Embed Size (px)
Citation preview
Annalisa Busetta, Valeria Cetorelli, and Ben Wilson
A universal health care system? Unmet need for medical care among regular and irregular immigrants in Italy Article (Accepted version) (Refereed)
Original citation: Busetta, Annalisa, Cetorelli, Valeria and Wilson, Ben (2017) A universal health care system? Unmet need for medical care among regular and irregular immigrants in Italy. Journal of Immigrant and Minority Health. ISSN 1557-1912 DOI: 10.1007/s10903-017-0566-8 © 2017 Springer Science+Business Media This version available at: http://eprints.lse.ac.uk/69876/ Available in LSE Research Online: March 2017 LSE has developed LSE Research Online so that users may access research output of the School. Copyright © and Moral Rights for the papers on this site are retained by the individual authors and/or other copyright owners. Users may download and/or print one copy of any article(s) in LSE Research Online to facilitate their private study or for non-commercial research. You may not engage in further distribution of the material or use it for any profit-making activities or any commercial gain. You may freely distribute the URL (http://eprints.lse.ac.uk) of the LSE Research Online website. This document is the author’s final accepted version of the journal article. There may be differences between this version and the published version. You are advised to consult the publisher’s version if you wish to cite from it.

A universal health care system? Unmet need for medical care
among regular and irregular immigrants in Italy
Annalisa Busetta1, Valeria Cetorelli2 and Ben Wilson3,4
Abstract
Italy has a universal health care system that covers, in principle, the whole resident population,
irrespective of citizenship and legal status. This study calculates the prevalence of unmet need for
medical care among Italian citizens, regular and irregular immigrants and estimates logistic regression
models to assess whether differences by citizenship and legal status hold true once adjusting for
potential confounders. The analysis is based on two Surveys on Income and Living Conditions of
Italian households and households with foreigners. Controlling for various factors, the odds of
experiencing unmet need for medical care are 27% higher for regular immigrants than for Italian
citizens and 59% higher for irregular immigrants. The gaps by citizenship and legal status are even
more striking among those with chronic illnesses. These results reveal the high vulnerability of
immigrants in Italy and the need to develop more effective policies to achieve health care access for
all residents.
Keywords: unmet need; health care access; immigrants; legal status; Italy
Affiliations:
1. Department of Economics, Business and Statistics (SEAS), University of Palermo, Palermo, Italy
2. Department of International Health, Johns Hopkins Bloomberg School of Public Health,
Baltimore, USA
3. Stockholm University Demography Unit (SUDA), Department of Sociology, Stockholm
University, Stockholm, Sweden
4. Department of Methodology, London School of Economics, London, UK
Corresponding author:
Annalisa Busetta
Dept. of Economics, Business and Statistics (SEAS)
University of Palermo
address: Viale delle scienze, ed. 13
zip: 90128, Palermo, Italy
e-mail: [email protected]

Introduction
The Italian public universal health care system covers - in principle - the whole resident population,
irrespective of citizenship and legal status. As such, it is classified as one of the most inclusive health
care systems in Europe [1-3]. Health as a right for all is explicitly recognised in article 32 of the Italian
Constitution, according to which “The Republic safeguards health as a fundamental right of the
individual and as a collective interest, and guarantees free medical care to the indigent”.
Despite this fact, there are significant inequalities in access to medical care. There is a higher
prevalence of unmet need for medical care for those who have a low income [4], and geographical
disparities in access to medical care have been exacerbated in the last two decades by the progressive
decentralisation of health services to regional administrations [5].
Inequality in access to medical care between citizens and immigrants is a phenomenon of
growing importance in Italy [6-9]. Immigrants seem to experience specific barriers to medical care,
which are in addition to existing economic and geographical inequalities [10]. Some studies have
argued that social class is the underlying determinant of this inequality [6], while others have
contended that ethnic discrimination compounds economic deprivation [7,11]. The concept of social
capital has also been used in explaining immigrants’ additional obstacles to accessing medical care
compared to the Italian population [12]. Lack of knowledge about national laws and administrative
regulations may limit immigrants’ ability to access health services, while language difficulties and
cultural factors may also represent serious barriers to access [13,14].
Unmet need for medical care may be related to socio-demographic characteristics and health
profiles. The international literature has shown that after an initial “healthy immigrant effect” - owing
to a self-selection process prior to migration - immigrants’ health tends to deteriorate with the time
spent in the host country, and this results in an increased need for medical care [15-17]. The worsening
health conditions after resettlements have been attributed to health-impairing work environments,
inadequate salaries, poor housing, as well as real and perceived social exclusion [18]. This is
increasingly the case in Italy, where the health profiles of immigrants have significantly deteriorated
over the last decade [19].
