Embed Size (px)
Citation preview

Journal of Neuro-Oncology 65: 173–175, 2003.© 2003 Kluwer Academic Publishers. Printed in the Netherlands.
Clinical Study
Anti-GAD antibody positive stiff-limb syndrome in multiple myeloma
David Schiff1, Josep Dalmau2 and Delynne J. Myers3
1Departments of Neurological Surgery, Neurology, and Medicine, University of Pittsburgh Medical Center;2Department of Neurology, University of Arkansas for Medical Sciences; 3Department of Medicine,University of Pittsburgh Medical Center, USA
Key words: anti-GAD antibodies, multiple myeloma, paraneoplastic syndrome, stiff-limb syndrome, stiff-personsyndrome, thalidomide
Summary
Although most cases of stiff-limb syndrome are unassociated with malignancy, occasional cases have been associatedwith breast and lung cancer. Only four reported patients have had cancer and stiff-limb syndrome associated withanti-GAD antibodies. We report the first case of stiff-limb syndrome in a patient with multiple myeloma undergoingtreatment with thalidomide, and explore the potential link to the cancer and its treatment.
Introduction
Stiff-person syndrome is characterized by the devel-opment of spasms, usually initially involving the axialmusculature, in middle-aged adults. Occasional casesproducing stiffness in a limb have been termed the stiff-limb syndrome [1]. Sixty percentage of stiff-personsyndrome cases are associated with anti-glutamic aciddecarboxylase (GAD) antibodies, as are 83% of stiff-limb cases [2,3]. Approximately 95% cases of stiff-person and stiff-limb syndromes are unassociated withcancer. Stiff-person syndrome has been reported as aparaneoplastic phenomenon in association with anti-amphiphysin antibodies, primarily in patients withbreast cancer but also in small cell lung cancer [4]. Onecase of stiff-person syndrome in a patient with undif-ferentiated mediastinal carcinoma has been associatedwith anti-gephyrin antibodies [5]. Only four patientswith anti-GAD antibodies and stiff-person syndromehave been reported to have cancer [6–9]; three (one ofwhom had concomitant anti-amphiphysin antibodies)had breast cancer, and one had Hodgkin’s disease. Wereport the first case of stiff-limb syndrome associatedwith multiple myeloma and anti-GAD antibodies.
Case report
A 47-year-old female was diagnosed 5 years ear-lier with IgG lambda multiple myeloma detected
incidentally following abnormal bloodwork. She ini-tially received Melphalan and prednisone; 18 monthsbefore neurologic presentation M protein increase ledher to start thalidomide 100 mg daily. Paresthesias lim-ited attempts at dose escalation. Nine months later shenoted difficulty climbing stairs and a tendency to trip.Gradually she developed stiffness in the right ankle,tingling in the right foot, and trouble wiggling the footand toes. Concerns of a neoplastic radiculopathy priorto a vacation led to the trial of prednisone, which allevi-ated the pain and clumsiness until it was discontinued.The patient denied back pain or similar symptoms inthe other extremities. Her past history was notablefor hypothyroidism and focal epilepsy in childhood;she did not have diabetes mellitus. Other medica-tions included levothyroxine and rofecoxib. Familyhistory was negative for malignancy, neurologic, orautoimmune disease.
Neurologic examination was notable for slightlyincreased tone at both knees and for a contracture atthe right ankle with the foot plantar flexed. Deep ten-don reflexes were slightly increased at both knees andankles, and Babinski’s sign was equivocally present onthe right but absent on the left. Power was full exceptfor mild right anterior tibialis weakness. There wasslightly decreased light touch and pinprick in a rightL5 distribution.
Magnetic resonance imaging of the brain and entirespinal column was normal, with no evidence of bone

174
metastases or other pathology. Nerve conduction stud-ies demonstrated normal right peroneal and tibialmotor responses including conduction velocities andF-waves. Concentric needle examination of right lowerextremity muscles and the left tibialis anterior showednormal motor unit potentials, although the patientwas unable to relax any of the muscles tested belowthe right knee and had frequent cramping in theright calf.
