Embed Size (px)
Citation preview
8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 1/27
1
Aripiprazole
From Wikipedia, the free encyclopedia
Jump to: navigation, search
Aripiprazole
Systematic (IUPAC) name
7-{4-[4-(2,3-dichlorophenyl)piperazin-1-yl]butoxy}-
3,4-dihydroquinolin-2(1H )-one
Identifiers
CAS number 129722-12-9
ATC code N05AX12
PubChem CID 60795
IUPHAR ligand
ID
34
DrugBank APRD00638
ChemSpider 54790
Chemical data
Formula C23H27Cl2N3O2
Mol. mass 448.385
SMILES eMolecules & PubChem
Pharmacokinetic data
Bioavailability 87%

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 2/27

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 3/27
3
In 2007, aripiprazole was approved by the FDA for the treatment of unipolar depression whenused adjunctively with an antidepressant medication.[17] It has not been FDA-approved for use asmonotherapy in unipolar depression.
Autism
In 2009, the United States FDA approved Abilify to treat irritability in persons with autism.[18] Itwas approved on the basis of two studies that showed it reduced aggression towards others, self-injury, quickly changing moods, irritability, and temper tantrums in autistic males and females6±17 years of age.
Cocaine dependency
Perhaps owing to its mechanism of action relating to dopamine receptors, there is some evidenceto suggest that aripiprazole blocks cocaine-seeking behaviour in animal models withoutsignificantly affecting other rewarding behaviours (such as food self-administration). [19]
Pharmacology
Aripiprazole's mechanism of action is different from those of the other FDA-approved atypicalantipsychotics (e.g., clozapine, olanzapine, quetiapine, ziprasidone, and risperidone). Rather thanantagonizing the D2 receptor, aripiprazole acts as a D2 partial agonist.[20][21] Aripiprazole is also apartial agonist at the 5-HT1A receptor, and like the other atypical antipsychotics displays anantagonist profile at the 5-HT2A receptor.[22][23] It also antagonizes the 5-HT77 receptor and actsas a partial agonist at the 5-HT2C receptor, both with high affinity. The latter action may underliethe minimal weight gain seen in the course of therapy.
[24]Aripiprazole has moderate affinity for
histamine and -adrenergic receptors and for the serotonin transporter, and no appreciable
affinity for cholinergic muscarinic receptors.
[25]
D2 and D3 receptor occupancy levels are high, with average levels ranging between ~71% at2 mg/day to ~96% at 40 mg/day.[26][27] Most atypical antipsychotics bind preferentially toextrastriatal receptors, but aripiprazole appears to be less preferential in this regard, as bindingrates are high throughout the brain.[28]
Recently, it has been demonstrated that in 5-HT7 receptor knockout mice, aripiprazole does notreduce immobility time in the forced swim test (FST), and actually increases it.[29][30] Thisimplicates 5-HT7 antagonism as playing a major role in aripiprazole's antidepressant effects,similarly to amisulpride.[29][30][31]
Aripiprazole produces 2,3-dichlorophenylpiperazine (DCPP) as a metabolite similarly to howtrazodone and nefazodone reduce to 3-chlorophenylpiperazine (mCPP) and niaprazine convertsto 4-fluorophenylpiperazine (pFPP).[32] It is unknown whether DCPP contributes to aripiprazole'spharmacology in any way, but the possibility cannot be excluded.
Pharmacokinetics

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 4/27
4
Aripiprazole displays linear kinetics and has an elimination half-life of approximately 75 hours.Steady-state plasma concentrations are achieved in about 14 days. Cmax (maximum plasmaconcentration) is achieved 3±5 hours after oral dosing. Bioavailability of the oral tablets is about90% and the drug undergoes extensive hepatic metabolization (dehydrogenation, hydroxylation,and N-dealkylation), principally by the enzymes CYP2D6 and CYP3A4. Its only known active
metabolite is dehydro-aripiprazole, which typically accumulates to approximately 40% of thearipiprazole concentration. The parenteral drug is excreted only in traces, and its metabolites,active or not, are excreted via feces and urine.[25] When dosed daily, brain concentrations of aripiprazole will increase for a period of 10-14 days, before reaching stable constant levels. Thisphenomenon is due to the long half life of aripiprazole, and is responsible for many of theadverse side effects that appear after multiple days of dosing (whereas the first dose normallydoes not cause these side effects). Aripiprazole possesses very high binding affinity for D2receptors throughout the brain. Although aripiprazole is described as a partial agonist, itsintrinisic affinity is lower than most other partial agonists, thus functioning as an antagonist inmost physiological instances. This is due to the normal presence of dopamine throughout thebrain, which possesses a much higher intrinsic activity for dopamine receptors. Single low doses
of ariprazole will only occupy small amounts of dopamine D2 receptors, which does not causeextrapyramidial symptoms, akathisia, or parkinsonism. However, even if the dose is low,consecutive daily administration will result in accumulation of brain concentrations, therebycausing undesirable side effects in many patients, such as Akathisia, anxiety, restless legsyndrome, and other side effects typical of traditional and atypical antipsychotic medications. Aneven higher risk for unwanted side effects, is present in situations of high-dose daily dosing(10mg and above/per day). Such dosing results in brain concentrations occupying up to 80% of dopamine D2 receptors in most areas of the brain. Common medical knowledge assumes thatdue to the partial agonist properties of aripiprazole, typical D2-blocking side effects will not besignificant. This assumption is incorrect: a partial agonist will always produce agonist effectsweaker than the endogenous full agonist (dopamine), specifically, aripiprazole's intrinsic agonistactivity is so weak, that in nearly all real-life cases, aripiprazole will function solely as anantagonist at dopamine D2 receptors throughout the brain. [33][34][35][36]
Patent status
Otsuka's US patent on aripiprazole expires on October 20, 2014;[37] however, due to a pediatricextension, a generic will not become available until at least April 20, 2015.[3] Barr Laboratories(now Teva Pharmaceuticals) initiated a patent challenge under the Hatch-Waxman Act in March2007.[38] As of 14 August 2009, this challenge is still in court.
Side effects
Akathisia, headache, unusual tiredness or weakness, nausea, vomiting, an uncomfortable feelingin the stomach, constipation, light-headedness, insomnia, sleepiness, shaking, and blurred vision.
Uncontrollable twitching or jerking movements, tremors, seizure, and weight gain. Some peoplemay feel dizzy, especially when getting up from a lying or sitting position, or may experience afast heart rate.

