Embed Size (px)
Citation preview

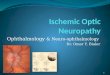
ANTERIOR ISCHEMIC OPTIC NEUROPATHY
(AION)
Jagdish Dukre

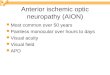
INTRODUCTION Anterior ischemic optic neuropathy (AION) is the most
common cause of acute optic neuropathy in older age groups.
AION is a potentially blinding disorder. Field defects typical of ischemic optic neuropathy were
first described by Knapp in 1875. Miller and Smith first used the term ʺischemic optic
neuropathyʺ in 1966, and Hayreh later added the term ʺanterior.ʺ
In 1924, Uhthoff first described severe visual loss, with field defects and swollen optic discs.

Clinical Features AION presents with rapid onset of painless, unilateral visual
loss manifested by decreased visual acuity, visual field, or both.
The level of visual acuity impairment varies widely, from minimal loss to no light perception, and the visual field loss may conform to any pattern of deficit related to the optic disc.
An altitudinal field defect is most common, but generalized depression, broad arcuate scotomas, and cecocentral defects also are seen.
A relative afferent pupillary defect invariably is present with monocular optic neuropathy.

The optic disc is edematous at onset, and edema occasionally precedes visual loss by weeks to months.
Although pallid edema has been described as the hallmark of AION, it is common to see hyperemic swelling, particularly in the nonarteritic form.

The disc most often is swollen diffusely, but a segment of more prominent involvement frequently is present, and either focal or diffuse surface telangiectasia is not unusual and may be quite pronounced.
Commonly, flame hemorrhages are located adjacent to the disc, and the peripapillary retinal arterioles frequently are narrowed.

Clinical Classification of AION
Depending upon the underlying cause, AION is of two types
1) Arteritic : This is the most serious type and is due to giant cell arteritis.
2) Non-arteritic: This is the most common one, and consists of all cases other than those due to giant cell arteritis.

Arteritic Anterior Ischemic Optic NeuropathyAAION

Pathogenesis AAION results from short posterior ciliary artery
(SPCA) vasculitis and the resultant optic nerve head infarction.
Human autopsy studies of acute AAION show optic disc edema with ischemic necrosis of the prelaminar, laminar, and
retrolaminar portions of the nerve and infiltration of the SPCAs by chronic inflammatory cells.
Segments of these vessels in some cases were occluded by inflammatory thickening and thrombus.

Fluorescein angiographic data support the histopathological evidence of involvement of the SPCAs in AAION.
Delayed filling of the optic disc and choroid is a consistent feature
extremely poor or absent filling of the choroid has been depicted as a characteristic of AAION
It has been suggested as one useful factor by which to differentiate AAION from NAION.
Delayed completion of choroidal fluorescein filling that averages 30–69seconds has been reported in AAION, compared with a mean of 5–13seconds in NAION.

Ocular Manifestations Typically, AAION develops in elderly patients, with a
mean age of 70years, with severe visual loss (visual acuity < 6/60 in the majority).
AAION is almost three times more common in women than in men.
It may be preceded by transient visual loss similar to that of carotid artery disease and when present, is highly suggestive of arteritis.
Pallor, which may be severe, chalky-white, is associated with the edema of the optic disc more frequently in AAION than in the nonarteritic form.

Choroidal ischemia may be associated with the optic neuropathy and produces peripapillary pallor and edema deep to the retina.
The disc of the fellow eye is of normal diameter most frequently, with a normal physiological cup.

In 5–10% of cases, AION may occur as a manifestation of the vasculitis associated with temporal arteritis.
Patients with the arteritic form usually note other symptoms of the disease – headache (most common), jaw claudication, and temporal artery or scalp tenderness
Malaise, anorexia, weight loss, fever, proximal joint arthralgia, and myalgia also are noted commonly.

However, the disease occasionally manifests with visual loss in the absence of overt systemic symptoms, so-called occult temporal arteritis.
the superficialtemporal artery is pulseless, nodular and thickened

Diagnosis The most important early step in the management of AION is
the differentiation of the arteritic from the nonarteritic form of the disease.
Active temporal arteritis usually is associated with an elevation of ESR to 70–120mm/hour, and in acute AION that is associated with other typical features, this finding suggests the arteritic form.
Abnormally high readings occur normally with increasing age and with other diseases, most commonly occult malignancy, other inflammatory disease, and diabetes.
Measurement of serum C-reactive protein (CRP), another acute-phase plasma protein, may aid in diagnosis.
Hayreh et al. reported 97% specificity for temporal arteritis in cases of AION in which both ESR >47mm/hour and CRP >2.45mg/dL were found.