Mammogram, gynecologic examination, and CT ofthe chest and abdomen were all normal. Studies per-formed at Mayo Medical Laboratory demonstratedserum anti-GAD65 antibodies at a concentrationof 76.3 nmol/l (normal <0.02). Antibodies againstGAD67 were not assayed. Anti-islet cell antibod-ies were present at a titer of 80 JDF units byindirect immunofluorescence (normal <1.25). Acetyl-choline receptor, mitochondrial, gastric parietal cell,thyroglobulin, and thyroid peroxidase antibodies wereall absent. Studies performed by using immunoblotof recombinant amphiphysin excluded the presence ofamphiphysin antibodies (data not shown). Immunohis-tochemical studies (see below) showed that the serumof the patient had polyclonal antibodies to GAD and,therefore, these antibodies were not produced by themyeloma cells.
A trial of diazepam 2.5 mg twice daily dramati-cally ameliorated the patient’s symptoms. The patientremained on thalidomide and remains neurologicallyimproved and hematologically stable 2 years later.
Immunohistochemical studies
MethodSeven micron-thick frozen sections of rat cerebellumwere fixed in methanol–acetone (4◦C) and sequentiallyincubated with 0.3% hydrogen peroxide in phosphatebuffered saline (PBS) for 10 min, 10% normal goatserum for 20 min, the patient’s serum diluted at 1 : 500for 2 h, biotinylated goat anti-human heavy + lightIgG, or biotinylated goat anti-human kappa light chain,or biotinylated goat anti-human lambda light chain(Vector, Burlingame, CA, USA) each diluted at 1 : 500,for 30 min, and the avidin biotin peroxidase complex(Vector) for 30 min. The reaction was developed with0.05% diaminobenzidine tetrahydrochloride (Sigma)with 0.01% hydrogen peroxide and 0.5% Triton X-100in PBS. Patient’s serum and secondary antibodies werediluted with 10% normal goat serum in PBS. Betweensteps slides were washed with PBS.
Results
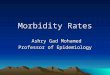
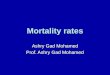
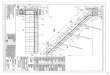
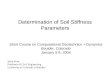
Using immunohistochemistry of rat brain, the patient’sserum showed a pattern of reactivity identical to thatobtained with a control serum with GAD antibod-ies. In cerebellum, this reactivity is characterized byintense labeling of synaptic rich regions in the molec-ular layer of the cerebellum as well as axon hillocksof the Purkinje cells (Figure 1A). To determine whetherthe patient’s GAD antibodies were monoclonal (andtherefore produced by myeloma cells), biotinylatedsecondary antibodies specific for kappa or lambdahuman chains were also used in these experiments.These studies showed that the patient’s GAD antibodiescorresponded to IgG kappa and lambda, and thereforewere not part of the monoclonal protein synthesized bythe myeloma cells (Figures 1B and C).
Discussion
This case report depicts a case of stiff-limb syndrome,presumed to be a variant of stiff-person syndrome, ina woman with multiple myeloma. The clinical presen-tation, response to both corticosteroids and diazepam,and presence of anti-GAD antibodies as well as otherautoimmune disease, are typical of this disorder [2].