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 5/27
5
Neuroleptic malignant syndrome (Combination of fever, muscle stiffness, faster breathing,sweating, reduced consciousness, and sudden change in blood pressure and heart rate.)
Aripiprazole also causes sexual dysfunction.
Tardive dyskinesia (As with all antipsychotic medication, patients using aripiprazole maydevelop the permanent neurological disorder tardive dyskinesia.[39][40][41])
Stroke (While taking aripiprazole some elderly patients with dementia have suffered from strokeor 'mini' stroke.)
Other elderly patients may experience high blood sugar or the onset or worsening of diabetes.
Allergic reaction (such as swelling in the mouth or throat, itching, rash), increased production of saliva, speech disorder, nervousness, agitation, fainting, reports of abnormal liver test values,inflammation of the pancreas, muscle pain, weakness, stiffness, or cramps.
Overdosage
Children or adults who ingested acute overdoses have usually manifested central nervous systemdepression ranging from mild sedation to coma; serum concentrations of aripiprazole anddehydroaripiprazole in these patients were elevated by up to 3-4 fold over normal therapeuticlevels, yet no deaths have yet been recorded.[42]
Drug interactions
Aripiprazole is a substrate of CYP2D6 and CYP3A4. Coadministration with medications that
inhibit (e.g. paroxetine, fluoxetine) or induce (e.g. carbamazepine) these metabolic enzymes areknown to increase and decrease, respectively, plasma levels of aripiprazole.[43] As such, anyonetaking Abilify should be aware that their dosage of Abilify may need to be decreased.
Aripiprazole may change the subjective effects of alcohol. One study[44] found that aripiprazoleincreased the sedative effect and reduced the sense of euphoria normally associated with alcoholconsumption. However, another alcohol study[45] found that there was no difference in subjectiveeffect between a placebo group and a group taking aripiprazole.
Dosage forms
y Intramuscular injection, solution: 7.5 mg/mL (1.3 mL)
y Solution, oral: 1 mg/mL (150 mL) [contains propylene glycol, sucrose 400 mg/mL, andfructose 200 mg/mL; orange cream flavor]
y Tablet: 2 mg, 5 mg, 10 mg, 15 mg, 20 mg, 30 mgy Tablet, orally disintegrating: 10 mg [contains phenylalanine 1.12 mg; creme de vanilla
flavor]; 15 mg [contains phenylalanine 1.68 mg; creme de vanilla flavor]
Chemistry
8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 6/27
6
Clozapine
From Wikipedia, the free encyclopedia
Jump to: navigation, searchNot to be confused with clonazepam or Klonopin.
Clozapine

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 7/27
7
Systematic (IUPAC) name
8-chloro-11-(4-methylpiperazin-1-yl)-
5H -dibenzo[b,e][1,4]diazepine
IdentifiersCAS number 5786-21-0
ATC code N05AH02
PubChem CID 2818
IUPHAR ligand
ID
38
DrugBank DB00363
ChemSpider 10442628
Chemical data
Formula C18H19ClN4
Mol. mass 326.823 g/mol
SMILES eMolecules & PubChem
Physical data
Melt. point 183 °C (361 °F)
Solubility in
water
0 mg/mL (20 °C)
Pharmacokinetic data
Bioavailability 60 to 70%
Metabolism
Hepatic, by several CYP
isozymes

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 8/27
8
Half-life
6 to 26 hours (mean value 14.2
hours in steady state conditions)
Excretion
80% in metabolized state: 30%
biliary and 50% renal
Therapeutic considerations
Pregnancy cat. B
Legal status
Prescription only, special
restrictions imposed in many
countries
Routes Oral
Clozapine (sold as Clozaril, Azaleptin, Leponex, Fazaclo, Froidir; Denzapine, Zaponex inthe UK; Klozapol in Poland, Clopine in NZ/Aus) is an antipsychotic medication used in thetreatment of schizophrenia. The first of the atypical antipsychotics to be developed, it was firstintroduced in Europe in 1971, but was voluntarily withdrawn by the manufacturer in 1975 after itwas shown to cause agranulocytosis, a condition involving a dangerous decrease in the number of white blood cells, that led to death in some patients. In 1989, after studies demonstrated that itwas more effective than any other antipsychotic for treating schizophrenia, the U.S. Food andDrug Administration (FDA) approved clozapine's use but only for treatment-resistantschizophrenia. The FDA requires blood testing for patients taking clozapine.[1][2] The FDA alsorequires clozapine to carry five black box warnings for agranulocytosis, seizures, myocarditis,for "other adverse cardiovascular and respiratory effects", and for "increased mortality in elderlypatients with dementia-related psychosis."[3] In 2002 the FDA approved clozapine for reducingthe risk of suicidal behavior for patients with schizophrenia.
Clozapine is usually used as a last resort in patients that have not responded to other anti-psychotic treatments due to its danger of causing agranulocytosis as well as the costs of having tohave blood tests continually during treatment. It is, however, one of the very effective anti-psychotic treatment choices.
[4]Patients are monitored weekly for the first six months. If there are
no low counts the patient can be monitored every two weeks for an additional six months.Afterwards, the patient may qualify for every 4 week monitoring.[5]
History
Clozapine was developed by Sandoz in 1961, and introduced in Europe in 1972. In 1975, after reports of agranulocytosis leading to death in some clozapine-treated patients, clozapine wasvoluntarily withdrawn by the manufacturer.[6] Clozapine fell out of favor for more than a decade.However, when studies demonstrated that clozapine was more effective against treatment-resistant schizophrenia than other antipsychotics, the FDA and health authorities in most other countries approved its use only for treatment-resistant schizophrenia, and required regular

