Embed Size (px)
Citation preview

1
ANNEX I
SUMMARY OF PRODUCT CHARACTERISTICS

2
1. NAME OF THE MEDICINAL PRODUCT
Enbrel 25mg powder and solvent for solution for injection.
2. QUALITATIVE AND QUANTITATIVE COMPOSITION
Each vial contains 25mg of etanercept. Etanercept is a human tumour necrosis factor receptor p75 Fc fusion protein produced by recombinant DNA technology in a Chinese hamster ovary (CHO) mammalian expression system. Etanercept is a dimer of a chimeric protein genetically engineered by fusing the extracellular ligand binding domain of human tumour necrosis factor receptor-2 (TNFR2/p75) to the Fc domain of human IgG1. This Fc component contains the hinge, CH2 and CH3 regions but not the CH1 region of IgG1. Etanercept contains 934 amino acids and has an apparent molecular weight of approximately 150 kilodaltons. The potency is determined by measuring the ability of etanercept to neutralise the TNFα-mediated growth inhibition of A375 cells. The specific activity of etanercept is 1.7 x 106 units/mg.
For Excipients, see 6.1.
3. PHARMACEUTICAL FORM
Powder and solvent for solution for injection.
4. CLINICAL PARTICULARS
4.1 Therapeutic indications
Treatment of active rheumatoid arthritis in adults when the response to disease-modifying antirheumatic drugs, including methotrexate (unless contraindicated), has been inadequate.

3
Treatment of active polyarticular-course juvenile chronic arthritis in children aged 4 to 17 years who have had an inadequate response to, or who have proved intolerant of, methotrexate. Enbrel has not been studied in children aged less than 4 years.
4.2 Posology and method of administration
Enbrel treatment should be initiated and supervised by specialist physicians experienced in the diagnosis and treatment of rheumatoid arthritis.
Adults (18-64 years)
25 mg Enbrel reconstituted in 1 ml of water for injections administered twice weekly as a subcutaneous injection, is the recommended dose for optimal therapeutic response. 25 mg administered once weekly gives a slower response and may be less effective.
Elderly patients (≥ 65 years)
No dose adjustment is required. Posology and administration are the same as for adults 18-64 years of age. Children and adolescents (≥ 4 to <18 years) 0.4 mg/kg (up to a maximum of 25 mg per dose) after reconstitution of 25 mg Enbrel in 1 ml of water for injections, given twice weekly as a subcutaneous injection with an interval of 3-4 days between doses.

4
Renal and hepatic impairment
No dose adjustment is required.
4.3 Contraindications
Hypersensitivity to the active substance or to any of the excipients.
Sepsis or risk of sepsis.
Treatment with Enbrel should not be initiated in patients with active infections including chronic or localised infections.
4.4 Special warnings and special precautions for use
Infections
In postmarketing reports, serious infections (fatal, life threatening, or requiring hospitalisation or intravenous antibiotics), have been reported with the use of Enbrel. Many of these serious events have occurred in patients with underlying diseases that in addition to their rheumatoid arthritis could predispose them to infections. Patients who develop a new infection while undergoing treatment with Enbrel should be monitored closely. Administration of Enbrel should be discontinued if a patient develops a serious infection. Physicians should exercise caution when considering the use of Enbrel in patients with a history of recurring infections or with underlying conditions which may predispose patients to infections such as advanced or poorly controlled diabetes.
Allergic reactions
Allergic reactions associated with Enbrel administration during clinical trials have been reported rarely (<1%). If any serious allergic or anaphylactic reaction occurs, Enbrel therapy should be discontinued immediately and appropriate therapy initiated.
Immunosuppression
The possibility exists for anti-TNF therapies, including Enbrel, to affect host defences against infections and malignancies since TNF mediates inflammation and modulates cellular immune responses. In a study of 49 patients with rheumatoid arthritis treated with Enbrel, there was no evidence of depression of delayed-type hypersensitivity, depression of immunoglobulin levels, or change in enumeration of effector cell populations. Whether treatment with Enbrel might influence the development and course of malignancies and active and/or chronic infections is unknown. The safety and efficacy of Enbrel in patients with immunosuppression or chronic infections have not been evaluated.

5
Two juvenile chronic arthritis patients developed varicella infection and signs and symptoms of aseptic meningitis which resolved without sequelae. Patients with a significant exposure to varicella virus should temporarily discontinue Enbrel therapy and be considered for prophylactic treatment with Varicella Zoster Immune Globulin.
Vaccinations
No data are available on the effects of vaccination in patients receiving Enbrel. Live vaccines should not be given concurrently with Enbrel. No data are available on the secondary transmission of infection by live vaccines in patients receiving Enbrel. It is recommended that juvenile chronic arthritis patients, if possible, be brought up to date with all immunisations in agreement with current immunisation guidelines prior to initiating Enbrel therapy.
Autoantibody formation
Treatment with Enbrel may result in the formation of autoimmune antibodies (see section 4.8).
Combination therapy
The long-term safety of Enbrel in combination with other disease-modifying antirheumatic drugs has not been established.

6
Renal and hepatic impairment
Based on pharmacokinetic data (see section 5.2), no dosage adjustment is needed in patients with renal or hepatic impairment; clinical experience in such patients is limited.
4.5 Interaction with other medicinal products and other forms of interaction
Interactions between Enbrel and other drugs have not been evaluated in formal studies. In clinical trials, no interactions have been observed when Enbrel was administered with glucocorticoids, salicylates, nonsteroidal anti-inflammatory drugs (NSAIDs), analgesics, or methotrexate. No data are available on the effects of vaccination in patients receiving Enbrel. See section 4.4 for vaccination advice.
4.6 Pregnancy and lactation
There are no studies of Enbrel in pregnant women. Developmental toxicity studies performed in rats and rabbits have revealed no evidence of harm to the foetus or neonatal rat due to etanercept. Preclinical data about peri- and postnatal toxicity of etanercept and of effects of etanercept on fertility and general reproductive performance are not available. Thus, the use of Enbrel in pregnant women is not recommended, and women of child-bearing potential should be advised not to get pregnant during Enbrel therapy.
Use during lactation
It is not known whether etanercept is excreted in human milk. Because immunoglobulins, in common with many medicinal products, can be excreted in human milk, a decision should be made whether to discontinue nursing or to discontinue Enbrel while nursing.
4.7 Effects on ability to drive and use machines
No studies on the effects on the ability to drive and use machines have been performed.
4.8 Undesirable effects
Undesirable effects in adults with rheumatoid arthritis

