Embed Size (px)
Citation preview

Age 4.5 years , First visit to dentist

Oral Bacteria
• Gram positive
• Gram negative



What options are there?
DENTAL ISSUES
Can the tooth/teeth be saved?
Yes
What is required ?
No
What is required ?
CHILD
Can the tooth/teeth be saved?
Yes
What is required ?
No
What is required ?

OPTIONS
Monitor and review Analgesics/antibiotics Treatment
Pulpectomy Extraction
Review
Local anaesthesia
Inhalation Sedation
Sedation
General Anaesthesia

EXTRACT OR RETAIN
Is the tooth restorable ?
What is the appropriate management for the child?
Do parents understand consequences ?
Will there be follow up ?

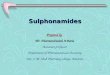
Bacteria in odontogenic infections
Streptococcus mutans 24.5%
Porphyromonas gingivalis 23.6
Porphroyromonas endodontalis 18.2%
Sretptococcus salivarius 10.1%
Streptococcus sanguis 8.3%
Strepotoccus pyogenes
Polymicrobial mixed infections most common (Cresente et al. 2018)

Control
Eliminate
Local measures
Systemic measures
Copyright Anne O'Connell

LA will not be effective in presence of infection

Copyright Anne O'Connell

Copyright Anne O'Connell

Copyright Anne O'Connell

Pulpectomy
Elimination of infection
Protection from future microbial invasion





Antibiotics?

When antibiotics are not the ‘first line’ management
• Pain
• Infection present but no systemic involvement
Draining sinus
Bone loss
• Ulceration
• Fever/malaise without obvious odontogenic origin
• Teething
Analgesics
Pulp therapy
Extraction
Incise and drain
Other

Copyright Anne O'Connell
INCISE AND DRAIN

Antibiotic may be required
Systemic signs related to dental infection
Immune compromised child
Local infection too large to allow effective LA
Intervention not possible due to behaviour eg. autism
In all cases, removing the cause of the infection must be planned

Are you using antibiotics correctly ?
Systemic signs only
Treat locally, where possible
Never use to control pain
Appropriate drug at appropriate dose with correct timing and instructions
Review and prevent future infection



Antibiotic Resistance

Resistance
“Antimicrobial resistance (AMR) is resistance of a
microorganism to an antimicrobial medicine to which it was previously sensitive.

In Asia one
infant dies
every 2 min
due to
infections
with resistant
bacteriaCars et al. 2007


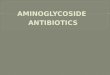
Timeline of antibiotic discovery
1941-1962 Golden Age
10 major classes of antibiotics introduced
Year
introduced
Class of drug
1935 Sulfonamides
1941 Penicillins
1944 Cephalosporins
1945 Aminoglycosides
1949 Chloramphenicol
1950 Tetracyclines
1952 Macrolides/ Lincosamides
1956 Glycopeptides
1957 Rifamycins
1959 Nitroimidazoles
1962 Quinolones
1968 Trimethoprim
2000 Oxalodinones
2003 Lipopeptides

PROGRESS

Health professionals can
Prevent infections ensuring your hands, instruments and environment are clean
Only prescribe and dispense antibiotics when they are needed, according to current guidelines
Prescribe the correct antibiotic using correct dose and duration
Talk to your patients about how to take antibiotics correctly, resistance and dangers of misuse.
Prevention and control of antibiotic resistance


Systemic Infection
Copyright Anne O'Connell



Is this right !
PainDiscomfortDehydrationDisruption of family3-4 days hospitalisationRisk of antibiotic related side effectsRisk of hospital acquired infectionsPsychological trauma

Systemic Infection


Penicillin
• Penicillin is the oral antibiotic of choice for mild to moderate odontogenic infections
• Has good activity against facultative Gram + cocci and gram –anaerobes
• If cellulitis, addition of metronidazole will increase activity against anaerobes.
• Penicillin resistant isolates from facial cellulitis can range up to 20%
• Allergy rate 0.7 – 10%
• Amoxicillin is as effective as Pen VK but is better absorbed
• Co-amoxiclav is active against beta lactamase producing bacteria
• Spreading cellulitis or not responsive to first dose

Compare
Amoxicillin
• Active orally• Not resistant to penicillinase• Contraindicated in penicillin
allergy• <40Kg 20-45 mg/kg/day q 12h• >40Kg 250-500mg q 8 hrs
500- 875 mg q 12h• Maximum dose 2 g/day• 5- 7 days
AugmentinAmoxicillin and potassium clavulanate
Inhibits some penicillinases and active against S aureus. Inhibits some lacatmases and active against gram – and penicillin resistant bacteria eg spreading cellulitis
• <40Kg 20-45 mg/kg/day q 12h
• >40Kg 500- 875 mg q 12h Increase x6 risk cholestatic
jaundice 5-7 days

Penicillin Allergic patientsClindamycin
Penicillin allergy or has had penicillin in last month
8-25 mg/kg q 8h for 7 days
Not for routine use
Serious side effects- AB related colitis
Used in endocarditis prophylaxis when allergy to penicillin
Azithromycin
Penicillin allergy or resistance
5-12mg/kg on day b1,5-6 mg/kg as daily dose(2-5 days)
Increasingly bacteria resistant
Common reactions diarrhoes, nausea, pain and macropapularrash

Metronidazole
Use with penicillins to increase spectrum
Use if penicillin taken in last month
Take with meals
Use with Amoxicillin
3-10 yrs 100 mg q 8h for 3-5 days
> 10 yrs 250 mg q 8h for 3-5 days

Severe infections
Loading dose
Use loading dose when severe infection and need to achieve therapeutic serum level ASAP
Eg Spreading cellulitis
Maintenance dose
May give double the recommended dose in severe infections for a short duration
Use where there is a need to control infection ASAP e.g. at risk child

Conclusion
Think before you write a prescription
Write prescription correctly with specific clear instructions
Ensure any antibiotic prescribed maximises effectiveness
Provide definitive care as soon as possible
Consider a loading dose or increase dose to achieve maximum levels
Consider shorter duration 3-7 days
Monitor the child during the course of the prescription
Educate parents, and local health providers