Embed Size (px)
DESCRIPTION
Antepartum Fetal Surveillance ‘HELLO BABY, HOW ARE YOU?’. Presented By: Janet L. Smith, RNC, BSN Author: Ruth Saathoff, RNC, BSN. OBJECTIVES:. At the end of this class the learner will be able to: Name 5 methods of monitoring the fetus for well-being - PowerPoint PPT Presentation
Citation preview
Antepartum Fetal Surveillance
‘HELLO BABY, HOW ARE YOU?’
Presented By: Janet L. Smith, RNC, BSN
Author: Ruth Saathoff, RNC, BSN
OBJECTIVES:At the end of this class the learner will be able to:
Name 5 methods of monitoring the fetus for well-being
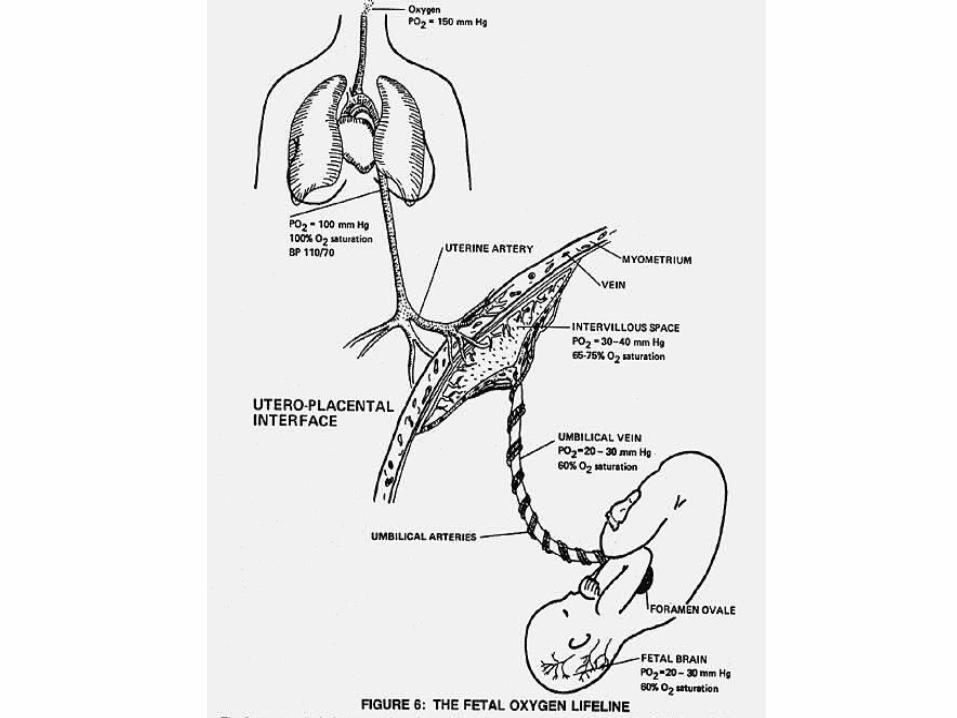
Describe the physiology of maternal and fetal circulation in the relationship to fetal reserve.
Identify the maternal and fetal conditions that indicate a need for fetal surveillance.
Indications for Fetal EvaluationMaternal risk factors
Pre-existing maternal disease Exposure to teratogens in 1st trimester Substance abuse Infertility or conception within 3 months of last
delivery(cont.)
Indications for Fetal Evaluation
Maternal Factors (cont) History of OB complication
• Oligohydramnios, Gestational Hypertension, etc. Previous pregnancy loss PROM > 24 hours Familial history of genetic abnormality Post dates
Indications for Fetal Evaluation
Fetal risk factors Prematurity SGA or LGA Intrauterine growth restriction (IUGR) Known anomaly History of IUFD Fetal cardiac arrhythmias Decreased fetal movement
Why and When
Why do we think of a well baby in terms of placental perfusion?
Oxygen & nutrients are needed for fetus Risk factors may reduce delivery to fetus Good oxygen & nutrient delivery results in movement
and growthWhen is surveillance started?
