Embed Size (px)
Citation preview

Anti-IL-17A therapy protects against bone erosion in experimentalmodels of rheumatoid arthritis
CHENG-CHI CHAO1,*, SHI-JUANCHEN1,
*, IANNIS E. ADAMOPOULOS1, NICOLEDAVIS2,
KYU HONG2, ANNAVU2, SYLVIA KWAN2, LAURENCE FAYADAT-DILMAN2,
AGELIO ASIO3, & EDWARD P. BOWMAN1
1Department of Immunology, Merck Palo Alto (formerly DNAX Research Institute), Palo Alto, CA 94304, USA, 2Department
of Bioanalytical and Protein Chemistry, Merck Palo Alto, Palo Alto, CA, USA, and 3Department of Experimental Pathology
and Pharmacology, Merck Palo Alto, Palo Alto, CA, USA
(Submitted 7 May 2010; revised 6 August 2010; accepted 19 August 2010)
AbstractInterleukin-17A (IL-17A) is a pro-inflammatory cytokine secreted by a subset of memory T cells and other innate immunecells. It is associated with rheumatoid arthritis (RA) due to IL-17A expression in RA synovial fluid. The severe bone erosive ratadjuvant-induced arthritis (rAIA) and mouse collagen-induced arthritis (mCIA) models were used to address the therapeuticefficacy of anti-IL-17A treatment with a focused investigation on bone protection. In the rAIA model, treatment with anti-IL-17A completely alleviated arthritis, lowered the level of receptor activator of NFkB ligand (RANKL), and inhibited structuraldamage to the bones. In the mCIA model, IL-17A neutralization coincident with arthritis development or in mice withestablished arthritis diminished joint swelling by inhibiting disease initiation and progression. Intriguingly, even the few jointsthat became outwardly severely inflamed in the presence of an anti-IL-17A antagonist had diminished joint histopathologyscores compared to severely inflamed, control-treated mice. The bone-preserving property correlated with decreased RANKLmessage in severely inflamed paws of arthritic mice. These data identify IL-17A as a key factor in inflammation-mediated bonedestruction and support anti-IL-17A therapy for the treatment of inflammatory bone diseases such as RA.
Keywords: IL-17A, rheumatoid arthritis, inflammation, adjuvant-induced arthritis, collagen-induced arthritis
Introduction
Rheumatoid arthritis (RA) is an autoimmune disease
characterized by joint inflammation initially resulting
in pain and swelling. In a majority of patients, there is
progressive bone and cartilage erosion of the joint with
current treatment regimens that aim to control the
inflammation to retard structural damage. Mild to
moderate RA is treated with disease-modifying anti-
rheumatic drugs such as methotrexate and steroids.
Methotrexate is often used in combination with TNF
antagonists, such as Etanercept or Infliximab, for
severe RA.
IL-17A is the signature pro-inflammatory cytokine
produced by Th17 memory T cells [1]. Th17 cells
have been identified as the key T-cell subset implicated
in multiple autoimmune conditions such as multiple
sclerosis, Crohn’s disease, and RA [2,3]. Multiple
lines of evidence point to the association of IL-17 with
RA. IL17A message is present in mononuclear cells
harvested from RA synovial fluid [4], and immuno-
histochemistry demonstrates the presence of IL17A
protein in infiltrating synovial cells [5–7]. A subset of
T-cell lines expanded in vitro from RA synovium
express IL-17A following activation [8]. IL-17A
protein is found in RA synovial fluid, but rarely in
osteoarthritis synovial fluid, consistent with the
inflammatory nature of RA vs. osteoarthritis [9–11].
Two prospective clinical trials not only supported
the association of IL-17A with RA, but importantly
implicated its correlation with poor disease prognosis.
*The first two authors (C. C. Chao and S. J. Chen) contributed equally to this work.
Correspondence: E. P. Bowman, Department of Immunology, Merck Palo Alto, 901 California Avenue, Palo Alto, CA 94304, USA.Tel: (650) 496 1249. Fax: (650) 496 1200. E-mail: [email protected]
Autoimmunity, May 2011; 44(3): 243–252q Informa UK, Ltd.ISSN 0891-6934 print/1607-842X onlineDOI: 10.3109/08916934.2010.517815
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
08/0
1/13
For
pers
onal
use
onl
y.

Raza et al. prospectively collected synovial fluid
samples within a few weeks after symptom onset
from patients with early synovitis. Patient outcomes
were subsequently noted 18 months after fluid
acquisition to determine which early factors were
correlated with the progression of synovitis to RA.
Patients were grouped into those who subsequently
progressed to RA, those who subsequently progressed
to nonrheumatoid persistent synovitis, or those whose
synovitis was resolved.
Importantly, IL17A was one of the few factors
whose expression in the earliest stages of disease was
associated with subsequent progression to RA [12].
Kirkham et al. [13] concluded that IL17A gene
expression in synovial membrane biopsies was one
factor that was predictive for subsequent bone erosion
and joint damage as assessed byMRI and radiography.
Collectively, these data support that IL-17A is present
in the inflamed synovium and that IL-17A expression
levels correlate with poor prognosis and greater joint
destruction.
Although previous lines of evidence supported that
IL-17A plays a pathogenic role in arthritis, how
IL-17A may be involved in arthritis-mediated joint
pathology was less specifically addressed. We have
used the bone erosive rat adjuvant-induced arthritis
(rAIA) and mouse collagen-induced arthritis (mCIA)
models to investigate the therapeutic benefits of anti-
IL17A in these models, with a focused analysis of
cartilage and bone protection.