Little is known, however, about the links between health care access and legal immigration
status. Immigrants in an irregular situation - i.e. those who do not fulfil conditions for entry or stay in
the country - constitute a particularly vulnerable group because they are more likely to be subjected to
exploitative working conditions and precarious housing [2]. Typically, they are also fearful that their
irregular status could be reported to the migration authorities, are largely unaware of their rights, and
often suffer from hostile and discriminatory attitudes [2]. The health of irregular immigrants is of
particular concern with respect to chronic illnesses such as respiratory disease, high blood pressure,
cardiovascular disease, diabetes, and cancer, as well as health problems arising from hard

living/working conditions, unhealthy lifestyles, and a lack of adequate access to preventive care.
Furthermore, their precarious situation makes continuity of care especially difficult [2].
To date no study has been carried out to quantify the extent of unmet need for medical care in
Italy by legal status. The present paper fills this knowledge gap and contributes to the growing body of
research on health inequities by assessing differences in unmet need for medical care between Italian
citizens, regular and irregular immigrants. The aim is to show whether differences exist, and whether
they remain after adjusting for socio-demographic characteristics, subjective health, poverty measures,
and geographical residence. We also examine whether the differential unmet need by legal status
widens in case of chronic illnesses that require long-term continuous care, and the extent to which our
findings are different for male and female immigrants. The importance of our results is not limited to
the Italian context as they provide useful insights for the health protection of regular and irregular
immigrants in other European countries who, like Italy, are currently experiencing sustained
immigration flows, including the onward flow of non-Italian immigrants from Italy.
Methods
This study is based on merged data from the 2009 standard Italian Survey on Income and Living
Conditions (SILC) and the 2009 special Italian Survey on Income and Living Conditions of
households with foreigners. Both surveys were conducted by the Italian National Institute for Statistics
(Istat), they used the same methodological tools (questionnaires, survey techniques, methods of
correction, imputation and integration of data, etc.), covered the same time period, and interviewed all
individuals aged 16 and over living in the selected households.
The standard Italian SILC was carried out on individuals living in about 26,000 households
selected with a standard two-stage stratified sampling design typically used by Istat in face-to-face
household surveys representative of the Italian population [20]. The special SILC is the largest survey
of the immigrant population ever conducted in Italy, covering over 6,000 households with at least one
foreign member. The sampling techniques took into account the size of different foreign-national
groups and their geographical distribution across the country [21]. All interviewees were asked about
their legal status; those who reported no regular resident permit constituted more than 17% of the
sample. As asserted by Istat, the sample of households with at least one foreigner members from the
special SILC survey is comparable with that of households made up exclusively of Italians from the
standard SILC survey.
Besides collecting a wide range of socio-demographic and economic variables, both surveys
included a series of questions about health. Unmet need for medical care was assessed using the
following question: “During the last 12 months, was there ever a time when you felt you needed a
medical examination or treatment for a health problem but you did not receive it?”. Interviewees who
replied affirmatively were considered to have experienced unmet need.

Our analytical sample includes 43,636 Italian citizens, 8,133 immigrants with a regular
resident permit, and 1,704 immigrants who are classified as irregular. This classification is based on a
question which asks immigrants whether they have a residence permit or a visa. The question includes
different response options to account for the variation in residence requirements for different
immigrant groups. All non-EU foreigners require a resident permit or a visa to reside in Italy
regularly, and although EU foreigners can circulate in Italy without any restriction, they are also
required to register their residence if they stay in Italy for more than 3 months. In order to be classified
as ‘regular’ in our analysis, this implies (in almost all cases) that immigrants either have a job, are
studying full-time, are a legal partner of a legal resident, or can demonstrate that they have enough
money to qualify for health insurance.
We calculate the prevalence of unmet need for medical care separately for Italian citizens,
regular and irregular immigrants. Next, we estimate logistic regression models to assess whether
differences by legal status hold true after controlling for potential confounders such as sex, age,
education, labour force participation, self-assessed health, and self-rated poverty. A regional variable
is also included to account for geographical disparities in supply and quality of health services. We run
the analysis on the whole sample and on the sub-sample of those who reported suffering from chronic
illnesses. We conclude by repeating the analysis separately for male and female immigrants, excluding
citizens, which shows how the differential in unmet need for medical care varies by sex when
comparing regular and irregular immigrants.
