Embed Size (px)
Citation preview

ANGIOTENSIN RECEPTOR SUBTYPES IN THE RABBIT
PULMONARY ARTERY
LISA TAN MAY YIN
BSc (Pharm) (Hons)
A THESIS SUBMITTED FOR THE DEGREE OF
DOCTOR OF PHILOSOPHY
DEPARTMENT OF PHARMACOLGOY
NATIONAL UNIVERSITY OF SINGAPORE
2003

ACKNOWLEDGEMENTS
Many people have contributed to my graduate education, as friends, colleagues and teachers. First and foremost, I would like to express my thanks to my supervisor, Associate Professor Sim Meng Kwoon, for encouraging me to
embark on this journey. His invaluable insights, guidance and support have helped me to mature as a student and as a researcher. I was also very fortunate
to be acquainted with Dr John W. Ferkany and Dr Terry Kenakin who, as experts in their fields, have struck me with their humility and helpfulness. I am
indebted to their kindness, encouragement and generosity in sharing their scientific expertise and extensive experience with me. In my department, I was surrounded by knowledgeable and friendly people who did not hesitate to show me how to operate equipment or loan me materials that were not available in
my laboratory. My thanks to Min Le, Wu Jian, Wen Qiang, Woei Shin, Wee Lee, Siew Lan, Xiao Guang, Mr Ang, Annie and Peter for their friendship and kind
help. For their financial support I would like to thank the National University of Singapore for the research scholarship. Finally, I would like to thank those
closest to me, especially my partner, for their absolute confidence in me and for providing me with the strength to persevere through the difficult times. Their
presence, patience, understanding and love helped make the completion of my graduate work possible.
ii

TABLE OF CONTENTS PAGE
List of publications and poster presentations vi List of figures vii List of tables ix List of abbreviations x Summary 1 . Chapter 1: General Introduction 7 1.1 Introduction 7 1.2 The Renin Angiotensin System (RAS) - Production 9 of Angiotensin II and Other Bioactive Angiotensin Peptides
1.2.1 Systemic and tissue RAS 9 1.2.2 Bioactive angiotensin fragments 9 1.2.3 Angiotensin III 11 1.2.4 Angiotensin IV 12 1.2.5 Angiotensin (1-7) 15 1.2.6 Des-Asp-angiotensin I 16
1.3 Angiotensin Receptors 18 1.3.1 Distribution in vasculature 18 1.3.2 AT1 receptor 19 1.3.3 AT2 receptor 21 1.3.4 AT3 receptor 22 1.3.5 AT4 receptor 23 1.4 AT1 Signaling Pathways in the Vasculature 23 1.4.1 Stimulation of phospholipase C and 25 inositol triphosphate signaling
1.4.2 Increase in intracellular calcium 26 1.4.3 Regulation of smooth muscle contraction 26 and relaxation 1.4.4 Activation of protein kinase C and 29 intracellular alkalinization 1.4.5 Activation of Src family kinases 31 1.4.6 Phospholipase A2 activation and arachidonic 31 acid metabolism 1.4.7 Phospholipase D activation 35 1.4.8 Modulation of cyclic nucleotides 36 1.4.9 Tyrosine kinase phosphorylation 37
1.5 Functional and Structural Complexity of Signal 39 Transduction via GPCRs 1.6 Role of RAS in Primary Pulmonary Hypertension 42 (PPH) 1.7 Conclusion 44
iii

TABLE OF CONTENTS PAGE
Chapter 2: Functional Studies on Isolated Rabbit Pulmonary 45 Trunk and Artery
2.1 Introduction 45 2.2 Materials and Methods 46
2.2.1 Isolation of rabbit pulmonary trunk and 46 artery 2.2.2 Preparation of pulmonary trunk and artery 47 2.2.3 Direct actions of angiotensin peptides 48 2.2.4 Effects of angiotensin peptides on 48 pre-contracted trunk and artery strips 2.2.5 Effects of receptor antagonists and enzyme 49
inhibitors 2.2.6 Structure-activity relationship of angiotensin 50
IV 2.2.7 Expression of results 50 2.2.8 Statistical analysis 51
2.3 Results 51 2.3.1 Direct actions of angiotensin peptides 51 2.3.2 Effects of angiotensin peptides on 53 pre-contracted trunk and artery strips
2.3.3 Effects of receptor antagonists and enzyme 53 inhibitors
2.3.4 Structure-activity relationship of angiotensin 56 IV
2.4 Discussion 56 Chapter 3: Receptor Binding Studies 62
3.1 Introduction 62 3.2 Materials and Methods 63
3.2.1 Membrane preparation 63 3.2.2 125I-Sar1-Ile8-angiotensin II competition 64 binding experiments 3.2.3 125I-angiotensin IV association binding 65
experiments 3.2.4 125I-angiotensin IV competition binding 66
experiments 3.2.5 Data analysis 66 3.2.6 Statistical analysis 67 3.2.7 Drugs and reagents 67
3.3 Results 68 3.4 Discussion 72
iv

TABLE OF CONTENTS PAGE
Chapter 4: RNA Studies 78
4.1 Introduction 78 4.2 Rationale for Experimental Design 79 4.3 Materials and Methods 81
4.3.1 Isolation of primary vascular smooth muscle 81 cells (VSMCs) – primary explant technique 4.3.2 Cell culture 82 4.3.3 Isolation and purification of RNA 83 4.3.4 Generation of probes for Northern Blot 85
4.3.4.1 Primers 85 4.3.4.2 RT-PCR and DNA cloning 85
4.3.5 Northern blot 87 4.4 Results 88 4.5 Discussion 88 Chapter 5: Signal Transduction Studies 93
5.1 Introduction 93 5.2 Rationale for Experimental Design 95
5.2.1 Prostaglandin studies 95 5.2.2 Inositol triphosphate studies 96
5.3 Materials and Methods 97 5.3.1 Prostaglandin studies 97 5.3.1.1 Cell culture 97 5.3.1.2 Measurement of PGE2 and 6-keto- 98 PGF1α release 5.3.1.3 Expression of results and 98 statistical analysis
5.3.2 Inositol triphosphate studies 99 5.3.2.1 Preparation of tissue 99 5.3.2.2 Agonist reaction 99 5.3.2.3 IP3-binding assay 100
5.4 Results 101 5.4.1 Prostaglandin studies 101 5.4.2 Inositol triphosphate studies 105 5.5 Discussion 105 Chapter 6: General Discussion 117 References 125
v

LIST OF PUBLICATIONS AND CONFERENCE PAPERS Lisa MY Tan and MK Sim Actions of angiotensin peptides on the rabbit pulmonary artery. Life Sciences, 2000; 66(19): 1839-1847. Lisa MY Tan and MK Sim Actions of angiotensin peptides on the rabbit pulmonary artery. International Forum on Angiotensin II Receptor Antagonism, 27-30 January 1999, Monte-Carlo
vi

LIST OF FIGURES
FIGURE
TITLE PAGE
1.1
Pulmonary trunk and artery 3
1.2
Metabolism of angiotensinogen 10
1.3
Angiotensin AT1 receptor-mediated signaling pathways in vascular smooth muscle cells
24
1.4
Regulation of smooth muscle contraction and relaxation 28
1.5
Modulation of the Ca sensitivity of myosin by modifying the activities of MLCK and MLCP
30
1.6
Arachidonic acid metabolism 34
2.1
Direct contractile action of angiotensin II, angiotensin III and angiotensin IV on the rabbit pulmonary trunk and artery.
52
2.2
Effect of angiotensin II, angiotensin III and angiotensin IV on the noradrenaline pre-contracted pulmonary trunk and artery
54
2.3
Influence of losartan and indomethacin on responses to angiotensin II, angiotensin III and angiotensin IV in the noradrenaline-contracted pulmonary trunk and artery
55
2.4 Influence of amastatin on responsese to angiotensin II, angiotensin III and angiotensin IV in the noradrenaline-contracted pulmonary trunk and artery
57
2.5 Influence of divalinal-angiotensin IV on responses to angiotensin IV in rabbit pulmonary trunk and artery
58
3.1 125I-Sar1-Ile8-angiotensin II competition curves in the rabbit pulmonary trunk and artery
69
3.2 125I-angiotensin IV competition curves in the rabbit pulmonary trunk and artery
73
4.1 Nucleotide sequence of cDNA encoding a rabbit kidney cortex angiotensin II receptor.
80
vii

FIGURE
TITLE PAGE
4.2 AT1 receptor mRNA in rabbit pulmonary trunk and artery vascular smooth muscle cells (VSMCs)
89
5.1 Stimulation of PGE2 and 6-keto-PGF1α production in rabbit pulmonary trunk and artery smooth muscle cells by angiotensin II
102
5.2
Stimulation of PGE2 and 6-keto-PGF1α production in rabbit pulmonary trunk and artery smooth muscle cells by angiotensin III
103
5.3
Stimulation of PGE2 and 6-keto-PGF1α production in rabbit pulmonary trunk and artery smooth muscle cells by angiotensin IV
104
5.4 Stimulation of inositol triphosphate production in rabbit pulmonary trunk and artery tissue by angiotensin II over time
106
5.5 Stimulation of inositol triphosphate production in rabbit pulmonary trunk and artery tissue by angiotensin IV over time
107
5.6
Scheme demonstrating mechanisms whereby angiotensin II and angiotensin IV stimulation of the AT1 receptor can elicit different cellular responses.
111
viii

LIST OF TABLES
TABLE
TITLE PAGE
1 Competition binding constants for 125I-Sar1-Ile8-angiotensin II and 125I-angiotensin IV binding to rabbit pulmonary trunk and artery membranes
71
2 Binding constants for AT4 receptors in various species and tissues (adapted from de Gasparo et al., 2000)
76
ix

LIST OF ABBREVIATIONS
6-keto-PGF1α 6-keto-prostaglandin F1αAA Arachidonic acid APA Aminopeptidase A APN Aminopeptidase N BSA CaM kinase
Bovine serum albumin Ca2+/Calmodulin-dependent kinase
cAMP Adenosine 3’,5’-cyclic monophosphate cGMP Guanosine 3’,5’-cyclic monophosphate DAG Diacylglycerol DAP Dipeptidylaminopeptidase GAP GTPase activating protein GEF Guanosine exchange factor GPCR G protein-coupled receptor HETE Hydroxyeicosatetraenoic acid IP3 Inositol triphosphate KCa Ca2+-activated K+ channels Kd Dissociation constant Ki Inhibition constant LT Leukotriene MAPK Myosin-activated protein kinase MBS Myosin binding unit MLC20 Regulatory light chains of myosin MLCK Myosin light chain kinase MLCP Myosin light chain phosphatase mM Millimolar NEP Neutral endopeptidase nM Nanomolar NO Nitric oxide cNOS Constitutive nitric oxide synthase PA Phosphatidic acid PACAP Pituitary adenylate cyclase-activating polypeptide PASMCs Pulmonary artery smooth muscle cells PBS Phosphate-buffered saline PC Phosphatidylcholine PDGF Platelet-derived growth factor PG Prostaglandin PI Phosphatidylinositol PIP2 Phosphatidylinositol-4,5-biphosphate PKA cAMP-dependent kinase / protein kinase A PKC protein kinase C PKG cGMP-dependent kinase / protein kinase G PLA2 Phospholipase A2PLC Phospholipase C PLD Phospholipase D
x

PP Phosphatidic acid phosphorylase PPH Primary pulmonary hypertension PTSMCs Pulmonary trunk smooth muscle cells RAS Renin angiotensin system SHR Spontaneously hypertensive rat SR Sarcoplasmic reticulum TXA2 Thromboxane A2VSMCs Vascular smooth muscle cells WKY Wistar Kyoto rat
xi

SUMMARY
Angiotensin II is known to be the main effector peptide of the renin-angiotensin
system (RAS) and acts on the angiotensin AT1 receptor to mediate the majority of
its effects. New evidence is emerging that demonstrates the bioactivity of a variety
of angiotensin II fragments, e.g., angiotensin III, angiotensin IV, des-Asp-
angiotensin I and angiotensin (1-7). This recent discovery has challenged our views
on the final effectors and regulation of the RAS and the significance of poly
angiotensins both physiologically and pathophysiologically.
The aim of this project is to evaluate the role of angiotensin II and its immediate
metabolites, angiotensin III, angiotensin IV, angiotensin (4-8) and angiotensin (3-7)
on the regulation of pulmonary blood flow in the rabbit. We investigated the actions
of these angiotensin peptides on isolated endothelium-denuded pulmonary trunk
and artery tissue, and characterised the angiotensin receptor subtypes in vascular
smooth muscle cells isolated from the rabbit pulmonary trunk and artery by receptor
binding and Northern blot analysis. Finally, we evaluated the signal transduction
pathways coupled to these receptors by measuring the production of inositol
triphosphate, prostaglandin E2 and PGI2. Two major findings resulted from these
experiments. We first provide evidence that the rabbit pulmonary vasculature is not
just a passive conduit but may be an important regulator of blood flow from the
heart to the lung. Secondly, we demonstrate the contribution of bioactive
angiotensin fragments, e.g., angiotensin III and angiotensin IV, to the fine-
regulation of pulmonary vascular control.
1

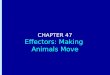
In the isolated tissue study, differential responses of the endothelium-denuded
sections of the rabbit pulmonary trunk (the vessel arising from the right ventricle of
the heart prior to its bifurcation into the left and right pulmonary arteries) and the
two pulmonary arteries (vessels distal to the bifurcation) (see Figure 1.1) to
angiotensin II and its immediate metabolites were observed. Angiotensin II further
contracted noradrenaline pre-contracted sections of the pulmonary trunk and artery.
In contrast, angiotensin III and angiotensin IV relaxed the pre-contracted sections of
the pulmonary trunk while they were either inactive (angiotensin IV) or further
contracted (angiotensin III) the pre-contracted sections of the pulmonary artery. The
AT1 receptor mediated both the vasoconstrictor and vasodilator response since
losartan, an AT1-selective receptor antagonist, blocked the vasoconstrictor and
vasodilator response caused by all three angiotensin peptides and PD123319, an
AT2-selective receptor antagonist, had no effect. Indomethacin, a cyclooxygenase
inhibitor, blocked only the vasodilator response induced by angiotensin III and
angiotensin IV in the trunk, indicating that vasodilator prostaglandins were
probably involved in mediating this response. Amastatin, a selective
aminopeptidase A and N inhibitor, blocked the angiotensin III-induced
vasoconstrictor and vasodilator response in the pulmonary artery and trunk,
respectively but did not significantly affect the angiotensin II and IV responses.
This suggested that the angiotensin III-induced responses were mediated in part by
a breakdown product of angiotensin III. Angiotensin IV is a likely candidate for this
2

Figure 1.1 The pulmonary trunk and artery
3

breakdown product since angiotensin III is broken down by APN to generate
angiotensin IV. Angiotensin (4-8) and angiotensin (3-7) were not bioactive in these
preparations.
Labelled Sar1-Ile8-angiotensin II bound with similar high affinity to pulmonary
trunk (Kd = 0.959 ± 0.609 nM, Bmax = 0.34 ± 0.20 pmol/mg protein) and artery
binding sites (Kd = 1.041 ± 0.330 nM, Bmax = 0.71 ± 0.19 pmol/mg protein) and was
displaced by losartan with a Ki of 0.45 ± 0.74 nM and 31.1 ± 26.1 nM, respectively,
but not by PD123319 and the AT4-selective antagonist, divalinal-angiotensin IV.
These data were confirmed by a Northern blot analysis which revealed the presence
of a single AT1 receptor subtype in both pulmonary trunk and artery VSMCs.
The activation of PLC and PLA2 in response to angiotensin II, angiotensin III and
angiotensin IV was evaluated by measuring inositol triphosphate production and
prostaglandin E2 and PGI2 release, respectively. This is a first report comparing the
angiotensin II-, angiotensin III- and angiotensin IV-induced prostaglandin and
inositol triphospate signaling in tissues of the rabbit pulmonary vasculature.
Angiotensin II significantly increased the production of both prostaglandin E2 and
PGI2 in the rabbit pulmonary trunk and artery VSMCs. This increase was inhibited
by losartan but not by PD123319, implicating the role of AT1 receptors in
mediating this response. The stimulation of pulmonary trunk and artery VSMCs by
angiotensin III and angiotensin IV was associated with an increase in both
4

vasodilator prostaglandins and a reduction of this release by losartan and
indomethacin. The magnitude of prostaglandin release did not differ significantly
between the trunk and artery cells for all three angiotensin peptides tested.
Following this finding, we demonstrated that angiotensin II stimulates a higher
production of IP3 in pulmonary trunk tissue slices compared to that by angiotensin
IV, suggesting that the differential angiotensin II-induced vasoconstrictor response
and angiotensin IV-induced vasorelaxant response in the rabbit pulmonary trunk
may be due to higher amounts of the inositol triphosphate second messenger being
produced when stimulated by angiotensin II compared to angiotensin IV.
Taken together, the present findings indicate that the response seen in the
pulmonary vasculature is likely a result of a balance of contractile, i.e., inositol
triphosphate production, and relaxant, i.e., prostaglandin release, signaling
components. It also supported the notion that a single AT1 receptor is involved, and
it is possible that this receptor is coupled to a single or multiple G proteins which,
when activated, triggers the activation of multiple signaling pathways that
contribute to the final vascular response. Moreover, the vasorelaxant action of
angiotensin IV, which is formed when angiotensin II is metabolized, may contribute
to the modulation of contractile actions mediated by angiotensin II in the pulmonary
trunk. Importantly, this fine-regulation of angiotensin responses in the pulmonary
trunk, which receives blood directly from the right ventricle, may play a role in the
protection of the delicate pulmonary capillaries from excessive systolic pressure.
5

Understanding these protective mechanisms may have important therapeutic
implications in the treatment of pulmonary hypertension.
6

CHAPTER 1
GENERAL INTRODUCTION
1.1 Introduction
The renin angiotensin system (RAS) plays an important role in the regulation of
blood pressure, plasma volume, sympathetic nervous activity and thirst responses.
Its remarkable diversity of physiologic actions include vasoconstriction in vascular
smooth muscle, cardiac contractility and heart rate through its actions on the
sympathetic nervous system, alteration of renal sodium and water absorption by
acting directly on renal vasculature and through its ability to stimulate the zona
glomerulosa cells of the adrenal cortex to synthesize and secrete aldosterone, thirst
enhancement in the brain and secretion of the antidiuretic hormone from the
pituitary gland. What is striking about the RAS is that despite its wide range of
actions on many different target organs in the body, angiotensin II is known to be
its main effector peptide and the AT1 receptor is established as the principle site of
the biological action of angiotensin II.
In contrast to other G-protein coupled receptor systems, such as the adrenoceptors,
muscarinic receptors, serotonin receptors and dopamine receptors, where subtypes
mediate a wide array of biological responses, it seemed an exception rather than the
norm that only one effector peptide (i.e. angiotensin II) and one receptor subtype
(i.e., AT1) mediate the majority of the effects of the RAS. It was only in the late
7

1980s that the existence of a second angiotensin receptor subtype, the AT2, was
demonstrated with the development of receptor specific antagonists, e.g. losartan
and PD 123319. However, this did little to account for the myriad of angiotensin
responses since the AT1 receptor mediates virtually all of the known physiological
actions of angiotensin II in target cells.
It is therefore of interest to note that new evidence is emerging that demonstrates, in
addition to angiotensin II and III, bioactivity of a variety of angiotensin fragments,
e.g. des-Asp-angiotensin I (Sim and Soh, 1995; Sim and Chai, 1996; Sim and Min,
1998; Min et al., 2000), angiotensin IV (Wright et al., 1995) and angiotensin (1-7)
(Ferrario et al., 1998). In addition, putative binding sites for angiotensin IV (AT4)
and angiotensin (1-7) have been demonstrated and pharmacologically characterized
(Swanson et al., 1992; Hall et al., 1993; Hanesworth et al., 1993; Nuess et al., 1994;
Wright et al., 1994; Bernier et al., 1995), although their cloning has not been
reported. These recent findings have challenged the ‘single’ regulatory peptide and
receptor concept of the RAS and opened up the possibilities of poly functional
angiotensins in the system.
The present literature review focuses on the formation of bioactive angiotensin
fragments from angiotensin I and angiotensin II, the angiotensin receptor types and
their distribution, vascular AT1 receptor signaling mechanisms, and finally evidence
for multiple signal transducers coupled to the angiotensin AT1 receptor subtype.
8

1.2 The Renin Angiotensin System (RAS) - Production of Angiotensin II
and Other Bioactive Angiotensin Peptides
1.2.1 Systemic and Tissue RAS
Angiotensin II is produced systemically via the classical RAS, and locally via tissue
RAS. In the classical RAS, circulating renal-derived renin cleaves hepatic-derived
angiotensinogen to form angiotensin I, which is converted to angiotensin II by
angiotensin converting enzyme in the lungs. The existence of a local tissue RAS is
evidenced by the localization of many of its components in tissues. All components
of the RAS, except renin, have been demonstrated to be produced in the
vasculature. The locally produced angiotensin II exerts paracrine and autocrine
effects in the vicinity of its site of formation.
1.2.2 Bioactive angiotensin fragments
Angiotensin II is metabolized into active angiotensin peptides by enzymes acting at
the two ends of the peptide (Figure 1.2). Its precursor, angiotensin I, can be
similarly degraded. Four angiotensin fragments are of biological interest:
angiotensin III, which is obtained by deletion of the N-terminal aspartic acid from
angiotensin II; angiotensin IV, which is obtained by deletion of the N-terminal
arginine from angiotensin III; angiotensin (1-7), which is obtained by deletion of
the C-terminal phenylalanine from angiotensin II; and des-Asp- angiotensin I,
which is obtained by deletion of the N-terminal aspartic acid from angiotensin I (see
Figure 1.2).
9

NH2-Asp1-Arg2-Val3-Tyr4-Ile5-His6-Pro7-Phe8-His9-Leu10-Val11-Ile12-His13-Asn14-COOH
(Angiotensinogen)
renin
NH2-Asp1-Arg2-Val3-Tyr4-Ile5-His6-Pro7-Phe8-His9-Leu10-COOH
(Angiotensin I)
prolyl/neutral ACE
endopeptidases chymase (in heart) aminopeptidase X
aminopeptidase A
NH2-Asp1-Arg2-Val3-Tyr4-Ile5-His6-Pro7-Phe8-COOH
(Angiotensin II)
NH2-Arg2-Val3-Tyr4-Ile5-His6-
Pro7-Phe8-His9-Leu10-COOH
(des-Asp-angiotensin I)
NH2-Asp1-Arg2-Val3-Tyr4
-Ile5-His6-Pro7-COOH aminopeptidase A
(Angiotensin (1-7)) ACE
NH2-Arg2-Val3-Tyr4-Ile5-His6-Pro7-Phe8-COOH
Inactive (Angiotensin III)
fragments (?) aminopeptidase N
NH2-Val3-Tyr4-Ile5-His6-Pro7-Phe8-COOH
(Angiotensin IV)
aminopeptidase N (?)
dipeptidylaminopeptidase (?)
carboxypeptidase N (?)
NH2-Tyr4-Ile5-His6-Pro7-Phe8-COOH11
NH2-Ile5-His6-Pro7-Phe8-COOH12
NHs-Val3-Tyr4-Ile5-His6-Pro7COOH13
other active/inactive fragments (?)
Figure 1.2 Metabolism of angiotensinogen
10

1.2.3 Angiotensin III
Angiotensin II is converted to angiotensin III by aminopeptidase A (APA) that
selectively cleaves the aspartyl residue of angiotensin II (Reaux et al., 1999b).
Angiotensin III is generally less potent in peripheral target tissues than angiotensin
II because it is rapidly degraded due to the large distribution of aminopeptidase N
(APN), which metabolizes angiotensin III, but not angiotensin II, to angiotensin IV
(Gaynes et al., 1978; Ahmad and Ward, 1990). However, angiotensin III was
recently demonstrated to be the main effector peptide in the central regulation of
blood pressure (Reaux et al., 1999a; Reaux et al., 2001), and in the hypothalamus in
the stimulation of antidiuretic hormone secretion (Zini et al., 1996). The studies
were carried out with the recently developed specific APA and APN inhibitors,
EC33 and PC18, respectively (Fournie-Zaluski et al., 1992; Chauvel et al., 1994;
Reaux et al., 1999a). These new agents represent invaluable new tools to ascribe a
physiological effect to a given angiotensin II fragment. For example, an effect
inhibited by EC33 and potentiated by PC18 can be attributed to angiotensin III.
Similarly, an effect inhibited by PC18 can be attributed to angiotensin IV. Central
inhibition of APA by EC33 not only blocked the pressor action of angiotensin II but
also caused a fall in basal blood pressure comparable to that caused by i.c.v.
administration of losartan, indicating a requirement for angiotensin III in the tonic
regulation of blood pressure. Furthermore, the inhibition of APN activity
(responsible for converting angiotensin III to angiotensin IV) by PC18 caused an
increase in blood pressure that was blocked by losartan. This suggests that
inhibition of angiotensin III degradation by PC18 causes an increase in angiotensin
11

