Embed Size (px)
Citation preview
Antiarrhythmics for Atrial Fibrillation: Practical Implications
of Latest Clinical Developments CME A. John Camm, MD; Stuart J. Connolly, MD; Jean-Yves F. Le Heuzey, MD
CME Released: 12/08/2011; Valid for credit through 12/08/2012
Download Slides
Updated atrial fibrillation guidelines issued by the European Society of Cardiology and in Canada in 2010
and the United States in 2011 may once again need revision, based on surprising results from the PALLAS
trial. Dronedarone was welcomed as a new alternative for patients with atrial fibrillation (AF) who also had
NYHA class I or II heart failure and coronary artery disease. It was also a consideration for patients with
most forms of AF (paroxysmal, persistent, or permanent); recommendations were based largely on the
ATHENA trial. New results from PALLAS looking at a different population of patients, primarily those with
varying degrees of heart failure and permanent AF, fared poorly. Drs Camm, Connolly, and Le Heuzey
review these perplexing results and outline which patients are and are not candidates for dronedarone
therapy.
Slide 1.
A. John Camm, MD: Hello. I'm John Camm from St. George's Hospital in London. I'm your moderator
today for this session, titled Antiarrhythmics for Atrial Fibrillation: Practical Implications of Latest Clinical
Trial Developments. I'm joined by Stuart Connolly from McMaster University in Hamilton, Ontario, Canada,
and Jean-Yves Le Heuzey from Hôpital Européen Georges-Pompidou in Paris. Well, gentlemen, we are
here at the American Heart Association meeting in Orlando, and we finally heard details of the PALLAS
study. Of course, we already knew some of the details, since the study was stopped early, and we learned
of the unfavorable trend of data which in Europe has already led to relabeling and new warnings for
patients with permanent atrial fibrillation (AF). So, let's start with reviewing the findings from PALLAS and
then discuss what these findings mean for our patients with AF, not only those with permanent AF but
those who may have paroxysmal or persistent AF and are currently doing well on antiarrhythmic therapy.
Stuart, tell us something of the PALLAS study results.
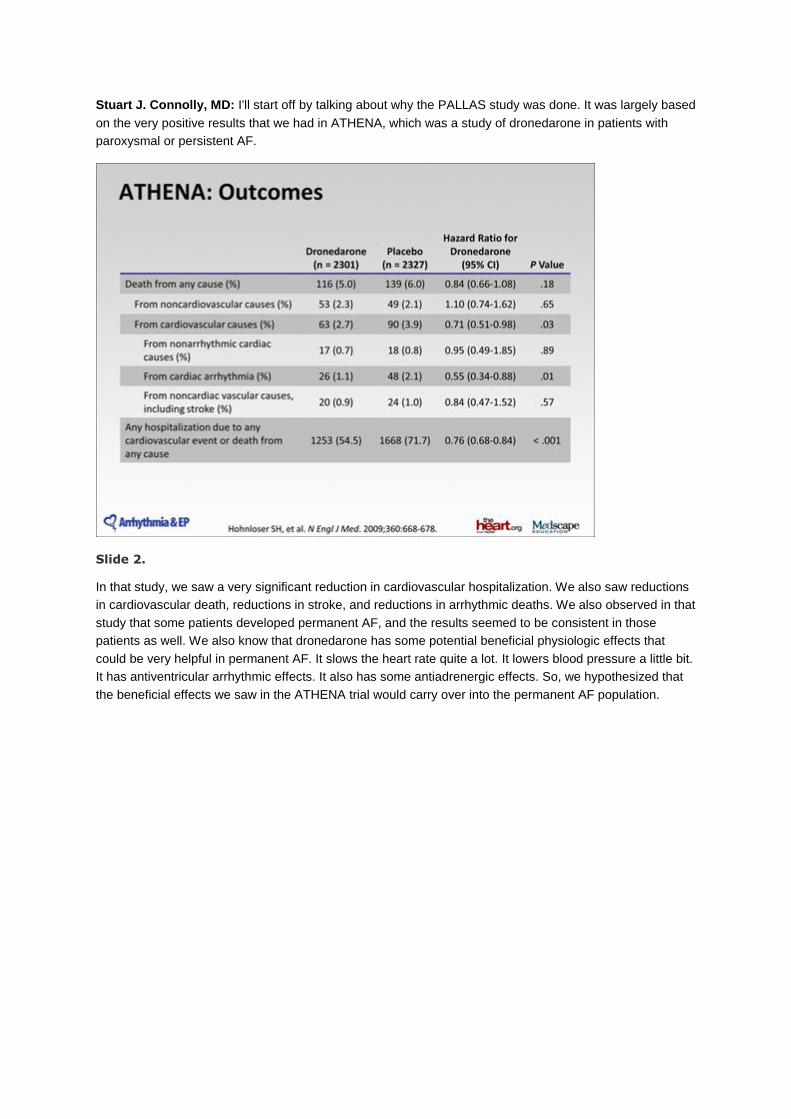
Stuart J. Connolly, MD: I'll start off by talking about why the PALLAS study was done. It was largely based
on the very positive results that we had in ATHENA, which was a study of dronedarone in patients with
paroxysmal or persistent AF.
Slide 2.
In that study, we saw a very significant reduction in cardiovascular hospitalization. We also saw reductions
in cardiovascular death, reductions in stroke, and reductions in arrhythmic deaths. We also observed in that
study that some patients developed permanent AF, and the results seemed to be consistent in those
patients as well. We also know that dronedarone has some potential beneficial physiologic effects that
could be very helpful in permanent AF. It slows the heart rate quite a lot. It lowers blood pressure a little bit.
It has antiventricular arrhythmic effects. It also has some antiadrenergic effects. So, we hypothesized that
the beneficial effects we saw in the ATHENA trial would carry over into the permanent AF population.
Slide 3.
