Embed Size (px)
Citation preview

INTERNATIONAL JOURNAL OF LEPROSY^
Volume 56, Number 4Printed in the U.S.A.
Antibodies to HIV-1 in Sera from Patients withMycobacterial Infections' , 2
Lalita ShivRaj, Shripad A. Patil, Anita Girdhar,Utpal Sengupta, K. V. Desikan, and H. Srinivasan3
The human immunodeficiency virus(HIV) (`'), a human retrovirus (lentivirus)earlier referred to as lymphadenopathy-as-sociated virus (LAV) ( 2) or human T-lym-photropic virus III (HTLV-111) (''), has beenidentified as the etiological agent of theacquired immunodeficiency syndrome(AIDS). The selective tropism of HIV forT-4 lymphocytes leads to T-cell depletionand the consequent lowering of T-cell de-fenses ( 1 "), giving rise to a variety of op-portunistic infections. Organisms such as theMycobacterium avium-complex and Af. tu-hemtlosis are reported to be present in asmany as 50% of the AIDS patients exam-ined for acid-fast bacilli ( 7 ). It has also beenreported that the immunological changes inlentivirus infections resemble those of lep-romatous leprosy (').
Both direct and indirect methods havebeen developed for identifying HIV-infect-ed persons ( 12). Almost all HIV-infectedpersons are seropositive for specific anti-bodies, and the virus can be isolated from50% to 80% of them ( 14 ' ' 8 ). A number ofserological tests, including the enzyme-linked immunosorbent assay (ELISA) ( 5 ' '')
and the Western blot (WB) ( 5 . 20 ) and im-munofluorescence (IF) ( 4 1 ) assays, are
' Received for publication on 18 February 1988; ac-cepted for publication in revised lbrm on 11 August1988.
= A part of this work was presented at the V Con-ference on Modern Approaches to Vaccines IncludingPrevention of AIDS, 9-13 September 1987, Cold SpringHarbor Laboratory, Cold Spring Harbor, New York,U.S.A. An abstract of the work appears in the abstractbook of the IV International Conference on AIDS held12-16 June 1988 in Stockholm, Sweden.
L. ShivRaj, Ph.D., Research Officer (Immunology);S. A. Patil, M.Sc., Assistant Research Officer (Immu-nology); A. Girdhar, M.13.13.S., Research Officer (Clin-ical); U. Sengupta, Ph.D., Deputy Director (Immu-nology); K. V. Desikan, M.D., Former Director; H.Srinivasan, F.R.C.S., Director, Central JALMA Insti-tute for Leprosy (ICMR), Taj Ganj, Agra 282001, In-dia.
available for the detection of anti-HIV an-tibodies. The ELISA and WB assay are beingused in most laboratories for the screeningand confirmation of HIV infection. How-ever, both false-positivity and crossreactiv-ity by W13 assay have been documented(3.8.17,21) .
The present study was undertaken to in-vestigate patients (of north India origin) withmycobacterial infections for the presence ofanti-HIV-1 antibodies and the possible an-tigenic crossreactivity between these twopathogens.
MATERIALS AND METHODSSubjects. Sera were collected from 348
patients with different types of leprosy (clas-sified according to Ridley-Jopling criteria),33 patients with pulmonary tuberculosis,and 29 healthy contacts of leprosy patients.There were two control groups. The firstcontrol group consisted of 30 normal healthyEuropean subjects, unlikely to have had sig-nificant exposure to environmental myco-bacteria; they were included to demonstratethat the assay conditions were adequate toprevent false-positive reactions. The secondcontrol group consisted of 38 normal healthyIndians, not closely exposed to tuberculosisor leprosy. This group would have hadgreater exposure to environmental myco-bacteria than the European controls.
ELISA. All of the 478 sera were testedfor antibodies to HIV-1 IgG by an ELISAusing the Wellcozyme HTLV-III kit (U.K.).