7
Enbrel has been studied in 1,809 patients with rheumatoid arthritis. Data presented from controlled studies included 349 patients who received Enbrel, and 152 patients who received placebo. The proportion of patients who discontinued treatment due to adverse events was the same in both the Enbrel and placebo treatment groups (4%).
Injection Site Reactions
Compared to placebo, patients treated with Enbrel had a significantly higher incidence of injection site reactions (37% vs. 10%). All injection site reactions were described as mild (erythema and/or itching, pain, or swelling). Injection site reactions generally occurred in the first month, if they occurred at all, and subsequently decreased in frequency. Mean duration was 3 to 5 days. No treatment was given for the majority of injection site reactions in the Enbrel treatment groups, and the majority of patients who were given treatment received topical preparations such as corticosteroids, or oral antihistamines. Additionally, some patients developed recall injection site reactions characterised by a skin reaction at the most recent site of injection along with the simultaneous appearance of injection site reactions at previous injection sites. These reactions were generally transient and did not recur with treatment.
Infections
In clinical trials, upper respiratory infections (“colds”) and sinusitis were the most frequently reported infections in patients receiving Enbrel or placebo. In placebo-controlled trials, the incidence of upper respiratory tract infections was 16% in the placebo treatment group and 29% in the group treated with Enbrel; 0.68 events per patient year in the placebo group and 0.82 events per patient year in the group treated with Enbrel when the longer observation of patients on Enbrel was accounted for. In placebo-controlled trials evaluating Enbrel, no increase in the incidence of serious infections (fatal, life threatening, or requiring hospitalisation or intravenous antibiotics) was observed (1.3% placebo, 0.9% Enbrel). Among the 1,809 Enbrel-treated patients, 99 serious infections were observed, including, for example, abscess (at various sites), bacteremia, bronchitis, bursitis, cellulitis, cholecystitis, diarrhoea, diverticulitis, endocarditis (suspected), gastroenteritis, herpes zoster, leg ulcer, mouth infection, osteomyelitis, peritonitis, pneumonia, pyelonephritis, sepsis, septic arthritis, skin infection, skin ulcer, urinary tract infection, vasculitis, and wound infection.
Serious infections have also been reported during post-marketing use of Enbrel. Some have occurred within a few weeks after initiating treatment with Enbrel in patients who have underlying conditions (e.g., diabetes, congestive heart failure, history of active or chronic infections) in addition to their rheumatoid arthritis. (See WARNINGS). Data from a sepsis clinical trial not specifically in patients with rheumatoid arthritis suggest that Enbrel treatment may increase mortality in patients with established sepsis.
Malignancies
Twenty new malignancies of various types were observed in 1,809 rheumatoid arthritis patients treated in clinical trials with Enbrel for up to 24 months. The observed rates and incidences were similar to those expected for the population studied.

8
Autoantibodies
Patients had serum samples tested for autoantibodies at multiple timepoints. Of the patients evaluated for antinuclear antibodies (ANA), the percentage of patients who developed new positive ANA (≥1:40) was higher in patients treated with Enbrel (11%) than in placebo-treated patients (5%). The percentage of patients who developed new positive anti-double-stranded DNA antibodies was also higher by radioimmunoassay (15% of patients treated with Enbrel compared to 4% of placebo-treated patients) and by Crithidia luciliae assay (3% of patients treated with Enbrel compared to none of placebo-treated patients). The proportion of patients treated with Enbrel who developed anticardiolipin antibodies was similarly increased compared to placebo-treated patients. No patients developed clinical signs suggestive of a lupus-like syndrome or other new autoimmune diseases. The impact of long-term treatment with Enbrel on the development of autoimmune diseases is unknown.
Other undesirable effects
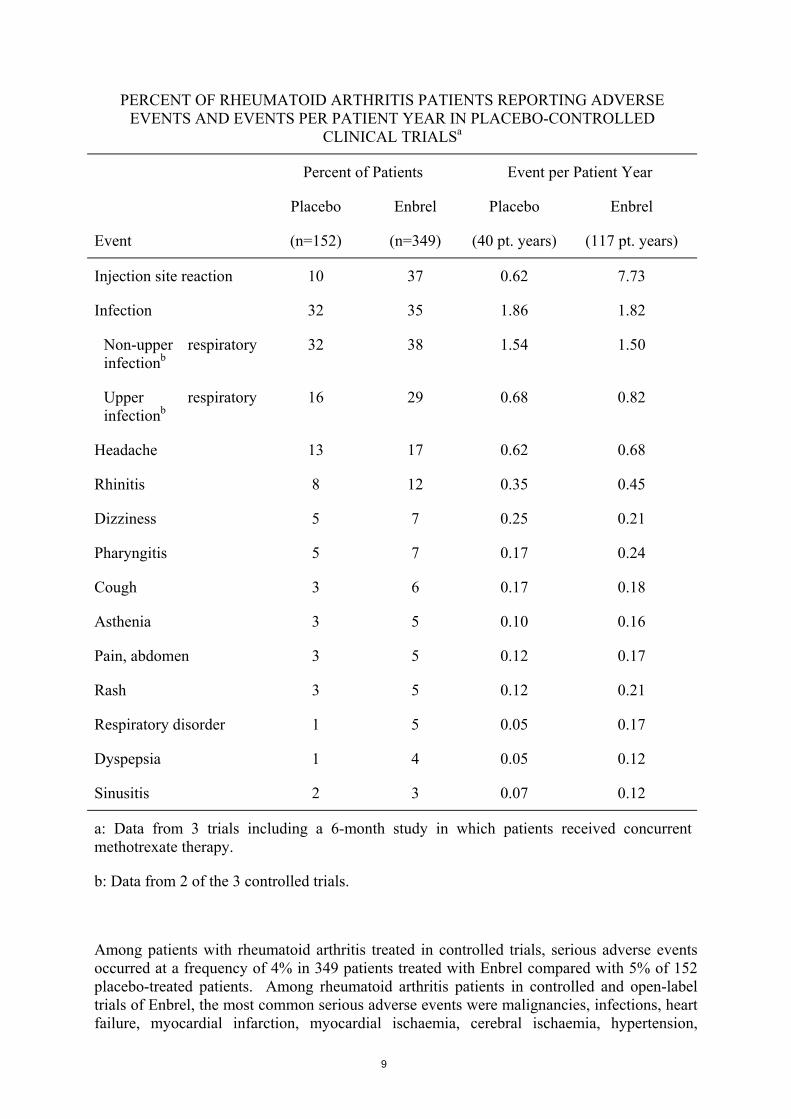
Events reported in at least 3% of all patients with higher incidence in patients treated with Enbrel compared to controls in placebo-controlled rheumatoid arthritis trials (including a trial of Enbrel and methotrexate in combination use) and events per patient year are summarised in the following table.
9
PERCENT OF RHEUMATOID ARTHRITIS PATIENTS REPORTING ADVERSE EVENTS AND EVENTS PER PATIENT YEAR IN PLACEBO-CONTROLLED
CLINICAL TRIALSa
Percent of Patients Event per Patient Year
Event
Placebo
(n=152)
Enbrel
(n=349)
Placebo
(40 pt. years)
Enbrel
(117 pt. years)
Injection site reaction 10 37 0.62 7.73
Infection 32 35 1.86 1.82
Non-upper respiratory infectionb
32 38 1.54 1.50
Upper respiratory infectionb
16 29 0.68 0.82
Headache 13 17 0.62 0.68
Rhinitis 8 12 0.35 0.45
Dizziness 5 7 0.25 0.21
Pharyngitis 5 7 0.17 0.24
Cough 3 6 0.17 0.18
Asthenia 3 5 0.10 0.16
Pain, abdomen 3 5 0.12 0.17
Rash 3 5 0.12 0.21
Respiratory disorder 1 5 0.05 0.17
Dyspepsia 1 4 0.05 0.12
Sinusitis 2 3 0.07 0.12
a: Data from 3 trials including a 6-month study in which patients received concurrent methotrexate therapy.
b: Data from 2 of the 3 controlled trials.
Among patients with rheumatoid arthritis treated in controlled trials, serious adverse events occurred at a frequency of 4% in 349 patients treated with Enbrel compared with 5% of 152 placebo-treated patients. Among rheumatoid arthritis patients in controlled and open-label trials of Enbrel, the most common serious adverse events were malignancies, infections, heart failure, myocardial infarction, myocardial ischaemia, cerebral ischaemia, hypertension,