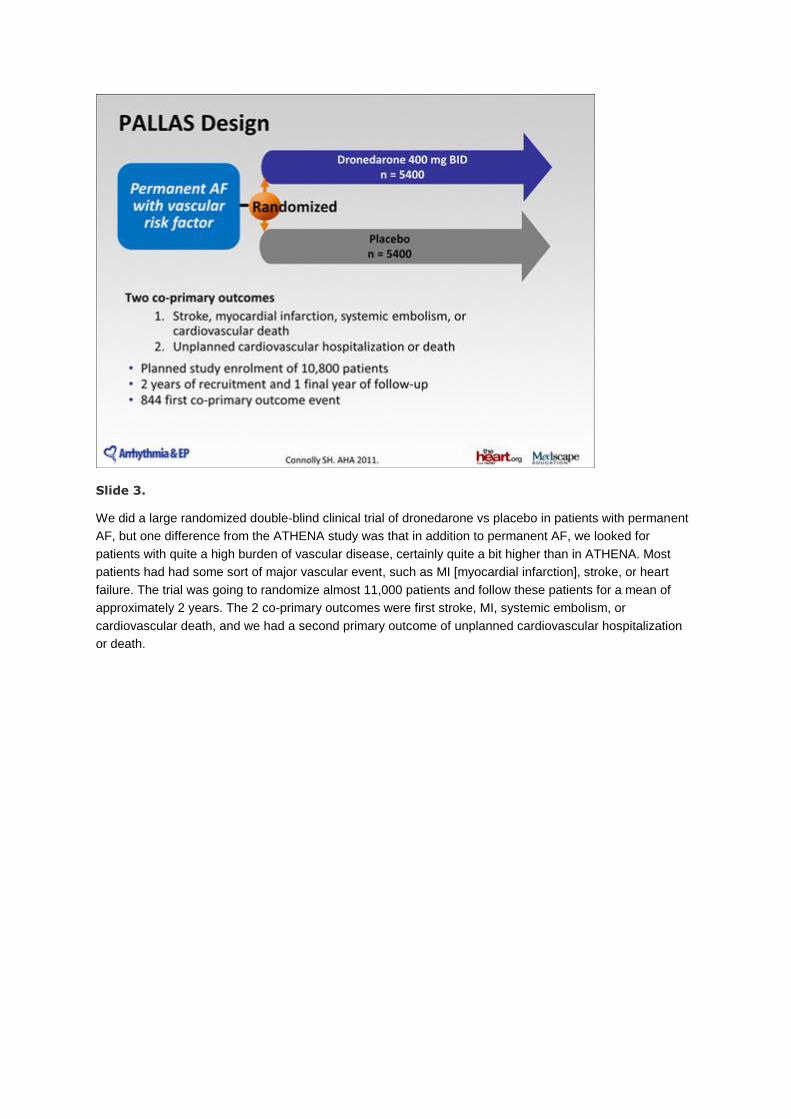
We did a large randomized double-blind clinical trial of dronedarone vs placebo in patients with permanent
AF, but one difference from the ATHENA study was that in addition to permanent AF, we looked for
patients with quite a high burden of vascular disease, certainly quite a bit higher than in ATHENA. Most
patients had had some sort of major vascular event, such as MI [myocardial infarction], stroke, or heart
failure. The trial was going to randomize almost 11,000 patients and follow these patients for a mean of
approximately 2 years. The 2 co-primary outcomes were first stroke, MI, systemic embolism, or
cardiovascular death, and we had a second primary outcome of unplanned cardiovascular hospitalization
or death.
Slide 4.
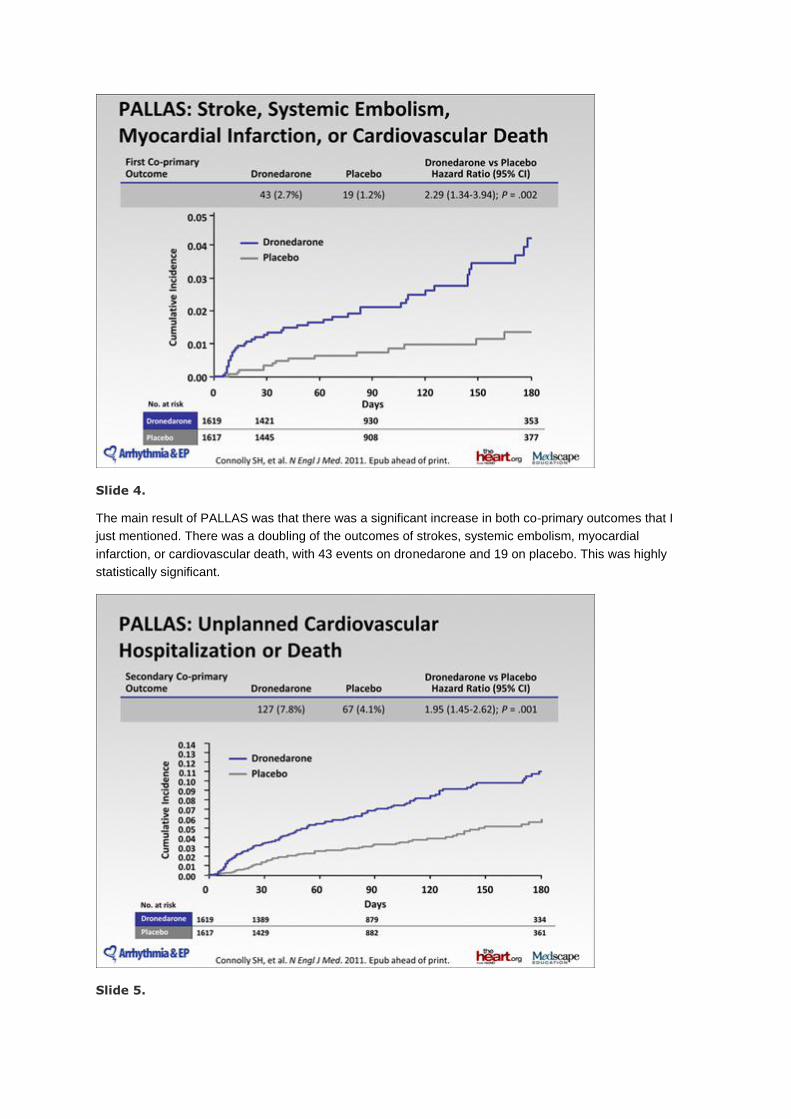
The main result of PALLAS was that there was a significant increase in both co-primary outcomes that I
just mentioned. There was a doubling of the outcomes of strokes, systemic embolism, myocardial
infarction, or cardiovascular death, with 43 events on dronedarone and 19 on placebo. This was highly
statistically significant.
Slide 5.