When risk is present IDDM (type 1) - 32 weeks Previous loss - 34 weeks
Patient: Kay SarahDoc: I. Ben Cursed M.D.
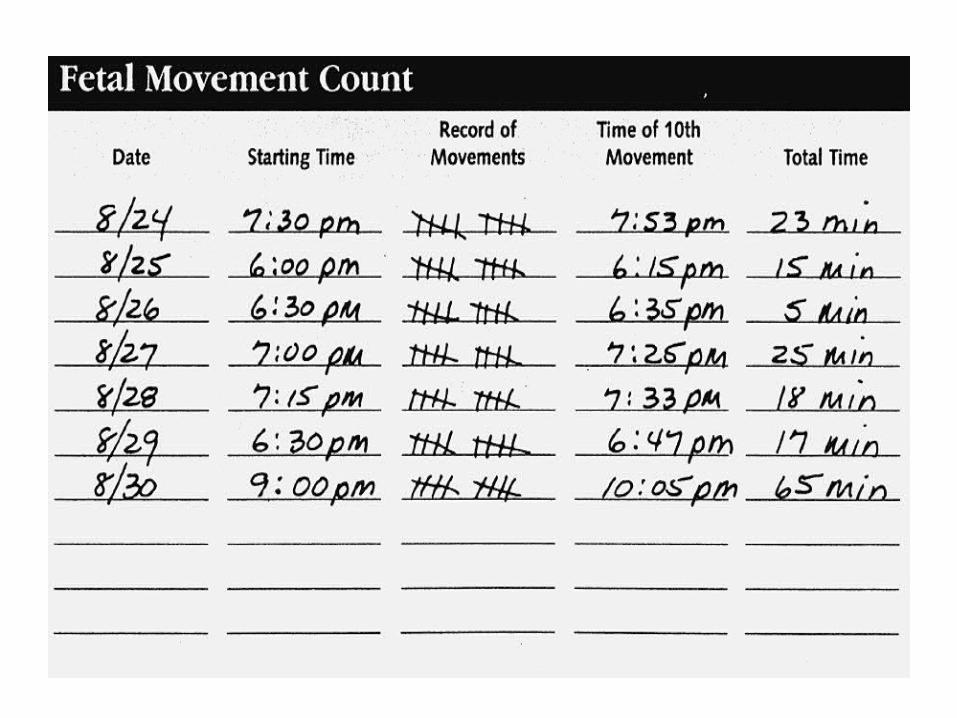
G 2 P1-0-0-0Previous stillbirth @ 39 weeksPresent gestation is 37 weeksHas been keeping a Fetal Activity Diary
(FAD) since 36 weeksNow to begin surveillance with weekly
NST
Fetal Movement Counts
FM indicator of intact Central Nervous System function
First line defense to identify the fetus in trouble
30-50% of IUFD occur in women with no identifiable risk factors
FAD
Methods for Fetal Movement Counts
Count-to-ten
Counting after meals
Evening monitoring
Interpretation
Report when criteria not metReport no movement over 8 hoursReport sudden violent increase in fetal
activity followed by cessation of movement
Report changes in normal pattern of fetal movement
Non-stress Test (NST)
Fetal movement typically accompanied by FHR accels when CNS intact and with adequate oxygenation
Procedure: Position sitting, semi-Fowler’s with tilt to
either side Good quality EFM tracing for 20-40 min May monitor up to 60 min
Interpretation
What to look at (5 parameters) What’s the baseline? Is there variability present? Any uterine activity present? Any accels present? Any decels present?
