Embed Size (px)
Citation preview

ANTERIOR VERSUS POSTERIOR WALKERS: A GAIT ANALYSIS STUDY
Lynne Logan Kathleen flyers-Hinkley Charles D. Ciccone
Therapeutic habilitation of young child- ren has often included the use of walkers as mobility aids (Bleck 1987). When properly prescribed and implemented, a walker can help provide mobility and enhance the ambulation skills of children with cerebral palsy, Down syndrome and similar developmental disabilities (Cusick 1980, Click and Davies 1985, Wilson 1988). Traditional walkers have four
d vertical legs, a horizontal bar in front of 0 the child, and horizontal bars on either 3 - side which also serve as hand-grips (Licht m- 1969). This type of walker can be
considered an ‘anterior’ walker, since the 0- OI child pushes it and walks behind it Q‘ (Fig. 1). There are numerous variations to 0 5 this traditional anterior design, including e fitting wheels on two or more of the legs,
varying the position of the hand-grips, providing forearm or trunk support, and
2 2 is adjusting the height, weight and shape of
the walker’s base (Finnie 1975, Bergen and Colangelo 1985).
.- One recurrent problem with anterior -u walkers is that the child often tends to 5 lean forward while pushing the walker k (Carmick 1985, Wilson 1988), and the
entire body is held in a forward, flexed position. This forward flexion can be quite pronounced, and excessive flexion
4 of the trunk, hips and other joints compromises the integrity and alignment
1044 of these joints. There is also an increased
00
m
-
2 QJ
2
\
2 . 3 z
tendency for the child to lose his balance and fall.
Recently walkers have been introduced which the child pulls along behind himself during ambulation i.e. ‘posterior’ walker (Fig. 2). These walkers have a horizontal bar at the rear and two horizontal bars which extend forward and serve as hand- grips. Preliminary clinical observations have suggested that children have a more erect, safer gait using a posterior walker. Some investigators have also postulated that the horizontal bar at the back pro- vides a facilitatory effect by striking the hip extensors while ambulating (Carmick 1985, Wilson 1988). However, there is little documented evidence that either type of walker offers any advantage in pro- viding improved posture, normalized gait pattern, or a safer means of ambulation.
The purpose of this investigation was to compare specific gait characteristics of children with developmental disabilities, while they ambulated with anterior and posterior walkers. In particular, we were interested in determining whether posterior walkers were associated with improved posture and a more typical gait pattern in these children.
Method Eight children (two females, six males) participated in the study, ranging in age from 2.5 to 8.0 years. Seven had
ri m
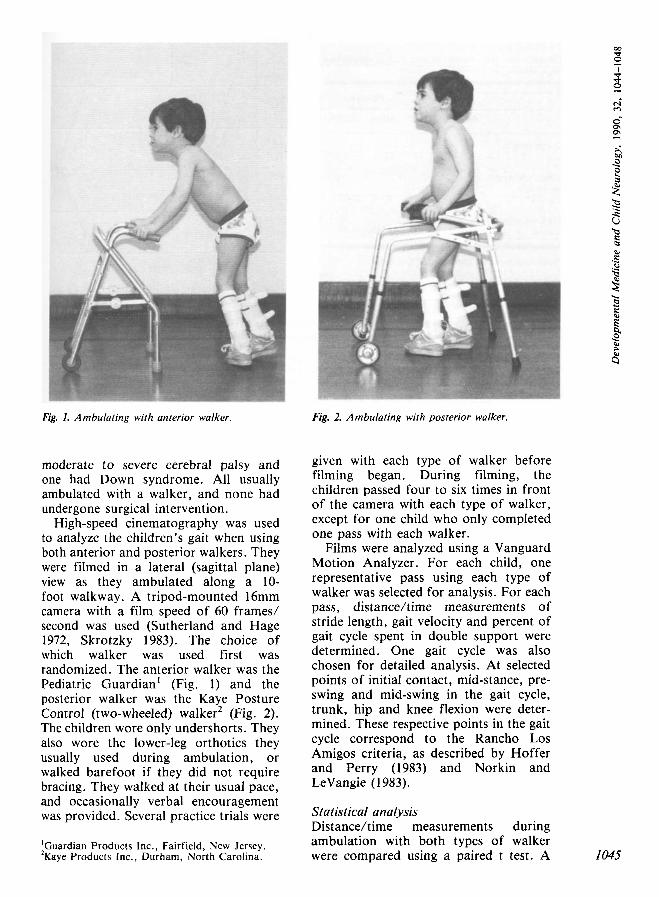
Fig. 1. Ambulating with anterior walker. Fig. 2. Ambulating with posterior walker.
moderate to severe cerebral palsy and one had Down syndrome. All usually ambulated with a walker, and none had undergone surgical intervention.