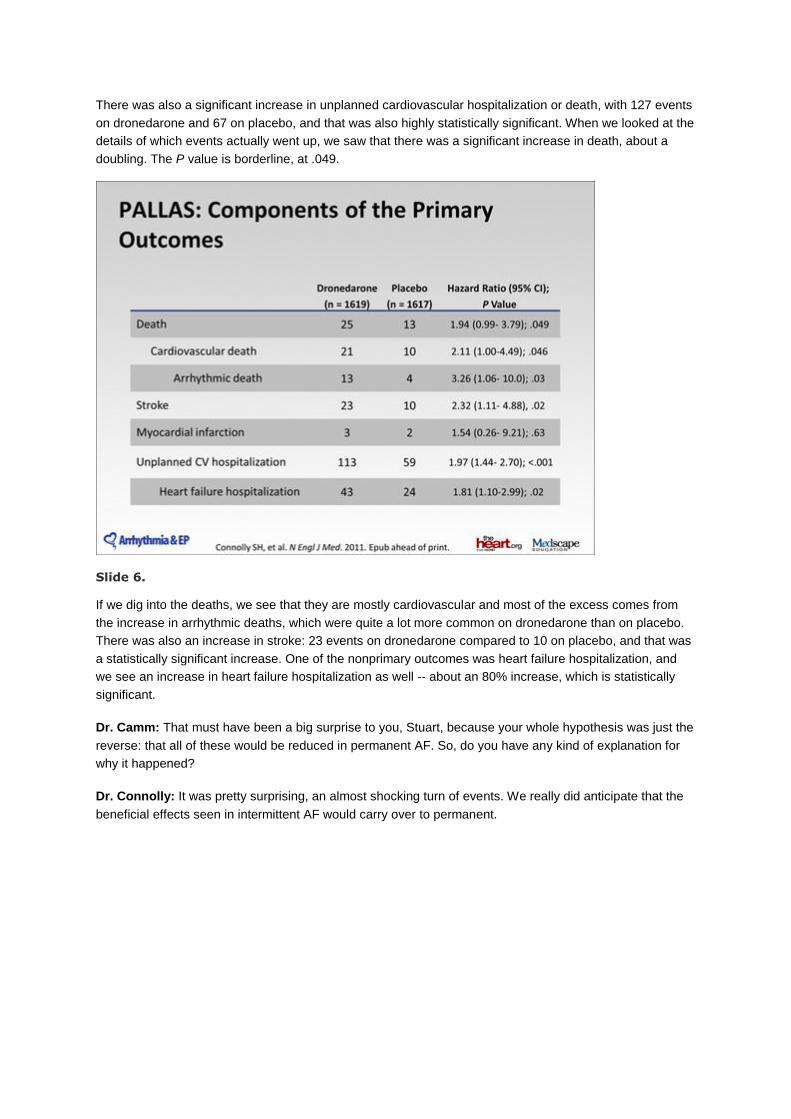
There was also a significant increase in unplanned cardiovascular hospitalization or death, with 127 events
on dronedarone and 67 on placebo, and that was also highly statistically significant. When we looked at the
details of which events actually went up, we saw that there was a significant increase in death, about a
doubling. The P value is borderline, at .049.
Slide 6.
If we dig into the deaths, we see that they are mostly cardiovascular and most of the excess comes from
the increase in arrhythmic deaths, which were quite a lot more common on dronedarone than on placebo.
There was also an increase in stroke: 23 events on dronedarone compared to 10 on placebo, and that was
a statistically significant increase. One of the nonprimary outcomes was heart failure hospitalization, and
we see an increase in heart failure hospitalization as well -- about an 80% increase, which is statistically
significant.
Dr. Camm: That must have been a big surprise to you, Stuart, because your whole hypothesis was just the
reverse: that all of these would be reduced in permanent AF. So, do you have any kind of explanation for
why it happened?
Dr. Connolly: It was pretty surprising, an almost shocking turn of events. We really did anticipate that the
beneficial effects seen in intermittent AF would carry over to permanent.
Slide 7.
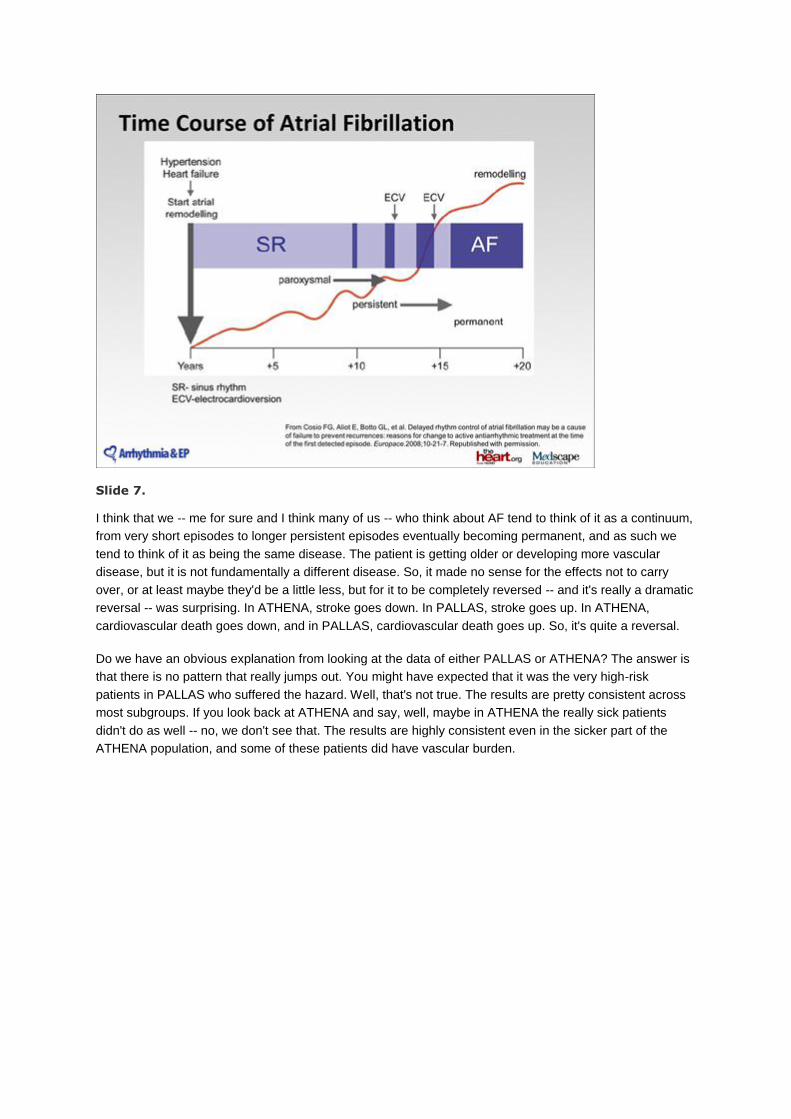
I think that we -- me for sure and I think many of us -- who think about AF tend to think of it as a continuum,
from very short episodes to longer persistent episodes eventually becoming permanent, and as such we
tend to think of it as being the same disease. The patient is getting older or developing more vascular
disease, but it is not fundamentally a different disease. So, it made no sense for the effects not to carry
over, or at least maybe they'd be a little less, but for it to be completely reversed -- and it's really a dramatic
reversal -- was surprising. In ATHENA, stroke goes down. In PALLAS, stroke goes up. In ATHENA,
cardiovascular death goes down, and in PALLAS, cardiovascular death goes up. So, it's quite a reversal.