10
hypotension, cholecystitis, pancreatitis, gastrointestinal haemorrhage, bursitis, depression, and dyspnoea.
Based on the results of clinical studies in rheumatoid arthritis, normally no special laboratory evaluations are necessary in addition to careful medical management and supervision of patients.
Undesirable effects in paediatric patients with juvenile chronic arthritis
In general, the adverse events in paediatric patients were similar in frequency and type to those seen in adult patients. Differences from adults and other special considerations are discussed in the following paragraphs.
Severe undesirable effects reported in a trial in 69 juvenile chronic arthritis patients aged 4 to 17 years included varicella with signs and symptoms of aseptic meningitis which resolved without sequelae (see also 4.4), gastroenteritis, depression/personality disorder, cutaneous ulcer, and oesophagitis/gastritis.
Forty-three of 69 (62%) children with juvenile chronic arthritis experienced an infection while receiving Enbrel during 3 months of the study (part 1 open-label). The types of infections reported in juvenile chronic arthritis patients were generally mild and consistent with those commonly seen in outpatient paediatric populations. The types and proportion of other adverse reactions in juvenile chronic arthritis patients were similar to those seen in trials of Enbrel in adult patients with rheumatoid arthritis, and the majority were mild. Several adverse events were reported more commonly in 69 juvenile chronic arthritis patients receiving 3 months of Enbrel compared to the 349 adult rheumatoid arthritis patients. These included headache (19% of patients, 1.7 events per patient year), nausea (9%, 1.0 event per patient year), abdominal pain (19%, 0.74 events per patient year), and vomiting (13%, 0.74 events per patient year).
11
4.9 Overdose
No dose-limiting toxicities were observed during clinical trials of rheumatoid arthritis patients. The highest dose level evaluated has been an intravenous loading dose of 32 mg/m2 followed by subcutaneous doses of 16 mg/m2 administered twice weekly. One rheumatoid arthritis patient mistakenly self-administered 62 mg Enbrel subcutaneously twice weekly for 3 weeks without experiencing undesirable effects. There is no known antidote to Enbrel.
5. PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Selective immunosuppressant agents.
ATC code:L04AA11
Tumour necrosis factor (TNF) is a dominant cytokine in the inflammatory process of rheumatoid arthritis. Etanercept is a competitive inhibitor of TNF-binding to its cell surface receptors and thereby inhibits the biological activity of TNF. TNF and lymphotoxin are pro-inflammatory cytokines that bind to two distinct cell surface receptors: the 55-kilodalton (p55) and 75-kilodalton (p75) tumour necrosis factor receptors (TNFRs). Both TNFRs exist naturally in membrane-bound and soluble forms. Soluble TNFRs are thought to regulate TNF biological activity.
TNF and lymphotoxin exist predominantly as homotrimers, with their biological activity dependent on cross-linking of cell surface TNFRs. Dimeric soluble receptors such as etanercept possess a higher affinity for TNF than monomeric receptors and are considerably more potent competitive inhibitors of TNF binding to its cellular receptors. In addition, use of an immunoglobulin Fc region as a fusion element in the construction of a dimeric receptor imparts a longer serum half-life.
Mechanism of action
Much of the joint pathology in rheumatoid arthritis is mediated by pro-inflammatory molecules that are linked in a network controlled by TNF. The mechanism of action of etanercept is thought to be its competitive inhibition of TNF binding to cell surface TNFR, preventing TNF-mediated cellular responses by rendering TNF biologically inactive.