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 9/27
9
hematological monitoring to detect granulocytopenia, before agranulocytosis develops. InDecember 2002, clozapine was also approved for reducing the risk of suicide in schizophrenic or schizoaffective patients judged to be at chronic risk for suicidal behavior. In 2005 FDA approvedcriteria to allow reduced blood monitoring frequency.[7]
Indications
Clozapine is used principally in treating treatment-resistant schizophrenia,[8] a term used for thefailure of symptoms to respond satisfactorily to at least two different antipsychotics;[9] It clearlyhas been shown to be more effective in reducing symptoms of schizophrenia than the older typical antipsychotics, with maximal effects in those who have responded poorly to other medication; though the relapse rate is lower and patient acceptability better, this has nottranslated to significant observed benefits in global functioning.[8]
It is also used for reducing the risk of suicide in patients judged to belong to a high-risk groupwith chronic risk for suicidal behavior. Clozapine was shown to prolong the time to suicidal
attempt significantly greater than olanzapine.
Clozapine works well against positive (e.g., delusions, hallucinations) and negative (e.g.emotional and social withdrawal) symptoms of schizophrenia. It has no dyscognitive effect oftenseen with other psychoactive drugs and is even able to increase the capabilities of the patient toreact to this environment and thereby fosters social rehabilitation.
Off-label and investigational drug use
y Treatment of psychosis in L-Dopa-treated patients (25 to 50 mg at bedtime is oftensufficient); this indication is currently approved in Switzerland
y Treatment of psychotic symptoms occurring in patients with dementia of the Lewy-body-type
y Treatment of otherwise resistant acute episodes of maniay Treatment of intractable chronic insomnia, if all other measures have failedy Treatment of schizoid personality disorder
Though much research has been done evaluating the benefit of clozapine in treating theaforementioned conditions, results have been inconclusive regarding its actual efficacy intreating those conditions.
Contraindications
Clozapine is contraindicated in individuals with uncontrolled epilepsy, myeloproliferativedisease, or agranulocytosis with prior clozapine treatment.
Many other (relative) contraindications (e.g. preexisting cardiovascular or liver damage,epilepsy) also exist.
Interactions
8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 10/27
10
Fluvoxamine inhibits the metabolism of clozapine leading to significantly increased blood levelsof clozapine.[10]
Adverse effects
The use of clozapine is associated with side effects, many of which are minor, though some areserious and potentially fatal: the more common include constipation, drooling, muscle stiffness,sedation, tremors, orthostasis, hyperglycemia, and weight gain. The risks of extrapyramidalsymptoms such as tardive dyskinesia are much less with clozapine when compared to the typicalantipsychotics; this may be due to clozapine's anticholinergic effects. Extrapyramidal symptomsmay subside somewhat after a person switches from another antipsychotic to clozapine.[citation
needed ]
Clozapine also carries black box warnings for seizures, myocarditis, and "other adversecardiovascular and respiratory effects." Lowering of the seizure threshold may be dose relatedand slow initial titration of dose may decrease the risk for precipitating seizures. Slow titration of
dosing may also decrease the risk for orthostatic hypotension and other adverse cardiovascular side effects.
Clozapine may have a synergistic effect with the sedating action of other drugs such asbenzodiazepines, and thus respiratory depression may result with concomitant use. Care shouldbe taken, especially if the latter drugs are given parenterally.
Many male patients have experienced ceasure of ejaculation during orgasm as a side effect of Clozapine, though this is not documented in official drug guides[citation needed ].
Agranulocytosis
Clozapine carries a black box warning for drug-induced agranulocytosis. Without monitoring,agranulocytosis occurs in about 1% of patients who take clozapine during the first few months of treatment;[11] the risk of developing it is highest about three months into treatment, and decreasessubstantially thereafter, to less than 0.01% after one year.
[12]Patients who have experienced
agranulocytosis with previous treatment of clozapine should not receive it again.
In 2007, a pharmacogenetic test was introduced to measure the probability of developingagranulocytosis. The test has two gradations - Higher and Lower risk, with a relativeagranulocytosis risk of 2.5 and 0.5 compared to general level. The company states that the test isbased on two SNPs of the HLA-DQB1 gene.
In the USA, patients taking clozapine are required to have a blood cell count every week, for thefirst six months of therapy. After this, they are required to have a blood cell count every other week for the second six months after therapy. After twelve months, blood cell counts need beperformed every four weeks. Patients are advised to inform their doctor if they develop a sorethroat, or fever. If the number of white blood-cells drops notably then referral to a hematologistis undertaken. The manufacturers of both the brand and generic clozapine are required by theFDA to track white blood cells counts for patients receiving clozapine, and pharmacies are