Materials and methods
Reagents and antibodies
The rat anti-rat IL-17A antibody JL8.18E10 used in
the rAIA model was developed using conventional
hybridoma technology to immunize rats with IL-17A
and screen for clones that bound to rat IL-17A.
JL8.18E10 has an affinity of 620 pM for rat IL-17A by
Biacore analysis and neutralizes 0.3 nM rat IL17A-
stimulated IL-6 production with an IC50 of 0.2 nM.
The neutralizing rat anti-mouse IL17A antibody
(1D10) used for the mCIA model was developed at
Schering-Plough Biopharma. It binds tightly to mouse
IL-17A (KD ¼ 10 pM by Kinexa) and neutralized
1 nM mouse IL-17A-stimulated ST2 cell IL-6
production with an IC50 of 0.5 ^ 0.2 nM. 1D10 did
not bind to any other mouse IL17 family member,
including IL17F, in an ELISA format.
Rat adjuvant-induced arthritis and mouse collagen-
induced arthritis
Male Dark Agouti rats were anesthetized with
isoflurane and 100ml of 10mg/ml Mycobacterium
butyricum cell wall suspension in paraffin oil, and
mannide monoleate (Difco, Detroit, MI, USA) was
injected intradermally into the base of the tail. Rats
with severe arthritis were dosed once on day 11 with
20mg/kg JL8.18E10 or isotype control antibody
subcutaneously. Some rats were sacrificed 3 days
post-dosing for gene expression studies, and other rats
were observed until day 23. Arthritis severity was
measured using calipers to measure paw thickness.
Male B10.RIII mice (Jackson Laboratory, Bar
Harbor, ME, USA) were immunized with bovine
type II collagen (CII) (Sigma-Aldrich, St. Louis, MO,
USA) emulsified intradermally with complete
Freund’s adjuvant (DIFCO). Fifty microliters of
1mg/ml of CII/CFA emulsion was injected on both
sides of the tail. Mice were challenged intradermally
21 days later with 1mg/ml CII emulsified in
incomplete Freund’s adjuvant. Mice were observed
daily until the first signs of a severely swollen paw
within the cohort. On that day (designated day 0), the
remaining mice were randomized to different treat-
ment groups, and received 20–30mg/kg anti-IL17A
or control antibody administered subcutaneously.
Subcutaneous dosing was repeated weekly for a total
of five doses, with sacrifice of mice seven days after the
last dose.
Microcomputed tomography imaging
Rat hind paws fixed in 10% neutral buffered formalin
were scanned by GE eXplore Lotus mCT scanner
(GE, Piscataway, NJ, USA). Data were acquired at
46mm isotropic voxel size with 720 projections by 360
degree scan, integration time of 400ms with six
frames, photon energy of 80KeV and current at
450mA. The duration of imaging was approximately
1 h per scan, followed by 40min of projection
correction and volume reconstruction. 3-D image
renderings were generated through original volumetric
reconstructed images using Microview software (GE).
Visual disease severity scoring system(DSS)
The number of swollen paws and the severity of edema
were tracked using a categorical visual disease severity
scoring (DSS) system. DSS ¼ 0 indicates no visual
change in paw appearance. DSS ¼ 1 indicates redness
and swelling in any one distal digit. DSS ¼ 2 indicates
redness and swelling in two or more distal digits or
swelling in the palm of the paw. DSS ¼ 3 indicates
swelling in palm/wrist plus swelling in any distal digit.
DSS ¼ 1 is fairly mild with limited focal inflam-
mation; DSS ¼ 2–3 were grouped together as
“severely inflamed paws”.
Histological analysis of inflamed joints
Paws were fixed in neutral buffered formalin,
de-calcified in EDTA solution, embedded in paraffin,
and stained. Sections were scored by a board-certified
C.-C. Chao et al.244
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
08/0
1/13
For
pers
onal
use
onl
y.

pathologist blinded to treatment arms and
were analyzed by a categorical scoring system
(Supplementary Table S1).
Statistical analysis
The differences in the clinical paw scores and paw
histology scores between isotype control-treated and
anti-IL-17A-treated mice were evaluated using the
non-parametric Mann–Whitney U-test. Note that
after statistical analysis, the original data were
manually modified slightly higher or lower than
original values in order to graphically present the
data in Figures 2C, 3, and 4.
Results
Therapeutic anti-IL-17A protects against bone erosion in
severely inflamed paws in rAIA
Arthritic rats were dosed with anti-IL-17A or control
antibody after severe arthritis had been established to
address the therapeutic potential of anti-IL17A
treatment to provide bone protection in an inflam-
mation-driven bone erosive environment. A single
dose of anti-IL-17A reversed the established arthritis,
and in 9 days the paws of the anti-IL17A-treated rats
reverted back to a practically naı̈ve state (Figure 1A).
mCT analysis of paws from control antibody-treated
rats confirmed massive bone erosion of a subset of
tarsal bones that had rendered them almost unrecog-
nizable in X-ray analysis.
The previously severely inflamed paws treated with
anti-IL-17A, in contrast, had little to no detectable
bone erosion (Figure 1B). Severely arthritic rats were
dosed with anti-IL-17A or control antibody for a short
time (3 days), and paw gene expression analysis was
performed to mechanistically ascertain how IL17A
neutralization gave rise to reduced bone erosion. After
only three days of IL17A neutralization (i.e., at a time
point prior to dramatic changes in paw swelling), the
arthritis-elevated and osteoclast-specific genes, such
as TRAP, cathepsin K (CatK) and MMP-9, were
decreased in the paws (Figure 1C). Anti-IL-17A also
significantly lowered the arthritis-elevated levels of
serum receptor activator of NFkB ligand (RANKL)
with minimal activity on serum osteoprotegrin (OPG)
levels (Figure 1D).