Western blot assay. Sixty-nine randomlychosen sera from among those tested byELISA were also tested for anti-HIV-1 IgGantibodies to the different protein antigenson nitrocellulose strips using the Biotech/DuPont kit (U.S.A.). These included 43samples from leprosy patients (14 LL, 13BB, 12 BT, 3 TT, IN), 21 from tuberculosispatients, and 5 from healthy contacts of lep-rosy patients. Thirty sera from the Euro-
546

Reaction to HIVantigen
Leprosy patients (N = 43)
^> p66^
5 (3BB, 2LL)
^
p66^
5 (21313, 2BT, 1 N)
^
p55^
22 (91313, 6LL, 5I3T, ITT, IN)
^
p51^
0
^
gp41^
I (BB)
^
p24^
14 (7BB, 4LL, 1 IIT, ITT, IN)
^
p17^
3 (2BI3, 113T)
56, 4^ SidiRaj, et al.: Antibodies to HIV-1^ 547
TABLE 1. Western blot (WB) reaction patterns in different types of leprosy.
Leprosyty pc.'
No. testedby WI3
No. showing'
reactions(%) p55
LL 14 11 (78.6) 6BB 13 12 (92.3) 9BT 12 7 (58.3) 5TT 3 2— IN 1 I I
Total 43 33 (76.7) 22
47^
3^2^
11^
2^1^
911^
3
14^5^5^3^1^50
No. showing reactions to HIV antigens^
Total
p24^>p66^p66^p17^gp41^bands
LL = lepromatous leprosy, 1313 = borderline borderline; BT = borderline tuberculoid; TT = tuberculoid; N= neuritic leprosy.
pean control group and 33 sera from theIndian control group were also tested by thismethod.
RESULTSNone of the 478 sera were positive for
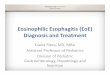
anti-HIV-1 antibodies by the ELISA. Thir-ty-three of 43 leprosy patients (Table 1), 7of the 21 tuberculosis patients, and 4 of the5 healthy contacts of leprosy patients showedone, two, or multiple bands to the differentHIV-1 proteins by the Western blot assay(Table 2). A reaction to p55 was observedin 31 of 69 sera tested, while no reactionwas observed to gp120, gp160, or p31 an-tigens (Fig. 1).
Reactions to the p24 protein antigen, oneof the specific markers for HIV-1 infection,were seen in 17 samples: 14 leprosy pa-tients, 2 healthy contacts, and 1 tuberculosispatient. A reaction to the gp41 antigen,another specific marker of HIV-1, was seenin 1 BB leprosy patient in combination withp24, p55, and a band above the p66 region(Table 3). One of the 33 normal healthyIndians showed a p17 band (Fig. 2), whilenone of the 30 European control sera showedany reaction (Fig. 3).
DISCUSSIONAn ELISA is used as a screening test for
the diagnosis of HIV-1 infection. In thisstudy of 478 sera from northern India sub-jects, none was positive for HIV-1 by ELISA.Miller, et al. (i 5 ) have also reported similarfindings on 311 leprosy sera screened bythem for anti-HIV-1 antibodies by ELISA.However, they had not tested any of theirsera by the WB method. Earlier studies ( 3 . 8 )have shown that although sera may be non-reactive by competitive ELISA (Wellcome)for HIV- I antibodies, they may still show"false-positive" reactions by the WB assay.Hence, 69 randomly chosen samples frompersons infected with or exposed to myco-bacteria along with 63 suitable controls, al-though all were negative by ELISA, weretested by us by WB assay. It is interestingthat 44 of the patients (tuberculosis and lep-rosy) and healthy contacts of leprosy pa-tients showed crossreactivity to variousHIV-1 proteins, while the remaining 25 weretotally nonreactive. In contrast, only 1 outof 63 controls showed a single band at thepI7 region. This subject had earlier sufferedfrom high proteinuria and albuminuria andis now normal.
TABLE 2. Frequency of HIV bands observed in patients with mycobacterial infectionsand healthy contacts.
Healthycontacts(N = 5)
TB patients Total (N = 69)(N = 21)
No.
0 7 100 6 9
3 6 31 450
0 017 25
0 4 6

548^ International Journal of Leprosy^ 1988
TABLE 3. W13 reaction patterns of sera from patients with mycobacteria infections andhealthy contacts.
