Embed Size (px)
Citation preview

Annual Impact ReportNovember 2016

Your support helps prompt the next era of innovation.
Your commitment empowers us all to imagine a world
free from cancer.
Alan Ashworth, PhD, FRS
President, UCSF Helen Diller Family Comprehensive Cancer Center
Senior Vice President for Cancer Services, UCSF Health
“”

Table of ContentsLetter from the President
Precision Cancer Medical Building
Molecular Oncology Initiative
Precise Imaging for Cancer & Therapy
The San Francisco Cancer Initiative
Center for BRCA Research
The Prostate Cancer Endowment
Investigational Trials Resource
The Cancer Immunotherapy Program
Impact Grant Awards
2
5
9
13
19
25
29
37
41
47
1

Dear Friends, The UCSF Helen Diller Family Comprehensive Cancer Center is more than a place where scientists
and clinicians strive to develop leading-edge therapeutics. In 2016, our brilliant researchers and
clinicians, patients and families, community groups, and government and industry partners continued
to work hand in hand to transform cancer into a manageable disease and cure it when possible. I’m
proud to share this year’s accomplishments, as well as our plans to build on these successes in the
years to come.
Our ambition is tangible, perhaps best represented by our UCSF Precision Cancer Medicine Building
(PCMB), due to open in 2019 on our Mission Bay campus. Located just steps from both our Helen
Diller Family Cancer Research Building and our UCSF Bakar Cancer Hospital, the PCMB is being
designed so that all patients have timely access to precise, coordinated, evidence-based care plans
that include everything from groundbreaking diagnostic tests and tumor sequencing to our extensive
portfolio of clinical trials and new therapies.
2

In addition to focusing on the PCMB, we participated in other exciting endeavors in 2016:
• Faculty members Mitchel Berger, MD, and Jeffrey Bluestone, PhD, were appointed to a Blue
Ribbon Panel as part of the Vice President of the United States’ National Cancer Moonshot
Initiative: http://tiny.ucsf.edu/ucsfblueribbonpanel. I also had the opportunity to offer input on this
initiative at a recent visit to the White House.
• Our growing Cancer Immunotherapy Program expands access to new therapies as we explore ways
to broaden their efficacy and reduce side effects. We are also one of six institutions comprising the
newly established Parker Institute for Cancer Immunotherapy, a collaborative effort that will accelerate
the development of breakthrough immune therapies capable of turning cancer into a curable disease:
http://tiny.ucsf.edu/ucsfparkerinstitute
• We’ve expanded our state-of-the-art cancer-imaging program, to more quickly assess disease
progression and treatment response, creating time to move patients to other therapies when
first-line therapies fail.
We’ve also launched the ambitious San Francisco Cancer Initiative, partnering with the City of San
Francisco, other health systems, community clinics, and a wide range of community groups on a
long-term effort to reduce cancer in San Francisco.
Your support helps prompt the next era of innovation. Your commitment empowers us all to imagine
a world free from cancer. I am deeply grateful for your participation as we work to find new ways to
diminish cancer, and to one day eradicate it altogether.
Sincerely,
Alan Ashworth, PhD, FRS President, UCSF Helen Diller Family Comprehensive Cancer Center Senior Vice President for Cancer Services, UCSF Health
3

To have one building house so many people dedicated to
impacting cancer on all fronts will be a huge advantage in
finding new treatments.
Eric Small, MD
Chief, Division of Hematology and Oncology
Deputy Director, Prostate Cancer Program
“”

Precision Cancer Medical Building When the UCSF Precision Cancer Medicine Building (PCMB) opens in early
2019, it will bring to fruition a facility in which all cancer patients can feel
confident that they are receiving the finest care in the world – a facility that
tailors care based on a detailed understanding of each individual’s biology and
life circumstances.
Just a few steps from the UCSF Helen Diller Family Cancer Research Building and UCSF Bakar
Cancer Hospital the PCMB’s six stories and 170,000 square feet will include 120 rooms for
multidisciplinary exams, procedures, and consultations. This will make it easier for UCSF cancer
patients to receive all of their care in one place, at one time. And with its location on UCSF’s
Mission Bay campus, the PCMB will facilitate ready collaboration among researchers, teaching
faculty, clinicians, patients, and families.
5

“To have one building house so many people dedicated to impacting cancer on all fronts will be a huge
advantage in finding new treatments,” says Eric Small, MD, chief of UCSF’s Division of Hematology
and Oncology and leader of the UCSF Helen Diller Family Comprehensive Cancer Center’s Prostate
Cancer Program. “Our plan is for the PCMB to be the epitome of integrated patient care.”
The building will encompass the latest technology, from advanced computational tools to lasers,
robotics, and advanced imaging, with room to grow built right into the design. The design will
empower UCSF to accelerate the discovery of new and more precise cancer treatments. Creating the
PCMB is especially urgent now because of recent game-changing advances in cancer treatment,
such as immunotherapy, enhanced imaging, and genetic counseling, which we intend to bring to all
of our patients.
By 2024, office visits related to cancer care in Northern California are projected to increase by 33
percent, so the PCMB will play a crucial role in guaranteeing patients timely access to these treatment
advances and in easing the emotional burden of dealing with a challenging disease.
Our plan is for the PCMB to be the epitome of
integrated patient care.
Eric Small, MD
Chief, Division of Hematology and Oncology
Deputy Director, Prostate Cancer Program
“ ”
6