Inhibition of collagen-induced arthritis (CIA)
disease progression by anti-IL-17A therapy in
mCIA
We next investigated whether the bone sparing activity
following IL-17A neutralization would hold true in the
mCIA model. Anti-IL-17A was administered to CII-
immunized mice either after severe arthritis was first
observed in the cohort (Figure 2A and C) or after each
mouse displayed a severely arthritic paw and was
recruited into the dosing phase of the study
(Figure 2D–E). Figure 2A shows that mice treated
with a control antibody, after severe arthritis was
observed in their cohort, had a disease incidence of
approximately 90% over the 5-week observation
period post-boost. In contrast, mice therapeutically
treated with an anti-IL-17A antibody showed delayed
and diminished disease incidence, which gave rise to
decreased total animal DSS in the anti-IL-17A-
treated cohorts, as shown in Figure 2B.
Unlike joint inflammation in rAIA, the joint
inflammation in a collagen-induced arthritis (CIA)
mouse is asynchronous and of variable intensity. For
reasons outlined below, it was important to view the
DSS of each paw individually vs. the conventional
method of summing the DSS of four paws to generate
an animal’s total DSS (Figure 2C). A high percentage
of paws in the control-treated group became severely
swollen (DSS ¼ 2–3), but some paws showed no signs
of swelling (i.e. joint swelling was neither synchronous
nor uniform within an isotype-treated CIA mouse). In
a cohort of mice, anti-IL17A treatment at disease
onset inhibited paws from progressing to a severely
swollen state over the 5-week observation period. The
few inflamed paws in the anti-IL-17A-treated
group would ultimately allow higher level analysis of
how IL-17A neutralization affects the natural disease
progression (cartilage and bone destruction) in a
severely inflamed environment, as reported next.
Alternatively, individual mice were recruited into
the dosing phase of the study, once each exhibited a
severely arthritic paw, and they were dosed weekly for
3 weeks. Control-treated mice demonstrated pro-
gressive, severe arthritis development in the “other”
paws, giving rise to increasing disease severity over
time (Figure 2E). In contrast, IL-17A neutralization
in a mouse with established arthritis prevented further
arthritis development in the remaining paws. None of
the recruited arthritic mice advanced more than one
severity score when dosed with anti-IL-17A
(Figure 2D). The outward clinical score of the
already arthritic paw that recruited the mouse into the
study was not changed by isotype or by anti-IL-17A
therapy.
Inhibition of joint structural damage by
anti-IL-17A therapy in the mCIA model
Figure 3 combines results from multiple studies to
outline the benefit of anti-IL-17A neutralization
on various histopathological changes that occur as a
consequence of autoimmune inflammation in the
articular joint. Anti-IL17A significantly decreased
leukocyte recruitment, pannus formation, articular
cartilage destruction, and bone erosion in the
cohort of treated mice. The effect of anti-IL17A on
all histological parameters was consistent with its
Anti-IL-17A therapy and bone erosion in RA 245
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
08/0
1/13
For
pers
onal
use
onl
y.

beneficial effect on swollen paw incidence. Impor-
tantly, all histology parameters (as reflections of
multiple components of the disease pathobiology)
were similarly sensitive to anti-IL-17A treatment.
Although there was statistically significant inhi-
bition of swollen paw incidence by anti-IL-17A
treatment, there were a few paws that became visually
severely swollen. Importantly, these few DSS ¼ 2–3
swollen paws then allowed investigation into the
impact of therapeutic IL-17A neutralization on the
natural disease progression that occurs in this
explosively erosive model even when paws are severely
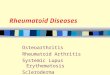
Figure 1. IL-17A neutralization inhibits arthritis progression and protects against structural joint damage in rAIA. A, Day 24 photographs of
front and hind paws of naı̈ve rats and arthritic rats treated with isotype or anti-IL-17A on day 11. Time course of swollen paw resolution by
20mg/kg anti-IL-17A dosed once at day 11 (data representative of three experiments). B, micro-CTanalysis of day 24 hind paw tarsal bones
(data representative of two experiments). C, gene expression of osteoclast markers from rAIA paws at day 14. D, serum RANKL/OPG levels
after treatment with isotype or anti-IL-17A antibody (data representative of two experiments). *p , 0.05, **p and ***p , 0.005 analyzed by
unpaired t-tests. ns, non-significant difference.
C.-C. Chao et al.246
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
08/0
1/13
For
pers
onal
use
onl
y.

swollen. Figure 4 shows the analysis of the various
histology parameters only in severely swollen
DSS ¼ 2–3 paws. By focusing on only severely
swollen paws, we have removed the prominent effect
of therapeutic anti-IL17A treatment on disease
initiation and have allowed focused analysis on the
mechanisms of joint destruction, and on whether
IL-17A neutralization changes the natural progression
of joint destruction once it occurs in this erosive
disease model.
