Embed Size (px)
Citation preview
Anne Arundel County Overdose Prevention Plan
JinleneChan,M.D.,M.P.HActingHealthOfficer
AnneArundelCountyDepartmentofHealth
June2013
AnneArundelCountyOverdosePreventionPlan June2013
1
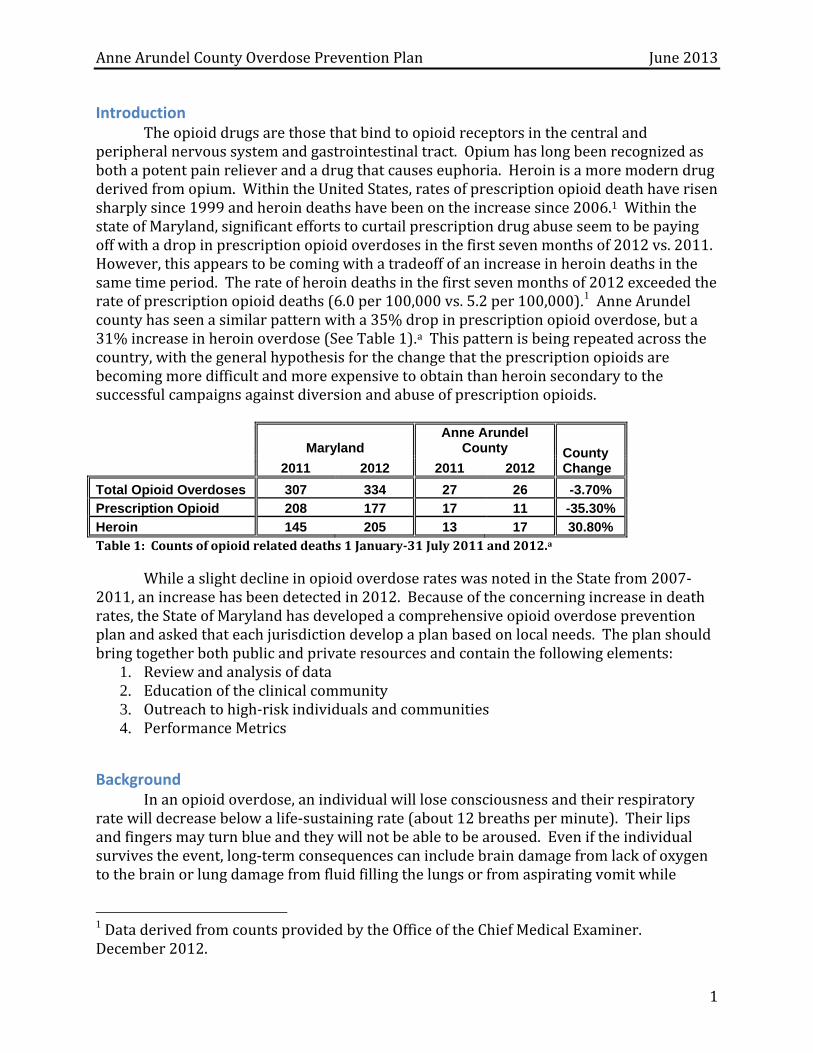
Introduction Theopioiddrugsarethosethatbindtoopioidreceptorsinthecentralandperipheralnervoussystemandgastrointestinaltract.Opiumhaslongbeenrecognizedasbothapotentpainrelieverandadrugthatcauseseuphoria.Heroinisamoremoderndrugderivedfromopium.WithintheUnitedStates,ratesofprescriptionopioiddeathhaverisensharplysince1999andheroindeathshavebeenontheincreasesince2006.1WithinthestateofMaryland,significanteffortstocurtailprescriptiondrugabuseseemtobepayingoffwithadropinprescriptionopioidoverdosesinthefirstsevenmonthsof2012vs.2011.However,thisappearstobecomingwithatradeoffofanincreaseinheroindeathsinthesametimeperiod.Therateofheroindeathsinthefirstsevenmonthsof2012exceededtherateofprescriptionopioiddeaths(6.0per100,000vs.5.2per100,000).1AnneArundelcountyhasseenasimilarpatternwitha35%dropinprescriptionopioidoverdose,buta31%increaseinheroinoverdose(SeeTable1).aThispatternisbeingrepeatedacrossthecountry,withthegeneralhypothesisforthechangethattheprescriptionopioidsarebecomingmoredifficultandmoreexpensivetoobtainthanheroinsecondarytothesuccessfulcampaignsagainstdiversionandabuseofprescriptionopioids.
Maryland Anne Arundel
County County Change 2011 2012 2011 2012
Total Opioid Overdoses 307 334 27 26 -3.70%
Prescription Opioid 208 177 17 11 -35.30%
Heroin 145 205 13 17 30.80% Table1:Countsofopioidrelateddeaths1January‐31July2011and2012.a
WhileaslightdeclineinopioidoverdoserateswasnotedintheStatefrom2007‐2011,anincreasehasbeendetectedin2012.Becauseoftheconcerningincreaseindeathrates,theStateofMarylandhasdevelopedacomprehensiveopioidoverdosepreventionplanandaskedthateachjurisdictiondevelopaplanbasedonlocalneeds.Theplanshouldbringtogetherbothpublicandprivateresourcesandcontainthefollowingelements:
1. Reviewandanalysisofdata2. Educationoftheclinicalcommunity3. Outreachtohigh‐riskindividualsandcommunities4. PerformanceMetrics
Background Inanopioidoverdose,anindividualwillloseconsciousnessandtheirrespiratoryratewilldecreasebelowalife‐sustainingrate(about12breathsperminute).Theirlipsandfingersmayturnblueandtheywillnotbeabletobearoused.Eveniftheindividualsurvivestheevent,long‐termconsequencescanincludebraindamagefromlackofoxygentothebrainorlungdamagefromfluidfillingthelungsorfromaspiratingvomitwhile
1DataderivedfromcountsprovidedbytheOfficeoftheChiefMedicalExaminer.December2012.
AnneArundelCountyOverdosePreventionPlan June2013
2
unarousable.Theoverdoselookssimilarregardlessofthetypeofopioidused.Eachopioidhasaspecificlengthoftimeitshouldlastinthebody.Heroinisfastacting,producingaquickhigh,whilemethadoneisverylongacting,leadingtoitslackofa“high.”Otherprescriptionopiateshaveanintermediatelengthoftimetheycontinueworking.Opiateoverdosescanhappenatlowerthanexpecteddoseswhentheopiatesarecombinedwithalcoholandotherdrugs,particularlybenzodiazepinesandcocaine.Itisimportantthatindividualsonlongeractingopiatesunderstandhowlongthedrugswillremainintheirsystemssothattheydonotinadvertentlyoverdose,thinkingthedrugwillnolongerhaveaneffect.
Whenratesofopioidabuse,overdose,andfatalityareevaluated,thenumberstypicallyreportedwilllookatallopioidstogetherandthenheroin,prescriptionopioids,andmethadonespecifically.Theterm“prescriptionopioid”doesnotimplythatthedrugwasprescribedtotheindividualorthattheindividualwastakingitforthepurposeforwhichitwasintended(typicallypainrelief).Additionally,methadoneistypicallyaprescribedopioidandmaybeundercountedasacauseofoverdoseinhospitalrecords,butwilllikelybeascribedcorrectlyinmedicalexaminerreports.