“When the PCMB opens, the floor plans include space for genetic counselors on each and every
practice floor so we can truly integrate with our oncology practices,” says Amie Blanco, MS, LCGC,
acting director of the UCSF Cancer Genetics and Prevention Program. “Our aim is to provide genetic
counseling and testing on-site, the day a patient comes in.”
Building such a leading-edge, patient-centric medical facility is estimated to cost $250 million,
with the majority of funding coming from a combination of campus investment and philanthropic
contributions. Faculty members involved in planning the building’s multidisciplinary programming
believe investing in such a centralized facility will yield tremendous benefits for patients and
their health care teams.
“The PCMB will make things easier on multiple levels,” says Michael Korn, MD, leader of UCSF’s
Molecular Oncology Initiative. “But the most important thing is looking at it from the patient’s
perspective. Our goal is to make their health care delivery efficient and accessible. We are preparing
so when the PCMB’s doors open, we are ready to provide care as soon as the patient shows up.
That is the huge advantage of having everyone in one building and under one roof.”
When the UCSF Precision Cancer Medicine Building
(PCMB) opens in 2019, it will make real the vision for
a home in which all cancer patients can feel confident
that they are receiving the finest care in the world.
Patient-Centered Focus
• Timely access to the most precise treatments, including
cutting-edge diagnostic tests and therapies, as well as
our extensive and growing volume of clinical trials.
• Individualized, evidence-based care plans that a team of
carefully coordinated providers creates – and which guide
patients through their personal journeys of coping with cancer.
• All complex needs for physical and emotional healing
met in one place, in an environment marked by calm beauty
and the steady, humane hum of attentive expertise.
UCSF RON CONWAY FAMILY GATEWAY
MEDICAL BUILDINGThe PCMB’s six stories and
170,000 square feet will create 120
rooms for multidisciplinary exams,
procedures, and consultations that
will make it much easier for UCSF
outpatients to receive their cancer
care in one place, at one time.
UCSF BENIOFF CHILDREN’S
HOSPITALUCSF BETTY IRENE MOORE
WOMEN’S HOSPITAL AND UCSF BAKAR CANCER HOSPITAL
2017SPRING:Commence Construction
2016SUMMER:Begin Design Process
2019SPRING:Open to Patients
4th St.16 th St.
Future Entrance
UCSF PRECISION CANCER MEDICINE
BUILDING
Timeline
UCSF Mission Bay Precision Cancer Medicine Building
Moving Beyond the Standard of Care
7

Our mission is to use the combined experience and
intelligence of many people across UCSF to turn
genomic findings into clinical recommendations for
individual patients.
Michael Korn, MD
“”

Molecular Oncology Initiative In January 2016, UCSF launched the Molecular Oncology Initiative (MOI) to
integrate molecular information found in most cancer types with the ever-
increasing number of therapeutics being developed in translational research and
clinical practice. The UCSF Molecular Tumor Board (MTB), a group of experts
that reviews molecular findings, was formed to interpret findings from the UCSF
500 gene panel assay, a pioneering sequencing test developed at UCSF to find
mutations in a patient’s cancer that particular medicines can attack.
9

“Right now, there are only a few genes where … we’ve found a predictable change in the gene and
can recommend treatment without hesitation,” explains Korn, who’s also chair of the MTB. “That’s
why the tumor board is there – to tackle this big gray zone in gene behavior and help physicians make
correct diagnoses for their patients and deliver appropriate treatment.
“The MTB reviews findings obtained by the UCSF 500 gene panel assay,” he continues. “Our mission
is to use the combined experience and intelligence of many people across UCSF to turn genomic
findings into clinical recommendations for individual patients.”
The MTB takes advantage of its close collaboration with the UCSF Clinical Cancer Genomics
Laboratory (CCGL), led by Boris Bastian, MD. Bastian’s laboratory provides the UCSF gene panel
assay, which tests tumor DNA and the patient’s germline (inherited) DNA, which many commercial
products do not test. The test can also provide information on inherited genetic changes that increase
an individual’s risk of developing cancer.
These findings benefitted not only the
affected patients but also their entire
families. This shows we are on a
very promising path that will greatly
influence how we diagnose and treat
cancer here.
Michael Korn, MD
“
”
10

Since the inception of the MOI and MTB, more than 190 patient cases have been reviewed by the
board. The UCSF 500 gene panel assay has also led to dramatic responses for some patients as a
result of treatments tailored to their diseases’ molecular profiles. After their cases were reviewed by
the MTB, their test results provided the rationale for enrolling them in clinical trials at UCSF.
“We were able to detect mutations in several individual patient germlines,” says Korn. “These
findings benefitted not only the affected patients but also their entire families. This shows we are on
a very promising path that will greatly influence how we diagnose and treat cancer here.”
11

Our imaging methods can help us determine at an early
stage whether treatments are having an impact, and if they
are not, we can to try alternative approaches in a more
timely manner than might have been possible in the past.
Sarah Nelson, PhD
Margaret Hart Surbeck Distinguished Professor of Advanced Imaging
Director, Surbeck Laboratory for Advanced Imaging
Leader, Precise Imaging for Cancer and Therapy
“”

Precise Imaging for Cancer and Therapy (PICT) Imaging has been an integral component of the breast, prostate, and brain
cancer programs for many years. By expanding the focus to include other
cancers and forging a stronger relationship with clinicians and scientists in
the Department of Radiology and Biomedical Imaging, the UCSF Helen Diller
Family Comprehensive Cancer Center has created opportunities to dramatically
increase avenues for collaborative research and enhance patient care.
“PICT enables us to take maximum advantage not only of our sophisticated imaging equipment
but also our expertise in developing new technologies and methodologies to improve diagnosis
and treatment monitoring,” says Sarah Nelson, PhD, the Margaret Hart Surbeck Distinguished
Professor of Advanced Imaging, director of the Surbeck Laboratory for Advanced Imaging, and
leader of PICT.
13

Imaging crucial for advanced therapies,
adaptive trials, research
The expanded role for imaging is tied to advances that allow it to support and refine a range of
precision cancer medicine approaches.
“Our imaging methods can help us determine at an early stage whether treatments are having an
impact, and if they are not, we can try alternative approaches in a more timely manner than might
have been possible in the past,” says Nelson. This is especially important for the way an increasing
number of clinical trials are designed to be adaptive: They use early clinical findings to reject ineffective
strategies and focus on the most promising options. With that in mind, says Nelson, “The more light
we can shed on what’s going on in the tumor, the better.”
Advances in imaging technology also are essential for complementing and enhancing information
supplied by genomic analyses. “We are finding that you need both approaches,” Nelson says.
“Detailed spatial information can direct you to sample tissue from the areas that are most malignant.
In heterogeneous tumors, that’s important because you are more likely to identify mutations that
define how the tumor is going to behave. That’s why image-guided biopsies are so important for
making an accurate diagnosis.”
We can help researchers answer
questions about the underlying
biology of a particular type of cancer
and help them design new treatments
that attack new targets.
Sarah Nelson, PhD
“”
14