High-speed cinematography was used to analyze the children's gait when using both anterior and posterior walkers. They were filmed in a lateral (sagittal plane) view as they ambulated along a 10- foot walkway. A tripod-mounted 16mm camera with a film speed of 60 frames/ second was used (Sutherland and Hage 1972, Skrotzky 1983). The choice of which walker was used first was randomized. The anterior walker was the Pediatric Guardian' (Fig. 1) and the posterior walker was the Kaye Posture Control (two-wheeled) walker2 (Fig. 2). The children wore only undershorts. They also wore the lower-leg orthotics they usually used during ambulation, or walked barefoot if they did not require bracing. They walked at their usual pace, and occasionally verbal encouragement was provided. Several practice trials were
'Guardian Products Inc., Fairfield, New Jersey. 2Kaye Products Inc., Durham, North Carolina.
given with each type of walker before filming began. During filming, the children passed four to six times in front of the camera with each type of walker, except for one child who only completed one pass with each walker.
Films were analyzed using a Vanguard Motion Analyzer. For each child, one representative pass using each type of walker was selected for analysis. For each pass, distancekime measurements of stride length, gait velocity and percent of gait cycle spent in double support were determined. One gait cycle was also chosen for detailed analysis. At selected points of initial contact, mid-stance, pre- swing and mid-swing in the gait cycle, trunk, hip and knee flexion were deter- mined. These respective points in the gait cycle correspond to the Rancho Los Amigos criteria, as described by Hoffer and Perry (1983) and Norkin and LeVangie (1 983).
Statistical analysis Distanceltime measurements during ambulation with both types of walker were compared using a paired t test. A 1045
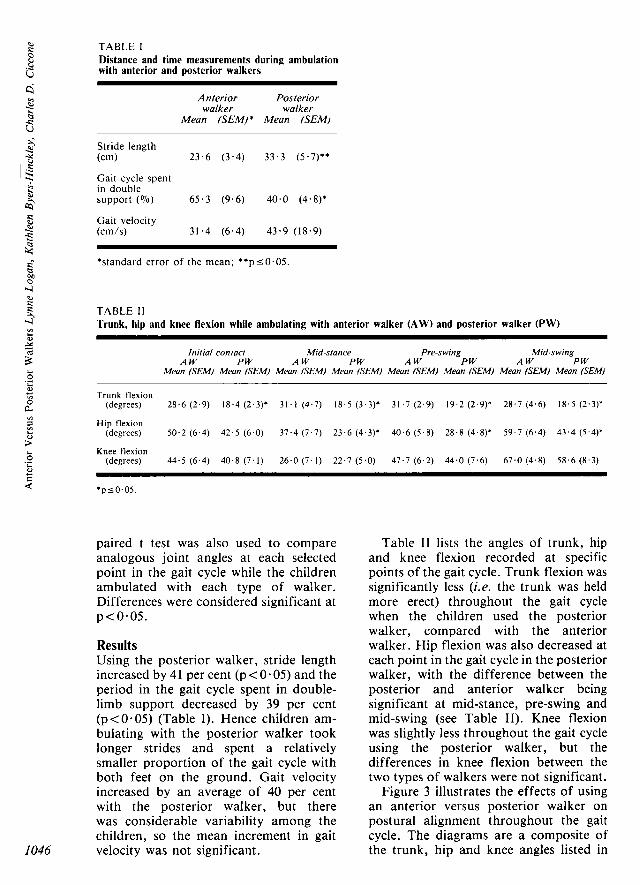
TABLE 1 Distance and time measurements during ambulation with anterior and posterior walkers
c j Anterior Posterior
walker walker Mean (SEM)* Mean (SEMI
Stride length (cm) 23 .6 (3 .4) 33.3 (5 .7)**
Gait cycle spent in double support ( 0 7 0 ) 65.3 (9.6) 40 .0 (4.8)*
Gait velocity (cm/s) 31.4 (6.4) 43 .9 (18.9)
*standard error of the mean; * * p ~ 0 . 0 5 .
