Embed Size (px)
Citation preview

COURSE 2 | MODULE 3
BloodbornePathogens
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Introduction
Introduction to BacteriaBacteria constitute a large domain of prokaryotic microorganisms. Typically a few micrometers in length, bacteria have a wide range of shapes, ranging from spheres to rods and spirals. There are typically 40 million bacterial cells in a gram of soil and a million bacterial cells in a milliliter of fresh water; in all, there are approximately five nonillion (5×1030) bacteria on Earth, forming a capsid that exceeds that of all plants and animals.
The ancestors of modern bacteria were single-celled microorganisms that were the first forms of life to appear on Earth, about 4 billion years ago. For about 3 billion years, all organisms were microscopic, and bacteria were the dominant forms of life.
There are approximately ten times as many bacterial cells in the human floraas there are human cells in the body, with large numbers of bacteria on the skinand as gut flora. The vast majority of the bacteria in the body are rendered harmless by the protective effects of the immune system, and a few are beneficial. However, a few species of bacteria are pathogenic and cause infectious diseases, including cholera, syphilis, anthrax, leprosy, and bubonic plague.
The most common fatal bacterial diseases are respiratory infections, with tuberculosis alone killing about 2 million people a year. In developed countries, antibiotics are used to treat bacterial infections. Bacterial cells do not contain a nucleus and rarely harbor membrane-bound organelles.
This eBook ends with a module review. Follow the link on the last page to log in to your Ansell Certified account to complete the module test.
A passing score of 85% is required on all module tests to receive a certificate.
Navigation links are provided in the sidebar. The Ansell Certified site and this eBook were developed to be iPad friendly. Use the Download link located in the site menu to save to your iPad with the Open in iBooks option for offline use in your library.
E. coli bacteria
Next >>
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
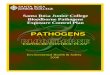
Structure of BacteriaBacteria display a wide diversity of shapes and sizes, called morphologies. Bacterial cells are typically 0.5–5.0 micrometers in length.
Most bacterial species are either spherical, called cocci (grain), or rod-shaped, called bacilli (stick). Elongation is associated with swimming. Some rod-shaped bacteria, called vibrio, are slightly curved or comma-shaped; others, can be spiral-shaped, called spirilla, or tightly coiled, called spirochaetes.
A small number of species even have tetrahedral or cuboidal shapes. This wide variety of shapes is determined by the bacterial cell wall and cytoskeleton, and is important because it can influence the ability of bacteria to acquire nutrients, attach to surfaces, swim through liquids and escape predators.
Many bacterial species exist simply as single cells, others associate in characteristic patterns: Neisseria form diploids (pairs), Streptococcus form chains, and Staphylococcus group together in “bunch of grapes” clusters. Bacteria can also be elongated to form filaments, for example the Actinobacteria.
Bacteria often attach to surfaces and form dense aggregations called biofilms or bacterial mats. These films can range from a few micro-meters in thickness to up to half a meter in depth, and may contain multiple species of bacteria.
Bacteria living in biofilms display a complex arrangement of cells and extracellular components, forming secondary structures such as micro colonies, through which there are networks of channels to enable better diffusion of nutrients.
Biofilms are also important in medicine, as these structures are often present during chronic bacterial
infections or in infections of implanted medical devices, and bacteria protected within biofilms are much harder to kill than individual isolated bacteria.
Structure of Bacteria
Scanning electron micrograph shows a strain of Actinobacteria-mycobacterium tuberculosis.
<< Back Next >>
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
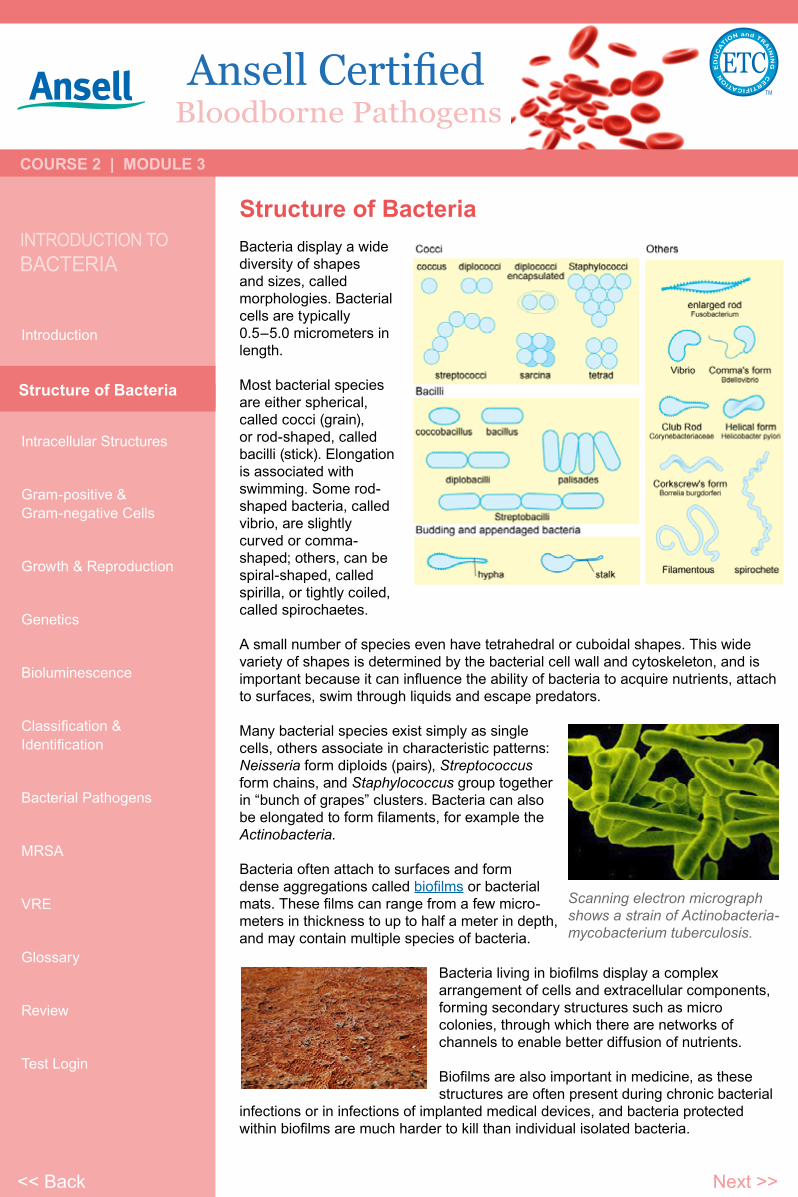
Intracellular StructuresThe bacterial cell is surrounded by a lipid membrane, or cell membrane, which encloses the contents of the cell and acts as a barrier to hold nutrients, proteins and other essential components of the cytoplasm within the cell. Most bacteria do not have a membrane-bound nucleus, and their genetic material is typically a single circular chromosome located in the cytoplasm in an irregularly shaped body called the nucleoid. Like all living organisms, bacteria contain ribosomes for the production of proteins.
Some bacteria produce intracellular nutrient storage granules, such as glycogen and polyphosphate. These granules enable bacteria to store compounds for later use. Certain bacterial species, such as the photosynthetic Cyanobacteria, produce internal gas vesicles, which they use to regulate their buoyancy – allowing them to move up or down into water layers with different light intensities and nutrient levels.
Extracellular structures
In most bacteria a cell wall is present on the outside of the cytoplasmic membrane. A common bacterial cell wall material is peptidoglycan, which is made from polysaccharide chains cross-linked by peptides containing D-amino acids. The cell wall is essential to the survival of many bacteria, and the antibiotic penicillin is able to kill bacteria by inhibiting a step in the synthesis of peptidoglycan.