Confirmation of the diagnosis of temporal arteritis is by superficial temporal artery biopsy.
Positive biopsy findings, such as intimal thickening, internal limiting lamina fragmentation, and chronic inflammatory infiltrate with giant cells, provide support for long-term systemic corticosteroid therapy.
A negative biopsy result, however, does not rule out arteritis; both discontinuous arterial involvement (“skip lesions”) and solely contralateral temporal artery inflammation may result in false-negative results.

Treatment Early treatment of AAION is essential and must be
instituted immediately in any suspected case of temporal arteritis.
High-dose systemic corticosteroids are standard.
intravenous methylprednisolone at 1g/day for the first 3 days has been recommended for AAION when the patient is in the acute phase of severe involvement.
Oral prednisone in the range of 60–100mg/day may be used initially and for follow-up to intravenous pulse therapy.

alternate day regimens do not suppress the disease effectively.
Treatment usually reduces systemic symptoms within several days.
A positive response is so typical that if it does not occur, an alternate disease process should be considered.
Treatment is usually continued at high dose for several months before beginning taper.

Course and Outcome The major goal of therapy in AAION is to prevent visual
loss in the fellow eye. Untreated, such involvement occurs in 54–95% of cases,
typically within 4months. With corticosteroid therapy, the rate of such
breakthrough is reduced to an estimated 13%. Prognosis for visual recovery in the affected eye that has
treatment generally is poor, but Recent reports suggest a 15–34% improvement rate,
which is higher with intravenous than with oral therapy. Worsening of vision in spite of therapy has been reported
in 9–17% of cases.

Nonarteritic Anterior Ischemic Optic Neuropathy
(NAION)

Pathogenesis The rapid onset, stable course with generally poor
recovery, association with vasculopathic risk factors, and similarity to AAION have implied a vascular cause for NAION as well, but the direct evidence remains limited.
Several histopathological reports document laminar and retrolaminar infarction, but cases of uncomplicated NAION are rare, and none has confirmed vasculopathy within the SPCAs or their distal branches.
The most commonly proposed pathogenic theory states that insufficiency of the optic disc circulation, exacerbated by structural crowding of nerve fibers and supporting structures at the nerve head, eventually reaches a point at which inadequate oxygenation produces ischemia and swelling of the disc.

These features may be mild and subclinical (no visual loss), reversible to some degree, or irreversible (infarction).
In some cases, a cycle of ischemia, axonal swelling, microvascular compression, and further ischemia may lead to progressive nerve damage.
Knox et al. have recently documented cavernous degeneration within ischemic regions of the optic nerve head, with distortion of adjacent axons, theorizing that this process may be responsible for the progressive course in some cases.
Periodic nocturnal systemic hypotension and the location of the optic disc in a watershed zone between distributions of lateral and medial SPCAs may be contributing factors.

Fluorescein angiographic studies in NAION also suggest impaired optic disc perfusion.
Detailed quantitative analysis of prelaminar optic disc and peripapillary choroidal filling in NAION confirms significantly delayed disc filling when compared with age-matched controls.
Delay in a segment of disc by at least 5 seconds, was present in 75.6% of such cases.
FFA (AAION) early AV phase. The temporal portion of the optic disc fills normally (small arrows), but the remaining sectors demonstrate markedly delayed filling (large arrows) approximately 10 seconds later.

In contrast, peripapillary choroidal filling was not delayed consistently and not significantly more than the degree of segmental delay often found in normal subjects.
These findings suggest that the impaired flow to the optic nerve head in NAION is distal to the SPCAs themselves, possibly at the level of the paraoptic branches that supply the optic nerve head directly
FFA (AAION) early AV phase. The temporal portion of the optic disc fills normally (small arrows), but the remaining sectors demonstrate markedly delayed filling (large arrows) approximately 10 seconds later.

Ocular Manifestations In 90–95% of cases, AION is unrelated to temporal
arteritis. The nonarteritic form of the disease occurs in a relatively
younger age group (mean age of 60years) and usually is associated with less severe visual loss.
Frequently, visual impairment is reported upon awakening, possibly related to nocturnal systemic hypotension.
The initial course of visual loss may be
a) static (with little or no fluctuation of visual level after the initial loss) or
b) progressive (with either episodic or visual loss that declines steadily over weeks to months prior to eventual stabilization).