TABLE I 1 Trunk, hip and knee flexion while ambulating with anterior walker (AW) and posterior walker (PW)
Initial contact Mid-stance Pre-swing Mid-swing A W PW A W PW A W PW A W PW
Mean (SEMI Mean (SEM) Mean (SEMI Mean (SEMI Mean (SEMI Mean (SEM) Mean (SEMI Mean (SEMI
Trunk flexion (degrees) 28 .6 (2 .9) 18.4 (2.3)* 31.1 (4 .7) 18.5 (3 .3)* 31.7 ( 2 . 9 ) 19.2 (2.9)' 28.7 (4 .6) 18.5 (2.3)'
Hip flexion
Knee flexion
(degrees) 50 .2 (6 .4) 42 .5 (6 .0) 37 .4 (7 .7) 23 .6 (4.3)' 4 0 . 6 (5 .8 ) 28 .8 (4.8). 5 9 . 7 (6 .4) 4 3 . 4 (5.4)*
(degrees) 44 .5 (6 .4) 40 .8 (7 .1) 26 .0 (7 .1) 22.7 (5.0) 47 .7 (6 .2) 4 4 . 0 (7 .6) 6 7 . 0 ( 4 . 8 ) 58 .6 (8 .3)
paired t test was also used to compare analogous joint angles at each selected point in the gait cycle while the children ambulated with each type of walker. Differences were considered significant at p < 0.05.
Results Using the posterior walker, stride length increased by 41 per cent (p < 0.05) and the period in the gait cycle spent in double- limb support decreased by 39 per cent (p<O.O5) (Table I). Hence children am- bulating with the posterior walker took longer strides and spent a relatively smaller proportion of the gait cycle with both feet on the ground. Gait velocity increased by an average of 40 per cent with the posterior walker, but there was considerable variability among the children, so the mean increment in gait
1046 velocity was not significant.
Table I1 lists the angles of trunk, hip and knee flexion recorded at specific points of the gait cycle. Trunk flexion was significantly less (Le. the trunk was held more erect) throughout the gait cycle when the children used the posterior walker, compared with the anterior walker. Hip flexion was also decreased at each point in the gait cycle in the posterior walker, with the difference between the posterior and anterior walker being significant at mid-stance, pre-swing and mid-swing (see Table 11). Knee flexion was slightly less throughout the gait cycle using the posterior walker, but the differences in knee flexion between the two types of walkers were not significant.
Figure 3 illustrates the effects of using an anterior versus posterior walker on postural alignment throughout the gait cycle. The diagrams are a composite of the trunk, hip and knee angles listed in
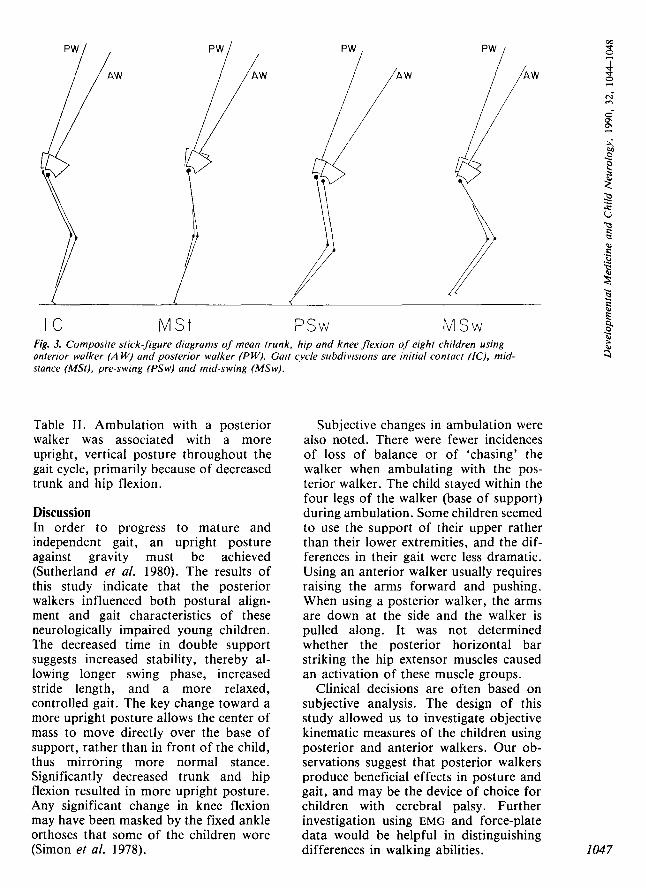
I C M S t PSW M S w Fig. 3. Composite stick-figure diagrams of mean trunk, hip and knee flexion of eight children using anterior walker (A W) and posterior walker (PW). Gait cycle subdivisions are initial contact (IC), mid- stance (MSt), pre-swing (PSw) and mid-swing (MSw).
