Embed Size (px)
Citation preview

Sports Med 2003; 33 (6): 455-471INJURY CLINIC 0112-1642/03/0006-0455/$30.00/0
© Adis Data Information BV 2003. All rights reserved.
Anterior Cruciate Ligament Injury inPaediatric and Adolescent PatientsA Review of Basic Science and Clinical Research
Kevin G. Shea,1 Peter J. Apel1 and Ronald P. Pfeiffer2
1 Intermountain Orthopaedics, Boise, Idaho, USA2 Department of Kinesiology, Boise State University, Boise, Idaho, USA
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4551. Risk Factors and Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4562. Natural History of Non-Reconstructive Management of Anterior Cruciate Ligament (ACL) Injuries 4563. Animal Studies, Mechanisms of Physeal Arrest and Growth Abnormalities . . . . . . . . . . . . . . . . . . . . . . 458
3.1 Bony Bar Formation and Hardware Placement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4583.2 Tenodesis Effect . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 461
4. Anatomy of the Proximal Tibia and Distal Femoral Physes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4625. Reported Complications After ACL Reconstruction in Skeletally Immature Patients . . . . . . . . . . . . . . 4636. Methods of ACL Reconstruction in Skeletally Immature Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 464
6.1 Physeal Sparing Techniques: Both Tibial and Femoral . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4646.2 Physeal Sparing Techniques: Femoral Side Only . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4676.3 Non-Physeal Sparing Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 468
7. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 469
Anterior cruciate ligament (ACL) injuries are recognised with greater frequen-Abstractcy in children and adolescents. Non-operative treatment of ACL injuries inchildren may lead to knee instability and secondary injuries, especially in thosewho return to sports. ACL reconstruction is controversial in skeletally immaturepatients because of potential damage to the proximal tibial and distal femoralphyses, which may lead to premature arrest and/or leg length discrepancies. Thispaper reviews studies of ACL injuries in children and adolescents, and examinesbasic science and clinical studies concerning physeal arrest secondary to ACLreconstruction tunnels. Some animal studies support the conclusion that ACLreconstructions in children have the potential to cause growth disturbances, andthere are reports of growth plate complications due to ACL reconstruction inskeletally immature patients. There is evidence that ACL reconstruction can beperformed in select skeletally immature patients, but the risk of growth platecomplications must be considered.

456 Shea et al.
1. Risk Factors and Epidemiology girls again had higher overall knee injury rates, kneesurgery rates, as well as knee surgery for ACL injury
Historically, mid-substance tears of the anterior (3.41 times as high for girls vs boys).cruciate ligament (ACL) have been considered rare Numerous factors have been identified as possi-in children and adolescents. Tibial spine avulsion ble causes of the difference in ACL injury rateinjuries are considered more common, but avulsions between males and females,[7,9] including athleticof the femoral attachment have also been report- technique, muscular strength, shoe-surface inter-ed.[1-4]
face, skill level,[10] joint laxity,[11] limb alignment,Recent studies have reported ACL tears in young notch dimensions,[12-14] hormonal/menstrual fac-
patients, especially in the adolescent age group; tors,[15,16] and ligament size. Currently, this is anhowever, there have been few epidemiological stud- area of active research.ies on the incidence of ACL injuries in paediatricand adolescent populations. Micheli et al.[5] reported 2. Natural History of Non-Reconstructiveon a retrospective review of ACL surgeries per- Management of Anterior Cruciateformed from 1992–1997 at a Boston hospital. They Ligament (ACL) Injuriesfound that the frequency of ACL injuries over the5-year period correlated with an increase in the level The natural history of non-reconstructive man-of participation in sports over the same period. In agement of ACL injuries has been well documentedaddition, they found that females were more likely in adult and skeletally immature athletes.[17-24] Non-to experience an ACL injury than males. reconstructive treatment has been shown to produce
unsatisfactory results and often leads to further me-Shea et al.[6] reported an analysis of 8215 insur-niscus and osteochondral injuries. Although non-ance claims filed on behalf of approximately 6 mil-operative treatment may be successful for childrenlion youth soccer players in the US. They noted thatwho do not desire a high level of activity,[20] or inclaims for ACL injuries were filed for children aschildren who will limit their activities and use ayoung as 12 (female) and 5 (male) years old. Fur-brace until they are older,[25] competitive athletesther, they noted that 31% of all claims for kneeand active adolescents are likely to have poor kneeinjuries in females were for ACL injury with 24% offunction with an ACL-deficient knee.all knee injury claims for ACL injury in males. The
The first report on the natural history of untreatedoverall ratio of ACL injury claims to total injuryACL injuries in adolescents was in 1988 by McCar-claims was consistently higher for the females com-roll et al.[21] They reported on the outcome of 16pared with their male counterparts beginning at agepatients with documented ACL tears who were12 years.treated conservatively with rehabilitation, bracingStudies in adult and adolescent patients have alsoand counselling. They found that after an average ofshown that females have a higher risk of ACL27 months, all had recurrent instability. In 1989,injury. Arendt and Dick[7] examined 5 years of dataAngel and Hall[18] reported on 27 patients treatedprovided by the National Collegiate Athletic Asso-conservatively. After an average follow-up of 51ciation and found female basketball and soccer play-months, 15 (55%) had recurrent instability.ers to have significantly higher rates of ACL injuries
Mizuta et al.[23] found instability in 17 of 18compared with males playing the same sports. Pow-patients who underwent conservative treatment at anell and Barber-Foss[8] examined high school data foraverage of 51 months follow-up; Aichroth et al.[17]the 3-year period from 1995–1997 across all sports.found instability in 23 of 23 patients treated withWhen they examined the injury data for both basket-rehabilitation and bracing after an average of 72ball and soccer they found that in basketball the girlsmonths follow-up.had higher rates of knee injury, knee surgery and
surgery for ACL injury (four times as high for girls Graf et al.[19] reported on eight patients who werevs boys). The results in soccer were similar in that treated conservatively, all complaining of instability
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

