Embed Size (px)
Citation preview
Scand J Infect Dis 18: 447-450, 1986
Antibiogram of Urinary Tract Isolates in Kuwait
INGEMAR HELIN and GEORGE E ARAJ From the Departments of Pediatrics and Microbiology, Kuwait University, Mubarak AI-Kabeer Hospital, Kuwait
1253 urinary tract isdates collected during 9 months (April - December 1984) were analysed by the agar diffusion method for sensitivity to 13 antimicrobial agents commonly used for the treatment of urinary tract infections in children and adults. We noticed an agitatingly high re- sistance of Escherichia coli to ampicillin, sulphonnmide and trimethoptindsulphamethox- mle and of Proteus spp. to ampidllin. As Kuwait is one of the countries where the total con- sumption of antibiotics is very high p8 compared to most of the western countries, we are in- dined to assume that this generous policy for the prescription of especially ampicillin and other broad spectrum antibiotics in uncomplicated infections has generated this serious con- sequence.
I . Helin, MD, PhD, Depamnent of Rdiatrics, Wculty of Medicine, Kuwait University, PO. Bar 24923, Kuwait-Ambian Curf
INTRODUCTION
To ensure an optimal treatment of urinary tract infections (UTI), the responsible organism must be completely eradicated. The use of susceptibility testing, employing a panel of anti- microbial agents against the organism has therefore become a standard part of practice. However, in the majority of cases with UTI, the choice of antibiotic must be made before the result of these tests is known. Consequently, the clinician will have to choose between a number of antimicrobials according to the mosf likely result of the sensitivity test. In many countries there is an extensive use of not only penicillin but also broad spectrum antibiotics for the treatment of common colds, unexplained fever and even gastroenteritis. This will in- evitably bring about a wide resistance among the bacteria in the gut flora, from which most of the UTI are known to originate.
This report summarizes the pattern of resistance to the most commonly used antimicro- bials for UTI in Kuwait over a period of 9 months in 1984. In this country a generous policy is adopted by physicians of different levels favouring the use of antibiotics in a wide variety of symptoms, not usually known to be caused by bacteria. Our report demonstrates the se- vere effects this policy may induce with regard to the treatment of UTI.
MATERIAL AND METHODS During the period April through December 1984, all urine cultures showing significant growth (316 bacteridml of urine) of one single strain or heavy mixed growth with one strain predominating, were re- viewed with regard to sensitivity pattern against a wide range of antimicrobial agents, including ampicil- lin, colistin, gentamicin, nalidixic acid, nitrofurantoin, oxolinic acid, sulphonamide, trimethoprim, trimethopridsulphamethoxazole, amikacin, cefuroxime, cephalothin and carbenicillin. The disc-agar- diffusion-method (2) was used and the results read as sensitive or resistant. The study was carried out at Mubarak Al-Kabeer University Hospital, a referral center for paediatric and adult nephrology and urology patients. The hospital statistics for 1984 shows 16 6% admissions, 78 501 outpatient visits and 15 120 casualty cases.
Antibiotic susceptibility testing technique. The antibiotic susceptibility testing of isolates was per- formed on diagnostic sensitivity agar (DST, lot CH 261, OXOID Lab., Basingstoke, UK). Standard strains of Escherichia coli (NCTC 10418) and Pseudomonas aeruginosa (NCTC 10662) were used as the comparative controls.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bri
tish
Col
umbi
a on
10/
29/1
4Fo
r pe
rson
al u
se o
nly.
448 1. Helin and G. E Araj Scand I Infect Dis 18 (1986)
RESULTS
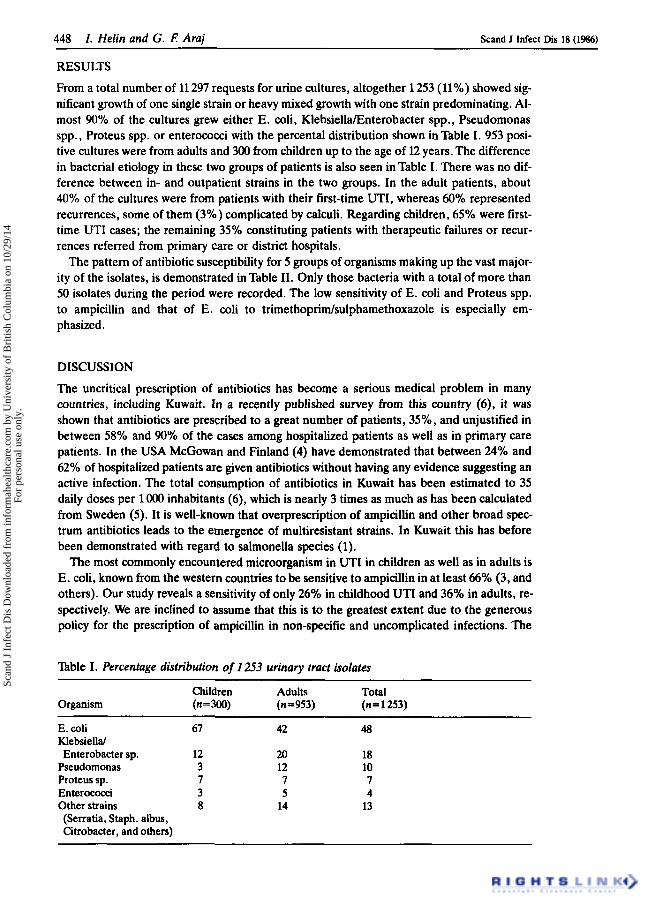
From a total number of 11 297 requests for urine cultures, altogether 1253 (11%) showed sig- nificant growth of one single strain or heavy mixed growth with one strain predominating. Al- most 90% of the cultures grew either E. coli, KlebsiellaEnterobacter spp., Pseudomonas spp., Proteus spp. or enterococci with the percental distribution shown in lhble I. 953 posi- tive cultures were from adults and 300 from children up to the age of 12 years. The difference in bacterial etiology in these two groups of patients is also seen in Table I. There was no dif- ference between in- and outpatient strains in the two groups. In the adult patients, about 40% of the cultures were from patients with their first-time UTI, whereas 60% represented recurrences, some of them (3%) complicated by calculi. Regarding children, 65% were first- time UTI cases; the remaining 35% constituting patients with therapeutic failures or recur- rences referred from primary care or district hospitals.