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 11/27
11
required to obtain a copy of the CBC prior to dispensing the medication to the patient. Thepurpose of the monitoring system is to prevent rechallenge with clozapine in patients with ahistory of clozapine-induced agranulocytosis and to detect leukopenic events among patientstaking clozapine. In other countries (e.g. in Europe), restrictions have been eased.
It has been suggested that coadministration of clozapine with an antioxidant such as vitamin C(ascorbic acid) can reduce the risk of agranulocytosis.[13]
Cardiac toxicity
A more recently identified and sometimes fatal side effect is that of myocarditis, which usuallydevelops within the first month of commencement and presents with signs of cardiac failure andcardiac arrhythmias.[14] Cardiomyopathy is another potentially fatal cardiac condition that mayarise less acutely. More recently, a regular six-monthly echocardiogram is also recommended todetect myocarditis.
Gastrointestinal hypomotility
Another underrecognized and potentially life-threatening side effect spectrum is gastrointestinalhypomotility, which may manifest as severe constipation, fecal impaction, paralytic ileus, bowelobstruction, acute megacolon, ischemia or necrosis. Monitoring of bowel function isrecommended, as untreated cases are occasionally fatal.[15]
Hypersalivation
Hypersalivation (drooling or 'wet pillow syndrome') is seen in up to 30% of patients onclozapine. It is a side effect not seen among the other anti-psychotics. While clozapine is a
muscarinic antagonist at the M1, M2, M3, and M5 receptors, clozapine is a full agonist at the M4subset. Because M4 is highly expressed in the salivary gland, its M4 agonist activity is thought tobe responsible for the hypersalivaiton.[16]
Central nervous system
Drowsiness, vertigo, headache, tremor, syncope, sleep disturbances, nightmares, restlessness,akinesia, agitation, seizures, rigidity, akathisia, confusion, fatigue, insomnia, hyperkinesia,weakness, lethargy, ataxia, slurred speech, depression, myoclonic Jerks, anxiety. Rarelydelusions, hallucinations, delirium, amnesia, libido increase or decrease, paranoia and irritability,abnormal EEG, worsening of psychosis, paresthesia, status epilepticus, and obsessive
compulsive symptoms.
[17]
Withdrawal effects
Abrupt withdrawal may lead to cholinergic rebound effects, severe movement disorders as wellas severe psychotic decompensation. It has been recommended that patients, families, andcaregivers are aware of the symptoms and risks of abrupt withdrawal of clozapine. When
8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 12/27
12
discontinuing clozapine, gradual dose reduction is recommended to reduce the intensity of withdrawal effects.[18][19]
Weight gain and diabetes
The FDA requires the manufacturers of all atypical antipsychotics to include a warning about therisk of hyperglycemia and diabetes with these medications. Indeed, there are case reports of clozapine-induced hyperglycemia and diabetes. In addition, there are also case reports of clozapine-induced diabetic ketoacidosis. There is data showing that clozapine can decreaseinsulin sensitivity. Clozapine should be used with caution in patients who are diagnosed withdiabetes or in patients at risk for developing diabetes. All patients receiving clozapine shouldhave their fasting blood glucose monitored.
In addition to hyperglycemia, significant weight gain is frequently experienced by patientstreated with clozapine.[20] Impaired glucose metabolism and obesity have been shown to beconstituents of the metabolic syndrome and may increase the risk of cardiovascular disease. The
data suggest that clozapine may be more likely to cause adverse metabolic effects than some of the other atypical antipsychotics.[21] Research has indicated that clozapine may cause adeficiency of selenium.[22]
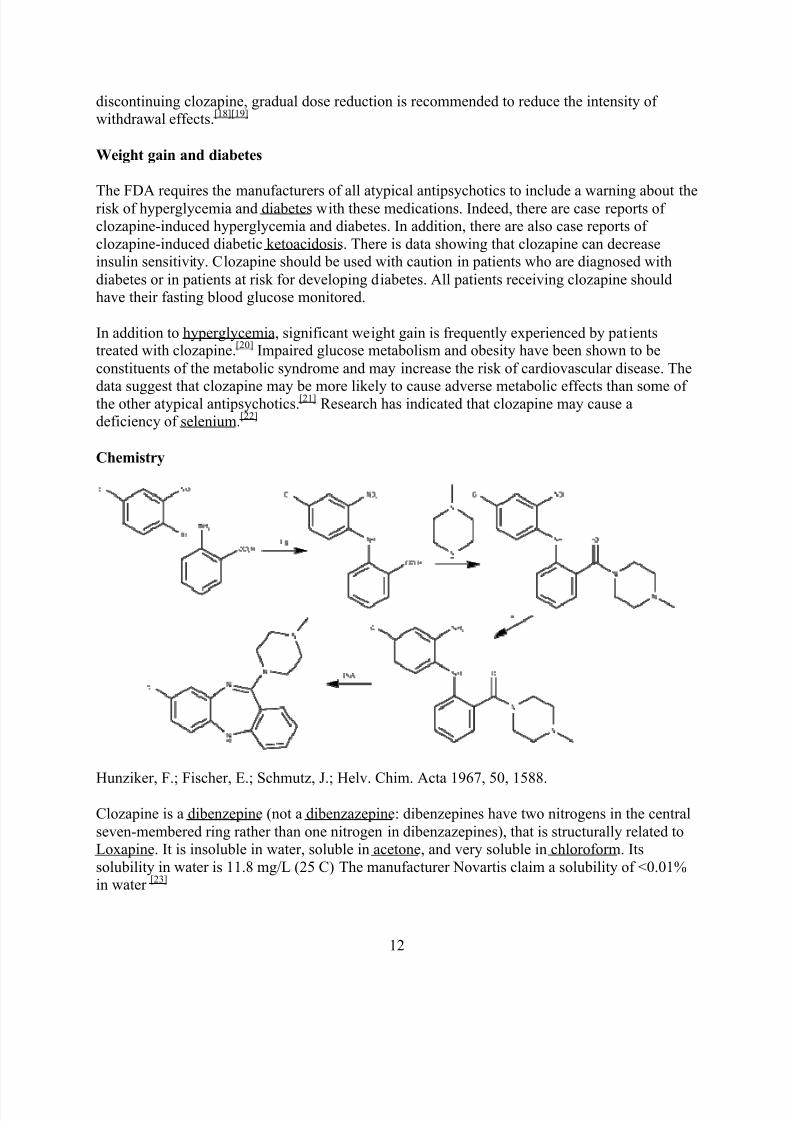
Chemistry
Hunziker, F.; Fischer, E.; Schmutz, J.; Helv. Chim. Acta 1967, 50, 1588.
Clozapine is a dibenzepine (not a dibenzazepine: dibenzepines have two nitrogens in the centralseven-membered ring rather than one nitrogen in dibenzazepines), that is structurally related toLoxapine. It is insoluble in water, soluble in acetone, and very soluble in chloroform. Itssolubility in water is 11.8 mg/L (25 C) The manufacturer Novartis claim a solubility of <0.01%in water [23]
8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 13/27
13
Mechanism of action
Clozapine is classified as an atypical antipsychotic drug because its profile of binding toserotonergic as well as dopamine receptors;[24] its effects on various dopamine mediatedbehaviors also differ from those exhibited by more typical antipsychotics. In particular, clozapine
interferes to a lower extent with the binding of dopamine at [[D1]], [[D2]], [[D3]] and [[D5]]receptors, and has a high affinity for the [[D4 receptor]], but it does not induce catalepsy nor inhibit apomorphine-induced stereotypy in animal models as is seen with 'conventional'neuroleptics. This evidence suggests clozapine is preferentially more active at limbic than atstriatal dopamine receptors and may explain the relative freedom of clozapine fromextrapyramidal side effects together with strong anticholinergic activity.
Several metabolites of Clozapine exhibit binding profiles similar to Clozapine. N-Desmethylclozapine may contribute significantly to the atypical effects of Clozapine treatment.N-desmethylclozapine acts a an agonist and/or partial agonist at D2, D3, -opioid, M1, M2, M3,M4, M5 receptors, and an antagonist/inverse agonist at 5-HT2A and 5-HT2C receptors.
Clozapine is also a partial agonist at the 5-HT1A receptor, putatively improving depression,anxiety, and the negative cognitive symptoms.[citation needed ]
Clozapine also is a strong antagonist at different subtypes of adrenergic, cholinergic andhistaminergic receptors, the last two being predominantly responsible for its side effect profile.
It has approximately the same potency as chlorpromazine.[clarification needed ]
Pharmacokinetics
The absorption of clozapine is almost complete, but the oral bioavailability is only 60 to 70%due to first-pass metabolism. The time to peak concentration after oral dosing is about 2.5 hours,and food does not appear to affect the bioavailability of clozapine. The elimination half-life of clozapine is about 14 hours at steady state conditions (varying with daily dose).
Clozapine is extensively metabolized in the liver, via the cytochrome P450 system, to polar metabolites suitable for elimination in the urine and faeces. The major metabolite, norclozapine (desmethyl-clozapine), is pharmacologically active. The cytochrome P450 isoenzyme 1A2 isprimarily responsible for clozapine metabolism, but 2C, 2D6, 2E1 and 3A3/4 appear to playroles as well. Agents that induce (e.g., cigarette smoke) or inhibit (e.g., theophylline,ciprofloxacin, fluvoxamine) CYP1A2 may increase or decrease, respectively, the metabolism of
clozapine. For example, the induction of metabolism caused by smoking means that smokersrequire up to double the dose of clozapine compared with non-smokers to achieve an equivalentplasma concentration.[25]
Clozapine and norclozapine plasma levels may also be monitored, though they show a significantdegree of variation and are higher in women and increase with age.[26]. Monitoring of plasmalevels of clozapine and norclozapine has been shown to be useful in assessment of compliance,metabolic status, prevention of toxicity, and in dose optimization.[25]
8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 14/27
14
Dosage
Due to risk of serious side effects, clozapine treatment is commenced at a very low dose andincreased slowly until a therapeutic dose is reached.[27][28] In severely ill and/or younger patientshigher doses may be needed, while in the elderly much lower doses may be sufficient. Once the
patient is stabilized and the maintenance dose has been determined, the greater part or all of thedaily dose may be given at bedtime.[28] This will ameliorate daytime sedation and orthostaticproblems; most people benefit from the sedation to get to sleep anyway. Furthermore,compliance on medication taken more frequently than once daily drops off dramatically.
Norclozapine - the primary metabolite of clozapine, which accumulates to, on average, 70% or so of the clozapine concentration in plasma at steady-state (their sample, i.e., pre-dose, ideally inthe morning). However, there is substantial variation in the clozapine:norclozapine concentrationratio between individuals.
A steady-state plasma clozapine concentration of 0.35 to 0.6 mg/L (NB. - quoted values may
vary slightly) should produce a clinical response in most patients.
Risperidone
From Wikipedia, the free encyclopedia
Jump to: navigation, search
Risperidone
Systematic (IUPAC) name
4-[2-[4-(6-fluorobenzo[d ]isoxazol-3-yl)-