Take‐homenaloxoneprograms:Manymodernopioidoverdosepreventionprogramsincludetheuseofnaloxone.Naloxonecanbeprescribedbyproviderstoindividualsreceivingopioidmedicationsforchronicpainorindividualsonmethadoneforeitherpainoropioidaddictiontreatment.Additionally,itmaybegiventoknownusersofillicitopioidsubstancesuchasdivertedprescriptionopioidsorheroin. Naloxoneisanopioidmedicationthatdisplacesthedrugsonthemureceptorsinthecentralnervoussystemthatcausea“high.”Naloxonehasveryfewserioussideeffectsexceptinthoseallergictoit.Allergyisrare.Itisunlikelytobedivertedforalternativeusesince,ratherthancausingahigh,itcauseswithdrawal,whichisveryunpleasant.Itisalsorelativelycheap(lessthan20dollarsperdose).Oncenaloxoneisadministered,withinafewminutes,thevictimshouldwakeupfromtheiroverdose.Itisgenerallyinjected,althoughsomeprogramshavedevelopedanintranasalformulationthatisnotcurrentlyFDAapproved(theyjustattachanatomizertoasyringe).Theintranasalformulationseeemstoworkaswellastheinjectable,buttakesalittlelongertowork.Naloxonewearsoffwithinanhourtoanhourandahalf,soifthedruglastsinthesystemlongerthanthat(mostprescriptionopioidmedicationsandmethadone),itneedstobereadministered.Primarydisadvantagesofnaloxonearethatitisaprescribed,scheduledmedicationandthereforeisonlytobeusedandadministeredbythepersontowhomtheprescriptionwaswritten.Asopposedtoanepipen,ifanindividualisoverdosing,theywon’tknowit,theywillbeasleep.Theycannotinjectthemselves.Someoneelsemustinjectthem.Otherprogramshaverecommendedtrainingboththeindividualbeingprescribedthenaloxone,theirfriendsandtheirfamilymembers.2 InBaltimore,57%ofIVdrugusers(IVDU)hadwitnessedanoverdoseintheirlifetime.Increaseriskofoverdosewasnotedinthehomeless,historyofinjectingalone,injectingheroinandcocainetogether,andlongerdurationofuse.3ASanFranciscostudyalsonotedthat68%offataloverdosevictimswerealoneatthetimetheyoverdosed,butencouragingindividualstohaveabuddyincreasesriskofneedle‐sharing.4Anadditionalriskfactorforfataloverdoseisrecentreleasefromprison.Individualswhowerewithin1‐2weeksofreleasefromprisonwere3.2to11timesmorelikelytodiefromanoverdose
AnneArundelCountyOverdosePreventionPlan June2013
3
thanindividualswithin5to12weeksofreleasefromprison.Thisislikelyduetodecreasedtolerancetoopioidmedicationsandcanalsooccurafterdetoxification.Individualsforgetthattheirtoleranceisdecreasedandwhentheyagainreturntoopioiduse,theyusemorethantheycantolerate.5Potentiallyeffectivemethodsofrevivinganindividualfromanopioidoverdoseinadditiontonaloxone,includeCPRwithrescuebreathing,sternalrub,andcalling911.Witnessesareoftenreluctanttocall911duetofearofpoliceinvolvement,butthosefearsaregenerallyoverstatedasfewerthan3%ofindividualsinanyoftheevaluatedstudiesreportedanarrestoccuringatthesceneofanoverdosewhen911wascalledtosaveavictim.3 TheCDCreportsthat10,171reversalswithnaloxonewerereportedthroughJuneof2010fromlocalitiesthathavebegunaddingnaloxonetotheiropioidoverdosepreventionprograms.6Inunpublisheddata,thestateofMassachusettsreportsthattherehasbeenadecreaseinthedeathratefromopioidsincommunitieswithinthestatewithanaloxoneprogramvsthosewithout,howeverEDvisitsareunchanged.7Useofnaloxonebyabystanderhasbeenshowntodecreasethelikelihoodthattherescuerwillcall911inafewstudies.8,9Itisunclearifnaloxoneiscoveredbylocalinsurancecompanies,butgiventhatitisgenericandrelativelyinexpensive,itlikelywouldbecovered.ItiscoveredbyMedicarepartD.Afullnarcankitwithtwoinjectors,instructionsonuse,abarrierdeviseforrescuebreathing,andalcoholswabsgenerallycanbeassembledfor$36to$50.Theybecomemoreexpensiveforintranasalnaloxoneduetoneedforanatomizer.Kitsarenotavailableforpurchasebutareassembledbytheprogramsthatprovidethem.
NewlegislationinMarylandwillrequireanindividualtoreceivestandardizededucationandtrainingandtoshowcertificationofhavingreceivedthistrainingbeforereceivingaNaloxoneprescriptionfromamedicalprovider.
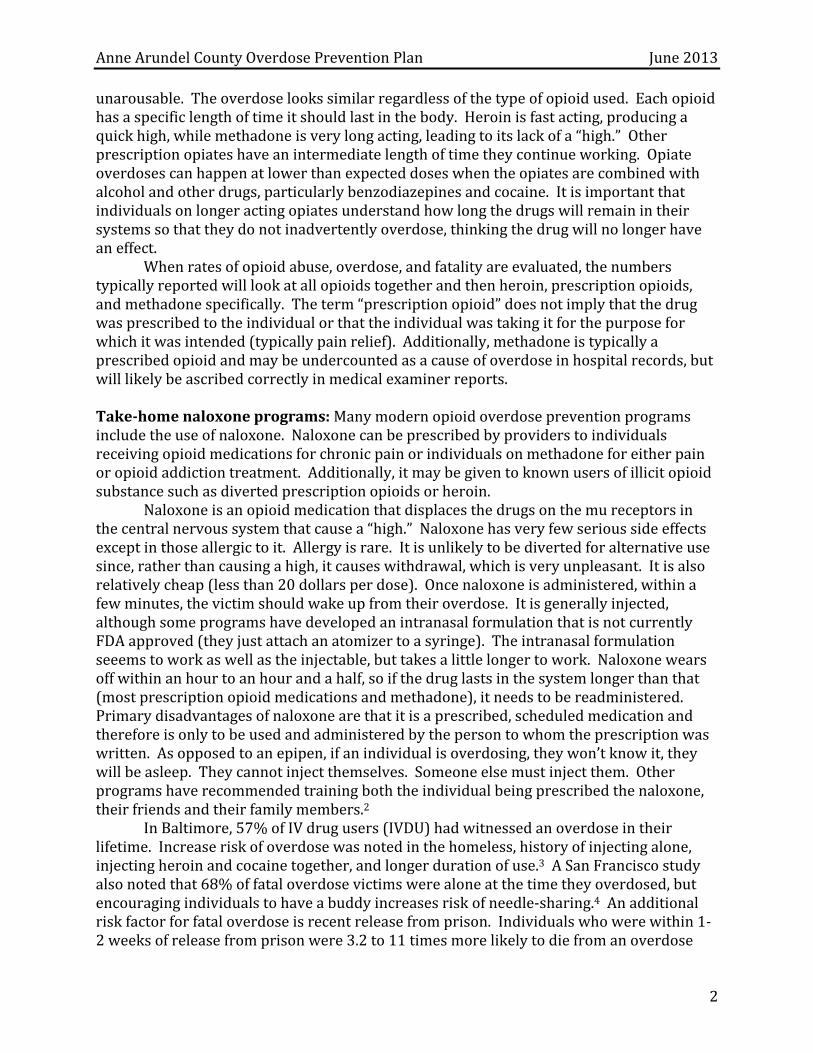
Review and Analysis of Local Data WhenthedeathdatapresentedinTable1isextrapolatedouttothefullyearandcomparedtoUSandStatedata,weseethatAnneArundelCountyhasaslightlylowerrateofprescriptionopioidoverdosethanboththeUSandtheStateofMaryland,butboththecountyandtheStatehaveamuchhigherrateofheroinrelateddeaths.