ACL Injury in Paediatric and Adolescent Patients 457
at follow-up, with the first episode of instability active or who sought to be more active (Tegnerscore ≥7) were less likely to benefit from conserva-being reported at an average of 7 months. Thesetive treatment and were more likely to go on topatients were evaluated at the time of injury andsurgery than those who had a Tegner score of ≤6.again after an average of 15 months. Seven of the
eight patients had a documented meniscal injury at It was also noted that the group who went on tofollow-up, but unfortunately, pre-treatment docu- surgery were on average 1.4 years older (11.9 vsmentation of meniscal injuries was incomplete. Graf 13.3 years). This difference was shown be an influ-et al. performed arthrograms in six of eight patients encing factor in the decision to go on to surgery,and arthroscopy in only three. although its role was less influential than activity
level. The authors conjectured that younger patientsThe most comprehensive study on the naturalwere more easily able to accommodate an unstablehistory of ACL tears in skeletally immature patients,knee and to modify their recreational activities ac-knee instability and meniscal injury was completedcordingly.by McCarroll et al.[22] in 1994. They reported on 38
athletes who were treated conservatively with activ- Recently, Kocher et al.[27] examined the function-ity modification and bracing. All patients were al outcome of a cohort of adolescents (n = 45) 17examined arthroscopically before treatment to iden- years of age or younger who were diagnosed withtify and repair meniscus tears. All 38 patients under- partial ACL tears as evidenced by way of: (i) MRIwent arthroscopically assisted ACL reconstruction signal changes; (ii) Lachman grade A or B, andat a later point and meniscal injuries were docu- pivot shift of grade A or B; or (iii) arthroscopicmented at that time. Thirty-seven patients (97%) had evidence of a partial tear. It should be noted that allepisodes of instability prior to ACL reconstruction, subjects presented with acute haemarthrosis on ini-and 27 of 38 (71%) had symptomatic meniscal tears tial examination. None of the subjects underwentat the time of surgery. Before reconstruction, only reconstructive management initially; however, they16 of 38 (50%) had attempted to return to their were treated with a hinged brace (to prevent passiveprevious level of activity. terminal extension for 6 weeks followed by active
terminal extension for 12 weeks). Average length ofJanarv et al.[20] investigated the causes for thefollow-up time was 6.1 years. A total of 14 subjectsfailure of conservative treatment by examining pati-(31%) underwent subsequent reconstructive proce-ents’ desired and actual activity levels using thedures, and in this group, significant associationsscoring system developed by Tegner andwere found between the need for surgery and tearsLysholm.[26] Janarv et al.[20] reported on 22 adoles-of greater than 50%, tears of the posterolateral bun-cents with ACL tears who were initially treateddle, grade B pivot shift, and older chronological andconservatively with rehabilitation. Fifteen patientsskeletal age. Kocher, et al.[27] recommend non-re-later elected to have surgery after an average of 19constructive management of partial ACL tears inmonths of conservative treatment. The decision topatients 14 years of age or younger who test atperform surgery was based on the patient’s instabili-normal or near-normal Lachman and pivot shiftty problems, desired activity level and the presenceexaminations.of new or emerging meniscal injuries. The seven
patients who did not elect to have surgery incurred Most studies of the natural history of ACL injuryno meniscal injuries in the 3–5 year follow-up in young patients consistently show that conserva-period. The Tegner scores of the seven patients who tively treated patients develop knee instability (tabledid not elect to have surgery were compared with I). This instability is likely to lead to secondarythose of the 15 patients who did go on to surgery. chondral or meniscal injuries if activity levels areThey found that patients’ desired and actual levels not modified. Woods and O’Connor[25] conducted aof activity were the strongest indicator for failure of retrospective case-controlled study of adolescent pa-conservative treatment. Adolescents who were more tients with ACL tears to assess the rate of additional
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

458 Shea et al.
Table I. Summary of natural history studies of anterior cruciate ligament injury
Study Year No. of patients Follow-up (mo) Instability (%) Meniscus tears (%)
McCarroll et al.[21] 1988 16 27 16/16 (100) NA
Angel and Hall[18] 1989 27 51 15/27 (55) NA
Graf et al.[19] 1992 8 24 8/8 (100) 7/8 (87)
McCarroll et al.[22] 1994 38 29 37/38 (97) 27/38 (71)
Mizuta et al.[23] 1995 18 51 17/18 (94) NA
Aichroth et al [17] 2002 23 72 23/23 (100) NA
Kocher et al.[27] 2002 45 (partial tears) 73 0/45 (All were Lachman A or B) 17/45 (38)NA = data not available.
knee injuries after delaying reconstruction until clo- immature may lead to partial or total physeal arrest;sure of tibial tubercle physis. Specifically, two either by the formation of bony bridges, the place-groups were compared with 32 age-matched con- ment of hardware or by tension across the physis.trols that had undergone ACL reconstructions after
3.1 Bony Bar Formation andtibial physis closure. Thirteen age-matched subjectsHardware Placementwith open tibial physes (‘physeal group’) followed a
regime of restricted sports activities, as well as worePhemister[39] reported in 1933 on a technique ofa derotation brace. A second age-matched, ‘delayed
intentional epiphysiodesis by excision ofgroup’ of 12 subjects with closed physes and notransphyseal sections of bone, curettage of theactivity restriction or derotation bracing was alsoepiphysis, and reimplantation of the inverted boneexamined. The results indicated that when comparedblock. In 1950, Haas[36] showed that the placementwith the control group, the rate of additional kneeof metal pins diagonally across the epiphysis ofinjuries in the physeal group did not differ signifi-rabbits caused growth disturbances. They noted thatcantly from the control group. However, the delayedmetal pins placed across the physis would not causegroup experienced a greater number of additionalgrowth disturbances if they were removed promptly.knee injuries, primarily medial meniscus tears.Haas[36] also discovered that pins placed across oneMany young patients, especially athletes, have aside of the physis caused angular deformities bystrong desire return to sports or refuse the limita-inducing partial growth arrest.tions of conservative treatment. Each of these stud-
Campbell and Zanconato[28] reported in 1959 thaties reported associated meniscal tears and other inju-variations in fixation devices and tunnel fillingsries in select patients, but none were able to confirmwere important factors in the degree of growth arrestthe absence of meniscal injuries by MRI or arthros-induced. Using the distal femoral physis of dogs,copy before starting conservative treatment.they examined holes of various diameters, that were:(i) left empty; (ii) filled with a cortical bone plug;3. Animal Studies, Mechanisms of(iii) filled with beeswax; (iv) filled with a smoothPhyseal Arrest andpin; and (v) filled with a threaded pin. They foundGrowth Abnormalitiesthat large drill holes, threaded pins, bone plugs, or
Various studies have been performed on the empty tunnels caused growth arrest or retardation.physes of animals in order to define the effects of Smooth pins and holes filled with beeswax did nottrauma, pressure and ligament reconstruction on affect growth, and smaller holes tended to have lessgrowing physes. Elements of ACL reconstruction effect overall than larger holes. Histologically, theythat have been examined are drill hole size,[28-32] the found that a physis would continue to grow if thereplacement of soft tissue grafts,[33-35] hardware place- was no osseous bridge between the epiphysis andment[28,36,37] and graft tension.[38] These studies have metaphysis, or if the bridge was relatively small inshown that ACL reconstruction in the skeletally diameter. They noted that eight to ten holes of
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

