Embed Size (px)
Citation preview

Ankle Instability: Current Concepts, Diagnosis, and Treatment
JOSEPH R. CASS, M.D. , BERNARD F. MORREY, M.D. , Department of Orthopedics
Our approach to the problem of ankle sprains and instability is reviewed. After diagnostic evaluation (including stress roentgenography, arthrography, or tenography if necessary), most of our patients are treated either by taping if they have a grade 1 or 2 sprain or by casting if they have a grade 3 disruption. If the injury should progress to chronic instability despite this treatment regimen, which is an unusual occurrence, satisfactory reconstructive procedures are available. Indications for acute primary repair are limited.
Inversion injuries to the ankle which cause sprains are common. Approximately 500 ankle sprains are evaluated each year at our institution. This estimate does not include the countless number of persons who "twist" their ankles but do not seek medical attention.
The anatomy and kinematics involved in ankle sprains are reviewed, and our approach to patients with these injuries from both a diagnostic and a therapeutic standpoint is outlined.
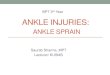
ANATOMY Standard anatomy textbooks well define the three lateral collateral ligaments of the ankle (Fig. 1), which are the structures that are disrupted in an ankle sprain. The anterior talofibular, calcaneofibular, and posterior talofibular ligaments are the static stabilizers of the ankle and are classically thought to be responsible for limiting excessive inversion of the ankle-hindfoot complex. Dynamic stabil ity may be provided by the peroneal musculature.
Classically, the anterior talofibular ligament has been thoughtto resist inversion if the ankle is in plantar flexion, and the calcaneofibular ligament has been thought to resist inversion if the ankle is in the neutral position. Dias,1 however, reported that the anterior talofibular ligament is the first ligamertf to be torn in an inversion injury regardless of the position of the ankle. This finding becomes important in the determination of what constitutes a severe sprain, as we wi l l outline in our section on the diagnosis of this injury.
KINEMATICS The ankle and subtalar articulations have been described as a universal joint.2 Rotation of the foot about its longitudinal axis is transmitted to the leg as a rotation about its longitudinal axis, which, with the ankle in the neutral position, isperpendiculartothatofthefoot(Fig. 2). These coupled motions are necessary. During the stance phase of gait, the lower extremity undergoes axial rotation as the gait cycle progresses.3 Because the foot is fixed (that is, it cannot externally rotate), it must absorb thisrotation. It does so by pronating in the early stance phase when the lower extremity is internally rotating and by supinating in the mid-to-late stance phase when the extremity is externally rotating. The lateral collateral ligaments are probably involved in this torque transmission, although their exact role has not been well established.
DIAGNOSIS Typically, the patient reports a twisting injury to the ankle, often suffered in a fall or a step on uneven ground. The physician must determine whether the ankle swelled immediately or some time later and whether the patient has a previous history of injury or instability. In addition, the physician must determine whether the patient is relatively sedentary or is involved in athletics at a recreational or competitive level. Also, a history of systemic disease should be sought so the clinician does not encounter any unsuspected condition; for example, in a patient with diabetes who has a previously unrecognized neuropathy of the foot, a relatively innocuous ankle
Mayo Clin Proc 59:165-170, 1984 165

166 ANKLE INSTABILITY Mayo Clin Proc, March 1984, Vol 59
Posterior talofibular ligament
Calcaneo- \ ( fibular \ Y
ligament \ep
\ Anterior \ talofibular | ligament
Fig. 1. Drawing of lateral collateral ligaments of ankle.
sprain can rapidly progress to extensive destruction of the ankle articulation unless it is appropriately treated. Al though this situation is rare, it is worthwhile to note in the initial history.
On examination, the areas of tenderness and swelling must be accurately defined. A determination that the patient has tenderness about the lateral aspect of the ankle is insufficient; rather, the physician should attempt
to determine precisely whether the patient has tenderness over the anter ior ta lo f ibu la r l igament , the ca l -caneofibular ligament, or both or perhaps elsewhere about the ankle or foot. Inversion of the ankle should reproduce^ymptoms. If the patient is examined late after the injury, when the swelling may be more diffuse, localization of the tenderness is difficult; however, at the time of initial examination, localization may be quite helpful in guiding the clinician to an accurate diagnosis.