The combination of advanced imaging equipment and sophisticated methods for quantitative
analysis allows researchers to more accurately describe the status of the tumor and detect changes
that would otherwise have been considered too small to act upon.
“These new methods offer more objective and precise measures of the tumor and its
microenvironment,” Nelson says. “The vascular density, the number of cells in a region, the
metabolic processes, and the mutations at work all play a role in determining which therapy might
work best.”
She adds that imaging also helps in planning and directing more focal treatments, such as radiation
therapy, focused ultrasound, and convection-enhanced delivery of chemotherapeutic agents. All of
these elements provide oncologists with new information that they can use to offer more informed
choices to their patients. This is especially valuable at a place like the HDFCCC, which is designed
to offer patients the benefits of integrating the latest knowledge from researchers and clinicians
across many disciplines.
The integration plays out in multiple ways. Not only does imaging play a role in the clinical setting,
it also is increasingly important in preclinical studies aimed at defining cancer mechanisms and
understanding how new therapeutic approaches might affect specific metabolic or molecular
pathways.
“We can help researchers answer questions about the underlying biology of a particular type of
cancer and help them design new treatments that attack new targets,” Nelson says.
15

A two-way research street
Nelson and her colleagues are also responsible for research on the imaging modalities themselves.
PICT is pushing the envelope on the use of a number of technologies and methodologies, including,
for example, metabolic imaging methods using hyperpolarized [1-13C] pyruvate to help distinguish
between benign and malignant tissue and to more confidently predict outcomes.
“The translation of this technology from preclinical systems to cancer patients has been championed
here at UCSF, and we are just beginning to define how to best make use of the information that it
provides,” Nelson says.
This work is aided by the fact that much of the state-of-the-art equipment and expertise resides
side by side in the clinical facilities at Mission Bay. This can enable radiologists to take advantage
of experimental techniques to enhance standard imaging exams. They are also available to support
16

promising new treatments such as immunotherapy, which can cause changes on standard images that
mimic tumor progression and may give a false picture of the long-term impact upon the cancer.
It’s a two-way street for mutual benefit. A clinical trials unit might contact the imaging group requesting
help to support the evaluation of a new treatment. Alternatively, imaging team members might develop
a methodology they believe reveals something new and important and then identify a population of
patients to determine whether the methodology is valid and can improve clinical outcomes.
Such work is essential because without validation, insurance companies are not likely to reimburse
providers for using these new techniques. Nelson believes that if PICT can zero in on the most effective
technologies – those that prevent unnecessary treatments and make new therapies more effective or
efficient – they can save money, as well as a substantial number of lives. “What we are doing here is
showing how these advances can have real benefits for real patients,” she says.
What we are doing here is showing
how these advances can have real
benefits for real patients.
Sarah Nelson, PhD
“”
17

The real tragedy is that up to half of cancers could be
avoided if what we currently know about the causes and
their prevention could be put into practice widely.
Robert Hiatt, MD, PhD
Associate Director, Population Sciences,
UCSF Helen Diller Family Comprehensive Cancer Center
“”

The San Francisco Cancer InitiativeDespite many remarkable clinical advances, cancer now kills more San Francisco
residents than any other cause, according to the California Department of
Public Health’s County Health Status Profiles 2016. There are thousands of new
cancer cases and more than a thousand deaths each year from the disease.
San Francisco’s cancers often disproportionately strike and kill people of color
and those most disadvantaged in society. They also cost San Francisco patients,
families, and taxpayers hundreds of millions of dollars each year.
“The real opportunity is that up to half of cancers could be avoided if what we currently know about
the causes and their prevention could be put into practice widely,” says Robert Hiatt, MD, PhD, the
Helen Diller Family Comprehensive Cancer Center’s associate director of population sciences. “The
San Francisco Cancer Initiative (SF CAN) aims to put what we know into practice to dramatically
reduce the incidence and impact of cancer across this city.”
SF CAN already has begun implementing a systematic and coordinated approach to improving
cancer prevention and screening in San Francisco that relies on forging partnerships between
UCSF and the city’s health systems, government, and community leaders. The San Francisco
Department of Public Health (SFDPH) recently joined the effort, as have many others, including
the San Francisco Medical Society, the American Cancer Society, community clinics, community
groups, and other health systems.
19

Initial focus: Leverage advances for largest
possible impact
The last few years have seen remarkable advances in precision population health, data and information
technology, and cancer treatments. In addition, San Francisco’s exceptional diversity, reasonable size
with approximately 850,000 residents, and forward-looking leadership make it a prime location for this
pioneering effort. “Our collective experience and existing working relationships create a potent catalyst
for change,” Hiatt says.
Spearheaded by Alan Ashworth, Helen Diller Family Comprehensive Cancer Center president, SF CAN is
expected to launch officially later this year with an intensive focus on five cancer types – breast, colorectal,
liver, prostate, and lung and other tobacco-induced cancers – chosen because they represent nearly half
of the city’s cancer cases or have large disparities in onset and outcomes. For each of these cancer types,
promising, evidence-based prevention and screening practices exist that can lead to fewer deaths but
which are not yet being fully implemented across all population groups in San Francisco.
Getting a jump start
Task forces are already forming for each of the five cancers. “There is leadership from community
advisors and the SFDPH, while the HDFCCC forms the organizational backbone and lends crucial
scientific expertise,” Hiatt says. “Our strategy of collective impact – drawing on the commitment and
integration of people who represent different groups – is the only way to make headway on something
so complex, and it’s what makes this effort so unique.”
Our collective experience and
existing working relationships
create a potent catalyst for change.
Robert Hiatt, MD, PhD
“”
20

Here are a few examples of work already being done by the task forces:
Joseph Guydish, PhD, MPH, is encouraged by the work already in progress for lung and other tobacco-
induced cancers. Leveraging numerous existing partnerships, this team has split into three distinct
threads, all focused on groups that are especially vulnerable to tobacco-induced cancers.
Guydish, Maya Vijayaraghavan, MD, MAS, and Dorie Apollonio, MPP, PhD, are working on reducing
smoking among low-income populations, including the homeless and persons enrolled in drug-
abuse treatment. “Smoking prevalence for those in low-income, safety-net services is two to three
times that in the general population,” Guydish says. To date, UCSF and its partners are doing needs
assessments and exploring methodologies that have worked well in other settings as well as creating
new interventions.
In the second thread, Pamela Ling, MD, MPH – who studies the social and cultural issues that drive
smoking – and Danielle Ramo-Larios, PhD, are working with internet and public radio station Youth
Radio to try to reduce smoking in the so-called “hipster” community: mostly young adults who
congregate in bars and tend to smoke at higher rates than the general population.
Valerie Yerger, ND, leads the third thread, which focuses on reducing smoking in San Francisco’s
African-American community. Studies show that African-Americans smoke at lower rates than the
general population does but have higher rates of lung cancer. Some research has indicated that menthol
cigarettes, which tobacco companies push hard in the African-American community, may be the culprit.
Yerger is working with the city and with the African-American Health Disparity Project to see if there’s
a way to ban menthol cigarettes in San Francisco. Local initiatives have been successful drivers for
policies like smoke-free bars, restaurants, and offices, and Yerger hopes to follow that pattern.
”
21