Results
Overall, around 7% of individuals in the sample reported to have experienced unmet need for medical
care during the last 12 months. Differences by legal status are notable: the prevalence of unmet need is
7% among Italian citizens, 8% among regular immigrants, and 11% among irregular immigrants.
Unmet need for medical care is higher for the sub-sample with chronic illnesses, and differences by
legal status are more substantial: the prevalence is 12% among Italian citizens, 20% among regular
immigrants and 32% among irregular immigrants (see figure 1).
Table 1 shows the results from two logistic regression models for the association between
legal status and the odds of experiencing unmet need for medical care. Model 1 refers to the whole
sample, and Model 2 only to the sub-sample of those suffering from chronic illnesses. Both models
control for self-rated health, self-assessed poverty, socio-demographic characteristics, and region of
residence.
After adjusting for potential confounders, there are still significant differences in access to
healthcare by legal status. For both regular and irregular immigrants, the odds of having unmet need
for medical care are significantly higher than Italian citizens, and the size of this differential is even
higher for those with chronic illness.
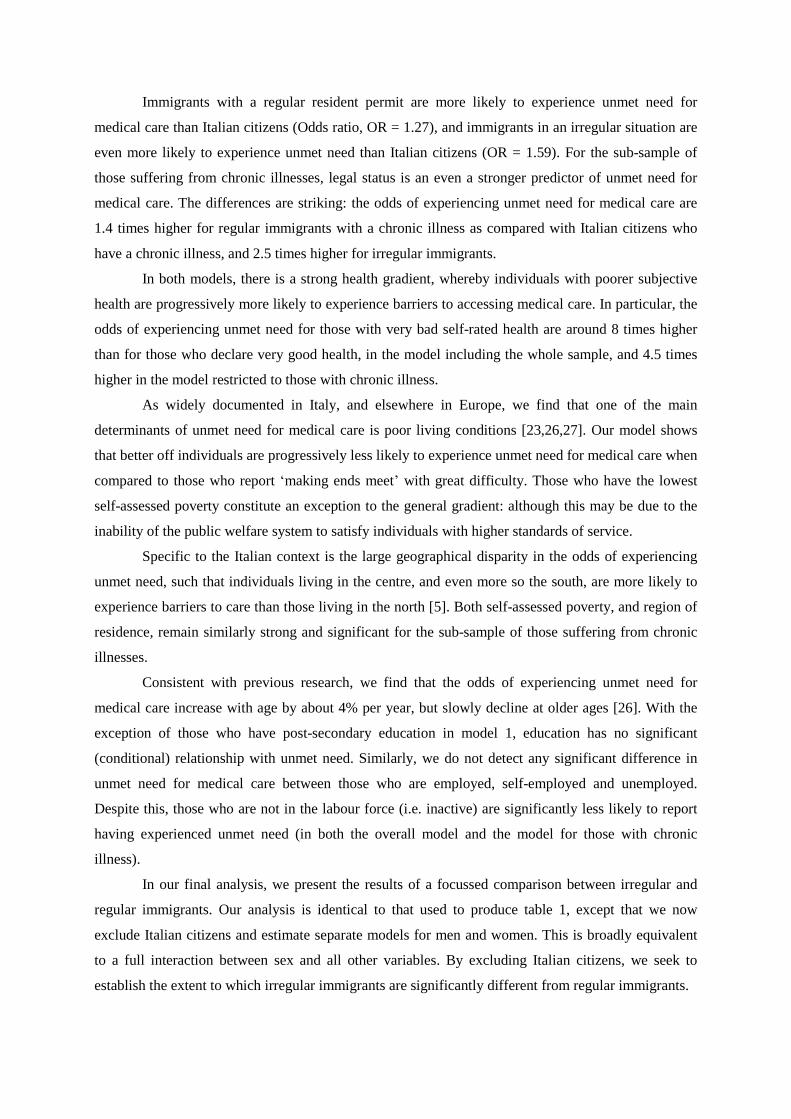
Immigrants with a regular resident permit are more likely to experience unmet need for
medical care than Italian citizens (Odds ratio, OR = 1.27), and immigrants in an irregular situation are
even more likely to experience unmet need than Italian citizens (OR = 1.59). For the sub-sample of
those suffering from chronic illnesses, legal status is an even a stronger predictor of unmet need for
medical care. The differences are striking: the odds of experiencing unmet need for medical care are
1.4 times higher for regular immigrants with a chronic illness as compared with Italian citizens who
have a chronic illness, and 2.5 times higher for irregular immigrants.