Do we have an obvious explanation from looking at the data of either PALLAS or ATHENA? The answer is
that there is no pattern that really jumps out. You might have expected that it was the very high-risk
patients in PALLAS who suffered the hazard. Well, that's not true. The results are pretty consistent across
most subgroups. If you look back at ATHENA and say, well, maybe in ATHENA the really sick patients
didn't do as well -- no, we don't see that. The results are highly consistent even in the sicker part of the
ATHENA population, and some of these patients did have vascular burden.
Slide 8.
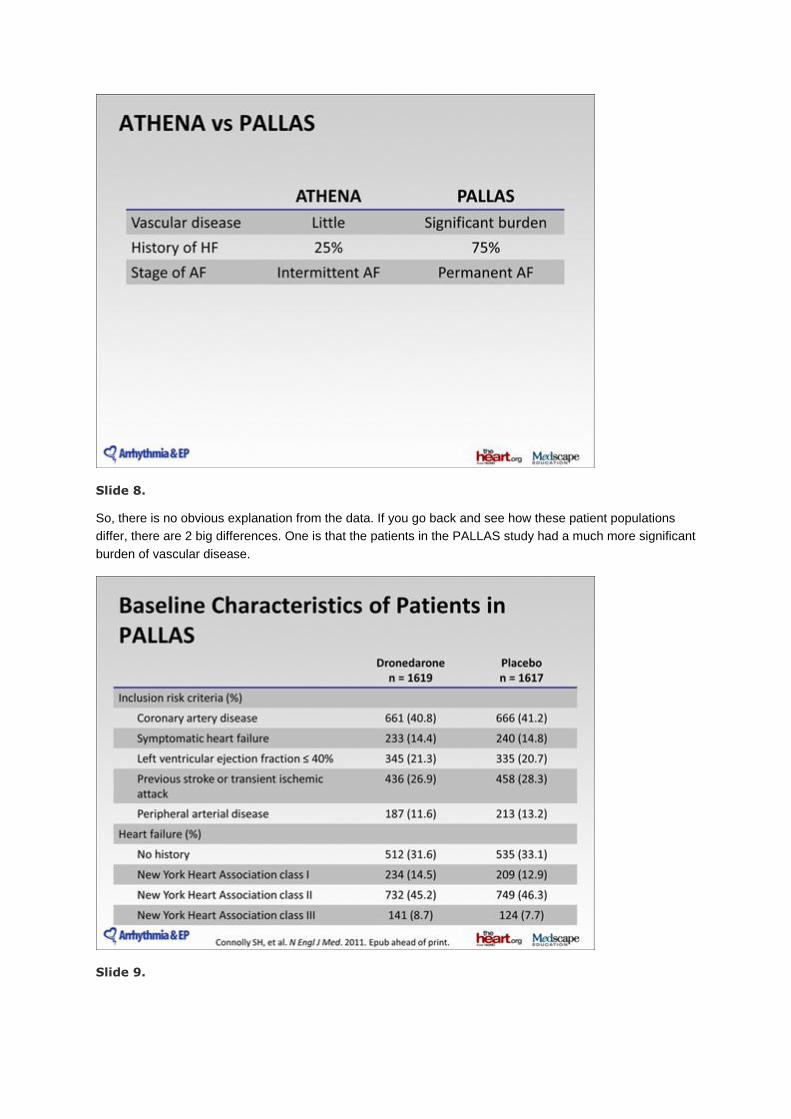
So, there is no obvious explanation from the data. If you go back and see how these patient populations
differ, there are 2 big differences. One is that the patients in the PALLAS study had a much more significant
burden of vascular disease.
Slide 9.
For example, about 75% of them had a history of heart failure in PALLAS, whereas in ATHENA only about
25%. Other risk factors are similarly different. The other big difference is the difference between intermittent
and permanent AF: All patients were intermittent going into the ATHENA study, and conversely, all patients
were permanent in PALLAS. That seems to be an important part of the explanation.
Dr. Camm: Of course, with the results of PALLAS, it's not surprising that the regulatory agencies are taking
a fresh look at the ways in which we should use dronedarone.
Slide 10.
We have already had some information from the European regulators, and as you might expect, we are no
longer to use dronedarone in patients who have permanent AF; they also identified heart failure as a
particular problem. Can you tell us a little bit about the result from PALLAS that stimulated the regulators to
identify heart failure?