Examination of and about the knee should also be included to rule out associated knee or proximal fibular injuries. When examining the ankle and hindfoot, the physician must determine the active and passive dor-siflexion and plantar flexion of the ankle, inversion and eversion of the hindfoot joints, and particularly what motions are painful. The neurovascular status should be assessed by palpation of the dorsalis pedis and posterior tibial arterial pulses and by sensory testing, particularly in the distribution of the sural nerve. Musculotendinous continuity should also be assessed by standard measures of resistive testing. A clinical estimate of stability should be obtained (as tolerated by the patient) first by forced inversion of the ankle by the examiner (Fig. 3) and second
Fig. 2. Drawing of coupled rotations involved in inversion of hindfoot. Fig. 3. Clinical assessment of degree of inversion instability.

Mayo Clin Proc, March 1984, Vol 59 ANKLE INSTABILITY 167
Fig. 4. Clinical assessment of degree of anterior instability.
by attempts to translate the foot anteriorly, with respect to the leg, by manual stress (clinical anterior drawer stress test) (Fig. 4). These motions should be compared with those found during clinical examination on the uninjured side in order to give the examiner an estimate of stability.
Although inversion injuries are common, several items in the differential diagnosis must continually be kept in mind (Table 1). Standard roentgenograms are usually obtained, but some of these injuries can be overlooked unless they are speci f ica l ly searched for on the roentgenogram.
After standard anteroposterior, lateral, and mortise roentgenographic views are studied (other views may be requested when appropriate), stress roentgenography may be warranted. The most common stress tests are the talar tilt and anterior drawer tests. Supplemental anesthesia may or may not be necessary, but the degree of patient cooperation is important in determining the re-
Table 1.—Differential Diagnosis of Ankle "Sprains"
Fractures Malleolar, Maisonneuve Talar neck Calcaneal anterior process Fifth metatarsal Osteochondral talar Cuboid
Dislocations Subtalar Talonavicular
Other Peroneal tendon subluxation Disruption of the inferior tibiofibular syndesmosis Deltoid ligament disruptions
liability of these measurements. Both measurements correlate poorly with measured findings, the degree of disruption, and symptoms of instability.
Anteroposterior roentgenographic views of the ankle are obtained during performance of the talar tilt stress test. The ankle is held in the neutral position to slight plantar flexion, and an inversion stress is applied to the foot either manually or by means of an inversion stress testing apparatus. Views of the uninjured side are obtained for comparison. The angle to be measured is that formed by a line parallel with the subchondral bone of the distal tibia and proximal talus (Fig. 5). Normal values have been reported to range from 5° 4 to 23°.5 A reasonable consensus seems to be that if the angle on the injured side is 5° to 10° more than on the uninjured side, both the anterior talofibular and calcaneofibular ligaments have been torn.
Fig. 5. Anteroposterior roentgenograms of ankle, showing positive talar tilt stress test of the ankle on the left.
The anterior drawer stress test is also performed with the ankle in the neutral position to slight plantar flexion. A lateral roentgenographic view of the ankle is obtained as an attempt is made manually to translate the foot anteriorly with respect to the leg. The sagittal plane translation of the talus with respect to the tibia is measured (Fig. 6). In comparison with the unstressed position, anterior subluxation of the talus of more than 2 to 3 mm6 is considered to be indicative of injury to the anterior talofibular ligament.
Several factors detract from the validity of these measurements: the degree of patient relaxation and cooperation, the amount of force used, the angle of ankle flexion, and the amount of laxity in the uninvolved ankle. As mentioned, these values correlate poorly with symptoms of instability but are the currently accepted methods of determining the degree of disruption of the lateral collateral ligaments.