Intracellular Structures
<< Back Next >>
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
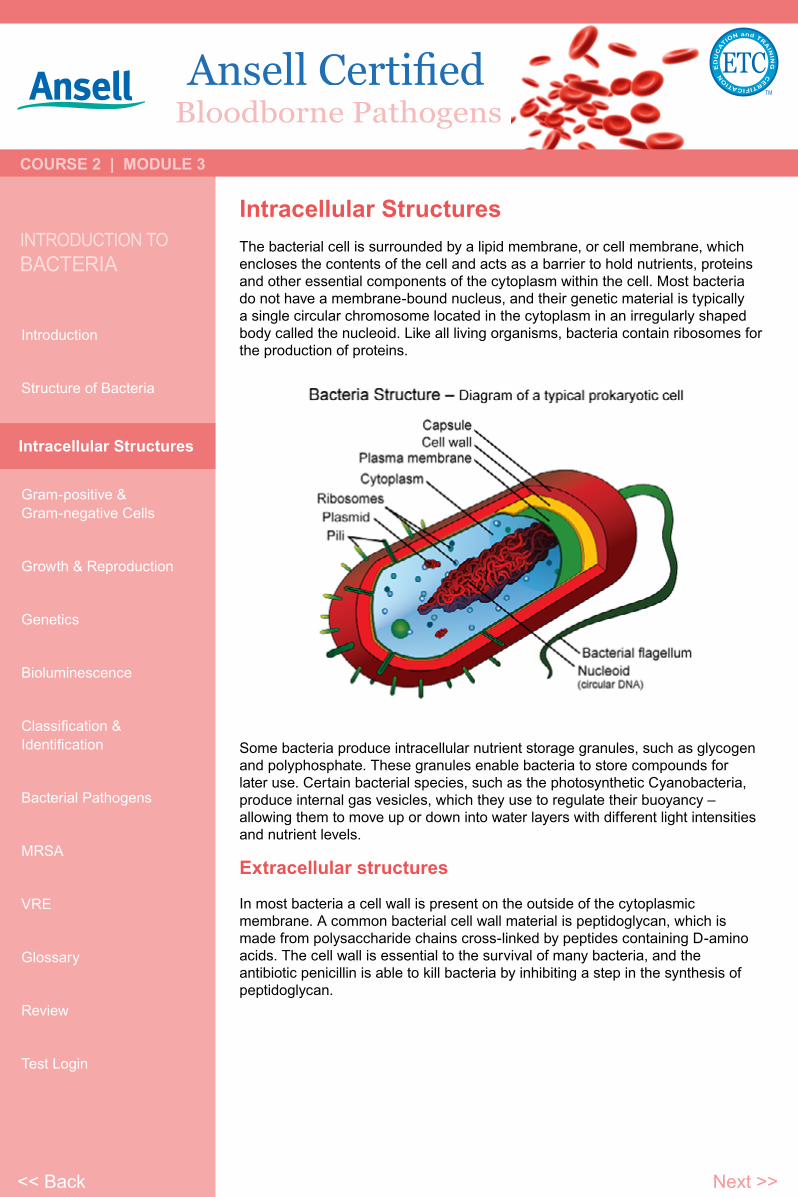
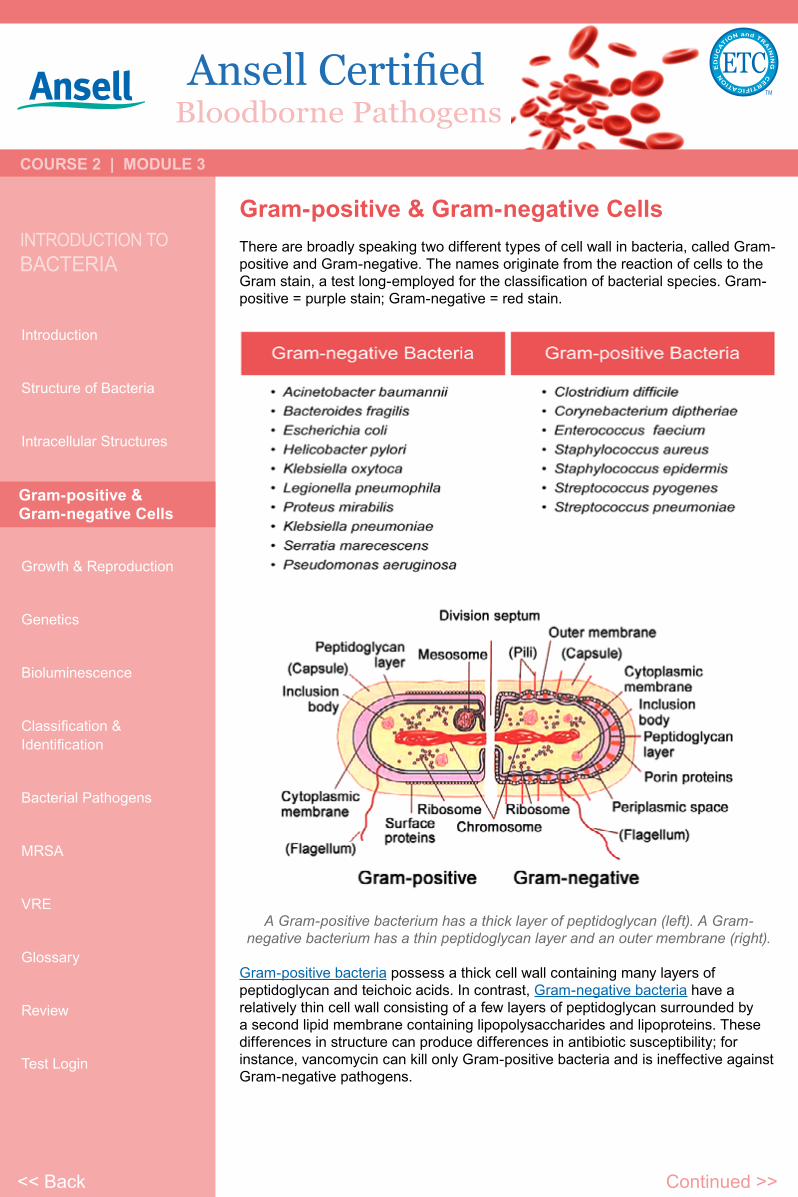
Gram-positive & Gram-negative CellsThere are broadly speaking two different types of cell wall in bacteria, called Gram-positive and Gram-negative. The names originate from the reaction of cells to the Gram stain, a test long-employed for the classification of bacterial species. Gram-positive = purple stain; Gram-negative = red stain.
A Gram-positive bacterium has a thick layer of peptidoglycan (left). A Gram-negative bacterium has a thin peptidoglycan layer and an outer membrane (right).
Gram-positive bacteria possess a thick cell wall containing many layers of peptidoglycan and teichoic acids. In contrast, Gram-negative bacteria have a relatively thin cell wall consisting of a few layers of peptidoglycan surrounded by a second lipid membrane containing lipopolysaccharides and lipoproteins. These differences in structure can produce differences in antibiotic susceptibility; for instance, vancomycin can kill only Gram-positive bacteria and is ineffective against Gram-negative pathogens.
Gram-positive & Gram-negative Cells
Continued >><< Back
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Gram-positive & Gram-negative Cells (continued)
In many bacteria an S-layer of rigidly arrayed protein molecules covers the outside of the cell. This layer provides chemical and physical protection for the cell surface and can act as a macromolecular diffusion barrier.
Flagella are rigid protein structures, about 20 nanometers (nm) in diameter and up to 20 micrometers (µm) in length that are used for motility. Flagella are driven by the energy released by the transfer of ions down an electrochemical gradient across the cell membrane.
Fimbriae are fine filaments of protein, just 2–10 nm in diameter and up to several micrometers in length. They are distributed over the surface of the cell, and resemble fine hairs when seen under the electron microscope. Fimbriae are believed to be involved in attachment to solid surfaces or to other cells and are essential for the virulence of some bacterial pathogens. Pili (sing. pilus) are cellular appendages, slightly larger than fimbriae that can transfer genetic material between bacterial cells in a process called conjugation.
Capsules or slime layers are produced by many bacteria to surround their cells, and vary in structural complexity: ranging from a disorganized slime layer of extra-cellular polymer, to a highly structured capsule. These structures can protect cells from engulfment by eukaryotic cells, such as macrophages. They can also act as antigens and be involved in cell recognition, as well as aiding attachment to surfaces and the formation of biofilms.
Endospores
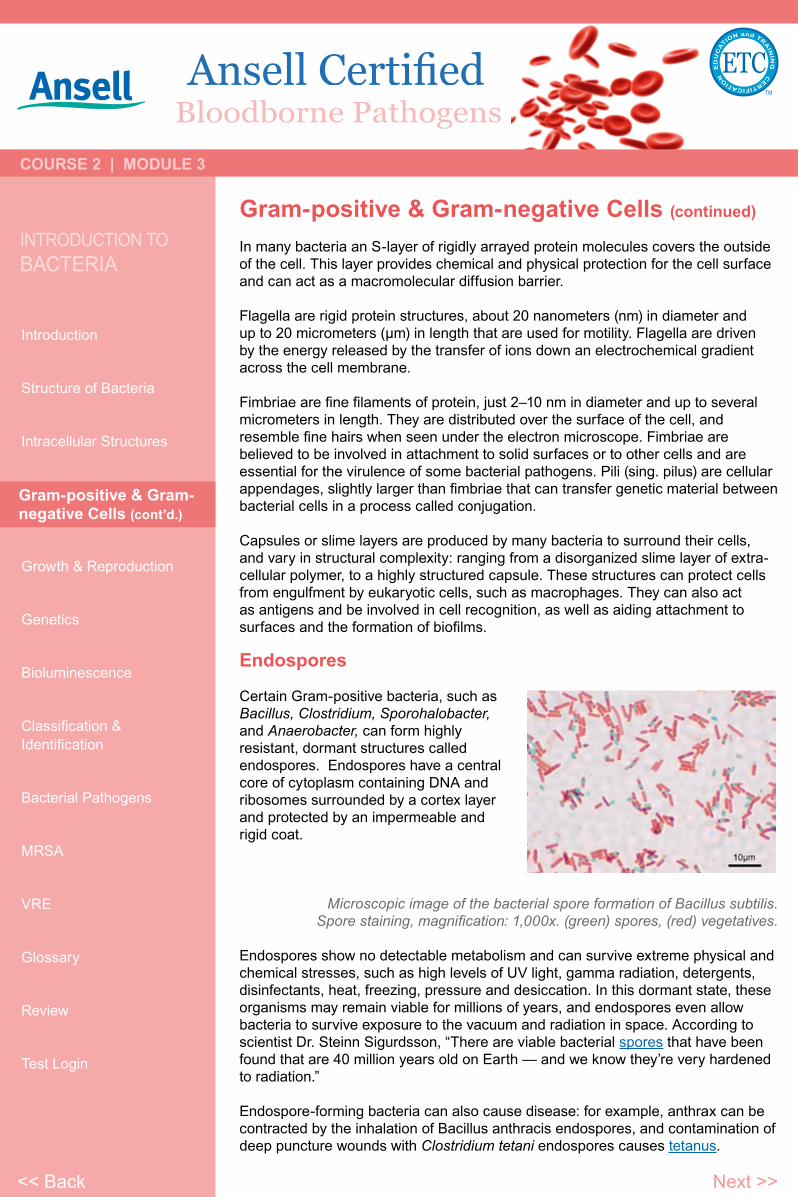
Certain Gram-positive bacteria, such as Bacillus, Clostridium, Sporohalobacter, and Anaerobacter, can form highly resistant, dormant structures called endospores. Endospores have a central core of cytoplasm containing DNA and ribosomes surrounded by a cortex layer and protected by an impermeable and rigid coat.