The progressive form has been reported in 22% to 37%
of NAION cases.
Usually, no associated systemic symptoms occur, although periorbital pain is described occasionally.
Fellow eye involvement is estimated to occur in 12–19% by 5years after onset.
Recurrent episodes of visual loss that result from NAION in the same eye are unusual and occur most often in younger patients.

The optic disc edema in NAION may be diffuse or segmental, hyperemic or pale, but pallor occurs less frequently than it does in AAION.
A focal region of more severe swelling often is seen but it does not correlate consistently with the sector of visual field loss.
The hyperemic disc edema is more prominentsuperiorly. Focal surface telangiectasia of disc vessels is seen superotemporally (arrows).

Diffuse or focal telangiectasia of the edematous disc may be present, occasionally prominent enough to resemble a vascular mass or neovascularization.
This finding may represent microvascular shunting from ischemic to nonischemic regions of the optic nerve head, so-called luxury perfusion.
The hyperemic disc edema is more prominentsuperiorly. Focal surface telangiectasia of disc vessels is seen superotemporally (arrows).

The optic disc in the contralateral eye typically is small in diameter and demonstrates a small or absent physiological cup.
The disc appearance in such fellow eyes has been described as the disc at risk, with postulated structural crowding of the axons at the level of the cribriform plate, associated mild disc elevation, and disc margin blurring without overt edema
Fellow eye in AAION. The optic disc is small in diameter, with absent physiological cup and slight blurring of the nasal margin.

Systemic Associations NAION has been reported in association with a number of
diseases that could predispose to reduced perfusion pressure or increased resistance to flow within the optic nerve head.
In NAION patients 47% of patients have hypertension and 24% have diabetes.
Repka et al. indicated that the prevalences of both hypertension and diabetes are increased over those of the control population in NAION patients in the age range 45–64years, but that in patients over 64years of age, no significant difference exists from those of the general population.
Diabetics in particular show a predisposition to NAION at a young age.

Also, NAION has been reported in association with multiple forms of vasculitis, acute systemic hypotension, migraine, optic disc drusen, and idiopathic vaso-occlusive diseases.
Other risk factors, such as hyperopia, smoking, the presence of HLA A29, and hyperlipidemia have been proposed.
Among these, nocturnal arterial hypotension (i.e. fall of blood pressure during sleep) seems to play a very important role in the development of non-arteritic AION and is often considered a precipitating factor.
Recent reports of the association of hyperhomocystinemia with AION, particularly in patients under 50, are inconclusive.
Prothrombotic risk factors, such as protein C and S and antithrombin III deficiencies, factor V Leiden mutation, and cardiolipin antibodies, do not seem to be associated with AION

Treatment There is no proven effective therapy for NAION.
Oral corticosteroids at standard dosage (1mg/kg per day) are not beneficial, and megadose intravenous therapy has not been evaluated systematically.
Optic nerve sheath decompression (ONSD) surgery has been attempted,
It was based on the theory that reduction of perineural subarachnoid cerebrospinal fluid pressure might improve local vascular flow or axoplasmic transport in the optic nerve head, and thus reduce tissue injury in reversibly damaged axons.

The Ischemic Optic Neuropathy Decompression Trial compared ONSD surgery in 119 patients with no treatment in 125 controls.
The study revealed no significant benefit for treatment and; it was recommended that ONSD not be performed
Hyperbaric oxygen, by marked elevation of the dissolved oxygen content in the blood, provides increased tissue oxygenation that might reduce damage in reversibly injured axons.
A controlled clinical pilot study of hyperbaric oxygen in 22 patients who had acute NAION, however, has shown no beneficial effect.
Neuroprotective agents have shown a beneficial effect in animal models of optic nerve damage, but are not proven to be effective in NAION.
The effect of aspirin in reducing risk of fellow eye involvement is unclear.

Course and Outcome
The course of untreated NAION varies considerably.
Reports indicate that 24–43% of cases demonstrate spontaneous improvement of visual acuity by three Snellen lines or more.
Even in the progressive form, improvement has been reported to occur in roughly 30%.
Whether NAION is static or progressive, visual acuity and field stabilize after several months.

Within 6weeks, occasionally sooner, the optic disc becomes visibly atrophic, either in a sectorial or diffuse pattern.
Further progression or recurrent episodes are extremely rare after 2months and, if present, should prompt evaluation for another cause of optic neuropathy.
2 months after onset of inferior visual field loss, is segmentally atrophic superiorly (arrows), with sparing and resolving edema inferiorly.


Thank You …