ACL Injury in Paediatric and Adolescent Patients 459
0.45mm in diameter, even though filled with osse- area of the physis caused permanent growth distur-ous tissue, would not retard growth, presumably bance and femoral shortening. In 1994, Guzzanti etbecause these bony bridges lacked the collective al.,[30] also studying rabbits, found that 3% damagetensile strength to halt the growing physis. to the cross-sectional area of the distal femoral
epiphysis did not cause physeal arrest, but that 4%In 1956, Ford and Key[29] examined the effects ofdamage to the proximal tibial physis did result intrauma to the distal femoral epiphysis of rabbits.shortening and valgus deviation. These researchersThey found that trauma to the peripheral region wasthen filled their drill holes with the semitendinosusmore likely to cause damage than holes drilled at thetendon left attached distally, threaded through thecentre of the physis. They found that a 3.175mm (1/tibial and femoral tunnels and sutured to the perios-8 inch) drill hole placed centrally across the femoralteum of the lateral femoral metaphysis. At the time,epiphysis of rabbits did not cause growth distur-it was unknown how the placement of ligamentsbances, but that the same size hole and curettage ofwithin the tunnels affected bony bridge strength andthe physis did cause growth arrest. They also show-growth arrest.ed that curettage of the lateral aspect of a physis
caused arrest and angular deformities, and that peri- In 1995, Stadelmaier et al.[35] showed that thepheral damage was more likely to cause angular placement of fascia lata autograft within 5/32 inchdeformities than a more centralised drill hole. Ford (~4mm) transphyseal tunnels in dogs prevented theand Key did not report on the size of the rabbit formation of bony bridges. Furthermore, they foundphysis at the time of the operation, thus the percent- no evidence of growth arrest or angular deformitiesage of physis violated is unknown. in the tibia or femur of their specimens. It was
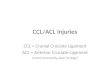
postulated that the complete filling of the hole withNordentoft[32] reported in 1969 on the placementthe tendon prevented osteogenic processes betweenof 3mm drill holes across the physis of rabbits andthe metaphysis and epiphysis, and subsequently pre-4–5mm drill holes placed across the physis of dogs.vented bony bridge formation and growth arrest.They documented the presence of bony bridges inFigure 1 shows the radiographs of Stadelmaier etall eight cases, but growth continued or was onlyal.[35] in which bony bridges span unfilled tunnels.transiently inhibited in all animals. In addition, theyFigure 2 shows their radiograph of tunnels filledfound that curettement of 10% of the growth platewith facia lata autograft. Note the absence of com-without violating the basement membrane causedmunication between the metaphysis and epiphysis.permanent arrest in only one of 11 cases. However,
when curettement was accompanied by drillingthrough basement plate, complete arrest occurred in13/17 (76%), suggesting that communication be-tween elements of the metaphysis or epiphysis andthe physis caused growth arrest.
In an effort to document the threshold for the sizeof bony bridge that will cause growth arrest, Makelaet al.[31] examined unfilled tunnels placed across theintercondylar portion of the distal femoral epiphysisof 5-week-old rabbits. In their 1988 study, they used2.0 and 3.2mm drill holes, removing 3% and 7% ofthe physis, respectively. Upon histological examina-tion, they found evidence of bony bar formation andalso documented growth arrest in the specimenstreated with a 3.2mm transphyseal tunnel. Theyconcluded that a 7% violation of the cross-sectional
Fig. 1. The presence of bony bridge across unfilled tunnels of thetibia of a dog (reproduced from Stadelmaier et al.,[35] with permis-sion from the American Journal of Sports Medicine).
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

460 Shea et al.
excessive graft tensioning, rather than by the place-ment of tunnels.
Houle et al.,[40] also studying rabbits, concludedthat violation of 1% of the physis will cause physealdeformities, and that the tibial physis is the mostvulnerable area to damage secondary to ACL recon-struction. They used computers to calculate the areaof the rabbit tibial physis and experimental drillhole, but their computer programs and mathematicalmethods used were not published, and as such, theirresults are neither reproducible nor verifiable. Fur-thermore, the authors’ conclusion that the tibia ismore vulnerable is in opposition to other animal and
Fig. 2. The absence of a bony bridge in tunnel filled with facia lataautograft (reproduced from Stadelmaier et al.,[35] with permissionfrom the American Journal of Sports Medicine).
clinical studies. From their radiographs, it appearsthat their tibial tunnels are more medial than normal
Janarv et al.[33] reported similar findings in aACL reconstructive tunnels, and it has been shown
rabbits, showing that the placement of various softthat medial placement of tibial drill holes is more
tissue grafts prevented bony bridge formation.likely to cause deformity (figure 3).[41] The 1956
Janarv et al.[33] also attempted to quantify the per-results of Ford and Key[29] suggest that lateral trau-
centage of physis that can be violated without caus-ing growth disturbances. Similar to Guzzanti etal.[30] and Makela et al.,[31] they concluded that a4–5% violation of the cross-sectional area of thephysis would not result in deformities, but that a7–9% violation would cause shortening of the af-fected limb.
In contrast to Stadelmaier et al.[35] and Janarv etal.,[33] Ono et al.[34] found that neither the placementof the iliotibial band or bone-patellar-tendon-bonegrafts in transphyseal tunnels prevented tibial de-formity and shortening. They performed ACL re-construction in 56 rabbits using bone-patellar ten-don-bone autografts in 31, and iliotibial bands in 25.They reported using 3mm drill holes, but did notrecord physeal area or the percentage of the physisviolated. Their experiments showed a high degree offailure – only five animals in each group had intactgrafts after 24 weeks. All of these ten had variousdeformities and shortening, yet they observed nobony bridges on microscopic examination. Ono etal.[34] argue that the physeal arrest observed mayhave been caused by tenodesis, yet they did notreport initial graft tensions. Furthermore, their highdegree of failure is remarkable and may be evidenceof poor experimental design or improper technique.The observed deformities may have been due to
Fig. 3. Lateral placement of tibial tunnel (reproduced from Houle etal.[40] with permission)
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

ACL Injury in Paediatric and Adolescent Patients 461
ma is more likely to cause angular deformities than important considerations in human ACL reconstruc-tion, and important factors in the induction ofmore centrally placed holes. The results of Houle etphyseal arrest.al.[40] do not show that a 1% violation in any location
The third limitation of these studies was theirwill cause arrest; rather they only show that a 1%lack of documentation of dissection near the per-violation in the periphery will cause growth arrest.ichondral ring,[42] which can also lead to physealThese animal studies are not without limitations.arrest. Future studies need to document more pre-First, no study, other than Houle et al.[40] reportscisely the placement of the tunnel in relation to thisactual measurements of each rabbit physis violated,and other anatomical structures.rather they relied on calculations and measurements
from models. Although Houle et al.[40] measured3.2 Tenodesis Effect
actual physes, their methods were not published andare difficult to analyse or verify. Furthermore, there ACL reconstruction includes the placement of aare problems with extrapolating results that were tensioned graft across the physis. The effect of pres-performed only on the peripheral aspect of the sure and tension on the growing physis has not beenphysis. In addition, the wide variation in the natural extensively studied. Few studies have examined theanatomy of rabbits and dogs makes calculations effects of pressure and tension across the growingfrom averages or models inappropriate. Janarv et epiphysis and no clear threshold values have beenal.[33] examined 14 rabbit distal femoral physes to established.find the average area, which they reported to be In 1951, Gelbke[43] reported on experiments to149.5 mm2. They reported variations between speci- test the ability of bones to grow when subjected tomens from 121–185 mm2. For a drill hole of 3.0mm, tensions opposite those of growth. They fashionedthis translates to a variation of 4.6% (unlikely to wires that looped from a tunnel in the diaphysis ofcause deformity as reported by Janarv et al.[33] and lambs and tethered around the intercondylar area.Guzzanti et al.[30]) to 7.1%. (likely to cause deformi- They found that the growing bone distorted thety) [table II]. Thus, without measuring each speci- shape of the wire loop until sufficient pressure builtmen, it is difficult to identify the threshold of per- up and subsequently prevented the bone from fur-centage physis that can be safely violated. ther elongating. They found that bone would contin-
ue to grow in the presence of pressure, but that atThe second limitation of these studies is that theyexcessively high tensions, physeal growth would bedid not consider the undulating anatomy of the fem-affected.oral physis or the location of the tibial tubercle with
Using springs, Porter[44] examined pressurerespect to their tunnels. The distal femoral physis ofacross the physis in a direction opposite that ofa rabbit is known to be complex,[33] as is the tibialGelbke.[43] They demonstrated that 10kg of pressureepiphysis.[41] The precise orientation of the tunnelspushing apart the metaphysis and epiphysis of theand their intersection with the physis cannot beproximal tibia in calves caused additional boneignored. Figure 4 and figure 5 show two possiblelengthening. Although their experiments resulted intunnel orientations for the proximal tibia. The start-angular deformities due to the uneven placement ofing position and orientation of the drill hole can
significantly affect the location of physeal injury, aswell as the volume of physeal injury. Without exam-ining each experimental specimen in three dimen-sions, it is impossible to know the exact placementof the tunnels, whether they crossed the anterior orcentral aspect of the tibial apophysis, their orienta-tion to the femoral physis, or their central/peripherallocation across the femoral physis – all critically
Table II. Variation in rabbit physeal area showing differences inpercentage of physis violated
Drill diameter Drill area Physeal area % of Physis(mm) (mm2) (mm2)
3.0 8.54 185 4.6
3.0 8.54 176 4.9
3.0 8.54 149.5 5.7
3.0 8.54 121 7.1
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