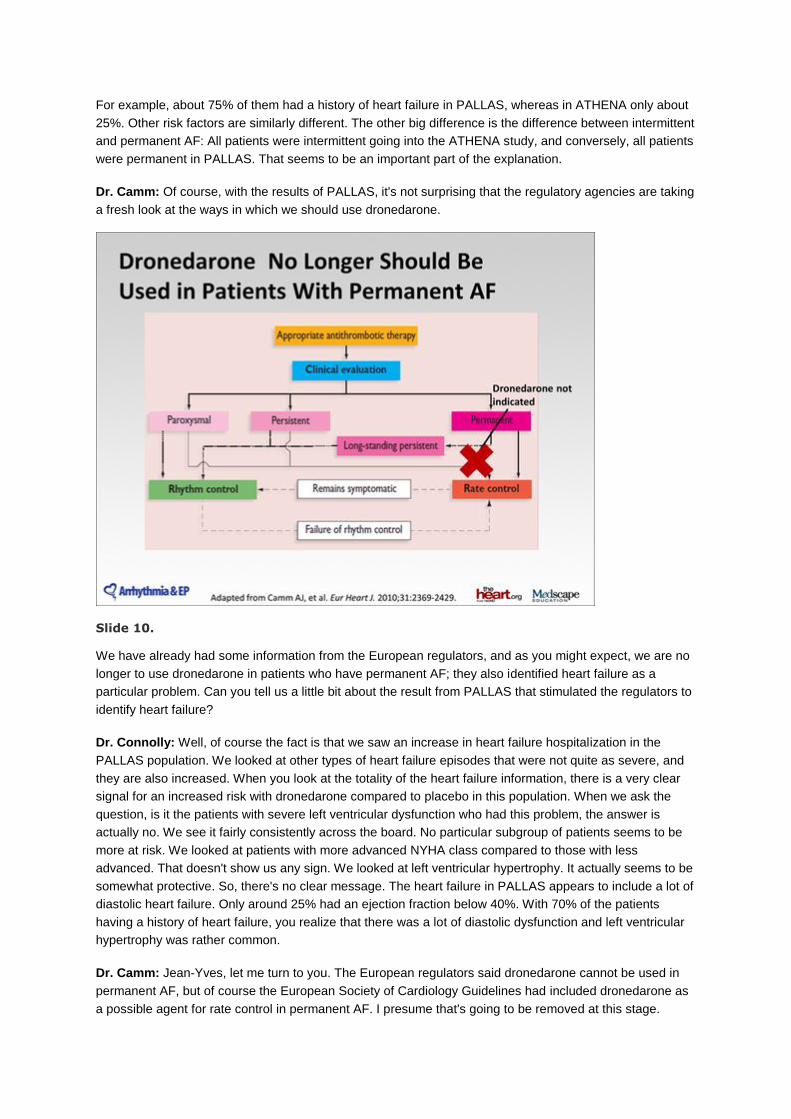
Dr. Connolly: Well, of course the fact is that we saw an increase in heart failure hospitalization in the
PALLAS population. We looked at other types of heart failure episodes that were not quite as severe, and
they are also increased. When you look at the totality of the heart failure information, there is a very clear
signal for an increased risk with dronedarone compared to placebo in this population. When we ask the
question, is it the patients with severe left ventricular dysfunction who had this problem, the answer is
actually no. We see it fairly consistently across the board. No particular subgroup of patients seems to be
more at risk. We looked at patients with more advanced NYHA class compared to those with less
advanced. That doesn't show us any sign. We looked at left ventricular hypertrophy. It actually seems to be
somewhat protective. So, there's no clear message. The heart failure in PALLAS appears to include a lot of
diastolic heart failure. Only around 25% had an ejection fraction below 40%. With 70% of the patients
having a history of heart failure, you realize that there was a lot of diastolic dysfunction and left ventricular
hypertrophy was rather common.
Dr. Camm: Jean-Yves, let me turn to you. The European regulators said dronedarone cannot be used in
permanent AF, but of course the European Society of Cardiology Guidelines had included dronedarone as
a possible agent for rate control in permanent AF. I presume that's going to be removed at this stage.
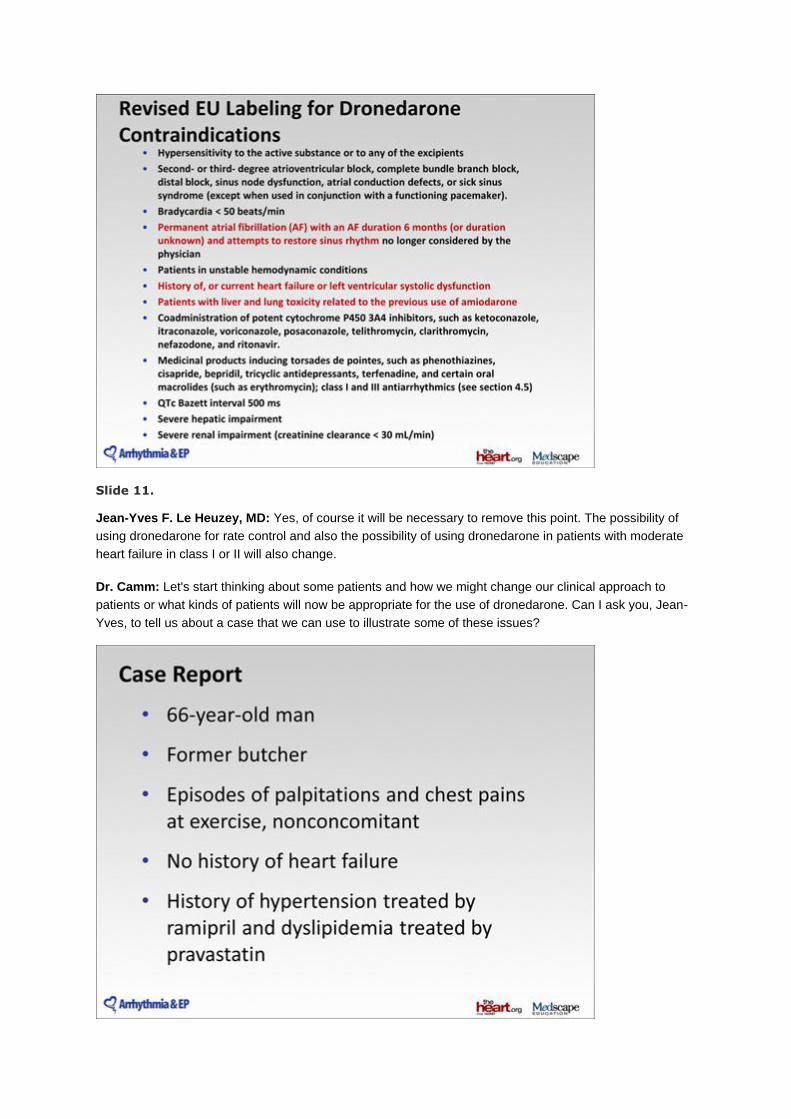
Slide 11.
Jean-Yves F. Le Heuzey, MD: Yes, of course it will be necessary to remove this point. The possibility of
using dronedarone for rate control and also the possibility of using dronedarone in patients with moderate
heart failure in class I or II will also change.