As expected from the results shown in Supplemen-
tary Figure S1 where the magnitude of paw swelling
was highly correlated with underlying joint histo-
pathology, control-treated paws that were severely
swollen had high histology scores for leukocyte
recruitment, pannus formation, cartilage destruction,
0 7 14 21 28 350
25
50
75
100
**
Time after mAb treatment (days)
Dis
ease
inci
denc
e
0 7 14 21 28 350
2
4
6
8
**
**
**
**
Time after mAb treatment (days)
Mea
n di
seas
e se
verit
y (0
-12)
A
B
0 7 14 21–2
0
2
4
6
8
10D
Time after anti-IL-17A treatment (days)
Cha
nge
in D
SS
pos
t-re
crui
tmen
t
0 7 14 21–2
0
2
4
6
8
10E
Time after isotype treatment (days)
Cha
nge
in D
SS
pos
t-re
crui
tmen
tIsotype Anti-IL-17A
0
1
2
3
C
p < 0.0001
D35
DS
S (
0-3)
/paw
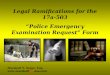
Figure 2. Anti-IL-17A therapy inhibits arthritis progression in mCIA. Mice were immunized, challenged with bovine CII, and randomized
to different treatment groups. When the first sign of severe paw swelling was seen in the cohort, the rest of the mice were then treated
subcutaneously with 20–30mg/kg anti-IL-17A (filled triangles) or an isotype control antibody (open diamonds) weekly for 5 weeks. Seven
independent experiments were combined to give mean ^ SEM for disease incidence (A) and disease severity (B). Seventy-two mice were
treated with isotype control antibody, and 52 mice were treated with anti-IL17A in total among the seven experiments. C, individual paw
scores are presented instead of summing the four paw scores, as shown in Figure 2A–B. Values from seven independent experiments have been
combined (288 paws from isotype control-treated mice and 208 paws from anti-IL-17A-treated mice) and presented slightly higher or lower
than the standard scores of 0, 1, 2, and 3 for graphical purposes. D and E, samemCIA protocol as panel A and B, but individual mice recruited
into study when any paw reached DSS . 2. The recruited mice (n ¼ 5) were dosed after arthritis established with anti-IL-17A (D) or control
antibody (n ¼ 5) (E). *p , 0.05 and **p , 0.01 vs. controls analyzed by the Mann–Whitney U-test.
Anti-IL-17A therapy and bone erosion in RA 247
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
08/0
1/13
For
pers
onal
use
onl
y.

and bone erosion. Intriguingly, severely swollen paws
from anti-IL-17A-treated mice had statistically lower
histopathology scores for pannus formation and bone
erosion (Figure 4A–D). The inhibition of joint
destruction was demonstrated in severely swollen
paws from anti-IL17A-treated mice. The mechanism
of joint protection could not be solely attributed to
modulation of leukocyte recruitment, since anti-
IL17A did not have a significant effect compared to
isotype control on the magnitude of the leukocyte
infiltrate (including neutrophils) in the severely
swollen joints.
Additionally, anti-IL-17A-treated mice had lower
bone erosion and pannus formation scores vs. isotype-
treated mice, even when severely swollen joints with
equal leukocyte infiltrate histology score (histology
score 2, 3, and 4) were compared. Potentially, anti-IL-
17A modulation of cartilage damage is more closely
tied to leukocyte infiltratem, since no significant
difference or trends in cartilage damage were observed
once severely swollen joints with equal leukocyte
infiltrate histology score (histology score 2, 3, and 4)
were compared between the two treatment groups.
Representative histology pictures from severely
inflamed paws treated with isotype or anti-IL-17A
are shown in Figure 4E–G.
Modulation of RANKL expression by
anti-IL-17A therapy
RANKL is critical in promoting pre-osteoclast
differentiation into mature osteoclasts. RANKL is
elevated in rodent arthritis models [14] and in human
RA [15] and has been used as an indicator of bone
erosion. Figure 5 shows that RANKL mRNA was
elevated in severely inflamed paws (DSS ¼ 3) and that
anti-IL-17A therapy normalized RANKL expression
even in the few DSS ¼ 3 paws that were outwardly
swollen. RANKL message was not elevated in paws
with only mild focal inflammation (DSS ¼ 1). Like-
wise, arthritis-induced elevated serum RANKL
protein was decreased by anti-IL17A treatment (data
not shown). The decreased RANKL in gene and
protein levels was also demonstrated in anti-IL-17A
treated adjuvant-induced arthritic rats, shown in
Figure 1C and D.
Discussion
IL-17A, present at the earliest stages of RA, is one of a
few proteins that retrospectively predicted patients
whose initial synovitis would ultimately progress to
RA [12,13]. Importantly, the validated RA targets
TNF and IL-1b were hardly present, much less
predictive, at this early stage of disease. We have
01234
Pan
nus
form
atio
n (0
-4)
01234
Car
tilag
e da
mag
e (0
-4)
01234
Bon
e er
osio
n (0
-4)
01234
Isotype Anti-IL-17A
Isotype Anti-IL-17A Isotype Anti-IL-17A
Isotype Anti-IL-17A
4
p < 0.001A B
C D
p < 0.001
p < 0.001p < 0.001
Leuk
ocyt
e in
filtr
ate
(0-4
)
Figure 3. Inhibition of histopathologic damage to joints by anti-IL-17A.Mice were immunized, challenged with bovine CII, and treated with
anti-IL-17A or an isotype control antibody at the first sign of severe paw swelling weekly for 5 weeks. After 35 days of treatment, front and back
paws were removed, fixed in neutral-buffered formalin, paraffin embedded, sectioned, stained with H and E, and scored by a board-certified
pathologist. The examined histological parameters were leukocyte infiltrate (A), pannus formation (B), cartilage damage (C), and bone
erosion (D). Horizontal bars indicate median values of the histological scores from 203 paws from isotype-treated mice and 208 paws from
anti-IL-17A-treated mice. Statistical analysis was performed by non-parametric Mann–Whitney U-analysis. Note that after statistical
analysis, the original data were manually modified slightly higher or lower than original values in order to graphically present the data (see
Materials and methods). The thick line represents the median value of histology scores prior to manual modification.