12
Etanercept may also modulate biologic responses controlled by additional downstream molecules (e.g., cytokines, adhesion molecules, or proteinases) that are induced or regulated by TNF.
Clinical trials
The efficacy of Enbrel was assessed in a randomised, double-blind, placebo-controlled study. The study evaluated 234 patients with active rheumatoid arthritis who were ≥ 18 years old, had failed therapy with at least one but no more than four disease-modifying antirheumatic drugs (DMARDs; e.g., hydroxychloroquine, oral or injectable gold, methotrexate, azathioprine, D-penicillamine, sulphasalazine), and had ≥ 12 tender joints, ≥ 10 swollen joints, and either erythrocyte sedimentation rate ≥ 28 mm/hr, C-reactive protein > 2.0 mg/dl, or morning stiffness for ≥ 45 minutes. Doses of 10 mg or 25 mg Enbrel or placebo were administered subcutaneously twice a week for 6 consecutive months. The results of this controlled trial were expressed in percentage improvement in rheumatoid arthritis using American College of Rheumatology (ACR) response criteria. The primary endpoint was achievement of an ACR 20 response at month 3. Subjects who failed to respond based on pre-specified criteria for lack of efficacy before month 3 were allowed to drop out early and were considered treatment failures. By definition, an ACR 20 response is achieved if a patient experiences a 20% improvement in their tender joint count and swollen joint count plus ≥ 20% improvement in at least three of the following five criteria: (1) patient pain assessment, (2) patient global assessment, (3) physician global assessment, (4) patient self-assessed disability, and (5) acute-phase reactant (erythrocyte sedimentation rate or C-reactive protein). ACR 50 and 70 responses are defined using the same criteria with a 50% improvement or a 70% improvement, respectively. ACR 20 and 50 responses were higher in patients treated with Enbrel at 3 and 6 months as seen in the table below:

13
ACR RESPONSES
Placebo Enbrela
Response (n=80) (n=78)
(% of patients)
ACR 20
Month 3 23% 62%b
Month 6 11% 59%b
ACR 50
Month 3 8% 41%b
Month 6 5% 40%b
a: 25 mg Enbrel SC twice weekly.
b: p ≤ 0.01, Enbrel vs. placebo
Approximately 15% of subjects who received Enbrel achieved an ACR 70 response at month 3 and month 6 compared to fewer than 5% of subjects in the placebo arm. Among patients receiving Enbrel, the clinical responses generally appeared within 1 to 2 weeks after initiation of therapy and nearly always occurred by 3 months. A dose response was seen; results with 10 mg were intermediate between placebo and 25 mg. Enbrel was significantly better than placebo in all components of the ACR criteria as well as other measures of rheumatoid arthritis disease activity not included in the ACR response criteria, such as morning stiffness. A Health Assessment Questionnaire (HAQ), which included disability, vitality, mental health, general health status, and arthritis-associated health status subdomains, was administered every 3 months during the trial. All subdomains of the HAQ were improved in patients treated with Enbrel compared to controls at 3 and 6 months.
An additional randomised, controlled, double-blind trial evaluated 180 patients with similar criteria to the first study. Doses of 0.25 mg/m2, 2 mg/m2, and 16 mg/m2 Enbrel were administered subcutaneously twice a week for 3 consecutive months. A dose-dependent increase in the proportion of subjects achieving an ACR 20 response was seen, with 75% of subjects responding in the highest dose group (16 mg/m2 Enbrel).
After discontinuation of Enbrel, symptoms of arthritis generally returned within a month. Reintroduction of treatment with Enbrel after discontinuations of up to 24 months resulted in

14
the same magnitudes of response as patients who received Enbrel without interruption of therapy based on results of open-label studies. Continued durable responses have been seen for up to 24 months in open-label extension treatment trials when patients received Enbrel without interruption; longer-term experience is not available.
Polyarticular-Course Juvenile Chronic Arthritis
The safety and efficacy of Enbrel were assessed in a two-part study in 69 children with polyarticular-course juvenile chronic arthritis who had a variety of juvenile chronic arthritis onset types. Patients ages 4 to 17 years with moderately to severely active polyarticular-course juvenile chronic arthritis refractory to or intolerant of methotrexate were enrolled; patients remained on a stable dose of a single nonsteroidal anti-inflammatory drug and/or prednisone (< 0.2 mg/kg/day or 10 mg maximum). In part 1, all patients received 0.4 mg/kg (maximum 25 mg per dose) Enbrel subcutaneously twice weekly. In part 2, patients with a clinical response at day 90 were randomised to remain on Enbrel or receive placebo for four months and assessed for disease flare. Responses were measured using the JRA Definition of Improvement (DOI), defined as ≥ 30% improvement in at least three of six and ≥ 30% worsening in no more than one of six JRA core set criteria, including active joint count, limitation of motion, physician and patient/parent global assessments, functional assessment, and erythrocyte sedimentation rate (ESR). Disease flare was defined as a ≥ 30% worsening in three of six JRA core set criteria and ≥ 30% improvement in not more than one of the six JRA core set criteria and a minimum of two active joints.
In part 1 of the study, 51 of 69 (74%) patients demonstrated a clinical response and entered part 2. In part 2, 6 of 25 (24%) patients remaining on Enbrel experienced a disease flare compared to 20 of 26 (77%) patients receiving placebo (p=0.007). From the start of part 2, the median time to flare was ≥ 116 days for patients who received Enbrel and 28 days for patients who received placebo. Of patients who demonstrated a clinical response at 90 days and entered part 2 of the study, some of the patients remaining on Enbrel continued to improve from month 3 through month 7, while those who received placebo did not improve.
Studies have not been done in patients with polyarticular-course juvenile chronic arthritis to assess the effects of continued Enbrel therapy in patients who do not respond within 3 months of initiating Enbrel therapy or to assess the combination of Enbrel with methotrexate.
Antibodies to Enbrel
Antibodies to Enbrel, all non-neutralising, were detected in 4 out of 96 rheumatoid arthritis patients who received Enbrel at a dose of 25 mg twice a week for up to 3 months. Although the experience does not exclude the possibility that a clinically relevant effect might occur, no apparent correlation of antibody development to clinical response or adverse events was seen
5.2 Pharmacokinetic properties
15
Etanercept serum values were determined by an ELISA method, which may detect ELISA-reactive degradation products as well as the parent compound.
Etanercept is slowly absorbed from the site of subcutaneous injection, reaching maximum concentration approximately 48 hours after a single dose. The absolute bioavailability is 76%. With twice weekly doses, it is anticipated that steady-state concentrations are approximately twice as high as those observed after single doses. After a single subcutaneous dose of 25 mg Enbrel, the average maximum serum concentration observed in healthy volunteers was 1.65 ± 0.66 μg/ml, and the area under the curve was 235 ± 96.6 μg•hr/ml. Dose proportionality has not been formally evaluated, but there is no apparent saturation of clearance across the dosing range.
A biexponential curve is required to describe the concentration time curve of etanercept. The central volume of distribution of etanercept is 7.6 l, while the volume of distribution at steady-state is 10.4 l.
Etanercept is cleared slowly from the body. The half-life is long, approximately 70 hours. Clearance is approximately 0.066 l/hr in patients with rheumatoid arthritis, somewhat lower than the value of 0.11 l/hr observed in healthy volunteers. Although there is elimination of radioactivity in urine after administration of radiolabelled etanercept to patients and volunteers, increased etanercept concentrations were not observed in patients with acute renal or hepatic failure. The presence of renal and hepatic impairment should not require a change in dosage. There is no apparent pharmacokinetic difference between men and women.
Methotrexate has no effect on the pharmacokinetics of etanercept. The effect of Enbrel on the human pharmacokinetics of methotrexate has not been investigated. Elderly patients
The impact of advanced age was studied in the population pharmacokinetic analysis of etanercept serum concentrations. Clearance and volume estimates in patients aged 65 to 87 years were similar to estimates in patients less than 65 years of age.
Patients with polyarticular-course juvenile chronic arthritis
In a polyarticular-course juvenile chronic arthritis trial with Enbrel, 69 patients (age 4 to 17 years) were administered 0.4 mg Enbrel/kg twice weekly for three months. Serum concentration profiles were similar to those seen in adult rheumatoid arthritis patients. The youngest children (4 years of age) had reduced clearance (increased clearance when normalised by weight) compared with older children (12 years of age) and adults. Simulation of dosing suggests that while older children (10-17 years of age) will have serum levels close to those seen in adults, younger children will have appreciably lower levels.