Dr. Camm: Let's start thinking about some patients and how we might change our clinical approach to
patients or what kinds of patients will now be appropriate for the use of dronedarone. Can I ask you, Jean-
Yves, to tell us about a case that we can use to illustrate some of these issues?
Slide 12.
Dr. Le Heuzey: I wanted to show you the story of one of my patients, who was a former butcher living in
Paris near the Eifel Tower. He was 66 years old when he came to see me for palpitations and chest pain at
exercise, but not concomitant; it was at different times. He had a history of hypertension treated by ramipril
and dyslipidemia treated by pravastatin. He has never had any episodes of heart failure.
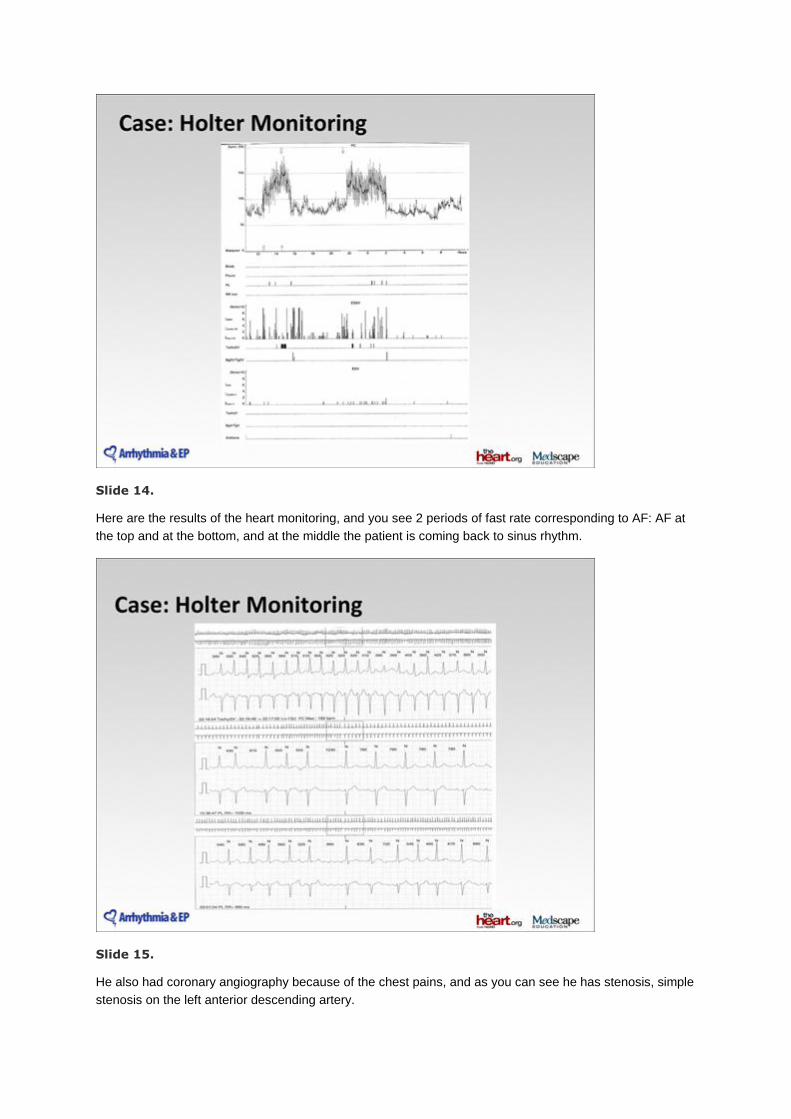
Slide 13.
When I saw him for the first time, as you can see from his ECG, he was in sinus rhythm and it showed a
normal ejection fraction. He had Holter heart monitoring.
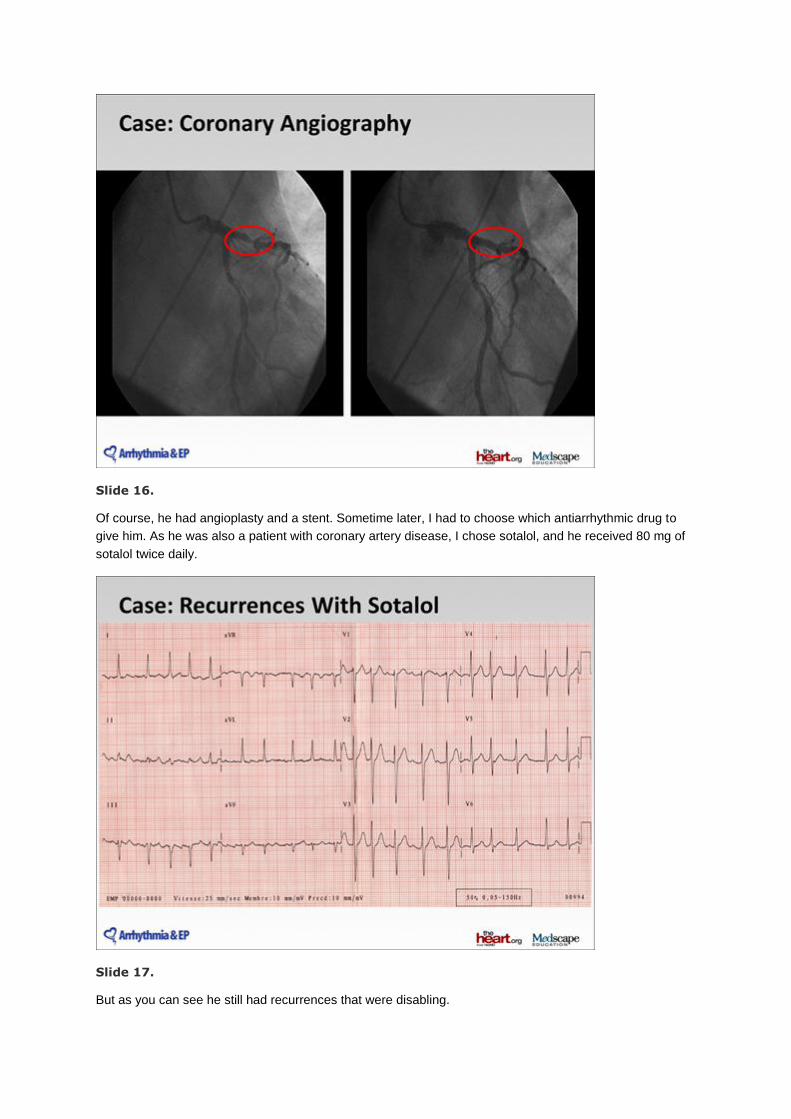
Slide 14.