Assessment
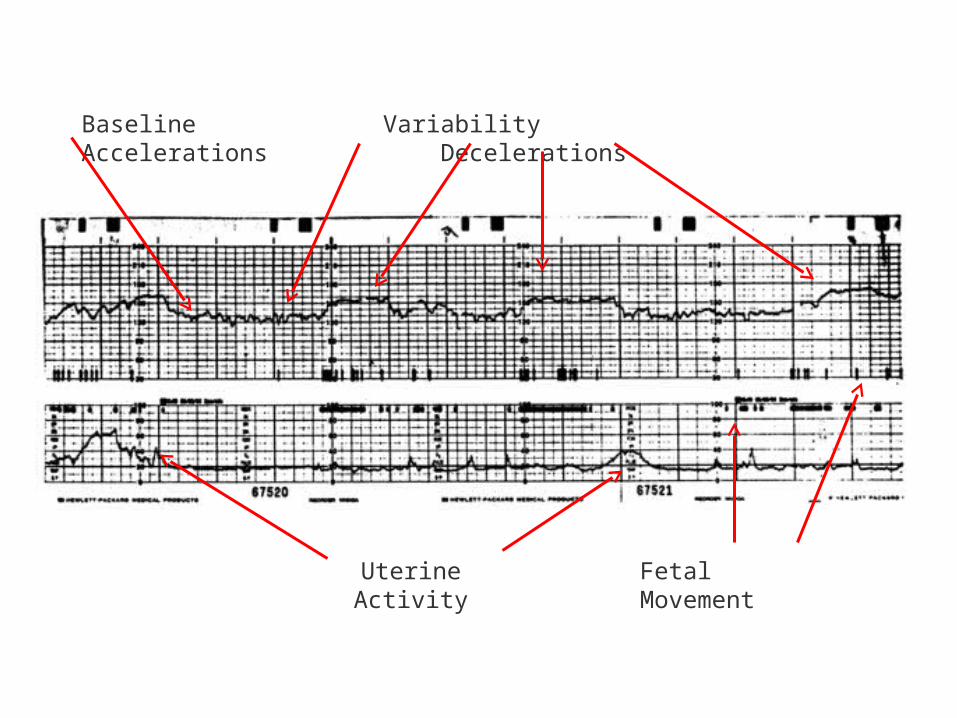
Baseline Variability Accelerations Decelerations
Uterine Activity Fetal Movement
Interpretation
Reactive: 2 accels in 20 min. 15 bpm X 15 sec. 15 sec. from start of accel to end of accel 15 bpm at apex of accel gestation < 32 weeks
• 10 bpm X 10 sec.• frequent decels of 10-20 sec.
Interpretation