III levels that elevates blood pressure through an action on AT1 receptors. These
observations indicate the potential applications of APA inhibitors as centrally acting
compounds in the management of hypertension (Reaux et al., 1999b, Reaux et al.,
2000).
1.2.4 Angiotensin IV
Angiotensin IV, formed from the action of APN on angiotensin III (Kugler, 1982;
Palmieri et al., 1989), appears to exhibit both the same properties as angiotensin II
via activation of AT1 receptors as a weak agonist, and specific properties via its
own putative receptors. Gardiner et al. (1993) noted that angiotensin IV-induced
reductions in renal and mesenteric blood flows and vascular conductances in
conscious rats were blocked by losartan. In agreement with these findings,
Fitzgerald et al. (1999) noted angiotensin IV-induced reductions in renal artery
blood flow, which were blocked by losartan, suggesting mediation by AT1
receptors. Champion et al. (1998, 1999) also reported that candesartan decreased
pressor responses to angiotensin IV in the anesthetized rat and the cat mesenteric
vascular bed with a shift to the right of the dose-response curve. Similarly,
angiotensin IV, although less potent than angiotensin II and angiotensin III,
produced a pressor response after i.c.v. injection, which was inhibited by losartan
(Wright et al., 1996).
In contrast, Kramar et al. (1997) and Coleman et al. (1998) reported that
angiotensin IV-induced elevation of cerebral and renal cortical blood flow was
12

blocked by a specific antagonist divalinal-angiotensin IV, and not by losartan or
PD123319. In a related study, Kramer et al. (1998) noted that pretreatment with the
NO synthase inhibitor, Nω-nitro-L-arginine (L-NAME) blocked the vasodilatory
effect of angiotensin IV on rat cerebral vasculature, suggesting that the latter action
is dependent upon the synthesis and release of NO from vascular endothelial cells.
Coleman et al. (1998) obtained similar results concerning kidney cortical blood
flow. Recently, Hill-Kapturczak et al. (1999) and Patel et al. (1998) suggested that
angiotensin IV mediated the angiotensin II-induced NO release and increase in
constitutive nitric oxide synthase (cNOS) activity, respectively, via the AT4
receptor in porcine pulmonary arterial endothelial cells since divalinal-angiotensin
IV blocked both angiotensin II- and angiotensin IV-induced NO release and
increases in cNOS activity while AT1 and AT2 blockade failed to influence these
responses. Interestingly, AT1 and AT4 receptors often mediate opposite effects.
Angiotensin IV has also been reported to block angiotensin II-induced RNA and
protein synthesis in chick cardiocytes (Baker et al., 1990, 1992), suggesting a
potential role for the angiotensin IV system in cardiac hypertrophy. Brazsko and
collegues (1988, 1991) established that i.c.v. injected angiotensin II and angiotensin
IV were equivalent at facilitating exploratory behaviour in rats tested in an open
field, and improved recall of passive avoidance conditioning and acquisition of
active avoidance conditioning. Divalinal-angiotensin IV disrupted recall of this
response (Wright et al., 1995), implicating the angiotensin IV system in memory
acquisition and recall. The binding site for angiotensin IV has recently been
13

identified as insulin-regulated aminopeptidase (IRAP), a transmembrane enzyme,
based on the fact that the two proteins share several pharmacological and
biochemical properties (Caron et al., 2003). This binding site also binds the
endogenous ligand, LVV-hemorphin-7, with high affinity and elicits similar
physiological effects as activation by the angiotensin IV ligand (Lee et al., 2003).
The identification of additional functions awaits further elucidation of this new
receptor system.
The degradation pathways of angiotensin IV are not yet fully elucidated but APN,
dipeptidylaminopeptidase (DAP) and carboxypeptidase N (CPN) have been
implicated in its N- and C-terminal degradation (De Silva et al., 1988; Welches et
al., 1991; Chansel et al., 1998). The possible degradation products of angiotensin IV
include the N-terminal-deleted angiotensin (4-8) and angiotensin (5-8), and the C-
terminal-deleted angiotensin (3-7) (Figure 1.2).
1.2.5 Angiotensin (1-7)
Angiotensin I can be processed into angiotensin (1-7) by prolylendopeptidase
(Welches et al., 1991) and three tissue endopeptidases, neutral endopeptidase (NEP)
24.11, NEP 24.15 and NEP 24.26 (Yamamoto et al., 1992; Ferrario et al., 1997).
Angiotensin (1-7) can also be derived from angiotensin II by the action of
prolylendopeptidase or carboxypeptidases. Once formed, angiotensin (1-7) can be
metabolized by aminopeptidases to generate angiotensin (2-7) and angiotensin (3-
7). ACE hydrolysis of angiotensin (1-7) to generate angiotensin (1-5) is recently
14

demonstrated to be an important route for inactivation of circulating and, possibly,
tissue angiotensin (1-7) (Yamada et al., 1998; Chappell et al., 2000).
The same receptor duality has been demonstrated for angiotensin (1-7). This
peptide exhibits several effects that are blocked by AT1 antagonists, including the
release of 3H-noradrenaline from rat atria (Gironacci et al., 1994) and the increase
in fluid absorption in the proximal tubule (Garcia et al., 1994) and in Henle’s loop
(Vallon et al., 1997). In addition to the AT1 receptors, angiotensin (1-7) recognizes
its own receptors, which have been described in a number of preparations (Diz and
Ferrario, 1996; Tallant et al., 1997).
Although a specific receptor for angiotensin (1-7) has yet to be cloned, there are a
number of evidence for its existence that are based on (i) opposing and/or
differential actions of angiotensin (1-7) when compared to angiotensin II, which
includes facilitation of baroreflex sensitivity (Benter et al., 1995; Oliveira et al.,
1996), absence of dipsogenic (Mahon et al., 1995) and pressor effect (Campagnole-
Santos et al., 1992) after i.c.v. injection, vasodilation (Benter et al., 1995), anti-
proliferative (Freeman et al., 1996) and anti-angiogenic actions (Machodo et al.,
2000) and increase in diuresis and natriuresis (Handa et al., 1996); (ii) the
characterization of a selective angiotensin (1-7) antagonist, D-Ala7-angiotensin (1-
7), which antagonized central and peripheral actions of angiotensin (1-7) (Ambuhl
et al., 1994; Bomtempo et al., 1998; Vallon et al., 1998; Widdop et al., 1999); and
(iii) the non-interference of D-Ala7-angiotensin (1-7) with the pressor, myotropic or
15

dipsogenic effect of angiotensin II or binding of 125I-angiotensin II to cortical or
medullary adrenal membranes that are rich in AT1 and AT2 receptors, respectively
(Santos et al., 1994).
1.2.6 des-Asp-angiotensin I
The formation of angiotensin III from angiotensin I via des-Asp-angiotensin I was
first described by Blair-West et al. (1971). In this pathway, angiotensin I undergoes
enzymatic NH2-terminal degradation to form des-Asp-angiotensin I, bypassing
ACE action to form angiotensin II. Des-Asp-angiotensin I is subsequently
metabolized by ACE to angiotensin III. Homogenates of endothelium, vascular
smooth muscle and hypothalamus was found to convert exogenous angiotensin I to
des-Asp-angiotensin I instead of angiotensin II (Sim MK, 1993; Sim and Qiu, 1994;
Sim et al., 1994a). The enzyme responsible for this conversion was found to be a
novel specific aminopeptidase (named aminopeptidase X) that is not inhibited by
EDTA, bestatin or amastatin (Sim et al., 1994). The existence of this specific
pathway and functional studies on des-Asp-angiotensin I seem to indicate that des-
Asp-angiotensin I is a likely functional angiotensin peptide of the RAS.
The significant increase in activity of aminopeptidase X in the hypothalamus of the
SHR suggests that in this hypertensive animal, the degradation of angiotensin I to
angiotensin II is shunted in favour of des-Asp-angiotensin I (Sim and Lim, 1997),
indicating that des-Asp-angiotensin I is possibly associated with blood pressure
regulation and hypertension. This role is supported by the ability of des-Asp-
16

angiotensin I to attenuate dose-dependently the central pressor actions of
angiotensin II and angiotensin III in both SHR and normotensive WKY rats (Sim
and Radhakrishnan, 1994).
In the heart, orally or intravenously administered des-Asp-angiotensin I attenuated
the development of experimentally-induced cardiac hypertrophy which was
comparable to the attenuation produced by losartan; the des-Asp-angiotensin I-
induced attenuation was blocked by indomethacin (Sim and Min, 1998). Isolated
tissue studies demonstrated that des-Asp-angiotensin I relaxed pre-contracted rabbit
pulmonary trunk strips but further contracted pre-contracted pulmonary artery
strips. Both des-Asp-angiotensin I-induced opposing actions were inhibited by
losartan, but not by PD123319; only the des-Asp-angiotensin I-induced relaxation
was inhibited by indomethacin (Sim and Chai, 1996). Binding studies also revealed
that the angiotensin receptor exists in two guanine nucleotide-differentiated
subtypes in the same pulmonary trunk and artery (Sim and Lim, 1998).
In the RAS, it is apparent that angiotensin peptides may bind to multiple receptor
subtypes that often exhibit different, and sometimes opposing, actions. For
example, angiotensin II has been shown to bind to both AT1 and AT2 receptors,
which are coupled to different effector systems and elicit different biological
responses. In addition, the signaling from the RAS appears to have an additional
level of complexity arising from extracellular processing of the ligand, the
17

metabolites of which bind the same or different receptors and induce additional
effects.
1.3 Angiotensin Receptors
Angiotensin II mediates its effects via at least two cell surface receptors, AT1 and
AT2. Both subtypes have been cloned and pharmacologically characterized and
belong to the G-protein coupled receptor (GPCR) superfamily. Pharmacologically
the receptors can be distinguished according to inhibition by specific antagonists,
e.g., biphenylimidazoles such as losartan for AT1 receptors and
tetrahydroimidazopyridines such as PD123319 for AT2 receptors (de Gasparo et al.,
1995; Ardaillou, 1999). Two other receptors (AT3 and AT4) have recently been
proposed but their transduction mechanisms are unknown and they have not yet
been cloned.
1.3.1 Distribution in vasculature
AT1 receptors are predominant in the control of angiotensin II-induced vascular
functions (Sadoshima, 1998; de Gasparo et al., 2000). In the vasculature, AT1
receptors are present at high levels in smooth muscle cells and relatively low levels
in the adventitia and are undetectable in the endothelium (Zhuo et al., 1998; Allen
et al., 2000). Conversely, AT2 receptors predominate in the adventitia and are
detectable in the media (Zhuo et al., 1998).
18

1.3.2 AT1 receptor
Two AT1 receptor subtypes that are encoded by different genes have been described
in rodents. The AT1A (which is the predominant subtype in all tissues except
adrenal and pituitary glands) and the AT1B (predominant subtype in adrenal and
pituitary glands) have greater than 95% amino acid sequence identity (Iwai and
Inagami, 1992). AT1A and AT1B receptors exhibit similar ligand binding and signal
transduction properties but differ in their tissue distribution and transcriptional
regulation.
The human AT1 receptor contains 359 amino acids and is encoded by a single gene.
The existence of a second AT1 gene in humans was suggested by the isolation of a
human cDNA clone that differed from the known sequence in 10 of its 359 residues
(Konishi et al., 1994; Kuroda et al., 1994) and by Southern blot analysis (Mauzy et
al., 1992). However, Southern blot (Curnow et al., 1992; Yoshida et al., 1992;
Bergsma et al., 1992; Aiyar et al., 1994; Su et al., 1996) and single stranded
conformational polymorphism analyses (Bonnardeaux et al., 1994) performed by
other laboratories do not support the presence of a second gene in humans. In
addition, the analysis of the evolution of AT1 gene in the mouse, rat, bovine and
human was consistent with rodents possessing two similar but separate genes, and
with bovine and human having only a single class gene (Yoshida et al., 1992).
Hence, it was suggested that the novel human AT1 cDNA clone obtained by
Konishi and collegues probably corresponded to an unusual allelic form of the AT1
gene that is not generally present in the human population (Curnow KM, 1996). In
19

the rabbit, Southern analysis of genomic DNA similarly revealed a single gene
encoding the AT1 receptor (Burns et al., 1993; Aiyar et al., 1994).
The human AT1 gene contains five exons that produce mature RNAs that encode
two receptor isoforms as a result of alternative splicing (Curnow KM, 1996). Exon
5 contains the open reading frame for AT1 (referred to as the short isoform) while
transcripts containing exon 3 spliced to exon 5 (exons 3/5) encode a receptor with
an amino terminal extension of 32 amino acids (long isoform). The relative
abundance of the mRNA splice variants encoding the long and short isoforms varies
widely in human tissues, suggesting that the isoforms may be functionally distinct
(Martin et al., 2001). In a similar study, Martin and colleagues (2001) also
demonstrated that the exons 3/5 splice variant encodes the long isoform in vivo and
that it has a diminished affinity for angiotensin II (> 3-fold) when compared to the
short isoform. This reduced affinity corresponded to a shift to the right in the does-
response curve for angiotensin II-induced IP3 production and Ca2+ mobilization.
Interestingly, losartan cannot discriminate between the two human AT1 receptor
isoforms. However, the physiological and pathophysiological roles of the long and
short AT1 receptors remain to be investigated.
Structural variation produced by alternative splicing observed in many GPCRs has
resulted in differences in signal transduction. For example, Pantaloni et al. (1996)
reported a splice variant of the pituitary adenylate cyclase-activating polypeptide
(PACAP) receptor, characterized by a 21-amino-acid deletion in the N-terminal
20

extracellular domain, which resulted in the increased potency of PACAP-27 in PLC
stimulation. The existence of this splice variant is suggested to be a possible way to
fine-tune PLC stimulation by PACAP. Differences in G protein coupling affinities,
and consequently different modes of signal transduction, have also been
demonstrated in two alternatively-spliced isoforms of the dopamine D2 receptor
which differ by a 29-amino-acid insertion in the putative third intracellular loop of
the receptor (Picetti et al., 1997). Similarly, Pierce et al. (1998) demonstrated that
splice variants of the prostanoid EP1, EP3, FP and TP receptors differed not only in
their second messenger pathways but also in their levels of constitutive activity and
their desensitization.
1.3.3 AT2 receptor
The human and rodent AT2 receptors contain 363 amino acids with 99% sequence
identity between rat and mouse and 72% identity between rat and human (Ichiki et
al., 1994; Tsuzuki et al., 1994). The divergence between rodent and human AT2
occurs mainly in the N-terminal region. AT1 and AT2 receptors have only 33 to
24% amino acid sequence identity (Kambayashi et al., 1993; Nakajima et al., 1993).
The residues in the transmembrane hydrophobic domains of the receptor which are
considered to be important for angiotensin II binding tended to be preserved, while
extensive differences between the AT1 and AT2 receptors are seen in the third
intracellular loop and the carboxyl terminal tail.
21

AT2 receptor expression is ubiquitous in the fetus but declines precipitously after
birth in many but not all tissues (de Gasparo et al., 2000). For example, it decreases
to undetectable levels in the skin after birth but in the adrenal and heart, the decline
stops at certain levels, and AT2 receptor expression persists for life (de Gasparo et
al., 2000). However, AT2 receptor expression can be up-regulated after tissue
injury, e.g., during wound healing of the skin (Kimura et al., 1992; Viswanathan
and Saavedra, 1992) and post balloon catheterization of rat carotid artery (Janiak et
al., 1992; Viswanathan et al., 1994). It is therefore postulated to play the role of a
modulator of biological programs in tissue development and repair.
Recent evidence also suggests that the AT2 receptor may have a physiological role
in the regulation of blood pressure, and may antagonize AT1-mediated effects by
inhibiting cell growth and by inducing apoptosis and vasodilation (Horiuchi et al.,
1997; Touyz et al., 1999b). Other novel, physiological effects attributed to the AT2
receptor include modulation of thirst, behaviour, and locomotor activity (Hein et al.,
1995; Ichiki et al., 1995).
1.3.4 AT3 receptor
A binding site observed in the Neuro-2a mouse neuroblastoma cell line that was not
blocked by losartan or PD123319, not affected by GTP analogs and has a low
affinity for angiotensin III, was assigned the AT3 receptor (Chaki and Inagami,
1992). It may however be more appropriate to classify it as a non-AT1-non AT2 site
until more information about its nature has been obtained.
22

1.3.5 AT4 receptor
The AT4 receptor binds angiotensin IV and specific antagonist divalinal-angiotensin
IV, but not losartan or PD 123319, and is prominently expressed in brain structures
concerned with cognitive processing, motor and sensory functions (Wright et al.,
1995). Peripheral tissues that reveal heavy distributions of AT4 sites are the kidney,
bladder, heart, spleen, prostate, adrenals and colon (de Gasparo et al., 2000). The
physiological functions so far associated with the AT4 receptor include memory
acquisition and recall, regulation of blood flow, inhibition of renal tubular
reabsorption, and cardiac hypertrophy (Braszko et al., 1988, 1991; Baker et al.,
1990, 1992; Kramer et al., 1997; Coleman et al., 1998; Handa et al., 1998).
1.4 AT1 Signaling Pathways in the Vasculature
Angiotensin II elicits complex and highly regulated cascades of intracellular signal
transduction that lead to short term vascular effects, such as contraction, and to
long-term biological effects, such as cell growth, migration, extracellular matrix
deposition, and inflammation (Touyz et al., 2000). The signal transducers
associated with the AT1 receptor include adenylate cyclase and phospholipases C, D
and A2 (PLC, PLD and PLA2) (Figure 1.3). The signaling processes are multiphasic
with distinct temporal characteristics. Immediate, early and late signaling events
occur within seconds, minutes, and hours, respectively.
23

A n g II
C O N TR A C TIO N
R E LA XA T IO N
IP 3 D A G
C a P K C
N A +-H +
intra ce llula r p H
PA
PIP2 P C PC
PL C P LD
P P
A A
PL A 2
Eic os a no ids
C a
p lasm am em b ran eA T 1 r e c
G p rote in
DAG l ipa se
R as /M AP K p ath w a y
Figure 1.3 Angiotensin AT1 receptor-mediated signaling pathways in vascular smooth muscle cells. Binding of angiotensin II to the AT1 receptor stimulates the activation of phospholipase C (PLC), phospholipase D (PLD) and phospholipase A2 (PLA2). PLC activation leads to phosphatidylinositol-4,5-biphosphate (PIP2) hydrolysis and the formation of inositol triphosphate (IP3) and diacylglycerol (DAG). IP3 releases Ca2+ (Ca) from sarcoplasmic reticular stores, and DAG activates protein kinase C (PKC), which in turn activates the Na+/H+ exchanger (Na+-H+). This latter event leads to intracellular alkalinization and together with the increase in intracellular Ca results in vascular smooth muscle contraction. Ca influx is also stimulated. PLD activation results in the hydrolysis of phosphatidylcholine (PC) to phosphatidic acid (PA), which can be converted to DAG by phosphatidic acid phosphorylase (PP). PLA2 activation results in the production of arachidonic acid which is processed into eicosanoids. These eicosanoids attenuate angiotensin responses by enhancing or attenuating angiotensin-induced vasoconstriction.
24

Vascular AT1-mediated signaling mechanisms that occur within seconds of ligand
binding include (a) G protein-mediated PLC activation, and subsequent formation
of inositol triphosphate (IP3) and diacylglycerol (DAG), (b) increase in intracellular
free calcium concentration by mobilizing intracellular Ca2+ and increasing Ca2+
influx, (c) activation of protein kinase C (PKC), (d) intracellular alkalinization via
stimulation of Na+/H+ exchanger, (e) increase in intracellular free sodium
concentration and decrease intracellular free magnesium concentration, and (f)
activation of Src family of kinases.
In addition to rapid signaling events, the vascular AT1 receptor also mediates early
signaling events that include (a) phospholipase A2 (PLA2) activation and
arachidonic acid metabolism, (b) phospholipase D (PLD) activation, (c) modulation
of cyclic nucleotides via adenylate and guanylate cyclases, (d) tyrosine kinase
phosphorylation (activation), and (e) mitogen-activated protein kinase (MAPK)
activation.
1.4.1 Stimulation of phospholipase C and inositol phosphate signaling
Activation of the AT1 receptor results in a rapid, PLC-dependent hydrolysis of
phosphatidylinositol-4,5-biphosphate (PIP2) to yield water soluble IP3 and
membrane bound DAG (Griendling et al., 1989) (Figure 1.3). There are at least
three isoforms of PLC: PLC-β, PLC-γ and PLC-δ (Rhee and Choi, 1992). PLC-β
isoforms are regulated by Gq/11 proteins (Smrcka et al., 1991), whereas PLC-γ
isoforms are regulated by tyrosine phosphorylation (Marrero et al., 1994). PLC-δ
25

regulation is unclear, but may involve intracellular Ca2+. All three isoforms have
been identified in vascular smooth muscle cells (VSMCs) (Schelling et al., 1991;
Ushio-Fukai et al., 1998). PLC-β appears to be important in the rapid generation of
IP3 (within 15 s), whereas PLC-γ seems to play a role in the later phase of IP3
formation (Ushio-Fukai et al., 1998). IP3 stimulates release of Ca2+ from
sarcoplasmic/endoplasmic reticular stores (which constitute the initial Ca2+ transient
phase) and DAG, with cofactors phosphatidylserine and Ca2+, activates PKC.
1.4.2 Increase in intracellular calcium
Exact mechanisms whereby AT1 activation stimulates subsequent Ca2+ influx (the
second Ca2+ phase) are unclear and may involve voltage-dependent calcium
channels, Ca2+-permeable and nonspecific dihydropyridine-sensitive cation
channels, receptor-gated Ca2+ channels, Ca2+-activated Ca2+ release channels, and
activation of the Na+/Ca2+ exchanger (Arnaudeau et al. 1996; Lu et al., 1996).
Transmembrane Ca2+ influx appears to contribute to the sustained AT1-induced
vasoconstriction (Ruan and Arendshorst, 1996b).
1.4.3 Regulation of smooth muscle contraction and relaxation
Smooth muscle contraction is regulated by the intracellular Ca2+ concentration and
by the Ca2+ sensitivity of the regulatory light chains of myosin (MLC20) (Somlyo et
al., 1994). The Ca2+ sensitivity of MLC20 is determined by the phosphorylation and
dephosphorylation of MLC20 catalyzed by Ca-calmodulin-activated myosin light-
chain kinase (MLCK) and myosin light-chain phosphatase (MLCP), respectively.
26

The amplitude of force generation thus depends on the balance of activities of
MLCK and MLCP. MLCK and MLCP are therefore targets for intracellular
signaling cascades, whose activities can be modulated independent of changes in
Ca2+. Smooth muscle tone appears to depend on a network of activating and
inhibiting intracellular signals integrating incoming extracellular signals where Ca2+
is just one, albeit important, player.
The angiotensin II-induced increase in intracellular Ca2+ results in the binding of
Ca2+ to calmodulin. Association of the Ca2+-calmodulin complex with the catalytic
subunit of MLCK activates this enzyme. MLCK then phosphorylates serine at
position 19 on MLC20, allowing the myosin ATPase to be activated by actin and the
muscle to contract. Conversely, a decrease in intracellular Ca2+ causes inactivation
of MLCK, thus permitting the dephosphorylation of MLC20 by MLCP and
subsequent deactivation of the actomyosin ATPase, resulting in relaxation (Somlyo
et al., 1994; Pfitzer G, 2001) (Figure 1.4).
In addition, recent evidence has demonstrated that angiotensin II can increase the
Ca2+ sensitivity of MLC20 by modifying, independently of Ca2+, the activity of the
MLCP (Seko et al., 2003). The major mechanism of G-protein coupled Ca2+
sensitization is the inhibition of MLCP, resulting in an increase in MLC20
phosphorylation, and hence contractile force, at a given intracellular Ca2+
concentration (Kitazawa et al., 1991). The inhibition of MLCP is mediated
primarily by a PKC- and Rho-kinase- (RhoA-activated kinase) dependent
27

AT1 rec plasma membrane
AngII
G protein
IP3SRCa
Ca
Calmodulin
Ca/Calmodulin complex
activated MLCK
myosinmyosin P
CONTRACTION
inactivated MLCK
inactivated myosin ATPase
activated myosin ATPase
RELAXATION
Ca
MLCP
Figure 1.4 Regulation of smooth muscle contraction and relaxation. Angiotensin II-induced increase in intracellular Ca results in binding of Ca to calmodulin. Association of the Ca-calmodulin complex with myosin light chain kinase (MLCK) causes MLCK activation and the subsequent phosphorylation of the regulatory light chains of myosin. This activates myosin ATPase resulting in contraction. A decrease in intracellular Ca results in inactivation of MLCK and this permits myosin light chain phosphatase (MLCP) to dephosphorylate myosin, resulting in deactivation of myosin ATPase and relaxation.
28

phosphorylation of CPI-17, an endogenous protein inhibitor of MLCP, at Thr-38,
via Gq/G11 and G12/G13 proteins (Kitazawa et al., 1991; Gohla et al., 2000; Niiro et
al., 2003; Seko et al., 2003) (Figure 1.5). It has been suggested that atypical PKCs
act upstream of Rho-kinase and are involved in the activation pathway of Rho
kinase although its mechanism is unclear (Gailly et al., 1997; Niiro et al., 2003).
Rho kinase is one of the major downstream targets of the monomeric GTPase
RhoA; RhoA is activated upon the exchange of bound GDP for GTP and its activity
is regulated by GTPase activating proteins (GAPs) and guanosine exchange factors
(GEFs) (Laufs and Liao, 2000; Somlyo and Somlyo, 2000). Angiotensin II was
demonstrated to cause RhoA activation in rat VSMCs and rabbit clitoral
cavernosum smooth muscle (Park et al., 2002; Seko et al., 2003) but not in isolated
rabbit aortic tissue (Sakurada et al., 2001). The role of RhoA in mediating the
signaling mechanism of angiotensin II-mediated vasoconstriction remains to be
determined. Other proposed mechanisms of MLCP inhibition include Rho-kinase-
induced phosphorylation of the myosin binding unit (MBS) of MLCP at Thr-641
and dissociation of MLCP by arachidonic acid (Gong et al., 1995; Hartshorne et al.,
1998).
1.4.4 Activation of protein kinase C and intracellular alkalinization
AT1 activation also stimulates the translocation of cytosolic PKC to the plasma
membrane where the activated enzyme phosphorylates specific proteins associated
with vascular function e.g., insulin receptor, glucose transporter, β-adrenergic
29

inactiveMLCP
myosinmyosin P CONTRACTIONRELAXATION
activeMLCK
activeMLCP
GTP-RhoA(active)
GDP-RhoA(inactive)
Rho-kinase
P
ATP
inactiveMLCP
CPI-17
CPI-17
PAA
PKC
inhibitor
GEF GAP
Ca
Calmodulin
Ca-Calmodulin complex
dissociation
Figure 1.5 Modulation of the Ca sensitivity of myosin by modifying the activities of MLCK and MLCP. MLCP can be inhibited by phosphorylated CPI-17 via a PKC- and Rho-kinase-dependent pathway. Arachidonic acid inhibits MCLP activity by dissociation of MLCP. Rho-kinase is the downstream effector of RhoA, which is activated by guanosine exchange factors (GEF) and inactivated by GTPase-activating proteins (GAP).
30

receptors, tyrosine kinase, cytochrome P450, HMG-CoA reductase (Walsh et al.,
1996; Damron et al., 1998). PKC is implicated in AT1-induced vascular contraction
as well as vascular smooth muscle cell growth (Rasmussen et al., 1987; Ruan and
Arendshorst, 1996a; Oriji and Keiser, 1997; Kirton and Loutzenhiser, 1998). PKC
activation of the Na+/H+ exchanger and the resultant intracellular alkalinazation
leads to vasoconstriction in some vascular beds by increasing Na+ and Ca2+ and by
sensitizing the contractile machinery to Ca2+ (Grinstein et al., 1989; Carr et al.,
1995; Ye, 1996; Tepel et al., 1998; Touyz et al., 1999a) (Figure 1.3).
1.4.5 Activation of Src family kinases
c-Src (one of at least 14 Src-related kinases identified) is phosphorylated when the
AT1 receptor is activated, with maximal activation occurring within 60s (Ishida et
al., 1995, 1998; Marrero et al., 1995; Touyz et al., 1999a). Src plays an important
role in AT1-induced PLC-γ phosphorylation and IP3 formation. AT1-induced Ca2+
concentration responses in human VSMCs are mediated, in part, via Src-dependent
mechanisms (Touyz et al., 2001).
1.4.6 Phospholipase A2 activation and arachidonic acid metabolism
In addition to rapid signaling events described above, early signaling processes,
such as the activation of PLA2 and arachidonic acid (AA) metabolism, are
simulated by AT1 activation within minutes (Rao et al., 1994). PLA2-derived
eicosanoids influence vascular mechanisms important in blood pressure regulation,
by both prohypertensive and antihypertensive mechanisms (Nasjletti, 1998). At
31

least three types of PLA2 exists: a low-molecular-weight (14-15 kDa) calcium-
dependent secreted PLA2 (sPLA2) which are subdivided into three groups (I, II and
III), a high-molecular-weight (80-160 kDa) calcium-dependent cytosolic PLA2
(cPLA2), and a calcium-independent PLA2 (iPLA2) (approximately 40 kDa)
(Dennis, 1997, 1994; Mayer et al., 1993; Clark et al., 1991; Hazen et al., 1990). The
high specificity of cPLA2 for sn-2-arachidonoyl-containing phospholipids and its
detection in a large variety of cells suggest that cPLA2 plays an important role in the
generation of AA-derived signaling molecules, although the involvement of other
PLA2 cannot be ruled out. Angiotensin II-elicited phosphorylation and activation of
cytosolic PLA2 (cPLA2) is dependent on intracellular Ca2+, Ca2+-calmodulin-
dependent protein kinase (CaM kinase II) and mitogen-activated protein kinase
(MAPK) (Muthalif et al., 1998). Ca2+ is not required for cPLA2 activity but serves
as a stimulus to translocate the enzyme from the cytoplasm to the membrane, where
its substrate, phospholipids, is localized (Clark et al., 1991). cPLA2 is a substrate for
MAPK (Lin et al., 1993). MAPK phosphorylates cPLA2 at Ser-505 and recent
evidence suggests that both CaM kinase II and MAPK are involved in the activation
of cPLA2 (Clark et al., 1995; Muthalif et al., 1998). The findings also suggest that
CaM kinase II acts upstream of MAPK in the activation of cPLA2 (Muthalif et al.,
1998).
PLA2 activation results in the release of arachidonic acid (AA) in vascular smooth
muscle from cell membrane phospholipids (Bonventre, 1992; Rao et al., 1994)
(Figure 1.3). Released AA is processed by (i) cyclooxygenases to the five major
32

prostanoids, thromboxane A2 (TXA2), prostaglandin (PG) I2, PGE2, PGD2 and
PGF2α (Smith et al., 1991), (ii) lipooxygenases to hydroxyeicosatetraenoic acids
(HETEs) and leukotrienes (LT) (Yamamoto et al., 1992), or (iii) cytochrome P450
oxygenases to epoxyeicosatrieenoic acids, 20- and 19- HETE and other HETEs
(Harder et al., 1995; Dennis, 1997) (Figure 1.6).
These eicosanoids may act both as intracellular second messengers by modifying
the activity of intracellular enzymes and ionic channels, and as local mediators
(autocoids) by being released outside the cell of origin and binding to specific cell
surface prostanoid receptors of neighbouring cells. TXA2 is produced mainly by
platelets and contracts smooth muscle and induces platelet aggregation. In contrast,
PGI2 and PGE2, the major vasodilator prostaglandins produced in the vasculature
(Hassid and Williams, 1983; Schror, 1993), are produced by vascular endothelial
and smooth muscle cells and strongly inhibit platelet aggregation (mediated by PGI2
only) and relax smooth muscle, thus attenuating the vasoconstriction induced by
angiotensin II (Wilcox and Lin, 1993). The interplay between prohypertensive and
antihypertensive functions subserved by cyclooxygenase- and lipoxygenase-derived
eicosanoids determines its modulatory effect on vascular responses to angiotensin.
Several lines of evidence suggest that the contractile effects of eicosanoids on
smooth muscle may be mediated by the release of calcium. In contrast, their
relaxation effects may be mediated by the generation of cAMP via the GS protein
(Turcato et al., 1999; Ruan et al., 1999; Wise and Jones, 1996), although cAMP
independent pathways, e.g., activation of ATP-sensitive and Ca2+-activated K+
33