Leprosy patients (N = 43)Healthycontacts(N = 5)
TBpatients(N
Total(N = 69)
5 (3LL, I B13, ITT) 0 I 62 (21311) 0 0 2I (11T) 0 0 1I (LL) 1 0 -)_1^(1313) 0 0 I2(11111,^IN) 0 0 2I^(1113) I 0 2I^(1311) 0 0 1
14 (6LL, 31111, 4BT, ITT) 1 5 20I (I3T) 0 0 II (LL) 0 0 II (B11) 0 0 II (13T) 0 0 I0 0 1 I1^(1313) 0 0 10 I 0 1
33 (121313, 1ILL, 713T, 2TT, IN) 4 7 44
Reaction to 111V antigens
p24 alonep24 + p55p24 + p17p24 + p66p24 + p55 + pI7p24 + p55 + p66p24 + p55 + >p66p24 1 p55 + gp4 I + >p66p55 alonep66 alone>p66 alonep17 alonep55 + p66p55 + p17p66 + >p66p55 + p51 + p66Total
False-positive WB reactions to the var-ious HIV-1 antigens have been reported inblood donors from Sweden ( 3), France ( 8),and The Netherlands ( 2 ') but the rate hasbeen quite low, less than 0.7%. There hasbeen no report so far on crossrcactivity byWB assay in mycobacterial infections. It istherefore interesting to find such a high rateof crossrcactivity (44/69, 64%) in this sam-ple of patients.
An isolated antibody reactivity to the p24protein of HIV-1 in WB may represent false-positivity, especially in low-risk popula-tions, and can persist for about 2 years with-out signs of HIV-1 infection (21 ); or it mayrepresent early HIV-1 infection ( 9 ' 13 ' 17 ). Ahigh rate of crossreactivity to the core pro-teins by Western blot has been observed inpatients with multiple sclerosis (42.2%), cu-taneous T-cell lymphoma (24%), and in pa-tients with dermatological disorders (12.7%)( 17) which may be due to either an infectionwith a virus immunologically related to theknown human retroviruses or an early in-fection with HIV-1. In the present study,sera from 14 leprosy patients, 2 healthy con-tacts of leprosy patients, and 1 tuberculosispatient have shown antibodies to the p24antigen alone or in combination with otherbands. One BB leprosy patient showed athin gp41 band in addition to the p24, p55,
and a band above p66. This patient has beenfollowed up for 18 months and his condi-tion has improved. His bacterial index (BI)which was 2 has become negative, but hecontinues to receive multiple drug therapyfor leprosy. He has not shown any signs ofHIV infection so far. In an earlier report( 2 !), among 150 healthy Finnish personstested by WB one had antibodies to p24 andp55 of HIV-1, but in the present study noneof the 63 normal persons showed antibodiesto these two core HIV-1 proteins.
There may be certain antigens in HIV-1and mycobacteria which may be similar,accounting for the crossreactivity observedin this study. Conceivably this could be re-lated to a similar immunologic impairmentin HIV-1 and mycobacterial infections, es-pecially lepromatous leprosy ('). Therefore,it would be worthwhile to conduct both im-munologic and genetic studies to look forcommon antigenic loci and similar gene se-quences between these two unrelated patho-gens.
Our study indicates that a significant pro-portion of leprosy sera react with severalHIV-1 antigens. In a country such as India,where leprosy and tuberculosis are highlyprevalent, the results of the Western blotassay should be interpreted with great cau-tion using stringent criteria for the diagnosis

56, 4^ ShivRaj, et al.: Antibodies to HIV-1^ 549
2345I7
I^•
■^1.1 _
t^
14Is
^ 1
11
_^ I^I 1^ 0_^ 11
^212•27
) 1{13 13 13 .0^if) la
1 .0 (XI al^-o -coLT1
1'4 0)0 0
FIG. I. Reactivity of representative samples testedfor anti-HIV-1 by WB. Lane I = negative control; lane10 = high positive control; lane 19 = weak positivecontrol; lanes 2, 9, 12, 16, 17, 18, 20, 22 = LL sera;lanes 3, 4, 5, 6, 8, 21, 25, 27 = BB sera; lanes 7, 11,14, 15, 23, 24, 26 = 11T sera; lane 13 = N serum.
of HIV-1 infection. Additional confirma-tory tests for HIV-1 already in practice maybe useful in such situations.