Table 11. Ambulation with a posterior walker was associated with a more upright, vertical posture throughout the gait cycle, primarily because of decreased trunk and hip flexion.
Discussion In order to progress to mature and independent gait, an upright posture against gravity must be achieved (Sutherland et al. 1980). The results of this study indicate that the posterior walkers influenced both postural align- ment and gait characteristics of these neurologically impaired young children. The decreased time in double support suggests increased stability, thereby al- lowing longer swing phase, increased stride length, and a more relaxed, controlled gait. The key change toward a more upright posture allows the center of mass to move directly over the base of support, rather than in front of the child, thus mirroring more normal stance. Significantly decreased trunk and hip flexion resulted in more upright posture. Any significant change in knee flexion may have been masked by the fixed ankle orthoses that some of the children wore (Simon et al. 1978).
Subjective changes in ambulation were also noted. There were fewer incidences of loss of balance or of ‘chasing’ the walker when ambulating with the pos- terior walker. The child stayed within the four legs of the walker (base of support) during ambulation. Some children seemed to use the support of their upper rather than their lower extremities, and the dif- ferences in their gait were less dramatic. Using an anterior walker usually requires raising the arms forward and pushing. When using a posterior walker, the arms are down at the side and the walker is pulled along. It was not determined whether the posterior horizontal bar striking the hip extensor muscles caused an activation of these muscle groups.
Clinical decisions are often based on subjective analysis. The design of this study allowed us to investigate objective kinematic measures of the children using posterior and anterior walkers. Our ob- servations suggest that posterior walkers produce beneficial effects in posture and gait, and may be the device of choice for children with cerebral palsy. Further investigation using EMG and force-plate data would be helpful in distinguishing differences in walking abilities. 1047
c j
I048
Accepted for publication 3rd May 1990. Special Children’s Center, Inc.; Lecturer, Depart- ment of Physical Therapy, Ithaca College, lthaca,
Authors’ Appointments New York. *Charles Ciccone, P.T., Ph.D., Associate Kathleen Byers-Hinkley, M.S., P.T., Physical Professor, Department of Physical Therapy, lthaca Therapist, The Special Children’s Center, Inc., College, School of Physical Therapy, Ithaca, New York 14850. Lynne Logan, M.A., P.T., Physical Therapist, The
Ithaca, New York.
*Correspondence to first author.
SUMMARY Eight children, who needed walkers to ambulate and who were able to use either anterior or posterior walkers, were selected for a comparative study of both types of walker. Data for gait analysis, using high-speed cinematography, were collected to determine stride length, time in double support and velocity. Trunk, hip and knee angles were also measured during four phases of the gait cycle. The results demonstrated significant improvements in both postural alignment and gait characteristics with the posterior walker.
RESUME Deambulateurs anterieurs ou posterieurs pour les enfants: etude analyfique de la demarche Huit enfants ayant besoin d’un deambulateur pour se deplacer et pouvant utiliser des deambulateurs anterieurs ou posterieurs, ont ete choisis pour une etude comparative des deux types de deambulateur. Des donnees d’analyse de la demarche, utilisant le cinema a grande vitesse, ont ete recueillies pour determiner la longueur du pas, le temps de double appui et la vitesse. Les angles du tronc, des hanches et des genoux ont ete tgalement mesures durant quatre phases du cycle de la demarche. Les resultats demontrerent des ameliorations significatives a la fois dans l’alignement postural et les caractkristiques de la demarche avec le deambulateur posterieur.