AT1 rec plasma membrane
AngII
PLA2
phosphatidylcholine arachidonic acid
Cyclooxygenase Cytochrome P450Lipooxygenase
HETEsEETsHETEsPGG2
PGH2
PGI synthase
PGI2PGE synthase
PGE2
6-keto-PGF1a
PGF2a PGD2
PGD synthase
TXA synthase
TXA2
TXB2
5-HPETE
LTA4
LTB4 LTC4
LTD4LTE4
dehydrase
Figure 1.6 Arachidonic acid metabolism. PG: prostaglandin, TX: thromboxane, LT: leukotriene, HETE: hydroxyeicosatetraenoic acid.
34

channels (KCa), may be involved (Jackson et al., 1993; Bouchard et al., 1994;
Schubert et al., 1997; Clapp et al., 1998; Purdy et al., 2001).
1.4.7 PLD activation
Angiotensin II also activates PLD, which hydrolyzes phosphatidylcholine (PC) to
choline and phosphatidic acid (Figure 1.3). Angiotensin II coupling to PLD
activation is suggested to be mediated by Gα12 and Gβγ via pp60c-src- and RhoA-
dependent mechanisms (Ushio-Fukai et al., 1999). In VSMCs, phosphatidic acid is
rapidly converted to DAG by phosphatidic acid phosphohydrolase, and arachidonic
acid is generated by the action of diacylglycerol lipase on diacylglycerol (Billah,
1993). Hence, the sustained PLD activation by angiotensin II plays an important
role in VSMC signaling, e.g., it contributes, in part, to the sustained production of
prostaglandins in VSMCs (Gomez-Cambronero et al., 1998). Recent studies using
rat and rabbit aortic VSMCs suggests that the angiotensin II-induced increase in
PLD activity is mediated by AA and/or its metabolites generated via cytochrome
P450 oxygenase and lipoxygenase as a result of cPLA2 stimulation (Shinoda et al.,
1997; Parmentier et al., 2001). These AA metabolites activate PLD via the ras/MAP
kinase pathway, which releases further arachidonic acid through the phosphatidate
phosphohydrolase/diacylglycerol lipase pathway. DAG is also the physiological
activator of PKC. This PLD pathway is the most important source of phosphatidic
acid and DAG and probably represents the major pathway by which PKC remains
activated in VSMCs (Lassegue et al., 1993; Dhalla et al., 1997).
35

1.4.8 Modulation of cyclic nucleotides
Angiotensin II has been shown to increase cyclic nucleotides adenosine 3’,5’-cyclic
monophosphate (cAMP) and guanosine 3’,5’-cyclic monophosphate (cGMP)
concentrations directly in VSMCs via activation of vascular or endothelial AT1
receptors (Hassid, 1986 ; Boulanger et al., 1995; Magness et al., 1996). The cAMP
and cGMP, which are generated intracellularly within minutes by adenylate cyclase
and guanylate cyclase, activate downstream targets including cAMP-dependent
kinase (PKA), cGMP-dependent kinase (PKG), intracellular Ca2+ and ionic
channels (Bentley and Beavo, 1992). PKA has been shown to phosphorylate the
calmodulin-binding domain of MLCK (site A) at a specific serine residue in vitro,
leading to a reduced affinity of MCLK for the Ca2+-calmodulin complex (Conti et
al., 1981). However, agonists that elevate cAMP in vivo had negligible effects on
MLCK phosphorylation and Ca2+ desensitization in bovine tracheal smooth muscle
(Stull et al., 1990), suggesting that cAMP desensitizes smooth muscle by an
alternative mechanism. PKA and PKG have also been shown to phosphorylate
RhoA at serine 188 and inactivate RhoA signaling, possibly by inhibiting RhoA
membrane translocation (Lang et al., 1996, Sawada et al., 2001). Since Rho-kinase
has been suggested to mediate the inhibition of MLCP (Seko et al., 2003), RhoA
inactivation increases MLCP activity and decreases Ca2+ sensitivity of
phosphorylation, leading to decreased myosin phosphorylation and attenuation of
smooth muscle contraction, or smooth muscle relaxation, upon agonist stimulation.
PKG was also shown to activate MLCP directly by phosphorylating the myosin
binding site of MLCP via a leucine zipper interaction (Lee et al., 1997; Surks et al.,
36

1999). In addition, other proposed mechanisms of cyclic-nucleotide-dependent
vasorelaxation include decreasing intracellular Ca2+ (McDaniel et al., 1991),
phosphorylation of IP3 receptor (Komalavilas et al., 1996) and phospholamban, an
inhibitor of smooth muscle sarcoplasmic reticulum Ca2+-ATPase (Lincoln and
Cornwell, 1991), activation of plasma membrane Ca2+-ATPase (Kimura et al.,
1982; Furakawa et al., 1988) and KCa, the latter inducing hyperpolarization and
reducing Ca2+ influx as a result of closure of voltage-gated L-type Ca2+ channels
(Thornbury et al., 1991; Schubert et al., 1996; Orlov et al., 1999).
1.4.9 Tyrosine kinase phosphorylation
It has recently become apparent that tyrosine phosphorylation plays an important
role in the signaling pathways of the AT1 receptor despite the fact that the AT1
receptor, unlike most growth factor receptors, harbors no intrinsic kinase activity.
Tyrosine phosphorylated proteins in VSMC include the AT1 receptor itself, PLC-γ
and Src family kinases, as well as JAK and TYK, FAK, Pyk2, p130cas, and
phosphatidylinositol 3-kinase (PI3K). Only Fyn and c-Src of the Src family kinases
are expressed in VSMC (Sayeski et al., 1998). The net effect of tyrosine
phosphorylation, and thus activation, of Fyn and c-Src is the subsequent facilitation
of guanine nucleotide exchange of Ras-GDP to Ras-GTP (i.e. Ras activation) via
the Shc-Grb2-Sos pathway (Schieffer et al., 1996; Sadoshima and Izumo, 1996).
Activated Ras-GTP interacts with the Ser/Thr kinase Raf (mitogen-activated protein
kinase kinase kinase (MAPKKK)), which translocates to the cell membrane. Raf
phosphorylates MAPKK (MAPK kinase), which in turn activates MAPK. Once
37

phosphorylated, MAPKs translocate to the nucleus to phosphorylate transcription
factors and thereby regulate gene expression of cell cycle-related proteins
(Treisman, 1996).
JAKs are key mediators of mRNA expression. JAKs accomplish this by
phosphorylating the signal transducers and activators of transcription (STATs).
Phosphorylated STATs translocate to the nucleus where they bind to Sis-inducible
promotor elements and stimulate transcription of the early growth response genes
such as c-fos, c-jun and c-myc. Studies have now shown that angiotensin II directly
activates the JAK/STAT pathway via the AT1 receptor and this may be a
mechanism whereby angiotensin II influences vascular growth, remodeling and
repair (Berk and Corson, 1997; Hefti et al., 1997).
Angiotensin II rapidly activates FAK in VSMCs (Polte et al., 1994). Upon
phosphorylation, FAK translocates to focal adhesions where it phosphorylates
substrates such as paxillin and p130cas, thus promoting cytoskeletal arrangement
(Burridge et al., 1992). The tyrosine phosphorylation of paxillin correlates
temporally with the formation of focal adhesion contacts in VSMCs and suggests
that FAK may play a role in coordinating VSMC proliferation/remodeling with
changes in cell structure (Turner et al., 1995). On the other hand, the tyrosine
phosphorylation of p130cas correlates temporally with its ability to bind at least 11
different phosphate-containing proteins in response to angiotensin II, supporting the
concept that it is an adaptor molecule. Three of the 11 proteins have been identified
38

as c-Src, PKCα and the integrin signaling molecule pp120. Thus, it appears that
p130cas serves as a convergence point for three very different signaling pathways,
namely, the c-Src tyrosine kinase pathway, the Ser/Thr PKC pathway, and the cell
adhesion-mediated pp120 pathway.
Of the many GPCRs, the AT1 receptor seems to be one of the most important in
vascular smooth muscle cell regulation. Exact reasons for the apparent selective
importance of angiotensin II actions via AT1 receptors are unclear but may be due
to the ability of angiotensin II to amplify its vascular responses via other agonists.
Angiotensin II stimulates production of growth factors, e.g., platelet-derived growth
factor (PDGF), and vasoactive peptides, e.g., endothelin-1 (ET1), as well as
transactivates multiple receptors, such as PDGF receptor and epidermal growth
factor receptor (Kim and Iwao, 2000), thereby amplifying VSMC signaling
responses to angiotensin II. The end result, contraction, hypertrophy, or
proliferation, is determined by the selective activation of multiple signaling
pathways, and the phenotype of the stimulated VSMC.
1.5 Functional and Structural Complexity of Signal Transduction via
GPCRs
AT1 and AT2 receptors belong to the GPCR superfamily, which utilizes
heterotrimeric GTP-binding proteins (G proteins) to govern effector proteins. The
AT1 receptor, like other GPCRs, has been proposed to spontaneously isomerize
between its inactive (R) and active (R*) states as described in the extended ternary
39

complex model (Samama et al., 1993; Chidiac et al., 1994). In the absence of
agonists, the receptor is preferentially maintained in an inactive R conformation by
stabilizing intramolecular interactions, as evidenced by the constitutive activity of
mutated AT1 receptors (Noda et a., 1996; Groblewski et al., 1997; Balmforth et al.,
1997). Binding of angiotensin II presumably selects or induces an active R*
conformation that initiates intracellular signaling (Noda et al., 1995).
It has become apparent that the vascular AT1 receptor is able to couple to multiple
signal transduction pathways, with temporal organization of the disparate signals.
The exact mechanism by which a single AT1 receptor is able to do this is unclear.
Recent evidence suggests that the activated AT1 receptor undergoes several
transitions into multiple conformational states and this has been postulated as a
mechanism for coupling to multiple signal transduction pathways. For example, it
has been shown that the agonist-induced activation of the AT1 receptor appears to
be triggered by an initial interaction between Tyr4 residue of angiotensin II and the
Asn111 residue located in the third transmembrane domain of the receptor (Noda et
al., 1996). The interaction of Phe8 of angiotensin II with His256 in the sixth
transmembrane domain of the receptor then appears to drive the AT1 receptor into
its fully active R* state (Noda et al., 1995). Thomas et al. (2000) also demonstrated
that the conformation of the activated AT1 receptor for receptor phosphorylation is
distinct from the conformation required for inositol phosphate signaling. Evidence
for conformational selection has also been reported with other GPCRs, including
the human 5-HT2C receptor, PACAP receptors and dopamine D2 receptors (Meller
40

et al, 1992; Splengler et al., 1993; Berg et al., 1998), suggesting that this could be a
common mechanism for coupling of GPCRs to multiple signal transduction
pathways.
This proposed mechanism of receptor activation has several important implications.
Firstly, it may explain how a single receptor may couple to multiple G proteins
since different conformational states of R* may provide a structural means of
differentially coupling to different G proteins to mediate different effector
pathways, resulting in subtle differences of response of a single receptor to different
agonists.
Secondly, it may explain why different agonists, e.g., angiotensin IV, can have
different efficacy by their ability to preferentially select for one of several receptor
conformations through their ligand structure (Le et al., 2002). The preferred
conformation may couple with low efficacy to G proteins or may selectively
activate a subset of the multiple signal transduction pathways that may be coupled
to a single receptor subtype. This phenomenon is also known as agonist-directed
trafficking of receptor signals (Kenakin, 1995).
In addition, as in many other GPCRs, it was recently demonstrated that the AT1
receptor can assemble with the bradykinin receptor to form heterodimers, resulting
in enhanced G protein activation and altered receptor sequestration (AbdAlla et al.,
41

2000). The heterodimerization of the AT1 receptor with other receptors may provide
an additional mechanism of cell-specific regulation of angiotensin responses.
1.6 Role of RAS in Primary Pulmonary Hypertension (PPH)
Primary pulmonary hypertension (PPH) is a rare and serious disease of unknown
cause characterized by abnormally high pressure in the pulmonary artery in the
absence of secondary causes. The pathogenesis of PPH is currently not clearly
understood. However, there is evidence to suggest that a genetic susceptability and
an imbalance in endothelium-derived vasoconstrictors and vasodilators resulting
from endothelial cell injury are involved (Runo et al., 2003). The increased vascular
resistance seen in PPH has been attributed to two major factors: 1) vasoconstriction
and 2) thickening or remodeling of the vascular arterial wall. There is also a
tendency for blood clots to form within the small vessels.
Studies in PPH patients have shown an imbalance in the ratio of the metabolites of
prostacyclin and thromboxane (Christman et al., 1992). Other studies have shown
an impaired synthesis of the endothelial-derived vasodilator, nitric oxide, that could
be due to a reduced level or activity of nitric oxide synthetase (Giaid et al., 1995).
Endothelin, a potent endothelial-derived vasoconstrictor, has been found to be at
abnormally high levels in PPH patients (Giaid et al., 1993). Current standard
therapies for PPH include the use of calcium channel blockers (nifedipine,
diltiazem), continuous intravenous epoprosternol (PGI2) or lung transplantation.
However, calcium channel blockers are only effective in about 30% of patients.
42

Epoprosternol remains the most effective therapy for PPH with majority of patients
responding favourably to the treatment (Runo et al., 2003). Because the half-life of
epoprosternol is short, continuous intravenous delivery and placement of a long-
dwelling catheter are necessary. As a result, complications from the delivery
system, including exit-site infections and bleeding, paradoxical embolism,
bacteraemia or sepsis, and delivery malfunction that may result in sudden, in some
cases fatal, decompensation may occur. Therefore, there is an urgent need for
improved treatment modalities for the management of PPH and drugs currently in
clinical development include inhaled iloprost (PGI2 analog), endothelin ET-1
receptor antagonist (bosentan, sitaxsentan), phosphodiesterase inhibitors (sildenafil)
and thromboxane synthase inhibitors and receptor antagonists.
There is recent evidence to suggest that the RAS may have a role in the
pathogenesis of PPH. Orte et al. (2000) demonstrated an increased expression of
endothelial angiotensin-converting enzyme in the intra-acinar arteries in patients
with PPH. Schuster et al. (1996) similar demonstrated increased ACE
immunoreactivity in the endothelium and sub-endothelial neointimal regions of
pulmonary arteries from PPH patients, suggesting that locally produced angiotensin
II may contribute to the pathogenesis of PPH. In addition, irbesartan, an AT1
receptor antagonist, was recently shown to prevent lung structural remodeling and
pulmonary hypertension following myocardial infarct in rats (Jasmin et al., 2003).
The role of RAS in the pathogenesis of PPH and the potential development of
therapies targeting the RAS for the management of PPH awaits further clarification.
43

1.7 Conclusion
The RAS is a highly complex system that generates pleiotropic effects in many
target organs, including the brain, kidneys and vasculature. The recent successful
clinical use of ACE inhibitors and AT1 receptor antagonists suggests the importance
of the RAS in the pathophysiology of many cardiovascular diseases. Most of the
known effects of the RAS are mediated through the AT1 receptor. The recent
demonstration that there are several pathways for degradation of angiotensin I and
angiotensin II leading to different bioactive fragments with their own binding sites
raises the question of the relative importance of these pathways in fine-tuning or
regulating angiotensin responses. The recent report of functionally distinct AT1
receptor isoforms derived from alternative splicing of a single AT1 gene, differing
in a 32 amino acid amino terminal extension, raises the possibility that angiotensin
II responsiveness can be fine-tuned by regulating the relative expression of the long
and short isoforms in a given tissue. Additionally, a single GPCR can couple to
multiple G proteins and signal transduction pathways. All three levels of
complexity can contribute to a cogent response to fine-tune angiotensin responses.
Although there has been significant progress in the elucidation of angiotensin-
induced signal transduction, which is mediated by G proteins, it still remains
unclear how receptors direct specificity and coordination of multiple signals to
produce a desired concerted response. Understanding how G proteins coordinate
these responses would perhaps help shed some light on the complexities of
angiotensin signal transduction.
44

CHAPTER 2
FUNCTIONAL STUDIES ON ISOLATED RABBIT
PULMONARY TRUNK AND ARTERY
2.1 Introduction
The angiotensin receptors are classified into two main types, namely the angiotensin
AT1 and angiotensin AT2 receptors (de Gasparo et al., 2000). Based on the
existence of two separate cDNAs for the angiotensin AT1 receptor, the receptor is
known to consist of the two subtypes, AT1A and AT1B receptors (Kakar et al.,
1992a; Iwai et al., 1992). Both of these subtypes are blocked by losartan but not by
PD123319, which selectively blocks angiotensin AT2 receptors. VSMCs express
primarily AT1A receptors and they have been suggested to mediate vascular smooth
muscle constriction. The angiotensin AT1B receptor subtype does not seem to
mediate vasoconstriction in vascular tissue, it being found in the brain, pituitary and
adrenal glomerulosa (Kakar et al., 1992b).
Two recent functional studies in our laboratory using des-Asp-angiotensin I indicate
that the rabbit pulmonary trunk and artery contain two functionally opposing
subtypes of the losartan-sensitive angiotensin AT1 receptor (Sim and Soh, 1995;
Sim and Chai, 1996). The pulmonary artery contains predominantly one of the
receptor subtypes, which mediated contraction of the pre-contracted artery by des-
Asp-angiotensin I and is identifiable with the angiotensin AT1A receptor. The other
45

receptor subtype is found to co-exist with the former in the pulmonary trunk and
mediates relaxation of the preconstricted artery. In addition to its susceptibility to
losartan, this other subtype is indomethacin-sensitive and is suggested to be
identifiable with the angiotensin AT1B receptor described by Kakar et al. (Kakar et
al., 1992b; Iwai et al., 1992). These studies show for the first time the likely
function of the AT1B-like receptor subtype and the vasorelaxant action of an
endogenous angiotensin. The existence of the angiotensin AT1B-like receptor in the
pulmonary trunk has been supported in a recent binding study (Sim and Lim, 1998).
The purpose of the present study was therefore to further investigate the two
receptor subtypes using additional angiotensin peptide fragments, namely
angiotensin II, angiotensin III, angiotensin IV, angiotensin (1-7), angiotensin (4-8),
and angiotensin (3-7) and to decipher the possible roles the receptors may have in
regulating blood flow from the heart to the lung. In addition, the structure-activity
relationship of angiotensin IV was also investigated.
2.2 Materials and Methods
2.2.1 Isolation of rabbit pulmonary trunk and artery
The pulmonary trunk and arteries of male albino rabbits weighing 1.5 – 2.5 kg
supplied by local University Animal Centre were used throughout the study. Each
rabbit was killed by either cervical dislocation or carbon dioxide poisoning. No
difference in response was found with both methods of killing. The pulmonary
trunk (the vessel arising from the right ventricle prior to its bifurcation into the left
and right pulmonary arteries) and the two pulmonary arteries (vessels distal to
46

bifurcation) were rapidly removed and transferred into freshly prepared Krebs
solution (118mM NaCl, 5mM KCl, 1.2mM MgSO4, 1.2mM KH2PO4, 2.5mM
CaCl2.2H2O, 25mM NaHCO3, 10mM glucose.H2O, 0.026mM EDTA, 0.3mM
ascorbic acid) presaturated with carbogen (95% oxygen, 5% carbon dioxide).
Connective and adipose tissue surrounding the vessels were gently removed.
2.2.2 Preparation of pulmonary trunk and artery strips
The isolated pulmonary trunk and arteries were cut transversely into 3mm rings.
The rings were cut open into strips and were denuded of endothelium by gently
rubbing the luminal surface with cotton buds. The rationale for the use of an
endothelium-denuded preparation was to allow for the investigation of the
physiological effects of angiotensin peptides in a clean vascular smooth muscle
preparation without the interference of endothelium-derived factors.
The ends of the strips were secured with suture and suspended under an optimal
resting load of 2 g in a 20 ml organ bath maintained at 37oC containing Krebs
solution presaturated with carbogen. Contractions were recorded isometrically with
an Ugo Basile isometric transducer attached to a MacLab/8 Virtual Instrument via a
MacLab Quad Bridge Amplifier. A 60-minute equilibration period was allowed
before any experimentation was begun.
47

2.2.3 Direct actions of angiotensin peptides
After equilibration, a non-cumulative dose response for each of the five angiotensin
peptides tested (angiotensin II, angiotensin III, angiotensin IV, angiotensin (1-7)
and angiotensin (4-8)) was obtained. This was done by adding increasing
concentrations of each angiotensin peptide to the pulmonary trunk and artery strips.
For each concentration, contractions were allowed to reach their maxima. A 30-
minute washout and rest period was allowed before the next concentration of the
angiotensin peptide was added. The non-cumulative dose response was done to
determine the threshold and optimal concentration of the angiotensin peptides on
noradrenaline-contracted pulmonary trunk and artery strips.
The effects of 1 µM losartan, an AT1-selective receptor antagonist, on the response
to maximal-effect concentrations of 100 nM angiotensin II, 1 µM angiotensin III
and 10 µM angiotensin IV were studied by pre-incubating the strips with losartan
for 30minutes prior to addition of the peptides.
At the end of the experiment, each strip was contracted with 60 mM KCl. This was
defined as the maximum tissue response and all contractions to angiotensins were
expressed as a percentage of this maximum response.
2.2.4 Effects of angiotensin peptides on pre-contracted trunk and artery strips
Following equilibration, the sections were pre-contracted with 100 nM
noradrenaline. After the contractions had reached a steady plateau (at 5 minutes),
48

each of the five angiotensin peptides was added and the response observed for a
further 5 minutes. The tissue was pre-contracted to produce an elevated contractile
tone so that any relaxation to the angiotensin peptides could be observed. In this
experiment, the effect of angiotensin (3-7) on the pre-contracted trunk and artery
strips was also studied.
At the end of the experiment, the sections were contracted with 100 nM
noradrenaline. This was followed by the addition of 1 µM acetylcholine to test the
extent of endothelial denudation. All sections contracted to acetylcholine,
indicating that the sections were completely denuded of endothelium.
2.2.5 Effects of receptor antagonists and enzyme inhibitors
To characterize the receptor subtypes mediating the response of the precontracted
strips to angiotensins, the strips were pre-incubated with 1 µM losartan (selective
AT1 receptor antagonist) or 1 µM PD123319 (selective AT2 receptor antagonist)
during the 30-minute washout and rest period. The effects of the receptor
antagonists on the actions of angiotensin II, angiotensin III and angiotensin IV (the
peptides found to be vasoactive) were studied.
To determine the involvement of prostaglandins, 10 µM indomethacin (non-
selective cyclooxygenase inhibitor) was used in place of losartan and PD123319.
49

To investigate if angiotensin metabolites contributed to the response observed,
pulmonary tissue was similarly pre-incubated with 30 µM amastatin (a selective
aminopeptidase A and N inhibitor).
The effect of 1 µM divalinal-angiotensin IV (putative selective AT4 antagonist) on
angiotensin IV-induced relaxation in pre-contracted pulmonary trunk strips was also
determined.
2.2.6 Structure-activity relationship of angiotensin IV
To determine the structure activity relationship of angiotensin IV, six glycine-
substituted analogs of angiotensin IV (each of the six amino acids in angiotensin IV
was substituted by glycine, in turn) were added to noradrenaline pre-contracted
rabbit pulmonary trunk and artery strips as previously described. The responses of
the strips to each of the six angiotensin IV analogs were observed. To explore if
these analogs had any antagonistic actions, the tissue strips were preincubated with
each analog for 30 minutes before angiotensin IV was added to noradrenaline-
precontracted tissue.
2.2.7 Expression of results
The contraction from the resting tension caused by 100 nM noradrenaline was
defined as the control contraction and the effect of each angiotensin on the pre-
contracted section was expressed as a percentage change of this control contraction.
The concentrations of vasoactive angiotensins used in this particular study were
50

based on the results of a preliminary concentration response experiment. The
concentrations chosen for angiotensin II (100 nM), angiotensin III (50 nM) and
angiotensin IV (5 µM) were based on the reproducibility of responses with each
concentration.
2.2.8 Statistical analysis
The data is presented as means ± standard error of mean (SEM) for n observations.
The influences of losartan, PD123319 and indomethacin on the action of
angiotensin peptides on the pre-contracted trunk and artery sections were analysed
using ANOVA with Tukey’s multiple range test for a posteriori comparisons.
2.3 Results
2.3.1 Direct actions of angiotensin peptides
Of the 5 angiotensin peptides tested, angiotensin (1-7) and angiotensin (4-8) were
not vasoactive in these experiments. Angiotensin II, angiotensin III and angiotensin
IV induced greater contractions in the rabbit pulmonary artery than in the
pulmonary trunk with angiotensin II being the most potent and angiotensin IV the
least (Figure 2.1). 10-6 M losartan but not 10-7 M PD123319 inhibited the maximum
actions of the angiotensins in the arterial and trunk sections indicating that the
contractile actions of the three angiotensins were mediated by the angiotensin AT1
receptor.
51

9.3 9 8.3 8 7.3 7 9 8.3 8 7.3 7 6.3 6 6 5.3 5 9 8.3 8 7.3 7 8 7.3 7 6.3 6 5.3 5
Ang II Ang III Ang IV Ang II Ang III Ang IV
0
40
80
Pulmonary Artery Pulmonary Trunk
Concentration of Angiotensins (-log moles/L)
% K
Cl(
60m
M) c
ontr
actio
n
Figure 2.1 Direct contractile actions of angiotensin II (Ang II), angiotensin III (Ang III) and angiotensin IV (Ang IV) on the rabbit pulmonary artery and pulmonary trunk. Each histogram gives the mean ± SEM of 3 experiments.
52

2.3.2 Effects of angiotensin peptides on pre-contracted trunk and artery strips
Of the 6 angiotensin peptides tested, Ang(1-7), Ang(4-8) and Ang(3-7) were not
vasoactive in these experiments. In the pre-contracted pulmonary artery strips,
angiotensin II and angiotensin III further contracted the strips, while angiotensin IV
had no effect. In contrast, in the pre-contracted pulmonary trunk, angiotensin II
further contracted the strips while angiotensin III and angiotensin IV relaxed the
pre-contracted strips (Figure 2.2).
2.3.3 Effects of receptor antagonists and enzyme inhibitors
Losartan, but not PD123319, inhibited the relaxation and further contraction of the
pre-contracted strips to angiotensin II, angiotensin III and angiotensin IV, indicating
that their actions were mediated by the angiotensin AT1 receptor. Indomethacin
inhibited only the relaxation induced by angiotensin III and angiotensin IV,
suggesting that the relaxation by these peptides were mediated by a prostaglandin-
coupled angiotensin AT1 receptor subtype (Figure 2.3).
Initial experiments indicated that angiotensin II further contracted both pre-
contracted pulmonary trunk and artery, with the contraction seen in the artery of a
greater magnitude compared to that seen in the trunk. However, in further
experiments, it was observed that angiotensin II relaxed 6 out of 16 pre-contracted
pulmonary trunk strips (Figure 2.4). In these experiments, amastatin significantly
increased angiotensin III-induced further contraction of pre-contracted pulmonary
artery and reduced angiotensin III-induced relaxation of pre-contracted pulmonary
53

-80
-60
-40
-20
0
20
40
60
80
TrunkArtery
Angiotensin II Angiotensin III
Artery ArteryTrunk Trunk
Angiotensin IV
% c
ontr
ol c
ontr
acti
on
Figure 2.2 Effect of angiotensin II (100 nM), angiotensin III (50 nM) and angiotensin IV (5 µM) on the noradrenaline pre-contracted rabbit pulmonary artery and pulmonary trunk. Each histogram gives the means ± SEM of 3 experiments.
54

Angiotensin III Angiotensin IV
Artery Artery
Trunk Trunk*
** * *
-70
-50
-30
-10
10
30
50
70
Artery Trunk
**
Angiotensin II
Ang peptide
Ang peptide + Losartan
Ang peptide + Indomethacin
0
% c
ontro
l con
tract
ion
Figure 2.3 Influence of losartan (1 µM) and indomethacin (10 µM) on responses to angiotensin II, angiotensin III and angiotensin IV in the noradrenaline pre-contracted rabbit pulmonary artery and pulmonary trunk. Each histogram gives the mean ± SEM of 3 experiments. *significantly different from angiotensin-induced response.
55

trunk. In contrast, amastatin did not significantly affect the responses of pre-
contracted strips to angiotensin II and angiotensin IV (Figure 2.4). Divalinal-
angiotensin IV did not have any significant effect on angiotensin IV-induced
relaxation of pre-contracted pulmonary trunk, indicating AT4 receptors did not
mediate the relaxant response (Figure 2.5).
2.3.4 Structure-activity relationship of angiotensin IV
There were no agonist and antagonist properties observed with the 6 glycine-
substituted analogs of angiotensin IV when these analogs were added to pre-
contracted trunk and artery strips.
2.4 Discussion
The present data demonstrate the differential responses of the rabbit pulmonary
trunk and artery to angiotensin III and angiotensin IV, and lend support to an earlier
finding that the rabbit pulmonary trunk and artery contain two losartan-sensitive
angiotensin receptor subtypes (Sim and Lim, 1998). The AT1A-like subtype that
mediates contraction is found predominantly in the pulmonary artery while the
pulmonary trunk contains a mixture of AT1A-like and AT1B-like subtypes (Sim and
Lim, 1998); the latter subtype has been shown to mediate relaxation (Sim and Chai,
1996). This unusual distribution of functionally opposing receptor subtypes and the
different affinity of each receptor subtype for the four vasoactive angiotensins
(angiotensin II, angiotensin III, angiotensin IV and des-Asp-angiotensin I) probably
contributed to the differential responses seen in this study. The absence of response
56