462 Shea et al.
shown how varying levels of tension affect physesof varying areas. Clearly, the physis of dogs and thephysis of humans are different sizes, and it may beargued that larger physes are able to tolerate greatertensions, but this also has yet to be demonstrated(table III).
4. Anatomy of the Proximal Tibia andDistal Femoral Physes
The anatomy of the ACL, tibial apophysis anddistal femoral physis has only recently been studiedin children.[42,47] Shea et al.[47] examined the tibialinsertion of the ACL using MRI in children andfound that although the overall dimensions of theFig. 4. Drill hole path with more significant damage to growth plate.
The drill hole crosses the growth plate twice. ACL and the tibia are smaller in children, the anteri-or and posterior limits of the ACL insertion are
the springs, they showed that pressure has an effect proportional to the AP dimension of the tibia. Theon active physes. tibial apophysis is located on the anterolateral aspect
of the tibia and extends inferiorly, tapering medial-In 2000, Edwards et al.[38] reported that 80Nly.[41] They found that the medial extension of the(~8.16kg) of graft tension on a reconstructed ACL inapophysis is within 3–4mm of the medial border ofyoung dogs can alter physeal growth in the absencethe tibial insertion of the ACL. A standard place-of bony bridges. Edwards et al.[38] showed that 80Nment of ACL drill holes can run parallel to andof tension on a facia lata autograft across the femoraloverlap the inferior aspect of the proximal tibialand tibial physis caused deformities of both theapophysis, removing large amounts of physeal tis-femur and the tibia. This study only examined ani-sue (figure 4). A drill hole in the proximal tibia canmals with grafts at 80N of tension, and there were nomiss the entire apophysis or can damage a largeexperiments on animals with grafts under less ten-volume of the physis depending on the position ofsion. Edwards et al.[38] used 80N upon the 1997the tunnel (figure 4 and figure 5).conclusions of Yasuda et al.,[45] who showed that
The relationship of the femoral insertion of the80N of graft tension in human ACL reconstructionACL in relation to the distal femoral physis hasresulted in less clinical laxity than grafts at 20N. It isrecently been described by Behr et al.[42] They foundworthy to note, however, that Yasuda et al.[45] alsothat in 20- to 36-week-old fetuses, the average dis-reported that grafts at 40N did not give significantlytance from the superior aspect of the ACL insertiondifferent results than grafts initially tensioned to
80N. Houle et al.[40]reported results similar to Ed-wards et al.[38] but the initial tension of Houle’sgrafts was not reported.
In 2002, Yoshiya et al.[46] showed that 25N ofinitial graft tension in human ACL reconstructiongave similar clinical results as did those tightened to50N (~5.08kg). The results from the study byYoshiya et al.[46] suggest that ACL reconstructionusing 25N of tension is acceptable, but it has yet tobe documented how this level of graft tension willaffect growth in animals. Furthermore, it remains be Fig. 5. Drill hole path with minimal damage to growth plate.
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

ACL Injury in Paediatric and Adolescent Patients 463
Table III. Summary of anterior cruciate ligament reconstruction studies in animals
Study Year Animal Drill diameter (mm) Bone % of Physis Tunnell filling Deformation
Ford and Key[29] 1956 Rabbits 3.2a Distal femur Gelfoam No
Stadelmaier et al.[35] 1995 Dogs 4.0a Femur, tibia Facia lata No
Janarv et al.[33] 1998 Rabbits 1.7 Distal femur 2–3 Tendon No
Janarv et al.[33] 1998 Rabbits 2.5 Distal femur 4–5 Tendon No
Janarv et al.[33] 1998 Rabbits 3.4 Distal femur 7–9 Tendon Yes
Ono et al.[34] 1998 Rabbits 3.0 Tibia ITB Yes
Ono et al.[34] 1998 Rabbits 3.0 Tibia PTB Yes
Edwards et al.[38] 2001 Dogs 4.0 Femur, tibia Facia lata Yes
Houle et al.[40]b 2001 Rabbits 1.95 Tibia 1.0 Patellar tendon Yes
Houle et al.[40]b 2001 Rabbits 2.25 Tibia 1.80 Patellar tendon Yes
a Approximate metric conversions: Ford and Key[29] (1/4in), Stadelmaier et al.[35] (5/32in), Houle et al.[40] (5/32in).
b Partial results listed.
ITB = iliotibial band; PTB = patellar tendon bone.
to the femoral physis is only 2.66 ± 0.18mm. They 5. Reported Complications After ACLReconstruction in Skeletallyalso examined adolescents aged 5–15 years old andImmature Patients
found that the average distance was only 2.92 ±0.68mm. Standard drill holes used in physeal-spar- Despite the concerns related to physeal arrest and
the results of animal studies, there are very few caseing or over-the-top femoral placements often violatereports or documentation of complications second-the femoral physis, as it is immediately adjacent toary to operative ACL reconstruction.[27,50,51]
and anterior to the placement site of the over-the-top In 1986, Lipscomb and Anderson[51] reported ontrough. the outcome of 24 skeletally immature athletes who
underwent ACL reconstruction following injury.The conclusions of Behr et al.[42] help to explainThey reported a 2cm leg length discrepancy in onethe three cases of femoral valgus reported by Kocherpatient due to the inadvertent stapling of both the
et al.[37] as anatomical variations can often cause the tibial and femoral physes when securing the graft.standard placement of these troughs to be through This placement mimicked that of a Blount physeal
staple, and as expected, caused epiphysiodesis.the physis. The analysis of Shea et al.[41] with respectTheir results are discussed more comprehensively into tibial tunnel placement offers an explanation forsection 6.2.
the results of Houle et al.,[40] Ono et al.[34] and Koman and Sanders[50] reported in 1999 a singleGuzzanti et al.[30] who documented tibial deformi- case of development of distal femoral valgus after a
hamstring ACL reconstruction. From their pub-ties in rabbits, versus the reports of Matava andlished radiographs, it is clear that the femoral fixa-Siegel[48] and Lo et al.,[49] who reported successfultion used for this case consisted of a transfixation
placement of tibial tunnels in adolescents, but who pin that crossed the lateral aspect of the femoralalso reported a qualitative modification in the place- physis (figure 6 and figure 7). This orientation of the
transfixation pin was very similar to the experimentsment of the tunnel to avoid the tibial apophysis.of Haas[36] who showed that the placement of metalFrom these analyses, it clear that anatomical consid-pins diagonally across the epiphysis of rabbits
erations are critically important in the placement ofcaused growth disturbances and lateral epiphysi-
drill holes for ACL reconstruction in humans as well odesis. In response to a letter by Oni,[52] Sanders[53]
as animals. acknowledged that hardware should not be placed
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