Microscopic image of the bacterial spore formation of Bacillus subtilis. Spore staining, magnification: 1,000x. (green) spores, (red) vegetatives.
Endospores show no detectable metabolism and can survive extreme physical and chemical stresses, such as high levels of UV light, gamma radiation, detergents, disinfectants, heat, freezing, pressure and desiccation. In this dormant state, these organisms may remain viable for millions of years, and endospores even allow bacteria to survive exposure to the vacuum and radiation in space. According to scientist Dr. Steinn Sigurdsson, “There are viable bacterial spores that have been found that are 40 million years old on Earth — and we know they’re very hardened to radiation.”
Endospore-forming bacteria can also cause disease: for example, anthrax can be contracted by the inhalation of Bacillus anthracis endospores, and contamination of deep puncture wounds with Clostridium tetani endospores causes tetanus.
Gram-positive & Gram-negative Cells (cont’d.)
<< Back Next >>
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Growth & ReproductionBacteria grow to a fixed size and then reproduce through binary fission, a form of asexual reproduction. Under optimal conditions, bacteria can grow and divide extremely rapidly, and bacterial populations can double as quickly as every 9.8 minutes. In cell division, two identical clone daughter cells are produced. Some bacteria, while still reproducing asexually, form more complex reproductive structures that help disperse the newly formed daughter cells.
In the laboratory, bacteria are usually grown using solid or liquid media. Solid growth media such as agar plates are used to isolate pure cultures of a bacterial strain. However, liquid growth media are used when measurement of growth or large volumes of cells are required.
Growth in stirred liquid media occurs as an even cell suspension, making the cultures easy to divide and transfer, although isolating single bacteria from liquid media is difficult. The use of selective media (with specific nutrients added or deficient or with antibiotics added) can help identify specific organisms.
Bacterial growth follows three phases:
• When a population of bacteria first enters a high-nutrient environment that allows growth, the cells need to adapt to their new environment. The first phase of growth is the lag phase, a period of slow growth when the cells are adapting to the high-nutrient environment and preparing for fast growth. The lag phase has high biosynthesis rates, as proteins necessary for rapid growth are produced.
• The second phase of growth is the logarithmic phase (log phase), also known as the exponential phase. The log phase is marked by rapid exponential growth. The rate at which cells grow during this phase is known as the growth rate, and the time it takes the cells to double is known as the generation time. During log phase, nutrients are metabolized at maximum speed until one of the nutrients is depleted and starts limiting growth.
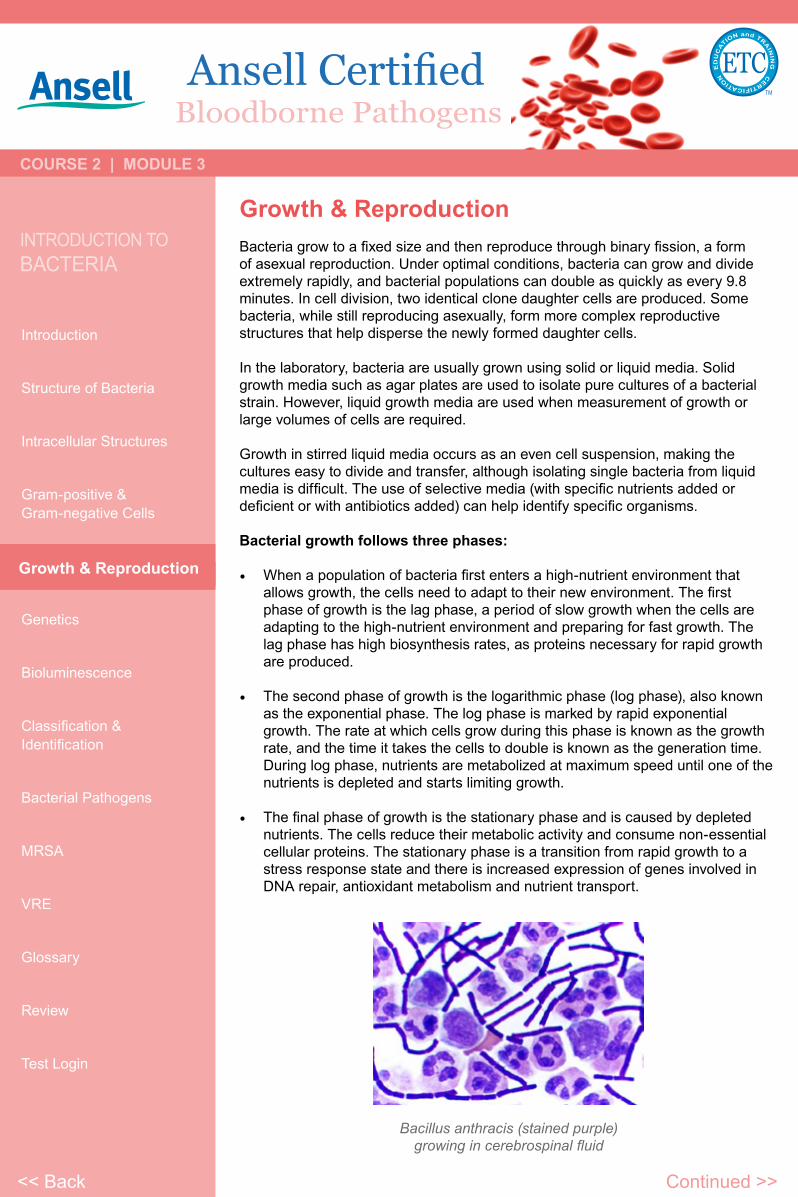
• The final phase of growth is the stationary phase and is caused by depleted nutrients. The cells reduce their metabolic activity and consume non-essential cellular proteins. The stationary phase is a transition from rapid growth to a stress response state and there is increased expression of genes involved in DNA repair, antioxidant metabolism and nutrient transport.