Angiotensin II
-30
-20
-10
0
10
20
30
40
Ang
Ang ama
Angiotensin III Angiotensin IV%
con
trol
con
trac
tion
*
k k kArtery k Artery
Figure 2.4 Inangiotensin II, apre-contracted histogram givesdifferent from a
Trun
peptide
peptide +statin
fluencngiote
rabbit the mngiote
Trun
e of amastatin (nsin III and ang
pulmonary arteeans ± SEM of 3nsin-induced re
Trun
*Artery
30 µM) on the riotensin IV in try and pulmona experiments. *sponse.
Trun
esponses to he noradrenaline ry trunk. Each significantly
57

Angiotensin IV
-30
-20
-10
0
10
20
AngIVAngIV + DV-AngIV
% c
ontr
ol c
ontr
actio
n Trunk
Artery
Figure 2.5 Influence of divalinal-angiotensin IV (DV-AngIV) (1uM) on the responses to angiotensin IV in the noradrenaline pre-contracted rabbit pulmonary artery and trunk. Each histogram represents the means ±SEM of 3 experiments. Asterisk indicates response is significantly different from control.
58

to angiotensin-(1-7) would indicate that the heptapeptide does not act on the two
receptor subtypes. This is not unexpected as the known vascular actions of the
angiotensin-(1-7) are quite different from those of angiotensin II and angiotensin
III. Angiotensin-(1-7) has antihypertensive and vasodilatory actions and these
actions were attenuated following inhibition of nitric oxide synthetase (Osei et al.,
1995; Nakamoto et al., 1995). It has recently been shown to act on a new
angiotensin receptor (Santos et al., 1994). Angiotensin-(4-8) and angiotensin-(3-7)
are not known to be vasoactive and are shown to be the case in this study. Although
angiotensin IV has been known to act on the AT4 receptor (Krebs et al., 1996), it is
unlikely that the AT4 receptor mediates the actions of angiotensin IV seen in this
study. This is because its actions were blocked by losartan and not by divalinal-
angiotensin IV. The weak contractile action of angiotensin IV seen in the arterial
section could be due to its poor affinity for the AT1A receptor or its degradation by
tissue peptidases.
At the trunk section where both the AT1A-like and AT1B-like receptors have been
shown to be present in comparable density (Sim and Lim, 1998), the response seen
with each angiotensin would be a resultant action of the peptide on the composite
receptor subtypes. Angiotensin IV induced feeble direct contractile response in the
trunk section. The responses to angiotensin II and angiotensin III were about a
quarter and a sixth, respectively, of those seen in the arterial sections. The lower
number of AT1A-like subtypes present in the trunk section (Sim and Lim, 1998)
could have contributed to the lower responses. However, the AT1B-like receptors
59

could also have contributed to the diminution of the responses especially in the case
of angiotensin III and angiotensin IV where the response was a sixth and a tenth,
respectively, of those seen in the arterial sections. Both angiotensin III and
angiotensin IV attenuated the contraction induced by noradrenaline, whereas
angiotensin II increased the level of contraction albeit to a lesser extent than in the
arterial section. These different responses are probably caused by angiotensin II
having a higher affinity for the AT1A-like over the AT1B-like subtypes while the
reverse holds true for angiotensin III and angiotensin IV. Applied to other vascular
tissues where a mixture of AT1A and AT1B receptors is also likely to be present, it
would be expected that angiotensin III and angiotensin IV would always be weaker
pressors.
Amastatin, a selective aminopeptidase A and N inhibitor (Ahmad and Ward, 1990),
attenuated angiotensin III-induced relaxation of noradrenaline pre-contracted
pulmonary trunk and enhanced the angiotensin III-induced further contraction of the
pre-contracted pulmonary artery. This suggests that the angiotensin III-induced
further contraction and relaxation of pre-contracted pulmonary artery and trunk,
respectively, are mediated in part by a breakdown product of angiotensin III.
Angiotensin IV is a likely candidate for this breakdown product since angiotensin
III is broken down by APN to generate angiotensin IV (Kugler, 1982; Palmieri et
al., 1989). In addition, the metabolites of angiotensin IV are not known to be active
(Chansel et al., 1998).
60

The presence of two functionally opposing angiotensin receptor subtypes in the
short pulmonary trunk and artery may suggest that the vessel is not just a passive
conduit but may be an important regulator of blood flow from the heart to the lung.
Further increase in vascular tone by angiotensins at the arteries may slow entry of
blood into the lung and lower the blood pressure post arterially. Decrease of
vascular tone by angiotensins at the pulmonary trunk may dampen the pulse without
producing excessive back pressure on the heart. Understanding the physiological
protective mechanisms for the fine control of pulmonary blood flow can have
important therapeutic implications for the development of targeted therapies in
pulmonary hypertension.
61

CHAPTER 3
RECEPTOR BINDING STUDIES
3.1 Introduction
Functional studies (chapter 2) demonstrated differential responses of the rabbit
pulmonary trunk and artery to angiotensin III, des-Asp-angiotensin I (Sim and Soh,
1995; Sim and Chai, 1996), and angiotensin IV; the three angiotensin peptides
caused a vasodilator response in the noradrenaline-contracted pulmonary trunk
while they were either inactive (e.g. angiotensin IV) or caused a further
vasoconstrictor response in the noradrenaline-contracted pulmonary artery.
Losartan blocked both the vasoconstrictor and vasodilator response while
indomethacin blocked only the vasodilator response. In the present study, we
determined the binding characteristics of the angiotensin receptors in the trunk and
arterial sections of the rabbit pulmonary artery.
Two different sets of competition binding studies were performed, one using 125I-
Sar1-Ile8-angiotensin II and the other using 125I-angiotensin IV as the radioligand.
125I-Sar1-Ile8-angiotensin II was selected because it binds to both subtypes of
receptors in the rabbit pulmonary trunk and main arteries with high affinity; it
blocked both the vasoconstrictor and vasodilator response to active angiotensins at a
concentration of 1 nM, 125I-angiotensin IV was selected because organ bath
experiments indicate that angiotensin IV may have selectivity for the receptor
mediating vasodilation; it caused a vasodilator response in the noradrenaline-
62

contracted pulmonary trunk via an AT1 receptor but had negligible response in the
main arteries, albeit at a high concentration of 10 µM.
The purpose of the receptor binding studies was to characterize the receptor
subtypes that mediate the opposing vasodilator and vasoconstrictor response in the
pulmonary trunk and artery, respectively. We wanted to find out if different
subtypes of the AT1 receptor mediated the opposing responses. Our experiments
also addressed the possibility that within either the trunk or the artery, the response
seen is a composite result of more than one receptor subtype, hence providing a
possible explanation for the observed differential responses.
3.2 Materials and Methods
3.2.1 Membrane preparation
Male or female New Zealand White rabbits were supplied by the local University
Animal Centre. Six rabbits were killed by carbon dioxide poisoning. The rabbit
pulmonary trunk and artery were rapidly removed and placed in ice-cold Krebs
buffer saturated with carbogen (95% oxygen, 5% carbon dioxide). Adhering tissue
was removed and vessel was denuded of endothelium by gently rubbing a cotton
bud over its luminal surface.
The trunk and artery were weighed, minced and homogenized in 20 volumes of ice-
cold homogenization buffer (50 mM Tris, 0.25 M sucrose, 5 mM EDTA, 0.1 mM
PMSF, 0.1 mM 1,10-phenanthroline adjusted to pH 7.4 at 4oC) using a glass
63

homogeniser with a Teflon plunger (4000 rpm, 4 x 30 strokes). The homogenate
was centrifuged at 700 g for 15 minutes at 4oC, the supernatent obtained filtered
through two layers of fine cheesecloth and kept on ice, and the pellet resuspended in
20 volumes of homogenization buffer, rehomogenized (4000 rpm, 3 x 30 strokes)
and recentrifuged as before. The second filtered supernatent was combined with the
first and centrifuged at 55,000 g for 45 minutes at 4oC. The supernatent was
discarded and the pelleted membranes were then resuspended in storage buffer (50
mM Tris, 5 mM MgCl2.6H20, 5 mM EDTA, 0.1 mM PMSF, 0.1 mM
phenanthroline, 2 mg/ml BSA, 1 mg/ml bacitracin adjusted to pH 7.4 at either 15oC
for 125I- Sar1-Ile8-angiotensin II binding or 37oC for 125I-angiotensin IV binding) by
passing the membrane suspension through a 25-guage needle for 20 times, to a
concentration of 250 µg protein/ml.
The membranes were stored in liquid nitrogen until subsequent use. Protein
concentration was determined using the Bio-Rad assay (Bio-Rad Protein Assay,
Bio-Rad Laboratories, Richmond, CA, USA) using BSA as a standard. The average
protein yield was about 3.8 (trunk) and 2.8 (artery) mg protein per g of wet tissue.
3.2.2 125I- Sar1-Ile8-angiotensin II competition binding experiments
Trunk and artery membranes (10 µg protein) were incubated in duplicate with 0.02
nM 125I-Sar1-Ile8-angiotensin II and increasing concentrations of competing ligands
at 15oC in a total volume of 100 µl of assay buffer (50 mM Tris, 5 mM
MgCl2.6H2O, 5 mM EDTA, 0.1 mM 1,10-phenanthroline, 0.1 mM PMSF, 2 mg/ml
64

bovine serum albumin, 1 mg/ml bacitracin, 50 µM Plummer’s inhibitor, 20 µM
bestatin, 20 µM amastatin, pH 7.4 at 15oC, freshly prepared) for 60 minutes, in
accordance to previously published protocols (Sim et al., 1998) with slight
modifications. Non-specific binding was determined in the presence of 1 µM
unlabeled Sar1-Ile8-angiotensin II, and was approximately 10% of total binding. The
receptor binding reaction was terminated by centrifugation at 27,500 g for 30
minutes at 4oC followed by three rapid washes with 0.4 ml ice-cold 50 mM Tris
buffer, pH 7.4 at 4oC. Radioactivity trapped in the tissue pellet was determined
using a Packard Cobra II automated gamma counter with 72% efficiency.
Competing ligands used include angiotensin II, angiotensin III, angiotensin IV, des-
Asp-angiotensin I, Sar1-Ile8-angiotensin II, losartan, PD123319 and divalinal-
angiotensin IV.
3.2.3 125I-angiotensin IV association binding experiments
To determine how long it takes to reach equilibrium, association binding
experiments were performed in the presence of 1 nM 125I-angiotensin IV over a
time course of 300 minutes, with specific binding determined for triplicate samples
at various time intervals. 125I-angiotensin IV association binding curves reached a
plateau at approximately 120 minutes which was maintained for at least an
additional 180 minutes, suggesting that minimal receptor and/or 125I-angiotensin IV
degradation had occurred. This was confirmed by HPLC analysis of 125I-angiotensin
IV following 120 minute incubation at 37oC with membranes. The unbound 125I-
angiotensin IV in the supernatant was separated by HPLC and the radioactivity was
65

directly quantitated by a Beckman radioisotope detector (Model 710) as previously
described (Sim and Manjeet, 1990). Briefly, 10 µl of supernatent (after incubation
mixture was centrifuged) was resolved through a Merck 5 µm C18 column and the
125I-angiotensin IV eluted by gradient chromatography (from 0.1% trifluoroacetic
acid to 70% acetonitrile, 0.085% trifluoroacetic acid). Controls showed that under
the incubation conditions, more than 90% of the radioligand remained intact.
3.2.4 125I-angiotensin IV competition binding experiments
Trunk and artery membranes (10 µg protein) were incubated in duplicate with 1 nM
125I-angiotensin IV and increasing concentrations of competing ligands at 37oC in a
total volume of 100 µl of assay buffer (pH 7.4 at 37oC, freshly prepared) for 120
minutes. Non-specific binding was determined in the presence of 100 µM unlabeled
angiotensin IV and was approximately 40% of total binding. The binding reaction
was terminated and radioactivity counted as before.
3.2.5 Data analysis
Competition binding data were analyzed using GraphPad Prism. Unless otherwise
stated, each data point reflects the results from three experiments conducted in
duplicate. This number of experiments for each data point was limited because of
the low protein yield from pulmonary trunk and artery tissue, and the considerable
cost of 125I-angiotensin IV. For example, tissue from six rabbits yielded
approximately 800 µg protein, which generally was only sufficient for 4 complete
radioligand binding experiments.
66

The Kd of angiotensin IV for the receptor and the Bmax in the trunk and artery was
determined using results from the homologous competitive binding experiment, i.e.
using angiotensin IV as the radioligand and competing ligand; the low affinity of
angiotensin IV for the receptor rendered the cost of 125I-angiotensin IV prohibitive
for a saturation analysis. Similar Kd and Bmax values were determined for the 125I-
Sar1-Ile8-angiotensin II binding site and compared to those obtained previously
(Sim et al., 1998).
3.2.6 Statistical analysis
The statistical significance of differences between the Ki values of trunk and artery
membranes were analyzed using the independent t-test, with p values less than 0.05
considered significant. For example, the Ki value of 125I-Sar1-Ile8-angiotensin II
competition binding using AngII as the competing ligand in trunk membranes was
compared to the Ki value obtained in the artery membranes. Significant deviation of
Hill slopes from –1.0 was analyzed using the one-sample t-test, with p values less
than 0.05 considered significant.
3.2.7 Drugs and reagents
125I-angiotensin IV (2200 Ci/mmol) and 125I-Sar1-Ile8-angiotensin II (2200
Ci/mmol) were purchased from NEN Life Science Products, Boston, USA. All
reagents and other peptides were purchased from Sigma Chemical Co, St Louis,
67

USA with the exception of Plummer’s inhibitor (Calbiochem- Novabiochem
Corporation, California, USA).
3.3 Results
Competition binding experiments were performed to characterize the binding of
various angiotensin ligands to the receptors mediating opposing vasodilator and
vasoconstrictor response in the pulmonary trunk and artery respectively. 125I-Sar1-
Ile8-angiotensin II bound with similar high affinity to the trunk (Kd = 0.959 ± 0.609
nM, Bmax = 0.34 ± 0.20 pmol/mg protein) and artery binding sites (Kd = 1.041 ±
0.330 nM, Bmax = 0.71 ± 0.19 pmol/mg protein). There were no significant
difference between the Kd and Bmax values obtained from the trunk and artery and
they are consistent with those obtained in a previous ligand binding study in the
rabbit pulmonary artery (Sim et al., 1998).
Angiotensin peptides and antagonists displaced the binding of 125I-Sar1-Ile8-
angiotensin II to trunk and artery membranes of the rabbit pulmonary artery with
the following rank order affinity: Sar1-Ile8-angiotensin II > losartan > angiotensin
II > angiotensin III > des-Asp-angiotensin I > angiotensin IV (Figure 3.1). PD
123319 and divalinal-angiotensin IV were only able to show some displacement at
concentrations higher than 10-4 M, indicating that AT1 but not AT2 and AT4
receptors were probably present in the pulmonary trunk and artery. The Ki values of
the competing ligands in the trunk and artery membranes were not significantly
68

125I-Sar1-Ile8-AngII Competition BindingCurves - Trunk
-13 -11 -9 -7 -5 -3 -1
0
20
40
60
80
100
120
Sar1-Ile8-AngIILosartanAngII
AngIII
Ang(2-10)
AngIV
PD 123319Divalinal-AngIV
Concentration of Competing Ligand (logM)
% S
peci
fic B
indi
ng
125I-Sar1-Ile8-AngII Competition BindingCurves - Artery
-13 -11 -9 -7 -5 -3 -1
0
20
40
60
80
100
120
Sar1-Ile8-AngII
Losartan
AngII
AngIII
Ang(2-10)
AngIV
PD 123319Divalinal-AngIV
Concentration of Competing Ligand(log M)
% S
peci
fic B
indi
ng
Figure 3.1 125I-Sar1-Ile8-angiotensin II competition curves in the rabbit pulmonary trunk and artery. 10 µg of membrane protein was incubated with 0.02 nM radioligand at 15oC for 60 minutes. Each point represents the mean of 3 experiments performed in duplicate.
69

different, highlighting similar structural requirements of the 125I-Sar1-Ile8-
angiotensin II binding sites in the trunk and artery (Table 1).
To test the presence of more than one angiotensin receptor subtype within either the
trunk or the artery, a comparison of fit for a one- and two-site model was done
using the F-test. All competition curves fit the one-site model significantly better
than the two-site model (see r2 values in Table 1), suggesting that only one
angiotensin binding site is present in both the trunk and artery. The corresponding
Hill slopes were not significantly different from –1.0, except competition curves
using Sar1-Ile8-angiotensin II and losartan in the trunk, further indicating no
cooperativity and suggestive of a single class of binding site.
In contrast to 125I-Sar1-Ile8-angiotensin II binding, 125I-angiotensin IV bound with a
250-fold lower affinity to the 125I-angiotensin IV binding sites in the trunk (Kd =
251.97 ± 84.34 nM, Bmax = 14.25 ± 1.64 pmol/mg protein) and artery (Kd = 254.47
± 42.36 nM, Bmax = 15.37 ± 1.81 pmol/mg protein). There were no significant
difference between the Kd and Bmax values from the trunk and artery. However, the
receptor number for the 125I-angiotensin IV binding site was significantly higher
than for the 125I-Sar1-Ile8-angiotensin II binding site (Bmax ≈ 0.5 pmol/mg protein)
(p < 0.001) which suggested distinct binding sites.
70

125I-Sar1-Ile8-Angiotensin II Competition Binding Curves Radioligand - tissue Competing
Ligand Ki (M) r2 for single
site fit Hill slope
125I-Sar1-Ile8-AngII - trunk
Sar1-Ile8-AngII 9.47 x 10-10 ± 5.89 x 10-10 0.923 ± 0.029 -0.798 ± 0.021*
Losartan 4.52 x 10-10 ± 7.35 x 10-10 0.909 ± 0.046 -0.789 ± 0.022*
AngII 2.52 x 10-8 ± 1.60 x 10-9 0.957 ± 0.015 -1.049 ± 0.117 AngIII 1.45 x 10-7 ± 6.69 x 10-8 0.948 ± 0.027 -1.051 ± 0.116 AngI(2-10) 2.39 x 10-6 ± 3.88 x 10-7 0.974 ± 0.006 -0.906 ± 0.040 AngIV 7.94 x 10-5 ± 2.44 x 10-5 0.944 ± 0.011 -0.892 ± 0.044 PD 123319 > 10-4 - - Divalinal-AngIV > 10-4 - - 125I-Sar1-Ile8-AngII - artery
Sar1-Ile8-AngII 1.04 x 10-9 ± 3.23 x 10-10 0.960 ± 0.007 -1.141 ± 0.053
Losartan 3.11 x 10-8 ± 2.61 x 10-8 0.949 ± 0.006 -0.929 ± 0.154 AngII 3.36 x 10-8 ± 6.36 x 10-9 0.957 ± 0.020 -1.084 ± 0.115 AngIII 1.35 x 10-7 ± 4.54 x 10-8 0.940 ± 0.015 -1.020 ± 0.110 Des-Asp-AngI 2.02 x 10-6 ± 2.62 x 10-7 0.985 ± 0.004 -1.016 ± 0.094 AngIV 7.66 x 10-5 ± 1.93 x 10-5 0.967 ± 0.000 -0.883 ± 0.057 PD 123319 > 10-4 - - Divalinal-AngIV > 10-4 - - 125I-Angiotensin IV Competition Binding Curves Radioligand - tissue Competing Ligand Ki (M) r2 for single
site fit Hill slope
125I-AngIV - trunk AngIV 2.41 x 10-7 ± 7.36 x 10-8 0.972 ± 0.007 -1.037 ± 0.003 Divalinal-AngIV 1.37 x 10-6 ± 1.97 x 10-7 0.935 ± 0.031 -1.311 ± 0.221 Des-Asp-AngI 6.63 x 10-6 ± 2.03 x 10-6 0.954 ± 0.015 -1.056 ± 0.072 AngIII 4.03 x 10-6 ± 5.94 x 10-7 0.916 ± 0.047 -1.054 ± 0.122 AngII 1.44 x 10-4 ± 8.52 x 10-5 0.803 ± 0.129 -1.360 ± 0.334 Losartan > 10-4 - - PD123319 > 10-4 - - Sar1-Ile8-AngII > 10-4 - - 125I-AngIV - artery AngIV 2.51 x 10-7 ± 4.17 x 10-8 0.940 ± 0.026 -1.058 ± 0.024 Divalinal-AngIV 2.01 x 10-6 ± 5.04 x 10-7 0.952 ± 0.018 -1.011 ± 0.123 Des-Asp-AngI 7.39 x 10-6 ± 5.66 x 10-7 0.913 ± 0.032 -1.224 ± 0.141 AngIII 1.36 x 10-5 ± 5.72 x 10-6 0.906 ± 0.039 -1.026 ± 0.050 AngII 4.63 x 10-5 ± 7.93 x 10-6 0.850 ± 0.108 -1.056 ± 0.072 Losartan > 10-4 - - PD123319 > 10-4 - - Sar1-Ile8-AngII > 10-4 - -
Table 1 Competition binding constants for 125I-Sar1-Ile8-angiotensin II and 125I-angiotensin IV binding to rabbit pulmonary trunk and artery membranes. Results are expressed as mean ± SEM; n = 3. *significantly different from –1.0.
71

Angiotensin peptides displaced the binding of 125I-angiotensin IV to trunk and
artery membranes of the rabbit pulmonary artery with the following rank order
affinity: angiotensin IV > divalinal-angiotensin IV > angiotensin III ≈ des-Asp-
angiotensin I > angiotensin II (Figure 3.2). The Ki values for losartan, PD 123319
and Sar1- Ile8-angiotensin II were more than 10-4 M. The Ki values of the
competition curves in the trunk were not significantly different from the artery. All
competition curves fit the one-site model significantly better than the two-site
model and the corresponding Hill slopes were not significantly different from –1.0
(Table 1).
3.4 Discussion
The binding of 125I-Sar1-Ile8-angiotensin II to the trunk and artery membranes of the
rabbit pulmonary artery was displaced by Sar1-Ile8-angiotensin II, losartan,
angiotensin II, angiotensin III, des-Asp-angiotensin I and angiotensin IV. The Ki
values correlated well with concentrations effective in either eliciting the
vasodilator and vasoconstrictor response or the blocking of these responses (Sar1-
Ile8-angiotensin II, losartan) in organ bath experiments. This provides evidence that
the 125I-Sar1-Ile8-angiotensin II binding site corresponds to the angiotensin receptors
mediating the opposing vasodilator and vasoconstrictor response in the trunk and
artery respectively. The ability of losartan and the inability of PD 123319 and
divalinal-angiotensin IV to displace the radioligand, and the rank order affinity of
the receptors for the competing angiotensin peptides indicate that the receptors are
of the AT1 subtype (Touyz et al., 2000). Correspondingly, losartan but not PD
72

125I-AngIV Competition Binding Curves -Trunk
-9 -8 -7 -6 -5 -4 -3 -2
0
20
40
60
80
100
120
AngIVDivalinal-AngIV
AngIII
Ang(2-10)
AngIILosartan
PD 123319Sar1-Ile8-AngII
Concentration of Competing Ligand(log M)
% S
peci
fic B
indi
ng
125I-AngIV Competition Binding Curves -Artery
-9 -8 -7 -6 -5 -4 -3 -2
0
20
40
60
80
100
120
AngIV
Divalinal-AngIV
Ang(2-10)
AngIIIAngII
Losartan
PD 123319Sar1-Ile8-AngII
Concentration of Competing Ligand(log M)
% S
peci
fic B
indi
ng
Figure 3.2 125I-angiotensin IV competition curves in the rabbit pulmonary trunk and artery. 10 µg of membrane protein was incubated with 1 nM radioligand at 37oC for 120 minutes. Each point represents the mean of 3 experiments performed in duplicate.
73

123319 and divalinal-angiotensin IV blocked the vasoconstrictor and vasodilator
response in organ bath experiments.
The similar Ki values in the trunk and artery membranes suggest similar structural
requirements for the functionally different receptors, and provide evidence against
two receptor subtypes mediating the differential response. A significantly better fit
for a one-site model for all the competition curves also tends to eliminate the
possibility that within either the trunk or the artery, the response seen is a composite
result of more than one receptor subtype, which could have contributed to the
differential response observed.
Competition binding experiments were repeated using 125I-angiotensin IV because
functional studies (chapter 2) indicate that angiotensin IV may have selectivity for
the receptor mediating vasodilation in the pulmonary trunk. Equilibrium
dissociation constants from homologous competition binding demonstrated large
differences in Bmax for the 125I-Sar1-Ile8-angiotensin II (approximate range: 0.1 to
0.9 pmol/mg protein) and 125I-angiotensin IV binding site (approximate range: 12 to
17 pmol/mg protein), which suggested that the radioligands bound to distinct
binding sites. The site defined by 125I-angiotensin IV bound with the following rank
order affinity to angiotensin IV > divalinal-angiotensin IV > angiotensin III ≈ des-
Asp-angiotensin I > angiotensin II, but were unable to bind to losartan, PD 123319
or Sar1-Ile8-angiotensin II. This pattern of binding correlated poorly with functional
responses in organ bath experiments and seems consistent with an AT4 binding site
74

(Swanson et al., 1992). However, the Kd of angiotensin IV for the 125I-angiotensin
IV binding site (approximate range: 167.63 to 296.83 nM) is much higher than what
is generally reported for the AT4 receptor (Kd ≈ 1 nM) (Wright et al., 1995). Table 2
provides the binding constants for AT4 receptors located in several peripheral
tissues in various species (de Gasparo et al., 2000). The discrepancy in Bmax,
the poor correlation of the Ki values with potencies producing a functional response
and the inability of Sar1-Ile8-angiotensin II and losartan to displace 125I-angiotensin
IV binding suggest that 125I-angiotensin IV did not bind to the pharmacological site
of interest.
No explanation was forthcoming for the inability of 125I-angiotensin IV to bind to
the angiotensin receptor of interest since angiotensin IV at 10 µM was able to elicit
a vasodilator response in the trunk of the rabbit pulmonary artery. Perhaps the
inclusion of the 125I moiety caused significant changes in conformation of
angiotensin IV such that the peptide was unable to fit into the ligand binding site of
the receptor. However, we were unable to explore this possibility as alternative
forms of radiolabeling angiotensin IV e.g. using 3H or 14C, which does not require
the inclusion of a foreign molecule, were not commercially available.
Taken together, the present findings support the observations that the angiotensin
receptors mediating the differential vasoconstrictor and vasodilator responses in the
artery and trunk of the rabbit pulmonary artery respectively are of the AT1 subtypes.
75

α Mean ± S.D., n = 2-4. Study performed with 125I-angiotensin IV.
Species Tissue Kd (nM) Bmax (pmol/mg protein)
Rabbit Heart 1.75 ± a5α 0.731 ± 0.163 Rat Heart 3.3 ± 1.1 0.320 ± 0.066 Bovine Adrenals 0.74 ± 0.14 3.82 ± 1.12 Guinea Pig Heart 1.33 ± 0.02 0.144 ± 0.019 Guinea Pig Hippocampus 1.29 ± 0.18 0.499 ± 0.062 Bovine Vascular smooth
muscle 1.85 ± 0.45 0.960 ± 0.100
Bovine Vascular smooth muscle
0.70 ± 1.0 0.476 ± 0.057
Guinea Pig Vascular smooth muscle
0.40 ± 0.09 1.040 ± 0.239
Monkey Kidney 1.5 ± 0.31 1.000 ± 0.212 Guinea Pig Colon 0.84 ± 0.08 0.659 ± 0.075 Human Prostate 0.60 ± 0.15 1.399 ± 0.152
Table 2 Binding constants for AT4 receptors in various species and tissues (adapted from Gasparo et al, 2000)
76

It further demonstrated that the angiotensin receptors in the trunk and artery shared
similar structural requirements for its ligands, suggesting that it is unlikely that
different angiotensin receptor subtypes mediated the opposing responses. Neither
were different composites of receptor types likely to be responsible for the
differential responses since the findings determined a single binding site for both
the trunk and artery of the rabbit pulmonary artery.
From the present results, it is difficult to define the mechanism of the opposing
vasoconstrictor and vasodilator response reported in the previous chapter. We
discounted vasodilator response mediated by the AT4 receptor since the binding
profile of 125I-angiotensin IV corresponded poorly with functional responses.
Furthermore, divalinal-angiotensin IV did not block the vasodilator response.
However, we cannot exclude the possibility of further angiotensin receptors that
are, as yet, uncharacterized and undistinguishable by Sar1-Ile8-angiotensin II and
losartan, including the existence of mRNA splice variants of the AT1 receptor that
could have contributed to the differential responses. Therefore, we next proceeded
to further characterize the angiotensin receptors in the pulmonary trunk and artery
by RNA analysis.
77