Opioid Overdose Rates Total
Opioid Rx
Opioid Heroin
United States 4.82 0.983
Maryland 9.92 5.26 6.09
Anne Arundel County 9.67 4.09 6.32 Table2:Annualizedratesofdeathextractedfrom2012StateandCountyJanuary‐Julydata.StateandCountypopulationsarebasedon2010Censusdata.Itshouldbenotedthatthenationaldataisbasedona2008estimateforprescriptionopioiddeathsanda2009estimateforheroindeaths.Allratesareper100,000personyears.
2“VitalSigns:OverdosesofPrescriptionOpioidPainRelievers—UnitedStates,1999‐2008.”MMWR.CDC2011;60(43).3EstimatefromNationalVitalstatistics2009whichstated“approximately3000heroindeaths.”
AnneArundelCountyOverdosePreventionPlan June2013
4
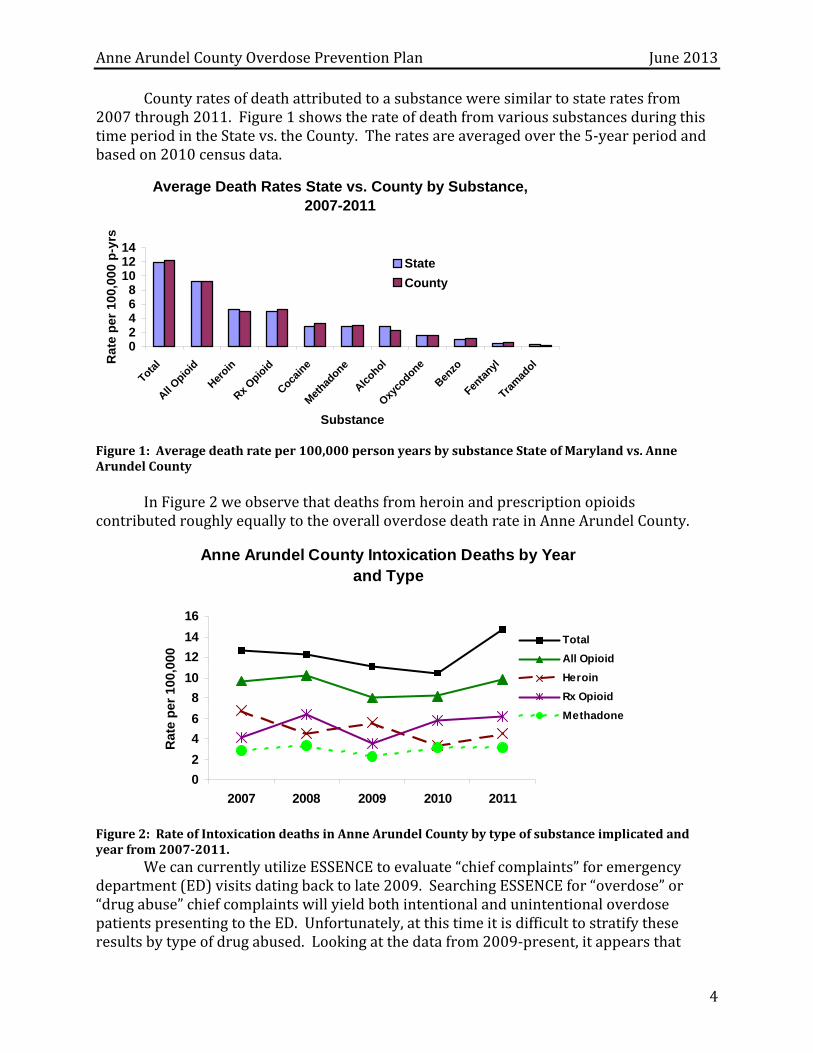
Countyratesofdeathattributedtoasubstanceweresimilartostateratesfrom2007through2011.Figure1showstherateofdeathfromvarioussubstancesduringthistimeperiodintheStatevs.theCounty.Theratesareaveragedoverthe5‐yearperiodandbasedon2010censusdata.
Average Death Rates State vs. County by Substance, 2007-2011
02468
101214
Total
All Opio
id
Heroin
Rx Opio
id
Cocain
e
Met
hadone
Alcohol
Oxyco
done
Benzo
Fenta
nyl
Tram
adol
Substance
Rat
e p
er 1
00,0
00 p
-yrs
State
County
Figure1:Averagedeathrateper100,000personyearsbysubstanceStateofMarylandvs.AnneArundelCounty InFigure2weobservethatdeathsfromheroinandprescriptionopioidscontributedroughlyequallytotheoveralloverdosedeathrateinAnneArundelCounty.
Anne Arundel County Intoxication Deaths by Year and Type
0
2
4
6
8
10
12
14
16
2007 2008 2009 2010 2011
Rat
e p
er 1
00,0
00
Total
All Opioid
Heroin
Rx Opioid
Methadone
Figure2:RateofIntoxicationdeathsinAnneArundelCountybytypeofsubstanceimplicatedandyearfrom2007‐2011.