Continued >>
Bacillus anthracis (stained purple) growing in cerebrospinal fluid
<< Back
Growth & Reproduction
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Growth & Reproduction (continued)
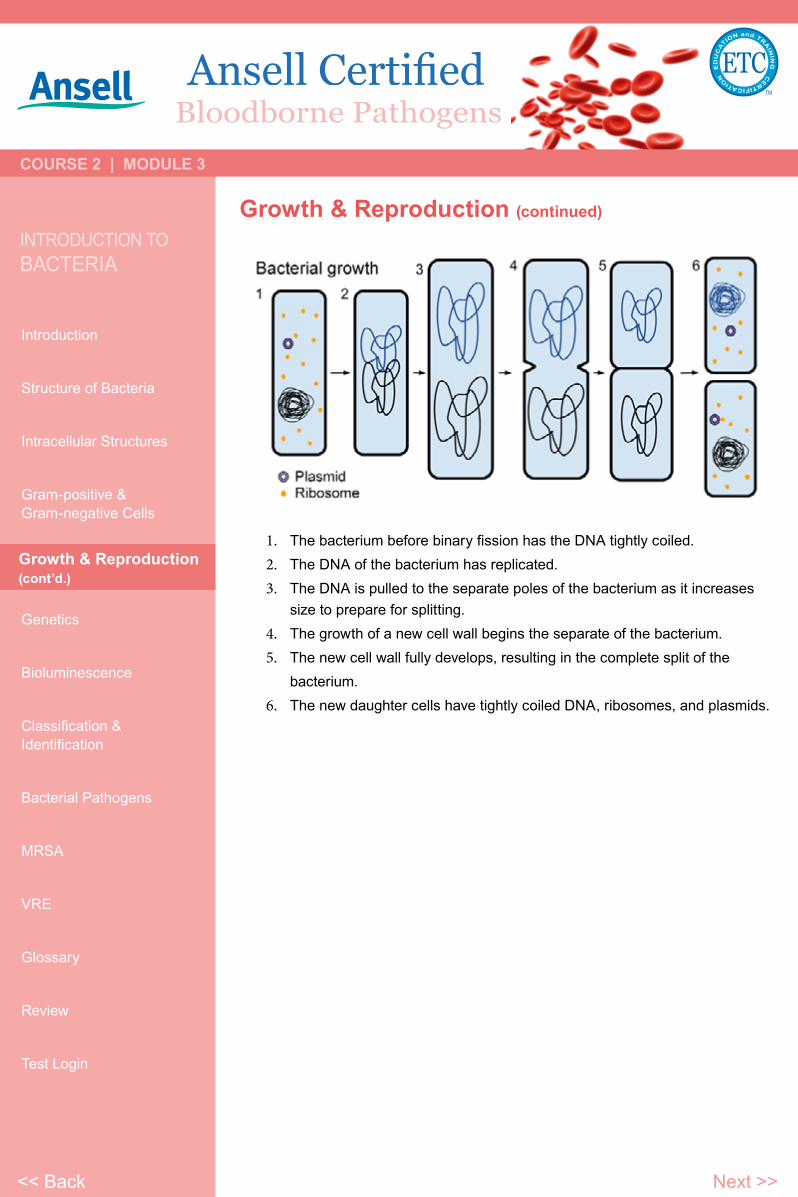
1. The bacterium before binary fission has the DNA tightly coiled.2. The DNA of the bacterium has replicated.3. The DNA is pulled to the separate poles of the bacterium as it increases
size to prepare for splitting.4. The growth of a new cell wall begins the separate of the bacterium.5. The new cell wall fully develops, resulting in the complete split of the
bacterium.6. The new daughter cells have tightly coiled DNA, ribosomes, and plasmids.
Growth & Reproduction(cont’d.)
<< Back Next >>
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
GeneticsMost bacteria have a single circular chromosomes. Bacteria may also contain plasmids, which are small extra-chromosomal DNAs that may contain genes for antibiotic resistance or virulence factors.
Bacteria, as asexual organisms, inherit identical copies of their parent’s genes (i.e., they are clonal). However, all bacteria can evolve by selection on changes to their genetic material DNA caused by genetic recombination or mutations. Mutations come from errors made during the replication of DNA or from exposure to mutagens. Mutation rates vary widely among different species of bacteria and even among different clones of a single species of bacteria. Genetic changes in bacterial genomes come from either random mutation during replication or “stress-directed mutation”, where genes involved in a particular growth-limiting process have an increased mutation rate.
Some bacteria also transfer genetic material between cells. This can occur in three main ways:
• First, bacteria can take up exogenous DNA from their environment, in a process called transformation.
• Genes can also be transferred by the process of transduction, when the integration of a bacteriophage introduces foreign DNA into the chromosome.
• The third method of gene transfer is bacterial conjugation, where DNA is transferred through direct cell contact. This gene acquisition from other bacteria or the environment is called horizontal gene transfer and may be common under natural conditions. Gene transfer is particularly important in antibiotic resistance as it allows the rapid transfer of resistance genes between different pathogens.
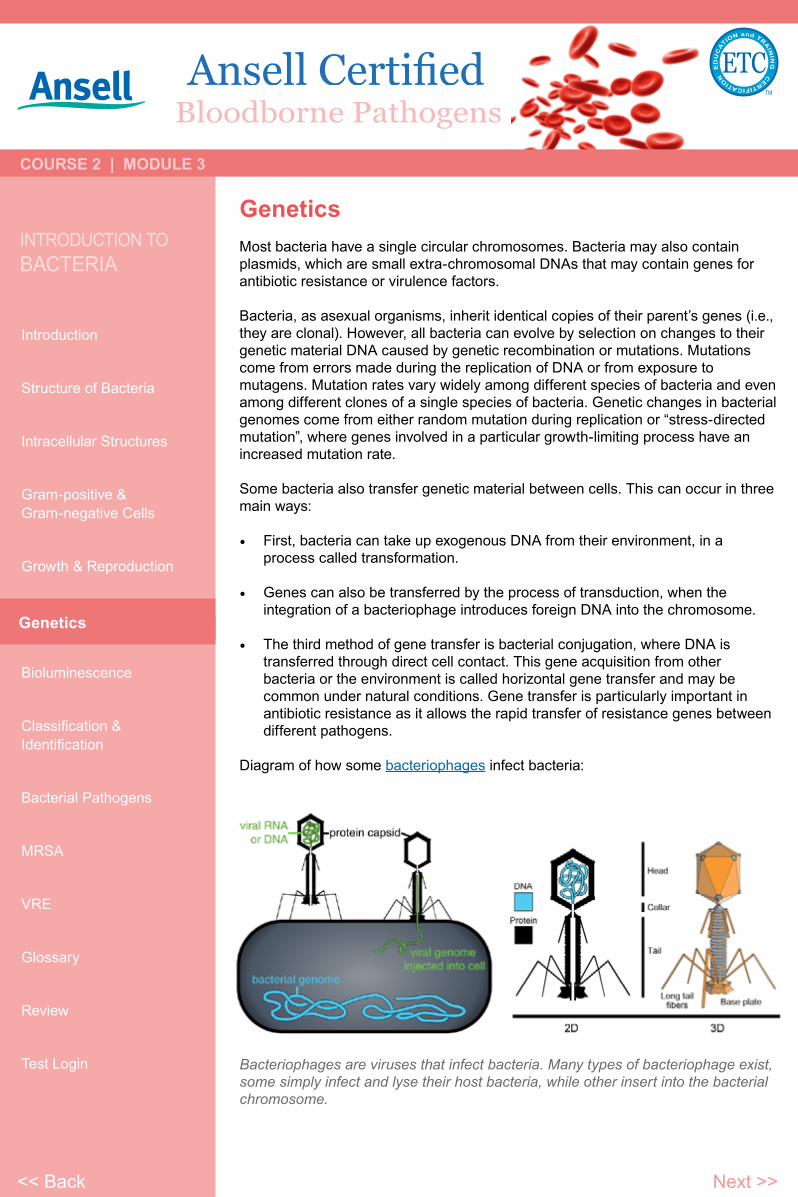
Diagram of how some bacteriophages infect bacteria:
Genetics
Bacteriophages are viruses that infect bacteria. Many types of bacteriophage exist, some simply infect and lyse their host bacteria, while other insert into the bacterial chromosome.
<< Back Next >>
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
BioluminescenceA few bacteria have chemical systems that generate light. This bioluminescence often occurs in bacteria that live in association with fish, and the light probably serves to attract fish or other large animals.
Multicellularity
Bacteria often function as multicellular aggregates known as biofilms, exchanging a variety of molecular signals for inter-cell communication, and engaging in coordinated multicellular behavior.
The communal benefits of multicellular cooperation include a cellular division of labor, accessing resources that cannot effectively be utilized by single cells, collectively defending against antagonists, and optimizing population survival by differentiating into distinct cell types. For example, bacteria in biofilms can have more than 500 times increased resistance to antibacterial agents than individual “planktonic” bacteria of the same species.