C.-C. Chao et al.248
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
08/0
1/13
For
pers
onal
use
onl
y.

confirmed that IL-17A is present in a subset of early
RA patients and that RA patients have the highest
frequency of detectable IL-17A compared to other
nonautoimmune arthritides. It was noteworthy that
most early RA patients who had detectable IL-17A
had also started to show detectable TNF and IL-1b
expression (data not shown), which had not been
observed by Raza et al. in very early RA patients. IL-6
was found at high levels in all synovitis condition,
regardless of whether they ultimately progressed to
RA [12], and IL-6 was present in all synovial fluids we
obtained regardless of disease type.
Several IL-17A antagonists have been used to
address the efficacy of therapeutic IL17A neutraliz-
ation in a variety of arthritis models. IL-17RA-Ig
therapy started after CII immunization, but prior to
challenge, decreased disease incidence and ankle
radiographic scores in a CIA model [16]. Polyclonal
E F G
Tb T
N C
0
1
2
3
4
p < 0.001
p < 0.001
Sev
erel
y in
flam
ed p
awpa
nnus
for
mat
ion
(0-4
)S
ever
ely
infla
med
paw
bone
ero
sion
(0-
4)
0
1
2
3
4
0
1
2
3
4
0
1
2
3
4
Isotype Anti-IL-17A Isotype Anti-IL-17A
Isotype Anti-IL-17A Isotype Anti-IL-17A
n.s.A B
C D
Sev
erel
y in
flam
ed p
awle
ukoc
yte
infil
trat
e (0
-4)
Sev
erel
y in
flam
ed p
awca
rtila
ge d
amag
e (0
-4) p < 0.05
0
1
2
3
4
5
DSS = 0 DSS = 3, Isotype DSS = 3, Anti-IL-17A
Figure 4. Diminished pannus formation, cartilage damage, and bone erosion in severely swollen paws by anti-IL-17A inhibition. Mice were
immunized, challenged with bovine CII, and treated with anti-IL-17A or an isotype-control antibody at the first sign of severe paw swelling
weekly for 5 weeks. After 35 days of treatment, the severely inflamed front and back paws were removed, fixed in neutral-buffered formalin,
paraffin embedded, sectioned, stained with H and E, and scored by a pathologist. Histological parameters examined were leukocyte infiltrate
(A), pannus formation (B), cartilage damage (C), and bone erosion (D) in severely swollen DSS ¼ 2–3 paws. Horizontal bars indicate median
histological values from 119 DSS ¼ 2–3 paws from isotype-treated mice paws and 50 DSS ¼ 2–3 paws from anti-IL-17A–treated mice in
each histopathologic parameter. Joint histology in control and severely swollen paws (E–G). E, Representative of a DSS ¼ 0 hind paw from an
anti-IL-17A-treated animal. It was never swollen at any time during the 5 weeks and was graded as “0” (no damage) for its bone erosion
histology. F, representative of DSS ¼ 3 hind paw from an isotype-treated animal. It was severely inflamed for 3 of the 5 weeks and received a
“4” (severe) for its bone erosion histology. A bone erosion score ¼ 4 was the median value for the many severely inflamed isotype-treated paws
in panel D. G, representative of DSS ¼ 3 hind paw from an anti-IL-17A treated animal. It was severely inflamed for 4 of the 5 weeks and
received a “3” (moderate) for its bone erosion histology. A bone erosion score ¼ 3 was the median value for the severely inflamed anti-IL-17A
treated paws in panel D. Tb, tibia; T, talus; N, navicular bone; C, cuneiform bone.
Anti-IL-17A therapy and bone erosion in RA 249
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
08/0
1/13
For
pers
onal
use
onl
y.

anti-IL-17A decreased clinical scores, resulting in
reduced synovitis, cartilage damage, chondrocyte
death, PG depletion, and bone erosion in collagen-
induced arthritis [17,18]. Polyclonal anti-IL17A
treatment inhibited antigen (mBSA) induced knee
swelling, PG depletion, and bone erosion in the
exacerbated smoldering knee [18]. Mice immunized
with formalin-fixed Borrelia burgdorferi and challenged
with live B. burgdorferi displayed transient joint
inflammation.
Knee swelling was reduced with either monoclonal
anti-IL17A or polyclonal anti-IL-17RA therapy;
ankles and knees were free of histopathological
changes following either therapy [19]. Lastly, rat
adjuvant arthritis models treated with IL17RA-Ig
demonstrated decreased paw swelling, joint histo-
pathology scores, and bone radiographic scores [20].
The above reports describe the effect of IL-17A
antagonists on reducing swollen joint incidence and
the resulting joint histopathology. Since outward joint
swelling is directly correlated with joint histology
(at least in the CIA model), it was unclear whether the
effect of the IL-17A antagonist on joint histology was
due solely to reducing the number of swollen paws or
to some aspect of disease-modifying, anti-rheumatic
effect. Our studies were undertaken to specifically
address this question by using two models of severe
arthritis that cause severe bone pathology (rAIA and
mCIA).