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 15/27
15
1-piperidyl]ethyl]-3-methyl-
2,6-diazabicyclo[4.4.0]deca-1,3-dien-5-one
Identifiers
CAS number 106266-06-2
ATC code N05AX08
PubChem CID 5073
IUPHAR ligand
ID
96
DrugBank DB00734
ChemSpider 4895
Chemical data
Formula C23H27FN4O2
Mol. mass 410.485 g/mol
SMILES eMolecules & PubChem
Pharmacokinetic data
Bioavailability 70% (oral)
Metabolism Hepatic (CYP2D6-mediated)
Half-life 3±20 hours
Excretion
Urinary
Therapeutic considerations
Pregnancy cat. C
Legal status
Prescription only
Routes
Oral and extended-release
intramuscular injection
Risperidone (pronounced Ris-PEAR-r-dne) is an atypical antipsychotic used to treatschizophrenia (including adolescent schizophrenia), schizoaffective disorder, the mixed andmanic states associated with bipolar disorder, and irritability in children with autism. The drugwas developed by Janssen-Cilag and first released in 1994[1]. It is sold under the trade nameRisperdal in the Netherlands, United States, Canada, Australia, United Kingdom, Portugal,Spain, Turkey, New Zealand and several other countries, Risperdal or Ridal in New Zealand,Sizodon or Riscalin in India, Rispolept in Eastern Europe, and Russia, and Belivon, or Rispen elsewhere.

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 16/27
16
Indications and Uses
y treatment of schizophrenia in adultsy treatment of schizophrenia in adolescents aged 13-17 yearsy alone or in combination with lithium or valproate, for the short-term treatment of acute
manic or mixed episodes associated with Bipolar I Disorder in adultsy alone in the short-term treatment of acute manic or mixed episodes associated with
Bipolar I Disorder in children and adolescents aged 10-17 yearsy treatment of irritability associated with autistic disorder in children and young adultsy it has also been used as a control drug for people with tourette syndrome and other tic
disorders.y treatment of major depression with psychotic features
Risperidone was approved by the United States Food and Drug Administration (FDA) in 1993for the treatment of schizophrenia.[2]
On August 22, 2007, risperidone was approved as the only drug agent available for treatment of schizophrenia in youth ages 13±17; it was also approved that same day for treatment of bipolar disorder in youth and children ages 10±17, joining lithium. Risperidone contains the functionalgroups of benzisoxazole and piperidine as part of its molecular structure. In 2003 the FDAapproved risperidone for the short-term treatment of the mixed and manic states associated withbipolar disorder. In 2006 the FDA approved risperidone for the treatment of irritability inchildren and adolescents with autism.[3] The FDA's decision was based in part on a study of autistic children with severe and enduring problems of violent meltdowns, aggression, and self-injury; risperidone is not recommended for autistic children with mild aggression and explosivebehavior without an enduring pattern.[4] Like other atypical antipsychotics, risperidone has alsobeen used off-label for the treatment of anxiety disorders, such as obsessive-compulsive
disorder; severe, treatment-resistant depression with or without psychotic features; tourettesyndrome; disruptive behavior disorders in children; and eating disorders, among others. In twosmall studies risperidone was reported to successfully treat the symptoms of phencyclidine (PCP)psychosis due to acute intoxication[5] and chronic use.[6]
A 2009 Cochrane Library review found no evidence from randomized controlled trials thatrisperidone is effective for the treatment of attention-deficit hyperactivity disorder (ADHD) inpeople with intellectual disabilities.[7] A multi-year UK study by the Alzheimer's Research Trustsuggested that this and other neuroleptic anti-psychotic drugs commonly given to Alzheimer'spatients with mild behavioural problems often made their condition worse. The study concludedthat:
³ For most patients with AD, withdrawal of neuroleptics had no overall detrimental effecton functional and cognitive status and by some measures improved functional andcognitive status. Neuroleptics may have some value in the maintenance treatment of moresevere neuropsychiatric symptoms, but this possibility must be weighed against theunwanted effects of therapy.
[8] ´
Availability