Here are the results of the heart monitoring, and you see 2 periods of fast rate corresponding to AF: AF at
the top and at the bottom, and at the middle the patient is coming back to sinus rhythm.
Slide 15.
He also had coronary angiography because of the chest pains, and as you can see he has stenosis, simple
stenosis on the left anterior descending artery.
Slide 16.
Of course, he had angioplasty and a stent. Sometime later, I had to choose which antiarrhythmic drug to
give him. As he was also a patient with coronary artery disease, I chose sotalol, and he received 80 mg of
sotalol twice daily.
Slide 17.
But as you can see he still had recurrences that were disabling.
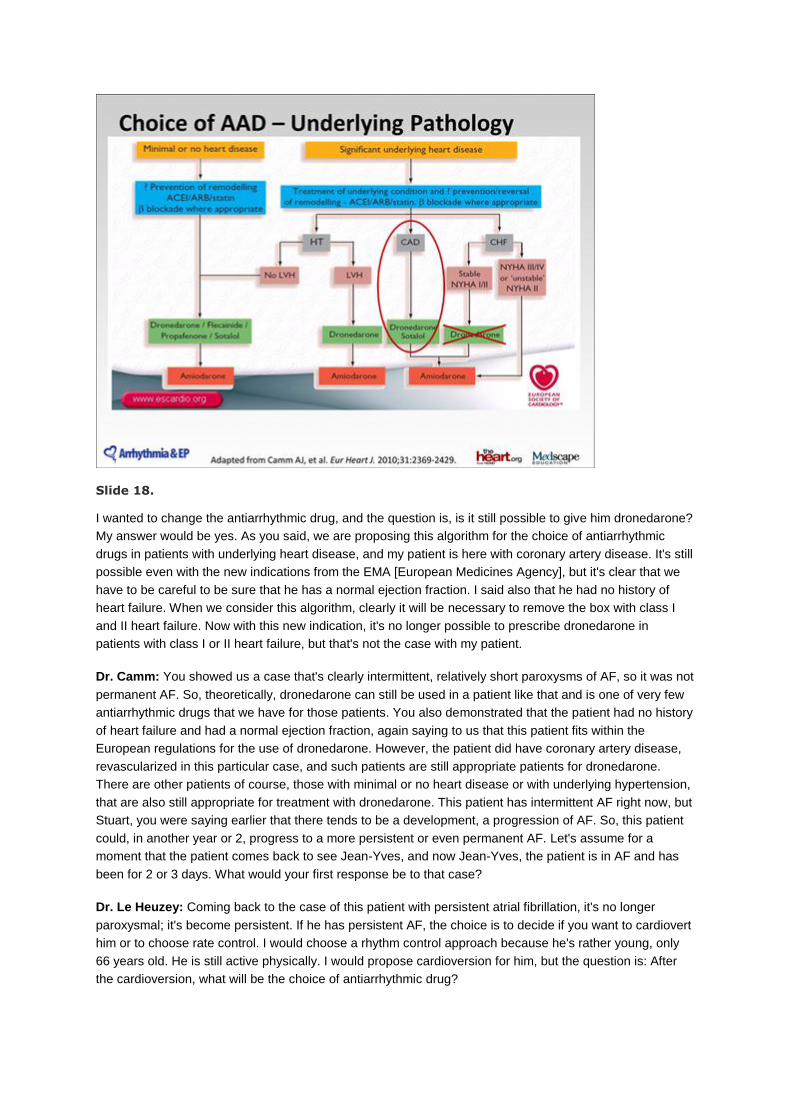
Slide 18.
I wanted to change the antiarrhythmic drug, and the question is, is it still possible to give him dronedarone?
My answer would be yes. As you said, we are proposing this algorithm for the choice of antiarrhythmic
drugs in patients with underlying heart disease, and my patient is here with coronary artery disease. It's still
possible even with the new indications from the EMA [European Medicines Agency], but it's clear that we
have to be careful to be sure that he has a normal ejection fraction. I said also that he had no history of
heart failure. When we consider this algorithm, clearly it will be necessary to remove the box with class I
and II heart failure. Now with this new indication, it's no longer possible to prescribe dronedarone in
patients with class I or II heart failure, but that's not the case with my patient.
Dr. Camm: You showed us a case that's clearly intermittent, relatively short paroxysms of AF, so it was not
permanent AF. So, theoretically, dronedarone can still be used in a patient like that and is one of very few
antiarrhythmic drugs that we have for those patients. You also demonstrated that the patient had no history
of heart failure and had a normal ejection fraction, again saying to us that this patient fits within the
European regulations for the use of dronedarone. However, the patient did have coronary artery disease,
revascularized in this particular case, and such patients are still appropriate patients for dronedarone.
There are other patients of course, those with minimal or no heart disease or with underlying hypertension,
that are also still appropriate for treatment with dronedarone. This patient has intermittent AF right now, but
Stuart, you were saying earlier that there tends to be a development, a progression of AF. So, this patient
could, in another year or 2, progress to a more persistent or even permanent AF. Let's assume for a
moment that the patient comes back to see Jean-Yves, and now Jean-Yves, the patient is in AF and has
been for 2 or 3 days. What would your first response be to that case?
Dr. Le Heuzey: Coming back to the case of this patient with persistent atrial fibrillation, it's no longer
paroxysmal; it's become persistent. If he has persistent AF, the choice is to decide if you want to cardiovert
him or to choose rate control. I would choose a rhythm control approach because he's rather young, only
66 years old. He is still active physically. I would propose cardioversion for him, but the question is: After
the cardioversion, what will be the choice of antiarrhythmic drug?
Slide 19.
If we think there is still a chance to maintain sinus rhythm, perhaps we can try another agent or give him
amiodarone, or if I want really to maintain sinus rhythm, there is also the possibility of ablation in this
patient.
Dr. Connolly: So, you're saying that if you plan to do a cardioversion, you wouldn't keep him on
dronedarone? It seems to me that if you're going to cardiovert this patient, it's reasonable to stay on
dronedarone and see if it controls him. Are you assuming that this is now a failure of dronedarone?