Nonreactive: does not meet above criteria if not reactive in 60 min. unlikely to become
so; call HCP isolated decels seen in as many as 33%
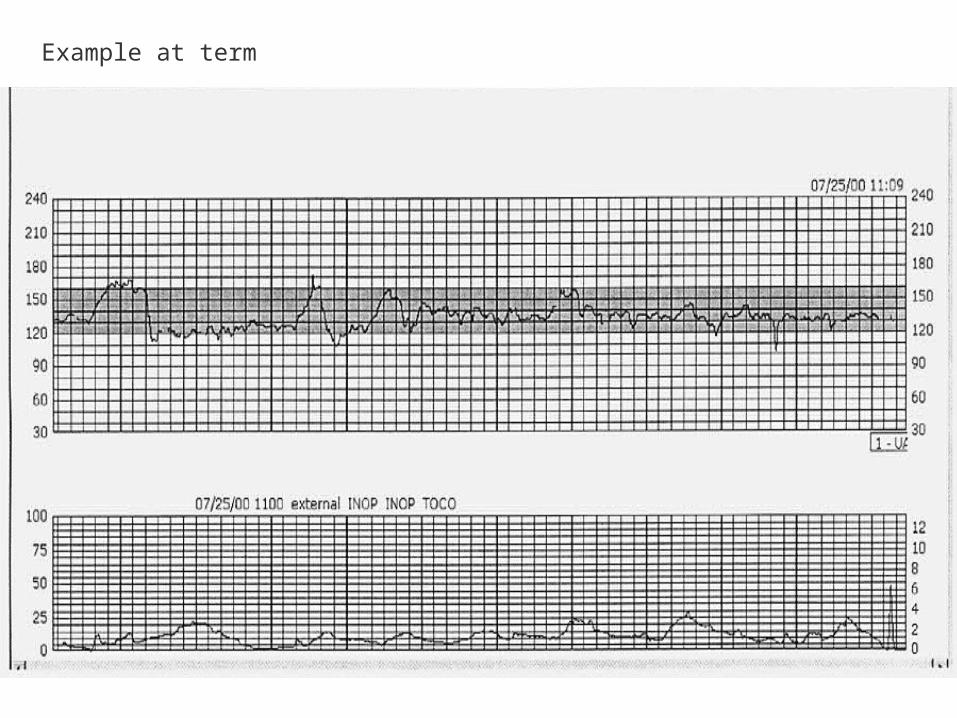
Example at term
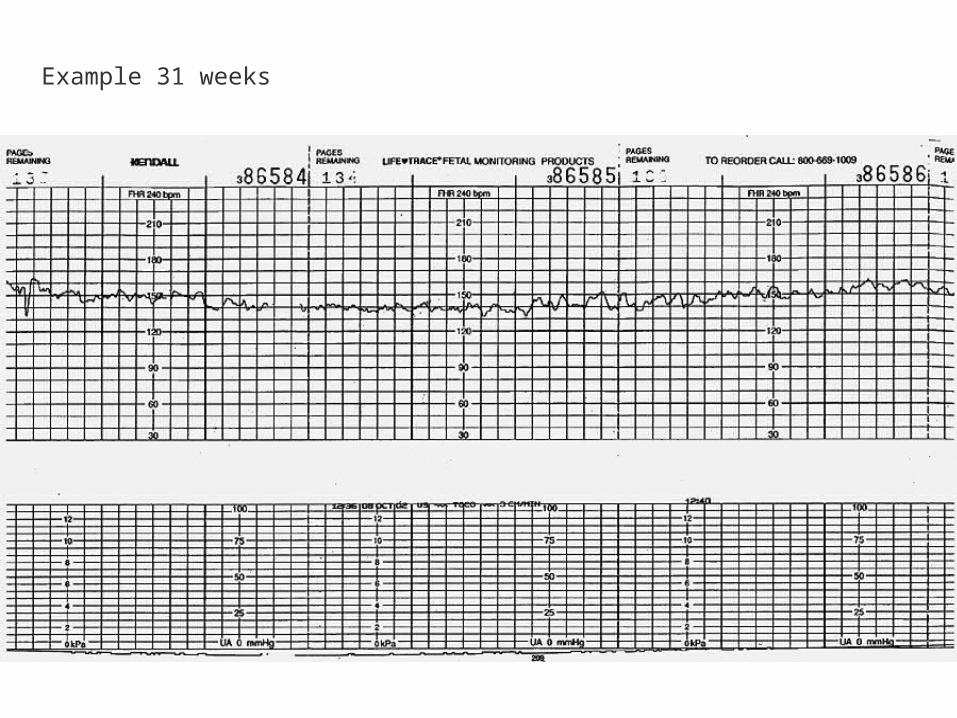
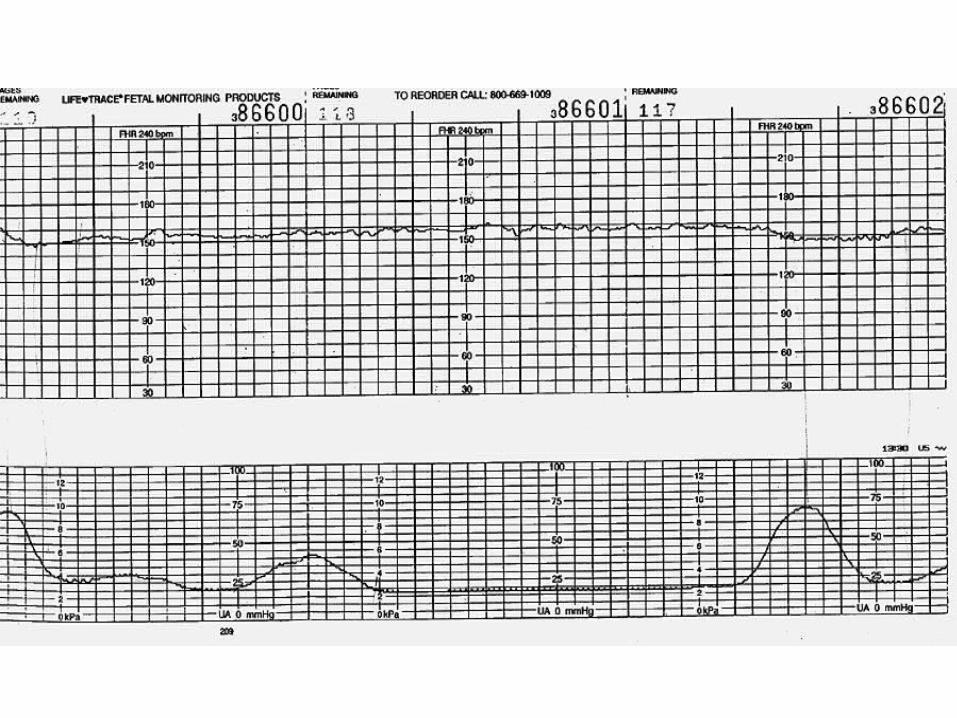
Example 31 weeks
Back to Ms. Sarah
Her NST is reactiveAnything else?