The colorectal cancer task force began by focusing on increasing screening in the city’s safety-net
populations through the use of inexpensive, evidence-based fecal immunochemical tests. “In San
Francisco, screening rates in privately insured populations are already quite high, but for the city’s
vulnerable and underinsured patient populations, this is often not the case,” says the HDFCCC’s
Michael Potter, MD, a family physician and researcher in the Department of Family and Community
Medicine. “Increasing screening rates in these groups is our most potent opportunity to reduce
colorectal cancer incidence and mortality in the city.”
The task force, which includes stakeholders from the San Francisco Community Clinic Consortium,
Zuckerberg San Francisco General (ZSFG), San Francisco Health Plan, and the American Cancer
Society, plans to increase access to screening within community clinics that serve the largest pockets
of unscreened adults between the ages of 50 and 75.
They’re beginning with a needs assessment to gather detailed information about current screening
rates and practices in the community health centers. “We expect to identify several opportunities
to implement tailored, evidence-based approaches to individual sites. These might include staff
training, improved patient-education materials, streamlined processes for outreach and follow-up, and
incentives for clinical teams to achieve certain targets,” says Potter, who also expects the task force
can help develop more efficient processes for directing high-risk patients to ZSFG for colonoscopy.
The liver cancer task force has forged partnerships with the SFDPH, community organizations,
and clinical providers from multiple health systems, with an initial focus on screening and treatment
for hepatitis B and hepatitis C, both of which significantly increase the risk of liver cancer. The
diseases affect a broad swath of the population, but liver cancer rates in Asian and Asian-American
communities are particularly high, and they are increasing rapidly in African-American, Latino, and
other underserved populations.
Tung Nguyen, MD, with a patient.
22

For hepatitis B, the group has instituted a phone navigation line where people can have questions
answered about testing, results, and follow-up care in English and Chinese. For hepatitis C, the
group worked with the SFDPH to launch an “End Hepatitis C” campaign in July 2016 to raise public
awareness. “We want to get people screened but also make sure people who have hepatitis C get
appropriate referrals and treatment, because it can be cured,” says the HDFCCC’s Tung Nguyen, MD,
the Stephen J. McPhee, MD, Endowed Chair in General Internal Medicine.
The task force is also:
• Working with the city to expand ZSFG’s capacity to do liver ultrasounds to catch the disease
earlier, which increases the chances for effective treatment.
• Initiating steps to create a referral network that will enable more people – and more diverse
populations – to access available clinical trials for liver cancer.
• Creating a policy paper on ways to make treatment for hepatitis C more affordable, because
existing treatments, while curative, are quite expensive.
Hiatt says the task forces are doing the crucial, frontline work to implement the SF CAN vision.
“SF CAN’s broad focus on the entire life course is a unique and novel approach to cancer control,”
he says. “We are bringing new knowledge about the origins of cancer to what we know about effective
prevention and early detection to make a difference at the population level. If we can make our impact
on the cancer burden a success, our model could spread through the entire Bay Area – and maybe
even California and the rest of the United States.”
SF CAN’s broad focus on the entire
life course is a unique and novel
approach to cancer control.
Robert Hiatt, MD, PhD
“”
23

We’ve received an overwhelmingly positive response
from BRCA-positive patients. We’re planning to continue
growing and refining our services and adding staff as our
patient population expands.
Pagan Morris, MPH
Program Manager, Center for BRCA Research at UCSF
“”

Center for BRCA Research Opened in 2015, the Center for BRCA Research at UCSF is only the second
comprehensive clinic in the nation – and the first on the West Coast – for
individuals carrying hereditary gene mutations in BRCA1 or BRCA2. These
mutations are widely recognized as inheritable causes of breast and ovarian
cancers, but less well known is that they also heighten the risk of pancreas and
prostate cancers, as well as melanoma.
The center at UCSF is one of the few to focus clinical and research activities directly on BRCA
mutations, concentrating on clinical care, screening and prevention (including a laboratory
science program), and education and outreach. The Hereditary Cancer Clinic within the center
has the capacity to treat 150 patients and conduct up to 100 genetic counseling sessions
each month.
25

“We’ve received an overwhelmingly positive response from BRCA-positive patients,” says Pagan
Morris, MPH, the center’s program manager. “We’re planning to continue growing and refining our
services and adding staff as our patient population expands.”
The Center for BRCA Research is powered by the labs of Drs. Alan Ashworth and Pamela Munster.
They are conducting studies to screen for risk-modifying biomarkers that can identify carriers at high
risk of developing cancer and with the most potential for responsiveness to therapy. Findings from
these studies will aid in further developing clinical guidelines for prevention and management, as well
as identifying genetic and other factors that modify risk for BRCA-related cancer in families.
On the education front, the center recently awarded the first hematology-oncology clinical research
fellowship and developed the UCSF BRCA Challenge Grant, designed to launch one research project
We plan to continue our work in each
of the center’s core areas of focus, from
growing our laboratory program
and the Clinical Fellow Program
to increasing the number of BRCA
Challenge grants, in order to train
future leaders in the field.
Alan Ashworth, PhD, FRS
“
”Alan Ashworth, PhD, FRS
26

a year focused on top priorities identified by the center’s steering committee. All of this is intended
to support and train postdoctoral and senior researchers to pursue the most promising BRCA
research projects.
The BRCA Center is also working with community partners to develop and launch a regional public
awareness plan. It has partnered with KinTalk.org, an educational and family communication portal
where at-risk family members can securely share important hereditary genetic health information. The
center has received national attention from The Wall Street Journal and NBC News.
“We plan to continue our work in each of the center’s core areas of focus, from growing our laboratory
program and the Clinical Fellow Program to increasing the number of BRCA Challenge grants, in order
to train future leaders in the field,” Ashworth says.
Pamela Munster, MD, director, Early Phase Clinical Trials Unit; and leader, Developmental Therapeutics Program, Helen Diller Family Comprehensive Cancer Center
27

