Embed Size (px)
Citation preview

Special reviews Antiarrhythmic and Haemodynamic Effects of the Commonly Used Intravenous Electrolytes
J. REDMAN, L. I. G. WORTHLEY Department of Critical Care Medicine, Flinders Medical Centre, Adelaide, SOUTH AUSTRALIA
ABSTRACT Objective: To review the physiology and cardiovascular effects of the commonly used intravenous electrolytes. Data sources: Abstracts, articles and published reviews of studies reported from 1966 to 2000 and identified through a MEDLINE search on cardiac arrhythmias and electrolytes. Summary of review: While isotonic saline solutions are used to improve the haemodynamic status in critically ill patients who are hypotensive and hypovolaemic, other intravenous solutions including potassium chloride, calcium chloride, magnesium sulphate and sodium or potassium phosphate as well as hypertonic saline and sodium bicabonate have unique and often therapeutically useful haemodynamic and antiarrhythmic effects. Potassium chloride solutions are used to treat hypokalaemia with a maximum speed of correction in an adult of 20 mmol per 30 minutes when an acute myocardial infarct is present. A greater infusion rate may be necessary when ventricular or supraventricular tachyarrhythmias are present although close ECG monitoring will be required. Magnesium sulphate (2 - 20 mmol) has been used for hypomagnesaemic and normomagnesaemic cardiac arrhythmias (particularly when digoxin induced) and calcium chloride (3.4 - 6.8 mmol) is used to treat hyperkalaemic and hypermagnesaemic cardiac arrhythmias. Both hypertonic sodium bicarbonate and sodium chloride solutions have antiarrhythmic effects that may be beneficial in conditions that include tricyclic poisoning, hyperkalaemia and bupivicaine toxicity, although sodium bicarbonate is generally used for tricyclic cardiotoxicity. Low cardiac output states and arrhythmias have also been reported in hypophosphataemic patients that are reversed by infusions of potassium or sodium phosphate. Conclusions: Intravenous potassium chloride, calcium chloride, magnesium sulphate, sodium and potassium phosphate, sodium bicarbonate and hypertonic saline can be used effectively to alter the haemodynamic status and manage cardiac arrhythmias. However, their indications are selective and complications may occur, so careful administration and monitoring are required with their use. (Critical Care and Resuscitation 2001; 3: 22-34)
Key words: Myocardial action potential, magnesium sulphate, potassium chloride, calcium chloride, sodium bicarbonate, hypertonic saline, sodium phosphate, potassium phosphate
Excitability of myocardial tissue depends upon the intracellular and extracellular concentrations of electro-
lytes including potassium, sodium, magnesium and calcium, with myocardial excitability varying with
Correspondence to: Dr. L. I. G. Worthley, Department of Critical Care Medicine, Flinders Medical Centre, Bedford Park, South Australia 5042 (e-mail: [email protected])
22

Critical Care and Resuscitation 2001; 3: 22-34 J. REDMAN, ET AL
changes in concentrations of these electrolytes. The cardiac cell membrane (i.e. sarcolemma) is an ion-impermeable lipid bilayer composed of phospho-lipid molecules that separate the myocardial extracell-ular fluid (ECF) and intracellular fluid (ICF) compart-ments. With the appropriate stimulus, macromolecular proteins that traverse the lipid bilayer (i.e. channels), selectively permit ions to move from one side of the sarcolemma to the other. These channels are selectively permeable to different ionic species and are controlled by ‘gates’ which may be voltage sensitive, time sensitive and receptor operated. Flow through the channel for a particular ion depends upon the driving force (i.e. the difference between the transmembrane potential and the equilibrium potential for that ion) and the ease with which the ion passes through the channel (i.e. the conductance). The differences in ionic concen-trations, or more precisely ionic activities, across the sarcolemma establish the electrochemical gradients. Concentration gradients for K+, Na+ and Ca2+ cause K+ to move from the intracellular to the extracellular compartment, and Na+ and Ca2+ from the extracellular to the intracellular compartment. Energy-dependent ionic pumps are required to maintain the differential ionic concentrations across the membrane. While abnormal concentrations of these electrolytes in the ECF may alter the excitability and contractility of myocardial cells, the ECF concentrations of the electrolytes may also be altered for therapeutic effect. We review the physiology of myocardial excitability and the effects of altered concentration of these electrolytes on the excitability and contractility of myocardial cells, as well as the therapeutic effects of an increase in their ECF concentrations. The resting membrane potential The resting membrane potential (RMP) is the potential difference across the cell membrane during electrical diastole. For the myocardial muscle fibre this is - 90 mV (i.e. the ICF has a negative potential when compared with the ECF). The RMP is largely determined by the K+ gradient across the cell membrane. As K+ is about 20 times more permeable than Na+, it tends to move down its concentration gradient leaving the interior of the cell negative. If, at rest, the sarcolemma was more permeable to Na+ than K+, then Na+ would tend to move to the interior of the cell and cause a positive RMP (this movement of sodium is only facilitated during phase 0 of the action potential). If one assumes the cell membrane is permeable to potassium only, the RMP may be derived from the Nernst equation. However, the membrane potential at any given time depends upon the distribution of all fluid ions and the cell membrane permeabilities to these ions
at that point in time. The Goldman constant field equation expands the Nernst equation to consider the effects of sodium, chloride and other ions as well as potassium on the trans-membrane potential.1 Neverthe-less, at rest, potassium plays the major role in determin-ing the resting membrane potential (RMP) thus the RMP is often derived from the Nernst equation which is represented as: EK = 61.5 x log [ K+ ]o / [ K+ ]i Where EK = RMP (equilibrium potential for K+) [ K+ ]o = K+ concentration outside the cell [ K+ ]i = K+ concentration inside the cell The Nernst equation reveals that the extracellular K+ has a greater effect on RMP than intracellular K+. An increase in ECF K+ reduces the RMP, inactivating the fast response and reducing the conducting velocity, all of which cause the electrocardiogram changes of, prolongation of the PR interval and QRS wave, which in the extreme may lead to sinus arrest and broad wave slow ventricular tachycardia, respectively. An increase in the ECF K+ also accelerates repolarisation, producing tall peaked T waves. A decrease in ECF K+ hyper-polarises the cell membrane, although as the permea-bility of the membrane to K+ reduces with hypo-kalaemia, the hyperpolarisation is smaller than that expected from the Nernst equation.2 The resting membrane potential is set largely by the inward rectifier K+ channels (IK1).3 The myocardial cell action potential This has been divided into four phases which are largely determined by the selective alterations in ion permeabilities of the sarcolemma (Figure 1). Phase 0. This represents the initial fast depolarisation phase due to a rapid inward sodium current (INa) which is initiated by a stimulus that elevates the RMP from - 90 mV to a threshold value of - 60 mV, increasing the membrane permeability to Na+. The stimulus also decreases the membrane permeability to K+ (as depolarisation deactivates the inward rectifier IK1 channels). Both of these changes cause the cell to reverse its polarity, with the interior of the cell changing from - 90 to + 30 mV. The deactivation of the inward rectifier IK1 channels is prolonged and is reactivated again during phase 3. The rapid inward current (INa) is dependent upon the RMP. If the RMP is less negative than - 90 mV, before the stimulus, the rate of depolarisation is slow and the impulse is conducted slowly. The rapid inward current is blocked by a RMP of less than - 60 mV, which may
23

J. REDMAN, ET AL Critical Care and Resuscitation 2001; 3: 22-34
occur with a high external (e.g. ECF) concentration of K+. If the RMP is more negative than - 90 mV before the stimulus, then the rate of depolarisation is rapid and the impulse is conducted rapidly.