WecancurrentlyutilizeESSENCEtoevaluate“chiefcomplaints”foremergencydepartment(ED)visitsdatingbacktolate2009.SearchingESSENCEfor“overdose”or“drugabuse”chiefcomplaintswillyieldbothintentionalandunintentionaloverdosepatientspresentingtotheED.Unfortunately,atthistimeitisdifficulttostratifytheseresultsbytypeofdrugabused.Lookingatthedatafrom2009‐present,itappearsthat
AnneArundelCountyOverdosePreventionPlan June2013
5
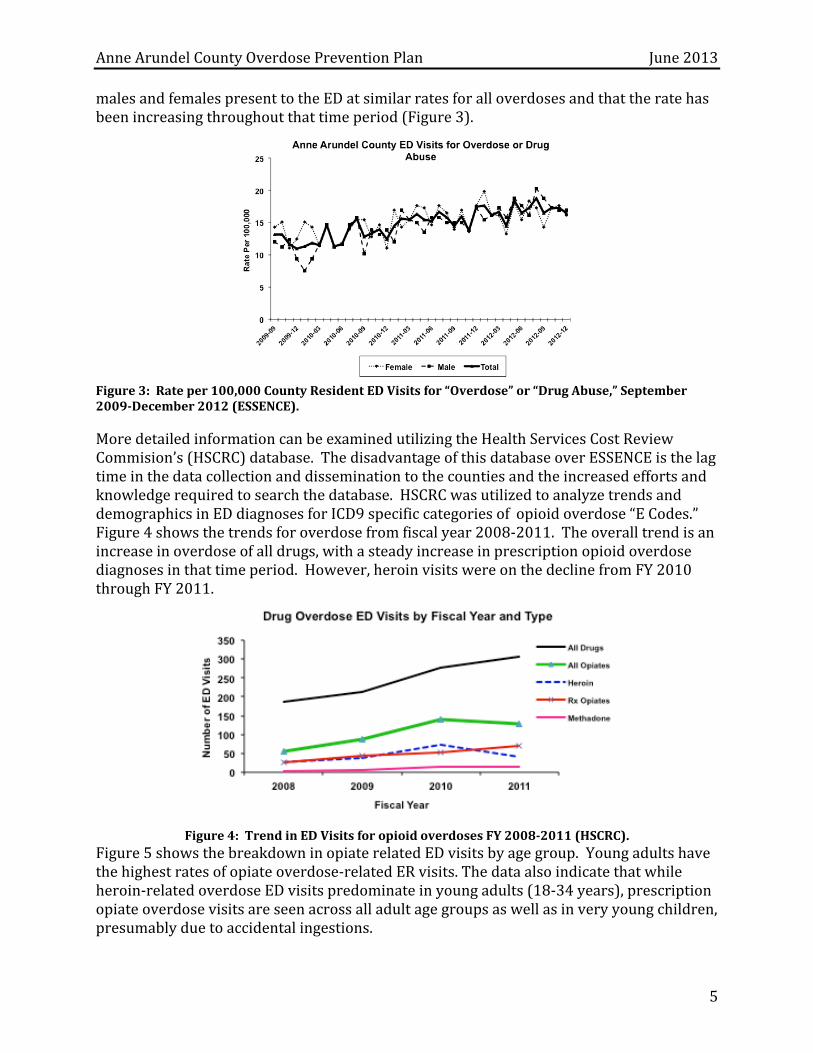
malesandfemalespresenttotheEDatsimilarratesforalloverdosesandthattheratehasbeenincreasingthroughoutthattimeperiod(Figure3).
Figure3:Rateper100,000CountyResidentEDVisitsfor“Overdose”or“DrugAbuse,”September2009‐December2012(ESSENCE). MoredetailedinformationcanbeexaminedutilizingtheHealthServicesCostReviewCommision’s(HSCRC)database.ThedisadvantageofthisdatabaseoverESSENCEisthelagtimeinthedatacollectionanddisseminationtothecountiesandtheincreasedeffortsandknowledgerequiredtosearchthedatabase.HSCRCwasutilizedtoanalyzetrendsanddemographicsinEDdiagnosesforICD9specificcategoriesofopioidoverdose“ECodes.”Figure4showsthetrendsforoverdosefromfiscalyear2008‐2011.Theoveralltrendisanincreaseinoverdoseofalldrugs,withasteadyincreaseinprescriptionopioidoverdosediagnosesinthattimeperiod.However,heroinvisitswereonthedeclinefromFY2010throughFY2011.
Figure4:TrendinEDVisitsforopioidoverdosesFY2008‐2011(HSCRC).
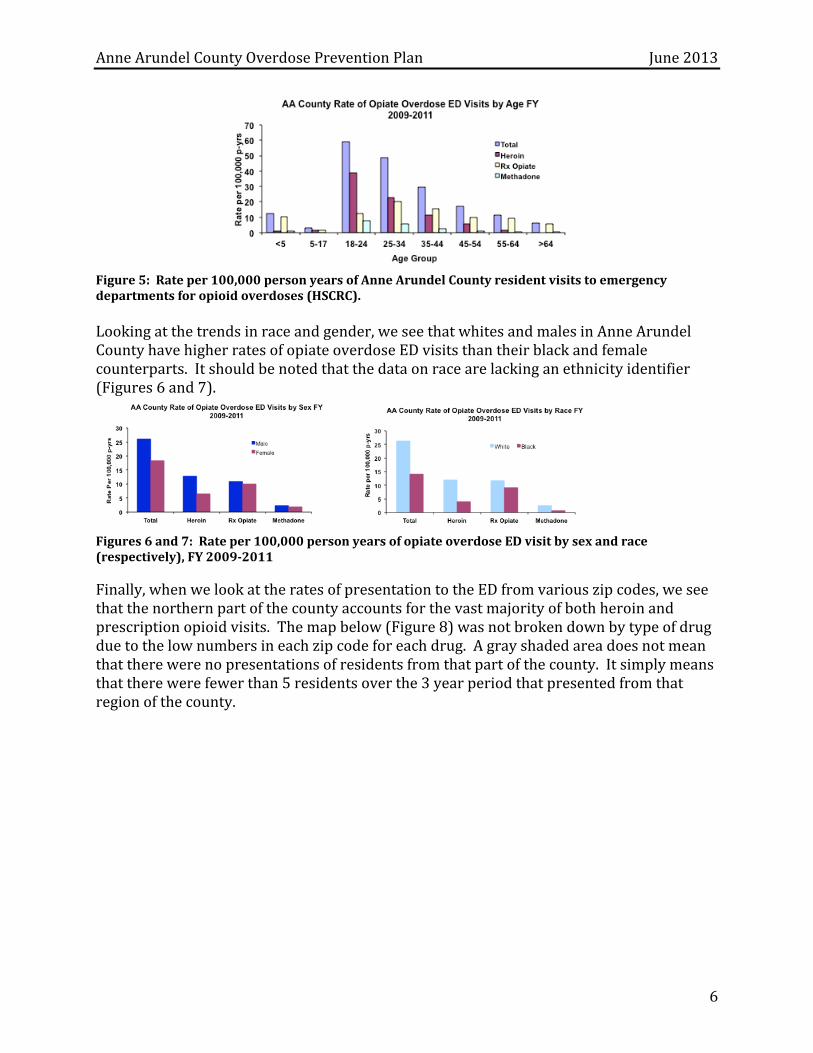
Figure5showsthebreakdowninopiaterelatedEDvisitsbyagegroup.Youngadultshavethehighestratesofopiateoverdose‐relatedERvisits.Thedataalsoindicatethatwhileheroin‐relatedoverdoseEDvisitspredominateinyoungadults(18‐34years),prescriptionopiateoverdosevisitsareseenacrossalladultagegroupsaswellasinveryyoungchildren,presumablyduetoaccidentalingestions.
AnneArundelCountyOverdosePreventionPlan June2013
6
Figure5:Rateper100,000personyearsofAnneArundelCountyresidentvisitstoemergencydepartmentsforopioidoverdoses(HSCRC). Lookingatthetrendsinraceandgender,weseethatwhitesandmalesinAnneArundelCountyhavehigherratesofopiateoverdoseEDvisitsthantheirblackandfemalecounterparts.Itshouldbenotedthatthedataonracearelackinganethnicityidentifier(Figures6and7).
