepare syringes. Desensitisation is required for each subsequent course on antibiotics including the problem drug. Each syringe except the final one is administered over 20 - 30 minutes via a syringe pump. The final syringe is given as a slow bolus. Observations must be carried out every 15 minutes and treatment stopped if there is any sign of a reaction. IV hydrocortisone 200mg, IM adrenaline 1 in 1000 (follow UK resuscitation council guidelines for treatment of anaphylaxis, 0.5mls for adults, repeated at 5 minute intervals as required and tolerated) and IV chlorpheniramine 5-10mg for treatment of allergies or anaphylaxis should be readily available throughout the procedure. A mild urticaria may be successfully treated with antihistamines which can allow treatment to continue. Subsequent desensitisation may successfully completed by giving chlorpheniramine 10mg IV and hydrocortisone 100mg IV before commencing antibiotic.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 17 -
Desensitisation should not be attempted if the history indicates a severe non-IgE-mediated reaction such as Stevens-Johnson syndrome, toxic epidermal necrolysis, hepatitis or haemolytic anaemia. If desensitisation is successful, the antibiotics should be continued at full dose. Allergic reactions are still possible up to the FOURTH dose. The patient should be warned to report any signs of a reaction immediately. Continued treatment is required to ensure desensitisation. If more than three consecutive doses in a course are missed, desensitisation must be repeated. References:
1. Khan D and Solensky R. Drug Allergy. J Allergy Clin Immunol 2010;125:S126-37. 2. Burrows J, Toon M, Bell S. Antibiotic desnsitization in adults with cystic fibrosis. Respirology 2003;8:359-364. 3. Moss R, Babin S, Hsu Y et al. Allergy to semisynthetic penicillins in cystic fibrosis. The Journal of Pediatrics 1984;104:460-466. 4. Ghosal S and Taylor C. Intravenous desensitization to ceftazidime in cystic fibrosis patients. J Antimicrob Chemotherapy 1997;39:556-557. 5. Wilson D, Owens R, Zuckerman J. Successful meropenem desensitization in a patient with cystic fibrosis. Ann Pharmacother 2003;37:1424-8. 6. Parmar J, Nasser S. Antibiotic allergy in cystic fibrosis. Thorax 2005;60:517-520.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 18 -
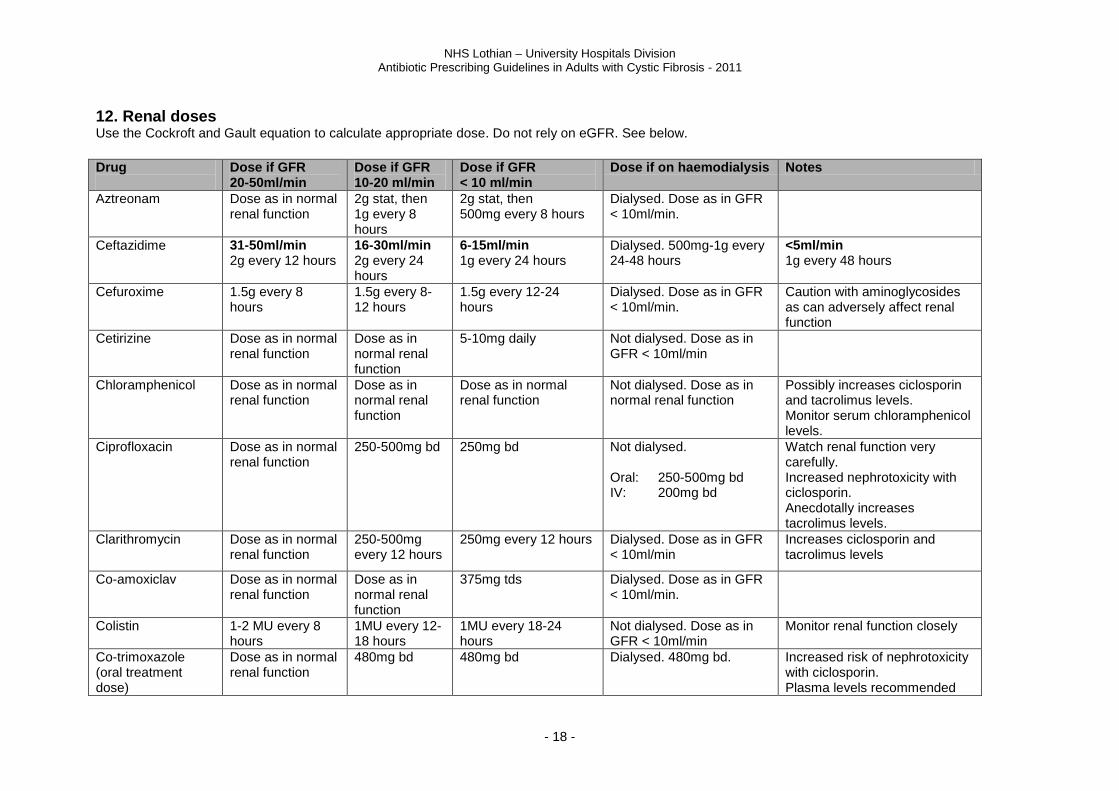
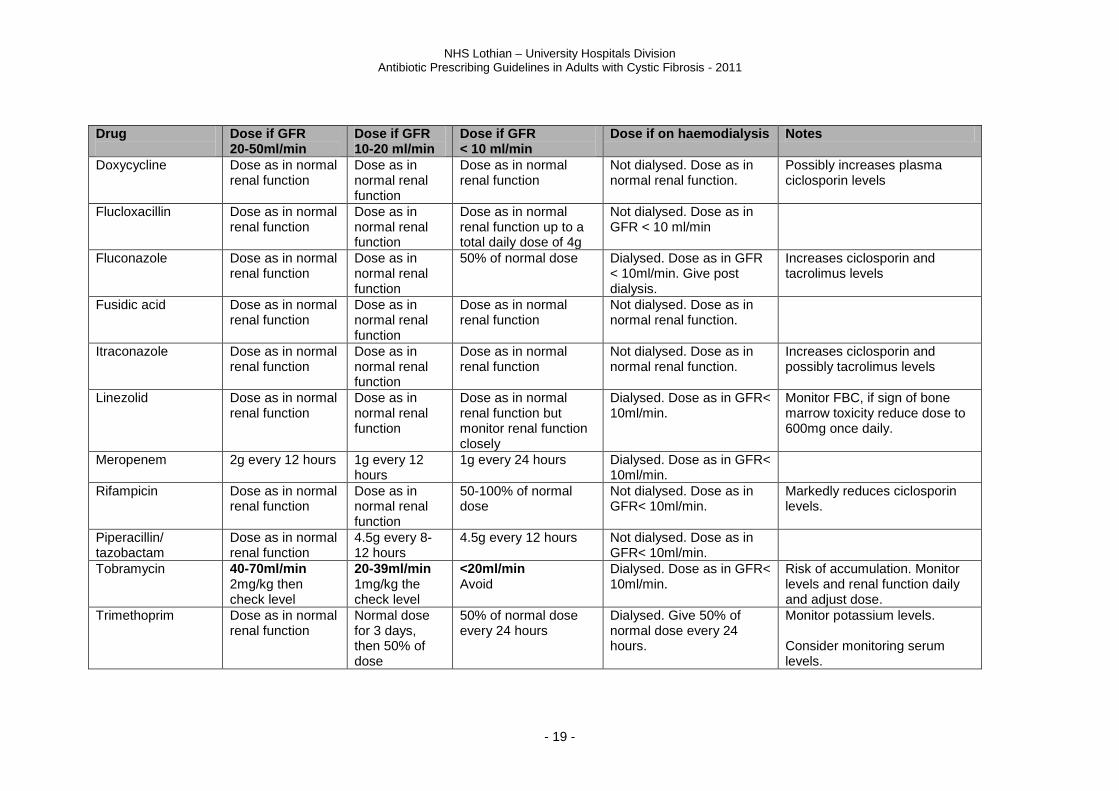
12. Renal doses
Use the Cockroft and Gault equation to calculate appropriate dose. Do not rely on eGFR. See below.
Drug
Dose if GFR 20-50ml/min
Dose if GFR 10-20 ml/min
Dose if GFR < 10 ml/min
Dose if on haemodialysis Notes
Aztreonam Dose as in normal renal function
2g stat, then 1g every 8 hours
2g stat, then 500mg every 8 hours
Dialysed. Dose as in GFR < 10ml/min.
Ceftazidime 31-50ml/min 2g every 12 hours
16-30ml/min 2g every 24 hours
6-15ml/min 1g every 24 hours
Dialysed. 500mg-1g every 24-48 hours
<5ml/min 1g every 48 hours
Cefuroxime 1.5g every 8 hours
1.5g every 8-12 hours
1.5g every 12-24 hours
Dialysed. Dose as in GFR < 10ml/min.