All of us – and the patients we serve – are grateful for the
support of the Helen Diller Family Foundation and the
ways it has helped us reduce the incidence and impact of
prostate cancer.
Peter Carroll, MD, MPH
Ken and Donna Derr-Chevron Distinguished Professor in Prostate Cancer
Chair, Department of Urology
Associate Director, Strategic Planning and Clinical Services,
UCSF Helen Diller Family Comprehensive Cancer Center
“”

The Prostate Cancer Endowment“The Helen Diller Family Foundation’s remarkably generous endowment
benefitting the Prostate Cancer Program has supported and sustained what we
believe is the finest research program in the country for this disease,” says Peter
Carroll, MD, MPH, chair of the Department of Urology.
Evidence of the program’s prowess is clear in both the numbers – for a second consecutive
year, the UCSF urology program received more biomedical research funding from the
National Institutes of Health (NIH) than any other urology program in the country – and in the
department’s people, whose influence is both broad and deep.
“Our investigators have a solid foothold in many different types of research, including clinical
care, symptom support, and translational science,” Carroll says. “They are a diverse group that
represents the entire research spectrum, and the Diller Professors profiled here represent people
across many departments, who continue to work in fascinating and impactful ways. All of us –
and the patients we serve – are grateful for the support of the Helen Diller Family Foundation
and the ways it has helped us reduce the incidence and impact of prostate cancer.”
29

Nynikka Palmer, DrPH, MPH
In 2016, Nynikka Palmer, DrPH, MPH, became the
Helen Diller Family Professor in Community Education
and Outreach for Urologic Cancer. Working primarily
from Zuckerberg San Francisco General (ZSFG),
Palmer seeks, through her research, to eliminate
disparities in care, particularly for African-American
men with prostate cancer. Studies have shown
African-American men have higher death rates from
the disease, are both undertreated and overtreated,
and struggle to cope with the side effects of treatment.
With this in mind, in October 2014, Palmer launched a prostate cancer support group for African-
American men in the Oakland area, which includes those with prostate issues, the newly diagnosed,
and long-term survivors. In addition to helping each other, these men have become an invaluable
sounding board for Palmer’s research. They are contributing to one current project, in which she is
developing the use of peer navigators in the health care safety net.
The navigators – African-American prostate cancer survivors who can bridge the cultural gap and
mistrust that often exists between African-American men and the health care system – interpret
information and help patients think through both the short- and long-term implications of
treatment decisions.
Palmer will test the peer navigator concept, which has shown good results in breast cancer settings,
at two Bay Area safety-net hospitals. In addition, she and UCSF researcher Rena Pasick, DrPH, are
examining a new perspective on shared decision-making and working together on a prostate cancer
task force for SF CAN, the collaborative, system-wide approach to reducing San Francisco’s cancer
burden. Palmer hopes insights from her work also can help improve early detection and health
outcomes in the African-American community.
“We are trying to address a huge, complex problem, but piece by piece, I believe we can change
the quality of care prostate cancer patients receive and eliminate the disparities,” she says.
30

Stacey Kenfield, ScD
Stacey Kenfield, ScD, became the Helen Diller
Family Professor in Population Science for Urologic
Cancer in 2016. Her research aims to understand
how nutritional and lifestyle changes can improve
prostate cancer prevention and survival.
In November 2015, a study Kenfield published
in the Journal of the National Cancer Institute
estimated that in the US, 47 percent of lethal
prostate cancer would be preventable if men over
age 60 adopted five or six habits related to diet,
exercise, and smoking cessation. She is now principal investigator (PI) of a pilot study called
Prostate 8 that examines whether men with prostate cancer can use a web-based program to
adopt and sustain lifestyle changes that include these healthy habits. She also has a NIH R01
grant to test whether a targeted lifestyle program will modify prostate biology and deter cancer
progression in men who opt for surgery.
“We have received positive feedback from patients in the pilot trial, especially related to the
wearable activity devices and personalized lifestyle reports,” says Kenfield, who also has
co-authored diet and lifestyle recommendations for the Prostate Cancer Foundation. “We look
forward to building on the pilot work and improving the patient experience for the larger trial.”
Kenfield is PI or co-PI on a number of other trials crossing multiple sites, organizations, countries,
and concepts to further test and refine emerging ideas about the positive effects of diet and
exercise on prostate cancer prevention and progression. In addition, she directs the Movember
Foundation-funded global exercise trial in metastatic prostate cancer patients, which spans more
than 20 institutions in seven countries. Her work also contributes to Carroll’s vision of creating a
patient portal at UCSF where patients can log in, review treatment management options, and get
wellness and clinical information.
“We are building the evidence base and translating our findings for patients,” Kenfield says. “It’s
taken us 10 years since the first studies were published. We now believe we can move forward
with recommendations for what men can do outside of clinical care that can lower their risk for
aggressive prostate cancer or prostate cancer progression.”
31

Michael Rabow, MD
Since being appointed the Helen Diller Family
Professor in Palliative Care in 2014, Michael Rabow,
MD, has continued to integrate palliative care into
multiple cancer specialty clinics, including the STAND
(Supportive Therapy in Androgen Deprivation) clinic
for prostate cancer patients.
“Our work in the STAND clinic is an important
model for treating cancer as a chronic disease in
which we pay attention to treatment complications
and a patient’s entire health picture,” says Rabow,
who directs the Symptom Management Service at the UCSF Helen Diller Family Comprehensive
Cancer Center.
The STAND model has a number of elements.
First, doctors from multiple disciplines see patients in one location, underlining the HDFCCC’s
commitment to a patient-centered approach.
Second, all clinicians – from palliative care specialists to oncologists – learn from each other by
working face-to-face with the same patient. “This advances primary palliative care, where all
clinicians have a knowledge and facility for treating such basic concerns as pain or symptom
management or straightforward depression,” Rabow says.
Third, patients and clinicians do advance-care planning together to ensure patients receive care
consistent with their priorities and values.
“With prostate cancer, there is a spectrum of response from watchful waiting to the most aggressive
chemotherapy,” Rabow says. “Because most patients now have more options, we need a much
more nuanced response to cancer that includes talk about outcomes, prognoses, side effects,
and values.”
Rabow, his HDFCCC colleagues, and a patient advisory group are now developing a program to
ensure every patient receives this type of advance-care planning.
“I could see people doing a first draft of advance directives as part of a group, because peers can
sometimes say things to each other that a health care provider cannot,” Rabow says. “For all of this,
we must remember that the patient, family, and community are the center of our universe.”
32