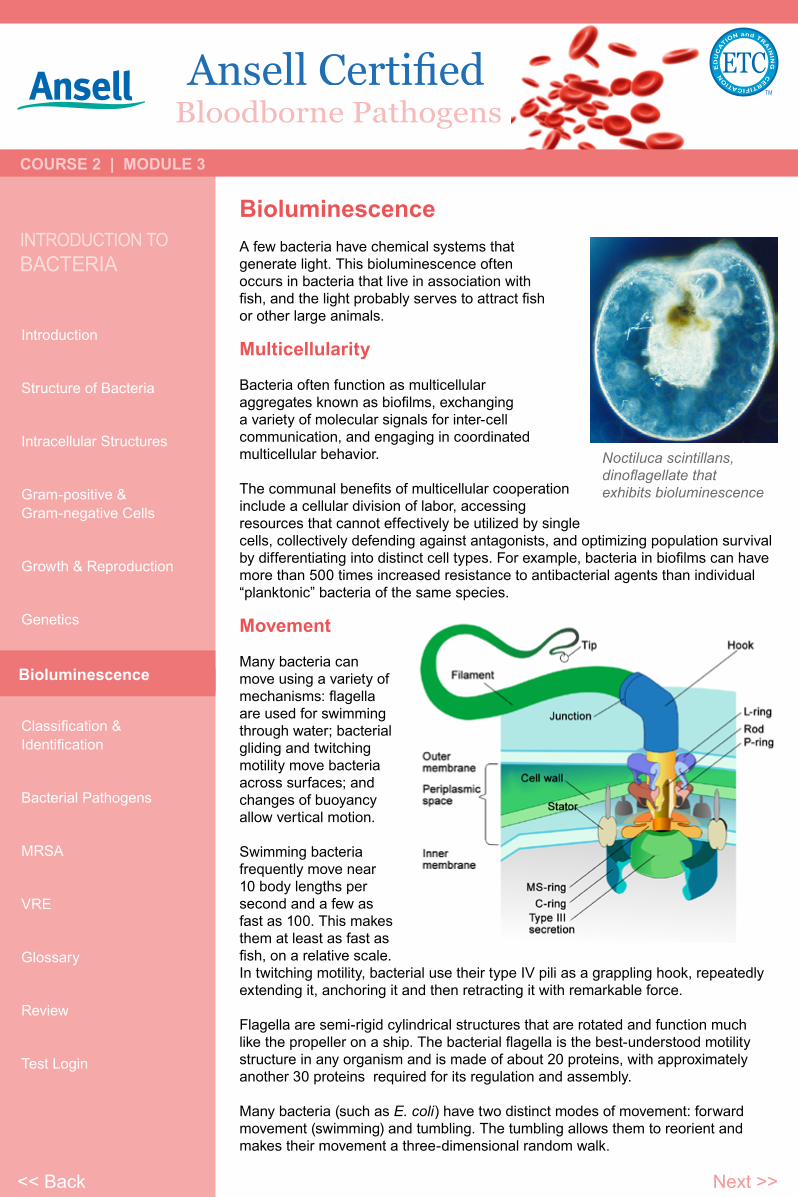
Movement
Many bacteria can move using a variety of mechanisms: flagella are used for swimming through water; bacterial gliding and twitching motility move bacteria across surfaces; and changes of buoyancy allow vertical motion.
Swimming bacteria frequently move near 10 body lengths per second and a few as fast as 100. This makes them at least as fast as fish, on a relative scale. In twitching motility, bacterial use their type IV pili as a grappling hook, repeatedly extending it, anchoring it and then retracting it with remarkable force.
Flagella are semi-rigid cylindrical structures that are rotated and function much like the propeller on a ship. The bacterial flagella is the best-understood motility structure in any organism and is made of about 20 proteins, with approximately another 30 proteins required for its regulation and assembly.
Many bacteria (such as E. coli) have two distinct modes of movement: forward movement (swimming) and tumbling. The tumbling allows them to reorient and makes their movement a three-dimensional random walk.
Bioluminescence
Noctiluca scintillans, dinoflagellate that exhibits bioluminescence
<< Back Next >>
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Classification & IdentificationIdentification of bacteria in the laboratory is particularly relevant in medicine, where the correct treatment is determined by the bacterial species causing an infection. Consequently, the need to identify human pathogens was a major impetus for the development of techniques to identify bacteria.
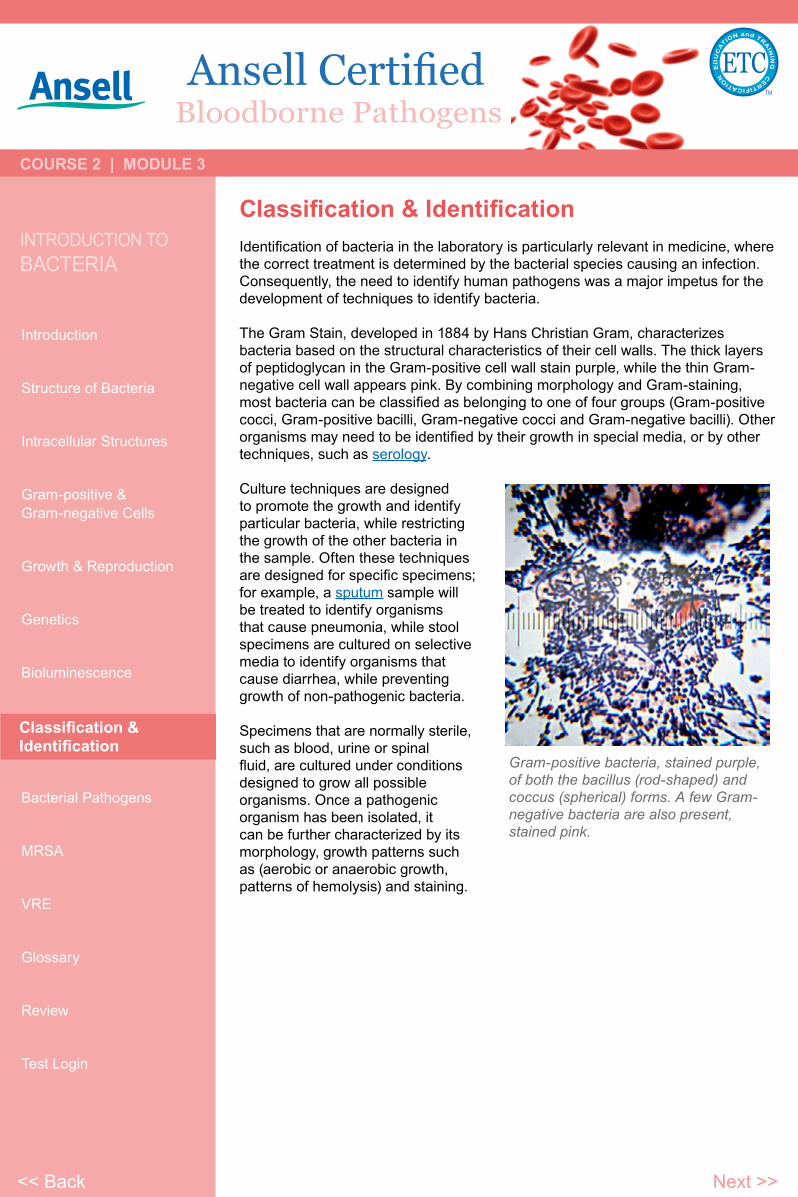
The Gram Stain, developed in 1884 by Hans Christian Gram, characterizes bacteria based on the structural characteristics of their cell walls. The thick layers of peptidoglycan in the Gram-positive cell wall stain purple, while the thin Gram-negative cell wall appears pink. By combining morphology and Gram-staining, most bacteria can be classified as belonging to one of four groups (Gram-positive cocci, Gram-positive bacilli, Gram-negative cocci and Gram-negative bacilli). Other organisms may need to be identified by their growth in special media, or by other techniques, such as serology.
Culture techniques are designed to promote the growth and identify particular bacteria, while restricting the growth of the other bacteria in the sample. Often these techniques are designed for specific specimens; for example, a sputum sample will be treated to identify organisms that cause pneumonia, while stool specimens are cultured on selective media to identify organisms that cause diarrhea, while preventing growth of non-pathogenic bacteria.
Specimens that are normally sterile, such as blood, urine or spinal fluid, are cultured under conditions designed to grow all possible organisms. Once a pathogenic organism has been isolated, it can be further characterized by its morphology, growth patterns such as (aerobic or anaerobic growth, patterns of hemolysis) and staining.
Classification & Identification
Gram-positive bacteria, stained purple, of both the bacillus (rod-shaped) and coccus (spherical) forms. A few Gram-negative bacteria are also present, stained pink.
<< Back Next >>
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Bacterial PathogensIf bacteria form a parasitic association with other organisms, they are classed as pathogens. Pathogenic bacteria are a major cause of human death and disease and cause infections such as tetanus, typhoid fever, diphtheria, syphilis, cholera, foodborne illness, leprosy and tuberculosis.
Each species of pathogen has a characteristic spectrum of interactions with its human hosts. Some organisms, such as Staphylococcus or Streptococcus, can cause skin infections, pneumonia, meningitis and even overwhelming sepsis, a systemic inflammatory response producing shock, massive vasodilation and death. Yet these organisms are also part of the normal human flora and usually exist on the skin or in the nose without causing any disease at all.
Other organisms invariably cause disease in humans, such as the Rickettsia, which are obligate intracellular parasites able to grow and reproduce only within the cells of other organisms. One species of Rickettsia causes typhus, while another causes Rocky Mountain spotted fever. Chlamydia, another phylum of obligate intracellular parasites, contains species that can cause pneumonia, or urinary tract infection and may be involved in coronary heart disease.
Finally, some species such as Pseudomonas aeruginosa, Burkholderia cenocepacia, and Mycobacterium avium are opportunistic pathogens and cause disease mainly in people suffering from immunosuppression or cystic fibrosis.