Caution with aminoglycosides as can adversely affect renal function
Cetirizine Dose as in normal renal function
Dose as in normal renal function
5-10mg daily Not dialysed. Dose as in GFR < 10ml/min
Chloramphenicol Dose as in normal renal function
Dose as in normal renal function
Dose as in normal renal function
Not dialysed. Dose as in normal renal function
Possibly increases ciclosporin and tacrolimus levels. Monitor serum chloramphenicol levels.
Ciprofloxacin Dose as in normal renal function
250-500mg bd 250mg bd Not dialysed. Oral: 250-500mg bd IV: 200mg bd
Watch renal function very carefully. Increased nephrotoxicity with ciclosporin. Anecdotally increases tacrolimus levels.
Clarithromycin Dose as in normal renal function
250-500mg every 12 hours
250mg every 12 hours Dialysed. Dose as in GFR < 10ml/min
Increases ciclosporin and tacrolimus levels
Co-amoxiclav Dose as in normal renal function
Dose as in normal renal function
375mg tds Dialysed. Dose as in GFR < 10ml/min.
Colistin
1-2 MU every 8 hours
1MU every 12-18 hours
1MU every 18-24 hours
Not dialysed. Dose as in GFR < 10ml/min
Monitor renal function closely
Co-trimoxazole (oral treatment dose)
Dose as in normal renal function
480mg bd 480mg bd Dialysed. 480mg bd. Increased risk of nephrotoxicity with ciclosporin. Plasma levels recommended
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 19 -
Drug
Dose if GFR 20-50ml/min
Dose if GFR 10-20 ml/min
Dose if GFR < 10 ml/min
Dose if on haemodialysis Notes
Doxycycline Dose as in normal renal function
Dose as in normal renal function
Dose as in normal renal function
Not dialysed. Dose as in normal renal function.
Possibly increases plasma ciclosporin levels
Flucloxacillin Dose as in normal renal function
Dose as in normal renal function
Dose as in normal renal function up to a total daily dose of 4g
Not dialysed. Dose as in GFR < 10 ml/min
Fluconazole Dose as in normal renal function
Dose as in normal renal function
50% of normal dose Dialysed. Dose as in GFR < 10ml/min. Give post dialysis.
Increases ciclosporin and tacrolimus levels
Fusidic acid Dose as in normal renal function
Dose as in normal renal function
Dose as in normal renal function
Not dialysed. Dose as in normal renal function.
Itraconazole Dose as in normal renal function
Dose as in normal renal function
Dose as in normal renal function
Not dialysed. Dose as in normal renal function.
Increases ciclosporin and possibly tacrolimus levels
Linezolid Dose as in normal renal function
Dose as in normal renal function
Dose as in normal renal function but monitor renal function closely
Dialysed. Dose as in GFR< 10ml/min.
Monitor FBC, if sign of bone marrow toxicity reduce dose to 600mg once daily.
Meropenem 2g every 12 hours 1g every 12 hours
1g every 24 hours Dialysed. Dose as in GFR< 10ml/min.
Rifampicin Dose as in normal renal function
Dose as in normal renal function
50-100% of normal dose
Not dialysed. Dose as in GFR< 10ml/min.
Markedly reduces ciclosporin levels.
Piperacillin/ tazobactam
Dose as in normal renal function
4.5g every 8-12 hours
4.5g every 12 hours Not dialysed. Dose as in GFR< 10ml/min.
Tobramycin 40-70ml/min 2mg/kg then check level
20-39ml/min 1mg/kg the check level
<20ml/min Avoid
Dialysed. Dose as in GFR< 10ml/min.
Risk of accumulation. Monitor levels and renal function daily and adjust dose.
Trimethoprim Dose as in normal renal function
Normal dose for 3 days, then 50% of dose
50% of normal dose every 24 hours
Dialysed. Give 50% of normal dose every 24 hours.