464 Shea et al.
across the physis, but argued that physeal arrest reported, all due to staples across the apophysis orsuturing to the tibial periosteum. In addition, therewould have occurred without the placement of thewere three femoral deformities reported secondarypin.to extra-articular procedures, two due to lateral ex-In a recent survey of orthopaedic surgeons,tra-articular tenodesis and one due to the placement
Kocher et al.[54] found that 108 of 139 respondentsof a graft in an over-the-top trough. There was one
operatively treat ACL injuries in skeletally imma-reported leg length discrepancy secondary to ACL
ture patients. They found 15 previously undocu- reconstruction wherein no transphyseal hardware ormented skeletal deformities secondary to ACL re- bone plugs were implicated. The patient was anconstruction. There were six cases of distal femoral 11-year-old girl whose ACL reconstruction in-valgus secondary to the placement of interference volved 6mm drill holes and a hamstring allograft.screws, staples, transfixation pins or bony plugs The survey by Kocher et al.[54] has been the mostacross the femoral physis. There were two cases of comprehensive investigation into the frequency ofgrowth arrest secondary to large (12mm) drill holes. growth disturbances secondary to ACL reconstruc-There were three cases of tibial genu recurvatum tion to date. However, this study was not without
limitations. The actual number of patients operatedon was not collected, thus risk calculations could notbe performed. Also, the placement of tunnels andtroughs were not reported. Differences in tunnel andhardware placement cannot be ruled out as factorsresponsible for the results reported. Thus, differ-ences in placement between surgeons and anatomi-cal variations of the orientation and extension of thetibia tubercle and distal femoral physis in relation tothe tunnels cannot be ruled out as factors responsiblefor the results reported.
6. Methods of ACL Reconstruction inSkeletally Immature Patients
6.1 Physeal Sparing Techniques: Both Tibialand Femoral
Various physeal-sparing techniques have beendescribed (table IV), including primary repair of theACL, techniques that avoid placing drill holesacross both the tibial and femoral physis, and thosethat avoid drilling across the femoral physis only.Physeal-sparing techniques have had varying re-sults, ranging from good to poor.
Primary repair of the ACL in adults and childrenhas been documented[55-57] and has been shown tofare no better than bracing, rehabilitation and coun-selling. DeLee and Curtis[55] treated three patientswith acute ACL injuries by the primary repairmethod of Marshall et al.[58] Upon follow-up at
Fig. 6. Radiograph of a skeletally immature patient who underwenthamstring anterior cruciate ligament reconstruction and subse-quently developed valgus deformity. Note the placement of thefemoral transfixation pin (reproduced from Koman and Sanders,[50]
with permission).
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

ACL Injury in Paediatric and Adolescent Patients 465
overall failure rate of 25%, and found a tibial anteri-or instability rate of 31%. These high rates of insta-bility and failure make primary repair of the ACL,even when treated within 48 hours of injury, anunsuitable long-term treatment.
In 1991, Brief[59] described a technique thatavoids the placement of tunnels across both thefemoral and tibial physes. This technique involvesdissection of the semitendinosus and gracilis ten-dons, leaving them attached at their pes anserinusinsertion. Theses tendons are then sutured togetherand threaded under the anterior horn of the medialmeniscus, through the intercondylar notch and at-tached with staples above the physis of the lateraldistal femoral condyle. Nine patients were treatedusing this procedure, and were followed for a mini-mum of 36 months with mixed results. There wereno reports of growth disturbances. Eight of the ninepatients were satisfied with their results. Only fivepatients were followed for 3 years, and all had a 1+Lachman and average of 2.6mm laxity as measuredby KT-1000.
Micheli et al.[60] described a femoral and tibialphyseal sparing technique in 1999. The iliotibialband was dissected free of its insertion on the femur20mm proximal to the joint line, and is threadedlaterally around the posterior aspect of the lateralfemoral condyle. There, it is attached and then
Fig. 7. Valgus deformity secondary to a transphyseal anterior cruci-ate ligament reconstruction using a hamstring graft. Note the place-ment of the transfixation pin, the lateral growth arrest of the distalfemur, and the valgus angulation. (reproduced from Koman andSanders,[50] with permission).
threaded medially through the intercondylar notchand sutured to the periosteum of the proximal tibia
approximately 2 years, two patients reported chronic medial of the tibial tubercle and distal to the physis.instability and episodes of giving way. This technique was used in eight prepubescent pati-
ents who were then followed to skeletal maturity.Engebretsen et al.[57] followed eight paediatricThere were no reported growth disturbances report-patients treated by primary repair of the ACL usinged at skeletal maturity. They reported good objec-four U-sutures attached to the stump of the ACL andtive stability measurements using a KT-1000 ma-pulled through two carefully placed drill holes in thechine. All eight patients denied instability and weredistal femur. They found that in all eight patientssatisfied with their results. The procedure was alsothere was laxity or instability, and that the averageperformed on nine other patients, but who had notpre-injury/follow-up Tegner scores dropped fromyet reached skeletal maturity at the time of publica-6.6 to 4.8, showing a marked decrease in competi-tion.tive ability and athletic activity. Engebretsen et
al.[56] reported again in 1989 on a more comprehen- These studies by Micheli et al.[60] and Brief[59]
sive study of 74 patients treated by primary suturing document innovative physeal sparing techniques;of the ACL following injury. The average follow-up however, they are limited by a small patient pooltime was 6 years. Engebretsen et al.[56] reported an and lack of long-term results. If these techniques are
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

466Shea et al.
© A
dis D
ata
Info
rma
tion
BV 2003. A
ll righ
ts rese
rved
.Sp
orts M
ed
2003; 33 (6)
Table IV. Summary of important clinical studies of anterior cruciate ligament reconstruction in paediatric patients
Study Year No. of pts Mean age Follow-up Technique Subjective results Laxity Growth(y) (mo)
femoral tibial return to pt Lysholm HSS average average average documentationsparing sparing sports satisfaction score score Lachman KT-1000 post- of growth
(%)a (%) score difference surgical(mm) growth
(mm)
Lipscombe 1986 24 13.5 35 Yes No 62 NR NR 45.9 <1a 1.8 NR NRandAnderson[51]
McCarroll 1988 10 13.3b 26.4b Yes Yes 100 NR NR NR NR NR NR NRet al.[21]
McCarroll 1988 14 13.3b 26.4b No No 100 NR NR NR NR 1.7 NR NRet al.[21]
Brief [59] 1991 9 17.2 36–78 Yes Yes 67 67 NR NR 1a 2.4 NR NR
Parker et 1994 5 13.3 33.2 Yes Yes 80 NR 95.2 96.6 NR 3.6 NR NRal.[65]
Andrews et 1994 8 13.5 58 Yes No 87 NR NR NR <1a 2.3c 45.4 NRal.[62]
Lo et al.[49] 1997 5 12.9 88.8 Yes No 80 NR NR NR <1a 1.0 177 NR
Matava and 1997 8 14.8 32 No No 100 NR NR NR NR 1.1 94 ScanogramSiegel[48]
Bisson et 1998 9 13 39 Yes No 77 NR 99 NR NR 2.8 NR NRal.[63]
Micheli et 1999 8 11 66.5 Yes Yes 100 100 97.4 NR <1a 1.1 NR NRal.[60]
Robert and 1999 8 11.4 42 Yes Yes NR NR NR NR NR 1.5 NR NRBonnard[61]
Aronowitz 2000 15 13.4 25 No No 100 100 97 NR <1a 1.7 NR NRet al.[64]
a Previous level or lower level for reasons unrelated to knee injury.
b Data combined in both McCarroll et al.[21] 1988 data sets.
c Estimate based on authors grouping of original data.
HSS = Hospital for Special Surgery; NR = not reported; pt = patient.

