Embed Size (px)
Citation preview

Anti-IgE in Asthma and Other Allergic Diseases
Harold S. Nelson. MD
Professor of Medicine
National Jewish Health
And University of Colorado School of Medicine.
Denver. Colorado, USA

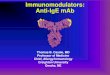
Run-InPhase
4-6 Weeks4-6 Weeks
Stable-Steroid Phase
16 Weeks16 Weeks
Steroid-ReductionPhase
12 Weeks12 Weeks
Double-Blind Extension Phase
24 Weeks24 Weeks
Placebo orOmalizumab +
Stable BDP
RandomizationRandomization
Placebo orOmalizumab
+ BDP reduction
Placebo orOmalizumab
BDP
BDPOptimization
Pivotal Trials: Study Design
Busse W, et al. J Allergy Clin Immunol. 2001;108:184-190; Soler M, et al. Eur Respir J. 2001;18(2):254-261.
EfficacyEfficacy28 Weeks 28 Weeks
TotalTotalSafetySafety
52 Weeks Total52 Weeks Total

Baseline Asthma Characteristics
008 009
Baseline characteristic†OMAL n = 268
Placebon = 257
OMAL n = 274
Placebo n = 272
Asthma, yr 21 (13) 23 (15) 20 (14) 19 (13)
IgE, IU/mL 172 (141) 186 (142) 223 (169) 206 (161)
BDP daily dose, µg 570 (149) 568 (148) 646 (199) 649 (222)
Rescue 2, puffs/day 5 (3) 5 (3) 4 (3) 5 (3)
Total asthma symptom score, 0 to 9
4 (1) 4 (1) 4 (1) 4 (1)
FEV1, % of predicted 68 (15) 68 (14) 70 (15) 70 (15)
Hospitalized for asthma past yr, %
2 4 4 7
ER visit for asthma past yr, %
10 14 12 10
†Mean (SD) unless otherwise indicated.

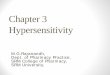
0.28 0.28
0.54
0.66
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Study 008 Study 009
Mean exacerbations per patient
0.39 0.36
0.660.75
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Study 008 Study 009
Mean exacerbations per patient
Reduction in Asthma Exacerbations
†van Elteren test; protocol-defined analysis with imputation.
Stable steroid phase16 wk
Steroid-reduction phase12 wk
P = .006†
P < .001† P = .003†
P < .001†
Omalizumab Placebo

Time to First Asthma Exacerbation
OMAL
Placebo
0
0.25
0.50
0.75
1.0
Pro
po
rtio
n o
f pa
tien
tse
xace
rba
tion
fre
e
Time since randomization
008
0
0.25
0.50
0.75
1.0
009
0 4 8 12 16 20 24 28 32 36 40 44 48 52
P = .0001†
HR = 0.51
0 4 8 12 16 20 24 28 32 36 40 44 48 52
P = .0067†
HR = 0.63

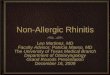
Reduction in Inhaled Steroid Use Studies 008 and 009 (Combined)
41.3
35.5
10.913.5
19.3
34.3
17.4
27.8
0
10
20
30
40
50
100% 50% - 99% 1% - 49% ≤ 0%
BDP reduction from baseline at wk 28
Patients, %
Xolair Placebo
BDP = Beclomethasone dipropionate.†van Elteren test.
P < .001†

Reduction in Albuterol Use
*P .05, van Elteren test.
008 009
0
1
2
3
4
5
0 4 8 12 16 20 24 280
1
2
3
4
5
0 4 8 12 16 20 24 28
* **
*
*
NSNS
NS
Pu
ffs
per
day
, n
Time, wk Time, wk
* * * **
*
* * *NS
NS NS
Xolair™ Placebo

0.0
0.5
1.0
1.5
2.0
0 4 8 12 16 20 24 28Time, wk
0.0
0.5
1.0
1.5
2.0
0 4 8 12 16 20 24 28Time, wk
0.0
1.0
2.0
3.0
4.0
0 4 8 12 16 20 24 28Time, wk
0.0
1.0
2.0
3.0
4.0
0 4 8 12 16 20 24 28Time, wk
Reduction of Symptoms008
009
* *
**
* *
NS
Omalizumab Placebo
*
**** * * * ***
** **
* * * * * *
Asthma symptom scores Nocturnal symptom scores
* * * * * *
* * * * * *
009
008
*P .05, van Elteren test.