Monitor potassium levels. Consider monitoring serum levels.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 20 -
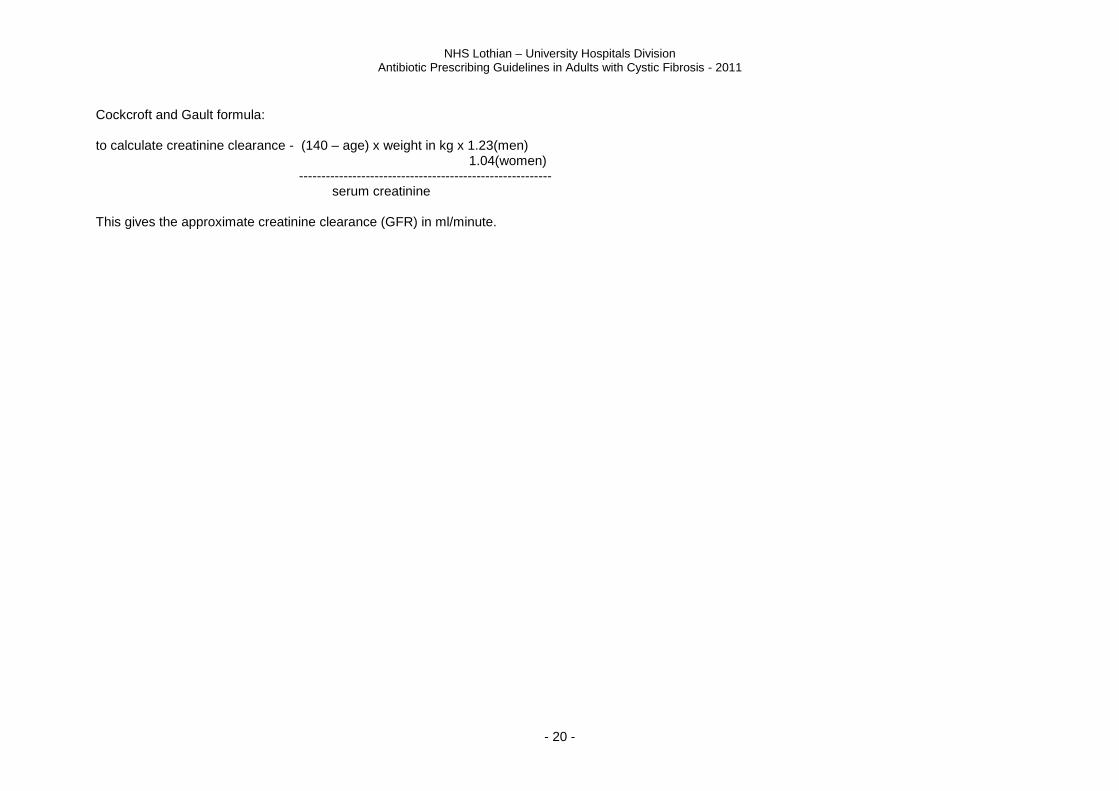
Cockcroft and Gault formula: to calculate creatinine clearance - (140 – age) x weight in kg x 1.23(men) 1.04(women) --------------------------------------------------------- serum creatinine This gives the approximate creatinine clearance (GFR) in ml/minute.
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 21 -
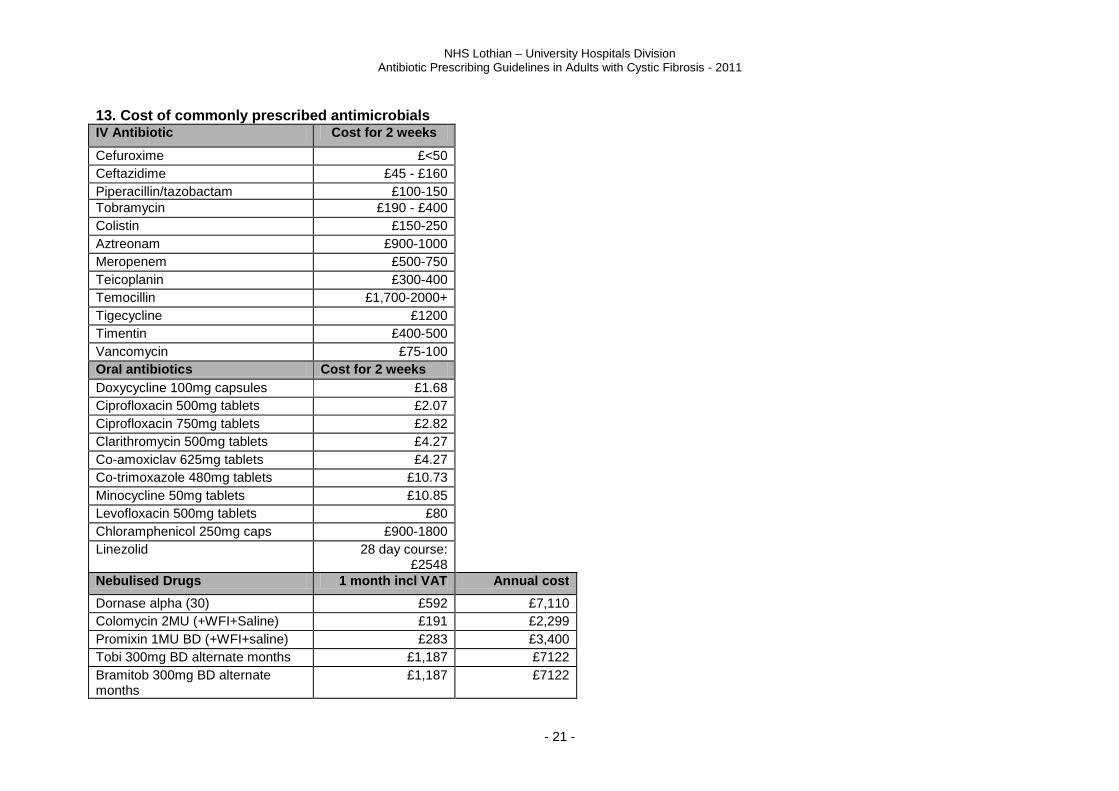
13. Cost of commonly prescribed antimicrobials IV Antibiotic Cost for 2 weeks
Cefuroxime £<50
Ceftazidime £45 - £160
Piperacillin/tazobactam £100-150
Tobramycin £190 - £400
Colistin £150-250
Aztreonam £900-1000
Meropenem £500-750
Teicoplanin £300-400
Temocillin £1,700-2000+
Tigecycline £1200
Timentin £400-500
Vancomycin £75-100
Oral antibiotics Cost for 2 weeks
Doxycycline 100mg capsules £1.68
Ciprofloxacin 500mg tablets £2.07
Ciprofloxacin 750mg tablets £2.82
Clarithromycin 500mg tablets £4.27
Co-amoxiclav 625mg tablets £4.27
Co-trimoxazole 480mg tablets £10.73
Minocycline 50mg tablets £10.85
Levofloxacin 500mg tablets £80
Chloramphenicol 250mg caps £900-1800
Linezolid 28 day course: £2548
Nebulised Drugs 1 month incl VAT Annual cost
Dornase alpha (30) £592 £7,110