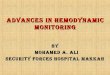
Figure 1. The ECG, intracellular cardiac action potential, myocardial tension and ionic conductances (rapid inward (Na+), slow inward (Ca2+), outward current (K+)). The absolute refractory period occurs between the first two dashed lines and the relative refractory period occurs between the last two dashed lines. (Modified from Poole-Wilson PA, Potassium and the heart, Clinis Endocrinol Metab 1984;13:249-260.) Phase 1. Phase 1 represents an initial period of rapid repolarisation due to closure of sodium channels and a transient outward current (Ito) caused by a rapid activation (i.e, increase in K+ permeability) then inactiv- ation of outward potassium channels.4 Phase 2. Phase 2 is a plateau period of repolarisation which results from an increase in the sarcolemmal K+
permeability, due to activation of the delayed rectifier potassium channels (IK) and a ‘slow’ inward current due to an inflow of Ca2+ (and Na+) ions through a ‘slow’ channel.4 This ‘slow’ channel is known as the calcium channel as it is 100 times more selective for Ca2+ than Na+, even though both Ca2+ and Na+ ions flow through it and Na+ ions may account for nearly one-third of the slow inward current (due to a higher ECF Na+ in comparison with Ca2+).5,6 During phases 1 and 2, there is a gradual return of the intracellular potential toward zero, due to an increase in Ca2+ permeability triggered initially by the inward sodium current. This slow inward calcium current is also responsible for the coupling of the excitation of the cell membranes to the activation of the contractile proteins and is sensitive to the ECF Ca2+ concentration. An important feature of many calcium channels is their sensitivity to control by sarcolemmal receptors. In cardiac muscle, β1 agonists, and in vascular smooth muscle α-adrenergic agonists increase Ca2+ influx via the slow inward current. In both cases, the increase in Ca2+ flux appears to be due to recruitment of an additional number of active calcium channels rather than an increase in the size of the channel or alteration in the rates at which the gates open or close. The calcium channels are also divided into two broad groups (i.e. voltage-sensitive or receptor operated) depending on the stimulus required to achieve the activated state. Channels which are activated in response to an appropriate change in the membrane action potential are known as voltage-sensitive channels. The receptor-operated channel is dependent for its activation on an interaction between cell surface receptors and specific neurotransmitters (e.g. acetylcholine, noradrenaline, histamine and adenosine). Phase 3. This represents a relatively fast period of repolarisation with a slow return of the intracellular potential to the RMP of - 90 mV due to a delayed increase in K+ permeability (due to a reactivation of the inward rectifier IK1 channels and deactivation of the delayed rectifier IK channels) and decrease in Ca2+ permeability. Phase 4. The action potential of the myocardial conducting tissue (with the exception of the mid atrioventricular nodal region) has an unstable resting membrane potential due to a steady inward current (If) carried by Na+ through a relatively nonspecific channel activated by polarisation to high membrane potentials in the sinoatrial (SA) and atrioventricular (AV) nodal cells and His-Purkinje cells.7 This channel is strongly modulated by neurotransmitters and is responsible for the tissue’s pacemaker activity. Acetylcholine decreases the slow inward current by activating the receptor operated muscarinic K+ channels (KAch). This channel is
24

Critical Care and Resuscitation 2001; 3: 22-34 J. REDMAN, ET AL
Arrhythmias. Hypokalaemia can cause atrial tachy-arrhythmias (e.g. paroxysmal supraventricular tachy-cardia, multifocal atrial tachycardia) and ventricular tachyarrhythmias (e.g. torsades de pointes,9,10 ventric-ular tachycardia, ventricular fibrillation) in the absence of underlying cardiac disease.11 Hypokalaemia (but not hypomagnesaemia12) is also a risk factor of ventricular tachycardia (VT) and ventricular fibrillation (VF) in the early post myocardial infarction period,13,14 which may be due to stress-related adrenaline secretion, rather than hypokalaemia per se.15-17 The increase in adrenaline secretion associated with an acute myocardial infarction causes hypokalaemia by inducing a β2 receptor mediated18,19 influx of K+ (largely in skeletal muscle cells16). Potassium supplementation reduces the incidence of VF in these patients.20 The risk of primary cardiac arrest is greater in hypertensive patients treated with thiazide diuretics, than in patients who are treated with a combination of thiazide and potassium-sparing diuretic agents.21
also opened by activation of the purinergic (adenosine) receptor. The speed with which the RMP reduces to the threshold potential, determines the rate at which the tissue discharges. The SA and upper AV node have a diastolic depolarisation phase (i.e. phase 4), a maximum RMP of -70 to - 50 mV, and a threshold potential (with depolarisation) which is - 40 mV, i.e. the slow inward current is activated when the fast inward current is inactivated, implying that an action potential can occur in partially depolarised cells in which the fast Na+ channels have been inactivated. The action potential of the AV node is due to the slow inward Ca2+ current alone, as it is resistant to Tetrodotoxin (a fast sodium channel inhibitor), and is sensitive to verapamil and manganese (i.e. slow calcium channel inhibitors).6 IK(ATP) is a K+ current carried through a channel which is opened by intracellular ADP (and other intracellular nucleoside diphosphonates) and blocked by ATP (an effect which is inhibited by adenosine, ADP and other intracellular nucleoside diphosphonates). The channel is not blocked by extracellular ATP. This channel contributes to the shortening of the action potential during myocardial ischaemia and has been associated with the cardioprotective mechanism of ischaemia related preconditioning.8
Myocardial inotropic effects. A reduction in concentration of extracellular potassium has a mild positive inotropic effect due to an associated increase in intracellular Na+, which activates a Na/Ca exchange and increases the intracellular Ca2+ concentration.22
The unique action potential of myocardial tissue provides the properties of: conductivity (i.e. the ability to conduct an impulse, the speed of which is related to speed of depolarisation), automaticity (i.e. the property of spontaneous impulse formation), excitability (i.e. the property of all myocardial tissue which relates to an ability to respond to a stimulus) and refractoriness (i.e. a period of reduced ability of the myocardium to respond to a stimulus).
Standard treatment of hypokalaemia usually involves administration of intravenous or oral potassium chloride, particularly when hypokalaemia is associated with metabolic alkalosis, although potassium may be replaced as a chloride, phosphate, citrate or acetate salt. If the patient has renal tubular acidosis and hypo-kalaemia, then potassium acetate or citrate is required. When phosphate depletion also exists, then potassium phosphate may be administered, although phosphate can only be infused slowly (e.g. maximum rate 2 - 6 mmol/hr/70 kg23,24) and is usually administered to correct a phosphate deficiency rather than potassium deficiency.
CARDIOVASCULAR EFFECTS OF ELECTROLYTES Potassium A linear relationship describing a decrease in plasma
potassium of 0.27 mmol/L/100 mmol deficit/70 kg body weight, has been described.25 However, this estimate should only be used as a guide. When replacing potassium, intravenous administration should normally not exceed 40 mmol/hr and plasma potassium levels should be monitored at 1 to 4-hourly intervals.26,27 In patients who have acute myocardial infarction and hypokalaemia, intravenous potassium is recommended at a rate of no greater than 10 mmol/30 min (in 50 - 100 mL of 5% dextrose), and repeated as necessary (rechecking the potassium level every hour) until the serum potassium is 4.0 - 4.5 mmol/L (or plasma potassium is 3.5 - 4.0 mmol/L).28 However in patients with severe hypokalaemia, administration of potassium
The extracellular K+ concentration is largely responsible for the resting membrane potential and therefore has a large influence on myocardial tissue excitability. Intravenous potassium is often used to treat hypokalaemic cardiac arrhythmias as the cardiac effects of hypokalaemia include excitability and contractility changes. For example: ECG changes. Hypokalaemia causes the U wave to become prominent, the T wave to flatten and invert, the ST segment to become depressed and the PR interval to increase. The QTc interval does not change although it may be mistaken for the QU interval or be prolonged due to an associated hypomagnesaemia.