16
5.3 Preclinical safety data
In the toxicological studies with Enbrel, no dose-limiting or target organ toxicity was evident. Enbrel was considered to be non-genotoxic from a battery of in vitro and in vivo studies. Carcinogenicity studies, and standard assessments of fertility and postnatal toxicity, were not performed with Enbrel due to the development of neutralising antibodies in rodents.
Enbrel did not induce lethality or notable signs of toxicity in mice or rats following a single subcutaneous dose of 2000 mg/kg or a single intravenous dose of 1000 mg/kg. Enbrel did not elicit dose-limiting or target organ toxicity in cynomolgus monkeys following twice weekly subcutaneous administration for 4 or 26 consecutive weeks at a dose (15 mg/kg) that resulted in AUC-based serum drug concentrations that were over 27-fold higher than that obtained in humans at the recommended dose of 25 mg.
6. PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Powder: mannitol, sucrose, and trometamol.
Solvent: Water for injections
6.2 Incompatibilities
In the absence of incompatibility studies, this medicinal product must not be mixed with other medicinal products.
6.3 Shelf life
18 months.
The reconstituted product should be used immediately (ie, within 6 hours if stored at 2°C - 8°C).
6.4 Special precautions for storage

17
Store at 2°C - 8°C. Do not freeze.
6.5 Nature and contents of container
Clear glass vial (4 ml, type I glass) with rubber stoppers, aluminium seals, and flip-off plastic caps. Enbrel is supplied with pre-filled syringes containing water for injections. The syringes are type I glass-fitted with stainless steel needles.
Cartons contain 4 vials of Enbrel with 4 prefilled syringe and 8 alcohol swabs.
6.6 Instructions for use, handling, and disposal
Enbrel 25 mg is reconstituted with 1 ml water for injections. Enbrel contains no antibacterial preservative, and therefore, solutions prepared with water for injections should be administered as soon as possible and within 6 hours following reconstitution.
Any unused product or waste material should be disposed of in accordance with local requirements.

18
7. MARKETING AUTHORISATION HOLDER
Wyeth Europa Ltd.
Huntercombe Lane South
Taplow, Maidenhead
Berkshire, SL6 0PH
United Kingdom
8. NUMBER(S) IN THE COMMUNITY REGISTER OF MEDICINAL PRODUCTS
9. DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION
10. DATE OF REVISION OF THE TEXT

19
ANNEX II
A. MANUFACTURING AUTHORISATION HOLDERS RESPONSIBLE FOR BATCH RELEASE AND MANUFACTURER OF THE BIOLOGICAL ACTIVE SUBSTANCE
B. CONDITIONS OF THE MARKETING AUTHORISATION

20
A. MANUFACTURING AUTHORISATION HOLDERS RESPONSIBLE FOR BATCH RELEASE AND MANUFACTURER OF THE BIOLOGICAL ACTIVE SUBSTANCE
Name and address of the manufacturer of the biological active substance
Boehringer Ingelheim Pharma KG
Birkendorfer Strasse 65
D-88397 Biberach an der Riss,
Germany
Manufacturing Authorisation issued on 1 January 1998 by Regierungspräsidium Tübingen, Germany
Name and address of the manufacturers responsible for batch release
John Wyeth & Brother Ltd. New Lane Havant Hants, P09 2NG UK
Wyeth Medica Ireland, Little Connell, Newbridge Co. Kildare Ireland
Manufacturing licenses issued respectively by the Medicines Control Agency on 26 January 1999 and by the Irish Medicines Board on 28 January 1999.
The printed package leaflet of the medicinal product must state the name and address of the manufacturer responsible for the release of the concerned batch.

21
B. CONDITIONS OF THE MARKETING AUTHORISATION
• CONDITIONS OR RESTRICTIONS REGARDING SUPPLY AND USE IMPOSED ON THE MARKETING AUTHORISATION HOLDER
Medicinal product subject to restricted medical prescription (See Annex I: Summary of Product Characteristics, 4.2).

22
ANNEX III
LABELLING AND PACKAGE LEAFLET

23
A. LABELLING

24
CARTON TEXT
Enbrel 25 mg Powder and solvent for solution for injection
etanercept
4 vials 25 mg.
4 prefilled syringes of solvent 1 ml.
8 pre-injection swabs
Each solvent syringe contains 1 ml water for injections.
Each vial of Enbrel contains 25 mg etanercept. Other ingredients include mannitol, sucrose and trometamol.
Subcutaneous use.
Read the package leaflet before use.
Store at 2°C - 8°C (in a refrigerator).
Do not freeze.
Enbrel should be administered within 6 hours following reconstitution (if stored at 2°C - 8°C).
Keep out of the reach and sight of children.
Medicinal product subject to medical prescription.
EU/X/XX/XXX/XXX.