Colomycin 2MU (+WFI+Saline) £191 £2,299
Promixin 1MU BD (+WFI+saline) £283 £3,400
Tobi 300mg BD alternate months £1,187 £7122
Bramitob 300mg BD alternate months
£1,187 £7122
NHS Lothian – University Hospitals Division Antibiotic Prescribing Guidelines in Adults with Cystic Fibrosis - 2011
- 22 -
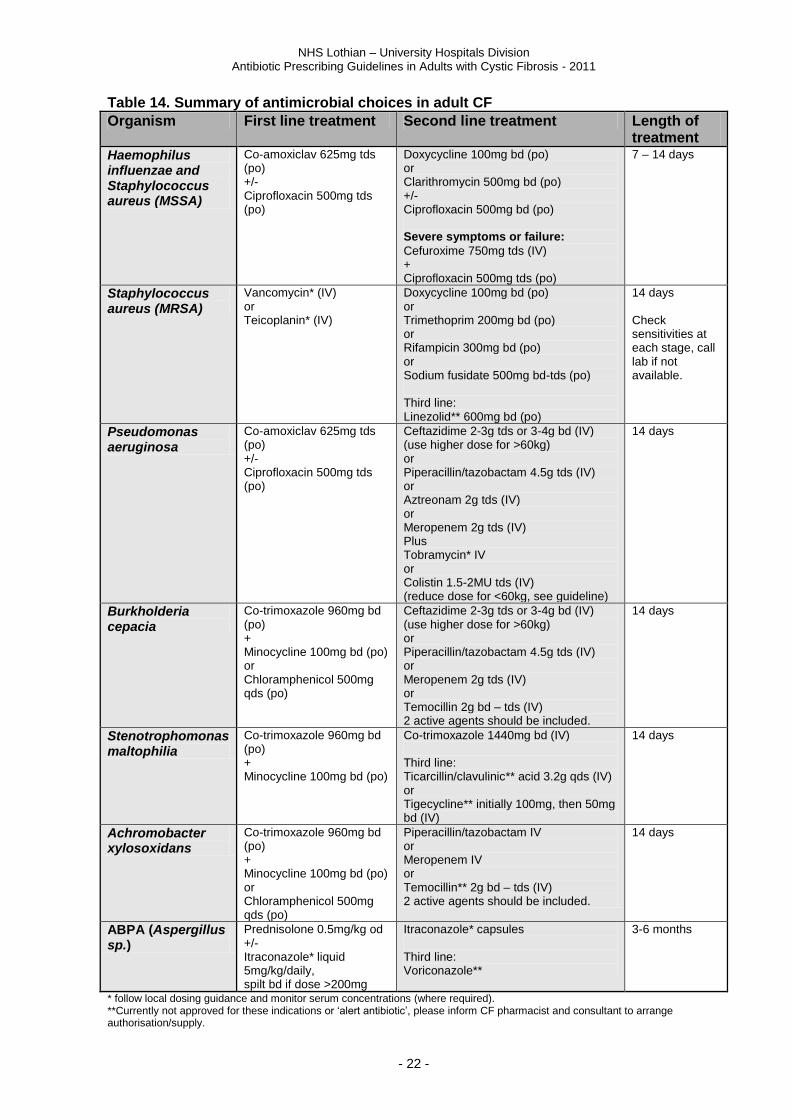
Table 14. Summary of antimicrobial choices in adult CF
Organism First line treatment Second line treatment Length of treatment
Haemophilus influenzae and Staphylococcus aureus (MSSA)
Co-amoxiclav 625mg tds (po) +/- Ciprofloxacin 500mg tds (po)
Doxycycline 100mg bd (po) or Clarithromycin 500mg bd (po) +/- Ciprofloxacin 500mg bd (po) Severe symptoms or failure:
Cefuroxime 750mg tds (IV) + Ciprofloxacin 500mg tds (po)
7 – 14 days
Staphylococcus aureus (MRSA)
Vancomycin* (IV) or Teicoplanin* (IV)
Doxycycline 100mg bd (po) or Trimethoprim 200mg bd (po) or Rifampicin 300mg bd (po) or Sodium fusidate 500mg bd-tds (po) Third line: Linezolid** 600mg bd (po)
14 days Check sensitivities at each stage, call lab if not available.
Pseudomonas aeruginosa
Co-amoxiclav 625mg tds (po) +/- Ciprofloxacin 500mg tds (po)
Ceftazidime 2-3g tds or 3-4g bd (IV) (use higher dose for >60kg) or Piperacillin/tazobactam 4.5g tds (IV) or Aztreonam 2g tds (IV) or Meropenem 2g tds (IV) Plus Tobramycin* IV or Colistin 1.5-2MU tds (IV) (reduce dose for <60kg, see guideline)