ZUSAMMENFASSUNG Anteriore und posteriore Gehhilfen fur Kinder: eine Ganganalyse Acht Kinder, die Gehhilfen brauchten und die sowohl anteriore oder posteriore Gehhilfen benutzen konnten, wurden fur eine Vergleichsstudie der beiden Gehhilfearten ausgesucht. Mit der Hochgeschwindigkeits-Cinematographie wurden Daten fur die Ganganalyse gesammelt, um die Schrittlange und die Zeit fur Abstutzung und Geschwindigkeit zu bestimmen. Aunerdem wurden Rumpf-Hiift- und Kniewinkel in vier Schrittphasen gemessen. Die Ergebnisse zeigten bei der Benutzung der posterioren Gehhilfen eine signifikante Besserung der Korperhaltung, sowie der Gangcharakteristika.
RESUMEN Andadores anteriores frente a posteriores en niiios: estudio analitico de la marcha Ocho niilos que necesitaban andadores para ambular y eran capaces de usar igualmente andadores anteriores o posteriores fueron seleccionados para un estudio comparativo entre ambos grupos de andadores. Se recogieron datos para el analisis de la marcha con cinema de aka velocidad para determinar la longitud de la zancada, el tiempo en soporte doble y la velocidad. Tambien se midieron el tronco, cadera, rodilla y tobillos en las cuatro fases del ciclo de la marcha. Los resultados mostraron mejorias significativas tanto en el alineamiento, como en las caracteristicas de la marcha usando un andador posterior.
References Bergen, A., Colangelo, C. (1985) Positioning of the
Client With Central Nervous System Deficits, 2nd Edn. Valhalla, NY: Valhalla Rehabilitation.
Bleck, E. E. (1987) Orthopaedic Management in Cerebral Palsy. Clinics in Developmental Medicine, Nos. 99-100. London: Mac Keith Press with Blackwell Scientific; Philadelphia: Lippincott.
Carmick, J. (1985) ‘Alternative standing and ambulating support.’ Totline, 2, 20.
Click, M., Davies, J. (1985) Moving Right Along. Developmental Goals for Physically Disabled Children. Mesa, AZ: Edcorp Publications.
Cusick, B. D. (1980) ‘Developmental programs for children in below-knee casts.’ In Wilson, J . M. (Ed.) Orthopedic Aspects of Developmental Disabilities. Chapel Hill, NC: University of North Carolina at Chapel Hill.
Finnie, N. R. (1915) Handling the Young Cerebral Palsied Child at Home. New York: Dutton.
Hoffer, M . M., Perry, J. (1983) ‘Pathodynamics of gait alterations in cerebral palsy and the significance of kinetic electromyography in evaluating foot and ankle problems.’ Foot and
Ankle, 4, 128-134. Licht, E. (1969) Therapeutic Exercise. Baltimore:
W averly . Norkin, C., LeVangie, P. (1983) ‘Gait.’ In Joint
Structure and Function: a Comprehensive Analysis. Philadelphia: Davis.
Simon, S. R., Deutsch, S. D., Nuzzo, R. M., Mansour, M. J., Jackson, J . L., Koskinen, M., Rosenthal, R. K. (1978) ‘Genu recurvatum in spastic cerebral palsy.’ Journal of Bone and Joint Surgery, 60A, 882-894.
Skrotzky, K. (1983) ‘Gait analysis in cerebral palsied and nonhandicapped children.’ Archives of Physi- cal Medicine and Rehabilitation, 64, 291-295.
Sutherland, D. H., Hage, J . L. (1972) ‘Measure- ments of gait movements from motion picture film.’ Journal of Bone and Joint Surgery, 54A,
Olshen, R., Cooper, L., Woo, S. L.-Y. (1980) ‘The development of mature gait.’ Journal of Bone and Joint Surgery, 62A, 336-353.
Wilson, J. (1988) ‘Selecting and using qosture walkers for children with cerebral palsy. Totline, 14, 15-16.
181-797. -







![Intracranial Solitary Fibrous Tumor - Ghent University · ventricles, falx cerebri, and posterior fossa [2]. Symptoms associated with an ISFT are headache, gait disturbance and imbalance,](https://img.pdfslide.us/doc/110x75/5c9f141588c993452d8cb165/intracranial-solitary-fibrous-tumor-ghent-university-ventricles-falx-cerebri.jpg)