Embed Size (px)
Citation preview
Shari Siying Li
PGY-2 UBC Emergency Medicine
ANTI-NMDA ENCEPHALITIS What is it?
- An autoimmune encephalitis with autoantibodies targeting CNS NMDA receptors - Discovered in 2007, now recognized as the most common non-viral cause of encephalitis
What does it look like?
- Patients mostly female (~80%), median age ~20yo o Range includes males and females from infants to elderly patients (rare) o About half of women of childbearing age have associated ovarian teratoma
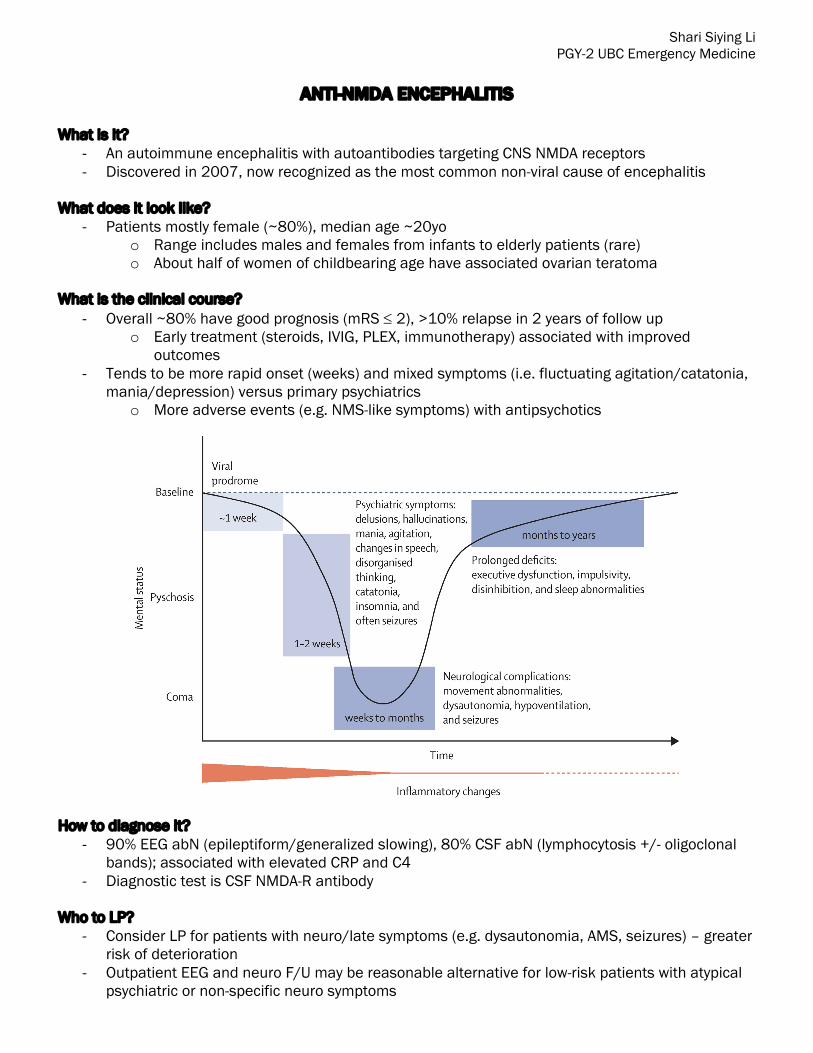
What is the clinical course?