IL-17A neutralization was sufficient to alleviate the
disease severity measured by paw swelling and it
completely blocked bone erosion in the rAIA model
(Figure 1). The joint-preserving efficacy correlated
mechanistically with decreased RANKL expression in
the arthritic paw following short-term anti-IL-17A
treatment. Similarly, markers of osteoclast numbers
such as TRAP and CatK were reduced by IL17A
neutralization. These reduced markers were still
elevated in relation to naive mice as expected, since
other proinflammatory cytokines such as TNF and
IL1a/b induce TRAPþ cells that exhibit osteoclastic
characteristics in inflammatory arthritis [21–23].
The B10.RIII mCIA model was also chosen due to
its high disease penetrance and to its high cartilage and
bone pathology properties. One property of the model
was that joint inflammation was asynchronous within
each mouse, which necessitated tracking disease in a
paw-specific (Figure 2C) vs. animal-specific
(Figure 2B) manner in order to delve into the details
of the therapeutic potential of anti-IL-17A to modify
the joint erosive processes.
IL-17A blockade slightly delayed the onset of joint
swelling (Figure 2A), potentially due to the late
therapeutic dosing scheme employed in this report.
Collagen-specific T cell responses and T-cell depen-
dent anti-CII antibody responses had already been
developed and were interacting to initiate disease at
the time of starting anti-IL-17A treatment. As
described previously, the number of paws that became
involved and the severity of the swelling response were
reduced by IL17A blockade.
Since the magnitude of paw swelling was directly
correlated with the underlying joint pathology
(Supplementary Figure S1), the anti-IL-17A therapy,
which reduced the frequency and severity of paw
swelling, should be reflected in reduced joint histology
scores. The expected score reduction was obtained for
leukocyte recruitment, pannus formation, cartilage
destruction, and bone erosion (Figure 3). Previous
reports that analyzed IL-17A blockade in a conven-
tional manner, however, did not allow further
investigation of anti-IL-17A’s disease-modifying
potential within an inflamed joint.
The severely inflamed joints from control-treated
mice showed fairly uniform high histology scores for
pannus formation, cartilage destruction, and bone
erosion (Figure 4). Conversely, mice with anti-IL-17A
therapy that had the same “clinical” risk factor for
joint destruction (i.e., the few severely swollen paws)
fared much better. Anti-IL-17A’s disease-modifying
effect was apparent regardless of which histology
parameter was examined: pannus formation, cartilage
destruction, or bone erosion.
The joint-protective effect could not be ascribed to
modulation of leukocyte recruitment, since non-
statistical significant effect of anti-IL17A on this
parameter in severely swollen paws was uncovered. To
our knowledge, these data are the first description of
anti-IL-17A therapy that demonstrated the potential
to modify joint disease. Previous reports had failed to
separate the ability of various IL-17A antagonists to
delay the onset of paw swelling with any joint-
preserving function, if and when a paw developed
outward signs of arthritis. We have removed the
prominent effect of anti-IL-17A on arthritis incidence
by post hoc analysis of the few severely swollen paws
that developed in the presence of anti-IL-17A.
– + – + – +0
100
200
300
DSS = 0 DSS = 1 DSS = 3
p = 0.001
Anti-IL-17A
RA
NK
-L (
norm
aliz
ed to
Ub)
Figure 5. Modulation of RANKL expression in arthritic paws in
mCIA mice after IL-17 therapy. DSS ¼ 0, DSS ¼ 1, and DSS ¼ 3
paws from anti-IL-17A and isotype-treated mice were harvested,
frozen, and mRNA isolated. RANKL message normalized to
ubiquitin levels was determined. Statistical analysis was performed
by non-parametric Mann–Whitney analysis. “ 2 ” and “ þ ”
symbols represent isotype and anti-IL-17A-treated groups,
respectively.
C.-C. Chao et al.250
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
08/0
1/13
For
pers
onal
use
onl
y.

In addition to using visual scores, we have
compared similarly infiltrated joints with bone
erosion, cartilage destruction, and pannus formation
by histology scores (Supplementary Figure S2). Our
analysis shows that anti-IL-17A greatly protects bone
erosion where the paws experience different degrees of
cellular infiltration from mild “score 1” to severe
“score 4” (Supplementary Figure S2A). Anti-IL-17A
inhibits cartilage destruction where paws have a mild
score (2), but do not have severe cellular infiltration.
The beneficial effect of anti-IL-17A also inhibits
pannus formation where mild (score 2) and severe
(score 3) infiltrates occur.
The therapeutic benefit of anti-IL-17A therapy was
observed when arthritic mice were dosed coincident
with arthritis development (Figure 2A–C). Further-
more, anti-IL-17A therapy prevented arthritis pro-
gression and lowered RANKL expression (Figures 1D
and 5), even when rats (Figure 1) and mice
(Figure 2D–E) were dosed after severe arthritis was
established. These results have significant impli-
cations for the therapeutic potential of IL17A
antagonism in RA. IL-17A is not required for arthritis
initiation (IL-17A 2 /2 are susceptible to CIA,
although less so than wild-type controls) [24], and
therapeutic IL-17A neutralization does not absolutely
halt disease in the highly joint-destructive B10.RIII
CIA model.
Similar conclusions are also drawn for TNF, since
TNF 2 /2 mice are susceptible to arthritis [25] and
therapeutic TNF antagonism does not stop, but
diminishes, joint-swelling responses [26,27]. IL-17A
blockade has two mechanisms to inhibit joint
histology. The first is via the conventional concept of
inhibiting joints from becoming inflamed. The
analogous human RA scenario would be using anti-
IL17A as front-line therapy in “early RA” patients
who have risk factors that predict that destructive joint
disease will quickly ensue in the initial inflamed joint
and will spread to other joints. A second, independent
mechanism by which anti-IL17A inhibits joint
pathology occurs in joints that are already inflamed.