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 17/27
17
Risperdal 4 mg tablets (UK)
Janssen's patent on Risperdal expired on December 29, 2003, opening the market for cheaper generic versions of the drug from other companies, and Janssen's exclusive marketing rightsexpired on June 29, 2004 (the result of a pediatric extension.)
Risperidone is available as a tablet in 0.25, 0.5, 1, 2, 3 and 4 mg sizes, as an oral solution (30ml,1 mg/ml), and as a 12.5 mg, 25 mg, 37.5 mg and 50 mg ampoule Risperdal Consta, which is adepot injection administered once every two weeks. It is also available as a wafer known in theUnited States and Canada as Risperdal M-Tabs and elsewhere as Risperdal Quicklets.
Risperidone became available as a generic drug in October 2008 from Teva Pharmaceuticals, Dr.Reddy's Laboratories, Inc. and Patriot Pharmaceutics. The Patriot generic is JanssenPharmaceutical's "authorized generic pharmaceutical."
Side effects
Risperidone has been associated with weight gain.[9] Other common side effects includeakathisia, sedation, dysphoria, insomnia, sexual dysfunction, low blood pressure, high bloodpressure, muscle stiffness, muscle pain, tremors, increased salivation, constipation, and stuffynose.
Many antipsychotics are known to cause hyperprolactinemia which may lead to hypogonadism-induced osteoporosis, galactorrhoea, gynaecomastia, irregular menstruation and sexualdysfunction. However, risperidone is known to increase prolactin to a greater extent than other atypical antipsychotics. Although lactation is possible in both sexes using other antipsychoticdrugs, risperidone is the biggest offender.[10][11] There is a higher association between pituitaryneoplasms with use of risperidone and amisulpride than with other antipsychotic agents.[12] It isthought that once risperidone raises prolactin, it may cause prolactinoma, a benign tumor of the

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 18/27
18
pituitary gland. Tumors, in general, are not considered reversible. Medical therapy may helpreduce tumor size and restore normal reproduction and pituitary function, however, dopamineagonists are not likely to be prescribed to antipsychotic users, thus, surgery or radiation treatmentmay be required. This condition may recur if the patient is switched to a different antipsychotic.Risperidone has been known to cause increased thoughts of suicide.[13]
Risperidone can potentially cause tardive dyskinesia (TD),[14] extrapyramidal symptoms(EPS),[14] and neuroleptic malignant syndrome (NMS).[14] Risperidone may also trigger diabetesand more serious conditions of glucose metabolism, including ketoacidosis and hyperosmolar coma, according to an FDA Warning Letter issued to Janssen Pharmaceutica, Inc. on 19-Apr-04.[15]
Pharmacology
This drug belongs to a class of antipsychotic drugs known as atypical antipsychotics that havemore pronounced serotonin antagonism than dopamine antagonism, but risperidone is unique in
this class because it retains dopamine antagonism. It has high affinity for D2 dopaminergicreceptors. It has actions at several 5-HT (serotonin) receptor subtypes. These are 5-HT2C, linkedto weight gain, 5-HT2A,linked to its antipsychotic action and relief of some of the extrapyramidalside effects (EPS) experienced with the typical neuroleptics.
It reaches peak plasma levels quickly regardless of whether it is administered as a liquid or pill.Risperidone is metabolised fairly quickly, so the potential for nausea subsides usually in two tothree hours. However, the active metabolite, 9-hydroxy-risperidone, which has similar pharmacodynamics to risperidone, lingers in the body for much longer, and has been developedas an antipsychotic in its own right, called paliperidone.
An intramuscular preparation, marketed as Risperdal Consta, can be given once every twoweeks. It is slowly released from the injection site. This method of administration may be usedon sanctioned patients who are declining, or consenting patients who may have disorganizedthinking and cannot remember to take their daily doses.[16] Doses range from 12.5 to 50 mg givenas an intramuscular injection once every two weeks.
Olanzapine
From Wikipedia, the free encyclopedia
Jump to: navigation, search
Olanzapine
8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 19/27
19
Systematic (IUPAC) name
2-methyl -4-(4-methyl -1-piperazinyl)-
10H-thieno[ 2,3-b][ 1,5]benzodiazepine
Identifiers
CAS number 132539-06-1
ATC code N05AH03
PubChem CID 4585
IUPHAR ligand
ID
47
DrugBank DB00334
ChemSpider 10442212
Chemical data

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 20/27
20
Formula C17H20N4S
Mol. mass 312.439
SMILES
eMolecules & PubChem
Physical data
Melt. point 195 °C (383 °F)
Solubility in
water
Practically insoluble in
water mg/mL (20 °C)
Pharmacokinetic data
Bioavailability 87% [1]
Metabolism
Hepatic (direct glucuronidation and
CYP mediated oxidation)
Half-life 21±54 hours
Excretion urine 57%, feces 30%
Therapeutic considerations
Pregnancy cat. C
Legal status
Prescription only
Routes oral, intramuscular