25

J. REDMAN, ET AL Critical Care and Resuscitation 2001; 3: 22-34
salts should be either as an undiluted solution through a central venous line or diluted in 0.9% saline, as potassium in dextrose solutions have been reported to initially worsen the hypokalaemia.29 Some have advocated an antiarrhythmic dose of 2 mmol as a bolus30 or 6 mmol over 1 minute (to increase the plasma potassium by 2 mmol/L)31 to manage hypokalaemic tachyarrhythmias; however even with such a low dose, it is conceivable that in patients with low cardiac outputs, a dangerously high level of plasma potassium might occur transiently to cause sudden sinus arrest, AV block or asystole.32 Magnesium supplementation may also be required in patients with hypokalaemia because hypokalaemia and hypomagnesaemia commonly coexist. Moreover, renal potassium wasting may occur with hypomagnes-aemia (particularly if the plasma magnesium is < 0.5 mmol/L);33 thus hypomagnesaemia may impede the correction of hypokalaemia.27 Spironolactone, triamte-rene, amiloride or ACE inhibitors are of use in preventing renal potassium loss rather than an adjunctive measure during the correction of an existing deficit.27 While there have been no studies that have shown that potassium has an antiarrhythmic effect in normokalaemic patients, in patients who have resistant ventricular tachyarrhythmias, plasma potassium levels of > 4.0 - 4.5 mmol/L are often preferred. Calcium Ionised Ca2+ in ECF is needed for myocardial contraction and excitation-contraction coupling. Calcium chloride (or gluconate) is used to treat the life-threatening cardiovascular effects of hyperkalaemia, hypermagnesaemia and hypocalcaemia. Hyperkalaemia In the severely hyperkalaemic patient, calcium does not reduce plasma potassium; it is used to counter the toxic cardiac effects (and reverse the ECG changes) of hyperkalaemia by increasing the intracellular calcium34 causing the threshold potential to be less negative.35 The cardiac effects of hyperkalaemia incude: ECG changes. Hyperkalaemia characteristically causes, a tall slender, peaked or ‘tented’ T wave at plasma K+ concentrations of 6 mmol/L or greater (due to an increase in repolarisation rate), a prolongation of the P wave, QRS wave and the PR interval at plasma K+ concentrations of 7 mmol/L or greater, a diminution in the amplitude of the P wave, which may progress to sinus arrest, and a diminution in R wave and widening of the QRS complex (caused by a reduction in conduction velocity, producing a slow idioventricular rhythm) at plasma K+ concentrations of 8 mmol/L or
greater, and ‘sine-wave’ VT or VF at a plasma K+ level of 9 mmol/L or greater. Arrhythmias. While a progressive rise in plasma K+ can produce ‘sine-wave’ VT or VF, an abrupt rise in plasma K+ may produce sinus arrest, AV nodal block, first-, second- or third- degree heart block and asystole. Myocardial inotropic effects. Hyperkalaemia exerts a negative inotropic effect, which is caused by the decrease in duration of the action potential (and thus the duration of the slow calcium current) causing a reduction in intracellular Ca2+ and hypotension. For mild hyperkalaemia (i.e. plasma K+ > 4.5 and < 5.5) treatment usually includes reducing the potassium intake, correcting renal failure and treating the cause (e.g. ceasing non-steroidal antiinflammatory drugs, potassium sparing diuretics or angiotensin converting enzyme inhibitors). Treatment of severe hyperkalaemia (i.e. plasma K+ > 5.5 mmol/L) includes reducing the plasma potassium (by shifting potassium into the ICF and enhancing potassium excretion) and reducing the cardiac effects of hyperkalaemia (e.g. intravenous calcium salts). The administration of intravenous glucose and insulin, and sodium bicarbonate will reduce the ECF potassium,36 although nebulised salbutamol (10 - 20 mg) may also be useful (due to a β2 adrenergic effect activating the Na+K+-ATPase), as it can reduce the plasma potassium by 0.6 - 1 mmol/L, after 20 - 30 min and will last for 2 hr.37 Resonium A (sodium polystyrene sulfonate) has the capacity to bind 3.1 mmol of potassium per gram by releasing 3.1 mmol sodium. However, its onset is slower (e.g. maximum effect in 4 hours) and while it may be given rectally, in the unconscious hyper-kalaemic critically ill patient it probably has little place. In severe hyperkalaemia, calcium salts should be given first (3.4 - 6.8 mmol or 5 - 10 mL of 10% calcium chloride), followed by insulin and glucose. However, glucose is only necessary with insulin if there is normoglycaemia and should be infused over 5 - 10 minutes as a sudden increase in tonicity due to hyperglycaemia may temporarily increase the plasma potassium by 0.1 - 0.6 mmol/L for each 10 mosmol/kg increase in tonicity.38 This may then be followed by sodium bicarbonate 50 - 100 mmol and nebulised salbutamol. As all of the methods to reduce the plasma potassium are only temporary, treatment should also be aimed at the underlying cause which may include dialysis. Class I antiarrhythmic agents (and probably magnes-ium sulphate) are contraindicated in patients with hyperkalaemia as they potentiate myocardial conduction abnormalities (e.g. sinus arrest, AV nodal block, first-, second- or third- degree heart block and asystole).
26

Critical Care and Resuscitation 2001; 3: 22-34 J. REDMAN, ET AL
Hypermagnesaemia. As severe hypermagnesaemia (i.e. > 5 mmol/ L) can produce a generalised depression of cardiac conduction causing, junctional or sinus bradycardia, sinoatrial block, AV block, and asystole,39 treatment of severe hypermagnesaemia (as well as increasing excretion of the ion, which may require dialysis) may require intravenous calcium chloride (3.4 - 6.8 mmol) to rapidly manage the cardiac conduction defects. Hypocalcaemia While the cardiac effects of hypocalcaemia have included the ECG changes of a prolonged and shortened QTc with hypocalcaemia and hypercalcaemia respectiv-ely, many of the early studies which described this association were performed in patients who had chronic hyper- or hypocalcaemia, and the Ca2+ measurements were of plasma total calcium rather than plasma ionised Ca2+.40,41 It is now recognised that hypocalcaemia severe enough to cause myocardial depression (e.g. an ionised calcium level of 0.5 mmol/L or less) may be associated with a normal QTc interval42,43 and therefore a normal QTc interval does not exclude hypocalcaemia. Hypocalcaemia per se rarely if ever causes an arrhythmia.44,45 Chronic hypocalcaemia, however, may cause cardiac failure.46-49 In chronic renal failure patients receiving haemodialysis with varying concen-trations of ionised Ca2+ in the dialysate, have had varying effects recorded. Some studies have found that left ventricular contractility varied directly with the plasma ionised Ca2+;50,51 other studies have noted no effect on the left ventricular systolic function with an increase in serum calcium caused by a rise in concentrations of ionised Ca2+ in the dialysate.52,53 An acute rise in serum calcium, however, has been found to impair diastolic function (i.e. negative lusitropy).54 Intravenous Ca2+ is often used to increase blood pressure in patients who have a low ionised calcium level (usually < 0.8 mmol/L) which it does by causing peripheral vasoconstriction and increasing cardiac contractility. The predominant haemodynamic response may depend upon the patients initial ionised Ca2+ level55 and the presence or absence of underlying heart disease. Peripheral vasoconstriction predominates if the patient’s plasma ionised Ca2+ is normal and there is no underlying cardiac disease. Enhancement of myocardial contractility predominates if the patients plasma ionised Ca2+ is low and the patient has underlying cardiac disease, because the myocardial performance is often correlated directly with ECF Ca2+ in the presence of β-receptor down regulation46 (i.e. in patients who have chronic heart disease or prolonged exposure to beta-agonists) or in the presence of beta-blockade.56 If the vasoconstrictive response predominates, then the rise in