Dr. Le Heuzey: That is an important point. It is important to know the circumstances of the relapse to AF.
For example, if the patient has relapsed because of the flu or because of excessive alcohol consumption or
something like that, my view would be different. If there is absolutely no contributing factor, probably I will
change and discuss with him the choice between amiodarone and ablation.
Dr. Camm: I might take this patient who, let's say, tried dronedarone for 6 or 9 months and has had no
symptomatic recurrences and then suddenly has this recurrence, I might well think, let's cardiovert the
patient now and see if he maintains a sinus rhythm keeping him on dronedarone. That would not be an
unreasonable approach at this stage rather than changing to a new antiarrhythmic, but I agree that there
are differences of opinion on how such patients like this can be handled. Let's say this patient continues in
AF, but he's not very symptomatic. You see him now, a couple of months after going into AF. You know
that he went into AF because he did go and see a doctor and he was diagnosed, but nothing was done
about it. He's still on dronedarone. What would you do now, 2 months down the line?
Dr. Connolly: For me, the typical situation is the patient comes back for routine follow-up and says he's
feeling fine. I look at the ECG, and lo and behold, he's in AF with a controlled ventricular rate on his β-
blocker and dronedarone. We don't know how long he's been in AF, but one presumes it's probably been
for quite some time. The patient's AF has now become permanent, and it's not infrequent that these
patients become permanent on dronedarone and perhaps another rate-controlling drug and don't have
many symptoms (if any) -- or sometimes they'll say, I had palpitations a few weeks ago when I was
exercising or something. It's pretty minimal. In that situation, you need to ask, how much do we want to
maintain sinus rhythm, or do we want to go the cardioversion route or try another drug or ablation? Those
are all viable options, and a lot depends on the patient's own preferences as well. In many situations, I
would advise the patient to try rate control. In that situation, even though it may appear that dronedarone
has helped with the rate control in fact, it may be keeping this patient comfortable, I think we would
definitely want to stop dronedarone and see whether we could get by without it.
Dr. Camm: You might have to provide a different form of rate control.
Dr. Connolly: Possibly, yes. One of the things that the PALLAS study has brought up is that we don't know
that much about rate control. There have been almost no trials in permanent AF. The only one is quite a
small trial with somewhat inconclusive results, the RACE-2 study. Other than that, there are virtually no
randomized trials focusing on this high-risk population, and trying to understand what is the best treatment
for them is difficult. We hypothesized that further rate slowing would be beneficial, and dronedarone
certainly provides that. Was the rate slowing actually harmful? We don't know, but one thing we do know is
we need to learn more about permanent AF.
Just as an aside, we see amiodarone used quite a lot for rate control. In Europe and in Latin America it's
used widely, and also in North America. Should we be using amiodarone for rate control at all, considering
that we know nothing about its benefits or harms in that setting?
Dr. Camm: It's often exactly the same story that I just developed with Jean-Yves' patient taking
dronedarone. Usually the patient has been taking amiodarone for rhythm control and despite that goes into
permanent AF, and the physician leaves the patient on amiodarone simply because it's providing good rate
control.
Dr. Connolly: And the patient feels well.
Dr. Camm: And the patient feels well, but we now know with dronedarone that that should not be the
policy. We should take patients off it.
Dr. Connolly: I would actually question whether this should be done with any of the antiarrhythmic drugs
based on the results of PALLAS, especially since these drugs have actions that we don't understand that
well in this population.
Dr. Camm: There is another group of patients where dronedarone should not be used nowadays. It's in
patients with a history of heart failure or actually with heart failure. The problem I have is the history of heart
failure. Breathlessness or ankle edema can occur for other causes other than heart failure. Calcium
antagonists cause ankle edema, for example, or COPD [chronic obstructive pulmonary disease] causes
breathlessness. How would you approach a patient with a history suggestive of heart failure before
deciding whether or not you should use dronedarone?
Dr. Le Heuzey: I would be very cautious with this patient, mainly because we don't know everything about
it.
It's clear that some patients have heart failure at the time of the occurrence of AF, but this heart failure is
due only to the AF, so-called tachycardia-induced cardiomyopathy, even if it's for a short period. So, this
patient after the AF episode may not have heart failure, neither systolic nor diastolic. If we give drugs to
avoid the episode of AF and in turn avoid heart failure, it would be logical to do that, but we need to be
cautious. I prefer to hold off doing that if I see a patient for whom I can't identify if he has or has had a
history of heart failure. I prefer to be cautious and avoid dronedarone.
Dr. Connolly: I agree with being cautious. We have to be cautious with the use of all antiarrhythmic drugs.
In general, they all have difficulties. One thing that struck me would be if you have a patient where it's

borderline: Is it heart failure or is it not heart failure? To me, it's always helpful to look for objective
evidence. If there's no systolic dysfunction and no serious diastolic dysfunction, perhaps that's a way to be
able to resolve the uncertainties. I don't know if that's the right way to do it or whether we should be
cautious.
Dr. Camm: Thank you very much, gentlemen. It's been an interesting discussion. It has been prompted by
the results of the PALLAS trial reported here in Orlando at the American Heart Association. Unexpected
findings: an increase in cardiovascular death, an increase in stroke, and an increase in hospitalizations for
heart failure. This has caused repercussions at the regulatory level in Europe, and we're now not supposed
to use dronedarone in patients with permanent AF and not supposed to use it in patients with heart failure
or indeed a history of heart failure. We've been exploring cases of this kind this morning, and we're
beginning to understand the true place of dronedarone. It's useful in patients with minimal or no heart
disease with or without hypertension, and it can still be used in patients with coronary artery disease.
Thank you very much.
Supported by an independent educational grant from sanofi.
This article is a CME certified activity. To earn credit for this activity visit:
http://www.medscape.org/viewarticle/754713
Disclaimer The material presented here does not necessarily reflect the views of Medscape, LLC, or companies that support educational programming on www.medscape.org. These materials may discuss therapeutic products that have not been approved by the US Food and Drug Administration and off-label uses of approved products. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or employing any therapies described in this educational activity. Medscape Education © 2011 Medscape, LLC
This article is a CME certified activity. To earn credit for this activity visit: http://www.medscape.org/viewarticle/754713




