Stiff-person syndrome may occur as a paraneoplas-tic manifestation of cancer, and most of these patientsharbor amphiphysin antibodies. The presence of GADantibodies is usually found in the non-paraneoplasticform of the disorder, although there are a few patientswho also had cancer [6–9]. In these patients, thepathogenic association between GAD-associated neu-rologic symptoms and cancer remains speculative. Inour patient, the occurrence of myeloma as underlyingneoplasm offered the unique opportunity to evaluatethe possibility of a close link between the synthesis ofGAD antibodies and the tumor. The detection of bothIgG kappa and lambda GAD antibodies in the patient’sserum argues against the production of GAD antibodiesas part of the IGM synthesized by the myeloma cells.Alternatively, the use of thalidomide may have playeda role in the patient’s disorder. Thalidomide’s mode ofaction in multiple myeloma remains unknown; it hasimmunomodulatory and inflammatory as well as anti-angiogenic effects. It has been utilized to treat putativeautoimmune disorders, including Behcet’s disease andCrohn’s disease. Thalidomide prolongs experimentalallergic neuritis in Lewis rats, increasing the pos-sibility that its immunomodulatory properties could

175
A
B
C
Figure 1. Immunohistochemical analysis of the patient’s serumwith rat cerebellum. Sections of rat cerebellum incubated withserum of a positive control patient with anti-GAD antibodies (A)and the patient’s serum (B and C). In A, the immunolabeling hasbeen detected with a conventional secondary antibody againsthuman heavy and light chains of IgG; in (B), the immunolabel-ing has been detected with a secondary antibody against humankappa chain; and in (C) with a secondary antibody against humanlambda chain. ‘P’ indicates the body of a Purkinje cell. All panelsshow a pattern of immunolabeling characteristic of GAD, includ-ing intense reactivity with synaptic rich regions of the molecularlayer, axon hillocks of the Purkinje cells (indicated with arrows),and milder reactivity with some synapses of the molecular layer.(Sections have been mildly counterstained with hematoxylin,400×.)
conceivably contribute to GAD immunity in a patientwith a prior history of another autoimmune disorder[10]. Finally, it is quite possible that the co-existenceof multiple myeloma and stiff-limb syndrome wasco-incidental. Extended follow-up on larger numbersof patients receiving thalidomide should shed light onthis potential association.
Acknowledgement
We appreciate the assistance of LB in acquiring thedata for the manuscript.
References
1. Barker RA, Revesz T, Thom M, Marsden CD, Brown P:Review of 23 patients affected by the stiff man syn-drome: clinical subdivision into stiff trunk (man) syndrome,stiff limb syndrome, and progressive encephalomyelitiswith rigidity. J Neurol Neurosurg Psychiatry 65: 633–640,1998
2. Meinck HM: Stiff man syndrome. CNS Drugs 15: 515–526,2001
3. Meinck HM, Thompson PD: Stiff man syndrome and relatedconditions. Mov Disorders 17: 853–866, 2002
4. Dropcho EJ: Antiamphiphysin antibodies with small-celllung carcinoma and paraneoplastic encephalomyelitis. AnnNeurol 39: 659–667, 1996
5. Butler MH, Hayashi A, Ohkoshi N, Villmann C, Becker CM,Feng G, De Camilli P, Solimena M: Autoimmunity togephyrin in Stiff-Man syndrome. Neuron 26: 307–312, 2000
6. Ferrari P, Federico M, Grimaldi LM, Silingardi V: Stiff-mansyndrome in a patient with Hodgkin’s disease. An unusualparaneoplastic syndrome. Haematologica 75: 570–572,1990
7. Sinnreich M, Assal F, Hefft S, Magistris MR, Chizzolini C,Landis T, Burkhard PR: Anti-GAD antibodies and breastcancer in a patient with stiff-person syndrome: a puzzlingassociation. Eur Neurol 46: 51–52, 2001
8. Rosin L, DeCamilli P, Butler M, Solimena M, Schmitt HP,Morgenthaler N, Meinck HM: Stiff-man syndrome in awoman with breast cancer: an uncommon central nervoussystem paraneoplastic syndrome. Neurology 50: 94–98,1998
9. Silverman IE: Paraneoplastic stiff limb syndrome. J NeurolNeurosurg Psychiatry 67: 126–127, 1999
10. Zhu J, Deng GM, Diab A, Zwingenberger K, Bakhiet M,Link H: Thalidomide prolongs experimental autoimmuneneuritis in Lewis rats. Scand J Immunol 48: 397–402,1998
Address for offprints: David Schiff, Box 800432, University ofVirginia Division of Neuro-Oncology, Charlottesville, VA 22908-0432, USA; Tel.: (434) 982-4415; Fax: (434) 982-4467; E-mail:[email protected]