25
Wyeth Europa Ltd.,
Huntercombe Lane South,
Taplow, Maidenhead,
Berkshire,
SL6 0PH, United Kingdom.
Lot: XXXX
EXP: XX/YYYY
Wyeth

26
VIAL LABEL
Enbrel 25 mg
Subcutaneous use
Store at 2°C - 8°C
Lot: XXXX
EXP: XX/YYYY
Wyeth
SYRINGE LABEL
Solvent for Enbrel
1 ml water for injections
Lot: XXXX
EXP: XX/YYYY
TRAY BACKING TEXT
Enbrel 25 mg powder and solvent for solution for injection
etanercept
Wyeth Europa Ltd
EXP: XX/YYYY
Lot: XXXX

27
B. PACKAGE LEAFLET

28
PACKAGE LEAFLET
Read all of this leaflet carefully before you start taking this medicine.
- Keep this leaflet. You may need to read it again.
- If you have further questions, please ask your doctor or your pharmacist.
- This medicine has been prescribed for you personally and you should not pass it on to others. It may harm them, even if their symptoms are the same as yours.
In this leaflet:
1. What Enbrel is and what it is used for
2. Before you inject Enbrel
3. How to take Enbrel
4. Possible side effects
5. Storing Enbrel
The name of your medicine is Enbrel 25 mg powder and solvent for solution for injection. Each vial of Enbrel contains 25 mg of the active substance etanercept. The other ingredients are mannitol, sucrose and trometamol. Each prefilled syringe contains 1 ml of water for injections.
The marketing authorisation holder for Enbrel is:
Wyeth Europa Ltd.
Huntercombe Lane South
Taplow, Maidenhead
Berkshire, SL6 0PH
United Kingdom
Enbrel is manufactured by:
Wyeth Laboratories or Wyeth Medica Ireland
New Lane Little Connell
Havant Newbridge
Hampshire, PO9 2NG Co. Kildare
United Kingdom Ireland

29
1. WHAT ENBREL IS AND WHAT IT IS USED FOR
Enbrel is supplied as a powder and solvent for solution for injection. Each pack contains 4 single dose vials, 4 prefilled syringes of water for injections and 8 pre-injection swabs.
Enbrel is a product of biotechnology. It is made from two human proteins. Many of the symptoms of rheumatoid arthritis may be due to another protein which causes inflammation. Enbrel works by attaching to this protein and blocking its activity. This blocking action reduces the pain and inflammation associated with rheumatoid arthritis.
Enbrel is an anti-rheumatic medicine that works by decreasing the pain and swelling in your joints. Enbrel is used for the treatment of active rheumatoid arthritis in adults when the response to disease-modifying antirheumatic drugs has been inadequate (including methotrexate unless you are unable to take methotrexatate). Enbrel is also used for the treatment of polyarticular-course juvenile chronic arthritis in children aged 4 to 17. Enbrel has not been tested in children less than 4 years old.
2. BEFORE YOU INJECT ENBREL
Do not inject Enbrel:
- If you or your child are hypersensitive (allergic) to etanercept or any of the other ingredients of Enbrel. If you or your child experience allergic reactions such as chest tightness, wheezing, dizziness or rash, do not inject more Enbrel and contact your doctor immediately.
- If you or your child have or are at risk of developing sepsis (blood poisoning). If you are not sure, please contact your doctor.
- If you or your child have an infection, including a long-term or localised infection (for example, leg ulcer) do not start Enbrel. If you are unsure, please contact your doctor.
Take special care with Enbrel:
− If you or your child are about to have any major surgery or develop a new infection. Your doctor may wish to monitor your treatment.

30
− Advise your doctor if you or your child have a history of recurrent infections or suffer from diabetes or other conditions that increase the risk of infection.
− Some vaccines, such as oral polio vaccine, should not be given while receiving Enbrel. Please check with your doctor before you or your child receive any vaccines.
− If possible, children should be up to date with all vaccinations before receiving Enbrel.
Pregnancy
The effects of Enbrel in pregnant women are not known, and so the use of Enbrel in pregnant women is not recommended. You are advised to not become pregnant while taking Enbrel therapy. In case you become pregnant, you should consult your doctor.
Breast-feeding
It is not known if Enbrel passes into breast milk. You should not breast-feed while taking Enbrel.
Taking other medicines:
Please inform your doctor or pharmacist if you or your child are taking or have recently taken any other medicines, even those not prescribed by your doctor.
The long-term safety of Enbrel in combination with other drugs for the treatment of rheumatoid arthritis has not been established.
3. HOW TO TAKE ENBREL
Dosing for adult patients
Your doctor will tell you how to inject Enbrel. The recommended dose for adults with rheumatoid arthritis is 25mg given twice a week as an injection under the skin. However, your doctor may determine an alternative frequency at which to inject Enbrel.
Dosing for children and adolescents:

31
The appropriate dose for your child will vary depending on your child’s body weight. Your child’s doctor will provide detailed directions for preparing and measuring the appropriate dose for your child.
If you feel that the effect of Enbrel is too strong or too weak, talk to your doctor or pharmacist.
Method and route of administration
Enbrel is injected under the skin. The injection can be self-administered or given by another person, for example a family member or friend, your doctor or his/her assistant. The detailed instructions on injection procedure provided in the attached leaflet should be followed. You should continue to inject Enbrel for as long as instructed by your doctor.
To help you remember, write in a diary which days of the week you or your child should receive an injection.
Enbrel must be dissolved before use. The injection should not be mixed in the same syringe or vial as any other medicine.
If you inject more Enbrel than you should:
If you accidentally inject more Enbrel than told to by your doctor, you should either call a doctor or go to the nearest hospital emergency department. Always take the outer carton or the vial of medicine with you, even if it is empty.
If you forget to inject Enbrel:
If you forget to give yourself or your child an injection you should inject the next dose of Enbrel as soon as you remember. Then continue to inject your medicine as prescribed by your doctor. Do not take a double dose to make up for forgotten individual doses.
4. POSSIBLE SIDE EFFECTS
Like all medicines, Enbrel can have side effects. If any side effects worry you, or if you or your child have any unusual effects, please call your doctor or pharmacist.