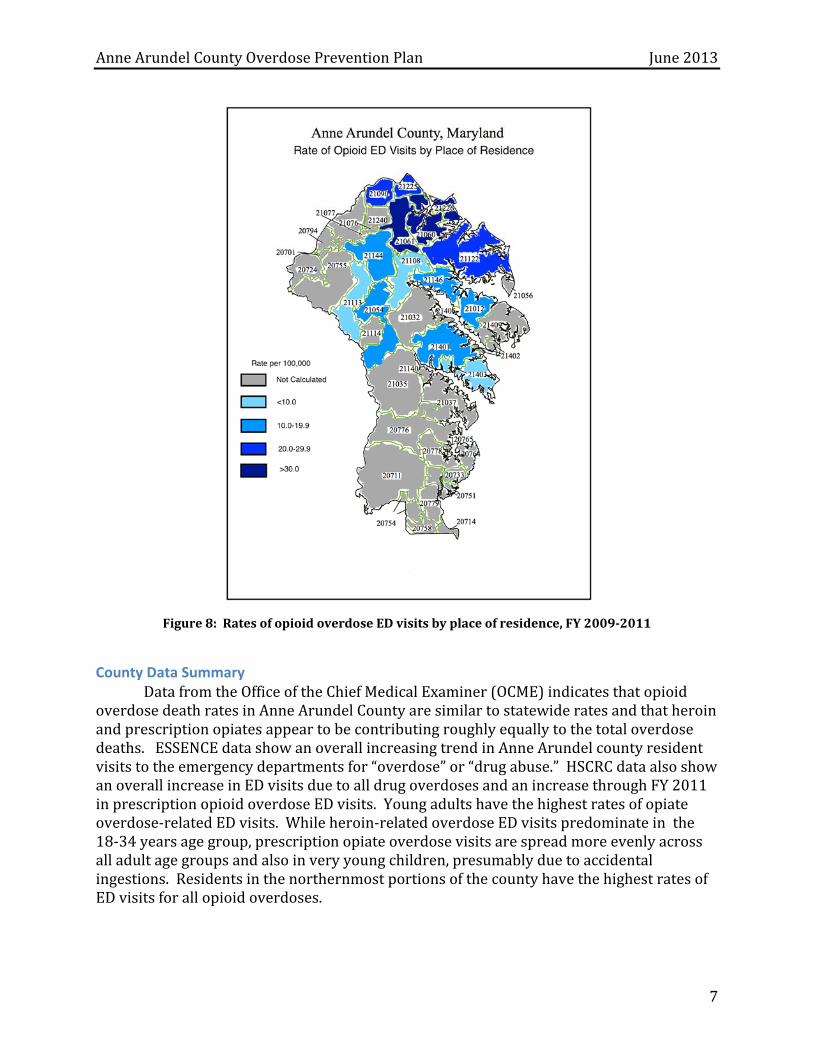
Figures6and7:Rateper100,000personyearsofopiateoverdoseEDvisitbysexandrace(respectively),FY2009‐2011 Finally,whenwelookattheratesofpresentationtotheEDfromvariouszipcodes,weseethatthenorthernpartofthecountyaccountsforthevastmajorityofbothheroinandprescriptionopioidvisits.Themapbelow(Figure8)wasnotbrokendownbytypeofdrugduetothelownumbersineachzipcodeforeachdrug.Agrayshadedareadoesnotmeanthattherewerenopresentationsofresidentsfromthatpartofthecounty.Itsimplymeansthattherewerefewerthan5residentsoverthe3yearperiodthatpresentedfromthatregionofthecounty.
AnneArundelCountyOverdosePreventionPlan June2013
7
Figure8:RatesofopioidoverdoseEDvisitsbyplaceofresidence,FY2009‐2011
County Data Summary DatafromtheOfficeoftheChiefMedicalExaminer(OCME)indicatesthatopioidoverdosedeathratesinAnneArundelCountyaresimilartostatewideratesandthatheroinandprescriptionopiatesappeartobecontributingroughlyequallytothetotaloverdosedeaths.ESSENCEdatashowanoverallincreasingtrendinAnneArundelcountyresidentvisitstotheemergencydepartmentsfor“overdose”or“drugabuse.”HSCRCdataalsoshowanoverallincreaseinEDvisitsduetoalldrugoverdosesandanincreasethroughFY2011inprescriptionopioidoverdoseEDvisits.Youngadultshavethehighestratesofopiateoverdose‐relatedEDvisits.Whileheroin‐relatedoverdoseEDvisitspredominateinthe18‐34yearsagegroup,prescriptionopiateoverdosevisitsarespreadmoreevenlyacrossalladultagegroupsandalsoinveryyoungchildren,presumablyduetoaccidentalingestions.ResidentsinthenorthernmostportionsofthecountyhavethehighestratesofEDvisitsforallopioidoverdoses.
AnneArundelCountyOverdosePreventionPlan June2013
8
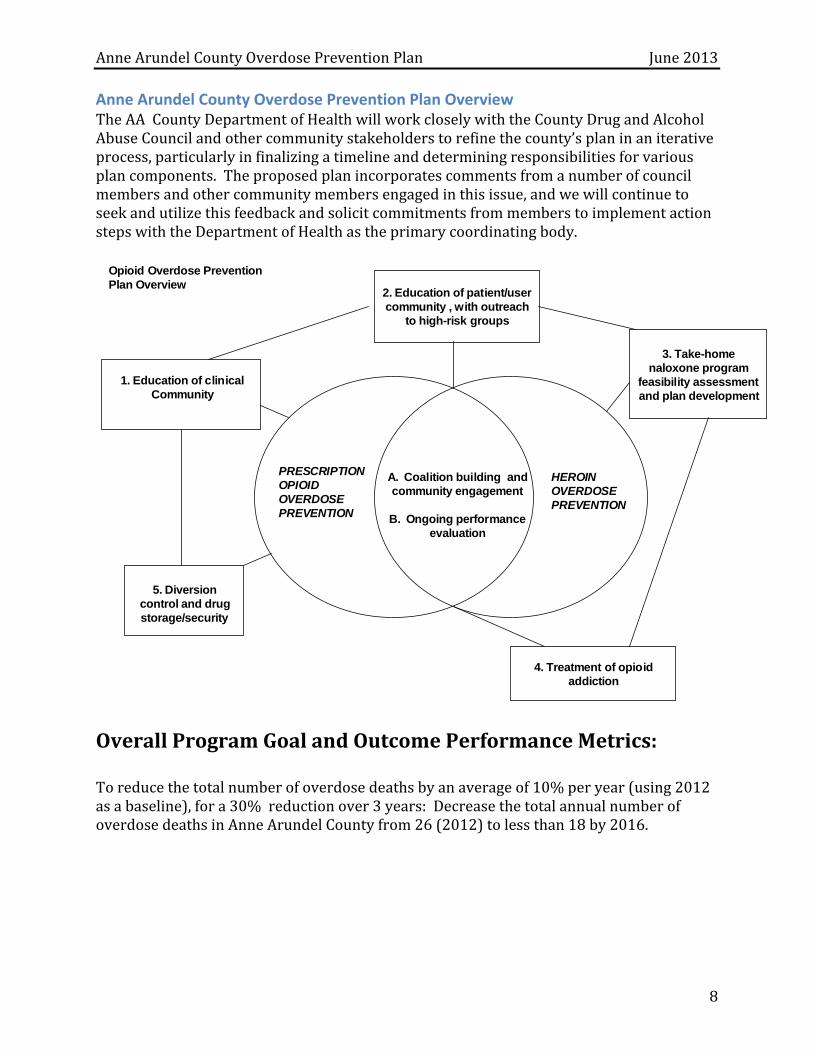
Anne Arundel County Overdose Prevention Plan Overview TheAACountyDepartmentofHealthwillworkcloselywiththeCountyDrugandAlcoholAbuseCouncilandothercommunitystakeholderstorefinethecounty’splaninaniterativeprocess,particularlyinfinalizingatimelineanddeterminingresponsibilitiesforvariousplancomponents.Theproposedplanincorporatescommentsfromanumberofcouncilmembersandothercommunitymembersengagedinthisissue,andwewillcontinuetoseekandutilizethisfeedbackandsolicitcommitmentsfrommemberstoimplementactionstepswiththeDepartmentofHealthastheprimarycoordinatingbody.