In both models, there is a strong health gradient, whereby individuals with poorer subjective
health are progressively more likely to experience barriers to accessing medical care. In particular, the
odds of experiencing unmet need for those with very bad self-rated health are around 8 times higher
than for those who declare very good health, in the model including the whole sample, and 4.5 times
higher in the model restricted to those with chronic illness.
As widely documented in Italy, and elsewhere in Europe, we find that one of the main
determinants of unmet need for medical care is poor living conditions [23,26,27]. Our model shows
that better off individuals are progressively less likely to experience unmet need for medical care when
compared to those who report ‘making ends meet’ with great difficulty. Those who have the lowest
self-assessed poverty constitute an exception to the general gradient: although this may be due to the
inability of the public welfare system to satisfy individuals with higher standards of service.
Specific to the Italian context is the large geographical disparity in the odds of experiencing
unmet need, such that individuals living in the centre, and even more so the south, are more likely to
experience barriers to care than those living in the north [5]. Both self-assessed poverty, and region of
residence, remain similarly strong and significant for the sub-sample of those suffering from chronic
illnesses.
Consistent with previous research, we find that the odds of experiencing unmet need for
medical care increase with age by about 4% per year, but slowly decline at older ages [26]. With the
exception of those who have post-secondary education in model 1, education has no significant
(conditional) relationship with unmet need. Similarly, we do not detect any significant difference in
unmet need for medical care between those who are employed, self-employed and unemployed.
Despite this, those who are not in the labour force (i.e. inactive) are significantly less likely to report
having experienced unmet need (in both the overall model and the model for those with chronic
illness).
In our final analysis, we present the results of a focussed comparison between irregular and
regular immigrants. Our analysis is identical to that used to produce table 1, except that we now
exclude Italian citizens and estimate separate models for men and women. This is broadly equivalent
to a full interaction between sex and all other variables. By excluding Italian citizens, we seek to
establish the extent to which irregular immigrants are significantly different from regular immigrants.

The results show that there is a significantly higher unmet need for medical care for irregular
male (versus regular male) immigrants, and that the same is true for females, although to a lesser
extent (see figure 2). For the sub-samples with chronic illness, this difference between men and
women is exacerbated, such that the odds of unmet need are 3 times higher (and significant) for
irregular male immigrants, as compared with regular males. This is in contrast to females with chronic
illness, where the odds ratio is smaller and non-significant.
Discussion
Health as a right for all is a core objective of the Italian public universal health care system. Despite
this, many individuals in Italy experience barriers to accessing medical care due to unaffordability and
unavailability of health services [4,5]. The situation is especially challenging for immigrants, who
often lack knowledge of national laws and administrative regulations, tend to experience cultural and
language difficulties, and suffer from precarious living conditions and social exclusion [2,13,14].
In this paper, we focus on differences in unmet need for medical care between citizens, regular
and irregular immigrants in Italy. Our analysis documents that, other things being equal, there are
considerable disparities in access to care not only between citizens and non-citizens, but also between
regular and irregular immigrants.
Compared to Italian citizens the odds of experiencing unmet need are greater for regular and
irregular immigrants, and these gaps are even more striking for the sub-sample of those suffering from
chronic health conditions. Research in Italy and elsewhere in Europe suggests that chronic illnesses
are becoming a serious concern for both the immigrant and native populations. Our results show that
regular and irregular immigrants with chronic illnesses are much more likely to experience unmet
need for medical care than Italian citizens with similar conditions.
Our results also demonstrate the importance of sex for understanding immigrant inequalities
in unmet need. Table 1 shows that there is a significant gender gap in unmet need for medical care,
with women being more likely to experience barriers accessing care than men. A similar gender gap
has been noted in both public and private health care systems [24,25]. But after excluding Italian
citizens, and making direct comparison between irregular and regular immigrants, the direction of this
association is reversed. Irregular female immigrants are less likely than men to experience unmet
need, especially if they have a chronic illness. One implication of this finding is that policies to reduce
the unmet need for medical care among immigrants must take account of differences between men and
women, and may even benefit from targeting men.
It is important to highlight that our analysis has some limitations due to data availability. First,
the use of the Survey of Income and Living Conditions of households with foreigners (i.e. individuals
living in households with at least one foreign member from population register) means that irregular
immigrants are included in the sample if and only if they live with someone that is in the population
register. This implies the exclusion of some immigrants who have an irregular migration status, in

particular those who are living in camps, are homeless, or have no stable residence. Given that these
immigrants may be even more marginalised than those in our study, we may in fact be
underestimating unmet need. On the other hand, some immigrants will acquire Italian citizenship by
naturalization, or by marriage to an Italian citizen, and if they are less likely than other immigrants to
experience unmet need, then there may be a bias in the other direction.