ACL Injury in Paediatric and Adolescent Patients 467
expected to last the patient through adulthood, more graft. The point of the femoral drill hole guide wasdocumentation on long-term results is needed. placed superior and posterior to the anatomical ori-
gin of the ACL and oriented 70–90° to the long axisRobert and Bonnard[61] described a technique inof the femur to avoid drilling across the femoral1999 that also avoids the femoral and tibial physes.physis. This placed the 8mm femoral drill holeA transdiaphyseal tunnel is created originating exit-
ing superior and posterior from the anatomical ori- wholly within the lateral femoral condyle epiphysis.gin of the ACL on the femur to avoid drilling across The semitendinosus and gracilis tendons werethe femoral physis. A bone-patellar tendon-bone passed through the tibial and femoral drill holes andgraft is harvested, stapled to the tibia, run through a sutured to the periosteum of the femur. Extra-articu-trough on the tibial plateau superior to the physis, lar techniques were also performed for supplemen-and is then attached proximally into the femoral tation. The patients were followed for an average oftunnel via an interference screw. They reported on 35 months. Fifteen of the 24 (62%) returned to theireight patients treated with this technique at an aver- previous level of activity. There was one reportedage follow-up of 3.5 years. All were able to return to case of a 2cm leg-length discrepancy due to thetheir previous level of activity (Tegner score aver- inadvertent placement of staples across both theage = 7.25). There was an average laxity difference femoral and tibia physis. Other than this case, thereof 1.5mm, and there were no reports of angular were no reports of significant leg length discrepan-deformities or physeal arrest. Unfortunately, this cies or angular deformities greater than 3°. Upontechnique necessitates a 30–45 day immobile cast clinical examination, there was an average laxity ofdue to the weak tibial fixation, and involves exces- 1.8mm between the affected and unaffected knee onsive removal of epiphyseal bone from the tibial passive anterior drawer tests measured by KT-1000.plateau. Although their technique aims to avoid McCarroll et al.[21] reported in 1988 on ten ath-injury to the apophyseal portion of the physis, the letes who were treated for acute ACL injuries bypotential for injury exists, which could lead to reconstruction using tibial drill holes and a physealphyseal arrest. sparing technique on the femur. Skeletal maturity
These studies show good results initially, but the was carefully assessed using bone age, Tanner clas-long-term result of such physeal sparing grafts has sification and family history of growth. A physeal-yet to be shown. Non-anatomical placement places sparing technique was used on the femoral side foradditional strain on the graft, and may influence the patients who were both unwilling to modify theirlong-term stability and function of the knee, and activities and who were not nearing skeletal maturi-laxity may eventually cause secondary meniscal and ty. All ten patients were able to return to theirosteochondral injuries. More long-term studies on previous level of activity, with only four reporting atthese techniques are necessary. least one episode of giving way. There were no
growth deformities at skeletal maturity.6.2 Physeal Sparing Techniques: Femoral
Andrews et al.[62] reported in 1994 on the out-Side Onlycome of eight skeletally immature athletes whoseACL was reconstructed with facia lata or AchillesIn 1986, Lipscomb and Anderson[51] reported ontendon allografts passed through tibial drill holestransphyseal tibial- and femoral-sparing ACL recon-and affixed to the femur in an over-the-top position.struction in 11 patients with open physes and 13They used 6–7mm drill holes with the tibial drillpatients with partially closed physes. The intra-artic-holes angled to intersect the tibial physis as perpen-ular reconstructions were supplemented with extra-dicular as possible and with care to avoid the peri-articular techniques. For the intra-articular recon-pheral ring. The average chronological age of theirstruction, they used the semitendinosus and gracilispatient was 13.4 years. Tanner stages and bone agestendons left attached distally and a 6.4mm tibial drill
hole placed to create an anatomically approximate were not reported. They did not report any unsatis-
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

468 Shea et al.
factory results due to limb shortening or angular biceps transfer or iliotibial band tenodesis. All 14deformities. Average anterior laxity was measured athletes returned to their previous level of activity,using KT-1000, and three of five patient tested were and upon KT-1000 testing, there was an average offound to have anterior translation greater than 3mm. 1.7mm anterior translation. There were no reported
growth problems, but it seems unlikely that thereIn 1997, Lo et al.[49] reported on five patients whowould be within this group, as they were pre-select-were treated for ACL tears with a similar techniqueed for skeletal maturity based on family history,that utilised tibial, but not femoral drill holes. EitherTanner staging and skeletal age before undergoinga single loop semitendinosus/gracilis graft or asurgery. These patients, who were not close to skele-quadriceps-patellar tendon graft was used. Atal maturity, were treated with extra-articular recon-6–7mm tibial tunnel was placed more vertically than
normal to minimise the cross-sectional area that structions.violated the physis. The tendon was passed through McCarrol et al.[22] reported again in 1994 on thethe tunnel and fixed in an over-the-top position on results of 60 athletes who were treated bythe femur using staples proximal to the distal femo- transphyseal ACL reconstruction involving both theral physis. After an average 7.4 years follow-up, femoral and tibial physes. They used bone-patellarfour patients had returned to their previous level of tendon-bone autografts in all patients. The averageactivity. There were no reports of leg length discrep- age was 14.2 years (range 13–17 years), and averageancy or angular deformities. Four patients had a follow-up was 4.2 years. The average increase innegative Lachman test, and the average KT-1000 height was only 2.3cm. There were no growth dis-difference was 1mm. Although these are good re- turbances or angular deformities, and 51/60 hadsults at a long follow-up, the study size was very KT-1000 differences of ≤3.5mm. Although thesmall (five patients) and it is difficult to conclude number of patients in this study is high, the smallthat this procedure will have similar results in a wide amount of growth indicated that most were nearingrange of patients. skeletal maturity.
Bisson et al.[63] reported in 1999 on the results ofIn 1997, Matava and Siegel[48] reported success-
nine patients who also underwent ACL reconstruc-ful intra-articular reconstruction in eight patients
tion using drill holes that crossed the central portion(average age 14.8 years) who an average of 9.4cm
of the tibial physis and were secured proximally ingrowth after their reconstruction. They used ham-
an over-the-top placement on the femur. Their fol-string tendon autografts placed through 7–9mm tun-
low-up was short (average of 39 months), but theynels and secured with buttons or staples. After an
did not observe any deformities or leg-length dis-average of 32 months follow-up, all eight athletes
crepancies. Seven of nine were able to return to theirwere able to return to their previous level of activity.
sport fully; the other two experienced complete rup-In those who did not have an injury to the contralat-
tures later. Two of six examined patients with intacteral knee, all had KT-1000 differences ≤2. In their
grafts had KT-1000 measured anterior laxity greateroperative technique, Matava and Siegel[48] reported
than 3.5mm.placing the tibial drill hole medial enough to avoidthe tibia tubercle; however, they did not quantify
6.3 Non-Physeal Sparing Techniquesthis modification. Additionally, they reported thatthey took care to drill the femoral tunnel as perpen-McCarroll et al.[21] reported in 1988 on 14 pati-dicular to the physis as possible, but again, there wasents who had transphyseal tibial and femoral recon-no quantification of this modification.structions augmented with extra-articular tech-
There was a 7mm shortening of the operated limbniques. They used A-O tenodesis of the iliotibialof one patient, 5mm of the femur and 2mm of theband. Athletes who were close to skeletal maturitytibia compared with the contralateral limb. The oth-were treated with standard bone-patellar tendon-er seven patients had ≤5mm difference. The averagebone reconstruction and reinforcement with either
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