Matthew Cooperberg,
MD, MPH
Named to the Helen Diller Family Professorship in
Urology in 2013, Matthew Cooperberg, MD, MPH,
continues to be central to numerous important
efforts to reduce the burden of prostate cancer.
In 2016, Cooperberg became PI on an R01
grant aimed at using microRNAs – blood-based
biomarkers – to improve risk stratification for men
with prostate cancer. Working with UCSF’s Robert
Blelloch, MD, PhD, who is the Peter R. Carroll, MD, MPH, Distinguished Professor in Urology, and
members of his lab, Cooperberg’s goal is to develop a blood test that can eventually replace or
at least compete with tissue-based testing. “Our thinking is that blood testing is easier to repeat,
less invasive, more economical, and gets around concerns about sampling in biopsies,” he says.
Because Blelloch’s lab can now sequence an entire microRNA panel, the team plans to use this
ability over the next five years to develop and validate the blood test on thousands of samples
that the HDFCCC has gathered over the past decade. “The fact that we have these samples is a
tribute to Peter Carroll’s prescient vision,” Cooperberg says.
Even as he plunges into this latest project, Cooperberg continues his work in many other areas.
The American Urological Association Quality Registry (AQUA), which he was instrumental
in developing and implementing, now has more than 1 million unique urology patients in its
database and is starting to yield insights into prostate cancer management trends nationwide.
He also has continued his passionate advocacy for retaining prostate-specific antigen (PSA)
screening, which he says is still one of the most successful biomarkers when used correctly.
As part of this effort, Cooperberg serves on the SF CAN prostate cancer task force, focusing on
increasing PSA screening in communities hardest hit by prostate cancer.
Cooperberg is a national leader in refining the use of active surveillance, continually honing the
concept through his work with CaPSURE (UCSF’s Cancer of the Prostate Strategic Urologic
Research Endeavor) and a related US Department of Defense-funded study. “We now know,
for example, that because some tumors will never metastasize, we don’t need to watch these
patients as carefully,” he says.
33

Davide Ruggero, PhD
In 2011, Davide Ruggero, PhD, a professor in the
departments of Urology and Cellular and Molecular
Pharmacology, was named the Helen Diller Family
Professor in Basic Research in Urologic Cancer.
Since then, his lab has generated a multitude of
important findings.
Ruggero and his team have focused their attention
on oncogenes – genes associated with the
conversion of normal cells into tumor cells – that
increase protein synthesis and metabolic activity,
which in turn induce a stressor to which cancer cells must respond to survive.
“This is a vulnerable point, because the increased protein-dependent stress response occurs
only in cancer cells, not in normal cells,” he says. “In a preclinical trial with genetically engineered
mouse models, we are using a pharmacogenetic approach to block the stress response, and
we’re finding that doing so blocks prostate tumor development.”
Ruggero’s lab is developing a patient-derived xenograft (PDX) model to further test this concept. In
PDX models, scientists implant human tumors in mice – an approach considered as close as one
can get to replicating human response. “We have five independent prostate patient PDX models
that are showing similar results when we block the stress response,” he says. He hopes these
findings can quickly lead to a human trial.
In related work, his lab is analyzing microarrays of 250 patients to track how this specific stress
response affected patients’ disease course. “We believe a high stress response is associated
with more aggressive tumors and relapse,” Ruggero says – a finding that, if verified, can lead to
a more personalized care approach. “Knowing whether a prostate cancer patient harbors these
oncogenes and engages this stress response allows us to identify, segregate, and refer properly.”
Finally, Ruggero is working with the biotech company eFFECTOR Therapeutics to develop the
first compounds for regulating the protein eIF4E. Last year, his lab found cancer cells hijack eIF4E
to fuel their growth but that reducing the protein by half in mice and human cells engendered
no ill effects in normal cells while suppressing tumor growth. “We now have ongoing clinical and
preclinical animal trials that target the eIF4E activity,” he says. “This is an exciting step forward.”
34

Katsuto Shinohara, MD
The clinical research of Katsuto Shinohara, MD,
who was named the Helen Diller Family Professor
in Clinical Urology in 2010, has enhanced access to
less invasive testing and treatment techniques for
patients with urologic cancers.
His primary focus in the last year was on magnetic
resonance imaging (MRI)-ultrasound fusion biopsy,
which is now a standard of care for prostate cancer
patients on active surveillance who previously have
had a positive biopsy. Shinohara helped pioneer this
image-guided, minimally invasive technique, which locates the cancer area using an MRI fused
with an ultrasound image. This helps clinicians better identify or exclude more aggressive cancers
and can help eliminate the need for repeat biopsies.
“In particular, we have shown MRI-fusion is good at identifying bigger and more aggressive types
of cancer, which helps us quickly recommend these patients for definitive treatment,” Shinohara
says. “It is also appropriate for the patient with a previously negative biopsy but whose PSA is
rising. If there is no evidence of cancer by MRI-fusion biopsy, then we can relax and continue to
follow these patients with PSA screening.”
Shinohara also has remained active in ongoing efforts that include improving biopsy specimen
handling by replacing paper with a small cassette, which enables clinicians to send the entire
length of the sample intact to pathology; and brachytherapy, which places radioactive “seeds” in
the prostate to reduce the exposure of healthy tissue to radiation.
“We have been using a new ultrasound device that can show simultaneous multiple views.
Though it’s too early to say, it looks as though the device has allowed us to more accurately
position the radioactive seed strand,” he says. Shinohara also treats prostate cancer with focal
cryoablation techniques. “Once we accrue a hundred patients, we need about 30 more, we will
publish efficacy and quality-of-life outcomes.”
35

The Investigational Trials Resource has been remarkably
responsive to the needs of our community, continually
adapting and innovating, and without its leadership and
responsiveness, progress would slow. The difference would
be night and day.
Alain Algazi, MD
Assistant Professor, Cutaneous Oncology Program
“”