Chart the 5 parameters on strip & chart Call HCP and report Schedule next appointment Continue FAD
Retesting
If no risk factors, unlikely to have FD in one week
With risk factors, repeat 2 times a week
If pregnancy status changes, repeat in 24-48 hours
Patient: Ms. HertzelotDoctor: I. Ben Cursed M.D.
37 weeks gestationG1 P0Has not felt baby move for 8 hoursPlease do NST
Assessment
NST: Non-reactive after 40 minPossible causes:
fetal sleep smoking before coming Maternal medications immature CNS fetal hypoxia
Well, now what?Juice mythDo Fetal Acoustic Stimulation Test
(FAST) Usually elicited after 28 weeks Can be done after 10 min of non-reactive
pattern Handheld device generates a low frequency
(82 decibels) vibro-acoustic stimulus Apply for 3-5 sec avoiding fetal head; may
repeat X 2 at least 1 min apart May cause some level of stress
Results of FASTCauses ‘Moro’ or startle reflex if CNS
intactIncrease in FHR
1 accel of 15 bpm over 2 minutes 2 accels of 15 bpm for at least 15 sec within
5 minutes of testUseful way to reduce number of non-
reactive NST'sShortens testing time
Vibroacoustic Stimulation
Back to Ms. Hertzelot
Well, now what?
NST reactive with FAST Monitor until BL is restored Home with FAD Document on Strip and Chart
Patient: Ms. Shirley I. M. LateDoctor: I Ben Cursed M.D.
40 & 5/7 weeks gestationPlease do NSTResults:
NST: non-reactive FAST (or VAS): still non-reactive More monitoring: still non-reactive
Well, now what?
Options: Contraction Stress Test (CST)
• assumes uteroplacental insufficiency will show hypoxia with late decels with contractions
Biophysical Profile (BPP)• Ultrasound assessment of acute and chronic
markers show good predictor of fetal well-being
CSTModes
Nipple stimulation (BST)• may be poorly received by patient• noninvasive
IV oxytocin (OCT)• requires invasive procedure
Spontaneous contractions
Interpretation
FHR response to stress of contractions 3 contractions lasting 40-60 sec. in 10 min.
‘Negative’ is absence of late decels (That’s good!) ‘Positive’ is presence of late decels (That’s bad!)