blood pressure tends to be transient; if an increase in contractility predominates, then the rise in blood pressure tends to be more prolonged.57 Critically ill trauma and septic patients often have low ECF Ca2+ levels which may only respond transiently to intravenous Ca2+ administration58,59 and it is thought that some of the ECF Ca2+ that moves intracellularly to increase cardiac contractility may, in the long term, be harmful.59,60 If intravenous calcium is considered necessary (i.e. to keep the ionised calcium > 0.8 mmol/L),61 then a continuous calcium infusion rather than a bolus dose is recommended.62,63 Vasoconstrictive agent: intravenous Ca2+ increases systemic blood pressure by increasing peripheral resistance64 (particularly in the presence of hypomagn-esaemia) due to a direct effect of the Ca2+ ion and an increase in catecholamine release at both the sympath-etic nerve ending and the adrenal medulla.57 Inotropic agent: intravenous Ca2+ increases myocar-dial contractility by increasing the amount of ECF Ca2+ available for myocardial contraction. Calcium also reverses the negative inotropic effect of a high ECF K+ level.65 Either calcium chloride or calcium gluconate may be used.66 Both are often packaged as 10 mL ampoules of a 10% solution. The 10% calcium chloride solution contains 0.68 mmol/mL of calcium, the 10% calcium gluconate solution contains 0.225 mmol/mL of calcium. As the clinical advantages of one salt when compared to the other have not been documented,57 and as recent clinical studies have shown rapid and equal dissociation of Ca2+ from both the chloride and gluconate salt66,67 (even in the absence of hepatic function67), it would seem that either salt may be used. Either 3 - 5 mL of 10% calcium chloride or 10 mL of 10% calcium gluconate may be administered under ECG control over 2 - 5 min. No more than 10 mL of the 10% calcium chloride solution should be given without measuring ionised Ca2+ levels to guide therapy. The mean plasma Ca2+ level in cardiac arrest patients was found to be 3.82 mmol/L, 5 min after a bolus of 5 mL of calcium chloride, which decreased to a mean level of 2.79 mmol/L after 10 min, and returned to normal after 15 min.67 If a continuous infusion of calcium is deemed necessary, then calcium chloride 10%, 1 - 5 mL/hr (i.e. 0.7 - 3.5 mmol/hr, to keep the plasma ionised calcium > 0.8 mmol/L and monitoring plasma ionised calcium 4-hourly) may be used.61 The clinical effects of intravenous Ca2+ are nausea, vomiting and generalised feeling of warmth and tingling, which may make the patient intensely uncomfortable. Acute administration of intravenous calcium may cause AV dissociation,
27

J. REDMAN, ET AL Critical Care and Resuscitation 2001; 3: 22-34
ventricular ectopics, VT and VF, particularly in the presence of digoxin toxicity or hypokalaemia.57,60,68 Other effects While there have been case reports where intravenous calcium salts have been used as pre-treatment of verapamil therapy that have caused reversion of paroxysmal supraventricular tachycardia69 (an effect which was probably was due to the concomitant elevation in blood pressure and reflex increase in cardiac parasympathetic tone that slowed atrioventricular conduction), reports of ventricular fibrillation have also been published.70 Magnesium Magnesium has been described as ‘nature’s physiol-ogic calcium blocker’, inhibiting Ca2+-induced muscle contraction by inhibiting the release of Ca2+ from the sarcoplasmic reticulum, increasing the uptake of Ca2+ by the sarcoplasmic reticulum (by stimulating the Ca-ATPase activity) and by competing with Ca2+ at certain binding sites on troponin C and myosin.71 Unlike the synthetic calcium-blockers, increasing extracellular Mg2+ has not been shown to block the entry of Ca2+ into the cell through the slow channel,71 although increasing intracellular magnesium experimentally inhibits calcium entry through the dihydropyridine-sensitive channels.72 In normomagnesaemic patients, intravenous magnesium sulphate causes coronary and systemic vasodilation (reducing coronary artery spasm and blood pressure, respectively), inhibits platelet function, and has antiarrhythmic effects when used to elevate plasma concentrations up to 2 mmol/L.73 It also causes a slight decrease in heart rate, a prolongation of the PR interval (due to an increase in the PA and AH interval without altering the HV interval), with no effect on the QRS (except at high doses) or QTc duration.74-77 Magnesium also decreases the sympathetic tone by causing a sympathetic ganglia blockade78 and reducing noradrenaline release and storage in the postganglionic sympathetic nerve fibres79,80 (although in normal individuals it increases plasma noradrenaline and neuropeptide-Y-like activity)81 and may also enhance parasympathetic tone.82 At plasma levels < 10 mmol/L, Mg2+ has no negative inotropic effects.83 Magnesium sulphate has been used as an antiarrhy-thmic agent to treat both hypomagnesaemic and normo-magnesaemic cardiac arrhythmias.84 Hypomagnesaemia The cardiac effects of hypomagnesaemia include ECG changes (e.g. prolongation of the QTc segment and U waves, although U waves are most likely due to an associated hypokalaemia), arrhythmias (e.g. ventricular
and atrial tachycardias44,85,86), negative myocardial inotropic effects (e.g. cardiac failure,87 cardiogenic shock88) and coronary ischaemia.89-92 Intravenous magnesium sulphate has been used in the treatment of: Arrhythmias. Both bolus and continuous intravenous infusions of magnesium sulphate have been used to treat ventricular ectopics and VT,85,93 even in the absence of overt hypomagnesaemia.94,95 It is the treatment of choice of alternating VF and asystole during cardiac arrest96 and is also effective in the treatment of halothane,97 digoxin98-100 or hypomagnesaemia101,102 -induced cardiac arrhythmias, torsades de pointes94,103 and multifocal atrial tachycardia104,105 (Figure 2 and Figure 3). In one study, magnesium sulphate was more effective than amiodarone in converting acute atrial tachyarrhythmias in critically ill patients.106 However, in a prospective randomised controlled study of in-hospital cardiac arrest, magnesium (8 mmol bolus followed by 32 mmol over the next 24 hours), did not improve immediate or long-term morbidity or mortality.107 Hypertension. Continuous infusions have been used to treat hypertension associated with pre-eclampsia or tetanus. Intravenous magnesium sulphate causes a direct peripheral arteriolar vasodilation which may be associa-ted with a generalised warm and tingling sensation and reduction in blood pressure.108 Cardiac failure. Intravenous infusions of magnesium sulphate do not have a direct effect on myocardial contractility in normal individuals.83 However, in hypomagnesaemic patients, cardiac failure87 and cardiogenic shock88 have been corrected with intravenous magnesium sulphate infusions. Acute myocardial infarction. An infusion of intravenous magnesium sulphate has been reported to be associated with a decrease in mortality in normo-magnesaemic patients with acute myocardial infarct-ion;73,86,109,110 even when thrombolytic and aspirin therapy were used, mortality was reduced by a further 25% (i.e. by 2.5 patients per 100 patients).73 The time of intravenous magnesium administration in acute myoca- rdial infarction may be critical, as magnesium given at a mean of 3 hours after the onset of chest pain appears to be beneficial whereas magnesium given at a mean of 8 hr is not.111 In the fourth international study of infarct survival (ISIS-4), no significant advantage was recorded with intravenous magnesium sulphate (8 mmol in 15 min followed by 72 mmol in 24 hr) in any patient group (e.g. with or without thrombolytic therapy, and in those in whom it was infused before thrombolytic reperfusion had probably occured).112 However, the optimal 24 hr dose of magnesium may be between 50 to 65 mmol and that doses of > 75 mmol (ISIS-4 used 80 mmol/24 hr) may increase mortality (due to an increase in bradyarrhythmias and heart failure);113 accordingly some
28

Critical Care and Resuscitation 2001; 3: 22-34 J. REDMAN, ET AL
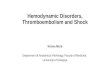
Figure 2. An ECG rhythm strip demonstrating multifocal atrial tachycardia (heart rate 166).