60
65
70
75
-8 -4 0 4 8 12 16 20 24 2860
65
70
75
-8 -4 0 4 8 12 16 20 24 28
Improvement in Pulmonary Function
Time since randomization, wk
* ** *
* * ** *
*
008 009
Mea
n F
EV
1 %
pre
dic
ted
*P ≤ .05, ANCOVA.
** * * * * * * *
Time since randomization, wk
NS
Omalizumab Placebo

Omalizumab: Mechanisms of Action
S Holgate, et al. Allergy 2009;64:1728-36
1. Omalizumab binds to the IgE molecule preventing its interaction with IgE receptors on inflammatory cells.
2. The fall in free-IgE leads to down regulation of FcεRI on basophils, mast cells and plasmacytoid dendritic cells.
3. The release of pro-inflammatory cytokines from basophils and mast cells is decreased.
4. The effect on pDCs may reduce allergen presentation to T-cells.
4. There is a decrease in levels of blood, tissue and sputum eosinophils.

Omalizumab in Patients with Severe Persistent Asthma
J Bousquet, et al. Allergy 2005;60:302-8
Data was pooled from 7 studies, with 4,308 subjects, 93% with severe persistent asthma.
Mean baseline values:ICS 1462 mcg BDP, LABA use by 57%,FEV1 70% predicted
Exacerbations (90% treated with OCS) - 38%Omalizumab 0.91/year Placebo 1.47/year p<.00001
Emergency Department Visits - 61% 0.026/y vs. 0.066/y p = 0.013
Hospitalizations - 50%0.03/y vs. 0.06/y p = 0.04

There Are No Predictors of a Good Response to Omalizumab
J Bousquet et al. Allergy 2005;60:302-8

Omalizumab in Children
B Lanier, ex al. J Allergy Clin Immunol 2009;124:1210-6
• 627 children ages 6 to 11 years with asthma not fully controlled on ≥ 200 mcg FP/d plus history of ≥ 2 exacerbations or ≥ 1 hospitalization in last year.
• Randomized 2:1 omalizumab: placebo for 52 weeks, steroid stable first 24 weeks.
• Exacerbation defined as doubling dose ICS or oral CS ≥ 3 days.

Omalizumab in Children: Exacerbation Rate
B Lanier, ex al. J Allergy Clin Immunol 2009;124:1210-6
: 24 WEEKS 52 WEEKS
Omalizumab 0.45 0.78
Placebo 0.64 1.36
% reduction / p value -31%/0.007 -43%/0.001

Omalizumab Safety:Anaphylaxis
• A joint task force of the AAAAI and ACAAI reviewed all post-marketing reports to the FDA from 1 June 2003 to December 31 2005.
• 35 patients experienced 41 episodes of anaphylaxis
• This represented 0.09% of patients receiving omalizumab.

Omalizumab Safety:Anaphylaxis
Timing 1-3rd Dose ≥ 4th Dose Total
< 30 min 11 5 16
30-60 min 6 1 7
1-2 hours 5 0 5
2-12 hours 4 1 5
> 12 hours 3 0 3
Unknown 3 2 5
Total 32 9 41
L. Cox, ex al. J Allergy Clin Immunol 2007120:1373-7

Omalizumab Safety: Recommendations for Administration
L. Cox, ex al. J Allergy Clin Immunol 2007120:1373-7
• Patient should sign informed consent.• Patient should be instructed in administration of
auto-injected epinephrine and carry for 24 hours after each dose of omalizumab
• Patients should remain under observation for 2 hours after the first 3 administrations, then 30 minutes after each subsequent administration.

Omalizumab: Unapproved and Unproven Uses
• Seasonal & perennial allergic rhinitis• Chronic urticaria:
- Autoimmune (JACI 2008;122:569-73)
- Non-autoimmune (JACI 2010;126:664-5)- Delayed pressure, dermagraphism, cholinergic
• Food allergy (Allergy Asthma Proc 2010;31:76-83)
• Chronic sinusitis (JACI 2008;121:257-8)
• Atopic dermatitis (Allergy Asthma Proc 2008;29:530-7)
• Allergic bronchopulmonary Aspergillosis (Ped Pulmonol 2009;44:516)

Omalizumab: Unapproved and Unproven Uses
• Idiopathic anaphylaxis Ann Allergy Asthma Immunol 2009;102:257-8)
• Fire ant anaphylaxis (immunotherapy failure) (JACI 2010;126:664-5)
• Occupational latex sensitivity (JACI 2004;113:360-1)• Systemic mastocytosis (JACI 2010;126:415-6)• Systemic mastocytosis plus anaphylaxis to bee sting
(Allergy 2009;64:1384-5)• Adjunct to hymenoptera immunotherapy (Allergy
2007;62:963-4).• Insulin allergy (N Engl J Med 2009;360:1045-7)