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 21/27
21
Zyprexa 10 mg tablets (AU)
Olanzapine (trade names Zyprexa, Zalasta, Zolafren, Olzapin, Rexapin, Zypadhera or incombination with fluoxetine Symbyax) is an atypical antipsychotic, approved by the FDA for the treatment of schizophrenia and bipolar disorder.[2] The olanzapine formulations aremanufactured and marketed by the pharmaceutical company Eli Lilly and Company, whosepatent for olanzapine proper expires in 2011 (in October 2009 a Canadian judge ruled that the1991 patent was invalid).[3] Sales of Zyprexa in 2008 were $2.2B in the US alone, and $4.7B intotal.[4]
Indications and Usage
y oral formulation: acute and maintenance treatment of Schizophrenia in adults, acutetreatment of manic or mixed episodes associated with Bipolar I Disorder (monotherapyand in combination with lithium or valproate)
y intramuscular formulation: acute agitation associated with Schizophrenia and Bipolar IMania in adults
y oral formulation combined with fluoxetine: acute treatment of depressive episodesassociated with Bipolar I Disorder in adults, or acute treatment of treatment resistantdepression in adults [5]
Known FDA approvals are as follows:
y approved for the treat ment of the manifestations of psychotic disorders on September 6,1996
[6]
y approved in combination with fluoxetine for the treat ment of depressive episodesassociated with Bipolar disorder on December 24, 2003
[7]
y approved for the long -ter m treat ment of bipolar I disorder on January 14, 2004[8]

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 22/27
22
y approved in combination with fluoxetine for treatment resistant depression on March 19,2009.[9]
Off-label uses
Case-reports, open-label, and small pilot studies suggest efficacy of olanzapine for the treatmentof some anxiety spectrum disorders (e.g. generalized anxiety disorder,[10] panic disorder,[11] post-traumatic stress disorder );[12] however, olanzapine has not been rigorously evaluated inrandomized, placebo-controlled trials for this use and is not FDA approved for these indications.Other common off-label uses of olanzapine include the treatment of eating disorders (e.g.anorexia nervosa) and as an adjunctive treatment for major depressive disorder without psychoticfeatures. It has also been used for Tourette syndrome and stuttering.
[13]Olanzapine is also used in
many addiction clinics as a sleep aid (usually 2.5±5 mg) due to its low abuse profile and zeroaddictive properties.[14]
Prevention of psychosis
Olanzapine has been considered as part of an early psychosis approach for schizophrenia. ThePrevention through Risk Identification, Management, and Education (PRIME) study, funded bythe National Institute of Mental Health and Eli Lilly, tested the hypothesis that olanzapine mightprevent the onset of psychosis in people at very high risk for schizophrenia. The study examined60 patients with prodromal schizophrenia, who were at an estimated risk of 36±54% of developing schizophrenia within a year, and treated half with olanzapine and half withplacebo.
[15]In this study, patients receiving olanzapine had a lower risk of progressing to
psychosis, although the difference did not reach statistical significance. Olanzapine was effectivefor treating the prodromal symptoms, but was associated with significant weight gain.[16]
Use in elderly
Citing an increased risk of stroke, in 2004 the Committee on the Safety of Medicines (CSM) inthe UK issued a warning that olanzapine and risperidone, both atypical antipsychoticmedications, should not be given to elderly patients with dementia. In the U.S., olanzapinecomes with a black box warning for increased risk of death in elderly patients. It is not approvedfor use in patients with dementia-related psychosis.[17] However, a BBC investigation in June2008 found that this advice was being widely ignored by British doctors.[18]
Dosage and administration
Olanzapine is available as a tablet in strengths of 2.5 mg, 5 mg, 7.5 mg, 10 mg, 15 mg and20 mg. It also comes as an orally disintegrating wafer (known as Zydis), which dissolves on thetongue, in strengths of 5 mg, 10 mg, 15 mg and 20 mg. It is also available as a 10 mg vial for arapid-acting intramuscular injection for short-term acute use.
Dose may be adjusted depending on the person' response to the drug. The dose also will dependon certain medical problems the person may have. It is generally recommended to be taken once

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 23/27
23
daily before bed as it is highly sedating. However, sedation tends to diminish as treatment ispursued.
Pharmacology
Olanzapine is structurally similar to clozapine, but is classified as a thienobenzodiazepine.Olanzapine has a higher affinity for 5-HT2 serotonin receptors than D2 dopamine receptors.
Like most atypical antipsychotics, compared to the older typical ones, olanzapine has a lower affinity for histamine, cholinergic muscarinic and alpha adrenergic receptors. Olanzapine alsoexhibits weak affinity for GABAA, BZD receptor site[19] which may contribute slightly to itssedating properties.[20] The mode of action of olanzapine's antipsychotic activity is unknown. Itmay involve antagonism at serotonin receptors. Antagonism of dopamine receptors is associatedwith extrapyramidal effects such as tardive dyskinesia, and with therapeutic effects.Antagonizing H1 histamine receptors causes sedation and may cause weight gain, althoughantagonistic actions at 5-HT2C receptors have also been implicated in weight gain.
Metabolism
Olanzapine is metabolized by the cytochrome P450 system isoenzymes 1A2 and 2D6 (minor pathway). Drug metabolism may be decreased or increased by agents that induce (e.g. cigarettesmoke) or inhibit (e.g. fluvoxamine or ciprofloxacin) CYP1A2 activity respectively.
Side effects, adverse reactions
as with all neuroleptic drugs, olanzapine can cause tardive dyskinesia and rare, but life-
threatening, neuroleptic malignant syndrome.
Other recognised side effects may include:
y Restlessnessy akathisia inability to remain still[21] y dry mouthy dizzinessy irritabilityy sedationy insomnia
y constipationy urinary retentiony orthostatic hypotensiony weight gainy increased appetitey runny nosey low blood pressurey impaired judgment, thinking, and motor skills