Figure 3. An ECG rhythm strip of the above patient 2 minutes after an infusion of 10 mmol of magnesium sulphate (heart rate 127). believe that the use of magnesium in myocardial infarction may warrant reexamination.114
Unstable angina. In patients with unstable angina, an infusion of intravenous magnesium sulphate (8 mmol bolus followed by 3 mmol/hr for 24h) has been reported to be associated with a reduction in CK-MB release, a more rapid regression of T wave changes and reduced adrenaline excretion, when compared with a placebo.115 Post cardiac surgery. In one study of post cardiac surgery patients an intravenous infusion of 8 mmol of magnesium chloride (over 20 min) decreased the incidence of ventricular arrhythmias and increase the cardiac index,116 although it does not alter the incidence of atrial fibrillation in post coronary artery bypass patents.117 Intravenous magnesium sulphate (2 - 8 mmol bolus over 2 - 5 min, up to 30 - 40 mmol during the first 12 hr post operative period) may also be used to control hypertensive episodes (and episodes of shivering and tachycardia). It also reduces postoperative analgesic requirements118 and promotes normal sleep.119 Magnesium sulphate may be administered as an 8 mmol intravenous bolus (over 5 min), followed by an infusion of 65 mmol in 50 - 500 mL of 5% dextrose over 24 hr, which increases, on average, the serum
magnesium concentration to 1.55 mmol/L, in patients without renal failure.73 If the bolus is not followed by an infusion, the serum magnesium level returns to normal after 20 min.120 While some believe that a rationale exists for the use of intravenous magnesium in patients with high plasma potassium levels,76 magnesium can potentiate myocard-ial conduction abnormalities (e.g. sinus arrest, AV nodal block, first-, second- or third- degree heart block and asystole) and therefore is probably contraindicated in patients with hyperkalaemia. In hyperkalaemia associat-ed with digoxin poisoning however, intravenous magnesium sulphate may eliminate refractory ventricul-ar tachycardia and decrease the serum potassium.121 Other effects of intravenous magnesium sulphate include an unpleasant flushing, and nausea and vomiting, particularly if administered too rapidly. Sodium bicarbonate Intravenous sodium bicarbonate as an 8.4% (1000 mmol/L) solution has been used for many acute cardiovascular disorders. For example: Hyperkalaemia. While intravenous sodium bicar-bonate (e.g. 100 mL of 8.4% or 100 mmol) is often used
29

J. REDMAN, ET AL Critical Care and Resuscitation 2001; 3: 22-34
in patients with hyperkalaemia and acidosis, in one study of patients with chronic renal failure, the effect of sodium bicarbonate was inconsistent and only reached significance at 4 hours after a constant administration.122 Therefore, severe cardiac dysfunction secondary to hyperkalaemia should be treated with intravenous calcium salts in the first instance. Tricyclic overdosage. Increasing arterial blood pH reduces free tricyclic blood levels.123 Hyperventilation, to induce respiratory alkalosis, is often used first to treat respiratory acidosis, metabolic acidosis, and the ventricular arrhythmias associated with tricyclic anti-depressant toxicity.124,125 If ventricular arrhythmias persist, both hyperventilation and sodium bicarbonate are used to keep the plasma pH greater than 7.45.126 Cardiac arrest. Administration of intravenous sodium bicarbonate does not improve the ability to defibrillate,127 improve left ventricular contractility,128 increase the cardiovascular response to circulating catecholamines129 or improve survival rates in cardiac arrest.130-133 It is now no longer recommended in the routine management of cardiac arrest.134 Hypertonic saline Hypertonic saline may be used as a 3% (510 mmol/L), 7.5% (1275 mmol/L) or 20% (3400 mmol/L) solution (usually < 100 mmol as a bolus) and has many cardiovascular effects when infused. For example: Hyponatraemia. Chronic hyponatraemia is assoc-iated with a positive inotropic effect, which is most likely due to an increase in the intracellular Na+ causing a Na+/Ca2+ exchange to increase the intracellular Ca2+.135 While some studies have reported a negative inotropic effect with the acute administration of hypertonic saline,136,137 other have reported an increase in cardiac output due to a positive inotropic effect, peripheral vasodilation and increase in preload.138,139 Hypertonic saline does not alter ischaemic injury associated with myocardial infarction and reperfusion.140 Antiarrhythmic effects. In an experimental model of tricyclic antidepression, hypertonic saline was more effective than sodium bicarbonate or hyperventilation in reversing prolongation of the QRS interval.141 In other experimental models, hypertonic saline abolished oubaine-induced arrhythmias,142 and (with pretreatment) provided significant protection against bupivicaine-induced ventricular arrhythmias.143 Phosphate In one study of patients without clinical cardiac disease who had hypophosphataemia, significant ventricular ectopic activity was recorded which improved or disappeared after phosphate replace-
ment.144 In another study of patients with acute myocardial infarction, a low serum phosphate (< 0.84 mmol/L) was a significant predictor of ventricular tachycardia during the first 24 hr of hospitalisation.145 Acute hypophosphataemia may be associated with a reversible form of cardiac failure.146 Received: 19 December 2000 Accepted: 27 February 2001 REFERENCES 1. Goldman DE. Potential impedance and rectification in
membranes. J Gan Physiol 1943;27:37-60. 2. Wong KC, Schafer PG, Schultz JR. Hypokalemia and
anesthetic implications. Anesth Analg 1993;77:1238-1260.
3. Surawicz B. Role of potassium channels in cycle length dependent regulation of action potential duration in mammalian cardiac Purkinje and ventricular muscle fibres. Cardiovasc Res 1992;26:1021-1029.
4. Task Force of the Working Group on Arrhythmias of the European Society of Cardiology. The Sicilian Gambit. A new approach to the classification of drugs based on their action on arrhythmogenic mechanism. Circulation 1991;84:1831-1851.
5. Reuter H, Scholz H. A study of the ion selectivity and the kinetic properties of the calcium dependent slow inward current in mammalian cardiac muscle. J Physiol (Lond) 1977;264:17-47.
6. Gilmore RF, Zipes DP. Slow inward current and cardiac arrhythmias. Am J Cardiol 1985;55:89B-101B.
7. DiFrancesco D, Ferroni A, Mazzanti M, Tromba C. Properties of the hyperpolarizing-activated current (if) in cells isoplated from the rabbit sinoatrial node. J Physiol 1986;377:61-88.
8. Terzic A, Jahangir A, Kurachi Y. Cardiac ATP-sensitive K+ channels: regulation by intracellular nucleotides and K+ channel opening drugs. Am J Physiol 1995;269(Cell Physiol.38):C525-C545.
9. Curry P, Fitchett D, Stubbs W, Krikler D. Ventricular arrhythmias and hypokalaemia. Lancet 1976;ii:231-233.
10. Ruder MA, Flaker GC, Alpert MA, Bertuso J. Hypokalemia as a cause of cardiac arrest: results of electrophysiologic testing and long-term follow-up. Am Heart J 1985;110:490-491.
11. Helfant RH. Hypokalaemia and arrhythmias. Am J Med 1986;80 (Supp 4A):13-22.
12. Higham PD, Adams PC, Murray A, Campbell RW. Plasma potassium, serum magnesium and ventricular fibrillation: a prospective study. Q J Med 1993;86:609-617.
13. Nordrehaug JE, Johannessen KA, von der Lippe G. Serum potassium concentration as a risk factor of ventricular arrhythmias early in acute myocardial infarction. Circulation 1985;71:645-649.
14. Nordrehaug JE, von der Lippe G. Hypokalaemia and ventricular fibrillation in acute myocardial infarction. Br Heart J 1983;50:525-529.
30

Critical Care and Resuscitation 2001; 3: 22-34 J. REDMAN, ET AL
35. Hoffman BF, Suckling EE. Effect of several cations on transmembrane potentials of cardiac muscle. Am J Physiol 1956;186:317-324.