32
If you or your child experience a severe rash or swollen face or difficulty breathing while taking Enbrel contact your doctor or seek emergency medical care immediately.
Side effects in adult patients
The most common undesirable effect in adults is a mild reaction in the area where the medicine was injected, including itching, soreness, redness, swelling or pain around the injection site. Generally, these reactions do not occur as often after the first month of treatment. If you are concerned about injection site reactions contact your doctor or pharmacist. When injecting Enbrel, some patients have developed a reaction at an injection site used before.
Other side effects which may occur in adults while taking Enbrel include: headache, runny nose, rash, upset or painful stomach, diarrhoea, increased cough, feeling weak, pain, dizziness, sore throat, high blood pressure, inflamed or irritated sinuses.
Less frequently, serious infections that have occurred in adults while taking Enbrel, include kidney or urinary infection, bronchitis, joint inflammation or infection, localised infections in the abdomen or legs, tissue and wound infection, bone marrow infection, pneumonia, shingles, mouth infection, skin infection, bowel inflammation, bursitis, endocarditis (suspected), gastroenteritis, peritonitis, skin ulcer, vasculitis, and blood poisoning. Patients who have other medical problems, which increase the risk of infection, may rarely develop serious infections including fatal sepsis, while taking Enbrel. Other serious side effects include malignancies, heart failure, heart attack, stroke, low blood pressure, gall bladder inflammation, inflammation of the pancreas, gastrointestinal bleeding, shortness of breath or depression. These side effects have occurred at a similar rate in patients with rheumatoid arthritis not taking Enbrel.
Side effects in children and adolescents
In general, the side-effects in children and adolescents are similar to those seen in adults. Side-effects reported more commonly in juvenile chronic arthritis patients than in adult rheumatoid arthritis patients were headache, nausea, stomach pain, and vomiting.
In clinical trials, juvenile chronic arthritis patients treated with Enbrel experienced infections which were generally mild and similar to those seen in juvenile chronic arthritis patients who were not receiving Enbrel. Two patients treated with Enbrel who had chickenpox developed signs of chickenpox meningitis. They both made a full recovery. If you or your child are exposed to chickenpox, tell your doctor at once so that appropriate advice and, if necessary,

33
preventative treatment can be given. Other serious events noted in children receiving Enbrel were depression/behaviour disorder, diarrhoea, skin ulcer, and inflammation of the throat and stomach.
If you think that you or your child are suffering from any side-effect of Enbrel treatment, whether or not it is described in this leaflet, please inform your doctor or pharmacist.

34
5. STORING ENBREL
Keep out of the reach and sight of children.
Store at 2°C - 8°C (in a refrigerator). Do not freeze.
After preparing the Enbrel solution it should be used immediately (within 6 hours when stored in the refrigerator at 2°C - 8°C). Carefully dispose of any Enbrel solution that has not been injected within 6 hours.
Do not use after the expiry date (EXP) stated on the carton.
This leaflet was last approved on {date}

35
Further information
For any information about this medicinal product, please contact the local representative of the Marketing Authorisation Holder.
LOCAL REPRESENTATIVE
België /Belgique/Belgien
AHP Pharma S.A.
Rue du Bosquet, 15
B-1348 Louvain-la-Neuve
Tél/ Tel: + 32 10 494711
France
Wyeth-Lederlé
Le Wilson 2
80, Avenue du General de Gaulle
Puteaux
F-92031 Paris la Défense, Cedex
Tél: + 33 1 41 02 70 00
Österreich
Wyeth-Lederle Pharma GmbH
Storchengasse 1
A-1150 Wien
Tel: + 43 1 891140
Danmark
Wyeth Lederle Denmark
Produktionsvej 24
DK-2600 Glostrup Tlf: + 45 44 888805
Ireland
Wyeth Laboratories
Huntercombe Lane South
Taplow, Maidenhead
Berkshire, SL6 0PH
UK
Tel: + 44 1628 604377
Portugal
Wyeth Lederle Portugal
(Farma) Lda.
Rua Dr. António Loureiro Borges, 2
Arquiparque - Miraflores
P-1495-131 Algés
Tel: + 35 1 1412 8200
Deutschland
Wyeth-Pharma GmbH
Schleebrüggenkamp 15
Italia
Wyeth Lederle S.p.A.
Via Nettunense, 90
Suomi/Finland
Wyeth Lederle Finland
Rajatorpantie 41C

36
D-48159 Münster
Tel: + 49 251 2040
I-04011 Aprilia (LT)
Tel: + 39 06 927151
FIN-01640 Vantaa
Puh/Tfn: + 358 9 8520 2180
Ελλάδα
Wyeth Hellas Α.Ε.Β.Ε.
Κύπρου 126 & 25ης Μαρτίου
GR-164 52 Αθήνα
Τηλ: + 301 99 81 600
Luxembourg/Luxemburg
AHP Pharma S.A.
Rue du Bosquet, 15
B-1348 Louvain-la-Neuve
Tél: + 32 1049 4711
Sverige
Wyeth Lederle Nordiska AB
Box 1822
S-171 24 Solna
Tln: + 46 8 470 3200
España
Wyeth Orfi SA
Ctra. de Burgos, km.23
E-28700 San Sebastian de Los Reyes
Madrid
Tel: + 34 91 334 6565
Nederland
AHP Pharma B.V.
Postbus 255
NL-2130 AG Hoofddorp
Tel: + 31 23 5672567
United Kingdom
Wyeth Laboratories
Huntercombe Lane South
Taplow, Maidenhead
Berkshire, SL6 0PH
UK
Tel: + 44 1628 604377

37
INSTRUCTIONS FOR PREPARING AND GIVING AN INJECTION OF ENBREL
Introduction
The following instructions explain how to prepare and inject Enbrel. Please read the instructions carefully and follow them step by step. You will be instructed by your doctor or his/her assistant on the technique of self-injection or giving an injection to your child. A “dose preparation guide” (specially designed underside of the tray) is provided to assist you with aligning the vial and the solvent syringe. Do not attempt to self-inject or give your child an injection until you are sure that you understand how to prepare and give the injection.
This injection should not be mixed in the same syringe or vial with any other medicine.
Setting up for an injection
• Wash your hands thoroughly.
• The dose tray should contain the items listed below. (If not, don’t use the dose tray and consult your pharmacist). Use only the items listed. Do NOT use any other syringe.
Enbrel vial
prefilled syringe containing clear, colourless solvent (water for injections)
syringe plunger
2 alcohol swabs
dose preparation guide (underside of the dose tray)
• Inspect the expiry dates on both the vial label and the syringe label. They should not be used after the month and year shown.
Choosing and preparing an injection site
• Choose an injection site on the thigh, stomach, or on the back part of the upper arm.