Investigational Trials Resource “It’s not enough to have a good idea, because in
clinical research, there are so many steps and so
much oversight and monitoring that infrastructure
becomes key,” says Alain Algazi, MD, who this
year initiated a clinical trial program for head and
neck cancers at the HDFCCC with the help of the
Investigational Trials Resource (ITR). “The ITR has
been remarkably responsive to the needs of our
community, continually adapting and innovating, and without its leadership and
responsiveness, progress would slow. The difference would be night and day,”
Algazi says.
Eric Small, MD, deputy director and director of clinical sciences in the HDFCCC, leads the ITR.
In the last year, he and his team worked with researchers throughout the HDFCC to transform
the program’s structure to reflect changes in our understanding of cancer and how research
is organized.
“Even as our anatomic disease-oriented programs continue to grow, we have found better
ways to integrate those trials and researchers with programs that are scientifically cross-
cutting, like Developmental Therapeutics, Cancer Immunotherapy, and the Center for BRCA
Research,” Small says.
A new set of standardized procedures
In brief, the ITR’s careful consensus-building led to the creation of a new set of standardized
procedures for enrolling patients, patient safety, and data safety across multiple trials, as well
as the nuts and bolts of deciding who will do what – all while keeping an eye on what benefits
the most patients.
“Our systematic approach makes it possible for the ITR to harmonize work across the
HDFCCC, create new efficiencies, and still remain flexible enough to adapt to ongoing
change,” Small says.
Alain Algazi, MD
37

This integrated approach provides support in three important areas:
• A National Cancer Institute-mandated Protocol Review and Monitoring System provides
essential scientific review and monitoring of all studies.
• A data and safety monitoring committee ensures patients are safe and maintains the scientific
integrity of all data.
• A clinical research support office provides an ever-expanding array of administrative services
for the researchers, including essential clinical research coordinators.
In addition, Algazi says, the ITR’s thoughtful approach to building working groups among young
research staffers fosters greater retention, more continuity, and higher quality trials executed with
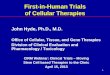
greater efficiency. The process has worked so well that in 2015, clinical interventional trial accruals
continued to increase to 1,191 patients.
Interventional Annual Accrual Summary
2010200920082007 2011 2012 2013 2014 2015
1200
1000
800
600
400
200
0
11171191
1015
879909
854
750
595506
NU
MB
ER
OF
PA
TIE
NT
S E
NR
OLL
ED
Sample Committee Network Web This structure is an example of how one cross-
cutting group works with anatomic site-specific
groups through a series of trials.
Developmental Therapeutics
Site Committee
Breast Cancer Site Committee
Other Sites
Heme/BMT Committee
GI Site Committee
GU Site Committee
Gyn Onc Site
Committee
Melanoma Site
Committee
Thoracic Oncology
Committee
38

Speeding new treatments to patients
Algazi is one of many grateful researchers. “We’ve been seeing patients in head and neck oncology for four or
five years, but until this year, there’s been virtually no research effort,” he says. “The ITR was essential to making
it happen. Its processes enabled us to quickly hire staff, apply resources, and get a viable and approved
program up and running that builds on UCSF’s strengths.”
The patient benefits are immediate, as multiple studies have shown that enrollment in trials correlates with
better clinical outcomes. In the head-and-neck group’s first year, it initiated five studies – including an innovative
pilot using gene therapy to stimulate anti-tumor immune responses, which has shown signs of being an
effective treatment – as well as several trials in collaboration with the Cancer Immunotherapy Program.
Small notes that when cancer clinicians moved to Mission Bay last year, it furthered cross-pollination among
diverse research teams. When the Precision Cancer Medicine Building opens in 2019, it will significantly
accelerate the movement from discovery to therapy and dramatically enhance what the ITR can do to facilitate
these processes.
“We are designing a building that truly reflects programmatic goals,” he says. “To have so many people side by
side in one unit will be an unprecedented opportunity to really make visible this concept of integrated care.”
39

Our goal is to have a clinical study or therapy available for
every patient referred to us.
Lawrence Fong, MD
Efim Guzik Distinguished Professor in Cancer Biology
Co-leader, Cancer Immunotherapy Program
“ ”

The Cancer Immunotherapy ProgramThe UCSF Helen Diller Family Comprehensive Cancer Center is a leader in
developing and refining cancer immunotherapies, which over the last few years
have achieved a durable response in a number of different cancers. These
therapies use the body’s immune system to fight cancer.
In 2015, to leverage its leadership role and drive next steps in developing these therapies, the
HDFCCC created the UCSF Cancer Immunotherapy Program, which pairs a high-powered
research effort with a state-of-the-art clinic and approximately 20 faculty members across
different disease groups and departments.
41

Direct patient care offers new hope
In the UCSF Cancer Immunotherapy Clinic (CIC), expert UCSF hematologists and oncologists from all
cancer sub-specialties work together to bring patients and their families an extensive and growing menu
of treatments, including cancer vaccines, cellular therapies, and other investigational agents.
“Our goal is to have a clinical study or therapy available for every patient referred to us,” says
Lawrence Fong, MD, Efim Guzik Distinguished Professor in Cancer Biology and co-leader of the
Cancer Immunotherapy Program.
Robert Thistle, 70, pictured above, is one such patient. Thistle has been battling metastatic kidney
cancer since he was diagnosed more than a decade ago. Originally, surgery appeared to have removed
the entire tumor, but in 2012, a bone metastasis was discovered in his upper arm. That also seemed to
have been successfully treated, but two years later, tumor nodules were discovered in his lungs.
While Thistle was reviewing alternatives to standard treatment that might have fewer side effects, Fong
was looking for potential candidates for a clinical trial. In January 2015, Thistle began treatment at UCSF
with an experimental checkpoint inhibitor drug. He then received a commercially available treatment that
targets blood-vessel growth in tumors, as well as an experimental immunotherapy drug. By August, the
nodules had shrunk to below their original size. Thistle was able to resume his normal life with the help
of regular immunotherapy infusions at UCSF. Now 70, he says, “I try to be more alive in each moment.”
42