Another limitation is the cross-sectional nature of the survey. Our cross-sectional data do not
allow for a proper measurement of health status and health access change over time. With these data, it
is not possible to verify if immigrants’ health deteriorates with duration spent in Italy, and if their need
for medical care increases consequently. In particular, it is not possible to verify if immigrants develop
severe chronic illnesses because they lack adequate access to preventive health care services, or to
study other more complex aspects of health selection. Finally, although our data provide information
about immigrant origins and ages at arrival, the heterogeneity across these variables does not allow us
to measure the links between unmet need for medical care and membership of different immigration
cohorts.
Conclusion
This study has revealed the high vulnerability of immigrants in Italy, and the urgent need to develop
more effective policies if the goal of health for all is to be achieved. Culturally-sensitive interventions
should be adopted to promote knowledge about the right to health, in particular among irregular
immigrants. These policies must pay attention to differences between men and women, and in the case
of irregular immigrants with chronic illness, may need to target men. Interventions addressing the
difficult and health-impairing environments in which irregular immigrants often live and work are also
required. More general policies should be oriented towards assisting individuals with a high level of
self-perceived poverty, and towards expanding availability of health services in the central and
southern regions. Finally, more detailed studies on the most vulnerable groups of immigrants are
necessary. These include irregular or regular immigrants (especially asylum seekers and refugees) who
do not have access to medical care (neither general practitioner nor specialist consultations) and do not
have enough economic resources to buy medications at full price in pharmacies.
"Compliance with Ethical Standards"
Author A declares that she has no conflict of interest. Author B declares that she has no conflict of
interest. Author C declares that he has no conflict of interest.
This article does not contain any studies with human participants or animals performed by any of the
authors.
References
[1] Romero-Ortuno R. Access to health care for illegal immigrants in the EU: should we be
concerned? European Journal of Health Law 2004;11:245-272.
[2] European Union Agency for Fundamental Rights. Migrants in an irregular situation: access to
healthcare in 10 European Union Member States. Luxembourg: Publications Office of the European
Union 2011.
[3] Marceca M., Geraci S., Baglio G. Immigrants’ health protection: political, institutional and social
perspectives at international and Italian level. Italian Journal of Public Health 2012; 9(3):e7498-1-11.
[4] OECD. Unmet health care needs. Health at a Glance 2014: OECD Indicators. OECD Publishing
2014.
[5] Cavalieri M. Geographical variation of unmet medical needs in Italy: a multivariate logistic
regression analysis. International Journal of Health Geographics 2013;12:27.
[6] Tognetti, M. Health Inequalities: Access to Services by Immigrants in Italy. Open Journal of
Social Sciences 2015;8.
[7] Tognetti M., Bordogna, M. (Ed). Immigrazione e disuguaglianza di salute. Franco Angeli, Milan
2008.
[8] Nuti, S., Maciocco, G. and Barsani, S. (Eds.) Immigrazione e salute. Percorsi d’integrazione
sociale. Il Mulino, Bologna 2012.
[9] ISTAT. Sanità: Statistiche in breve, Salute e ricorso ai servizi sanitari della popolazione straniera
residente in Italia. 11 December 2008.
[10] Giannoni M. Migrants inequalities in unmet need for access to health care in Italy. Paper
presented at 15° Aies Conference–Moncalieri (TO) 2010.
[11] Marceca, M., Geraci, S. and Martino, A. Esperienza migratoria, salute e disuguaglianze.
Osservatorio Italiano sulla Salute Globale—OISG. In: A caro prezzo. Secondo rapporto sulle
disuguaglianze, ETS, Pisa, 2006;304-318.
[12] Bianco, M.L. L’Italia delle disuguaglianze. Carocci, Rome 2001.
[13] De Luca G., Ponzo M., Andrés A.R. Health care utilization by immigrants in Italy. International
Journal of Health Care Finance Economics 2013;13:1–31.
[14] WHO Regional Office for Europe. How health systems can address health inequities linked to
migration and ethnicity. Copenhagen: WHO Regional Office 2010.
[15] Bollini, P. and Sien, H. No Real Progress towards Equity: Health of Migrants and Ethnic
Minorities on the Eve of the Year 2000. Social Science & Medicine 1995;41:819-828.