38
A different site should be used for each new injection. Each new injection should be given at least 3 cm from an old site. Do NOT inject into areas where the skin is tender, bruised, red, or hard. (It may be helpful to keep notes on the location of the previous injections.)
• Wipe the injection site where Enbrel is to be injected with an alcohol swab, using a circular motion. Do NOT touch this area again before giving the injection.
Prepare the Enbrel dose for injection using the “dose preparation guide” (underside of the dose tray)
• Remove the contents of the tray and turn the tray over. The underside of the tray is a “dose preparation guide.” It is specially designed to hold the vial and syringe in place while preparing the Enbrel solution.
• Remove the plastic cap from the Enbrel vial. Do NOT remove the grey stopper or aluminium ring around the top of the vial.
• Use a new alcohol swab to clean the grey stopper on the Enbrel vial. After cleaning, do not touch the stopper with your hands.
• Press the Enbrel vial into the space to the right of the ∧ mark in the dose preparation guide; the grey stopper will face the centre of the tray.
• Remove the needle cover from the syringe taking care not to touch the needle or allowing it to touch any surface.

39
• With the needle pointed at the vial align the “0.5 ml” mark on the syringe with the edge of the dose preparation guide. Slide the syringe into the dose preparation guide until the needle goes through the grey stopper of the vial.
• Slide the plunger into the syringe.
• Turn the plunger clockwise until a slight resistance is felt.
ADDING SOLVENT
• SLOWLY push the plunger in until all the solvent is in the vial. This will help reduce foaming (lots of bubbles).
40
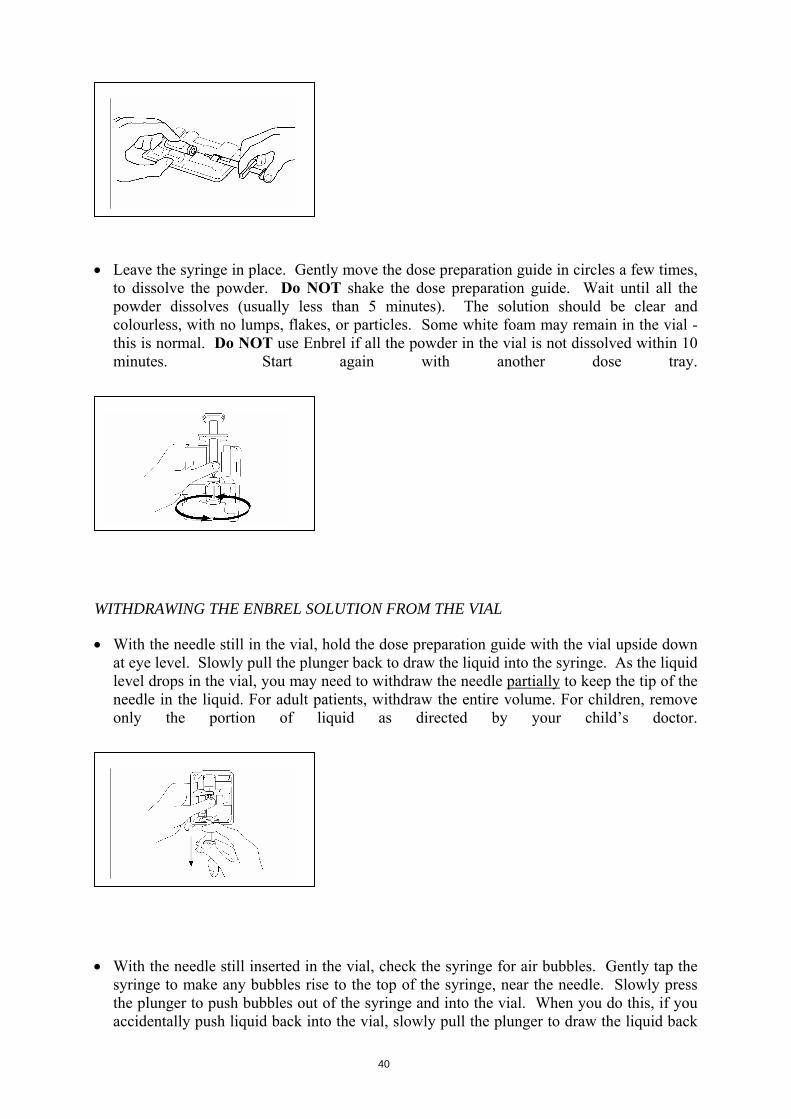
• Leave the syringe in place. Gently move the dose preparation guide in circles a few times, to dissolve the powder. Do NOT shake the dose preparation guide. Wait until all the powder dissolves (usually less than 5 minutes). The solution should be clear and colourless, with no lumps, flakes, or particles. Some white foam may remain in the vial - this is normal. Do NOT use Enbrel if all the powder in the vial is not dissolved within 10 minutes. Start again with another dose tray.
WITHDRAWING THE ENBREL SOLUTION FROM THE VIAL
• With the needle still in the vial, hold the dose preparation guide with the vial upside down at eye level. Slowly pull the plunger back to draw the liquid into the syringe. As the liquid level drops in the vial, you may need to withdraw the needle partially to keep the tip of the needle in the liquid. For adult patients, withdraw the entire volume. For children, remove only the portion of liquid as directed by your child’s doctor.
• With the needle still inserted in the vial, check the syringe for air bubbles. Gently tap the syringe to make any bubbles rise to the top of the syringe, near the needle. Slowly press the plunger to push bubbles out of the syringe and into the vial. When you do this, if you accidentally push liquid back into the vial, slowly pull the plunger to draw the liquid back

41
into the syringe.
• Slide the syringe out of the dose preparation guide. Again, do not touch the needle or allow it to touch any surface.
(Note: After you have completed these steps, a small amount of liquid may remain in the vial. This is normal.)
Injecting the Enbrel Solution
• With one hand, gently pinch the cleaned area of skin and hold it firmly. With the other
hand, hold the syringe at about a 45º angle to the skin.
With a quick, short motion, push the needle into the skin.
• Let go of the skin with the other hand.
• With your free hand, slowly push the plunger to inject solution.

42
When the syringe is empty, remove the needle from the skin being careful to keep it at the same angle it was, when it was inserted.
• Press a cotton ball over the injection site for 10 seconds. Slight bleeding may occur. Do NOT rub the injection site. A bandage is optional.
Disposing of Supplies
• The syringe and needle should NEVER be reused. Never recap a needle. Dispose of the needle and syringe as instructed by your doctor, nurse or pharmacist.
All questions should be handled by a doctor, nurse or pharmacist familiar with Enbrel





