168 ANKLE INSTABILITY Mayo Clin Proc, March 1984, Vol 59
Fig. 6. Lateral roentgenograms of ankle, showing positive anterior drawer stress test of the ankle on the right.
Other roentgenographic techniques have been developed in an effort to increase the accuracy of diagnosis. Arthrography of the ankle has been used in an attempt to delineate the specific pathologic changes in the ligaments. The incidence of extravasation of dye into various tendons around the ankle (particularly the flexor hallucis longus and peroneal sheaths), however, has been estimated to be as high as 25%7; thus, the diagnostic value of arthrography is diminished. Peroneal tenography, or injection of dye into the peroneal sheath, has also been advocated. The developers of this technique believe that if dye escapes into the ankle joint, the calcaneofibular ligament has been torn, and because this ligament seldom tears without a concomitant tear of the anterior talofibular ligament, a serious disruption of the lateral collateral ligaments has occurred.8
Once the diagnosis of a "sprained ankle" has been made, the severity of the injury must be established. The standard nomenclature for ligamentous ruptures comprises three broad categories: grade 1, mild stretch of the ligament and no instability; grade 2, moderate but incomplete tear of the ligament and mild instability; and grade 3, complete tear of the ligament and gross instability.
From a more practical standpoint, a grade 3 sprain is usually considered to be a complete disruption of both
the anterior talofibular and calcaneofibular ligaments. Although by definition a complete tear of the anterior talofibular ligament with the calcaneofibular ligament intact is a grade 3 ligamentous disruption, it is not commonly considered to be a grade 3 sprain. Roentgeno-graphically, a substantial increase in the talar tilt indicates disruption of the anterior talofibular and calcaneofibular ligaments. Anterior translation of more than 2 mm indicates disruption of the anterior talofibular ligament because the calcaneofibular ligament is thought to have little effect on anterior subluxation.
TREATMENT The controversy continues regarding operative or non-operative treatment of these injuries, particularly those of grade 3 severity. Proponents of operation report both subjective and objective satisfactory results. Proponents of nonoperative treatment report good subjective results but only variable objective results with postinjury stability. When the number of sprains is compared with the number of patients who present with chronic instability, however, chronic instability is relatively unusual regardless of primary treatment. A recent long-term follow-up study an average of 9 years after primary repair or delayed reconstruction for ankle ligamentous disruption demonstrated that equivalent results could be obtained after either treatment modality.9 Because a reconstructive procedure that provides functionally equivalent results is available and because chronic instability is relatively unusual, primary complete restoration of ligamentous continuity would not seem to be necessary.
On the basis of these data, our current approach is to treat the patient as follows. Sprains of grade 1 or2severity are treated by taping, and a determination of the rate of return to activity is based on the patient's symptoms. If the patient is unable to walk comfortably with the ankle taped because of swelling or pain, a compressive dressing followed by casting for 2 or 3 weeks is reasonable. This type of case should alert the clinician to the fact that a more extensive ligamentous disruption is probably present. For several weeks after the casting period, the ankle should be protected with tape during any stressful activities. Again, determination of the rate of return to activity should be based on the patient's symptoms. Accurate data regarding the healing time for the lateral ligaments of the ankle are lacking. The period of protection is thus somewhat empiric. If the patient has a grade 3 ligamentous injury as manifested by symptoms or abnormal findings on stress roentgenograms or ar-thrograms, the ankle is immobilized for 3 to 6 weeks in a walking cast. After the cast has been removed, graded return to activity is allowed and the ankle is protected by

Mayo Clin Proc, March 1984, Vol 59 ANKLE INSTABILITY 169
Fig. 7. Drawing of modified Evans reconstruction. I
adhesive tape. A program of strengthening of the per- t oneal muscles has been recommended by some authors s as well. 1
Primary repair of grade 3 injuries has limited value in s our scheme. Although objective stability (as determined ί from normal results of the talar tilt and anterior drawer s stress tests) is restored by repair, the risks and logistics of s repair in comparison with the results after cast treatment i are such that the only indication for acute repair is in a c high-level competitive athlete (that is, an athlete whose career is or is intended to be competitive athletics). s
Should chronic instability develop, as manifested by \ either symptoms of pain or recurrent giving way, a sur- ( gical reconstruction is worthwhile. Occasionally, pa- i
Fig. 8. Drawing of Watson-Jones reconstruction.