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 24/27
24
y impaired spatial orientationy impaired responses to sensesy seizurey trouble swallowingy dental problems and discoloration of teethy
missed periodsy problems with keeping body temperature regulatedy apathy, lack of emotiony Endocrine side effects have included hyperprolactinemia, hyperglycemia, and diabetes
mellitusy Hyperprolactinemia causing sexual dysfunction, menstrual irregularities, and
osteoporosis
Metabolic effects
The Food and Drug Administration requires all atypical antipsychotics to include a warning
about the risk of developing hyperglycemia and diabetes, both of which are factors in themetabolic syndrome. These effects may be related to the drugs' ability to induce weight gain,although there are some reports of metabolic changes in the absence of weight gain.[citation needed ] Of all the atypical antipsychotics, olanzapine is one of the most likely to induce weight gainbased on various measures.[22][23][24][25] The effect is not dose dependent. [dubious ± discuss] Olanzapine may directly affect adipocyte function, promoting fat deposition.[26] There are somecase reports of olanzapine-induced diabetic ketoacidosis.[27] Olanzapine may decrease insulinsensitivity[28] though one 3-week study seems to refute this.[29] It may also increase triglyceridelevels.[23]
Despite weight gain, a large multi-center randomized National Institute of Mental Health study
found that olanzapine was better at controlling symptoms because patients were more likely toremain on olanzapine than the other drugs.[30] One small, open-label, non-randomized studysuggest that taking olanzapine by orally dissolving tablets may induce less weight gain,[31] butthis has not been substantiated in a blinded experimental setting.
Animal Toxicology
In a placebo-compared study of six Macaque monkeys receiving olanzapine between 17 and 27months, a significant brain volume and weight decreases (8-11%) were detected.
[32]In latter
studies of the stored samples, the changes were attributed to astrocyte and oligodendrocyteloss,[33] with the neurons spared but positioned more closely compared to the controls. [clarification
needed ] However according to this study the neurons does not seem to be completeley spared. Thegray matter shrinking found was 14.6%, but the neuron density increase was only 10.2% whichcorresponds to approximately a loss of 5% of the neurons.[citation needed ]
Olanzapine has demonstrated carcinogenic effects in multiple studies when exposed chronicallyto female mice and rats, but not male mice and rats. The tumors found were in either the liver or mammary glands of the animals.[34]
8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 25/27
25
Overdose
Symptoms of an overdose include tachycardia, agitation, dysarthria, decreased consciousnessand coma. Death has been reported after an acute overdose of 450 mg, but also survival after anacute overdose of 1500 mg.[35] There is no known specific antidote for olanzapine overdose, and
even physicians are recommended to call a certified poison control center for information on thetreatment of such a case.[35]
Controversy, lawsuits and settlements
Further information: Eli Lilly Controversy
According to a N ew York Times article published on December 17, 2006,[36] "Eli Lilly hasengaged in a decade-long effort to play down the health risks of Zyprexa, its best-sellingmedication for schizophrenia, according to hundreds of internal Lilly documents and e-mailmessages among top company managers", most of which had been disclosed as the result of
lawsuits by individuals who had taken the drug against the company though some had beenstolen.[37] These had been sent to a number of journalists by a lawyer advocate for individualswith a psychiatric diagnosis opposed to forced psychiatric treatment. Eli Lilly filed a protectionorder to stop the dissemination of certain Eli Lilly documents about Zyprexa which they, and thejudge, believed to be confidential and "not generally appropriate for public consumption".[37] Temporary injunctions required those who had been received the documents to return them andthat the documents be removed from websites which had posted them.[38] In his final judgement,Judge Weinstein issued a permanent judgement against further dissemination of the documentsand requiring their return by a number of parties named by Lilly.[37] These health risks include anincreased risk for diabetes through Zyprexa's links to obesity and its tendency to raise bloodsugar. Zyprexa is Lilly¶s top-selling drug, with sales of $4.2 billion last year.
The documents, given to The N ew York Times by Jim Gottstein, show that Lilly executives keptimportant information from doctors about Zyprexa¶s links to obesity and its tendency to raiseblood sugar ² both known risk factors for diabetes. The Times of London also obtained copiesof the documents and reported that as early as October 1998, Lilly considered the risk of drug-induced obesity to be a "top threat" to Zyprexa sales.[39] In another document, dated October 9,2000, senior Lilly research physician Robert Baker noted that an academic advisory board hebelonged to was "quite impressed by the magnitude of weight gain on olanzapine andimplications for glucose."[39]
Lilly¶s own published data, which it told its sales representatives to play down in conversations
with doctors, has shown that 30 percent of patients taking Zyprexa gain 22 pounds or more after a year on the drug, another study showed 16% of Zyprexa patients gained at least 30 kg (66pounds) in one year, and some patients have reported gaining 100 pounds or more. But Lilly wasconcerned that Zyprexa¶s sales would be hurt if the company was more forthright about the factthat the drug might cause unmanageable weight gain or diabetes, according to the documents,which cover the period 1995 to 2004. In 2006, Lilly paid $700 million to settle 8,000 lawsuitsfrom people who said they had developed diabetes or other diseases after taking Zyprexa.Thousands more suits are still pending.[40]

8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 26/27
26
In 2002, British and Japanese regulatory agencies warned that Zyprexa may be linked todiabetes, but even after the FDA issued a similar warning in 2003, Lilly did not publicly disclosetheir own findings.
Eli Lilly agreed on January 4, 2007 to pay up to $500 million to settle 18,000 lawsuits from
people who claimed they developed diabetes or other diseases after taking Zyprexa. Includingearlier settlements over Zyprexa, Lilly has now agreed to pay at least $1.2 billion to 28,500people who claim they were injured by the drug. At least 1,200 suits are still pending, thecompany said. About 20 million people worldwide have taken Zyprexa since its introduction in1996.[41] On January 8, 2007, Judge Jack B. Weinstein refused the Electronic Frontier Foundation's motion to stay his order.[42]
On January 15, 2009 Eli Lilly plead guilty to a misdemeanor charge of illegally marketingZyprexa for off-label use, and agreed to pay $1.4 billion.[43] Although Lilly had evidence that itis not effective for dementia, Zyprexa was marketed for elderly Alzheimer's patients.[44] The drugcarries an F.D.A. warning that it increases the risk of death in older patients with dementia-
related psychosis.
[45]
In order to make up for the costs for settling the lawsuits and shrinking sales figures for Zyprexain the U.S.A. the company increased the prices for this medication in Germany in May 2007 by18 percent. [46][47]
Chemistry
8/7/2019 anti psychotics odt's
http://slidepdf.com/reader/full/anti-psychotics-odts 27/27
V V V ...S S S ...M M M ...DDDE E E E E E P P P AAAK K K
















![Developmental disabilities [Read-Only] - Community Networks · 10/11/2012 2 Medications Ritalin Atypical anti-psychotics Mood stabilizers SSRIs Benzodiazepines Anti Convulsants Typical](https://img.pdfslide.us/doc/110x75/5d5b30b988c993b8138bc411/developmental-disabilities-read-only-community-10112012-2-medications.jpg)