14 days
Burkholderia cepacia
Co-trimoxazole 960mg bd (po) + Minocycline 100mg bd (po) or Chloramphenicol 500mg qds (po)
Ceftazidime 2-3g tds or 3-4g bd (IV) (use higher dose for >60kg) or Piperacillin/tazobactam 4.5g tds (IV) or Meropenem 2g tds (IV) or Temocillin 2g bd – tds (IV) 2 active agents should be included.
14 days
Stenotrophomonas maltophilia
Co-trimoxazole 960mg bd (po) + Minocycline 100mg bd (po)
Co-trimoxazole 1440mg bd (IV) Third line: Ticarcillin/clavulinic** acid 3.2g qds (IV) or Tigecycline** initially 100mg, then 50mg bd (IV)
14 days
Achromobacter xylosoxidans
Co-trimoxazole 960mg bd (po) + Minocycline 100mg bd (po) or Chloramphenicol 500mg qds (po)
Piperacillin/tazobactam IV or Meropenem IV or Temocillin** 2g bd – tds (IV) 2 active agents should be included.
14 days
ABPA (Aspergillus sp.)
Prednisolone 0.5mg/kg od +/- Itraconazole* liquid 5mg/kg/daily, spilt bd if dose >200mg
Itraconazole* capsules Third line: Voriconazole**
3-6 months
* follow local dosing guidance and monitor serum concentrations (where required). **Currently not approved for these indications or ‘alert antibiotic’, please inform CF pharmacist and consultant to arrange authorisation/supply.





