n. Fig. 9. Drawing of Chrisman-Snook modified Elmslie reconstruction.
ling of the per- tients with chronic instability wi l l complain of these y some authors symptoms but the stress roentgenograms wil l be normal.
These patients should undergo thorough studies because imited value in stress roentgenography has limited reliability. Intra-(as determined articular pathologic findings within either the ankle or the
anterior drawer subtalar joint complex and peroneal tendon subluxation and logistics of should be ruled out. Also, the differential diagnosis of an r cast treatment acute sprain should be kept in mind because the initial te repair is in a diagnosis may have been in error, l athlete whose If the symptoms, signs, and physician's impressions are e athletics). strong enough, regardless of the degree of roent-, manifested by genographic instability, an operative approach is logical, ing way, a sur- Our approach would be to explore the lateral structures, casionally, pa- if they are repairable, in order to perform a "delayed
primary" repair according to the method of Broström.10 If this approach is not feasible, we do an Evans-type reconstruction. In our comparative study9 of the Evans, Watson-Jones, and Chrisman-Snook modified Elmslie reconstructions11 (Fig. 7 to 9), substantial differences were not found. Therefore, the technically less demanding Evans reconstruction is our procedure of choice.
SUMMARY The three lateral collateral ligaments of the ankle (ante-rior talofibular, calcaneofibular, and posterior talo-
y fibular) are probably involved in torque transmission of 'S^s"---^_ the foot and leg and are the structures that are disrupted in
^~~~~~] an ankle sprain. As with all injuries, accurate diagnosis is / the key to successful treatment. Several satisfactory
—■ treatment options (operative and nonoperative) are avail-^ able. If chronic instability ensues, results after a recon
struction are nearly as good as those after acute repair.

170 ANKLE INSTABILITY Mayo Clin Proc, March 1984, Vol 59
REFERENCES 1. Dias LS: The lateral ankle sprain: an experimental study. J Trauma
19:266-269, 1979 2. Inman VT: The Joints of the Ankle. Baltimore, Williams & Wilkins
Company, 1976 3. Inman VT, Ralston HJ, Todd F: Human Walking. Baltimore,
Williams & Wilkins Company, 1981 4. Cox JS, Hewes TF: "Normal" talar tilt angle. Clin Orthop
140:37-41, 1979 5. Rubin G, Wirten M: The talar-tilt angle and the fibular collateral
ligaments: a method for the determination of talar tilt. J Bone Joint Surg [Am] 42:311-326, 1960
6. Anderson KJ, LeCocq JF, LeCocq EA: Recurrent anterior sub-luxation of the ankle joint: a report of two cases and an experimental study. J Bone Joint Surg |Am] 34:853-860, 1952
7. Broström L, Liljedahl S-O, Lindvall N: Sprained ankles. II. Ar-thrographic diagnosis of recent ligament ruptures. Acta Chir Scand 129:485-499, 1965
8. Black H: Roentgenographic considerations. Am J Sports Med 5:238-240, 1977
9. Cass JR, Morrey BF: Ankle instability: a long-term follow-up comparison of primary repair and delayed reconstruction. Presented at the American Association of Orthopedic Surgery (AAOS) general session, March 1983
10. Broström L: Sprained ankles. VI. Surgical treatment of "chronic" ligament ruptures. Acta Chir Scand 132:551-565, 1966
11. Edmonson AS, Crenshaw AH: Campbell's Operative Orthopaedics. Sixth edition. St. Louis, CV Mosby Company, 1980
END OF SYMPOSIUM ON SPORTS MEDICINE