Bacterial Pathogens
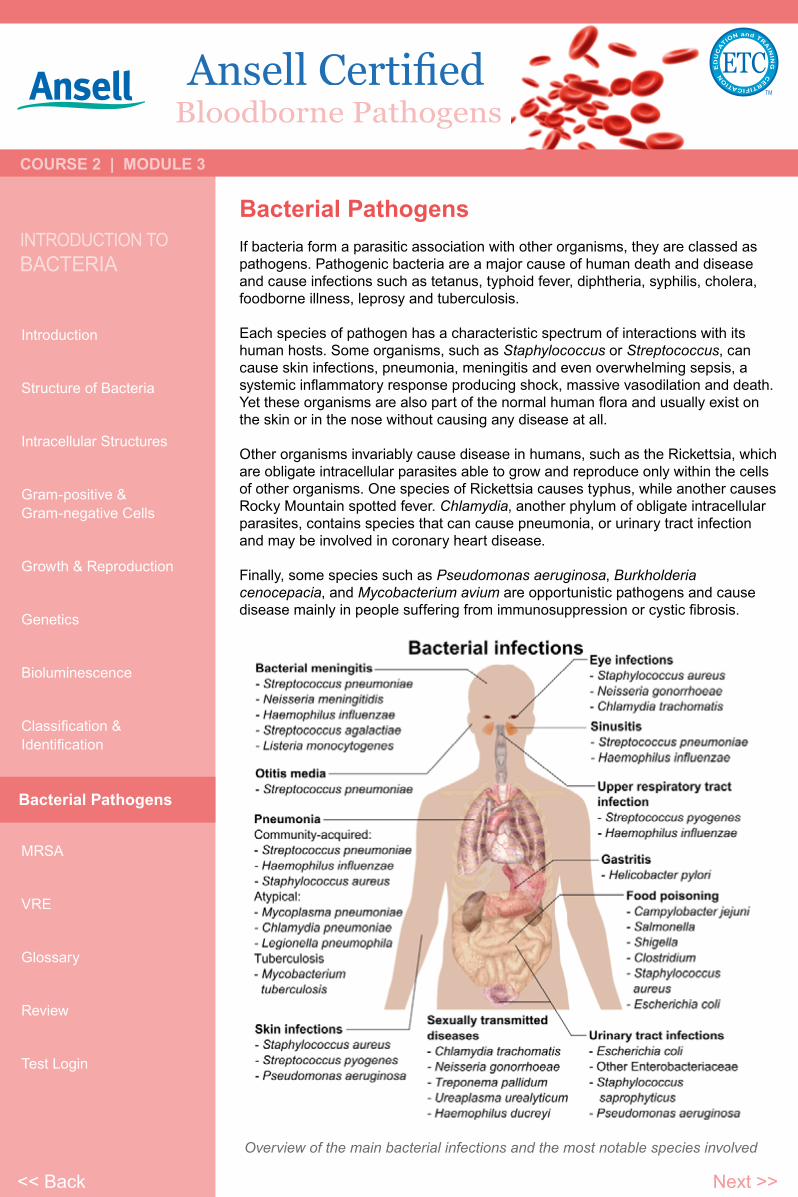
Overview of the main bacterial infections and the most notable species involved
<< Back Next >>

Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Major Pathogens of Concern to Healthcare ProvidersMethicillin-resistant Staphylococcus aureus (MRSA)
Methicillin-resistant Staphylococcus aureus, also called multidrug-resistant Staphylococcus aureus and oxacillin-resistant Staphylococcus aureus (ORSA), is a type of staph bacteria that is resistant to certain antibiotics called beta-lactams (β-lactam). These antibiotics include methicillin and other more common antibiotics such as oxacillin, penicillin, and amoxicillin. In the community, most MRSA infections are skin infections. More severe
or potentially life-threatening MRSA infections occur most frequently among patients in healthcare settings.
In 1959 methicillin was licensed in England to treat penicillin-resistant S. aureus infections. Just as bacterial evolution had allowed microbes to develop resistance to
penicillin, strains of S. aureus evolved to become resistant to methicillin. In 1961 the first MRSA isolates were reported in a British study, and between 1961 and 1967 there were infrequent hospital outbreaks in Western Europe and Australia. In 1974 2% of hospital-acquired S. aureus infections could be attributed to MRSA. The rate had increased to 22% by 1995, and by 1997 the percent of hospital S. aureus infections attributable to MRSA had reached 50%.
MRSA infections can occur in any geographic location and anywhere on a person’s body and can affect anyone. Historically, MRSA infections occurred in hospitalized patients, but now these infections are common in the community.
The biggest risk factor for MRSA infection is open or broken skin (such as a wound or surgical site); however, infections can occur even on areas of the skin where there is no obvious wound or break in the skin. Worldwide, an estimated 2 billion people are asymptomatic carriers of some form of S. aureus; of these, up to 53 million (2.7% of carriers) are thought to carry MRSA.
Healthcare SettingsPatients in healthcare facilities have weakened immune systems and undergo procedures (such as surgery) or have catheters inserted into the skin that make it easier for MRSA to get into the body. It is for this reason that healthcare personnel must follow infection control procedures (such as hand hygiene and proper catheter care) to prevent patients from acquiring MRSA infections. When patients get MRSA in healthcare facilities, the infections tend to be severe. Common infections include surgical wound infections, urinary tract infections, and the bloodstream.
Hands may become contaminated with MRSA by contact with:• colonized or infected patients;• colonized or infected body sites of the personnel themselves; or• devices, items, or environmental surfaces contaminated with body fluids
containing MRSA.
Appropriate hand hygiene such as washing with soap and water or using an alcohol-based hand rub can prevent the spread of MRSA.
Magnified 50,000x, this SEM scan depicts a grouping of methicillin-resistant Staphylococcus aureus (MRSA) bacteria.
MRSA
<< Back Continued >>
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Methicillin-resistant Staphylococcus aureus (continued)
Signs & Symptoms
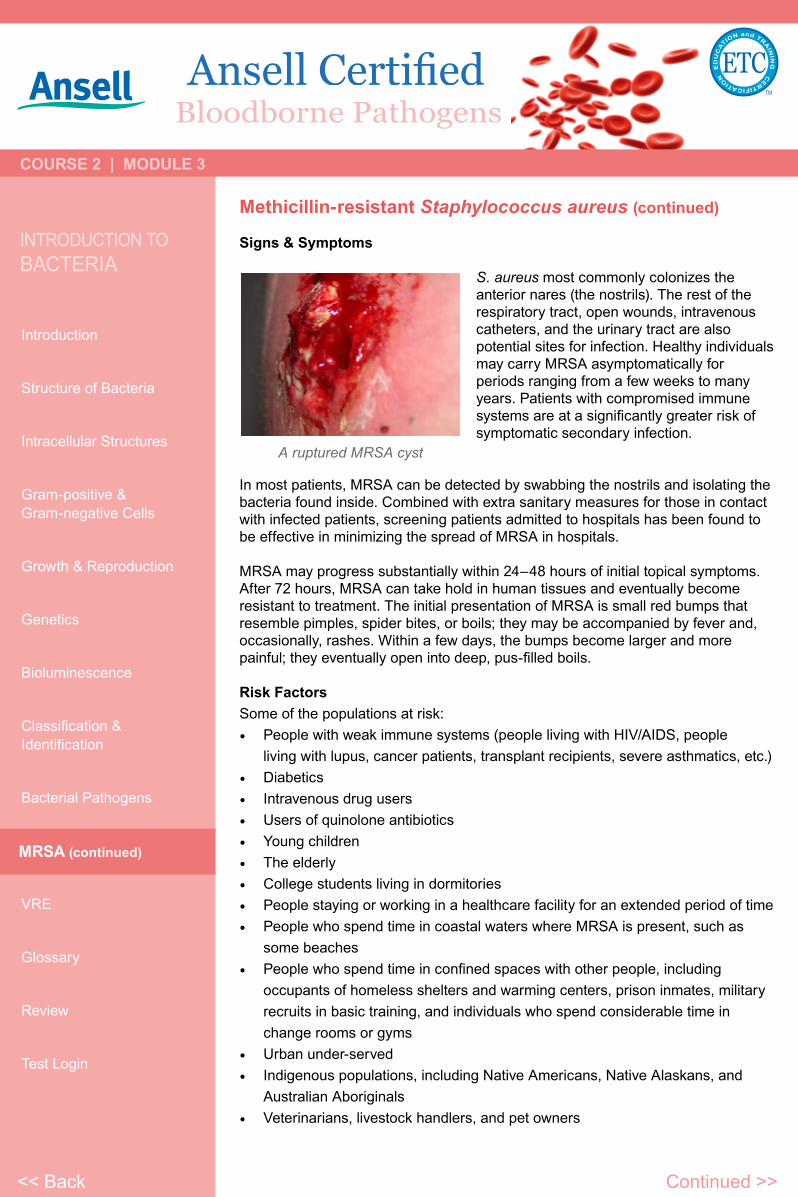
S. aureus most commonly colonizes the anterior nares (the nostrils). The rest of the respiratory tract, open wounds, intravenous catheters, and the urinary tract are also potential sites for infection. Healthy individuals may carry MRSA asymptomatically for periods ranging from a few weeks to many years. Patients with compromised immune systems are at a significantly greater risk of symptomatic secondary infection.
In most patients, MRSA can be detected by swabbing the nostrils and isolating the bacteria found inside. Combined with extra sanitary measures for those in contact with infected patients, screening patients admitted to hospitals has been found to be effective in minimizing the spread of MRSA in hospitals.