SUMMARYSera from 478 persons (348 leprosy pa-
tients, 33 tuberculosis patients, 29 healthycontacts of leprosy patients, 38 normalhealthy Indians, and 30 normal healthy Eu-ropeans) were screened for anti-HIV-1 IgGantibodies by ELISA. None was positive. Inaddition, 132 samples (from 43 leprosy pa-tients, 21 tuberculosis patients, 5 healthycontacts of leprosy patients, 33 normalhealthy Indians, and 30 normal healthy Eu-ropeans) were also tested by Western blotassay for anti-HIV-1 IgG antibodies. Only1 of the 63 healthy subjects expressed aprominent p17 band. One or more bandswere found in 44 (leprosy patients 33/43,tuberculosis patients 7/21, and leprosy con-tacts 4/5) of the remaining 69 sera. Anti-
123
5678910111213
15IL I I^I TM 16
1718192021222324252627282930313233343536
I-0
I-0 j/( Tv
40 V V V to^Ura(,)
-0^4.71 CJI 01 -0•ts• —• al as
FIG. 2. Reactivity of normal human sera from In-dians to HIV- l antigens by W13. Lane 7 = negativecontrol; lane 16 = high positive control; lane 25 = weakpositive control; remaining lanes = normal healthy In-dian sera (33); lane 20 = normal healthy subject whohad suffered from proteinuria and albuminuria show-ing p17 band.
body to the HI V-1-speci fic antigen p24 wasexpressed by 17 of these subjects (14/43 lep-rosy patients, 1/21 tuberculosis patients, and2/5 leprosy contacts), either as a single bandor in combination with other bands. Thisraises the possibility of a common antigenicpattern between HIV-1 and mycobacteria,especially Mycobacterium leprac.
RESUMENUsando un ensayo inmunoenzimiitico se buscaron
anticuerpos IgG anti-HIV-1 en los sueros de 478 per-sonas (348 pacientes con lepra, 33 pacientes con tu-berculosis, 29 contactos sanos de pacientes con lepra,38 individuos sanos de la India, y 30 europeos sanos).
■
-^I
-0

5 50^ International Journal of Leprosy^ 1988
123456789■ • '• IMO III I io11121314151G17
192021222324252627
230313233
/^
I ItOtit;^10 tOV ui ui m
o, N Q100
FIG. 3. Reactivity of normal healthy European serato HIV- l antigens by WII. Lane 1 = negative control;lane 10 = high positive control; lane 19 = weak positivecontrol; remaining lanes = normal healthy Europeansera from 30 subjects negative for anti-HIV-1 IgG an-tibodies.
Ninguno result() positivo. Ademds, 132 muestras (de43 pacientes con lepra, 21 pacientes con tuberculosis,5 contactos sanos de pacientes con lepra, 33 indiies y30 europeos sanos) tambien se probaron por inmu-noelectrotransferencia ("Western blot assay") parabuscar anticuerpos IgG anti-HIV-1. Solo I de 63 su-jetos sanos expresO una banda p17 prominente. Unao mds bandas fueron encontradas en 44 de los 69 suerosrestantes (33/43 pacientes con lepra, 7/21 pacientes contuberculosis, 4/5 contactos de pacientes con lepra). Diezy siete de estos individuos (14/43 pacientes con lepra,1/12 pacientes con tuberculosis, y 2/5 contactospacientes con lepra) tuvieron anticuerpos contra elantigeno p24 especifico de HIV-1 de manera aislada oen combinaciOn con otras bandas. Esto introduce laposibilidad de que pueda existir algUn patron antige-nico comim entre HIV-1 y las microbacterias, espe-cialmente Mycobacterium leprae.