[16] Razum, O. Commentary: Of Salmon and Time Travellers—Musing on the Mystery of Migration
Mortality. International Journal of Epidemiology, 2006;34:919-921.
[17] Razum, O., Zeeb, H. and Rohrmann, S. The Healthy Migrant Effect—Not Merely a Fallacy of
Inaccurate Denominator Figures. International Journal of Epidemiology 2000;29:191-192.
[18] IOM International Organisation for Migration. Migration health: Better health for all in Europe.
2009. Final report.
[19] Fernandes, A., & Miguel, J. P. Health and migration in the European Union: Better health for all
in an inclusive society. Lisboa: Instituto Nacional de Saúde Doutor Ricardo Jorge 2007.
[20] Istat. Survey on Income and Living Conditions (SILC) 2009.
[21] Istat. Survey of Income and Living Conditions of households with foreigners 2009.
[22] Istat. Households with foreigners: indicators of economic distress. Notes for the press - 28
February 2011. Istat, Rome 2011.
[23] Busetta A. Foreigners in Italy: economic living conditions and unmet medical needs. Genus
2016;LXXI(2-3):157-175. ISSN: 2035-5556.
[24] Bryant T., Leaver C., Dunn J. Unmet healthcare need, gender, and health inequalities in Canada.
Health Policy 2009;91:24-32.
[25] Rustgi S.D., Doty M.M., Collins S.R. Women at risk: why many women are forgoing needed
health care. Issue Brief, The Commonwealth Fund 2009.
[26] Cylus J., Papanicolas I. An analysis of perceived access to health care in Europe: How universal
is universal coverage? Health Policy 2015;119:1133-1144.
[27] Koolman, X. Unmet need for health care in Europe. Comparative EU statistics on income and
living conditions: issues and challenges. Proceedings of the EU-SILC conference. Helsinki: Eurostat
2007.
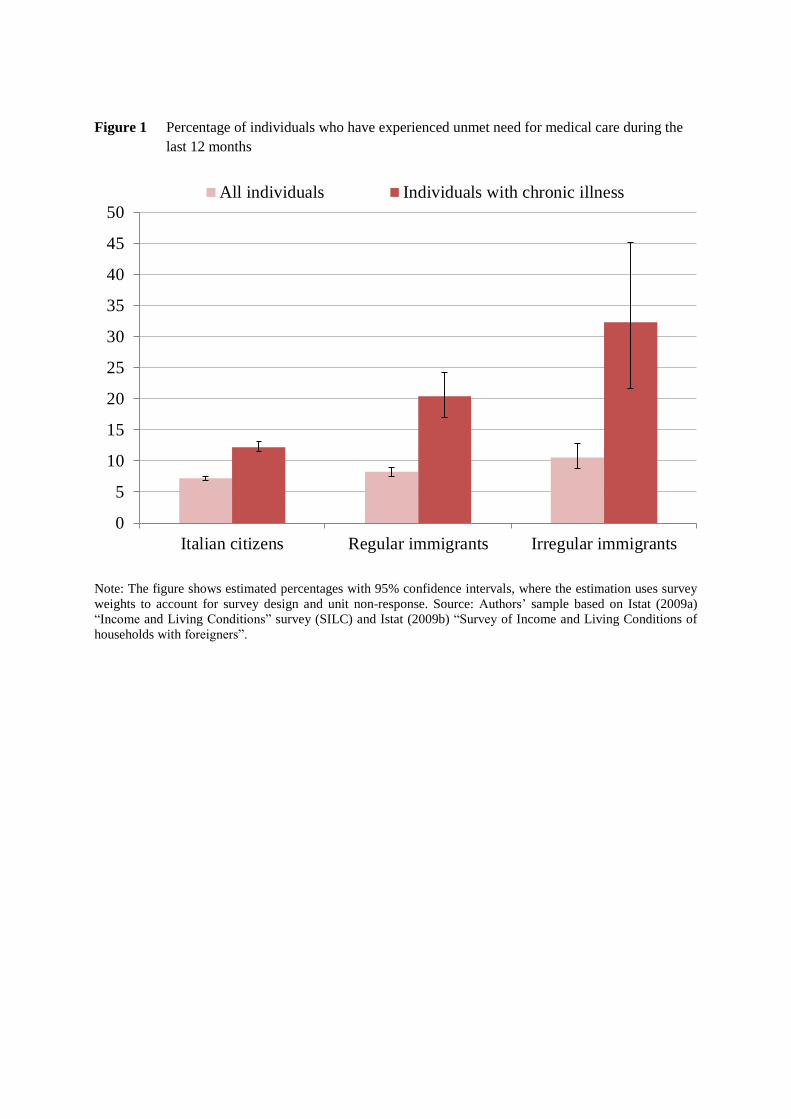
Figure 1 Percentage of individuals who have experienced unmet need for medical care during the
last 12 months
Note: The figure shows estimated percentages with 95% confidence intervals, where the estimation uses survey
weights to account for survey design and unit non-response. Source: Authors’ sample based on Istat (2009a)
“Income and Living Conditions” survey (SILC) and Istat (2009b) “Survey of Income and Living Conditions of
households with foreigners”.