We’ve already published a study
where we showed we are inducing
immune responses that target
prostate cancer prior to surgical
resection.
Lawrence Fong, MD
“”
Expanding patient access
Immunotherapies have emerged as a standard of care for a number of common cancers, including
melanoma and cancers of the prostate, lung, blood, bladder, and kidney. Nevertheless, Fong says, the
therapies don’t work as well for everybody as they have for Thistle, and they can cause side effects.
Scientists are now racing to better understand which immunotherapies will be effective across cancer
types, why they work in some people and not in others, and how to create more precise treatments
that reflect individual biology, tumors, and immune system response.
“Our program is trying to dramatically shrink the proportion of patients who don’t get any benefit and
also discover combination therapies that will achieve responses without the toxicities,” Fong says.
Clinicians at the CIC use immunotherapies as first- or second-line treatments when possible and
offer clinical studies – both phase I and “basket” trials, which apply the therapies across disease
states. In some cases, physicians prescribe the therapies alone; in others, they combine them with
things like targeted therapies, chemotherapy, or radiation. In still other cases, physicians give patients
immunotherapy treatment before surgical resection to activate the immune system while the cancer is
still present, so it will recognize any metastases that occur post-surgery. “We’ve already published a
study where we showed we are inducing immune responses that target prostate cancer prior to
surgical resection,” Fong says.
Gabriel Mannis, MD, is the CIC’s co-director for hematological cancers. From years of performing
blood and bone marrow transplants, Mannis has acquired extensive experience with immune
system modification.
“It’s exciting that many of these new immunotherapies appear to mimic the effects of bone marrow
transplant, potentially without the associated risks of graft-versus-host disease or the need for a
43

bone marrow donor,” he says. “We can even envision an end to the era of traditional bone marrow
transplantation.”
CAR-T cells – a specific type of immune system cell – that are removed from the patient, modified,
and then reinfused, have shown exciting results in several types of blood cancers and are the key to
success in this area. “If we can get CAR-T cells to stick around rather than being eliminated by the
body over time, we could have long-lasting remissions or cures without the need for a transplant,”
Mannis says.
Amy Lin, MD, co-director for solid tumors, says the clinic also offers access to immunotherapies for
nearly any type of solid tumor, with numerous individual studies defining what qualifies a patient for a trial.
“There is a lot to be learned, and that’s the whole point of this type of clinic,” she says. “We’re adding
therapies, mixing therapies, studying immunology, and learning at an exponential rate.”
However, Mannis adds, because many of these therapies are still investigational, they need to be
administered at a center with the expertise to manage the potential complications. “We’ve built an
infrastructure designed to do just that. It’s part of the strength of being at UCSF,” he says.
”FPO
Gabriel Mannis, MD, and Lawrence Fong, MD, explain treatment to a patient.
44

Close collaboration to speed precision
medicine approaches
To continue refining clinicians’ understanding of the right therapies or right sequence of therapies,
Fong says the CIC and its companion Cancer Immunotherapy Laboratory (CIL) offer patients a unique
advantage that goes even beyond rare access to novel treatments.
“We obtain samples from every patient – not just blood, but sputum, stool, or biopsies – and have
world-leading scientists study what’s going on with the person’s individual tumor and immune system so
we can move toward having the right cancer therapy and right immunotherapy for every patient,” says
Fong. “We believe this precision approach means the days when you get a diagnosis and a drug off a
shelf are numbered. My dream is that eventually precision immunotherapies will kill cancers outright and
completely avert the need for surgery or conventional therapies.”
Without the HDFCCC’s support and UCSF’s prominence in the field, none of this could have come
to fruition, and Fong says he’s excited by the potential for accelerated advances. Through the CIL,
he and his colleagues collaborate with the newly created Parker Institute for Cancer Immunotherapy,
where some faculty members have joint appointments, and he has forged research agreements with
companies like Bristol-Myers Squibb, Amgen, Genentech, AbbVie, and Merck.
“These companies are working with us to specifically understand immune responses in human
cancer,” says Fong. “We share our findings as part of different collaborations.” If these innovations and
collaborations can yield the hoped-for results, then many more patients can benefit as Thistle has.
My dream is that eventually
precision immunotherapies will
kill cancers outright and completely
avert the need for surgery or
conventional therapies.
Lawrence Fong, MD
“”
45

The Impact Grants aim to find high-risk, high-reward
projects that would not otherwise get support in the
current environment.
Alan Ashworth, PhD, FRS
“”

Impact Grant Awards Earlier this year, the Helen Diller Family Comprehensive Cancer Center brought
“Shark Tank”-style competition to cancer research. HDFCCC president Alan
Ashworth, PhD, FRS, launched the inaugural Impact Grant Awards by asking
a simple question: “Do you have a wild idea that could significantly impact
cancer?” Entries were encouraged from anyone in the UCSF community,
including students, researchers, and staff not affiliated with the HDFCCC.
“The Impact Grants aim to find high-risk, high-reward projects that would not otherwise get
support in the current environment,” Ashworth says. “By easing application criteria, we received
bold ideas from applicants spanning multiple disciplines and career levels at UCSF.”
47

Six finalists were chosen in a competitive selection process from a pool of 52 applicants. The ideas
were judged on four criteria: Cancer relevance, novelty of approach, impact, and unlikelihood of
being funded by conventional mechanisms.
The competition included lively five-minute presentations from each of the six finalists, as well as
extremely engaging Q&A, and provocative suggestions for future themes in each project.
Immediately following the presentations, Ashworth announced two $250,000 grants. Eleni Linos,
MD, MPH, DrPH, an assistant professor of dermatology at UCSF, and Stephen Francis, PhD, MS,
a postdoctoral scholar in epidemiology and biostatistics, received the first UCSF HDFCCC
Impact Grants.
Linos pitched a project to study whether connecting with women through social media could
motivate them to avoid harmful indoor tanning beds. Francis proposed a study looking at
The six finalists in the inaugural Impact Grant Awards, with Alan Ashworth, PhD, FRS.
48

whether in utero cytomegalovirus infection is a causal factor in the development of childhood acute
lymphoblastic leukemia. The Impact Grants will provide Linos and Francis the time to gather and
analyze data so they can then apply for funding from conventional sources such as the NIH.
Ashworth is quick to note the true impact of these grant awards goes beyond providing research
projects with initial funding.
“The application process also provided an excellent mechanism for anyone at UCSF to make me
personally aware of their particular research aims, something that doesn’t always naturally happen,”
he says. “I now have 52 excellent projects that I can share with potential philanthropic partners. This
is a winning scenario for everyone, particularly in the case of our junior researchers who are just
beginning their careers in cancer.”
Next year’s Impact Grant Awards pitch sessions, scheduled for early March 2017, promise to be even
more exciting, with three $250,000 research grants to be awarded.
The application process also provided
an excellent mechanism for anyone
at UCSF to make me personally
aware of their particular research
aims, something that doesn’t always
naturally happen.
Alan Ashworth, PhD, FRS
“
”2016 Impact Grant Award recipients Steven Francis, PhD, MS, and Eleni Linos, MD, MPH, DrPH, with Alan Ashworth, PhD, FRS.
49

© 2016 The Regents of the University of California
Photographers: Steve Babuljak, Sonya Yruel
C251A