> 50% of contractions--need to deliver
‘Equivocal’ is presence of some lates <50% of contractions
Hyperstimulation or Unsatisfactory Results Considered testing failure and are not clinically useful
‘Suspicious’ Variable Decelerations
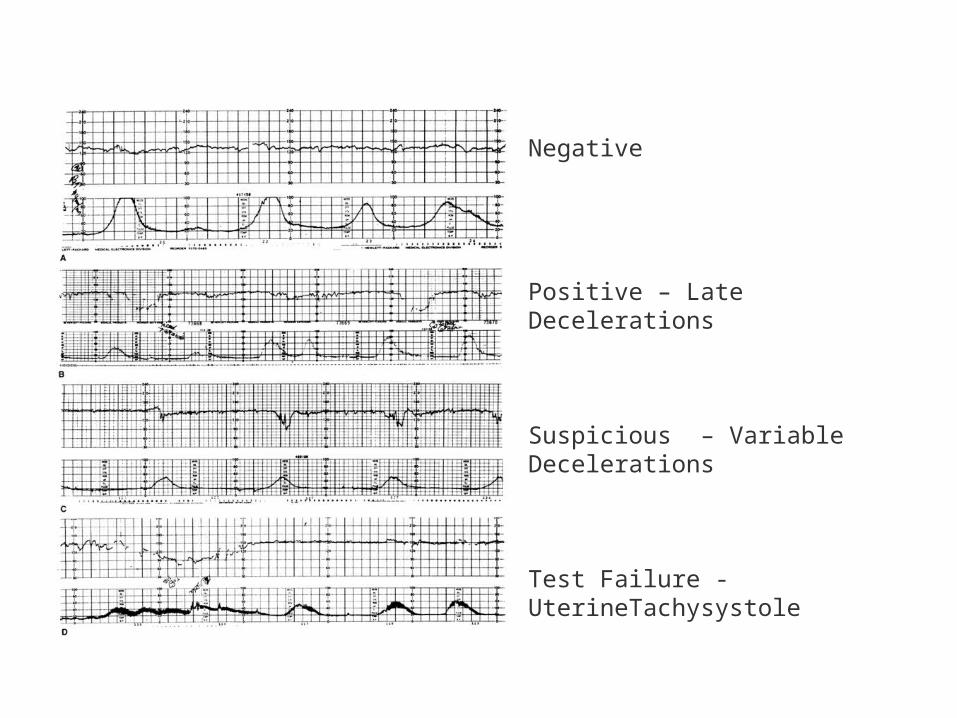
Negative
Positive – Late Decelerations
Suspicious – Variable Decelerations
Test Failure - UterineTachysystole
BPPParameters
Fetal Tone (FT) (7-8wks)
Fetal Movement (FM) (9wks)
Fetal Breathing Movements (FBM)) (20-21wks)
Amniotic Fluid Index (AFI) > 6 cms NST (Accelerations 30-32 wks)
Need high tech equipment/skilled technician
Non-invasive, highly predictive
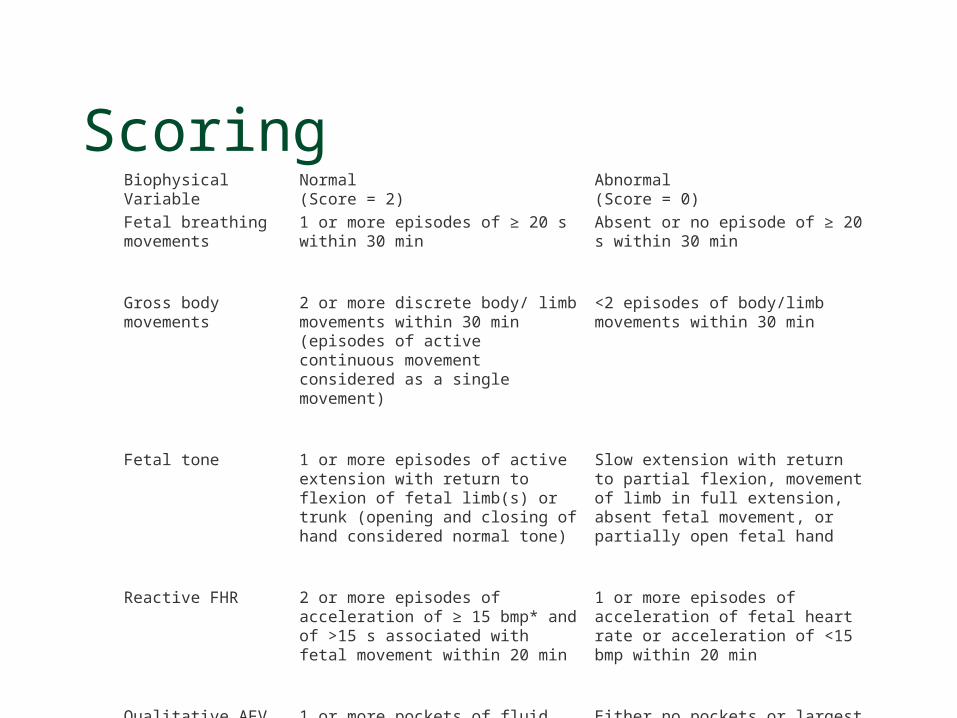
ScoringBiophysicalVariable
Normal(Score = 2)
Abnormal(Score = 0)
Fetal breathing movements
1 or more episodes of ≥ 20 s within 30 min Absent or no episode of ≥ 20 s within 30 min
Gross body movements 2 or more discrete body/ limb movements within 30 min (episodes of active continuous movement considered as a single movement)
<2 episodes of body/limb movements within 30 min
Fetal tone 1 or more episodes of active extension with return to flexion of fetal limb(s) or trunk (opening and closing of hand considered normal tone)