0
5
10
15
20
25
30
35
40
45
50
Italian citizens Regular immigrants Irregular immigrants
All individuals Individuals with chronic illness
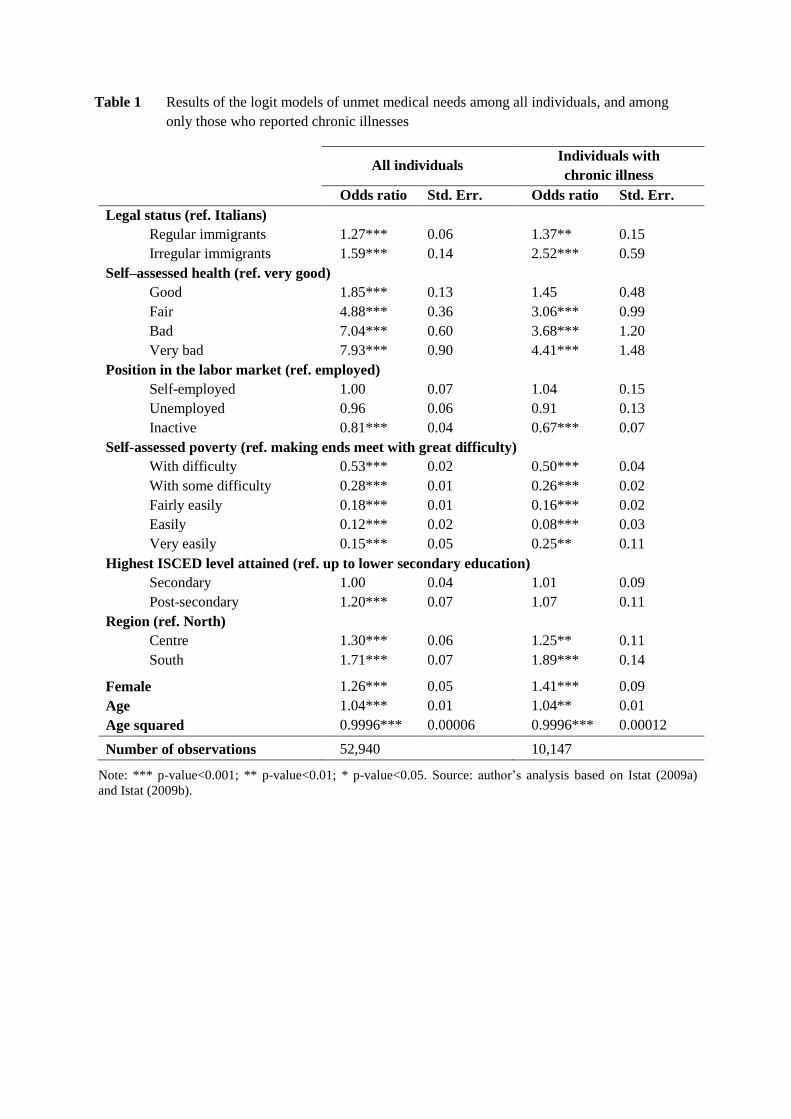
Table 1 Results of the logit models of unmet medical needs among all individuals, and among
only those who reported chronic illnesses
All individuals
Individuals with
chronic illness
Odds ratio Std. Err. Odds ratio Std. Err.