The analogous human RA scenario would be in
patients who have inadequate or no response to the
current gold-standard TNF antagonists.
It should be noted that anti-IL17A may have joint
protective benefits, even in patients where the outward
signs of arthritis are not modulated by IL-17A
antagonism. This concept has some similarities to
Denosumab/Anti-RANKL, which has profound bone
protective effects, but no effects on the outward
systemic signs of arthritis. Anti-IL17A therapy differs
from RANKL blockade in animal models, because
neutralizing RANKL in treated arthritic animals has
no effect on joint swelling and minimal cartilage
protection. Therefore, anti-IL-17A is both anti-
inflammatory and joint-preserving, whereas, anti-
RANKL is only the latter.
Chronic arthritis in RA can cause peri-articular
bone erosion due to an imbalance in bone erosion and
bone formation. In these inflammatory arthritic
models, we have also found that new bone formation
along with bone erosion was displayed in the cortical
surface of different areas. The higher activity of bone
turnover frequently occurs in the areas of the bones
having more severe erosion. Since anti-IL-17A
treatment inhibits bone loss, less activity of bone
remodeling and new bone formation were observed in
the anti-IL-17A-treated paws. Bone erosion is not a
purely resorptive process, but a complex interaction of
bone resorption and formation. An interplay between
cellular (osteoclasts and osteoblasts) and molecular
(RNAKL, BMPs/Wnt) levels, and a net outcome of
bone remodeling will be further investigated in our
models [28].
In summary, treatment with anti-IL-17A comple-
tely alleviates arthritis, decreases inflammation-driven
RANKL levels, and provides protection in the bone-
erosive rAIA model. Furthermore, therapeutic
IL-17A neutralization after CII challenge diminishes
the DSS by inhibiting the number of paws that
become inflamed in the mCIA model. Unexpectedly,
even paws that became outwardly severely inflamed in
the presence of an IL-17A antagonist had diminished
joint histopathology scores compared to severely
inflamed control-treated mice. No evidence was
obtained that anti-IL-17A therapy altered T cell
cytokine response or diminished B-cell anti-collagen
responses (date not shown). IL-17A blockade rep-
resents a novel approach to attack the underlying
pathomechanism that initiates and perpetuates
inflammatory joint disease.
Declaration of interest: All authors were employees
of Schering-Plough (now Merck) during the time of
these studies, there are no other conflicts of interest.
References
[1] FossiezF,DjossouO,ChomaratP,Flores-RomoL,Ait-YahiaS,
Maat C, Pin JJ, Garrone P, Garcia E, Saeland S, Blanchard D,
Gaillard C, Das Mahapatra B, Rouvier E, Golstein P,
Banchereau J, Lebecque S. T cell interleukin-17 induces
stromal cells to produce proinflammatory and hematopoietic
cytokines. J Exp Med 1996;183:2593–2603.
[2] McGeachy MJ, Cua DJ. The link between IL-23 and Th17
cell-mediated immune pathologies. Semin Immunol 2007;19:
372–376.
[3] Kawaguchi M, Adachi M, Oda N, Kokubu F, Huang SK.
IL-17 cytokine family. J Allergy Clin Immunol 2004;114:
1265–1273; quiz 1274.
[4] Hwang SY, Kim HY. Expression of IL-17 homologs and their
receptors in the synovial cells of rheumatoid arthritis patients.
Mol Cells 2005;19:180–184.
[5] Honorati MC, Meliconi R, Pulsatelli L, Cane S, Frizziero L,
Facchini A. High in vivo expression of interleukin-17 receptor
in synovial endothelial cells and chondrocytes from arthritis
patients. Rheumatology (Oxford) 2001;40:522–527.
Anti-IL-17A therapy and bone erosion in RA 251
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
08/0
1/13
For
pers
onal
use
onl
y.

[6] Joosten LA, Radstake TR, Lubberts E, van den Bersselaar LA,
van Riel PL, van Lent PL, Barrera P, van den Berg WB.
Association of interleukin-18 expression with enhanced levels
of both interleukin-1beta and tumor necrosis factor alpha in
knee synovial tissue of patients with rheumatoid arthritis.
Arthritis Rheum 2003;48:339–347.
[7] Page G, Sattler A, Kersten S, Thiel A, Radbruch A, Miossec P.
Plasma cell-like morphology of Th1-cytokine-producing cells
associated with the loss of CD3 expression. Am J Pathol 2004;
164:409–417.
[8] Aarvak T, Chabaud M, Miossec P, Natvig JB. IL-17 is
produced by some proinflammatory Th1/Th0 cells but not by
Th2 cells. J Immunol 1999;162:1246–1251.
[9] Ziolkowska M, Koc A, Luszczykiewicz G, Ksiezopolska-
Pietrzak K, Klimczak E, Chwalinska-Sadowska H,
Maslinski W. High levels of IL-17 in rheumatoid arthritis
patients: IL-15 triggers in vitro IL-17 production via
cyclosporin A-sensitive mechanism. J Immunol 2000;164:
2832–2838.
[10] Chabaud M, Durand JM, Buchs N, Fossiez F, Page G,
Frappart L, Miossec P. Human interleukin-17: A T cell-
derived proinflammatory cytokine produced by the rheuma-
toid synovium. Arthritis Rheum 1999;42:963–970.