The pattern of antibiotic susceptibility for 5 groups of organisms making up the vast major- ity of the isolates, is demonstrated in Table 11. Only those bacteria with a total of more than 50 isolates during the period were recorded. The low sensitivity of E. coli and Proteus spp. to ampicillin and that of E. coli to trimethopridsulphamethoxazole is especially em- phasized.
DISCUSSION
The uncritical prescription of antibiotics has become a serious medical problem in many countries, including Kuwait. In a recently published survey from this country (6), it was shown that antibiotics are prescribed to a great number of patients, 35%, and unjustified in between 58% and 90% of the cases among hospitalized patients as well as in primary care patients. In the USA McGowan and Finland (4) have demonstrated that between 24% and 62% of hospitalized patients are given antibiotics without having any evidence suggesting an active infection. The total consumption of antibiotics in Kuwait has been estimated to 35 daily doses per 1 OOO inhabitants (6), which is nearly 3 times as much as has been calculated from Sweden ( 5 ) . It is well-known that overprescription of ampicillin and other broad spec- trum antibiotics leads to the emergence of multiresistant strains. In Kuwait this has before been demonstrated with regard to salmonella species (1).
The most commonly encountered microorganism in UTI in children as well as in adults is E. coli, known from the western countries to be sensitive to ampicillin in at least 66% (3, and others). Our study reveals a sensitivity of only 26% in childhood UTI and 36% in adults, re- spectively. We are inclined to assume that this is to the greatest extent due to the generous policy for the prescription of ampicillin in non-specific and uncomplicated infections. The
n b l e I. Percentage distribution of 1253 urinary tract isolates
Organism (n=300) (n = 953) (n=1253) Children Adults Total
E. coli 67 42 48 Klebsielld Enterobacter sp. 12 20 18
Pseudomonas 3 12 10 Proteus sp. 7 7 7 Enterococci 3 5 4 Other strains 8 14 13 (Serratia, Staph. albus, Citrobacter, and others)
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bri
tish
Col
umbi
a on
10/
29/1
4Fo
r pe
rson
al u
se o
nly.
Scand I Infect Dis 18 (1986) Urinary tract isolates in Kuwait 449
same is probably true also regarding our high frequency of resistance of E. coli to sulphon- amide and trimethoprim/sulphamethoxazole, as particularly the latter drug is also frequently used for medication in uncomplicated upper respiratory tract infections. I? mirabilis is usu- ally sensitive to ampicillin in more than 80% of the isolates. In our study, all proteus species were put together as it was not regularly reported from the laboratory which strain that was present. As I? mirabilis is the most commonly encountered strain of this group and also sen- sitive to ampicillin in more than 90% (3), it seems that with regard to this microorganism, the generous policy of antibiotic prescribing has caused a serious consequence. The same is prob- ably true concerning the high resistance of Proteus spp. to trirnethopridsulphamethoxazole.
A judicious treatment of UTI requires prior knowledge of antimicrobial sensitivity for the causative organism before prescribing an antimicrobial agent. As judged from our study, the treatment of acute lower uncomplicated UTI is easy to accomplish. Nitrofurantoin and nalidixic acid are both good alternatives when a high concentration of the drug is wanted in the urine. However, none of these substances gives a concentration within the renal par- enchyma that is considered sufficient to eradicate the bacteria involved in a complicated upper UTI, e.g. pyelonephritis. As seen from this study, only potent antibiotics with a bac- tericidal effect can make sure that the organism is eradicated early. These include colistin, gentamicin and amikacin, all known to be very effective against E. coli, KlebsiellaRntero- bacter, and, with regard to gentamicin and amikacin, also Proteus spp.