Legal status (ref. Italians)
Regular immigrants 1.27*** 0.06 1.37** 0.15
Irregular immigrants 1.59*** 0.14 2.52*** 0.59
Self–assessed health (ref. very good)
Good 1.85*** 0.13 1.45 0.48
Fair 4.88*** 0.36 3.06*** 0.99
Bad 7.04*** 0.60 3.68*** 1.20
Very bad 7.93*** 0.90 4.41*** 1.48
Position in the labor market (ref. employed)
Self-employed 1.00 0.07 1.04 0.15
Unemployed 0.96 0.06 0.91 0.13
Inactive 0.81*** 0.04 0.67*** 0.07
Self-assessed poverty (ref. making ends meet with great difficulty)
With difficulty 0.53*** 0.02 0.50*** 0.04
With some difficulty 0.28*** 0.01 0.26*** 0.02
Fairly easily 0.18*** 0.01 0.16*** 0.02
Easily 0.12*** 0.02 0.08*** 0.03
Very easily 0.15*** 0.05 0.25** 0.11
Highest ISCED level attained (ref. up to lower secondary education)
Secondary 1.00 0.04 1.01 0.09
Post-secondary 1.20*** 0.07 1.07 0.11
Region (ref. North)
Centre 1.30*** 0.06 1.25** 0.11
South 1.71*** 0.07 1.89*** 0.14
Female 1.26*** 0.05 1.41*** 0.09
Age 1.04*** 0.01 1.04** 0.01
Age squared 0.9996*** 0.00006 0.9996*** 0.00012
Number of observations 52,940 10,147
Note: *** p-value<0.001; ** p-value<0.01; * p-value<0.05. Source: author’s analysis based on Istat (2009a)
and Istat (2009b).
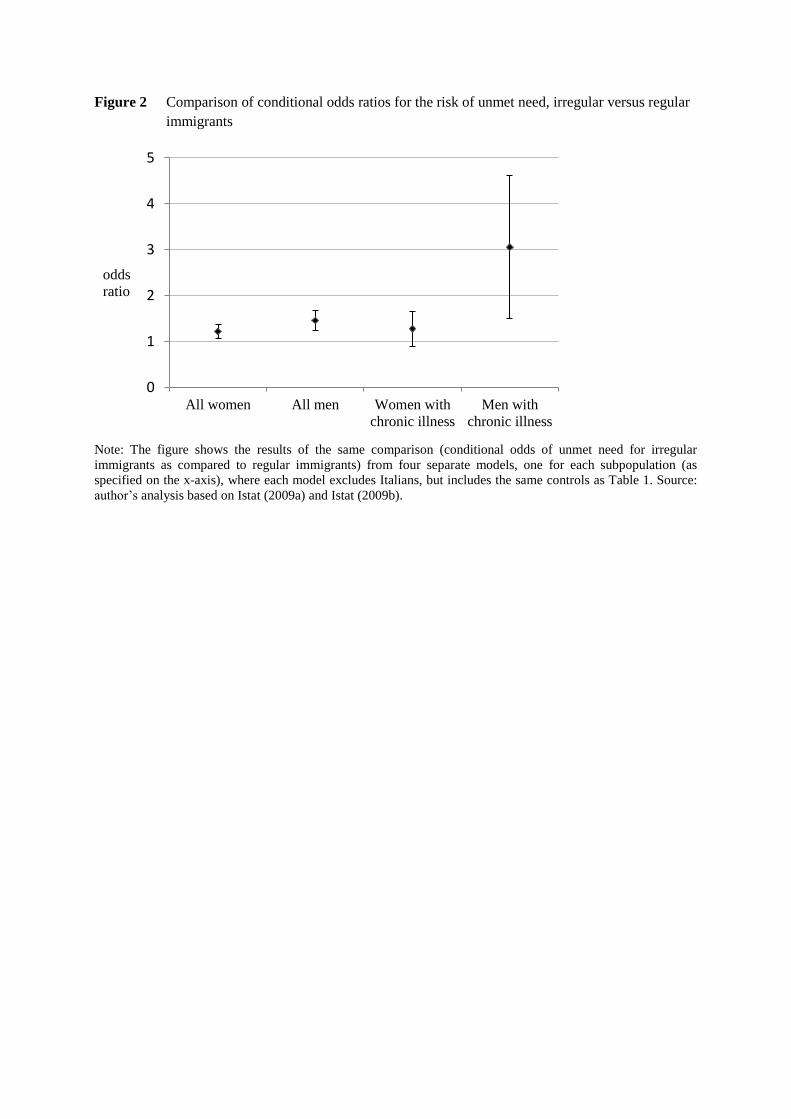
Figure 2 Comparison of conditional odds ratios for the risk of unmet need, irregular versus regular
immigrants
Note: The figure shows the results of the same comparison (conditional odds of unmet need for irregular
immigrants as compared to regular immigrants) from four separate models, one for each subpopulation (as
specified on the x-axis), where each model excludes Italians, but includes the same controls as Table 1. Source:
author’s analysis based on Istat (2009a) and Istat (2009b).
0
1
2
3
4
5
All women All men Women with
chronic illness
Men with
chronic illness
odds
ratio