Slow extension with return to partial flexion, movement of limb in full extension, absent fetal movement, or partially open fetal hand
Reactive FHR 2 or more episodes of acceleration of ≥ 15 bmp* and of >15 s associated with fetal movement within 20 min
1 or more episodes of acceleration of fetal heart rate or acceleration of <15 bmp within 20 min
Qualitative AFV 1 or more pockets of fluid measuring ≥ 2 cm in vertical axis
Either no pockets or largest pocket <2 cm in vertical axis
Interpretation
Scoring 10 point scale (if performed with a NST) 8-10 indicates fetus in good condition 6 indicates need to repeat in 4-6 hours <6 indicates need for delivery AFI < 6 cms indicates delivery
Back to Ms. Late
Well, now what? NST: non-reactive CST: negative BPP: 6/10 (FT-2, FM-2, FBM-0, AFI-2,
NST-0) Report to HCP/document all findings Home with FAD Reschedule for repeat NST/BPP in 2-3 days
Other Surveillances
Amniocentesis Fetal lung maturity Testing- genetic, cultures, change in
optical density
Ultrasound Examination Uterine contents Fetal biometry / dating Fetal anatomic examination
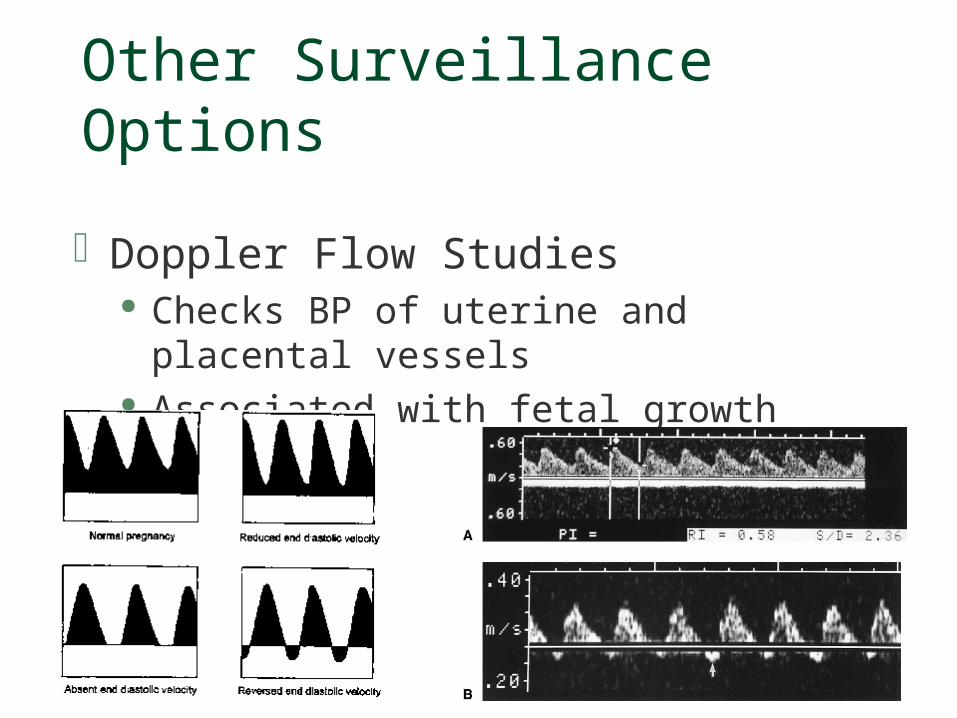