It is obvious to us that a generous policy in prescribing antibiotics for uncomplicated infec- tions leads to serious problems. One of the most harmful effects is demonstrated in this sur- vey: difficulties in choosing the most suitable antimicrobial agent for the treatment of acute pyelonephritis before the results of the sensitivity tests are known. While looking for specific antibiotics to use in UTI exclusively, we must recommend that all patients in whom an upper UTI cannot be excluded from clinical and biochemical findings must be hospitalized awaiting the result of the sensitivity pattern for the organism involved. This study thereby also de-
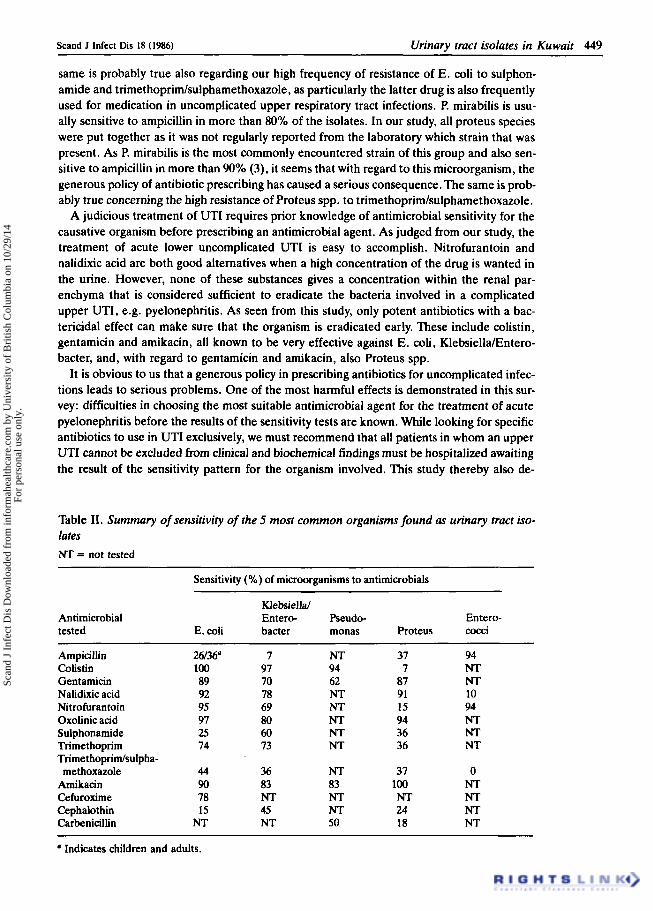
Table 11. Summary of sensitivity of the 5 most common organisms found as urinary tract iso- lates NT = not tested
Sensitivity (YO) of microorganisms to antimicrobials
Klebsiella/ Antimicrobial Entero- Pseudo- Entero- tested E. coli bacter monas Proteus cocci
Ampicillin 26/36' 7 NT 37 94 Colistin 100 97 94 7 NT Gentarnicin 89 70 62 87 NT Nalidixic acid 92 78 NT 91 10 Nitrofurantoin 95 69 NT 15 94 Oxolinic acid 97 80 NT 94 NT
Trirnethoprim 74 73 NT 36 NT Trirnethopridsulpha-
methoxazole 44 36 NT 37 0 Amikacin 90 83 83 100 NT Cefuroxime 78 NT NT NT NT Cephalothin 15 45 NT 24 NT Carbenicillin NT NT 50 18 NT
Sulphonamide 25 60 NT 36 NT
a Indicates children and adults.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bri
tish
Col
umbi
a on
10/
29/1
4Fo
r pe
rson
al u
se o
nly.

450 I . Helin and G. i! Araj Scand J Infect Dis 18 (1986)
monstrates another expensive consequence of unjustified antibiotic prescribing. There is an urgent need to solve this problem. Physicians must be educated on indications for antibiotic treatment. The population must be educated about the self-limiting course of the vast major- ity of upper respiratory tract infections (6). Furthermore, this report also emphasizes the im- portance of regularly monitoring the antibiogram for bacteria involved in infections where prescription of an antibiotic is justified.
REFERENCES
1. ChughTD, Suheir A. Drug resistance among salmonellae in Kuwait. Tkop Geogr Med 35: 37, 1983. 2. Ericsson H. The paper disc method for determination of bacterial sensitivity to antibiotics. Relation-
ship between the diameter of the zone of inhibition and the minimum inhibitory concentration. Scand J Clin Lab Invest 12: 408, 1960.
3. Fair WR, Fair WR 111. Clinical value of sensitivity determinations in treating urinary tract infections. Urology 19: 565, 1982.
4. McGowan JE Jr, Finland M. Infection and antibiotic usage at Boston City Hospital: Changes in pre- valence during the decade 19S1973. J Infect Dis 129: 421, 1974.
5. Nordic Council on Medicine. No 8, Stockholm 1980. 6. Thulesius 0, Mark A, Khalil S , Kollberg H, El-Hait SA, Kurian L. Patterns of antibiotic prescription
in Kuwait. J Kwt Med Assoc 18: 135, 1985.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bri
tish
Col
umbi
a on
10/
29/1
4Fo
r pe
rson
al u
se o
nly.