MRSA may progress substantially within 24–48 hours of initial topical symptoms. After 72 hours, MRSA can take hold in human tissues and eventually become resistant to treatment. The initial presentation of MRSA is small red bumps that resemble pimples, spider bites, or boils; they may be accompanied by fever and, occasionally, rashes. Within a few days, the bumps become larger and more painful; they eventually open into deep, pus-filled boils.
Risk FactorsSome of the populations at risk:• People with weak immune systems (people living with HIV/AIDS, people
living with lupus, cancer patients, transplant recipients, severe asthmatics, etc.)• Diabetics• Intravenous drug users• Users of quinolone antibiotics• Young children • The elderly• College students living in dormitories• People staying or working in a healthcare facility for an extended period of time • People who spend time in coastal waters where MRSA is present, such as
some beaches• People who spend time in confined spaces with other people, including
occupants of homeless shelters and warming centers, prison inmates, military recruits in basic training, and individuals who spend considerable time in change rooms or gyms
• Urban under-served• Indigenous populations, including Native Americans, Native Alaskans, and
Australian Aboriginals• Veterinarians, livestock handlers, and pet owners
MRSA (continued)
A ruptured MRSA cyst
<< Back Continued >>

Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Methicillin-resistant Staphylococcus aureus (continued)
DiagnosisDiagnostic microbiology laboratories and reference laboratories are key for identifying outbreaks of MRSA. New rapid techniques for the identification and characterization of MRSA have been developed. This notwithstanding, the bacterium generally must be cultured via blood, urine, sputum, or other body fluid cultures, and cultured in the lab in sufficient quantities to perform these confirmatory tests first.
Consequently, there is no quick and easy method to diagnose a MRSA infection. Therefore, initial treatment is often based upon ‘strong suspicion’ by the treating physician, since any delay in treating this type of infection can have fatal consequences.
GeneticsA defining characteristic of MRSA is its ability to thrive in the presence of penicillin-like antibiotics, which normally prevent bacterial growth by inhibiting synthesis of cell wall material. This is due to a resistance gene, mecA, which stops β-lactam antibiotics from inactivating the enzymes (transpeptidases) that are critical for cell wall synthesis.
PreventionTesting patients for MRSA upon admission, isolating MRSA-positive patients, decolonization of MRSA-positive patients, and terminal cleaning of patients’ rooms and all other clinical areas they occupy is the current best practice protocol for nosocomial MRSA.
Patient ScreeningPatient screening upon hospital admission, with nasal cultures, prevents the cohabitation of MRSA carriers with non-carriers, and exposure to infected surfaces. The test used (whether a rapid molecular method or traditional culture) is not as important as the implementation of active screening.
Surface sanitizingIn healthcare environments, MRSA can survive on surfaces and fabrics, including privacy curtains or garments worn by care providers. Complete surface sanitation is necessary to eliminate MRSA in areas where patients are recovering from invasive procedures.
Hand washingA June 2008 report centered on a survey by the Association for Professionals in Infection Control and Epidemiology concluded that poor hygiene habits remain the principal barrier to significant reductions in the spread of MRSA.
IsolationTo prevent the spread of staph or MRSA in the healthcare setting, employers should ensure the availability of adequate facilities so that patients with MRSA can be isolated to prevent the spread of this infection. Hand sanitizing and hand washing
can have a significant impact in reducing MRSA in the healthcare setting.
MRSA (continued)
<< Back Continued >>
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
MRSA (continued)
<< Back Continued >>
Methicillin-resistant Staphylococcus aureus (continued)
Restricting antibiotic useGlycopeptides, cephalosporins and in particular quinolones are associated with an increased risk of colonization of MRSA. Reducing use of antibiotic classes that promote MRSA colonization, especially fluoroquinolones, is recommended.
Decolonization / TreatmentCare should be taken when trying to drain boils, as disruption of surrounding tissue can lead to larger infections, or even infection of the blood stream (often with fatal consequences). All infectious lesions should be kept covered with a dressing. Mupirocin (Bactroban) 2% ointment can be effective at reducing the size of lesions. A secondary covering of clothing is preferred.
The nose is a common refuge for MRSA, and a test swab can be taken of the nose to indicate whether MRSA is present. If MRSA is detected via nasal culture, 2% ointment can be applied inside each nostril twice daily for 7 days, using a cotton-tipped swab.
Toilet seats are a common vector for infection, and wiping seats clean before and/or after use can help to prevent the spread of MRSA. Door handles, faucets, light switches, etc. can be disinfected regularly with disinfectant wipes. Spray disinfectants can be used on upholstery. Carpets and floors can be washed with disinfectant. Alcohol-based sanitizers can be placed near bedsides, near sitting areas, etc. to encourage their use.
Doctors may also prescribe antibiotics such as clindamycin, doxycycline or trimethoprim/ sulfamethoxazole.
Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Major Pathogens of Concern to Healthcare ProvidersVancomycin-resistant Enterococcus (VRE)
Vancomycin is a glycopeptide antibiotic used in treatment of infections caused by Gram-positive bacteria. Vancomycin was first isolated in 1953. The original indication for vancomycin was for the treatment of penicillin-resistant Staphylococcus aureus, a use kept alive for many years by the fact that compound had to be given intravenously and was thus not abused outside hospitals.
For many years since its initial use, vancomycin has traditionally been reserved as a drug of “last resort,” used only after treatment with other antibiotics had failed. Recently, however, vancomycin resistant organisms are becoming common. Thus, vancomycin is increasingly being displaced from this role by newer antibiotics.
Vancomycin-resistant Enterococcus, or vancomycin-resistant enterococci (VRE), are bacterial strains of the genus Enterococcus that are resistant to the antibiotic vancomycin. Enterococci are bacteria that are normally present in the human intestines and in the female genital tract and are often found in the environment. High-level vancomycin-resistant E. faecalis and E. faecium clinical isolates were first documented in Europe in the late 1980s. Since then, VRE have been associated with outbreaks of hospital-acquired (nosocomial) infections around the world.
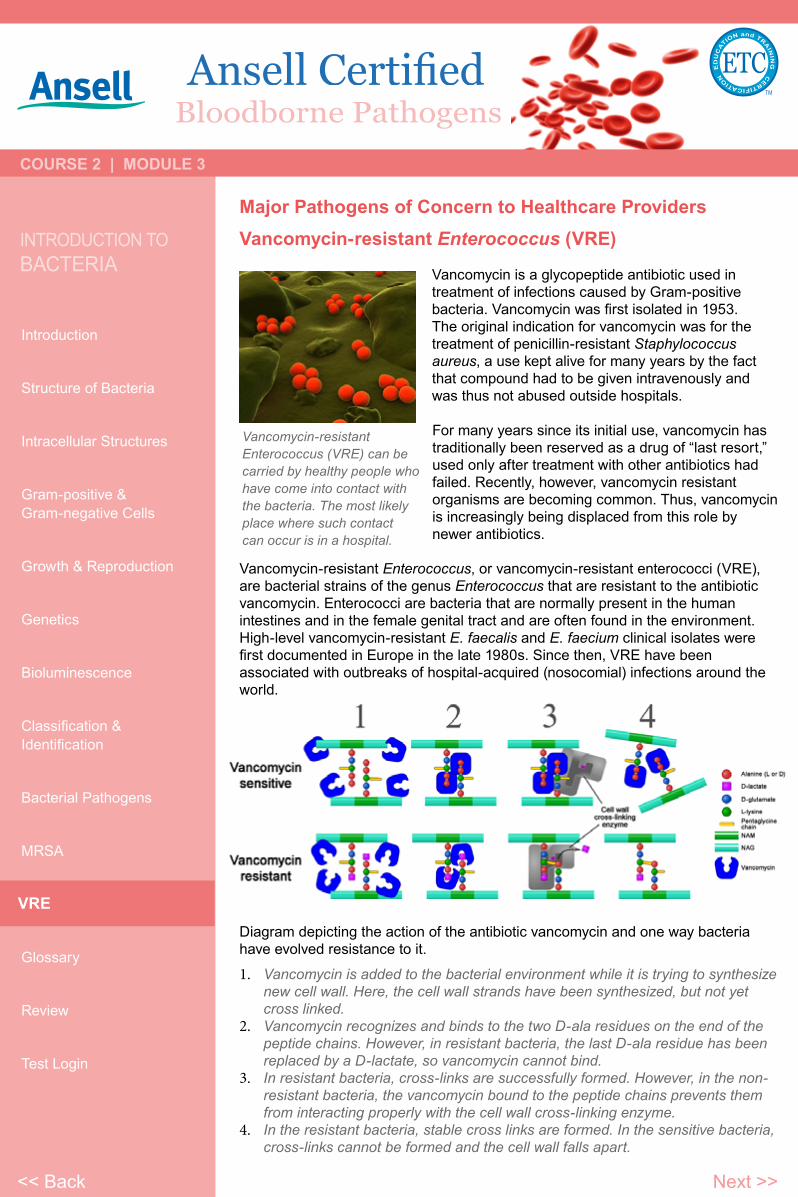
Diagram depicting the action of the antibiotic vancomycin and one way bacteria have evolved resistance to it.