CHAPTER 4
RNA STUDIES
4.1 Introduction
The actions of angiotensin II are mediated by two pharmacologically characterized
classes of angiotensin receptors, AT1 and AT2 (de Gasparo et al., 2000). While the
physiological role and the intracellular signaling pathways of the AT2 receptor are
not clearly defined, the angiotensin AT1 receptors have been extensively studied
and shown to mediate virtually all of the known physiological actions of
angiotensin II in cardiovascular, renal, neuronal, endocrine, hepatic and other target
cells (de Gasparo et al., 2000). Genome analysis and homology cloning
demonstrated that the rat and mouse AT1 receptors exist as two distinct subtypes,
termed AT1A and AT1B, which are encoded by two different genes (Iwai and
Inagami, 1992) They have approximately 95% identity in their amino acid
sequences and are also similar in terms of their ligand binding and activation
properties but differ in their tissue distribution, chromosomal localization, genomic
structure, and transcriptional regulation (Iwai and Inagami, 1992). This suggests
that they could mediate different physiological function. None of the other cloned
mammalian AT1 receptors, including those from the cow (Sasaki et al., 1991),
human (Bergsma et al., 1992; Curnow et al., 1992), pig (Itazaki et al., 1993), rabbit
(Burns et al., 1993), and dog (Burns et al., 1994) appear to have subtypes. Southern
hybridization analysis of at least eight different restriction enzyme fragments of the
78

rabbit genomic DNA using rabbit AT1 cDNA as a probe did not produce evidence
for a subtype of the AT1 receptor (Burns et al., 1993).
The existence of two distinct angiotensin AT1 receptor subtypes differentially
distributed in the rabbit pulmonary trunk and artery is suggested by differential
response between the pulmonary trunk and artery to angiotensin peptides. Although
Southern analysis indicates that a single gene encodes one AT1 receptor in the
rabbit (Burns et al., 1993), the possibility that AT1 receptor splice variants in the
rabbit could account for the differences in response cannot be ruled out. The
purpose of the present study was therefore to further characterize the angiotensin
receptors in the rabbit pulmonary trunk and artery and to determine if different
subtypes of the AT1 receptor, including splice variants, exist in the rabbit using
Northern blot analysis.
4.2 Rationale for Experimental Design
In contrast to reports of two angiotensin AT1 receptor subtypes being identified in
rodents (AT1A and AT1B), only a single AT1 receptor subtype has been reported in
the rabbit. In our experimental strategy to determine if more than one AT1 receptor
subtype exists in the rabbit, we generated two probes from published rabbit cDNA
sequence (Burns et al., 1993) (see Figure 4.1), one from the coding region (hereafter
known as the coding probe) and the other from the non-coding region (hereafter
known as the non-coding probe), for hybridization in subsequent Northern blots.
The basis for this strategy was the observed high sequence homology (~96%)
79

1 gatttgaaat atctagatta ttctaaaatg gctgggtttt tatctgaata agtcaaagaa 61 gccatccagg aagtcaacat cagctgcgtt tgatgagaca aattcaaccc aggccatcaa 121 aatgatgctc aactcttcta ccgaagatgg tatcaaaaga atccaggatg actgtcccaa 181 agctggaagg cacaattaca tatttgtcat gattcctact ctgtatagca tcatctttgt 241 ggtgggaata tttgggaaca gcttggcggt gattgtcatt tacttttaca tgaaactcaa 301 gactgtggcc agtgtttttc ttttgaattt agcattggct gacttatgct ttttactgac 361 tttgccactc tgggctgtct acactgctat ggaataccgc tggccctttg gcaattacct 421 gtgtaagatt gcttcggcca gtgtcagttt caacctctat gccagtgtat ttctactcac 481 gtgtctcagc attgaccgct acctggctat tgtccacccg atgaagtctc gccttcgacg 541 cacaatgctt gtagccaaag tcacctgcat cattatttgg ctgctggctg gcttggccag 601 tttaccagct atcatccacc gaaacgtatt tttcatcgag aacaccaaca tcacggtttg 661 tgctttccat tacgagtccc aaaactcaac cctccccata gggctaggcc tgaccaaaaa 721 tatactgggc ttcctatttc cctttctgat cattcttaca agctacactc ttatttggaa 781 ggccctcaag aaggcttacg agattcagaa gaacaagcca agaaatgatg atatttttaa 841 gatcattatg gcaattgtgc ttttcttttt cttctcctgg gttccccacc aaatattcac 901 tttcctggat gtgttgattc agctgggggt cattcacgac tgcagaatcg cagatatcgt 961 ggacactgcc atgcccatca ccatctgcat agcttatttt aacaactgcc tgaatcccct1021 tttttatggc tttctgggga aaaaatttaa gaaatatttt ctccagcttc ttaaatatat 1081 tcccccgaaa gccaaatccc attcaaatct atcaacaaag atgagcacgc tctcctaccg 1141 cccctcagat aacgtgagct catcctccaa gaagcccgtg ccctgctttg aggttgagtg 1201 acatgttcaa aacctgttgg tgaagcaact ttgtcaaaga aggagccaaa gaaacattcc 1261 tgcacagcac tgcgctacca aatgagcatt agctactttt caggatgtaa ggagaagttg 1321 gatcaattgg actgaaccgc cggcttgtct acagctcgaa caaaagcttt ccttttcttt 1381 agcaacaaaa caaagcagag ccacattttg cattaaatac aagatggctg ctcaaagaat 1441 gatgacagaa actggacaaa tgtgttgatt tcagaaattt tgctggcgga aatgcagtct 1501 cgccagtctt ctcttgttct attatttttg atttctatat aaaggtattt agaggaagtg 1561 aaatctacag agcagcaaca ggagatcaca gttcaggatt gttctttctg cccaatttcc 1621 aaggggcgat gaagctttta tgcctgttta gccattagca gctgtgacca cttgtacctg 1681 ctccaatgca tttcgtgcaa aaatgtgcta agcagtagtt gtcaagtttc agaacctttt 1741 atgaaattca accagagtca taaagattca cactgccaaa ataatggtgg cagaatggct 1801 tcttgcaaaa tggtgttact aaagttacgt gtaagagtta aatactagca aaggtgtcac 1861 tctagtccca gggagttgtg ttctcctggt catattagtc ttatttcata tctgataact 1921 gtatatagtt tatagtaaaa agattatata tcgtaaagta tgccaagctg tttcaacaaa 1981 gtatatattt tacatacaca tctacatgta tcaatgtcgt taaactgttg ttacttgatt2041 caaatctagc aaagctctat ttaccttaaa taaaataatt gtaggaatt Figure 4.1 Nucleotide sequence of cDNA encoding a rabbit kidney cortex angiotensin II receptor. The open reading frame is the nucleotide sequence in bold and consists of nucleotides encoding 359 amino acids. The underlined sequence represents the upstream and downstream reverse primers used to generate the coding and non-coding probes, respectively, for Northern blot analysis of total RNA isolated from the rabbit pulmonary trunk and artery.
80

within the coding regions of the rat AT1A and AT1B cDNAs, but marked differences
in the non-coding regions. We made the assumption that if AT1 receptor subtypes
exist in the rabbit, they would similarly share a high sequence homology in the
coding region and a low sequence homology in the non-coding region of the rabbit
AT1 receptor sequence. The coding probe would thus hybridise to the coding
regions of all putative rabbit AT1 subtype mRNAs in a Northern blot while the non-
coding probe would only be able to selectively bind to the non-coding region of the
published AT1 subtype mRNA but not other putative AT1 subtypes. The presence of
additional bands in a Northern blot of total RNA isolated from rabbit pulmonary
vasculature using the coding probe, that are not observed in a similar Northern blot
using the non-coding probe, would indicate the presence of more than one rabbit
AT1 receptor subtypes.
4.3 Materials and Methods
4.3.1 Isolation of primary vascular smooth muscle cells (VSMCs) – primary
explant technique
A male albino rabbit weighing 1.5 - 2.5 kg was killed by cervical dislocation or
carbon dioxide poisoning. The thorax area was disinfected with 70% ethanol and
the thorax opened by cutting longitudinally along the median line with sterile
scissors and forceps, ensuring sterility throughout the procedure. The heart was
removed and transferred to a petri dish containing cold phosphate-buffered saline
(PBS). The pulmonary trunk and artery were located with the aid of a sterile 1 ml
pipette and connective and fatty tissue was removed.
81

The isolated pulmonary trunk and artery was transferred to fresh PBS and cut into
two pieces: the trunk and artery. Each vessel was then cut open. With the
endothelium side face up, endothelial cells were gently removed by scrapping the
luminal surface with the blunt end of a surgical blade. The luminal surface was
intensely rinsed with PBS.
Using two fine forceps, one having a curved tip, the medial layer was stripped off
from the adventitia. The adventitia was grasped at the lateral margin with a straight
forceps and the medial layer was carefully detached from the adventitia with the
curved forceps. The medial layer obtained was then transferred to culture medium
(DMEM/F12 1:1, pH 7.4) and cut into approximately 0.1 cm2 media explants with
surgical blades. The media explants were transferred to 6-well plates containing
small volumes of medium just covering the explants. The explants were incubated
in a 37oC humidified incubator with an atmosphere of 95% air and 5% CO2. The
medium was changed every 48 hours.
4.3.2 Cell culture
Between day 3 and day 5 after the isolation of media explants, smooth muscle cells
(SMCs) started to migrate out from the explants. After 14-21 days the plastic
bottom was covered with SMCs. To passage the cells, the media explants were
removed using fine forceps. The primary SMCs were trypsinized using
82

trypsin/EDTA and counted using the coulter counter. The SMCs were routinely
seeded at a density of 10,000 cells/cm2 and cultured in 75 cm2 flasks.
To determine that no other cell type (fibroblasts or endothelial cells) had
contaminated the SMC cultures, the SMCs were identified morphologically
(spindle-shaped apperance) and by their growth pattern (characteristic “hill and
valley” growth pattern) with a light microscope as well as characterized by
immunological staining of the cytoskeleton protein, alpha-smooth muscle actin,
using flow cytometry.
4.3.3 Isolation and purification of RNA
Total RNA was isolated from rabbit pulmonary trunk and artery VSMCs using a
total RNA isolation system (Promega RNAgents® Total RNA Isolation System).
Approximately two 75 cm2 culture flasks per cell type (trunk or artery) of confluent
cells containing a total of about 5 x 106 cells were used for each RNA isolation. The
isolation of RNA was carried out in a designated ribonuclease-free environment
using sterile disposables, ribonuclease (RNase)-free glassware and sterile
techniques.
Confluent cells were washed with phosphate-buffered saline (PBS), trypsinized and
pelleted at 4oC. The pelleted cells were washed with culture medium containing
serum, pelleted and cell membranes disrupted by mixing thoroughly with pre-
chilled denaturing solution (55% guanidine thiocyanate, 45% citrate/sarcosine/β-
83

mercaptoethanol (CBS) buffer) to denature nucleoprotein complexes, release RNA
and inactivate intracellular ribonuclease (RNase). Contaminating DNA and proteins
were removed by adding sodium acetate followed by phenol:chloroform:isoamyl
alcohol (125:24:1) (acid extraction) and mixed by inversion; DNA and proteins
partitioned into the organic phase while the RNA partitioned selectively into the
aqueous phase. After the phases were separated by centrifugation, the top aqueous
phase was removed and RNA precipitated by adding isopropanol. The RNA was
pelleted by centrifugation, washed with 70% ethanol to remove salt, air dried and
dissolved in nuclease-free water.
The yield (µg/µl) and purity of RNA were determined spectrophotometrically at
260 and 280 nm, where 1 absorbance unit (A260) ~ 40 µg of single-stranded
RNA/ml (precise = 44.19 µg RNA/ml) and pure RNA has a A260/A280 ratio of 2.0 ±
0.05 (acceptable range: 1.7 – 2.0). The integrity of isolated RNA was determined by
denaturing agarose gel electrophoresis using formaldehyde as the denaturing agent.
Only samples which show a 2:1 ratio of 28S to 18S eukaryotic ribosomal RNA by
ethidium bromide staining were used in subsequent experiments.
For RNA preparations used for the generation of probes, the total RNA samples
were treated with DNA polymerase (DNase) to remove trace amounts of
contaminating genomic DNA. Removal of DNA is important because amplification
products will be generated from subsequent reverse transcriptase-polymerase chain
reaction (RT-PCR) if any trace DNA is present.
84

4.3.4 Generation of probes for Northern blot
4.3.4.1 Primers
The primers derived from the coding region of the published rabbit cDNA sequence
(Figure 4.1) for synthesizing the coding probe were 1) upstream primer, 5’
ATCAAAAGAATCCAGGATGAC 3’ and 2) downstream reverse primer, 5’
AAAAAAGGGGATTCAGGCAGTT 3’. The primers derived from the non-coding
region for synthesizing the non-coding probe were 1) upstream primer, 5’
AAAGAAGGATCCAAAGAAACA 3’ and 2) downstream reverse primer, 5’
AGAGCTTTTCTAGATTTGAAT 3’.
All primers were synthesized by the National University Medical Institutes,
Singapore.
4.3.4.2 RT-PCR and DNA cloning
Reverse transcription and amplification of the coding and non-coding probes were
carried out using the Access RT-PCR System (Promega). The reaction mix was
prepared by combining specified volumes of the previously isolated total RNA,
upstream and downstream primers, dNTP mix, magnesium sulphate, reverse
transcriptase, DNA polymerase in reaction buffer on ice, using nuclease-free water
to make up to a total volume of 50 µl. The reaction was initiated by adding the
RNA template (total RNA). The reaction was overlayed with 2 drops of mineral oil
to prevent condensation and evaporation. The reaction tubes were incubated at 48oC
85

for 45 minutes to allow synthesis of first-strand cDNA by reverse transcriptase
reaction, followed by incubation at 94oC for 2 minutes to denature the RNA/cDNA
hybrid. Denaturing, annealing of upstream and downstream primers, and extension
were then carried out for 40 cycles of 94oC for 30 s, 60oC for 1 minute and 68oC for
2 minutes, respectively. A final 7 minute extension at 68oC was allowed after the
final cycle.
The PCR products obtained were separated by agarose gel electrophoresis and
identified by UV transillumination of an ethidium-stained gel. The following PCR
products were obtained: 1) coding probe – 0.8 kb fragment; 2) non-coding probe –
0.8 kb fragment. Following isolation of the coding and non-coding probes using
low melting point agarose gels, the gel slices containing the two DNA probes were
removed from the gel, melted at 70oC for 30 minutes and subjected to phenol
extraction and ethanol precipitation. The coding and non-coding DNA probes
obtained were washed with ethanol and reconstituted in water.
The coding and non-coding DNA probes were inserted into the pBluescript SK (+)
(pKS) plasmid by restriction digestion (coding: BamHI, EcoRI; non-coding:
BamHI, XBaI) and ligation. E. Coli cells were grown to an OD590 of 0.4,
concentrated by centrifugation and resuspended in ice-cold calcium chloride to
make the cells competent. Ligation products were added to competent E. Coli cells,
heat-shocked at 45oC for 1.5 minutes and cultured at 37oC in a shaking water bath
for 45 minutes. Single inoculums of cells were then streaked across agar plates to
86

isolate single colonies of transformed cells and incubated at 37oC until colonies
became visible.
Single colonies of E. Coli cells were cultured overnight in LB medium containing
ampicillin in a 37oC shaking water bath and cells concentrated by centrifugation.
The cells were lysed by resuspension in STET solution (8% sucrose, 5% Triton X-
100, 50 mM EDTA and 50 mM Tris.Cl, pH 8.0) followed by immersion in a 100oC
water bath for 1 to 2 minutes and centrifugation. Plasmid DNA in the supernatant
was precipitated with isopropanol, centrifuged and the plasmid DNA pellet washed
with ethanol and resuspended in water. The plasmid DNA was identified by
selective restriction digestion and subsequent agarose gel electrophoresis, as well as
base sequencing to ensure that the correct coding and non-coding probes were
obtained. The plasmid DNA was restriction digested, the coding and non-coding
probes isolated by low melting point agarose gel electrophoresis and subjected to
phenol extraction and ethanol precipitation as described previously. The sizes of
both coding and non-coding probes were 0.8 kb.
4.3.5 Northern Blot
For Northern blot analysis, 20 µg of total RNA, isolated as previously described in
Section 2.4.3, was separated by 1.0 % agarose-formaldehyde gel electrophoresis
and transferred onto nylon membranes overnight. The coding and non-coding
probes were labeled with [32P]-dCTP using the Klenow fragment of DNA
polymerase I by the random primer method (Prime-a-Gene Labeling System,
87

Promega). Pre-hybridisation was performed at 68oC for 2 hours in a solution of 6X
SSC (1X SSC = 0.2 M NaCl and 0.3 M sodium citrate, pH 7.0), 5X Denhardt’s,
0.5% sodium dodecyl sulfate (SDS) and 100 µg/ml of salmon sperm DNA.
Hybridisation was performed overnight at 68oC in a solution of 6X SSC, 0.5% SDS
and [32P]-dCTP-labeled probe. The membranes were washed 4 times in 1X SSC and
0.1% SDS at 38oC for 10 minutes each, then 2 times in 0.2X SSC and 0.1% SDS at
38oC for 20 minutes each, and then exposed to radiographic film at -70oC for 7-10
days.
4.4 Results
Total RNA was extracted from rabbit pulmonary trunk and artery. Representative
autoradiograms derived from a Northern blot analysis are shown (Figure 4.2). Both
the coding and non-coding probe hybridized to a single band in a Northern blot of
total RNA from the rabbit pulmonary trunk and artery, suggesting that with
reasonable probability the rabbit pulmonary trunk and artery express a single AT1
receptor subtype.
4.5 Discussion
Differential vasoconstrictor and vasodilator response to angiotensin II, angiotensin
III and angiotensin IV suggest two distinct angiotensin AT1 receptor subtypes exist
differentially distributed in the rabbit pulmonary trunk and artery. To determine if
more than one AT1 receptor subtype exists in the pulmonary vasculature, Northern
88

Artery Trunk (pulmonary end)
Trunk (cardiac end)
well
AT1 coding probe
well
AT1 non-
coding probe
Figure 4.2 AT1 receptor mvascular smooth muscle cells (trunk and artery VSMCs. (Arabbit AT1 coding probe. Simiand trunk (both pulmonary ahybridization to a rabbit AT1in the pulmonary artery and tr
B
A
RNA in rabbit pulmonary trunk and artery VSMC). Total RNA was extracted from cultured ) Northern blot analysis by hybridization to a lar mRNA was detected in the pulmonary artery nd cardiac end). (B) Northern blot analysis by
non-coding probe. Similar mRNA was detected unk (both pulmonary and cardiac end).
89

blot analysis of total RNA isolated from the rabbit pulmonary trunk and artery was
carried out using two probes generated from the coding and non-coding regions of
published rabbit AT1 cDNA sequence (Burns et al., 1993). Based on what was
similarly observed for AT1A and AT1B receptor subtypes in the rat, the coding
regions of possible rabbit AT1 receptor subtypes were assumed to share a high
sequence homology while the non-coding regions share a low sequence homology.
The presence of additional bands in a Northern blot using the coding probe
(generated from the coding region of the rabbit AT1 published cDNA sequence)
when compared to a similar Northern blot using the non-coding probe (generated
from the non-coding region) would indicate the presence of more than one AT1
receptor subtype in the rabbit. In our present findings, both the coding and non-
coding probe hybridized to a single band in a Northern blot of total RNA isolated
from rabbit pulmonary trunk and artery, suggesting with reasonable probability the
presence of a single AT1 receptor subtype in the pulmonary vasculature. This
finding confirms our previous findings from receptor binding studies which also
indicate a single class of AT1 receptors in the pulmonary vasculature. It is also
consistent with similar previous reports that the rabbit contains only a single AT1
receptor subtype, in contrast to rodents (Burns et al., 1993).
Although both Southern blot analysis carried out by Burns and colleagues (1993)
and Northern blot analysis in our laboratory have suggested the presence of a single
AT1 receptor in the rabbit pulmonary trunk and artery, the possibility that other AT1
receptor subtypes exist cannot be ruled out for several reasons. Firstly, the
90

experimental strategies for both Southern and Northern blot analysis require that the
AT1 receptor subtypes share significant homology with the AT1 receptor sequence
used to generate the probe to allow detection. In addition, the lengths of mRNAs of
AT1 receptor subtypes must differ such that they can be visualized as distinct bands
on a Northern blot when hybridized with a complementary radioactive probe.
Hence, AT1 receptor subtypes with significant differences in sequence with the
published AT1 receptor sequence or those with similar mRNA lengths would not be
detected by these experimental strategies.
The present findings suggest that the rabbit pulmonary trunk and artery contain a
single AT1 receptor subtype and that this receptor is responsible for the differential
responses observed in the rabbit pulmonary trunk and artery. These findings raise
the question of how a single AT1 receptor subtype is regulated to mediate opposing
vasoconstrictor and vasodilator responses in different segments of the short rabbit
pulmonary artery. Rowe and Dixon (2000) recently reported that intravenous bolus
administration of angiotensin II, angiotensin III and angiotensin IV produced a
pressor peak followed by a depressor phase in the arterial blood pressure in the
rabbit, with angiotensin III being a more potent depressor than angiotensin II and
angiotensin IV being 100-fold less potent than angiotensin III. Both angiotensin III-
induced pressor and depressor components were blocked by losartan but not by
PD123319, suggesting that both pressor and depressor actions were AT1-mediated
effects. Unlike other members of the G-protein coupled receptor superfamily in
which a specific receptor subtype is usually coupled to a specific effector, AT1
91

receptors are coupled to multiple, distinct signal transduction processes, leading to
diverse biological actions even within a single cell type i.e. the vascular smooth
muscle cell (Touyz et al., 2000). The signaling processes are highly complex and
multiphasic with distinct temporal characteristics. Angiotensin II is known to
induce phospholipase C (PLC) phosphorylation (leading to formation of IP3 and
DAG) and Src activation within seconds, phospholipase A2 (PLA2), phospholipase
D (PLD), tyrosine kinase and mitogen-activated protein kinase (MAPK) activation
within minutes, and proto-oncogene expression and protein synthesis within hours.
Our present data suggests that the AT1 receptor present in the pulmonary trunk and
artery may be identical yet mediate a distinct and opposite biological response. The
subsequent receptor-coupled signal transduction cascade may confirm such
differences in the receptor role. As the vasodilator response of the rabbit pulmonary
trunk to angiotensin III, angiotensin IV and des-Asp-angiotensin I is blocked by
indomethacin, angiotensin-induced production of vasodilator prostaglandins (PGE2
and/or PGI2) is implicated in its signal transduction pathway. In our next study, we
investigated the angiotensin-induced prostaglandin release as well as the inositol
triphosphate signaling pathways in cultured VSMCs from the trunk and artery of
the rabbit pulmonary artery.
92

CHAPTER 5
SIGNAL TRANSDUCTION STUDIES
5.1 Introduction
We reported earlier the differential responses of the rabbit pulmonary trunk and
artery to angiotensin II, angiotensin III and angiotensin IV, with both contractile
and relaxant responses mediated by a single AT1 receptor. The next logical question
to ask was, “What intracellular processes mediate these contradictory responses.”
Hence, an attempt was made to elucidate the signal transduction mechanisms that
may mediate these opposing responses.
One of the earliest events in VSMCs following angiotensin II stimulation is the
activation of phospholipase C (PLC) through the heterotrimeric Gq protein, which
results in the rapid hydrolysis of phosphatidylinositol 4,5-bisphosphate to inositol
1,4,5-triphosphate (IP3) and diacylglycerol (DAG) (Griendling et al., 1989). As a
result, IP3 levels increase albeit transiently due to its rapid metabolism, often
returning towards basal levels within 15 – 30 seconds (Minami et al., 1991;
Wojcikiewicz et al., 1993). IP3 interacts with IP3 receptors to release calcium from
intracellular stores. Consequently, the transient increase in IP3 is correlated with an
initial increase in cytosolic Ca2+ and the phasic component of vascular smooth
muscle contraction.
93

In addition to the activation of PLC, angiotensin II has been shown to
simultaneously activate phospholipase A2 in vascular smooth muscle (Kubalak et
al., 1993). PLA2 activation leads to the release of arachidonic acid, which is
thereafter metabolized into prostaglandins. An increase in prostaglandin release,
mainly PGI2 and PGE2, in response to angiotensin II has been described in VSMCs
(McGiff, 1981; Nasjletti et al., 1982; Lang and Vallotton, 1989; Jaiswal et al.,
1993). PGI2 activates adenylyl cyclase and increase adenosine 3’,5’-cyclic
monophosphate (cAMP) to relax vascular smooth muscle (Bolton, 1979). This
vasorelaxation may modulate angiotensin II-induced contraction, thus buffering the
effect of vasoconstriction (Jackson and Herzer, 1993). Consequently, the vascular
smooth muscle tone is controlled by a balance between the cellular signaling
pathways that mediate the generation of force (contraction) and the release of force
(relaxation).
In endothelium denuded noradrenaline pre-contracted rabbit pulmonary vessels,
angiotensin II elicited a further contractile response in both the trunk and the artery.
Angiotensin III similarly elicited a further contractile response in the artery but
relaxed the pre-contracted trunk. Angiotensin IV caused no changes in the vascular
tone in the artery and relaxed the pre-contracted trunk. These angiotensin responses
were all found to be blocked by losartan (selective AT1 receptor antagonist), but not
PD123319 (selective AT2 receptor antagonist). In addition, indomethacin blocked
the angiotensin III- and angiotensin IV-mediated relaxant response in the trunk,
94

suggesting that the vasorelaxation was probably mediated by the release of
prostaglandins like PGE2 and PGI2.
To elucidate the signaling mechanisms involved in these differential responses, we
first compared the release of PGE2 and PGI2 from both rabbit pulmonary trunk and
artery VSMCs when stimulated with angiotensin II, angiotensin III and angiotensin
IV. Next, we measured the inositol (1,4,5)-triphosphate (IP3) mass content in
angiotensin II- and angiotensin IV-stimulated rabbit pulmonary trunk tissue slices.
5.2 Rationale for experimental design
5.2.1 Prostaglandin studies
Primary cultures of rabbit pulmonary trunk (PTSMCs) and artery smooth muscle
cells (PASMCs) were used for measuring prostaglandin release because the use of
SMC culture is well established and convenient for measurement of signal
transduction modalities. Culture systems have several advantages, including
obtaining a pure smooth muscle population devoid of endothelial, adventitial and
other cell contamination, enabling signal transduction investigations to be solely
attributed to smooth muscle cells.
PGE2 and PGI2 are the major vasodilator prostaglandins produced in the vasculature
(Hassid and Williams, 1983; Schror, 1993). This governed our choice of
prostaglandins to measure from the rabbit pulmonary trunk and artery.
95

5.2.2 Inositol triphosphate studies
Determinations of IP3 have been mainly indirect, relying on the loading of tissue or
cells with myo-2-[3H]inositol ([3H]inositol), which incorporates to
phosphotidylinositol 4,5-biphosphate (PIP2). PIP2 is broken down to IP3 on receptor
stimulation. The IP3 isomers thus obtained are subsequently separated and
quantitated by HPLC. The disadvantages of such procedures are: (1) the assumption
that all pools of inositol phosphates have been labeled to equilibrium is rarely
established, and (2) agonist-induced changes in the specific radioactivity of inositol
triphophates are sometimes inevitable. In addition, such techniques are laborious
and time-consuming. Hence, although the method is not as widely adopted, we
chose a mass measurement method using a radioreceptor assay (Challiss et al.,
1988), which allows the estimation of the ‘active’ calcium-mobilizing isomer (IP3)
of the inositol phosphates. This method takes advantage of the presence of
saturable, high-affinity binding sites for IP3 in microsomal fractions of bovine
adrenal cortex or rat cerebellum (Challiss et al., 1988; Bredt et al., 1989; Palmer et
al., 1989; Nibbering et al., 1990).
In this study, only IP3 production stimulated by angiotensin II and angiotensin IV in
the pulmonary trunk was measured. The angiotensin III-mediated stimulation of IP3
production was not measured since isolated tissue experiments suggest that its
actions are mediated by a break down product, likely angiotensin IV. Because the
differential vasoconstrictor and vasodilator response was observed in the trunk but
not in the artery, only trunk tissue slices were used.
96