15. Struthers AD, Reid JL, Whitesmith R, Rodger JC. Effects of intravenous adrenaline on the electrocardiogram, blood pressure and serum potassium. Br Heart J 1983;49:90-98. 36. Blumberg A, Weidmann P, Gnadinger M. Effect of
various therapeutic approaches on plasma potassium and major regulating factors in terminal renal failure. Am J Med 1988;85:507-512.
16. Brown MJ, Brown DC, Murphy MB. Hypokalemia from beta2-receptor stimulation by circulating epinephrine. N Engl J Med 1983;309:1414-1419.
37. Allon M, Dunlay R, Copkney C. Nebulized albuterol for acute hyperkalaemia in patients on hemodialysis. Ann Intern Med 1989;110:426-429.
17. Editorial. Adrenaline and potassium: everything in flux. Lancet 1983;ii:1401-1403.
18. Struthers AD, Reid JL, Whitesmith R, Rodger JC. The effect of cardioselective and nonselective beta-adrenoreceptor blockade on the hypokalaemic and cardiovascular responses to adrenomedullary hormone in man. Clin Sci 1983;65:143-147.
38. Saxton CR, Seldin DW. Clinical interpretation of laboratory values. In Kokko JP, Tannen RL (eds). Fluids and Electrolytes. WB Saunders Co, Philadelphia, 1986, pp 3-62.
39. Berns AS, Kollmeyer KR. Magnesium-induced bradycardia. Ann Intern Med 1976;85:760-761.
19. Brown MJ. Hypokalaemia from beta2-receptor stimulation by circulating epinephrine. Am J Cardiol 1985;56:3D-9D. 40. Nierenberg DW, Ransil BJ. Q-aTc interval as a clinical
indicator of hypercalcemia. Am J Cardiol 1979;44:243-248.
20. Gettes LS, Surawicz B, Kim KH. Role of myocardial K and Ca in initiation of ventricular fibrillation. Am J Physiol 1966;211:699-702. 41. Bronsky D, Dubin A, Waldstein SS et al. Calcium and
the electrocardiogram Am J Cardiol 1961;7:823-832. 21. Siscovick DS, Raghunathan TE, Psaty BM, Koepsell TD, Wicklund KG, Lin X, Cobb L, Rautaharju PM, Copass MK, Wagner EH. Diuretic therapy for hypertension and the risk of primary cardiac arrest. N Engl J Med 1994;330:1852-1857.
42. Rumancik WM, Denlinger JK, Nahrwold ML, Falk RB. The Q-T interval and the serum ionized calcium JAMA 1978;240:366-368.
43. Scheidegger D, Drop LJ. The relationship between duration of Q-T interval and plasma ionized calcium concentration. Anesthesiology 1979;51:143-148.
22. Langer GA. The intrinsic control of myocardial contraction - ionic factors. N Engl J Med 1971;285:1065-1071. 44. Commerford PJ, Lloyd EA. Arrhythmias in patients with
drug toxicity, electrolyte, and endocrine disturbances. Med Clin N Amer 1984;68:1051-1078.
23. Vannatta JB. High-dose intravenous phosphorous therapy for severe complicated hypophosphatemia. Southern Med J 1983;76:1424-1429. 45. Wong KC, Schafer PG, Schultz JR. Hypokalemia and
anesthetic implications. Anesth Analg 1993;77:1238-1260.
24. Lentz RD. Treatment of severe hypophosphatemia. Ann Intern Med 1978;89:941-948.
46. Ginsburg R, Esserman LJ, Bristow MR. Myocardial performance and extracellular ionized calcium in a severely failing human heart. Ann Int Med 1983;98:603-606.
25. Sterns RH, Cox M, Felig PU, et al. Internal potassium balance and the control of the plasma potassium concentration. Medicine 1981;60:339-354.
26. Stockigt JR. Potassium metabolism. Anaesth Intens Care 1977;5:317-325. 47. Levine SN, Rheams CN. Hypocalcemic heart failure.
Am J Med 1985;78:1033-1035. 27. Tannen RL. Potassium disorders. In Kokko JP, Tannen RL (eds). Fluids and Electrolytes. WB Saunders Co, Philadelphia, 1986, pp 150-228.
48. Connor TB, Rosen BL, Blaustein MP, Applefeld MM, Doyle LA. Hypocalcemia precipitating congestive cardiac failure. N Engl J Med 1982;307:869-872. 28. Standards and guidelines for cardiopulmonary
resuscitation (CPR) and emergency cardiac care (ECC). JAMA 1992;268:2172-2288.
49. Bashour T, Basha HS, Cheng TO. Hypocalcemic cardiomyopathy. Chest 1980;78:663-665.
50. Lang RM, Fellner SK, Neumann A, Bushinsky DA, Borow KM. Left ventricular contractility varies directly with blood ionized calcium. Ann Intern Med 1988;108:524-529.
29. Agarwal A, Wingo CS. Treatment of hypokalaemia. N Engl J Med 1999;340:154-155.
30. Selmonosky CA. The effect of small doses of potassium on postoperative ventricular arrhythmias. J Thorac Cardiovasc Surg 1967;53:349-352. 51. Henrich WL, Hunt JM, Nixon JV. Increased ionized
calcium and left ventricular contractility during haemodialysis. N Engl J Med 1984;310:19-23.
31. Halpern ML, Kamel KS. Potassium. Lancet 1998;352:135-140.
52. Näppi SE, Saha HH, Virtanen VK, Mustonen JT, Pasternack AI. Hemodialysis with high-calcium dialysate impairs cardiac relaxation. Kidney Int 1999;55:1091-1096.
32. Tanaka K Pettinger WA. Pharmacokinetics of bolus potassium injections for cardiac arrhythmias. Anesthesiology 1973;38:587-589.
33. Gennari FJ. Hypokalaemia. N Engl J Med 1998;339:451-458. 53. Sztajzel J, Ruedin P, Monin C, Stoermann C, Leski M,
Rutishauser W, Lerch R. Effect of altered loading conditions during haemodialysis on left ventricular filling pattern. Eur Heart J 1993;14:655-661.
34. Bisogno JL, Langley A, von Dreele MM. Effect of calcium to reverse the electrocardiographic effects of hyperkalemia in the isolated rat heart: a prospective, dose-response study. Crit Care Med 1994;22:697-704.
31

J. REDMAN, ET AL Critical Care and Resuscitation 2001; 3: 22-34
54. Virtanen VK, Saha HH, Groundström KW, Seppälä ES, Pasternack AI. Calcium infusion and left ventricular diastolic function in patients with chronic renal failure. Nephrol Dial Transplant 1998;13:384-388.
55. Drop LJ, Scheidegger D. Plasma ionized calcium concentration. Important determinant of the haemodynamic response to calcium infusion. J Thorac Cardiovasc Surg 1980;79:425-431.
56. Stulz PM, Scheidegger D, Drop LJ Lowenstein E, Laver MB. Ventricular pump performance during hypocalcemia. J Thorac Cardiovasc Surg 1979;78:185-194.
57. Drop LJ. Ionized calcium, the heart, and haemodynamic function. Anesth Analg 1985;64:432-451.
58. Drop LJ, Laver MB. Low plasma ionized calcium and response to calcium therapy in critically ill man Anesthesiology 1975;43:300-306.
59. Harrigan C, Lucas CE, Ledgerwood AM. Significance of hypocalcemia following hypovolaemic shock. J Trauma 1983;23:488-492.
60. Carlon GC, Howland WS, Goldiner PL, Kahn RC, Bertoni G, Turnbull AD. Adverse effects of calcium administration. Arch Surg 1978;113:882-885.
61. Zaloga GP. Hypocalcemia in critically ill patients. Crit Care Med 1992;20:251-262.
62. Steinhorn DM, Sweeney MF, Layman LK. Pharmacodynamic response to ionized calcium during acute sepsis. Crit Care Med 1990;18:851-857.