RESUME
Des Cchantillons de serum provenant de 478 indi-vidus (348 malades de la lepre, 33 patients atteints de
tuberculose, 29 contacts sains de malades de Ia lepre,38 indiens en bonne sante et 30 curopeens egalementen bonne sante) ont etc passes en revue afin de mettreen evidence les anticorps IgG anti HIV 1, au moyende methodes ELISA. Aucun serum n'a etc trouve po-sitil. En outre, on a egalement etudie 132 Cchantillons,provenant de 43 malades de la lepre, 21 sujets tuber-culeux, de 5 contacts sains de malades de la lepre, de33 indiens normaux en bonne sante, ct de 30 europeensegalement en bonne sante, en utilisant une epreuve deWestern blot pour les anticorps IgG anti I II V 1. Unseul seulement des 63 individus en bonne sante a revileune bande p 1 7. Dans 44 des Cchantillons de serum,parmi les 69 autres, on a observe une ou plusieursbandes : chez 33 malades de la lepre sur 43, chez 7sujets tuberculeux sur 21, et chez 4 contacts sur 5. Chez17 de ces individus, un anticorps contre l'antigene spe-cifique P24 de 111V-1, etait exprime : chez 14 maladesde la lepre sur 43, chez 1 malade dc tuberculose sur21, et chez 2 contacts lepreux sur 5 parmi les contactsde malades de la lepre. Ces anticorps Ctaient exprimessoit sous forme (rune bande unique, soil en combi-naison avec d'autres bandes. Ces resultats font entre-voir Ia possibilite d'un profil antigCnique commun entreHIV-1 et les mycobacteries, en particulier Mycobac-terium leprae.
Acknowledgments. We thank Mr. P. N. Sharma forthe technical assistance, Mr. Hari Om Agarwal for pho-tography, and Mr. Anil Chopra for secretarial exper-tise. Normal healthy European sera were obtained withthe kind courtesy of Dr. H. D. Engers, World HealthOrganization, Geneva, Switzerland, and Western blotkits were kindly supplied by LEPRA, U.K.
REFERENCESI. BARNASS, S. Lentiviruses and mycobacterial dis-
eases. Immunol. Today 8 (1987) 9.2. BARRE SINOUSSI, F., CHERMANN, J. C., REY, F.,
NUGEYRE, M. T., CHAMARET, S., GRUEST, J.,DAUGUET, C., AXLER-BLIN, C., VFZINET-BRUN, F.,Rouzioux, C., ROZENBAUM, W. and MONTAGNIER,
L. Isolation of a T-lymphotropic retrovirus froma patient at risk for acquired immuno-deficiencysyndrome (AIDS). Science 220 (1983) 868-871.
3. BIBERFELD, G., BREDBERG-RADEN, U., BOTTIGER,
B., PUTKONEN, P. 0., BLOMI3ERG, J., JUTO, P. andWADELL, G. Blood donor sera with false positiveWestern blot reactions to human immunodefi-ciency virus. Lancet 2 (1986) 289-290.
4. BLUMBERG, R. S., SANDSTROM, E. G., PARADIS, T.J., NEUMEYER, D. N., SARNGADIIARAN, M. G.,HARTSHORN, K. L., BYINGTON, R. E., HIRSCH, M.S. and SCHOOLEY, R. T. Detection of human T-celllymphotropic virus type III-related antigens andanti-human T-cell lymphotropic virus type Iii an-tibodies by anticomplementary immunofluores-cence. J. Clin. Microbiol. 23 (1986) 1072-1077.
5. CENTERS FOR DISEASE CONTROL. Provisional Pub-lic Health Service inter-gency recommendation for

56, 4^ ShivRaj, et al.: Antibodies to HIV-1^ 551
screening donated blood and plasma for antibodyto the virus causing acquired immunodeficiencysyndrome. MMWR 34 (1985) 1-5.
6. COFFIN, J., HAASE, A., LEVY, J. A., MONTAGNIER,
L., OROSZLAN, S., TEICH, N., TEMIN, H.,Tovosii MA, K., VARMUS, H., VOGT, P. and WEISS,
R. Human immunodeficiency viruses. Science 232(1986) 697.
7. COLLINS, F. M. Mycobacterium arium -complexinfections and development of the acquired im-munodeficiency syndrome: casual opportunist orcausal cofactor? Int. J. Lepr. 54 (1986) 458-474.
8. COUROUCE, A.-M., MULLER, J.-Y. and RicilARD,D. False-positive Western blot reactions to humanimmunodeficiency virus in blood donors. Lancet2 (1986) 921-922.
9. ESTEBAN, J. I., Suns , J. W. K., TAI, C. C., BODNER,
A. J., KAY, J. W. D. and ALTER, H. J. Importanceof Western blot analysis in predicting infectivityof anti-HTLV-III/LAV positive blood. Lancet 2(1985) 1083-1086.