Endothelium-denuded rabbit pulmonary trunk tissue slices were used instead of
cultured VSMCs (VSMCs) for measurement of IP3 release for several reasons. We
encountered several technical difficulties in the use of pulmonary trunk and artery
VSMCs for the PG assays. Firstly, approximately 5 passages of the primary VSMC
culture were required to obtain sufficient number of cells to be assayed because of
the low proliferative capability of the primary VSMC culture. Hence, VSMCs from
passage 5 to 12 were used in the PG assays. High variability in the PG assay results
was also observed which may be related to the phenotypic modulation of VSMCs in
culture for many passages (Chamley-Campbell et al., 1979; McMurray et al., 1991;
Birukov et al., 1993). In an attempt to address these difficulties, we used pulmonary
trunk and artery tissue slices instead of VSMCs in our IP3 assay. In addition to
avoiding phenotypic modulation of VSMCs in the intact tissue, tissue slices allow
ready tissue handling and retain some degree of structural integrity. VSMCs also
remain in close proximity with the extracellular matrix and other tissue, thus
contributing to the maintenance of a high degree of functional integrity relative to
the in vivo situation.
5.3 Materials and Methods
5.3.1 Prostaglandin studies
5.3.1.1 Cell culture
Primary cultures of rabbit pulmonary trunk and artery SMCs were prepared as
described previously in Section 4.3.1 and 4.3.2.
97

5.3.1.2 Measurement of PGE2 and 6-keto-PGF1α release
Confluent PTSMCs and PASMCs cultured on 6-well plates were washed twice with
phosphate-buffed saline (PBS) and incubated in 1 ml of serum-free medium
containing 0.1% BSA in a 37oC humidified incubator with an atmosphere of 95%
air and 5% CO2. After a 30-minute equilibration period, cells were pre-stimulated
with 100 nM noradrenaline for 5 minutes and stimulated with the angiotensin
peptide for a further 5 minutes; the timing for addition of noradrenaline and
angiotensin peptide was to enable correlation with results obtained from isolated
tissue experiments. After incubation, the medium was aspirated and prostaglandin
levels in the medium were determined using the prostaglandin E2 and 6-keto-
prostaglandin F1ά (stable metabolite of prostaglandin I2) enzyme immunoassay kits
from Assay Designs, Inc, MI, USA.
The angiotensin peptides tested include angiotensin II (100 nM), angiotensin III
(100 nM) and angiotensin IV (10 µM). To investigate the effects of losartan (1
µM), PD123319 (10 µM) and indomethacin (10 µM) on angiotensin-induced
prostaglandin release, these compounds were added to the wells at the start of the
30-minute equilibration period.
5.3.1.3 Expression of results and statistical analysis
PGE2 and 6-keto-PGF1α content of aspirated culture medium was expressed as %
basal PGE2 or % basal 6-keto-PGF1α. Basal PGE2 and 6-keto-PGF1α was defined as
98

basal PGE2 and 6-keto-PGF1α release prior to the addition of noradrenaline and
angiotensin peptide. Control PGE2 and 6-keto-PGF1α were defined as the
noradrenaline-induced PGE2 and 6-keto-PGF1α release prior to the addition of
angiotensin peptide. All statistical comparisons were performed using the general
linear method (univariate) with Tukey’s multiple range test for a posteriori
comparisons.
5.3.2 Inositol triphosphate studies
5.3.2.1 Preparation of tissue
Fresh rabbit pulmonary trunks were removed into ice-cold carbogen-saturated
Krebs solution as previously described. Connective and adipose tissue were gently
removed. The vessels were cut open and denuded of endothelium by gently rubbing
the luminal surface with cotton buds. Cross-chopped pulmonary trunk tissue slices
(200 x 200 µm) were prepared using a McIlwain tissue chopper. The tissue slices
were then suspended in 20 ml ice-cold carbogen-saturated Krebs solution per gram
of tissue and incubated for 1 hour at 37oC in a shaking water bath with replacement
of carbogen-saturated Krebs solution every 15 minutes.
5.3.2.2 Agonist reaction
Chopped tissue slices were dispensed as 170-µl aliquots into polypropylene flat-
bottomed vials containing Krebs solution to yield a final volume of 300 µl after
addition of agonist. The tissue slices were incubated for 15 minutes before the
addition of agonist. After addition of agonist, the reaction was terminated at
99

selected times by addition of 100 µl of 1.2 M ice-cold perchloric acid. The vials
were chilled on ice for 15 minutes before the mixture was neutralized with 100 µl
of 1.2 M freshly prepared potassium bicarbonate. The suspension was centrifuged
for 10 minutes at 3,000 g at 4oC and the supernatant stored at -20oC for less than 6
weeks before analysis.
All additions of agonists were made in a volume of 15 µl. The agonists used were
100 nM angiotensin II and 10 µM angiotensin IV.
5.3.2.3 IP3-binding assay
The binding assay was carried out using an IP3 kit (D-myo-Inositol 1,4,5-
triphosphate (IP3) [3H]assay system, Amersham Pharmacia Biotech).
Briefly, assays were performed at 4oC in a final volume of 400 µl. 100 µl of assay
buffer, 100 µl of diluted tracer ([3H]IP3) and 100 µl of IP3 bovine adrenal binding
protein were added to 100 µl of sample (supernatant) or 100 µl containing a known
amount of IP3,. The mixtures were vortex mixed, incubated on ice for 15 minutes
and centrifuged for 10 minutes at 2,000 g at 4oC to separate the bound and free
[3H]IP3. The supernatant was discarded and the [3H]IP3 bound to the receptor was
extracted by adding 1 ml of 0.15 M sodium hydroxide, vortex mixing and
incubating the mixture at room temperature for 10 minutes. The extract was
neutralized with 50 µl of 10 % acetic acid, vortex mixed, decanted into scintillation
100

vials, mixed with 10 ml of scintillation fluid and counted in a β-scintillation
counter.
5.4 Results
5.4.1 Prostaglandin studies
In noradrenaline-stimulated pulmonary artery smooth muscle cells (PASMCs),
angiotensin II caused a significant 2.6-fold increase in both PGE2 and PGI2
(measured as its stable metabolite 6-keto-PGF1α) after 5 minutes (Figure 5.1). In
similarly treated pulmonary trunk smooth muscle cells (PTSMCs), angiotensin II
caused a 2.6-fold increase in PGE2 and a 6.1-fold increase in PGI2 above
noradrenaline-induced PG release (Figure 5.1). These angiotensin II-induced PG
release was completely inhibited by losartan and indomethacin. In contrast, the AT2
antagonist, PD123319 did not block the angiotensin II-induced release of
prostaglandins, suggesting that this effect is mediated only by the AT1 receptor.
Angiotensin III caused a 2.7-fold increase in PGE2 and a 1.6-fold increase in PGI2 in
PASMCs, and a 1.8-fold increase in PGE2 and a 1.7-fold increase in PGI2 in
PTSMCs (Figure 5.2). Smaller increases in PGE2 (1.4-fold) and PGI2 (0.4-fold) in
PASMCs and in PGE2 (1.7-fold) and PGI2 (1.5-fold) in PTSMCs were also
observed with angiotensin IV (Figure 5.3). However, both the angiotensin III and
angiotensin IV-induced increase in prostaglandins were not statistically different
from control (i.e., noradrenaline-induced PG release), except the angiotensin III-
induced PGE2 release from PASMCs and angiotensin IV-induced PGE2 release
from PTSMCs. There were no significant differences in the angiotensin-induced
101

artery
-100-50
050
100150200250300350
NA AngIIAngII + Los AngII + PDAngII + Indo
trunk
**
artery
-100-50
050
100150200250300350
trunk
****
**
**
**
**
* *
***
**
% b
asal
PG
E2%
bas
al 6
-ket
o-PG
F1a
Figure 5.1 Stimulation of prostaglandin E2 (PGE2) and 6-keto-prostaglandin F1α (6-keto-PGF1α) production in rabbit pulmonary trunk and artery vascular smooth muscle cells by angiotensin II. Increases in PGE2 and 6-keto-PGF1α production are given as a percentage of the basal PG level and represents the means ± SEM of 5 independent experiments performed in duplicate. *significantly different from control PG. **significantly different from angiotensin II-induced PG.
102

**
trunk
artery
-100-50
050
100150200250300350
trunk
**
**
artery
-100
-50
0
50
100
150
200
250
300
350
NA AngIIIAngIII + Los AngIII + PDAngIII + Indo
**
*
**%
bas
al P
GE2
% b
asal
6-k
eto-
PGF1
a
Figure 5.2 Stimulation of prostaglandin E2 (PGE2) and 6-keto-prostaglandin F1α (6-keto-PGF1α) production in rabbit pulmonary trunk and artery vascular smooth muscle cells by angiotensin III. Increases in PGE2 and 6-keto-PGF1α production are given as a percentage of the basal PG level and represents the means ± SEM of 9 independent experiments performed in duplicate. *significantly different from control PG. **significantly different from angiotensin III-induced PG.
103

artery
-100
-50
0
50
100
150
200
250
300
350
artery
-100
-50
0
50
100
150
200
250
300
350
NA AngIVAngIV + Los AngIV + PDAngIV + Indo
**
trunk
*
**
trunk
**
% b
asal
PG
E2%
bas
al 6
-ket
o-PG
F1a
***
Figure 5.3 Stimulation of prostaglandin E2 (PGE2) and 6-keto-prostaglandin F1α (6-keto-PGF1α) production in rabbit pulmonary trunk and artery vascular smooth muscle cells by angiotensin IV. Increases in PGE2 and 6-keto-PGF1α production are given as a percentage of the basal PG level and represents the means ± SEM of 6 independent experiments performed in duplicate. *significantly different from control PG. **significantly different from angiotensin II-induced PG.
104

increase in PGE2 and PGI2 between PTSMCs and PASMCs for all three angiotensin
peptides tested.
5.4.2 Inositol triphosphate studies
Rabbit pulmonary trunk tissue slices had an average basal IP3 mass level of 153.5 ±
39.9 pmol/mg protein. Angiotensin II induced a rapid increase in IP3 (3.3-fold),
with peak IP3 production within 15 seconds of angiotensin II stimulation, and a
return to baseline levels thereafter (Figure 5.4). In contrast, angiotensin IV
stimulated a minimal increase in IP3 (Figure 5.5).
5.5 Discussion
In order to address two key questions we focused in on the intracellular processes
responsible for vasoconstriction and vasodilation in VSMCs. Firstly, does the AT1
receptor mediate distinct and opposite biological responses in the rabbit pulmonary
trunk and artery due to differences in the receptor-coupled signal transduction
cascade? Secondly, what is the principle component of the intracellular signaling
cascade that mediates this action? Although the production of IP3 and
prostaglandins are well documented events following angiotensin II stimulation, the
present study profiled and compared for the first time the angiotensin II-,
angiotensin III- and angiotensin IV-induced prostaglandin and IP3 release from the
rabbit pulmonary trunk and artery.
105

AngII-induced IP3 release
0 5 10 15 20 25 30 35 40 45 50 55 60
0100200300400500600700800
Time (s)
IP3
(pm
ol/m
g pr
otei
n)
Figure 5.4 Stimulation of inositol triphosphate production in rabbit pulmonary trunk tissue by angiotensin II over time. Increases in inositol triphosphate production are given in pmoles per mg protein and represents means ± SEM of 4 independent experiments done in duplicate.
106

AngIV-induced IP3 release
0 5 10 15 20 25 30 35 40 45 50 55 60
0100200300400500600700800
Time (s)
IP3
(pm
ol/m
g pr
otei
n)
Figure 5.5 Stimulation of inositol triphosphate production in rabbit pulmonary trunk tissue by angiotensin IV over time. Increases in inositol triphosphate production are given in pmoles per mg protein and represents means ± SEM of 3 independent experiments done in duplicate.
107

The results of the present study showed that angiotensin II increased the production
of two intracellular signaling molecules, PGE2 and PGI2, in the rabbit pulmonary
trunk and artery. This finding is consistent with previous findings showing that
angiotensin II stimulates the synthesis of vasodilator prostaglandin in vascular
tissues and vascular cells in culture, which functions to modulate the vascular effect
of angiotensin II (Webb, 1982; Wilcox and Lin, 1993). The inhibition of
angiotensin II-induced prostaglandin production by losartan demonstrates the role
of the AT1 receptor in mediating prostaglandin synthesis in the rabbit pulmonary
vasculature, which corresponds to similar findings by other studies (Rao et al.,
1994; Shinoda et al., 1997; Muthalif et al., 1998; Freeman et al., 1998; Silfani and
Freeman, 2002). Interestingly, the high levels of PG production stimulated by
angiotensin II in the pulmonary trunk could explain the vasodilation observed in 6
our of 16 pre-contracted tissue in the isolated tissue experiments (see Figure 2.4,
page 56). The stimulation of pulmonary trunk and artery VSMCs by angiotensin III
and angiotensin IV is associated with an increase in both vasodilator prostaglandins
and a reduction of this release by losartan and indomethacin. However, these
findings were not statistically significant probably due to the high inter-sample
variability observed. A possible explanation for the variability observed may be a
result of phenotypic variations through the continual passage of cells. VSMCs are
reported to modulate from a physiological ‘contractile state’ to a more ‘synthetic
state’ when in culture (Chamley-Campbell et al., 1979). High seeding densities and
a short time to confluency are some of the factors that help to maintain cells in their
physiological contractile state (McMurray et al., 1991; Birukov et al., 1993). In our
108

experiments, cells from passage 5-12 were used. The variability may be contributed
by PG release from cells from different passages. Interestingly, the prostaglandin
levels did not differ between the pulmonary trunk and artery SMCs for all
angiotensin peptides tested, suggesting that it is unlikely that the opposing
contractile and relaxant responses observed in the pulmonary artery and trunk were
a consequence of correspondingly low and high levels of synthesis of vasodilator
prostaglandins, respectively.
Following this finding, we next investigated if a difference in the IP3 signaling
component might be responsible for the heterogeneous response of rabbit
pulmonary trunk and artery to angiotensin peptides. Our present findings
demonstrate that angiotensin II stimulates a higher production of IP3 in pulmonary
trunk tissue slices compared to that by angiotensin IV, suggesting that the
differential angiotensin II-induced vasoconstrictor response and angiotensin IV-
induced vasorelaxant response in the rabbit pulmonary trunk may be due to higher
amounts of the IP3 second messenger being produced when stimulated by
angiotensin II compared to angiotensin IV.
The use of different tissue types for the measurement of PGs and IP3, i.e., use of
cultured SMCs for PG measurement and tissue slices for IP3 measurement, can
make direct comparisons of IP3 versus PG release in the same tissue difficult. In any
future experiments, an improved methodology would allow the simultaneous
measurement of agonist-induced IP3 production and AA release from the same
109

population of cells/tissue. However, it should be noted that the design and findings
of this study sought to determine if a contractile response was a result of a
predominance of contractile signaling pathways over relaxant pathways and vice
versa for relaxant responses. Therefore the findings of this study were adequate to
address this question even though the assays were performed in different tissue
systems.
Taken together with the results from the prostaglandin studies, the present findings
indicate that the response seen in the pulmonary vasculature is likely a result of a
balance of contractile and relaxant signaling components. In the pulmonary artery,
angiotensin II and angiotensin III stimulate a higher level of IP3 that predominates
over the simultaneous production of vasodilator prostaglandin, resulting in an
overall contractile response. In the pulmonary trunk, because lower levels of IP3 are
produced, the vasodilator effect of prostaglandins predominates, resulting in
vasorelaxation. Our present findings suggest that in the rabbit pulmonary trunk, the
contractile response seen with angiotensin II, in contrast to a relaxant response seen
with angiotensin IV, was due to a predominant IP3 signaling mechanism that masks
the vasorelaxing effect of the simultaneous production of vasodilator
prostaglandins, while angiotensin IV stimulation results in a weak IP3 response
which is insufficient to overwhelm the modulating effect of vasodilator
prostaglandins. This results in an overall relaxant response instead (Figure 5.6).
110

Ang II / Ang IV
CONTRACTION RELAXATION
IP3 DAG
Ca
PA
PIP2 PC PC
PLC PLD
PP
AA
PLA2
PGE2, PGI2
plasmamembrane
RESULTANT RESPONSE
AT1 rec
G protein
DAG lipase
Ras/MAPKpathway
Figure 5.6 Scheme demonstrating mechanisms whereby angiotensin II and angiotensin IV stimulation of the AT1 receptor can elicit different cellular responses. The resultant response, i.e., contraction or relaxation is dependent on the predominance of one signal transduction pathway over another. Cross talk can occur between the multiple signal transduction pathways activated.
111

Multiple mechanisms of divergence may contribute to the multiple signal
transduction pathways, i.e., IP3 and PG signaling pathways, stimulated by
angiotensins in the rabbit pulmonary vasculature. One of the first possibilities we
considered was the presence of two or more receptor subtypes mediating distinct
signal transduction pathways possibly via distinct G protein couplings. However,
both receptor binding and Northern blot analyses suggested that only a single
receptor subtype mediated these responses. Our isolated tissue and current findings
also support the notion that a single AT1 receptor was involved, and it is possible
that this receptor is coupled to a single G protein which, when activated, triggers the
activation of multiple signaling pathways that contribute to the final vascular
response. There is increasing evidence to suggest that cross-talk occurs between
intracellular effectors activated by angiotensin II. For example, angiotensin II
stimulates the Gαq/11-coupled PLC-dependent hydrolysis of PIP2 to yield IP3 and
DAG (Griendling et al., 1989). These messengers mediate the intracellular release
of Ca2+ and activate PKC, respectively. DAG can be converted to AA by the action
of DAG lipase, which can be metabolized to prostaglandins (Billah, 1993). In
addition, both Ca2+ and PKC have been implicated in a number of cross-regulation
of other signaling pathways, including the Ca2+- and CaM kinase II-dependent
phosphorylation and activation of cytosolic cPLA2 (Muthalif et al., 1998).
Moreover, the temporal characteristics of each divergent signaling pathway may
also contribute to the fine-tuning of angiotensin responses. For example,
angiotensin II has also been shown to activate PLD, which hydrolyzes
phosphatidylcholine (PC) to choline and phosphatidic acid (Ushio-Fukai et al.,
112

1999). Recent studies suggest that the PLD pathway contributes in part to the
sustained production of prostaglandins via the formation of DAG in VSMCs
(Gomez-Cambronero et al., 1998) and represents the major pathway by which PKC
remains activated (Lassegue et al., 1993; Dhalla et al., 1997). The qualitative and
temporal interaction between multiple signaling pathways may contribute to the
coordinated angiotensin response seen in the rabbit pulmonary vasculature.
It is also possible that a single AT1 receptor coupled to a single G protein may
mediate signal divergence via Gα as well as the Gβγ subunit. A critical role of Gβγ
as a signal transducer for PLC activation was demonstrated by the inhibition of
angiotensin II-stimulated IP3 formation by electroporation of anti-Gβγ antibody in
rat VSMCs (Ushio-Fukai et al., 1998). Since it has been suggested that Gβγ-
mediated activation of PLC-β is associated with a relatively low increase in IP3
(Zhang and Muallem, 1992), it is possible that both Gβγ and Gαq/11 cooperatively
activate PLC-β to produce large amounts of IP3 in intact VSMCs. Gβγ derived from
Gα12/13 has also been found to transduce AT1 receptor-mediated tonic PLD
activation in rat VSMCs (Sasaki et al., 1991).
However, the question still remains of how differential responses are obtained by
different angiotensin agonists acting on the same AT1 receptor in the pulmonary
trunk. Angiotensin IV is generally considered a weak agonist of the AT1 receptor,
thus one general mechanism is through differences in the strength of the stimulus by
angiotensin II and angiotensin IV. For example, if one second messenger triggers
113

the activation of a second measurable response, the magnitude of the second
response will be more sensitive to the strength of the original signal (Kenakin,
1995). Therefore, an angiotensin peptide with a higher efficacy, e.g., angiotensin II,
may produce measurable effects from both signaling pathways, i.e., IP3 and PG
production, while the peptide with a lower efficacy, e.g., angiotensin IV, may
produce measurable effects from the second pathway, i.e., PG production, but
extremely low amounts of the first, IP3 production. The other mechanism is via the
recently proposed agonist-directed trafficking of receptor signals (Kenakin, 1995).
Agonist-directed trafficking is a phenomenon whereby agonists preferentially select
for one of several receptor conformations, and selectively activate a subset of the
multiple signal transduction pathways that may be coupled to a single receptor
subtype. The existence of intermediate or multiple active conformations of GPCRs
have already been described previously (Gether, 1998, 2000; Kenakin and Onaran,
2002). It has been shown that the AT1 receptor can attain distinct conformations
leading to phosphorylation and/or inositol phosphate signaling using angiotensin II
and Sar1-Ile4-Ile8-angiotensin II, an analog that only activates signaling through the
constitutive receptors, which underlines the importance of multiple active
conformations of the AT1 receptor (Thomas, 2000).
Finally, the possibility of a single AT1 receptor coupling to multiple G proteins with
distinct signaling pathways in the rabbit pulmonary vasculature cannot be ruled out.
The first evidence for functional coupling of the AT1 receptor with multiple G
proteins of different classes was demonstrated in 7315c cells (derived from a rat
114

anterior pituitary tumour) expressing angiotensin receptors by Crawford and
colleagues (1992). The findings from this study indicated that, in addition to the
AT1-mediated inhibition of adenylate cyclase via the pertussis toxin-sensitive Gi/o
protein, the AT1 receptor stimulated IP3 production via a G protein that was
insensitive to pertussis toxin. In a separate study, Ushio-Fukai and collegues also
showed that the coupling of AT1 receptor in rat VSMCs to both Gαq/11 and Gα12
proteins was necessary to activate PLC-β (1998). Electroporation of anti-Gαq/11 and
-Gα12 antibodies significantly inhibited the angiotensin II-induced IP3 production in
these cells.
The angiotensin IV-stimulated relaxant response mediated by AT1 receptors was an
unexpected finding, since studies on angiotensin IV have reported either a weak
contractile response mediated via AT1 receptors (Wright et al., 1996; Champion et
al., 1998, 1999; Fitzgerald et al., 1999) or a relaxant response mediated via AT4
receptors in the vasculature (Kramar et al., 1997, 1998; Patel et al., 1998; Coleman
et al., 1998; Hill-Kapturczak et al., 1999). This is the first report to our knowledge
of a relaxant response of angiotensin IV mediated by AT1 receptors. Angiotensin II
is converted to angiotensin IV by the action of APA and APN that sequentially
cleave two amino acids from the peptide (Reaux et al., 1999a, b). In the pulmonary
trunk, the vasorelaxant action of angiotensin IV, which is formed when angiotensin
II is metabolized, may contribute to the modulation of contractile actions mediated
by angiotensin II. Importantly, this fine-regulation of angiotensin responses in the
pulmonary trunk, which receives blood directly from the right ventricle, may play a
115

role in the protection of the delicate pulmonary capillaries from excessive systolic
pressure. Understanding these protective mechanisms may have important
therapeutic implications in the treatment of pulmonary hypertension.
In conclusion, our present findings demonstrate that AT1 receptors in the rabbit
pulmonary trunk and artery are coupled to multiple signal transduction pathways.
Stimulation of the pulmonary trunk and artery with angiotensin II and its immediate
metabolites, angiotensin III and angiotensin IV, results in a coherent response that
is a composite of the multiple, often functionally opposing signaling cascades. This
complex regulation of the rabbit pulmonary vasculature may represent a novel
mechanism for generating an adequate, highly organized and coherent signal in
response to environmental factors and suggests that the vessel is not just a passive
conduit but may be an important regulator of blood flow from the heart to the lung.
116

CHAPTER 6
GENERAL DISCUSSION
Angiotensins play a fundamental role in controlling the functional and structural
integrity of the arterial wall and are involved in the physiological processes
regulating blood pressure and in pathological mechanisms underlying vascular
disease. The majority of the effects of angiotensins in vascular responses are
mediated by angiotensin II acting on the AT1 receptor subtype (Touyz and
Schriffin, 2000). New evidence is emerging that demonstrates, in addition to
angiotensin II and III, bioactivity of a variety of angiotensin fragments, e.g. des-
Asp-angiotensin I (Sim and Soh, 1995; Sim and Chai, 1996; Sim and Min, 1998;
Min et al., 2000), angiotensin IV (Wright et al., 1995) and angiotensin (1-7)
(Ferrario et al., 1998). In addition, putative binding sites for angiotensin IV (AT4)
and angiotensin (1-7) have been demonstrated and pharmacologically characterized
(Wright et al., 1994; Hanesworth et al., 1993; Swanson et al., 1992; Hall et al.,
1993; Bernier et al., 1995; Nuess et al., 1994), although their cloning has not been
reported. These recent findings have challenged the ‘single’ regulatory peptide and
receptor concept of the renin angiotensin system and opened up the possibilities of
poly functional angiotensins in the system.
Angiotensin II elicits complex highly regulated cascades of intracellular signal
transduction that lead to short term vascular effects, such as contraction, and to
long-term biological effects, such as cell growth, migration, extracellular matrix
117

deposition, and inflammation. Because of its important role in cardiovascular
diseases associated with vascular smooth muscle cell contraction and growth such
as hypertension and atherosclerosis, understanding the mechanisms of actions and
interactions between angiotensin II and its metabolites is of crucial importance.
Here we provide evidence confirming segment to segment variations previously
reported in the rabbit pulmonary trunk and artery (Sim and Soh, 1995; Sim and
Chai, 1996) to angiotensin II and its immediate metabolites, angiotensin III and
angiotensin IV and propose the cellular mechanisms responsible for this fine
regulation of pulmonary blood flow from the heart to the lung. Isolated tissue
experiments show that administration of angiotensin III, angiotensin IV, and in
some cases angiotensin II, produce opposing responses in the pulmonary trunk and
artery, respectively, as previously described for the angiotensin peptide, des-Asp-
angiotensin I (Sim and Soh, 1995; Sim and Chai, 1996). The differential response
between the pulmonary trunk and artery to angiotensin peptides suggests the
existence of two AT1 receptors. Our findings correlated with a recent report
showing that angiotensin III produced a pressor followed by a depressor response in
conscious rabbits (Rowe and Byron, 2000). Different receptor mechanisms were
initially proposed to mediate the opposing responses since equipressor doses of
angiotensin II were less effective at producing depressor responses. However, both
pressor and depressor responses were demonstrated to be mediated by AT1
receptors since losartan abolished both responses whereas PD 123319 had no effect.
118

Similar opposing contractile and relaxant responses mediated by AT1 receptors
have also been previously reported (Yoshikazu et al., 1995). Angiotensin II was
shown to contract canine pulmonary artery and relax the pulmonary vein. Losartan
abolished both the artery contraction and the vein relaxation whereas indomethacin
augmented the artery contraction and abolished the vein relaxation, suggesting the
involvement of AT1 receptors and the production of vasodilator PGs in both
responses.
To explore the presence of more than one AT1 receptor subtypes in the rabbit
pulmonary vasculature, we characterised the angiotensin receptors in the rabbit
pulmonary trunk and artery by receptor binding studies and RNA analysis. Labelled
125I-Sar1-Ile8-angiotensin II bound to both rabbit pulmonary trunk and artery tissue
with high affinity and was displaced by Sar1-Ile8-angiotensin II, losartan,
angiotensin II, angiotensin III, des-Asp-angiotensin I and angiotensin IV but not by
PD123319 and divalinal-angiotensin IV, suggesting the existence of a single class
of AT1 receptors in the pulmonary vascular tissue. These data were supported by
our finding, using Northern blot analysis, of a single AT1 receptor mRNA in both
pulmonary trunk and artery tissue. Consistent with our results, Burns et al. (1993)
previously reported the existence of a single AT1 receptor gene in the rabbit.
How then is this differential response mediated? First, are there still unidentified
receptor subtypes? Second, are the signaling pathways different in the pulmonary
trunk and artery or are the signaling cascades agonist-dependent?
119

There remains a possibility that rabbit AT1 receptor subtypes and/or splice variants
exist but were not detected by Southern (Burns et al., 1993) or Northern blot
analyses. This may occur if the base sequences between subtypes share a low
homology such that the receptor probe hybridizes to one but not the other receptor
subtype, or if they do not differ significantly in length to be visualized as distinct
bands in a Northern blot.
To elucidate the signaling mechanisms in the rabbit pulmonary trunk and artery, we
carried out both IP3 and PG measurements. The rationale for investigating these
signaling molecules was that the PLC-IP3-Ca2+ cascade is the major signaling
pathway for vascular contraction and vasodilator PGs were implicated in the
angiotensin-induced relaxation in the rabbit pulmonary trunk as demonstrated by
the inhibitory effect of indomethacin. Our results demonstrate that angiotensin II
significantly increased the synthesis of vasodilator PGE2 and PGI2 in the rabbit
pulmonary trunk and artery, with angiotensin III and angiotensin IV showing a
similar trend in increasing PG synthesis. This supports previous findings by Wilcox
and Lin (1993) of angiotensin-stimulated prostaglandin synthesis in the vasculature
and corroborates the well established role of vasodilator PGs in attenuating
angiotensin responses (Muthalif et al., 1998). Interestingly, when we compared PG
levels in angiotensin-stimulated rabbit pulmonary trunk and artery, no significant
differences were observed. This suggested that it is unlikely that a higher level of
120