1. Vancomycin is added to the bacterial environment while it is trying to synthesize new cell wall. Here, the cell wall strands have been synthesized, but not yet cross linked.
2. Vancomycin recognizes and binds to the two D-ala residues on the end of the peptide chains. However, in resistant bacteria, the last D-ala residue has been replaced by a D-lactate, so vancomycin cannot bind.
3. In resistant bacteria, cross-links are successfully formed. However, in the non-resistant bacteria, the vancomycin bound to the peptide chains prevents them from interacting properly with the cell wall cross-linking enzyme.
4. In the resistant bacteria, stable cross links are formed. In the sensitive bacteria, cross-links cannot be formed and the cell wall falls apart.
Vancomycin-resistant Enterococcus (VRE) can be carried by healthy people who have come into contact with the bacteria. The most likely place where such contact can occur is in a hospital.
VRE
<< Back Next >>

Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Vancomycin-resistant Enterococcus (VRE) (continued)
RiskThe following persons are at increased risk becoming infected with VRE:• People who have been previously treated with the antibiotic vancomycin or
other antibiotics for long periods of time. • People who are hospitalized, particularly when they receive antibiotic treatment
for long periods of time.• People with weakened immune systems such as patients in intensive care
units, or in cancer or transplant wards.• People who have undergone surgical procedures such as abdominal or chest
surgery.• People with medical devices that stay in for some time such as urinary
catheters or central intravenous (IV) catheters.• People who are colonized with VRE.
Treatment• People with colonized VRE (bacteria are present, but have no symptoms of an
infection) do not need treatment.• Most VRE infections can be treated with antibiotics other than vancomycin.• Laboratory testing of the VRE can determine which antibiotics will work.• For people who get VRE infections in their bladder and have urinary catheters,
removal of the catheter when it is no longer needed can also help get rid of the infection.
Spread• VRE is often passed from person to person by the contaminated hands of
caregivers.• VRE can get onto a caregiver’s hands after they have contact with other
people with VRE or after contact with contaminated surfaces.• VRE can also be spread directly to people after they touch surfaces that are
contaminated with VRE.• VRE is not spread through the air by coughing or sneezing.
Prevention• If a patient or someone in their household has VRE, the following are some
things they can do to prevent the spread of VRE:• Keep their hands clean. Always wash their hands thoroughly after using the
bathroom and before preparing food. Clean their hands after contact with persons who have VRE. Wash with soap and water (particularly when visibly soiled) or use alcohol-based hand rubs.
• Wear gloves if hands may come in contact with body fluids that may contain VRE, such as stool or bandages from infected wounds. Always wash their hands after removing gloves.
• If someone has VRE, be sure to tell healthcare providers so that they are aware of the infection. Healthcare facilities use special precautions to help prevent the spread of VRE to others.
VRE (continued)
<< Back Next >>

Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
GlossaryAnthrax (noun) \ an-thraks\An acute disease caused by the bacterium Bacillus anthracis. Most forms of the disease are lethal, and it affects both humans and animals. There are effective vaccines against anthrax, and some forms of the disease respond well to antibiotic treatment
Asymptomatic carrier (noun) \ ey-simp-tuh-mat-ik\ kar-ee-er\A person or other organism that has contracted an infectious disease, but who displays no symptoms; although unaffected by the disease themselves, carriers can transmit it to others; a number of animal species can act as a vector of human disease
Bacteriophage (noun) \ bak-teer-ee-uh-feyj\Also called phage or bacterial virus; any of a group of viruses that infect bacteria; phages are simple organisms that consist of a core of genetic material (nucleic acid) surrounded by a protein capsid. The nucleic acid may be either DNA or RNA and may be double-stranded or single-stranded.
Biofilm (noun) \ bahy-oh\ film\An aggregate of microorganisms in which cells adhere to each other on a surface
Colonized (verb) \ kol-uh-nahyz d\When a person carries the organism / bacteria but shows no clinical signs or symptoms of infection they are considered colonized; for Staph aureus, the most common body site colonized is the nose
Gram-negative bacteria (noun) \ gram\ neg-uh-tiv\ bak-teer-ee-uh\Bacteria that do not retain crystal violet dye in the Gram-staining protocol. In a Gram stain test, a counterstain (commonly safranin) is added after the crystal violet, coloring all Gram-negative bacteria with a red or pink color
Gram-positive bacteria (noun) \ gram\ poz-i-tiv/ bak-teer-ee-uh\Bacteria that are stained dark blue or violet by Gram staining
Human flora (noun) \ hyoo-muhn\ flawr-uh\The aggregate of microorganisms that reside on the surface and in deep layers of skin, in the saliva and oral mucosa, in the conjunctiva, and in the gastrointestinal tracts; they include bacteria, fungi and archaea
Serology (noun) \ si-rol-uh-jee\The scientific study of blood serum and other bodily fluids
Spore noun \ spor\A reproductive structure, some of which are adapted for dispersal and surviving for extended periods of time in unfavorable conditions
Sputum (noun) \ spyoo-tuh m\Mucus is coughed up from the lower airways
Tetanus (noun) \ tet-n-uh s\A medical condition characterized by a prolonged contraction of skeletal muscle fibers; the primary symptoms are caused by tetanospasmin, a neurotoxin produced by the Gram-positive, rod-shaped, obligate anaerobic bacterium Clostridium tetani
Glossary
<< Back Next >>Click on the glossary term to return.

Bloodborne Pathogens
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test Login
Review• Bacterial cells are typically 0.5–5.0 micrometers in length. Bacteria have a
wide range of shapes, ranging from spheres to rods and spirals. There are approximately 10x as many bacterial cells in the human flora as there are human cells, with large numbers of bacteria on the skin and as gut flora.
• The vast majority of the bacteria in the body are rendered harmless by the protective effects of the immune system. However, a few species of bacteria are pathogenic and cause infectious diseases.
• The bacterial cell is surrounded by a lipid membrane, or cell membrane, which encloses the contents of the cell and acts as a barrier to hold nutrients, proteins and other essential components of the cytoplasm within the cell.
• Bacteria often attach to surfaces and form dense aggregations called biofilms. These films can range from a few micrometers in thickness to up to half a meter in depth, and may contain multiple species of bacteria.
• There are two different types of cell wall in bacteria, called Gram-positive and Gram-negative. The names originate from the reaction of cells to the Gram stain, a test long-employed for the classification of bacterial species.
• Identification of bacteria in the laboratory is particularly relevant in medicine, where the correct treatment is determined by the bacterial species causing an infection. The thick layers of peptidoglycan in the Gram-positive cell wall stain purple, while the thin Gram-negative cell wall appears pink.
• The major bacterial pathogens of concern to healthcare providers are methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus, or vancomycin-resistant enterococci (VRE).
• MRSA is a type of staph bacteria that is resistant to certain antibiotics called beta-lactams. These antibiotics include methicillin and other more common antibiotics such as oxacillin, penicillin, and amoxicillin.
• Historically, MRSA infections occurred in hospitalized patients, but now these infections are common in the community. The biggest risk factor for MRSA infection is open or broken skin (such as a wound or surgical site); however, MRSA infections can occur even on areas of the skin where there is no obvious wound or break in the skin.
• Healthy individuals may carry MRSA asymptomatically for periods ranging from a few weeks to many years. Patients with compromised immune systems are at a significantly greater risk of infection.
• VRE are bacterial strains of the genus Enterococcus that are resistant to the antibiotic vancomycin. Enterococci are bacteria that are normally present in the human intestines and in the female genital tract and are often found in the environment.
• VRE is often passed from person to person by the contaminated hands of caregivers.
• VRE can get onto a caregiver’s hands after they have contact with other people with VRE or after contact with contaminated surfaces.
• VRE can also be spread directly to people after they touch surfaces that are contaminated with VRE.
• VRE is not spread through the air by coughing or sneezing.• People with colonized VRE (bacteria are present, but have no symptoms of
an infection) do not need treatment. Most VRE infections can be treated with antibiotics other than vancomycin. Laboratory testing of the VRE can determine which antibiotics will work.
Review
<< Back Next >>

Bloodborne Pathogens
® and ™ are trademarks owned by Ansell Limited or one of its affiliates. © 2013 Ansell Limited. All Rights Reserved.
COURSE 2 | MODULE 3
IntroductIon toBActErIA
Introduction
Structure of Bacteria
Intracellular Structures
Gram-positive &Gram-negative Cells
Growth & Reproduction
Genetics
Bioluminescence
Classification &Identification
Bacterial Pathogens
MRSA
VRE
Glossary
Review
Test LoginTEST Login
TestYou have completed the Introduction to Bacteria module of the Bloodborne Pathogens course.
Please login and complete the online test for Module 3 now.
LOGIN
<< Back