10. Fixeci, A. S. Acquired immunodeficiency syn-drome: epidemiologic immunologic and therapeu-tic considerations. Ann. Intern. Mcd. 110 (1984)92-106.
1 I. GALLO, D., Dices, J. L., SHELL, G. R., DAILEY, P.J., HOFFMAN, M. N. and RIGGS, J. L. Comparisonof detection of antibody to the acquired immu-nodeficiency syndrome virus by enzyme immu-noassasy, immuno-fluorescence and Western blotmethods. J. Clin. Microbiol. 23 (1986) 1049-1051.
12. GUPTA, P., BALACHANDRAN, R., GROVIT, K.,WEBSTER, D. and RINALDO, C., JR. Detection ofhuman immunodeficiency virus by reverse tran-scriptase assay, antigen capture assay and radioim-munoassay. J. Clin. Microbiol. 25 (1987) 1122-1125.
13. LANGE, J. M. A., COUTINHO, R. A., KRONE, W. J.A., VERDONCK, L. F., DANNER, S. A., NOORDAA,J. V. D. and GOUDSMIT, J. Distinct IgG recognitionpatterns during progression of sub-clinical infec-tion with lymphadenopathy associated virus/hu-man T-Iymphotropic virus III. Br. Mcd. J. 292(1986) 228-230.
14. MARKHAM, P. D., SALAHUDDIN, S. Z., POPOVIC,M., PATEL, A., VEREN, K., FLADAGER, A., ORN-
DORFF, S. and GALLO, R. C. Advances in the iso-lation of HTLV-III from patients with AIDS andAIDS-related complex and from donors at risk.Cancer Res. 45 Suppl. (1985) 45885-4591S.
15. MILLER, R. A., COLLIER, A. C., BUCHANAN, T. M.and HANDSFIELD, H. H. Seroepidemiologic screen-ing for antibodies to LAV/HTLV III in Sri Lanka,1980-1982. N. Engl. J. Med. 313 (1985) 1352-1353.
16. PoEovic, M., SARNGADHARAN, M. G., READ, E.and GALLO, R. C. Detection, isolation and con-tinuous production of cytopathic retroviruses(IITLV-III) from patients with AIDS and pre-AIDS. Science 224 (1984) 497-500.
17. RANKI, A., JOHANSSON, E. and KROHN, K. Inter-pretation of antibodies reacting solely with humanretroviral core proteins. N. Engl. J. Med. 318 (1988)448-449.
18. SALAHUDDIN, S. Z., MARKHAM, P. D., POPOVIC,M., SARNGADHARAN, M. G., ORNDORFF, S., FLAD-
AGER, A., PATEL, A., GOLD, J. and GALLO, R. C.Isolation of infectious human T-cell leukemia/lymphotropic virus type III (HTLV-III) from pa-tients with acquired immunodeficiency syndrome(AIDS) or AIDS-related complex (ARC) and fromhealthy carriers; a study of risk groups and tissuesources. Proc. Natl. Acad. Sci. U.S.A. 82 (1985)5530-5534.
19. SARNGADHARAN, M. G., PoPovic, M., BRUCH, L.,SCHUPBACII, J. and GALLO, R. C. Antibodies re-active with human T-lymphotropic rctroviruses(I ITLV-III) in the serum of patients with AIDS.Science 224 (1984) 506-508.
20. TSANG, V. C. W., HANCOCK, K., WILSON, M.,
PALMER, D. F., WHALEY, S. D., MCDOUGAL, J. S.and KENNEDY, S. Enzyme-linked immunoelectro-transfer blot technique (Western blot) for humanT-lymphotrophic virus type III/lymphadenopa-thy-associated virus (HTLV-I I I/LAV) antibodies.Atlanta: Centers for Disease Control, 1986, Im-munology Series No. 15 Procedural Guide.
21. VAN DER POEL, C. L., REESINK, H. W., TERSMETTE,
M., LELIE, P. N., HUISMAN, J. G. and MIEDEMA,
F. Blood donations reactive for HIV in Westernblot, but noninfective in culture and recipients ofblood. Lancet 2 (1986) 752-753.