PG synthesis in the pulmonary trunk, relative to the artery, accounted for its
predominantly vasorelaxant response to angiotensins.
Because angiotensin II elicits a similar contractile response in both the rabbit
pulmonary trunk and artery, we next compared the IP3 signaling profile mediated by
angiotensin II and angiotensin IV in the pulmonary trunk. We found that
angiotensin II stimulates a higher production of IP3 in pulmonary trunk tissue slices
compared to that by angiotensin IV. Taken together, these results suggest that when
AT1 receptors are stimulated in the rabbit pulmonary vasculature, IP3 and PG
signaling cascades are activated. The resultant vascular response is a balance of
contractile and relaxant signaling components which are regulated by synergistic
interactions and cross-talk between these signaling pathways.
Traditionally, signal transduction pathways are conceptualized in a linear fashion,
i.e., one receptor subtype coupling to one G protein that activates one effector.
However, recent evidence has accumulated that demonstrate that the same AT1
receptor can be coupled to different G protein and/or signaling cascades in the same
tissue, either simultaneously or in a sequential manner, to elicit multiple
intracellular signals (Crawford et al., 1991; Ushio-Fukai et al., 1998; Permentier et
al., 2001). For example, Ushio-Fukai et al. (1998) has previously reported that the
dual coupling of AT1 receptors in rat VSMCs to both Gαq/11 and Gα12 proteins was
necessary for angiotensin II-induced PLC-β1 activation. In addition, the angiotensin
II-induced IP3 production was mediated by the sequential activation of PLC-β1 and
121

PLC-γ, suggesting a novel mechanism for a temporally controlled, highly organized
and convergent angiotensin-signaling network in VSMCs. Angiotensin II was also
reported to sequentially activate cPLA2 and PLD via AT1 receptors in rabbit
VSMCs (Permentier et al., 2001). In this study, the angiotensin II-induced PLD
activation was shown to be mediated by arachidonic acid metabolites generated
from the initial stimulation of cPLA2. Thus it is becoming clear that AT1 receptors
couple to multiple G proteins and/or signaling cascades, as has been reported with
other G protein-coupled receptors (Hermans, 2003). These synergistic interactions
between multiple G protein signaling pathways may have an important role in fine-
tuning vascular angiotensin responses.
In addition, recent studies using constitutively activated mutant AT1 receptors
provide evidence for agonist-dependent conformational selection of the AT1
receptor (Thomas et al., 2000; Hunyady et al., 2003), which has also been reported
in other GPCRs (Strange, 1999). Constitutive activation of the AT1 receptor by
mutations of Asn111 in the third transmembrane helix, the interacting residue for
Tyr4 of angiotensin II, suggests that the AT1 receptor is maintained in an inactive
conformation by stabilizing intramolecular interactions which are released upon
agonist binding (Noda et al., 1996; Balmforth et al., 1997; Groblewski et al., 1997).
It was proposed that the activation of the AT1 receptor may involve the initial
disruption of Asn111-dependent stabilizing interactions by Arg2 of angiotensin II,
which subsequently allows the receptor to be fully activated. This may account for
the lack of potency of angiotensin IV for the wild-type AT1 receptor since it does
122

not contain the Arg2 residue. Supporting this hypothesis was the increased affinity
of angiotensin IV for these constitutively active AT1 receptors (Le et al., 2002).
Importantly, agonist-dependent conformational selection of the vascular AT1
receptor influences our understanding of the role of bioactive angiotensin fragments
in regulating vascular responses to angiotensins.
Tissue heterogeneity may also contribute to regional differences in vascular
response to angiotensins. Different cell population within media smooth muscle
layer in cell wall exist (Archer, 1996; Frid et al., 1997) which may possess different
sets of signaling proteins that contribute to the heterogeneous responses when the
AT1 receptor is stimulated in different cells or segments of the pulmonary
vasculature. The metabolic pathways of angiotensin peptides may also serve as a
further fine-tuning tool. Angiotensin II may be broken down to an angiotensin
peptide that has a lower efficacy in vasoconstriction or may act on its own receptor
to oppose the original angiotensin II response. Finally the roles of AT1 receptor
splice variants in providing a further level of fine control of angiotensin responses
remain to be established.
Altogether, these processes provide cells with a diverse repertoire of mechanisms
for fine-tuning angiotensin responses that are appropriately adaptive to specific
environmental signals. Recent evidence suggests that the renin-angiotensin system
may play a role in contributing to the pathogenesis of pulmonary hypertension,
since irbesartan, an AT1 receptor antagonist, was shown to prevent lung structural
123

remodeling and pulmonary hypertension following myocardial infarct in rats
(Jasmin et al., 2003). As pulmonary vasoconstriction is a feature of pulmonary
hypertension, understanding the role of angiotensins in regulating the pulmonary
circulation may open up novel therapies that target the renin-angiotensin system in
the management of pulmonary hypertension.
Our present findings urge a re-evaluation of the complexity of angiotensin signaling
and the role of the RAS in vascular diseases. Only a complete understanding of the
mechanisms involved in angiotensin receptor activation and intracellular signaling
pathways will enable targeted therapies to be developed, which can compensate for
the intrinsic variation in the function of the angiotensin receptor throughout the
vasculature. The data presented in this thesis represents a significant step in this
direction.
124

REFERENCES AbdAlla S, Lother H, Quitterer U: AT1-receptor heterodimers show enhanced G-protein activation and altered receptor sequestration. Nature 2000, 407:94-98.
Ahmad S, Ward PE: Role of aminopeptidase activity in the regulation of the pressor activity of circulating angiotensins. J.Pharmacol.Exp.Ther. 1990, 252:643-650.
Aiyar N, Baker E, Wu HL, Nambi P, Edwards RM, Trill JJ, Ellis C, Bergsma DJ: Human AT1 receptor is a single copy gene: characterization in a stable cell line. Mol.Cell Biochem. 1994, 131:75-86.
Allen AM, Zhuo J, Mendelsohn FA: Localization and function of angiotensin AT1 receptors. Am.J.Hypertens. 2000, 13:31S-38S.
Ambuhl P, Felix D, Khosla MC: [7-D-ALA]-angiotensin-(1-7): selective antagonism of angiotensin-(1-7) in the rat paraventricular nucleus. Brain Res.Bull. 1994, 35:289-291.
Archer SL: Diversity of phenotype and function of vascular smooth muscle cells. J.Lab Clin.Med. 1996, 127:524-529.
Ardaillou R: Angiotensin II receptors. J.Am.Soc.Nephrol. 1999, 10 Suppl 11:S30-S39.
Arnaudeau S, Macrez-Lepretre N, Mironneau J: Activation of calcium sparks by angiotensin II in vascular myocytes. Biochem.Biophys.Res.Commun. 1996, 222:809-815.
Baker KM, Aceto JF: Angiotensin II stimulation of protein synthesis and cell growth in chick heart cells. Am.J.Physiol 1990, 259:H610-H618.
Baker KM, Booz GW, Dostal DE: Cardiac actions of angiotensin II: Role of an intracardiac renin- angiotensin system. Annu.Rev.Physiol 1992, 54:227-241.
Balmforth AJ, Lee AJ, Warburton P, Donnelly D, Ball SG: The conformational change responsible for AT1 receptor activation is dependent upon two juxtaposed asparagine residues on transmembrane helices III and VII. J.Biol.Chem. 1997, 272:4245-4251.
Benter IF, Diz DI, Ferrario CM: Pressor and reflex sensitivity is altered in spontaneously hypertensive rats treated with angiotensin-(1-7). Hypertension 1995, 26:1138-1144.
125

Bentley JK, Beavo JA: Regulation and function of cyclic nucleotides. Curr.Opin.Cell Biol. 1992, 4:233-240.
Berg KA, Maayani S, Goldfarb J, Scaramellini C, Leff P, Clarke WP: Effector pathway-dependent relative efficacy at serotonin type 2A and 2C receptors: evidence for agonist-directed trafficking of receptor stimulus. Mol.Pharmacol. 1998, 54:94-104.
Bergsma DJ, Ellis C, Kumar C, Nuthulaganti P, Kersten H, Elshourbagy N, Griffin E, Stadel JM, Aiyar N: Cloning and characterization of a human angiotensin II type 1 receptor. Biochem.Biophys.Res.Commun. 1992, 183:989-995.
Berk BC, Corson MA: Angiotensin II signal transduction in vascular smooth muscle: role of tyrosine kinases. Circ.Res. 1997, 80:607-616.
Bernier SG, Servant G, Boudreau M, Fournier A, Guillemette G: Characterization of a binding site for angiotensin IV on bovine aortic endothelial cells. Eur.J.Pharmacol. 1995, 291:191-200.
Billah MM: Phospholipase D and cell signaling. Curr.Opin.Immunol. 1993, 5:114-123.
Birukov KG, Frid MG, Rogers JD, Shirinsky VP, Koteliansky VE, Campbell JH, Campbell GR: Synthesis and expression of smooth muscle phenotype markers in primary culture of rabbit aortic smooth muscle cells: influence of seeding density and media and relation to cell contractility. Exp.Cell Res. 1993, 204:46-53.
Blair-West JR, Coghlan JP, Denton DA, Funder JW, Scoggins BA, Wright RD: The effect of the heptapeptide (2-8) and hexapeptide (3-8) fragments of angiotensin II on aldosterone secretion. J.Clin.Endocrinol.Metab 1971, 32:575-578.
Bolton TB: Mechanisms of action of transmitters and other substances on smooth muscle. Physiol Rev. 1979, 59:606-718.
Bomtempo CA, Santos GF, Santos RA, Campagnole-Santos MJ: Interaction of bradykinin and angiotensin-(1-7) in the central modulation of the baroreflex control of the heart rate. J.Hypertens. 1998, 16:1797-1804.
Bonnardeaux A, Davies E, Jeunemaitre X, Fery I, Charru A, Clauser E, Tiret L, Cambien F, Corvol P, Soubrier F: Angiotensin II type 1 receptor gene polymorphisms in human essential hypertension. Hypertension 1994, 24:63-69.
Bonventre JV: Phospholipase A2 and signal transduction. J.Am.Soc.Nephrol. 1992, 3:128-150.
126

Bouchard JF, Dumont E, Lamontagne D: Evidence that prostaglandins I2, E2, and D2 may activate ATP sensitive potassium channels in the isolated rat heart. Cardiovasc.Res. 1994, 28:901-905.
Boulanger CM, Caputo L, Levy BI: Endothelial AT1-mediated release of nitric oxide decreases angiotensin II contractions in rat carotid artery. Hypertension 1995, 26:752-757.
Braszko JJ, Kupryszewski G, Witczuk B, Wisniewski K: Angiotensin II-(3-8)-hexapeptide affects motor activity, performance of passive avoidance and a conditioned avoidance response in rats. Neuroscience 1988, 27:777-783.
Braszko JJ, Wlasienko J, Koziolkiewicz W, Janecka A, Wisniewski K: The 3-7 fragment of angiotensin II is probably responsible for its psychoactive properties. Brain Res. 1991, 542:49-54.
Bredt DS, Mourey RJ, Snyder SH: A simple, sensitive, and specific radioreceptor assay for inositol 1,4,5-trisphosphate in biological tissues. Biochem.Biophys.Res.Commun. 1989, 159:976-982.
Burns KD, Inagami T, Harris RC: Cloning of a rabbit kidney cortex AT1 angiotensin II receptor that is present in proximal tubule epithelium. Am.J.Physiol 1993, 264:F645-F654.
Burns L, Clark KL, Bradley J, Robertson MJ, Clark AJ: Molecular cloning of the canine angiotensin II receptor. An AT1-like receptor with reduced affinity for DuP753. FEBS Lett. 1994, 343:146-150.
Burridge K, Turner CE, Romer LH: Tyrosine phosphorylation of paxillin and pp125FAK accompanies cell adhesion to extracellular matrix: a role in cytoskeletal assembly. J.Cell Biol. 1992, 119:893-903.
Campagnole-Santos MJ, Heringer SB, Batista EN, Khosla MC, Santos RA: Differential baroreceptor reflex modulation by centrally infused angiotensin peptides. Am.J.Physiol. 1992, 263:R89-R94.
Caron AZ, Arguin G, Guillemette G: Angiotensin IV interacts with a juxtamembrane site on AT(4)/IRAP suggesting an allosteric mechanism of enzyme modulation. Regul.Pept. 2003, 113:9-15.
Carr P, McKinnon W, Poston L: Mechanisms of pHi control and relationships between tension and pHi in human subcutaneous small arteries. Am.J.Physiol. 1995, 268:C580-C589.
Chaki S, Inagami T: Identification and characterization of a new binding site for angiotensin II in mouse neuroblastoma neuro-2A cells. Biochem.Biophys.Res.Commun. 1992, 182:388-394.
127

Challiss RA, Batty IH, Nahorski SR: Mass measurements of inositol(1,4,5)trisphosphate in rat cerebral cortex slices using a radioreceptor assay: effects of neurotransmitters and depolarization. Biochem.Biophys.Res.Commun. 1988, 157:684-691.
Chamley-Campbell J, Campbell GR, Ross R: The smooth muscle cell in culture. Physiol Rev. 1979, 59:1-61.
Champion HC, Czapla MA, Kadowitz PJ: Responses to angiotensin peptides are mediated by AT1 receptors in the rat. Am.J.Physiol 1998, 274:E115-E123.
Champion HC, Bivalacqua TJ, Lambert DG, McNamara DB, Kadowitz PJ: Analysis of the effects of candesartan on responses to angiotensin II in the hindquarters vascular bed of the cat. J.Am.Soc.Nephrol. 1999, 10 Suppl 11:S101-S103.
Chansel D, Czekalski S, Vandermeersch S, Ruffet E, Fournie-Zaluski MC, Ardaillou R: Characterization of angiotensin IV-degrading enzymes and receptors on rat mesangial cells. Am.J.Physiol 1998, 275:F535-F542.
Chappell MC, Gomez MN, Pirro NT, Ferrario CM: Release of angiotensin-(1-7) from the rat hindlimb: influence of angiotensin-converting enzyme inhibition. Hypertension 2000, 35:348-352.
Chauvel EN, Llorens-Cortes C, Coric P, Wilk S, Roques BP, Fournie-Zaluski MC: Differential inhibition of aminopeptidase A and aminopeptidase N by new beta-amino thiols. J.Med.Chem. 1994, 37:2950-2957.
Chidiac P, Hebert TE, Valiquette M, Dennis M, Bouvier M: Inverse agonist activity of beta-adrenergic antagonists. Mol.Pharmacol. 1994, 45:490-499.
Christman BW, McPherson CD, Newman JH, King GA, Bernard GR, Groves BM, Loyd JE: An imbalance between the excretion of thromboxane and prostacyclin metabolites in pulmonary hypertension. N.Engl.J.Med. 1992, 327(2):70-75.
Clapp LH, Turcato S, Hall S, Baloch M: Evidence that Ca2+-activated K+ channels play a major role in mediating the vascular effects of iloprost and cicaprost. Eur.J.Pharmacol. 1998, 356:215-224.
Clark JD, Lin LL, Kriz RW, Ramesha CS, Sultzman LA, Lin AY, Milona N, Knopf JL: A novel arachidonic acid-selective cytosolic PLA2 contains a Ca(2+)- dependent translocation domain with homology to PKC and GAP. Cell 1991, 65:1043-1051.
Clark JD, Schievella AR, Nalefski EA, Lin LL: Cytosolic phospholipase A2. J.Lipid Mediat.Cell Signal. 1995, 12:83-117.
128

Coleman JK, Krebs LT, Hamilton TA, Ong B, Lawrence KA, Sardinia MF, Harding JW, Wright JW: Autoradiographic identification of kidney angiotensin IV binding sites and angiotensin IV-induced renal cortical blood flow changes in rats. Peptides 1998, 19:269-277.
Conti MA, Adelstein RS: The relationship between calmodulin binding and phosphorylation of smooth muscle myosin kinase by the catalytic subunit of 3':5' cAMP- dependent protein kinase. J.Biol.Chem. 1981, 256:3178-3181.
Crawford KW, Frey EA, Cote TE: Angiotensin II receptor recognized by DuP753 regulates two distinct guanine nucleotide-binding protein signaling pathways. Mol.Pharmacol. 1992, 41:154-162.
Curnow KM: Human type-1 angiotensin II (AT1) receptor gene structure and function. Clin.Exp.Pharmacol.Physiol Suppl 1996, 3:S67-S73.
Damron DS, Nadim HS, Hong SJ, Darvish A, Murray PA: Intracellular translocation of PKC isoforms in canine pulmonary artery smooth muscle cells by ANG II. Am.J.Physiol 1998, 274:L278-L288.
de Gasparo M, Husain A, Alexander W, Catt KJ, Chiu AT, Drew M, Goodfriend T, Harding JW, Inagami T, Timmermans PB: Proposed update of angiotensin receptor nomenclature. Hypertension 1995, 25:924-927.
de Gasparo M, Catt KJ, Inagami T, Wright JW, Unger T: International union of pharmacology. XXIII. The angiotensin II receptors. Pharmacol.Rev. 2000, 52:415-472.
De Silva PE, Husain A, Smeby RR, Khairallah PA: Measurement of immunoreactive angiotensin peptides in rat tissues: some pitfalls in angiotensin II analysis. Anal.Biochem. 1988, 174:80-87.
Dennis EA: Diversity of group types, regulation, and function of phospholipase A2. J.Biol.Chem. 1994, 269:13057-13060.
Dennis EA: The growing phospholipase A2 superfamily of signal transduction enzymes. Trends Biochem.Sci. 1997, 22:1-2.
Dhalla NS, Xu YJ, Sheu SS, Tappia PS, Panagia V: Phosphatidic acid: a potential signal transducer for cardiac hypertrophy. J.Mol.Cell Cardiol. 1997, 29:2865-2871.
Diz DI, Ferrario CM: Angiotensin receptor heterogeneity in the dorsal medulla oblongata as defined by angiotensin-(1-7). Adv.Exp.Med.Biol. 1996, 396:225-235.
Ferrario CM, Chappell MC, Tallant EA, Brosnihan KB, Diz DI: Counterregulatory actions of angiotensin-(1-7). Hypertension 1997, 30:535-541.
129

Ferrario CM, Iyer SN: Angiotensin-(1-7): a bioactive fragment of the renin-angiotensin system. Regul.Pept. 1998, 78:13-18.
Fitzgerald SM, Evans RG, Bergstrom G, Anderson WP: Renal hemodynamic responses to intrarenal infusion of ligands for the putative angiotensin IV receptor in anesthetized rats. J.Cardiovasc.Pharmacol. 1999, 34:206-211.
Fournie-Zaluski MC, Coric P, Turcaud S, Bruetschy L, Lucas E, Noble F, Roques BP: Potent and systemically active aminopeptidase N inhibitors designed from active-site investigation. J.Med.Chem. 1992, 35:1259-1266.
Freeman EJ, Chisolm GM, Ferrario CM, Tallant EA: Angiotensin-(1-7) inhibits vascular smooth muscle cell growth. Hypertension 1996, 28:104-108.
Freeman EJ, Ruehr ML, Dorman RV: ANG II-induced translocation of cytosolic PLA2 to the nucleus in vascular smooth muscle cells. Am.J.Physiol 1998, 274:C282-C288.
Frid MG, Dempsey EC, Durmowicz AG, Stenmark KR: Smooth muscle cell heterogeneity in pulmonary and systemic vessels. Importance in vascular disease. Arterioscler.Thromb.Vasc.Biol. 1997, 17:1203-1209.
Furakawa K, Tawada Y, Shigekawa M: Regulation of the plasma membrane Ca2+ pump by cyclic nucleotides in cultured VSMCs. J.Biol.Chem. 1998, 263:8058-8065.
Gailly P, Gong MC, Somlyo AV, Somlyo AP: Possible role of atypical protein kinase C activated by arachidonic acid in Ca2+ sensitization of rabbit smooth muscle. J.Physiol 1997, 500 ( Pt 1):95-109.
Garcia NH, Garvin JL: Angiotensin 1-7 has a biphasic effect on fluid absorption in the proximal straight tubule. J.Am.Soc.Nephrol. 1994, 5:1133-1138.
Gardiner SM, Kemp PA, March JE, Bennett T: Regional haemodynamic effects of angiotensin II (3-8) in conscious rats. Br.J.Pharmacol. 1993, 110:159-162.
Gaynes RP, Szidon JP, Oparil S: In vivo and in vitro conversion of des-1-Asp angiotensin I to angiotensin III. Biochem.Pharmacol. 1978, 27:2871-2877.
Gether U: Uncovering molecular mechanisms involved in activation of G protein- coupled receptors. Endocr.Rev. 2000, 21:90-113.
Giaid A, Yanagisawa M, Langleben D, Michel RP, Levy R, Shennib H, Kimura S, Masaki T, Duguid WP, Stewart DJ: Expression of endothelin-1 in the lungs of patients with pulmonary hypertension. N.Engl.J.Med. 1993, 328(24):1732-1739.
130

Giaid A, Saleh D: Reduced expression of endothelial nitric oxide synthase in the lungs of patients with pulmonary hypertension. N.Engl.J.Med. 1995, 333(4):214-221.
Gironacci MM, Adler-Graschinsky E, Pena C, Enero MA: Effects of angiotensin II and angiotensin-(1-7) on the release of [3H]norepinephrine from rat atria. Hypertension 1994, 24:457-460.
Gohla A, Schultz G, Offermanns S: Role for G(12)/G(13) in agonist-induced vascular smooth muscle cell contraction. Circ.Res. 2000, 87:221-227.
Gomez-Cambronero J, Keire P: Phospholipase D: a novel major player in signal transduction. Cell Signal. 1998, 10:387-397.
Gong MC, Kinter MT, Somlyo AV, Somlyo AP: Arachidonic acid and diacylglycerol release associated with inhibition of myosin light chain dephosphorylation in rabbit smooth muscle. J.Physiol 1995, 486 ( Pt 1):113-122.
Griendling KK, Tsuda T, Berk BC, Alexander RW: Angiotensin II stimulation of vascular smooth muscle. J.Cardiovasc.Pharmacol. 1989, 14 Suppl 6:S27-S33.
Grinstein S, Rotin D, Mason MJ: Na+/H+ exchange and growth factor-induced cytosolic pH changes. Role in cellular proliferation. Biochim.Biophys.Acta 1989, 988:73-97.
Groblewski T, Maigret B, Larguier R, Lombard C, Bonnafous JC, Marie J: Mutation of Asn111 in the third transmembrane domain of the AT1A angiotensin II receptor induces its constitutive activation. J.Biol.Chem. 1997, 272:1822-1826.
Hall KL, Hanesworth JM, Ball AE, Felgenhauer GP, Hosick HL, Harding JW: Identification and characterization of a novel angiotensin binding site in cultured vascular smooth muscle cells that is specific for the hexapeptide (3-8) fragment of angiotensin II, angiotensin IV. Regul.Pept. 1993, 44:225-232.
Handa RK, Ferrario CM, Strandhoy JW: Renal actions of angiotensin-(1-7): in vivo and in vitro studies. Am.J.Physiol 1996, 270:F141-F147.
Handa RK, Krebs LT, Harding JW, Handa SE: Angiotensin IV-AT4 receptor system in the rat kidney. Am.J.Physiol 1998, 274:F290-F299.
Hanesworth JM, Sardinia MF, Krebs LT, Hall KL, Harding JW: Elucidation of a specific binding site for angiotensin II(3-8), angiotensin IV, in mammalian heart membranes. J.Pharmacol.Exp.Ther. 1993, 266:1036-1042.
131

Harder DR, Campbell WB, Roman RJ: Role of cytochrome P-450 enzymes and metabolites of arachidonic acid in the control of vascular tone. J.Vasc.Res. 1995, 32:79-92.
Hartshorne DJ, Ito M, Erdodi F: Myosin light chain phosphatase: subunit composition, interactions and regulation. J.Muscle Res.Cell Motil. 1998, 19:325-341.
Hassid A, Williams C: Vasoconstrictor-evoked prostaglandin synthesis in cultured vascular smooth muscle. Am.J.Physiol 1983, 245:C278-C282.
Hassid A: Increase of cyclic AMP concentrations in cultured vascular smooth muscle cells by vasoactive peptide hormones. Role of endogenous prostaglandins. J.Pharmacol.Exp.Ther. 1986, 239:334-339.
Hazen SL, Stuppy RJ, Gross RW: Purification and characterization of canine myocardial cytosolic phospholipase A2. A calcium-independent phospholipase with absolute f1- 2 regiospecificity for diradyl glycerophospholipids. J.Biol.Chem. 1990, 265:10622-10630.
Hefti MA, Harder BA, Eppenberger HM, Schaub MC: Signaling pathways in cardiac myocyte hypertrophy. J.Mol.Cell Cardiol. 1997, 29:2873-2892.
Hein L, Barsh GS, Pratt RE, Dzau VJ, Kobilka BK: Behavioural and cardiovascular effects of disrupting the angiotensin II type-2 receptor in mice. Nature 1995, 377(6551):744-747.
Hermans E: Biochemical and pharmacological control of the multiplicity of coupling at G-protein-coupled receptors. Pharmacol.&Ther. 2003, 99:25-44.
Hill-Kapturczak N, Kapturczak MH, Block ER, Patel JM, Malinski T, Madsen KM, Tisher CC: Angiotensin II-stimulated nitric oxide release from porcine pulmonary endothelium is mediated by angiotensin IV. J.Am.Soc.Nephrol. 1999, 10:481-491.
Horiuchi M, Hayashida W, Kambe T, Yamada T, Dzau VJ: Angiotensin type 2 receptor dephosphorylates Bcl-2 by activating mitogen-activated protein kinase phosphatase-1 and induces apoptosis. J.Biol.Chem. 1997, 272:19022-19026.
Hunyady L, Vauquelin G, Vanderheyden P: Agonist induction and conformational selection during activation of a G- protein-coupled receptor. Trends Pharmacol.Sci. 2003, 24:81-86.
Ichiki T, Herold CL, Kambayashi Y, Bardhan S, Inagami T: Cloning of the cDNA and the genomic DNA of the mouse angiotensin II type 2 receptor. Biochim.Biophys.Acta. 1994, 1189(2):247-250.
132