PRESCRIPTION OPIOID OVERDOSE PREVENTION
HEROIN OVERDOSE PREVENTION
3. Take-home naloxone program
feasibility assessment and plan development
4. Treatment of opioid addiction
5. Diversion control and drug storage/security
1. Education of clinical Community
2. Education of patient/user community , with outreach
to high-risk groups
A. Coalition building and community engagement
B. Ongoing performance
evaluation
Opioid Overdose Prevention Plan Overview
OverallProgramGoalandOutcomePerformanceMetrics:Toreducethetotalnumberofoverdosedeathsbyanaverageof10%peryear(using2012asabaseline),fora30%reductionover3years:DecreasethetotalannualnumberofoverdosedeathsinAnneArundelCountyfrom26(2012)tolessthan18by2016.
AnneArundelCountyOverdosePreventionPlan June2013
9
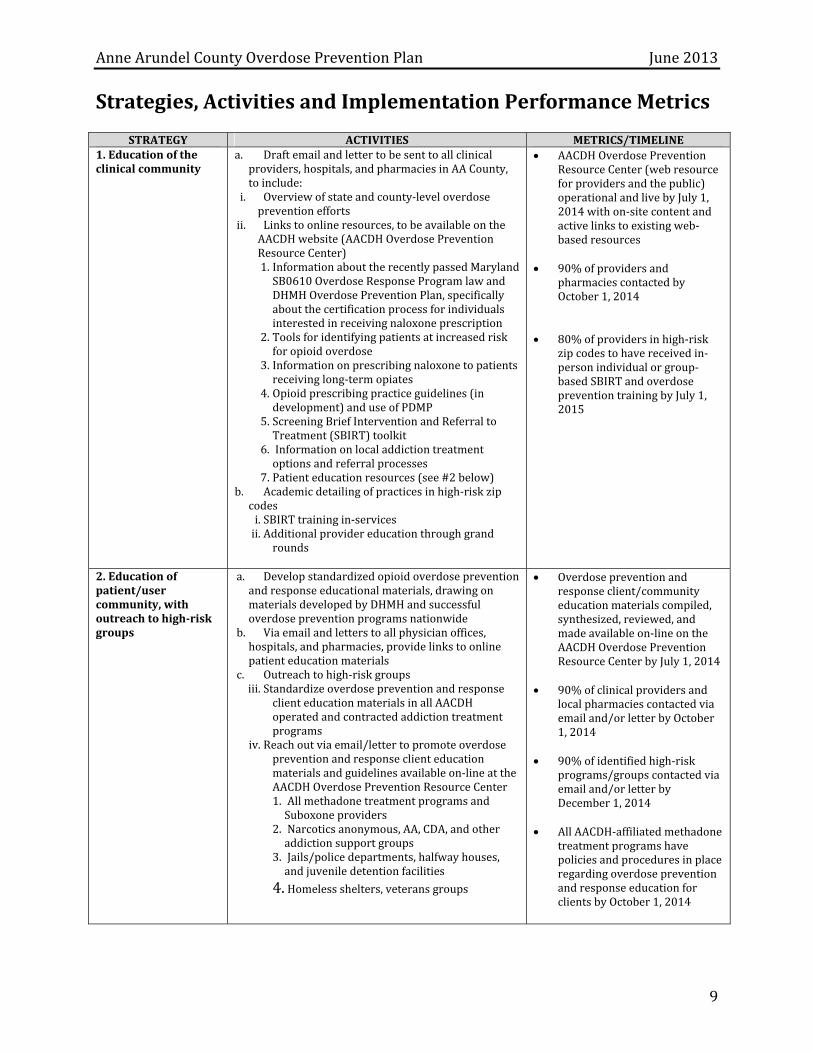
Strategies,ActivitiesandImplementationPerformanceMetrics
STRATEGY ACTIVITIES METRICS/TIMELINE1.Educationoftheclinicalcommunity
a. Draftemailandlettertobesenttoall clinicalproviders,hospitals,andpharmaciesinAACounty,toinclude:
i. Overviewofstateandcounty‐leveloverdosepreventionefforts
ii. Linkstoonlineresources,tobeavailableontheAACDHwebsite(AACDHOverdosePreventionResourceCenter)1. InformationabouttherecentlypassedMarylandSB0610OverdoseResponseProgramlawandDHMHOverdosePreventionPlan,specificallyaboutthecertificationprocessforindividualsinterestedinreceivingnaloxoneprescription
2. Toolsforidentifyingpatientsatincreasedriskforopioidoverdose
3. Informationonprescribingnaloxonetopatientsreceivinglong‐termopiates
4. Opioidprescribingpracticeguidelines(indevelopment)anduseofPDMP
5. ScreeningBriefInterventionandReferraltoTreatment(SBIRT)toolkit
6. Informationonlocaladdictiontreatmentoptionsandreferralprocesses
7. Patienteducationresources(see#2below)b. Academicdetailingofpracticesinhigh‐riskzipcodesi. SBIRTtrainingin‐servicesii. Additionalprovidereducationthroughgrand
rounds
AACDHOverdosePreventionResourceCenter(webresourceforprovidersandthepublic)operationalandlivebyJuly1,2014withon‐sitecontentandactivelinkstoexistingweb‐basedresources
90%ofprovidersand
pharmaciescontactedbyOctober1,2014
80%ofprovidersinhigh‐risk
zipcodestohavereceivedin‐personindividualorgroup‐basedSBIRTandoverdosepreventiontrainingbyJuly1,2015
2.Educationofpatient/usercommunity,withoutreachtohigh‐riskgroups
a. Developstandardizedopioidoverdosepreventionandresponseeducationalmaterials,drawingonmaterialsdevelopedbyDHMHandsuccessfuloverdosepreventionprogramsnationwide
b. Viaemailandletterstoallphysicianoffices,hospitals,andpharmacies,providelinkstoonlinepatienteducationmaterials
c. Outreachtohigh‐riskgroupsiii. Standardizeoverdosepreventionandresponse
clienteducationmaterialsinallAACDHoperatedandcontractedaddictiontreatmentprograms