Omalizumab as an Adjunct in Allergen Immunotherapy

Omalizumab Pretreatment Decreases Acute Reactions after Rush
Immunotherapy for ragweed-induced Seasonal Allergic Rhinitis
123 adults with ragweed allergic rhinitis Pretreated with 9 weeks of omalizumab or placebo1 day rush immunotherapy to top dose of 1.2 mcg Amb a 1 Followed by 12 weeks of combined omalizumab or placeb and weekly immunotherapy with increase in dose to 12 mcg Amb a 1.
TB Casale, et al J Allergy Clin Immunol 2006;117:134-40

Reduction of IgE by Pre-Treatment with Omalizumab: Results
Anaphylaxis risk vs. placebo during RIT:IT alone OR 12.1 Om plus IT OR 2.1
Anaphylaxis risk vs. placebo during weekly buildup:IT alone 9.7%Om plus IT 0%
TB Casale, et al. J. Allergy Clin Imm 20061117:134-40

Effect of Pretreatment with Omalizumab on the Tolerability of
Specific Immunotherapy in Patients with Persistent Symptomatic Asthma Inadequately Controlled with Inhaled
Corticosteroids
Massanari M, Nelson H, Casale T, Busse W, Kianifard F, Geba G, Zeldin R

Omalizumab as an Adjunct to Immunotherapy: Study Design
Subjects with at least moderate persistent allergic asthma.- Symptomatic on inhaled corticosteroids
- FEV1 ≥ 75% predicted- Positive prick skin test to cat, dog or house dust mite standardized extract.
Excluded for severe asthma, oral corticosteroid-requiring exacerbation within 3 months, ED visit or hospitalization within 6 months.

Omalizumab Cluster IT
Placebo
Maintenance IT
Maintenance ITCluster IT
Screening
Period 1 Period 2 Period 3 Period 4
3 wk overlap
Xolair and Immunotherapy: Study Design275 Patients, Randomized 1:1
Visit 0 Visit 1 Visit 5 Visit 11 Visit 14 Visit 19
-2wks 0 13wks 16 wks 17 wks 24 wks

Change in Average Total Asthma Symptom Score Before Initiating Immunotherapy
-0.70
-0.47
-0.8
-0.7
-0.6
-0.5
-0.4
-0.3
-0.2
-0.1
0.0N=124 N=119
Omalizumab Placebo
Baseline Mean Score
(Day -14 to Day -1) 1.15 1.17
Change From Baseline to Visit 5 in Total Average Asthma Symptom Score
(Average total symptom score Day 91 to Day 97)

Proportion of Patients Who Experienced a Systemic Allergic Reaction
13.5%
26.2%
0%
5%
10%
15%
20%
25%
30%
Omalizumab Placebo
Percent of Patients with SARs
N=126 N=122
P= 0.017
N = 32 N = 17

SARs in Patients According to Average Total Asthma
Symptom Scores* Pre Immunotherapy
17.6%
8.8%
16.7%
32.4%
0%
5%
10%
15%
20%
25%
30%
35%
0 (N=116) 0 (N=128)
Percent of Patients with SARs
Omalizumab Placebo
>
*Average total symptom score Day 91 to Day 97

Severity of First Systemic Allergic Reaction
7
2
6
2
6
0
24
2
0
5
10
15
20
25
30
Grade 1 (Skin) Grade 2 (GI) Grade 3(Resp)
Grade 4 (CV)
Number of Patients
Omalizumab PlaceboN=17 N=32

Proportion of Patients Who Experienced a Systemic Allergic Reaction According to
Allergen Sensitivity
15.2%13.3%
14.4%
24.0%
17.6%
31.9%
0%
5%
10%
15%
20%
25%
30%
35%
Cat Dog HDM
Percent of Patients with SARs
Omalizumab PlaceboN=209 N=188N=168
N=29N=11 N=14N=25 N=15N=16
15 g Fel d 1, 15 g Can d 1, 7 g Der p 1

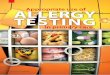
Percent of Patients who Achieved Target Maintenance IT Dose
87.3%
72.1%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Omalizumab (N=126) Placebo (N=122)
Percent of Patients
p=0.004

Conclusions Pretreatment with omalizumab
significantly reduced systemic allergic reactions from IT
Pretreatment with omalizumab resulted in a clinically meaningful shift in severity of systemic allergic reactions from IT
A significantly higher proportion of omalizumab patients were able to reach target maintenance dose of IT
Omalizumab was well tolerated