- Overall ~80% have good prognosis (mRS £ 2), >10% relapse in 2 years of follow up o Early treatment (steroids, IVIG, PLEX, immunotherapy) associated with improved
outcomes - Tends to be more rapid onset (weeks) and mixed symptoms (i.e. fluctuating agitation/catatonia,
mania/depression) versus primary psychiatrics o More adverse events (e.g. NMS-like symptoms) with antipsychotics
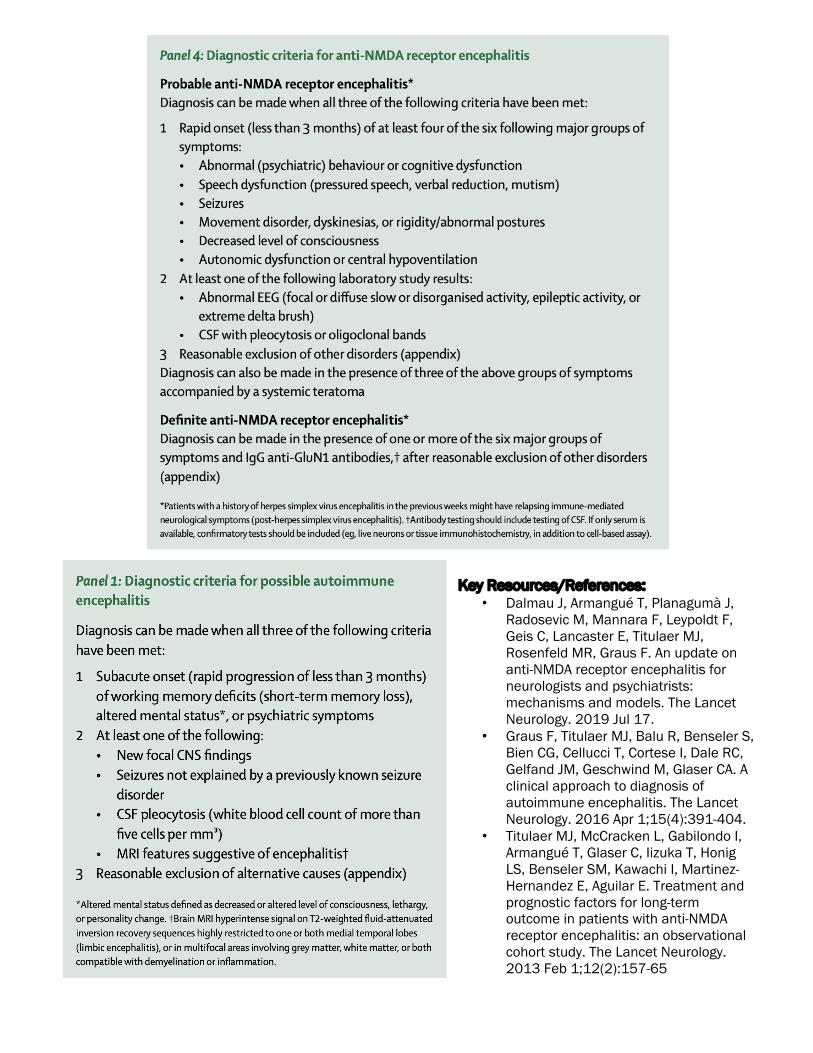
How to diagnose it?
- 90% EEG abN (epileptiform/generalized slowing), 80% CSF abN (lymphocytosis +/- oligoclonal bands); associated with elevated CRP and C4
- Diagnostic test is CSF NMDA-R antibody Who to LP?
- Consider LP for patients with neuro/late symptoms (e.g. dysautonomia, AMS, seizures) – greater risk of deterioration
- Outpatient EEG and neuro F/U may be reasonable alternative for low-risk patients with atypical psychiatric or non-specific neuro symptoms
Key Resources/References:
• Dalmau J, Armangué T, Planagumà J, Radosevic M, Mannara F, Leypoldt F, Geis C, Lancaster E, Titulaer MJ, Rosenfeld MR, Graus F. An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models. The Lancet Neurology. 2019 Jul 17.
• Graus F, Titulaer MJ, Balu R, Benseler S, Bien CG, Cellucci T, Cortese I, Dale RC, Gelfand JM, Geschwind M, Glaser CA. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology. 2016 Apr 1;15(4):391-404.
• Titulaer MJ, McCracken L, Gabilondo I, Armangué T, Glaser C, Iizuka T, Honig LS, Benseler SM, Kawachi I, Martinez-Hernandez E, Aguilar E. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. The Lancet Neurology. 2013 Feb 1;12(2):157-65





