iv. Reachoutviaemail/lettertopromoteoverdosepreventionandresponseclienteducationmaterialsandguidelinesavailableon‐lineattheAACDHOverdosePreventionResourceCenter1. AllmethadonetreatmentprogramsandSuboxoneproviders
2. Narcoticsanonymous,AA,CDA,andotheraddictionsupportgroups
3. Jails/policedepartments,halfwayhouses,andjuveniledetentionfacilities
4. Homelessshelters,veteransgroups
Overdosepreventionandresponseclient/communityeducationmaterialscompiled,synthesized,reviewed,andmadeavailableon‐lineontheAACDHOverdosePreventionResourceCenterbyJuly1,2014
90%ofclinicalprovidersand
localpharmaciescontactedviaemailand/orletterbyOctober1,2014
90%ofidentifiedhigh‐risk
programs/groupscontactedviaemailand/orletterbyDecember1,2014
AllAACDH‐affiliatedmethadone
treatmentprogramshavepoliciesandproceduresinplaceregardingoverdosepreventionandresponseeducationforclientsbyOctober1,2014
AnneArundelCountyOverdosePreventionPlan June2013
10
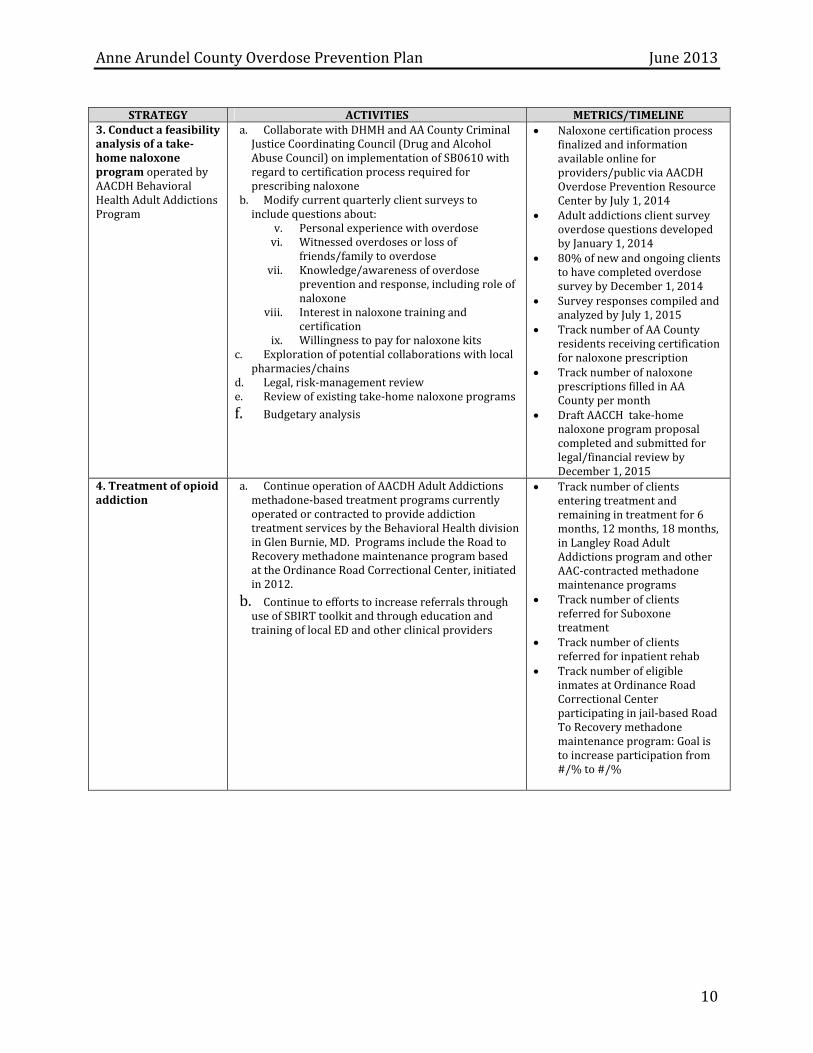
STRATEGY ACTIVITIES METRICS/TIMELINE
3.Conductafeasibilityanalysisofatake‐homenaloxoneprogramoperatedbyAACDHBehavioralHealthAdultAddictionsProgram
a. CollaboratewithDHMHandAACountyCriminalJusticeCoordinatingCouncil(DrugandAlcoholAbuseCouncil)onimplementationofSB0610withregardtocertificationprocessrequiredforprescribingnaloxone
b. Modifycurrentquarterlyclientsurveystoincludequestionsabout:
v. Personalexperiencewithoverdosevi. Witnessedoverdosesorlossof
friends/familytooverdosevii. Knowledge/awarenessofoverdose
preventionandresponse,includingroleofnaloxone
viii. Interestinnaloxonetrainingandcertification
ix. Willingnesstopayfornaloxonekitsc. Explorationofpotentialcollaborationswithlocal
pharmacies/chainsd. Legal,risk‐managementreviewe. Reviewofexistingtake‐homenaloxoneprograms
f. Budgetaryanalysis
Naloxonecertificationprocessfinalizedandinformationavailableonlineforproviders/publicviaAACDHOverdosePreventionResourceCenterbyJuly1,2014
AdultaddictionsclientsurveyoverdosequestionsdevelopedbyJanuary1,2014
80%ofnewandongoingclientstohavecompletedoverdosesurveybyDecember1,2014
SurveyresponsescompiledandanalyzedbyJuly1,2015
TracknumberofAACountyresidentsreceivingcertificationfornaloxoneprescription
TracknumberofnaloxoneprescriptionsfilledinAACountypermonth
DraftAACCHtake‐homenaloxoneprogramproposalcompletedandsubmittedforlegal/financialreviewbyDecember1,2015
4.Treatmentofopioidaddiction
a. ContinueoperationofAACDHAdultAddictionsmethadone‐basedtreatmentprogramscurrentlyoperatedorcontractedtoprovideaddictiontreatmentservicesbytheBehavioralHealthdivisioninGlenBurnie,MD.ProgramsincludetheRoadtoRecoverymethadonemaintenanceprogrambasedattheOrdinanceRoadCorrectionalCenter,initiatedin2012.