[11] Kotake S, Udagawa N, Takahashi N, Matsuzaki K, Itoh K,
Ishiyama S, Saito S, Inoue K, Kamatani N, Gillespie MT,
Martin TJ, Suda T. IL-17 in synovial fluids from patients with
rheumatoid arthritis is a potent stimulator of osteoclastogen-
esis. J Clin Invest 1999;103:1345–1352.
[12] Raza K, Falciani F, Curnow SJ, Ross EJ, Lee CY, Akbar AN,
Lord JM, Gordon C, Buckley CD, Salmon M. Early
rheumatoid arthritis is characterized by a distinct and transient
synovial fluid cytokine profile of T cell and stromal cell origin.
Arthritis Res Ther 2005;7:R784–R795.
[13] Kirkham BW, LassereMN, Edmonds JP, Juhasz KM, Bird PA,
Lee CS, Shnier R, Portek IJ. Synovial membrane cytokine
expression is predictive of joint damage progression in
rheumatoid arthritis: A two-year prospective study (the
DAMAGE study cohort). Arthritis Rheum 2006;54:
1122–1131.
[14] Mori H, Kitazawa R,Mizuki S, NoseM,Maeda S, Kitazawa S.
RANK ligand, RANK, and OPG expression in type
II collagen-induced arthritis mouse. Histochem Cell Biol
2002;117:283–292.
[15] Gravallese EM, Manning C, Tsay A, Naito A, Pan C,
Amento E, Goldring SR. Synovial tissue in rheumatoid
arthritis is a source of osteoclast differentiation factor. Arthritis
Rheum 2000;43:250–258.
[16] Lubberts E, Joosten LA, Oppers B, van den Bersselaar L,
Coenen-de Roo CJ, Kolls JK, Schwarzenberger P, van de Loo
FA, van den Berg WB. IL-1-independent role of IL-17 in
synovial inflammation and joint destruction during collagen-
induced arthritis. J Immunol 2001;167:1004–1013.
[17] Lubberts E, Koenders MI, Oppers-Walgreen B, van den
Bersselaar L, Coenen-de Roo CJ, Joosten LA, van den
Berg WB. Treatment with a neutralizing anti-murine inter-
leukin-17 antibody after the onset of collagen-induced arthritis
reduces joint inflammation, cartilage destruction, and bone
erosion. Arthritis Rheum 2004;50:650–659.
[18] Koenders MI, Lubberts E, Oppers-Walgreen B, van den
Bersselaar L, HelsenMM,Di Padova FE, Boots AM,GramH,
Joosten LA, van den Berg WB. Blocking of interleukin-17
during reactivation of experimental arthritis prevents joint
inflammation and bone erosion by decreasing RANKL and
interleukin-1. Am J Pathol 2005;167:141–149.
[19] Burchill MA, Nardelli DT, England DM, DeCoster DJ,
Christopherson JA, Callister SM, Schell RF. Inhibition of
interleukin-17 prevents the development of arthritis in
vaccinated mice challenged with Borrelia burgdorferi. Infect
Immun 2003;71:3437–3442.
[20] Bush KA, Farmer KM, Walker JS, Kirkham BW. Reduction of
joint inflammation and bone erosion in rat adjuvant arthritis by
treatment with interleukin-17 receptor IgG1 Fc fusion protein.
Arthritis Rheum 2002;46:802–805.
[21] Lam J, Takeshita S, Barker JE, Kanagawa O, Ross FP,
Teitelbaum SL. TNF-alpha induces osteoclastogenesis by
direct stimulation of macrophages exposed to permissive levels
of RANK ligand. J Clin Invest 2000;106:1481–1488.
[22] Nakamura I, Kadono Y, Takayanagi H, Jimi E, Miyazaki T,
Oda H, Nakamura K, Tanaka S, Rodan GA, Duong LT. IL-1
regulates cytoskeletal organization in osteoclasts via TNF
receptor-associated factor 6/c-Src complex. J Immunol 2002;
168:5103–5109.
[23] Adamopoulos IE, Sabokbar A, Wordsworth BP, Carr A,
Ferguson DJ, Athanasou NA. Synovial fluid macrophages are
capable of osteoclast formation and resorption. J Pathol 2006;
208:35–43.
[24] Nakae S, Nambu A, Sudo K, Iwakura Y. Suppression of
immune induction of collagen-induced arthritis in IL-17-
deficient mice. J Immunol 2003;171:6173–6177.
[25] Campbell IK, O’Donnell K, Lawlor KE, Wicks IP. Severe
inflammatory arthritis and lymphadenopathy in the absence of
TNF. J Clin Invest 2001;107:1519–1527.
[26] Joosten LA, Helsen MM, van de Loo FA, van den Berg WB.
Anticytokine treatment of established type II collagen-induced
arthritis in DBA/1 mice. A comparative study using anti-TNF
alpha, anti-IL-1 alpha/beta, and IL-1Ra. Arthritis Rheum
1996;39:797–809.
[27] Butler DM, Malfait AM, Maini RN, Brennan FM, Feldmann
M. Anti-IL-12 and anti-TNF antibodies synergistically
suppress the progression of murine collagen-induced arthritis.
Eur J Immunol 1999;29:2205–2212.
[28] Zwerina J, Tuerk B, Redlich K, Smolen JS, Schett G.
Imbalance of local bone metabolism in inflammatory arthritis
and its reversal upon tumor necrosis factor blockade: Direct
analysis of bone turnover in murine arthritis. Arthritis Res
Ther 2006;8:R22.
C.-C. Chao et al.252
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
08/0
1/13
For
pers
onal
use
onl
y.