ACL Injury in Paediatric and Adolescent Patients 469
shortening was –1mm. There were no angular defor- patients (12.5 years), and identification ofmities. prepubescence clearly indicates that these patients
had growth remaining, and that the surgical recon-Aronowitz et al.[64] reported on transphyseal ACLstruction did not affect growth.reconstruction in 19 adolescents of skeletal age >14
years using Achilles tendon allografts. After 257. Conclusionsmonths, 16 of 19 had returned to their previous level
of sport. The average KT-1000 difference wasMidsubstance ACL injury in children and adoles-
1.7mm, with no patient greater than 3.0mm. Thesecents is increasingly recognised. Natural history
are excellent results; however, the minimum skeletalstudies of non-reconstructive management of ACL
age for inclusion into this study precludes extrapola-injury demonstrate poor outcomes in young patients
tion of these results into paediatric and prepubescentwho return to sports. ACL reconstruction in young
populations.patients with significant growth remaining carry a
The results of these studies are promising; how- poorly quantified risk of growth plate injury. Futureever, they have several limitations: (i) there was a studies should focus on defining these risks andlack of documentation of preoperative Tanner stage devising surgical techniques that minimise the risksor skeletal maturity; (ii) they were performed on of clinically significant growth plate injury.limited numbers of patients; (iii) formal physicalevaluation or radiographic assessment was not done Acknowledgementsroutinely on all patients. There is documentation of
No funding was used to assist in the preparation of thissuccess for patients who are nearing skeletal maturi-manuscript and there are no conflicts of interest with respectty, but there is a lack of data on ACL reconstructionto any of the authors and the information presented in this
on patients who have significant growth remaining. paper.In 2002, Aichroth et al.[17] reported on a prospec-
tive study wherein 45 patients were treated for ACL Referencesinjuries, all undergoing transphyseal procedures. 1. Auringer ST, Anthony EY. Common pediatric sports injuries.
Semin Musculoskelet Radiol 1999; 3: 247-56The average chronological age was 12.5 years. Also2. Iobst CA, Stanitski CL. Acute knee injuries. Clin Sports Med
documented were Tanner stages and skeletal maturi- 2000; 19: 621-353. Micheli LJ. Pediatric and adolescent sports injuries: recentty. There were six patients who were prepubescent,
trends. Exerc Sport Sci Rev 1986; 14: 359-7418 who were undergoing puberty, and 21 post-4. Tohyama H, Kutsumi K, Yasuda K. Avulsion fracture at the
pubescent patients. All of the patients underwent femoral attachment of the anterior cruciate ligament afterintercondylar eminence fracture of the tibia. Am J Sports Medreconstruction using a four-strand hamstring tech-2002; 30: 279-82nique with placement of the fixation devices well 5. Micheli LJ, Metzl JD, Di Canzio J, et al. Anterior cruciate
away from the femoral and tibial physes. Drill holes ligament reconstructive surgery in adolescent soccer and bas-ketball players. Clin J Sport Med 1999; 9: 138-41originated from the anatomical footprint of the ACL
6. Shea K, Wang J, Pfeiffer R, et al. Age related risk factors forand were oriented to cross the physis as perpendicu- ACL injury in pediatric and adolescent soccer players-differ-
ences between male and females. American Academy oflarly as possible. At a mean follow-up of 49 months,Orthopaedic Surgeons Annual Meeting; 2001 Feb; San Fran-they reported no leg length discrepancies or physeal cisco. Orlando (FL): American Academy of Orthopaedic Sur-
arrest. geons, 20017. Arendt E, Dick R. Knee injury patterns among men and women
This study clearly documented that placement of in collegiate basketball and soccer: NCAA data and review ofliterature. Am J Sports Med 1995; 23: 694-701transphyseal tunnels may not cause clinically signif-
8. Powell JW, Barber-Foss KD. Sex-related injury patterns amongicant growth arrest when anatomy and placement ofselected high school sports. Am J Sports Med 2000; 28: 385-91
fixation devices are carefully considered. The only 9. Hewett TE. Neuromuscular and hormonal factors associatedwith knee injuries in female athletes: strategies for interven-limitation of this study is the incomplete documenta-tion. Sports Med 2000; 29: 313-27tion of Tanner staging, skeletal age, and subsequent 10. Harmon KG, Dick R. The relationship of skill level to anterior
growth. Nonetheless, the young average age of their cruciate ligament injury. Clin J Sport Med 1998; 8: 260-5
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