63. Chernow B. Calcium: does it have a therapeutic role in sepsis. Crit Care Med 1990;18:895-896.
64. Nerothin DD, Kane PB. Calcium-vasodilator or vasoconstrictor?. Anesth Analg 1984;63:255.
65. Wiggers CJ. Monophasic and deformed ventricular complexes resulting from surface applications of potassium salts. Am Heart J 1930;5:346-351.
66. Cote CJ, Drop LJ, Daniels AL, Hoaglin DC. Calcium chloride versus calcium gluconate: comparison of ionization and cardiovascular effects in children and dogs. Anesthesiology 1987;66:465-470.
67. Martin TJ, Kang Y, Robertson KM, Virji MA, Marquez JM. Ionization and hemodynamic effects of calcium chloride and calcium gluconate in the absence of hepatic function. Anesthesiology 1990;73:62-65.
68. Dembo HD. Calcium in advanced life support. Crit Care Med 1981;9:358-359.
69. O'Brien JF, Tremml GP, Falk JL. Intravenous calcium chloride in the conversion of paroxysmal supraventricular tachycardia to normal sinus rhythm. Am J Emerg Med 1996;14:50-52.
70. Chin RL, Garmel GM, Harter PM. Development of ventricular fibrillation after intravenous calcium chloride administration in a patient with supraventricular tachycardia. Ann Emerg Med 1995;25:416-419.
71. Iseri LT, French JH. Magnesium: nature's physiologic calcium blocker. Am Heart J 1984;108:188-193.
72. White RE, Hartzell HC. Effects of intracellular free magnesium on calcium current in isolated cardiac myocytes. Science 1988;239:778-780.
73. Woods KL, Fletcher S, Roffe C, Haider Y. Intravenous magnesium sulphate in suspected acute myocardial
infarction: results of the second Leicester Intravenous Magnesium Intervention Trial (LIMIT-2). Lancet 1992;339:1553-1558.
74. Rasmussen HS, Thomsen PEB. The electrophysiological effects of intravenous magnesium on human sinus node, atrioventricular node, atrium, and ventricle. Clin Cardiol 1989;12:85-90.
75. DiCarlo LA Jr, Morady F, de Buitlier M, Krol RB, Schurig L, Annesley TM. Effects of magnesium sulfate on cardiac conduction and refractoriness in humans. J Am Coll Cardiol 1986;7:1356-1362.
76. Arsenian MA. Magnesium and cardiovascular disease. Prog Cardiovasc Dis 1993;35:271-310.
77. Kulick DL, Hong R, Ryzen E, Rude RK, Rubin JN, Elkayam U, Rahimtoola SH, Bhandari AK. Electrophysiological effects of intravenous magnesium in patients with normal conduction systems and no clinical evidence of significant heart disease. Am Heart J 1988;115:367-373.
78. Stanbury JB. The blocking action of magnesium ion on sympathetic ganglia. J Pharmacol Exp Ther 1948;93:52-62.
79. Von Euler US, Lishajko F. Effects of Mg++ and Ca++ on norepinephrine release and uptake in adrenergic nerve granules in different media. Acta Physiol Scand 1973;89:415-422.
80. James MFM, Beer RE, Esser JD. Intravenous magnesium sulfate inhibits catecholamine release associated with tracheal intubation. Anesth Analg 1989;68:772-776.
81. Leppert J, Myrdal U, Hedner T, Edvinsson L, Tracz Z, Ringqvist I. Magnesium sulphate increases plasma noradrenaline and neuropeptide-Y-like immunoreactivity. Lancet 1995;346:1307-1308.
82. Somjen GG, Baskerville EN. Effect of excess magnesium on vagal inhibition and acetylcholine sensitivity of the mammalian heart in situ and in vitro. Nature 1968;217:679-680.
83. Lin Y, Matin K, Lee T, Lee C. Inotropism of magnesium. Anesthesiology 1991;75 (suppl 3A);A374.
84. Connolly E, Worthley LIG. Intravenous magnesium. Critical Care and Resuscitation 1999;1:162-172.
85. Iseri LT, Freed J, Bures AR. Magnesium deficiency and cardiac disorders. Am J Med 1975;58:837-846.
86. Rasmussen HS, Norregard P, Lindeneg O, McNair P, Backer V, Balslev S. Intravenous magnesium in acute myocardial infarction. Lancet 1986;i:234-236.
87. Fonseca V, Havard CWH. Electrolyte disturbances and cardiac failure with hypomagnesaemia in anorexia nervosa. Br Med J 1985;291:1680-1682.
88. Vincent JL, Buset M, Dufaye J. Degaute JP, Kahn RJ. Circulatory shock associated with magnesium depletion. Intens Care Med 1982;8:149-152.
89. Turlapaty PDMV, Altura BM. Magnesium deficiency produces spasms of coronary arteries: relationship to aetiology of sudden death ischaemic heart disease. Science 1980;208:198-220.
90. Hanline M. Hypomagnesemia causes coronary artery spasm. JAMA 1985:253:342.
32

Critical Care and Resuscitation 2001; 3: 22-34 J. REDMAN, ET AL
110. Teo KK, Yusuf S, Collins R, Held PH, Peto R. Effects of intravenous magnesium in suspected acute myocardial infarction: overview of randomised trials. Br Med J 1991;303:1499-1503.
91. Rasmussen HS, Aurup P, Hojberg S, Jensen EK, McNair P. Magnesium and acute myocardial infarction. Arch Int Med 1986;146:872-874.
92. Rasmussen HS, McNair P, Goransson L, Balslov S, Larsen OG, Aurup P. Magnesium deficiency in patients with ischaemic heart disease with and without acute myocardial infarction uncovered by an intravenous load test. Arch Intern Med 1988;148:329-332.
111. Casscells W. Magnesium and myocardial infarction. Lancet 1994;343:807-809.
112 . ISIS-4. ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58 050 patients with suspected acute myocardial infarction. Lancet 1995;345:669-685.
93. Boriss MN, Papa L. Magnesium: a discussion of its role in the treatment of ventricular dysrhythmia. Crit Care Med 1988;16:292-293. 113 . Galløe A, Gradual N. Magnesium and myocardial
infarction. Lancet 1994;343:1286-1287. 94. Roden DM. Magnesium treatment of ventricular arrhythmias. Am J Cardiol 1989;63:43G-46G. 114 . Seelig MS, Elin RJ. Reexamination of magnesium
infusions in myocardial infarction. Am J Cardiol 1995;76:172-173.
95. Scechter M, Hod H, Marks N, Behar S, Kaplinsky E, Rabinowitz B. Beneficial effect of magnesium sulphate in acute myocardial infarction. Am J Cardiol 1990;66:271-274.
115 . Redwood S, Leatham E, Huang J, Vazquez J, Bashir Y, Kaski J-C, Camm J. A double blind randomised trial of a 24 hour infusion of magnesium sulphate in unstable angina. J Am Coll Cardiol 1995;(February suppl):421A.
96. Schamroth L. The disorders of cardiac rhythm. Oxford: Blackwell Scientific Publications, 1971.
116. England MR, Gordon G, Salem M, Chernow B. Magnesium administration and dysrhythmias after cardiac surgery. A placebo-controlled, double-blind randomised trial. JAMA 1992;268:2395-2402.
97. Mayer DB, Feld J, Miletich DJ, Albrecht RF. The efficacy of magnesium sulfate in the treatment of halothane epinephrine induced cardiac arrhythmias. Anesthesiology 1985;63:A86.
117. Archbold RA, Zaman AG. Magnesium for atrial fibrillation after coronary artery bypass graft surgery: its role in aetiology and prevention. Critical Care and Resuscitation 2000;2:260-268.