Other Surveillance Options
Doppler Flow Studies Checks BP of uterine and placental vessels Associated with fetal growth deficiency
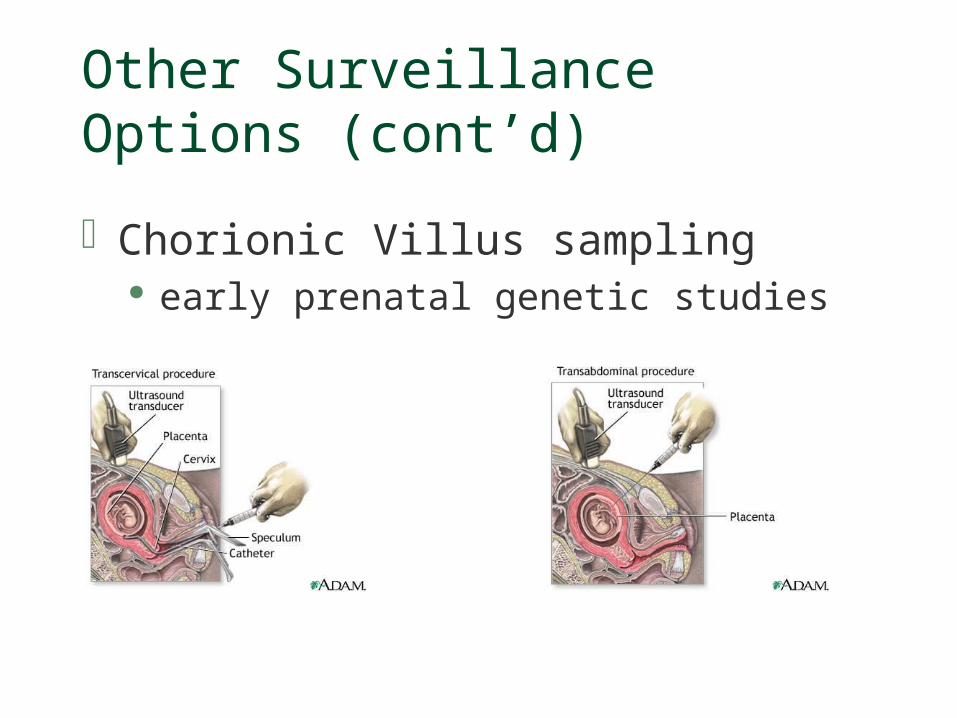
Other Surveillance Options (cont’d)
Chorionic Villus sampling early prenatal genetic studies

References:American Academy of Pediatrics, American College of Obstetricians &
Gynecologists, Guidelines for Perinatal Care (5th ed. 2002), Antepartum surveillance, pp. 89-107.
AWHONN Fetal Heart Rate Monitoring Principles and Practices 4th Ed.
Christensen FC, Olson K, Rayburn WF (2003). Cross-over trial comparing maternal acceptance of two fetal movement charts. Journal of Maternal-Fetal and Neonatal Medicine, 14(2), pp. 118-122.
Devoe, L, Glob. libr. women's med.,(ISSN: 1756-2228) 2008; DOI 10.3843/GLOWM.10210
Martin, E.J., Intrapartum Management Modules (3rd ed. 2002), Performing fetal surveillance testing, pp. 411-413.
Mattson, S., Smith, J.E., Core Curriculum for Maternal-Newborn Nursing (3rd. ed.,2004), Clinical practice pp. 165-166.
Simpson, K. R., Creehan, P.A., Perinatal Nursing (2nd ed., 2001), Fetal surveillance, pp. 147-154.





