470 Shea et al.
11. Rozzi SL, Lephart SM, Gear WS, et al. Knee joint laxity and 31. Makela EA, Vainionpaa S, Vihtonen K, et al. The effect ofneuromuscular characteristics of male and female soccer and trauma to the lower femoral epiphyseal plate: an experimentalbasketball players. Am J Sports Med 1999; 27: 312-9 study in rabbits. J Bone Joint Surg Br 1988; 70: 187-91
32. Nordentoft EL. Experimental epiphyseal injuries: grading of12. Barrett GR, Rose JM, Ried EM. Relationship of anterior cruci-traumas and attempts at treating traumatic epiphyseal arrest inate ligament injury to notch width index (a roentgenographicanimals. Acta Orthop Scand 1969; 40: 176-92study). J Miss State Med Assoc 1992; 33: 279-83
33. Janarv PM, Wikstrom B, Hirsch G. The influence of13. Good L, Odensten M, Gillquist J. Intercondylar notch measure-transphyseal drilling and tendon grafting on bone growth: anments with special reference to anterior cruciate ligamentexperimental study in the rabbit. J Pediatr Orthop 1998; 18:surgery. Clin Orthop 1991; 263: 185-9149-5414. Teitz CC, Lind BK, Sacks BM. Symmetry of the femoral notch
34. Ono T, Wada Y, Takahashi K, et al. Tibial deformities andwidth index. Am J Sports Med 1997; 25: 687-90failures of anterior cruciate ligament reconstruction in imma-
15. Myklebust G, Maehlum S, Holm I, et al. A prospective cohortture rabbits. J Orthop Sci 1998; 3: 150-5
study of anterior cruciate ligament injuries in elite Norwegian35. Stadelmaier DM, Arnoczky SP, Dodds J, et al. The effect ofteam handball. Scand J Med Sci Sports 1998; 8: 149-53
drilling and soft tissue grafting across open growth plates: a16. Wolman RL. Association between the menstrual cycle and histologic study. Am J Sports Med 1995; 23: 431-5
anterior cruciate ligament in female athletes. Am J Sports Med36. Haas S. Restriction of bone growth by pins through the epiphys-1999; 27: 270-1
eal cartilaginous growth plate. J Bone Joint Surg 1950; 22A:17. Aichroth PM, Patel DV, Zorrilla P. The natural history and 338-43
treatment of rupture of the anterior cruciate ligament in chil- 37. Kocher MS, Saxon HS, Hovis WD, et al. Management anddren and adolescents: a prospective review. J Bone Joint Surg complications of anterior cruciate ligament injuries in skeletal-Br 2002; 84: 38-41 ly immature patients: survey of the Herodicus Society and The
18. Angel KR, Hall DJ. Anterior cruciate ligament injury in children ACL Study Group. J Pediatr Orthop 2002; 22: 452-7and adolescents. Arthroscopy 1989; 5: 197-200 38. Edwards TB, Greene CC, Baratta RV, et al. The effect of
19. Graf BK, Lange RH, Fujisaki CK, et al. Anterior cruciate placing a tensioned graft across open growth plates: a grossligament tears in skeletally immature patients: meniscal patho- and histologic analysis. J Bone Joint Surg Am 2001; 83:logy at presentation and after attempted conservative treat- 725-34ment. Arthroscopy 1992; 8: 229-33 39. Phemister D. Operative arrestment of longitudinal growth of
20. Janarv PM, Nystrom A, Werner S, et al. Anterior cruciate bones in the treatment of deformities. J Bone Joint Surg 1933;ligament injuries in skeletally immature patients. J Pediatr 15: 1-5Orthop 1996; 16: 673-7 40. Houle JB, Letts M, Yang J. Effects of a tensioned tendon graft in
a bone tunnel across the rabbit physis. Clin Orthop 2001; 391:21. McCarroll JR, Rettig AC, Shelbourne KD. Anterior cruciate275-81ligament injuries in the young athlete with open physes. Am J
Sports Med 1988; 16: 44-7 41. Shea K, Apel P, Showalter LD, et al. ACL reconstruction inchildren: minimizing the injury to the proximal tibia physis22. McCarroll JR, Shelbourne KD, Porter DA, et al. Patellar tendonwith variation in tibial drill hole placement. American Acade-graft reconstruction for midsubstance anterior cruciate liga-my of Orthopaedic Surgeons Annual Meeting; 2001 Feb; Sanment rupture in junior high school athletes: an algorithm forFrancisco. Orlando (FL): American Academy of Orthopaedicmanagement. Am J Sports Med 1994; 22: 478-84Surgeons, 200123. Mizuta H, Kubota K, Shiraishi M, et al. The conservative
42. Behr CT, Potter HG, Paletta Jr GA. The relationship of thetreatment of complete tears of the anterior cruciate ligament infemoral origin of the anterior cruciate ligament and the distalskeletally immature patients. J Bone Joint Surg Br 1995; 77:femoral physeal plate in the skeletally immature knee: an890-4anatomic study. Am J Sports Med 2001; 29: 781-724. Pressman AE, Letts RM, Jarvis JG. Anterior cruciate ligament
43. Gelbke H. The influence of pressure and tension on growingtears in children: an analysis of operative versus nonoperativebone in experiments with animals. J Bone Joint Surg 1951; 33:treatment. J Pediatr Orthop 1997; 17: 505-11947-53
25. Woods GW, O’Connor DP. Delayed anterior cruciate ligament44. Porter RW. The effect of tension across a growing epiphysis. Jreconstruction in skeletally immature adolescents. Am J Sports
Bone Joint Surg Br 1978; 60B: 252-5Med. In press45. Yasuda K, Tsujino J, Tanabe Y, et al. Effects of initial graft
26. Tegner Y, Lysholm J. Derotation brace and knee function in tension on clinical outcome after anterior cruciate ligamentpatients with anterior cruciate ligament tears. Arthroscopy reconstruction: autogenous doubled hamstring tendons con-1985; 1: 264-7 nected in series with polyester tapes. Am J Sports Med 1997;
27. Kocher MS, Micheli LJ, Zurakowski D, et al. Partial tears of the 25: 99-106anterior cruciate ligament in children and adolescents. Am J 46. Yoshiya S, Kurosaka M, Ouchi K, et al. Graft tension and kneeSports Med 2002; 30: 697-703 stability after anterior cruciate ligament reconstruction. Clin
28. Campbell CJ, Grisolia A, Zanconato G. The effects produced in Orthop 2002; 394: 154-60the cartilagenous epiphyseal plate of immature dogs by experi- 47. Shea KG, Apel PJ, Pfeiffer RP, et al. The tibial attachment ofmental surgical trauma. J Bone Joint Surg 1959; 41A: 1221-42 the anterior cruciate ligament in children and adolescents:
29. Ford LT, Key J. A study of experimental trauma to the distal analysis of magnetic resonance imaging. Knee Surg Sportsfemoral epiphysis in rabbits. J Bone Joint Surg 1956; 38: 84-92 Traumatol Arthrosc 2002; 10: 102-8
30. Guzzanti V, Falciglia F, Gigante A, et al. The effect of intra- 48. Matava MJ, Siegel MG. Arthroscopic reconstruction of the ACLarticular ACL reconstruction on the growth plates of rabbits. J with semitendinosus-gracilis autograft in skeletally immatureBone Joint Surg Br 1994; 76: 960-3 adolescent patients. Am J Knee Surg 1997; 10: 60-9
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)

ACL Injury in Paediatric and Adolescent Patients 471
49. Lo IK, Kirkley A, Fowler PJ, et al. The outcome of operatively 59. Brief LP. Anterior cruciate ligament reconstruction without drilltreated anterior cruciate ligament disruptions in the skeletally holes. Arthroscopy 1991; 7: 350-7immature child. Arthroscopy 1997; 13: 627-34 60. Micheli LJ, Rask B, Gerberg L. Anterior cruciate ligament
50. Koman JD, Sanders JO. Valgus deformity after reconstruction reconstruction in patients who are prepubescent. Clin Orthopof the anterior cruciate ligament in a skeletally immature 1999; 364: 40-7patient: a case report. J Bone Joint Surg Am 1999; 81: 711-5 61. Robert H, Bonnard C. The possibilities of using the patellar
51. Lipscomb AB, Anderson AF. Tears of the anterior cruciate tendon in the treatment of anterior cruciate ligament tears inligament in adolescents. J Bone Joint Surg Am 1986; 68: 19-28 children. Arthroscopy 1999; 15: 73-6
52. Oni OO. Physeal arrest [letter]. J Bone Joint Surg Am 2000; 62. Andrews M, Noyes FR, Barber-Westin SD. Anterior cruciate82A: 1204 ligament allograft reconstruction in the skeletally immature
53. Sanders JO. Anterior cruciate ligament reconstruction in the athlete. Am J Sports Med 1994; 22: 48-54skeletally . Arthroscopy 2000; 16 (4): 392-3
63. Bisson LJ, Wickiewicz T, Levinson M, et al. ACL reconstruc-54. Kocher MS, Steadman RJ, Briggs K, et al. Determinants of tion in children with open physes. Orthopedics 1998; 21:
patient satisfaction with outcome after anterior cruciate liga- 659-63ment reconstruction. J Bone Joint Surg Am 2002; 84A:
64. Aronowitz ER, Ganley TJ, Goode JR, et al. Anterior cruciate1560-72ligament reconstruction in adolescents with open physes. Am J55. DeLee JC, Curtis R. Anterior cruciate ligament insufficiency inSports Med 2000; 28: 168-75children. Clin Orthop 1983; 172: 112-8
65. Parker AW, Drez Jr D, Cooper JL. Anterior cruciate ligament56. Engebretsen L, Benum P, Sundalsvoll S. Primary suture of theinjuries in patients with open physes. Am J Sports Med 1994;anterior cruciate ligament: a 6-year follow-up of 74 cases. Acta22 (1): 44-7Orthop Scand 1989; 60: 561-4
57. Engebretsen L, Svenningsen S, Benum P. Poor results of anteri-or cruciate ligament repair in adolescence. Acta Orthop Scand
Correspondence and offprints: Kevin G. Shea, Intermoun-1988; 59: 684-6tain Orthopaedics, 600 N. Robbins Rd., Boise, ID 83702,58. Marshall JL, Warren RF, Wickiewicz TL, et al. The anteriorUSA.cruciate ligament: a technique of repair and reconstruction.
Clin Orthop 1979; 143: 97-106 E-mail: [email protected]
© Adis Data Information BV 2003. All rights reserved. Sports Med 2003; 33 (6)