98. Szekely P, Wynne NA. Effects of magnesium on cardiac arrhythmias caused by digitalis. Clin Sci 1951;10:241-246.
99. Seller RH. Role of magnesium in digitalis toxicity. Am Heart J 1971;82:551-556. 118. Koinig H, Wallner T, Marhofer P, Andel H, Hörauf K,
Mayer N. Magnesium sulfate reduces intra- and postoperative analgesic requirements. Anesth Analg 1998;87:206-210.
100. Neff MS, Mendelssohn S, Kim KE, Banach S, Swartz C, Seller RH. Magnesium sulphate in digitalis toxicity. Am J Cardiol 1972;29:377-382.
119. Tramèr MR, Schneider J, Marti R-A, Rifat K. Role of magnesium sulfate in postoperative analgesia. Anesthesiology 1996;84:340-347.
101. Chadda KD, Lichstein E, Gupta P. Hypomagnesemia and refractory cardiac arrhythmia in a non digitalized patient. Am J Cardiol 1973;31:98-100.
120. Millane TA, Camm AJ. Magnesium and the myocardium. Br Heart J 1992;68:441-442.
102. Loeb HS, Pietras RJ, Gunnar RM, Tobin JR Jr. Paroxysmal ventricular fibrillation in two patients with hypomagnesemia. Circulation 1968;37:210-215. 121. French JH, Thomas RG, Siskind AP, et al. Magnesium
therapy in massive digoxin intoxication. Ann Emerg Med 1984;13:562-566.
103. Tzivoni D, Keren A, Cohen AM, Loebel H, Zahavi I, Chenzbraun A, Stern S. Magnesium therapy for torsedes de pointes. Am J Cardiol 1984;53:528-530. 122. Blumberg A, Weidmann P, Ferrari P. Effect of
prolonged bicarbonate administration on plasma potassium in terminal renal failure. Kidney Int 1992;41:369-374.
104. McCord JK, Borzak S, Davis T, Gheorghiade M. Usefulness of intravenous magnesium for multifocal atrial tachycardia in patients with chronic obstructive pulmonary disease. Am J Cardiol 1998;81:91-93. 123. Levitt MA, Sullivan JB, Owens SM, Burnham L, Finley
PR. Amitriptyline plasma protein binding: effect of plasma pH and relevance to clinical overdose. Am J Emerg Med 1986;4:121-125.
105. Iseri LT, Fairshter RD, Hardemann JL, Brodsky MA. Magnesium and potassium therapy in multifocal atrial tachycardia. Am Heart J 1985;110:789-794.
124. Editorial. Sodium bicarbonate and tricyclic-antidepressant poisoning. Lancet 1976;ii:838.
106. Moran JL, Gallagher J, Peake SL, Cunningham DN, Salagaras M, Leppard P. Parenteral magnesium sulphate versus amiodarone in the therapy of atrial tachyarrhythmias: a prospective, randomised study. Crit Care Med 1995;23:1816-1824.
125. Strom J, Madsen PS, Nielsen NN, Sorensen MB. Acute self-poisoning with tricyclic antidepressants in 295 consecutive patients treated in an ICU. Acta Anaesthesiol Scand 1984;28:666-670. 107. Thel MC, Armstrong AL, McNulty SE, Califf RM,
O'Connor CM, for the Duke Internal Medicine Housestaff. Randomised trial of magnesium in in-hospital cardiac arrest. Lancet 1997;350:1272-1276.
126. Frommer DA, Kulig KW, Marx JA, Rumack B. Tricyclic antidepressant overdose. A review. JAMA 1987;257:521-526.
127. Guerci AD, Chandra N, Johnson E, Rayburn B, Wurmb E, Tsitlik J, Halperin HR, Siu C, Weisfeldt ML. Failure of sodium bicarbonate to improve resuscitation from
108. Dyckner T, Wester PO. Effect of magnesium on blood pressure. Br Med J 1983;286:1847-1849.
109. Ladusans EJ. Magnesium infusion in acute myocardial infarction. Lancet 1986;i:551.
33

J. REDMAN, ET AL Critical Care and Resuscitation 2001; 3: 22-34
ventricular fibrillation in dogs. Circulation. 1986;74(6 Pt 2):IV75-79.
128. Cooper DJ, Herbertson MJ, Werner HA, Walley KR. Bicarbonate does not increase left ventricular contractility during L-lactic acidemia in pigs. Am Rev Resp Dis 1993;148:317-322.
129. Cooper DJ, Walley KR, Wiggs BR, Russell JA. Bicarbonate does not improve hemodynamics in critically ill patients who have lactic acidosis. Ann Intern Med 1990;112:492-498.
130. Graf H, Arieff AI. The use of sodium bicarbonate in the therapy of organic acidosis. Intens Care Med 1986;12:285-288.
131. Cooper DJ, Worthley LIG. Adverse haemodynamic effects of sodium bicarbonate in metabolic acidosis. Intens Care Med 1987;13:425-427.
132. Telivuo L, Maamies T, Siltanen P, et al. Comparison of alkalinizing agents in resuscitation of the heart after ventricular fibrillation. Ann Chir Gynaecol 1968;57:221-224.
133. Minuck M, Sharma GP. Comparison of THAM and sodium bicarbonate in resuscitation of the heart after ventricular fibrillation in dogs. Anesth Analg 1977;56:38-45.
134. Guidelines 2000 for cardiopulmonary resuscitation and emergency cardiovascular care. International consensus on science. Circulation 2000;102(suppl I):I-1-384.
135. Langer GA. The intrinsic control of myocardial contraction - ionic factors. N Engl J Med 1971;285:1065-1071.
136. Kozeny GA, Murdock DK, Euler DE, Hano JE, Scanlon PJ, Bansal VK, Vertuno LL. In vivo effects of acute changes in osmolality and sodium concentration on myocardial contractility. Am Heart J 1984;109:290-296.
137. Chuck LHS, Refsum H, Rouleau J-L, Mathey D, Sievers RE, Parmley WW. Direct pharmacologic and osmolal
effects of contract media on the mechanics of heart muscle isolated from cats. Am Heart J 1984;108:97-104.
138. Rowe GG, McKenna DH, Corliss RJ, Sialer S. Hemodynamic effects of hypertonic sodium chloride. J Appl Physiol 1972;32:182-184.
139. Kien ND, Kramer GC, White DA. Direct cardiac effect of hypertonic saline in anesthetized dogs. Anesth Analg 1989;68:S147.
140. Waagstein LM, Wennberg E, Waagstein F, Haljamäe H. Hypertonic saline without or with dextran-70 in the treatment of experimental acute myocardial ischemia and reperfusion. Crit Care Med 1999;27:605-616.
141. McCabe JL, Cobaugh DJ, Menegazzi JJ, Fata J. Experimental tricyclic antidepressant toxicity: a randomized, controlled comparison of hypertonic saline solution, sodium bicarbonate, and hyperventilation. Ann Emerg Med 1998;32(3 Pt 1):329-333.
142. Shakibi JG, Aryanpur I, Paydar M, Reyhani F, Siassi B. Antiarrhythmic effect of hypertonic sodium bicarbonate and sodium chloride in ouabain-induced arrhythmias. Jpn Heart J 1976;17:54-60.
143. Scalabrini A, Simonetti Md, Velasco IT, Rocha e Silva M. Hypertonic NaCl solution prevents bupivacaine-induced cardiovascular toxicity. Circ Shock 1992;36:231-237.
144. Venditti FJ, Marotta C, Panezai FR, Oldewurtel HA, Regan TJ. Hypophosphatemia and cardiac arrhythmias. Miner Electrolyte Metab 1987;13:19-25.
145. Ognibene A, Ciniglio R, Greifenstein A, Jarjoura D, Cugino A, Blend D, Whittier F. Ventricular tachycardia in acute myocardial infarction: the role of hypophosphatemia. South Med J 1994;87:65-69.
146. Ritz E. Acute hypophosphataemia. Kidney Int 1982;22:84-94.
34