b. ContinuetoeffortstoincreasereferralsthroughuseofSBIRTtoolkitandthrougheducationandtrainingoflocalEDandotherclinicalproviders
Tracknumberofclientsenteringtreatmentandremainingintreatmentfor6months,12months,18months,inLangleyRoadAdultAddictionsprogramandotherAAC‐contractedmethadonemaintenanceprograms
TracknumberofclientsreferredforSuboxonetreatment
Tracknumberofclientsreferredforinpatientrehab
TracknumberofeligibleinmatesatOrdinanceRoadCorrectionalCenterparticipatinginjail‐basedRoadToRecoverymethadonemaintenanceprogram:Goalistoincreaseparticipationfrom#/%to#/%
AnneArundelCountyOverdosePreventionPlan June2013
11
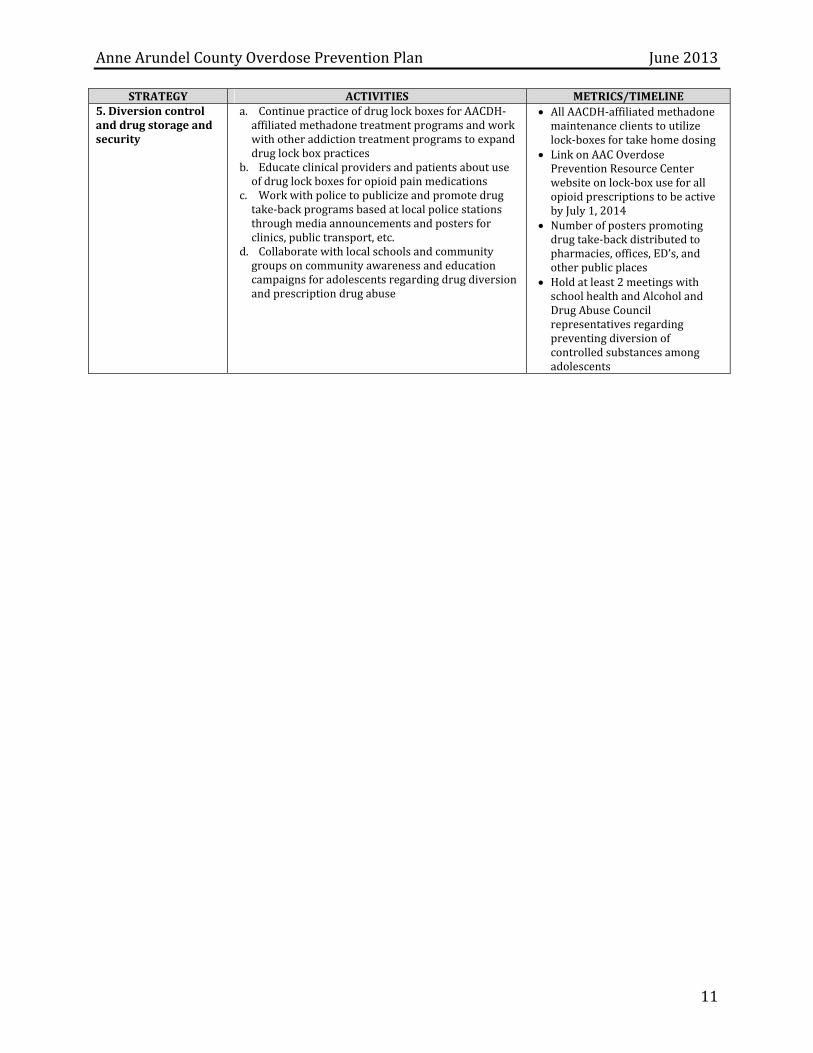
STRATEGY ACTIVITIES METRICS/TIMELINE5.Diversioncontrolanddrugstorageandsecurity
a. ContinuepracticeofdruglockboxesforAACDH‐affiliatedmethadonetreatmentprogramsandworkwithotheraddictiontreatmentprogramstoexpanddruglockboxpractices
b. Educateclinicalprovidersandpatientsaboutuseofdruglockboxesforopioidpainmedications
c. Workwithpolicetopublicizeandpromotedrugtake‐backprogramsbasedatlocalpolicestationsthroughmediaannouncementsandpostersforclinics,publictransport,etc.
d. Collaboratewithlocalschoolsandcommunitygroupsoncommunityawarenessandeducationcampaignsforadolescentsregardingdrugdiversionandprescriptiondrugabuse
AllAACDH‐affiliatedmethadonemaintenanceclientstoutilizelock‐boxesfortakehomedosing
LinkonAACOverdosePreventionResourceCenterwebsiteonlock‐boxuseforallopioidprescriptionstobeactivebyJuly1,2014
Numberofposterspromotingdrugtake‐backdistributedtopharmacies,offices,ED’s,andotherpublicplaces
Holdatleast2meetingswithschoolhealthandAlcoholandDrugAbuseCouncilrepresentativesregardingpreventingdiversionofcontrolledsubstancesamongadolescents
AnneArundelCountyOverdosePreventionPlan June2013
12
References 1. CalcaterraS,GlanzJ,BinswangerIA.Nationaltrendsinpharmaceuticalopioid
relatedoverdosedeathscomparedtoothersubstancerelatedoverdosedeaths:1999‐2009.DrugAlcoholDepend.Jan42013.
2. DarkeS,HallW.Thedistributionofnaloxonetoheroinusers.Addiction.Sep1997;92(9):1195‐1199.
3. ShermanSG,ChengY,KralAH.PrevalenceandcorrelatesofopiateoverdoseamongyounginjectiondrugusersinalargeU.S.city.DrugAlcoholDepend.May112007;88(2‐3):182‐187.
4. PJD,RLM,AHK,AAG,BRE,ARM.Fatalheroin‐relatedoverdoseinSanFrancisco,1997‐2000:acasefortargetedintervention.JournalofUrbanHealth.2003;80(2):261‐273.
5. MerrallEL,KariminiaA,BinswangerIA,etal.Meta‐analysisofdrug‐relateddeathssoonafterreleasefromprison.Addiction.Sep2010;105(9):1545‐1554.
6. Community‐basedopioidoverdosepreventionprogramsprovidingnaloxone‐UnitedStates,2010.MMWRMorbMortalWklyRep.Feb172012;61(6):101‐105.
7. WalleyAY.BystanderoverdoseeducationandnaloxonedistributioninMassachusetts.Paperpresentedat:RoleofNaloxoneinOpioidOverdoseFatalityPrevention;12April,2012;SilverSpring,MD.
8. BennettAS,BellA,TomediL,HulseyEG,KralAH.Characteristicsofanoverdoseprevention,response,andnaloxonedistributionprograminPittsburghandAlleghenyCounty,Pennsylvania.JUrbanHealth.Dec2011;88(6):1020‐1030.
9. LankenauSE,WagnerKD,SilvaK,etal.InjectionDrugUsersTrainedbyOverdosePreventionPrograms:ResponsestoWitnessedOverdoses.JCommunityHealth.Jul312012.
AnneArundelCountyOverdosePreventionPlan June2013
13
Acknowledgements CompilationandTechnicalAssistanceProvidedby:
JanaMcAninch,MD,MPH.,MS
TammyServies,MD
SpecialthankstotheOverdosePreventionPlanningCommittee:
JinleneChan,MD,MPH,AnneArundelCountyDepartmentofHealth
WilliamRufenacht,MA,LCADC,AnneArundelCountyDepartmentofHealth
SandraO’Neill,LCPC,AnneArundelCountyDepartmentofHealth
BarbaraHatch,RN,AnneArundelCountyDepartmentofHealth
HildrethClagett,NCC,AnneArundelCountyDepartmentofHealth
BabakImanoel,DO,AnneArundelCountyDepartmentofHealth
HeatherEshleman,CPP,CHES,MPH,AnneArundelCountyDepartmentofHealth
ArleneHall,RN,MSN,CARN,BaltimoreWashingtonMedicalCenter
LeighRagan,LCADC,FirstStepRecoveryCenter
HelenReines,BA,RN,PathwaysatAnneArundelMedicalCenter
ShirleyKnelly,MS,CPHQ,LCADC,PathwaysatAnneArundelMedicalCenter





