Ichiki T, Labosky PA, Shiota C, Okuyama S, Imagawa Y, Fogo A, Niimura F, Ichikawa I, Hogan BL, Inagami T: Effects on blood pressure and exploratory behaviour of mice lacking angiotensin II type-2 receptor. Nature 1995, 377(6551):748-750.
Ishida M, Marrero MB, Schieffer B, Ishida T, Bernstein KE, Berk BC: Angiotensin II activates pp60c-src in vascular smooth muscle cells. Circ.Res. 1995, 77:1053-1059.
Ishida M, Ishida T, Thomas SM, Berk BC: Activation of extracellular signal-regulated kinases (ERK1/2) by angiotensin II is dependent on c-Src in vascular smooth muscle cells. Circ.Res. 1998, 82:7-12.
Itazaki K, Shigeri Y, Fujimoto M: Molecular cloning and characterization of the angiotensin receptor subtype in porcine aortic smooth muscle. Eur.J.Pharmacol. 1993, 245:147-156.
Iwai N, Inagami T: Identification of two subtypes in the rat type I angiotensin II receptor. FEBS Lett. 1992, 298:257-260.
Jackson EK, Herzer WA: Angiotensin II/prostaglandin I2 interactions in spontaneously hypertensive rats. Hypertension 1993, 22:688-698.
Jackson WF, Konig A, Dambacher T, Busse R: Prostacyclin-induced vasodilation in rabbit heart is mediated by ATP- sensitive potassium channels. Am.J.Physiol 1993, 264:H238-H243.
Jaiswal N, Jaiswal RK, Tallant EA, Diz DI, Ferrario CM: Alterations in prostaglandin production in spontaneously hypertensive rat smooth muscle cells. Hypertension 1993, 21:900-905.
Janiak P, Pillon A, Prost JF, Vilaine JP: Role of angiotensin subtype 2 receptor in neointima formation after vascular injury. Hypertension 1992, 20:737-745.
Jasmin JF, Calderone A, Leung TK, Villeneuve L, Dupuis J: Lung structural remodeling and pulmonary hypertension after myocardial infarction: complete reversal with irbesartan. Cardiovas.Res. 2003, 58:621-631.
Kakar SS, Sellers JC, Devor DC, Musgrove LC, Neill JD: Angiotensin II type-1 receptor subtype cDNAs: differential tissue expression and hormonal regulation. Biochem.Biophys.Res.Commun. 1992, 183:1090-1096.
Kakar SS, Riel KK, Neill JD: Differential expression of angiotensin II receptor subtype mRNAs (AT-1A and AT-1B) in the brain. Biochem.Biophys.Res.Commun. 1992, 185:688-692.
Kambayashi Y, Bardhan S, Takahashi K, Tsuzuki S, Inui H, Hamakubo T, Inagami T: Molecular cloning of a novel angiotensin II receptor isoform involved in
133

phosphotyrosine phosphatase inhibition. J.Biol.Chem. 1993, 268(33):24543-24546.
Kenakin T: Agonist-receptor efficacy. II. Agonist trafficking of receptor signals. Trends Pharmacol.Sci. 1995, 16:232-238.
Kenakin T, Onaran O: The ligand paradox between affinity and efficacy: can you be there and not make a difference? Trends Pharmacol.Sci. 2002, 23:275-280.
Kim S, Iwao H: Molecular and cellular mechanisms of angiotensin II-mediated cardiovascular and renal diseases. Pharmacol.Rev. 2000, 52:11-34.
Kimura B, Sumners C, Phillips MI: Changes in skin angiotensin II receptors in rats during wound healing. Biochem.Biophys.Res.Commun. 1992, 187:1083-1090.
Kimura M, Kimura I, Kobayashi S: Relationship between cyclic AMP-dependent protein kinase activation and Ca uptake increase of sarcoplasmic reticulum fraction of hog biliary muscles relaxed by cholecystokinin-C-terminal peptides. Biochem.Pharmacol. 1982, 31:3077-3083.
Kirton CA, Loutzenhiser R: Alterations in basal protein kinase C activity modulate renal afferent arteriolar myogenic reactivity. Am.J.Physiol 1998, 275:H467-H475.
Kitazawa T, Masuo M, Somlyo AP: G protein-mediated inhibition of myosin light-chain phosphatase in vascular smooth muscle. Proc.Natl.Acad.Sci.U.S.A 1991, 88:9307-9310.
Komalavilas P, Lincoln TM: Phosphorylation of the inositol 1,4,5-trisphosphate receptor. Cyclic GMP-dependent protein kinase mediates cAMP and cGMP dependent phosphorylation in the intact rat aorta. J.Biol.Chem. 1996, 271:21933-21938.
Konishi H, Kuroda S, Inada Y, Fujisawa Y: Novel subtype of human angiotensin II type 1 receptor: cDNA cloning and expression. Biochem.Biophys.Res.Commun. 1994, 199:467-474.
Kramar EA, Harding JW, Wright JW: Angiotensin II- and IV-induced changes in cerebral blood flow. Roles of AT1, AT2, and AT4 receptor subtypes. Regul.Pept. 1997, 68:131-138.
Kramar EA, Krishnan R, Harding JW, Wright JW: Role of nitric oxide in angiotensin IV-induced increases in cerebral blood flow. Regul.Pept. 1998, 74:185-192.
Krebs LT, Kramar EA, Hanesworth JM, Sardinia MF, Ball AE, Wright JW, Harding JW: Characterization of the binding properties and physiological
134

action of divalinal-angiotensin IV, a putative AT4 receptor antagonist. Regul.Pept. 1996, 67:123-130.
Kubalak SW, Webb JG: Angiotensin II enhancement of hormone-stimulated cAMP formation in cultured vascular smooth muscle cells. Am.J.Physiol 1993, 264:H86-H96.
Kugler P: Aminopeptidase A is angiotensinase A. II. Biochemical studies on aminopeptidase A and M in rat kidney homogenate. Histochemistry 1982, 74:247-261.
Kuroda S, Konishi H, Okishio M, Fujisawa Y: Novel subtype of human angiotensin II type 1 receptor: analysis of signal transduction mechanism in transfected Chinese hamster ovary cells. Biochem.Biophys.Res.Commun. 1994, 199:475-481.
Lang P, Gesbert F, Delespine-Carmagnat M, Stancou R, Pouchelet M, Bertoglio J: Protein kinase A phosphorylation of RhoA mediates the morphological and functional effects of cyclic AMP in cytotoxic lymphocytes. EMBO J. 1996, 15:510-519.
Lang U, Vallotton MB: Effects of angiotensin II and of phorbol ester on protein kinase C activity and on prostacyclin production in cultured rat aortic smooth- muscle cells. Biochem.J. 1989, 259:477-483.
Lassegue B, Alexander RW, Clark M, Akers M, Griendling KK: Phosphatidylcholine is a major source of phosphatidic acid and diacylglycerol in angiotensin II-stimulated vascular smooth-muscle cells. Biochem.J. 1993, 292 ( Pt 2):509-517.
Laufs U, Liao JK: Targeting Rho in cardiovascular disease. Circ.Res. 2000, 87:526-528.
Le MT, Vanderheyden PM, Szaszak M, Hunyady L, Vauquelin G: Angiotensin IV is a potent agonist for constitutive active human AT1 receptors. Distinct roles of the N-and C-terminal residues of angiotensin II during AT1 receptor activation. J.Biol.Chem. 2002, 277: 23107-23110.
Lee J, Mustafa T, McDowall SG, Mendelsohn FA, Brennan M, Lew RA, Albiston AL, Chai SY: Structure-activity study of LVV-hemorphin-7: angiotensin AT4 receptor ligand and inhibitor of insulin-regulated aminopeptidase. J.Pharmacol.Exp.Ther. 2003, 305:205-211.
Lee MR, Li L, Kitazawa T: Cyclic GMP causes Ca2+ desensitization in vascular smooth muscle by activating the myosin light chain phosphatase. J.Biol.Chem. 1997, 272:5063-5068.
135

Lin LL, Wartmann M, Lin AY, Knopf JL, Seth A, Davis RJ: cPLA2 is phosphorylated and activated by MAP kinase. Cell 1993, 72:269-278.
Lincoln TM, Cornwell TL: Towards an understanding of the mechanism of action of cyclic AMP and cyclic GMP in smooth muscle relaxation. Blood Vessels 1991, 28:129-137.
Lu HK, Fern RJ, Luthin D, Linden J, Liu LP, Cohen CJ, Barrett PQ: Angiotensin II stimulates T-type Ca2+ channel currents via activation of a G protein, Gi. Am.J.Physiol 1996, 271:C1340-C1349.
Machado RD, Santos RA, Andrade SP: Opposing actions of angiotensins on angiogenesis. Life Sci. 2000, 66:67-76.
Magness RR, Rosenfeld CR, Hassan A, Shaul PW: Endothelial vasodilator production by uterine and systemic arteries. I. Effects of ANG II on PGI2 and NO in pregnancy. Am.J.Physiol 1996, 270:H1914-H1923.
Mahon JM, Allen M, Herbert J, Fitzsimons JT: The association of thirst, sodium appetite and vasopressin release with c-fos expression in the forebrain of the rat after intracerebroventricular injection of angiotensin II, angiotensin-(1-7) or carbachol. Neuroscience 1995, 69:199-208.
Marrero MB, Paxton WG, Duff JL, Berk BC, Bernstein KE: Angiotensin II stimulates tyrosine phosphorylation of phospholipase C- gamma 1 in vascular smooth muscle cells. J.Biol.Chem. 1994, 269:10935-10939.
Marrero MB, Schieffer B, Paxton WG, Heerdt L, Berk BC, Delafontaine P, Bernstein KE: Direct stimulation of Jak/STAT pathway by the angiotensin II AT1 receptor. Nature 1995, 375:247-250.
Martin MM, Willardson BM, Burton GF, White CR, McLaughlin JN, Bray SM, Ogilvie JW, Jr., Elton TS: Human angiotensin II type 1 receptor isoforms encoded by messenger RNA splice variants are functionally distinct. Mol.Endocrinol. 2001, 15:281-293.
Mauzy CA, Hwang O, Egloff AM, Wu LH, Chung FZ: Cloning, expression, and characterization of a gene encoding the human angiotensin II type 1A receptor. Biochem.Biophys.Res.Commun. 1992, 186:277-284.
Mayer RJ, Marshall LA: New insights on mammalian phospholipase A2(s); comparison of arachidonoyl-selective and -nonselective enzymes. FASEB J. 1993, 7:339-348.
McDaniel NL, Rembold CM, Richard HM, Murphy RA: Cyclic AMP relaxes swine arterial smooth muscle predominantly by decreasing cell Ca2+ concentration. J.Physiol 1991, 439:147-160.
136

McGiff JC: Prostaglandins, prostacyclin, and thromboxanes. Annu.Rev.Pharmacol.Toxicol. 1981, 21: 479-509.
McMurray HF, Parrott DP, Bowyer DE: A standardised method of culturing aortic explants, suitable for the study of factors affecting the phenotypic modulation, migration and proliferation of aortic smooth muscle cells . Atherosclerosis 1991, 86:227-237.
Meller E, Puza T, Diamond J, Lieu HD, Bohmaker K: Comparative effects of receptor inactivation, 17 beta-estradiol and pertussis toxin on dopaminergic inhibition of prolactin secretion in vitro. J.Pharmacol.Exp.Ther. 1992, 263:462-469.
Min L, Sim MK, Xu XG: Effects of des-aspartate-angiotensin I on angiotensin II-induced incorporation of phenylalanine and thymidine in cultured rat cardiomyocytes and aortic smooth muscle cells. Regul.Pept. 2000, 95:93-97.
Minami M, Kanayama Y, Inariba H, Negoro N, Inoue T, Takeda T: Angiotensin II induced biphasic inositol 1,4,5-triphosphate response in rat vascular smooth muscle cells. Eur.J.Pharmacol. 1991, 208:93-95.
Muthalif MM, Benter IF, Uddin MR, Harper JL, Malik KU: Signal transduction mechanisms involved in angiotensin-(1-7)-stimulated arachidonic acid release and prostanoid synthesis in rabbit aortic smooth muscle cells. J.Pharmacol.Exp.Ther. 1998, 284:388-398.
Nakajima M, Mukoyama M, Pratt RE, Horiuchi M, Dzau VJ: Cloning of cDNA and analysis of the gene for mouse angiotensin II type 2 receptor. Biochem.Biophys.Res.Commun. 1993, 197(2):393-399.
Nakamoto H, Ferrario CM, Fuller SB, Robaczewski DL, Winicov E, Dean RH: Angiotensin-(1-7) and nitric oxide interaction in renovascular hypertension. Hypertension 1995, 25:796-802.
Nasjletti A, Malik KU: Interrelations between prostaglandins and vasoconstrictor hormones: contribution to blood pressure regulation. Fed.Proc. 1982, 41:2394-2399.
Nasjletti A: Arthur C. Corcoran Memorial Lecture. The role of eicosanoids in angiotensin-dependent hypertension. Hypertension 1998, 31:194-200.
Neuss M, Regitz-Zagrosek V, Hildebrandt A, Fleck E: Human cardiac fibroblasts express an angiotensin receptor with unusual binding characteristics which is coupled to cellular proliferation. Biochem.Biophys.Res.Commun. 1994, 204:1334-1339.
137

Nibbering PH, Zomerdijk TP, van Haastert PJ, van Furth R: A competition binding assay for determination of the inositol (1,4,5)- trisphosphate content of human leucocytes. Biochem.Biophys.Res.Commun. 1990, 170:755-762.
Niiro N, Koga Y, Ikebe M: Agonist-induced changes in the phosphorylation of the myosin- binding subunit of myosin light chain phosphatase and CPI17, two regulatory factors of myosin light chain phosphatase, in smooth muscle. Biochem.J. 2003, 369:117-128.
Noda K, Saad Y, Karnik SS: Interaction of Phe8 of angiotensin II with Lys199 and His256 of AT1 receptor in agonist activation. J.Biol.Chem. 1995, 270:28511-28514.
Noda K, Feng YH, Liu XP, Saad Y, Husain A, Karnik SS: The active state of the AT1 angiotensin receptor is generated by angiotensin II induction. Biochemistry 1996, 35:16435-16442.
Oliveira DR, Santos RA, Santos GF, Khosla M, Campagnole-Santos MJ: Changes in the baroreflex control of heart rate produced by central infusion of selective angiotensin antagonists in hypertensive rats. Hypertension 1996, 27:1284-1290.
Oriji GK, Keiser HR: Protein kinase C mediates angiotensin II-induced contractions and the release of endothelin and prostacyclin in rat aortic rings. Prostaglandins Leukot.Essent.Fatty Acids 1997, 57:135-141.
Orlov SN, Tremblay J, Hamet P: cAMP signaling inhibits dihydropyridine-sensitive Ca2+ influx in VSMCs. Hypertension 1999, 27:774-780.
Orte C, Polak JM, Haworth SG, Yacoub MH, Morrell NW: Expression of pulmonary vascular angiotensin-converting enzyme in primary and secondary plexiform pulmonary hypertension. J.Pathol. 2000, 192(3):379-384.
Osei SY, Ahima RS, Minkes RK, Weaver JP, Khosla MC, Kadowitz PJ: Differential responses to angiotensin-(1-7) in the feline mesenteric and hindquarters vascular beds. Eur.J.Pharmacol. 1993, 234:35-42.
Palmer S, Hughes KT, Lee DY, Wakelam MJ: Development of a novel, Ins(1,4,5)P3-specific binding assay. Its use to determine the intracellular concentration of Ins(1,4,5)P3 in unstimulated and vasopressin-stimulated rat hepatocytes. Cell Signal. 1989, 1:147-156.
Palmieri FE, Bausback HH, Ward PE: Metabolism of vasoactive peptides by vascular endothelium and smooth muscle aminopeptidase M. Biochem.Pharmacol. 1989, 38:173-180.
Pantaloni C, Brabet P, Bilanges B, Dumuis A, Houssami S, Spengler D, Bockaert J, Journot L: Alternative splicing in the N-terminal extracellular domain of the pituitary adenylate cyclase-activating polypeptide (PACAP) receptor
138

modulates receptor selectivity and relative potencies of PACAP-27 and PACAP-38 in phospholipase C activation. J.Biol.Chem. 1996, 271:22146-22151.
Park JK, Lee SO, Kim YG, Kim SH, Koh GY, Cho KW: Role of rho-kinase activity in angiotensin II-induced contraction of rabbit clitoral cavernosum smooth muscle. Int.J.Impot.Res. 2002, 14:472-477.
Parmentier JH, Muthalif MM, Nishimoto AT, Malik KU: 20-Hydroxyeicosatetraenoic acid mediates angiotensin ii-induced phospholipase d activation in vascular smooth muscle cells. Hypertension 2001, 37:623-629.
Patel JM, Martens JR, Li YD, Gelband CH, Raizada MK, Block ER: Angiotensin IV receptor-mediated activation of lung endothelial NOS is associated with vasorelaxation. Am.J.Physiol 1998, 275:L1061-L1068.
Picetti R, Saiardi A, Abdel ST, Bozzi Y, Baik JH, Borrelli E: Dopamine D2 receptors in signal transduction and behavior. Crit Rev.Neurobiol. 1997, 11:121-142.
Pierce KL, Regan JW: Prostanoid receptor heterogeneity through alternative mRNA splicing. Life Sci. 1998, 62:1479-1483.
Polte TR, Naftilan AJ, Hanks SK: Focal adhesion kinase is abundant in developing blood vessels and elevation of its phosphotyrosine content in vascular smooth muscle cells is a rapid response to angiotensin II. J.Cell Biochem. 1994, 55:106-119.
Purdy KE, Arendshorst WJ: Iloprost inhibits inositol-1,4,5-trisphosphate-mediated calcium mobilization stimulated by angiotensin II in cultured preglomerular vascular smooth muscle cells. J.Am.Soc.Nephrol. 2001, 12:19-28.
Rao GN, Lassegue B, Alexander RW, Griendling KK: Angiotensin II stimulates phosphorylation of high-molecular-mass cytosolic phospholipase A2 in vascular smooth-muscle cells. Biochem.J. 1994, 299 ( Pt 1):197-201.
Rasmussen H, Takuwa Y, Park S: Protein kinase C in the regulation of smooth muscle contraction. FASEB J. 1987, 1:177-185.
Reaux A, de Mota N, Zini S, Cadel S, Fournie-Zaluski MC, Roques BP, Corvol P, Llorens-Cortes C: PC18, a specific aminopeptidase N inhibitor, induces vasopressin release by increasing the half-life of brain angiotensin III. Neuroendocrinology 1999a, 69:370-376.
Reaux A, Fournie-Zaluski MC, David C, Zini S, Roques BP, Corvol P, Llorens-Cortes C: Aminopeptidase A inhibitors as potential central antihypertensive agents. Proc.Natl.Acad.Sci.U.S.A 1999b, 96:13415-13420.
139

Reaux A, Iturrioz X, Vazeux G, Fournie-Zaluski MC, David C, Roques BP, Corvol P, Llorens-Cortes C: Aminopeptidase A, which generates one of the main effector peptides of the brain renin-angiotensin system, angiotensin III, has a key role in central control of arterial blood pressure. Biochem.Soc.Trans. 2000, 28:435-440.
Reaux A, Fournie-Zaluski MC, Llorens-Cortes C: Angiotensin III: a central regulator of vasopressin release and blood pressure. Trends Endocrinol.Metab 2001, 12:157-162.
Rhee SG, Choi KD: Regulation of inositol phospholipid-specific phospholipase C isozymes. J.Biol.Chem. 1992, 267:12393-12396.
Rowe BP, Dixon B: Angiotensin III depressor action in the conscious rabbit is blocked by losartan but not PD 123319. Hypertension 2000, 35:130-134.
Ruan X, Arendshorst WJ: Role of protein kinase C in angiotensin II-induced renal vasoconstriction in genetically hypertensive rats. Am.J.Physiol 1996, 270:F945-F952.
Ruan X, Arendshorst WJ: Calcium entry and mobilization signaling pathways in ANG II-induced renal vasoconstriction in vivo. Am.J.Physiol 1996, 270:F398-F405.
Ruan X, Chatziantoniou C, Arendshorst WJ: Impaired prostaglandin E(2)/prostaglandin I(2) receptor-G(s) protein interactions in isolated renal resistance arterioles of spontaneously hypertensive rats. Hypertension 1999, 34:1134-1140.
Runo JR, Loyd JE: Primary Pulmonary Hypertension. The Lancet 2003, 361:1533-1544.
Sadoshima J, Izumo S: The heterotrimeric G q protein-coupled angiotensin II receptor activates p21 ras via the tyrosine kinase-Shc-Grb2-Sos pathway in cardiac myocytes. EMBO J. 1996, 15:775-787.
Sadoshima J: Versatility of the angiotensin II type 1 receptor. Circ.Res. 1998, 82:1352-1355.
Sakurada S, Okamoto H, Takuwa N, Sugimoto N, Takuwa Y: Rho activation in excitatory agonist-stimulated vascular smooth muscle. Am.J.Physiol Cell Physiol 2001, 281:C571-C578.
Samama P, Cotecchia S, Costa T, Lefkowitz RJ: A mutation-induced activated state of the beta 2-adrenergic receptor. Extending the ternary complex model. J.Biol.Chem. 1993, 268:4625-4636.
140

Santos RA, Campagnole-Santos MJ, Baracho NC, Fontes MA, Silva LC, Neves LA, Oliveira DR, Caligiorne SM, Rodrigues AR, Gropen JC, .: Characterization of a new angiotensin antagonist selective for angiotensin-(1-7): evidence that the actions of angiotensin-(1-7) are mediated by specific angiotensin receptors. Brain Res.Bull. 1994, 35:293-298.
Sasaki K, Yamano Y, Bardhan S, Iwai N, Murray JJ, Hasegawa M, Matsuda Y, Inagami T: Cloning and expression of a complementary DNA encoding a bovine adrenal angiotensin II type-1 receptor. Nature 1991, 351:230-233.
Sawada N, Itoh H, Yamashita J, Doi K, Inoue M, Masatsugu K, Fukunaga Y, Sakaguchi S, Sone M, Yamahara K, Yurugi T, Nakao K: cGMP-dependent protein kinase phosphorylates and inactivates RhoA. Biochem.Biophys.Res.Commun. 2001, 280:798-805.
Sayeski PP, Ali MS, Harp JB, Marrero MB, Bernstein KE: Phosphorylation of p130Cas by angiotensin II is dependent on c-Src, intracellular Ca2+, and protein kinase C. Circ.Res. 1998, 82:1279-1288.
Schelling P, Fischer H, Ganten D: Angiotensin and cell growth: a link to cardiovascular hypertrophy? J.Hypertens. 1991, 9:3-15.
Schieffer B, Paxton WG, Chai Q, Marrero MB, Bernstein KE: Angiotensin II controls p21ras activity via pp60c-src. J.Biol.Chem. 1996, 271:10329-10333.
Schror K: Prostaglandin-mediated actions of the renin-angiotensin system. Arzneimittelforschung. 1993, 43:236-241.
Schubert R, Serebryakov VN, Engel H, Hopp HH: Iloprost activates KCa channels of vascular smooth muscle cells: role of cAMP-dependent protein kinase. Am.J.Physiol 1996, 271:C1203-C1211.
Schubert R, Serebryakov VN, Mewes H, Hopp HH: Iloprost dilates rat small arteries: role of K(ATP)- and K(Ca)-channel activation by cAMP-dependent protein kinase. Am.J.Physiol 1997, 272:H1147-H1156.
Schuster DP, Crouch EC, Parks WC, Johnson T, Botney MD: Angiotensin converting enzyme expression in primary pulmonary hypertension. Am.J.Respir.Crit.Care.Med. 1996, 154(4 Pt 1):1087-91.
Seko T, Ito M, Kureishi Y, Okamoto R, Moriki N, Onishi K, Isaka N, Hartshorne DJ, Nakano T: Activation of RhoA and inhibition of myosin phosphatase as important components in hypertension in vascular smooth muscle. Circ.Res. 2003, 92:411-418.
Shinoda J, Kozawa O, Suzuki A, Watanabe-Tomita Y, Oiso Y, Uematsu T: Mechanism of angiotensin II-induced arachidonic acid metabolite release in
141

aortic smooth muscle cells: involvement of phospholipase D. Eur.J.Endocrinol. 1997, 136:207-212.
Silfani TN, Freeman EJ: Phosphatidylinositide 3-kinase regulates angiotensin II-induced cytosolic phospholipase A2 activity and growth in vascular smooth muscle cells. Arch.Biochem.Biophys. 2002, 402:84-93.
Sim MK, Manjeet S: Properties of muscarinic receptors mediating second messenger responses in the rabbit aorta. Eur.J.Pharmacol. 1990, 189(6):399-404.
Sim MK: Degradation of angiotensin I in the endothelium and smooth muscle of the rat aorta. Biochem.Pharmacol. 1993, 45:1524-1527.
Sim MK, Qiu XS: Formation of des-Asp-angiotensin I in the hypothalamic extract of normo- and hypertensive rats. Blood Press 1994, 3:260-264.
Sim MK, Choo MH, Qiu XS: Degradation of angiotensin I to [des-Asp1]angiotensin I by a novel aminopeptidase in the rat hypothalamus. Biochem.Pharmacol. 1994, 48:1043-1046.
Sim MK, Radhakrishnan R: Novel central action of des-Asp-angiotensin I. Eur.J.Pharmacol. 1994, 257:R1-R3.
Sim MK, Soh KS: Effects of des-Asp-angiotensin I on the electrically stimulated contraction of the rabbit pulmonary artery. Eur.J.Pharmacol. 1995, 284:215-219.
Sim MK, Chai SK: Subtypes of losartan-sensitive angiotensin receptor in the rabbit pulmonary artery. Br.J.Pharmacol. 1996, 117:1504-1506.
Sim MK, Lim BC: Determination of aminopeptidase X activity in tissues of normo- and hypertensive rats by capillary electrophoresis. J.Chromatogr.B Biomed.Sci.Appl. 1997, 697:259-262.
Sim MK, Min L: Effects of des-Asp-angiotensin I on experimentally-induced cardiac hypertrophy in rats. Int.J.Cardiol. 1998, 63:223-227.
Sim MK, Lim SL: Angiotensin AT1 receptor subtypes in the rabbit pulmonary artery. A ligand binding study. Receptors.Channels 1998, 5:323-329.
Smith WL, Marnett LJ, DeWitt DL: Prostaglandin and thromboxane biosynthesis. Pharmacol.Ther. 1991, 49:153-179.
Smrcka AV, Hepler JR, Brown KO, Sternweis PC: Regulation of polyphosphoinositide-specific phospholipase C activity by purified Gq. Science 1991, 251:804-807.
142

Somlyo AP, Somlyo AV: Signal transduction and regulation in smooth muscle. Nature 1994, 372:231-236.
Somlyo AP, Somlyo AV: Signal transduction by G-proteins, rho-kinase and protein phosphatase to smooth muscle and non-muscle myosin II. J.Physiol 2000, 522 Pt 2:177-185.
Spengler D, Waeber C, Pantaloni C, Holsboer F, Bockaert J, Seeburg PH, Journot L: Differential signal transduction by five splice variants of the PACAP receptor. Nature 1993, 365:170-175.
Strange PG: G-protein coupled receptors: conformations and states. Biochem.Pharmacol. 1999, 58:1081-1088.
Stull JT, Hsu LC, Tansey MG, Kamm KE: Myosin light chain kinase phosphorylation in tracheal smooth muscle. J.Biol.Chem. 1990, 265:16683-16690.
Su B, Martin MM, Beason KB, Miller PJ, Elton TS: The genomic organization and functional analysis of the promoter for the human angiotensin II type 1 receptor. Biochem.Biophys.Res.Commun. 1994, 204:1039-1046.
Surks HK, Mochizuki N, Kasai Y, Georgescu SP, Tang KM, Ito M, Lincoln TM, Mendelsohn ME: Regulation of myosin phosphatase by a specific interaction with cGMP- dependent protein kinase Ialpha. Science 1999, 286:1583-1587.
Swanson GN, Hanesworth JM, Sardinia MF, Coleman JK, Wright JW, Hall KL, Miller-Wing AV, Stobb JW, Cook VI, Harding EC, .: Discovery of a distinct binding site for angiotensin II (3-8), a putative angiotensin IV receptor. Regul.Pept. 1992, 40:409-419.
Tallant EA, Lu X, Weiss RB, Chappell MC, Ferrario CM: Bovine aortic endothelial cells contain an angiotensin-(1-7) receptor. Hypertension 1997, 29:388-393.
Tepel M, Jankowski J, Ruess C, Steinmetz M, van der GM, Zidek W: Activation of Na+, H+ exchanger produces vasoconstriction of renal resistance vessels. Am.J.Hypertens. 1998, 11:1214-1221.
Thomas WG, Qian H, Chang CS, Karnik S: Agonist-induced phosphorylation of the angiotensin II (AT(1A)) receptor requires generation of a conformation that is distinct from the inositol phosphate-signaling state. J.Biol.Chem. 2000, 275:2893-2900.
Thornbury KD, Ward SM, Dalziel HH, Carl A, Westfall DP, Sanders KM: Nitric oxide and nitrosocysteine mimic nonadrenergic, noncholinergic hyperpolarization in canine proximal colon. Am.J.Physiol 1991, 261:G553-G557.
143

Touyz RM, He G, Deng LY, Schiffrin EL: Role of extracellular signal-regulated kinases in angiotensin II- stimulated contraction of smooth muscle cells from human resistance arteries. Circulation 1999, 99:392-399.
Touyz RM, Endemann D, He G, Li JS, Schiffrin EL: Role of AT2 receptors in angiotensin II-stimulated contraction of small mesenteric arteries in young SHR. Hypertension 1999, 33:366-372.
Touyz RM, Schiffrin EL: Signal transduction mechanisms mediating the physiological and pathophysiological actions of angiotensin II in vascular smooth muscle cells. Pharmacol.Rev. 2000, 52:639-672.
Touyz RM, Wu XH, He G, Park JB, Chen X, Vacher J, Rajapurohitam V, Schiffrin EL: Role of c-Src in the regulation of vascular contraction and Ca2+ signaling by angiotensin II in human vascular smooth muscle cells. J.Hypertens. 2001, 19:441-449.
Treisman R: Regulation of transcription by MAP kinase cascades. Curr.Opin.Cell Biol. 1996, 8:205-215.
Tsuzuki S, Ichiki T, Nakakubo H, Kitami Y, Guo DF, Shirai H, Inagami T: Molecular cloning and expression of the gene encoding human angiotensin II type 2 receptor. Biochem.Biophys.Res.Commun. 1994, 200(3):1449-1454.
Turcato S, Clapp LH: Effects of the adenylyl cyclase inhibitor SQ22536 on iloprost-induced vasorelaxation and cyclic AMP elevation in isolated guinea-pig aorta. Br.J.Pharmacol. 1999, 126:845-847.
Turner CE, Pietras KM, Taylor DS, Molloy CJ: Angiotensin II stimulation of rapid paxillin tyrosine phosphorylation correlates with the formation of focal adhesions in rat aortic smooth muscle cells. J.Cell Sci. 1995, 108 ( Pt 1):333-342.
Ushio-Fukai M, Griendling KK, Akers M, Lyons PR, Alexander RW: Temporal dispersion of activation of phospholipase C-beta1 and -gamma isoforms by angiotensin II in vascular smooth muscle cells. Role of alphaq/11, alpha12, and beta gamma G protein subunits. J.Biol.Chem. 1998, 273:19772-19777.
Ushio-Fukai M, Alexander RW, Akers M, Lyons PR, Lassegue B, Griendling KK: Angiotensin II receptor coupling to phospholipase D is mediated by the betagamma subunits of heterotrimeric G proteins in vascular smooth muscle cells. Mol.Pharmacol. 1999, 55:142-149.
Vallon V, Richter K, Heyne N, Osswald H: Effect of intratubular application of angiotensin 1-7 on nephron function. Kidney Blood Press Res. 1997, 20:233-239.
144

Vallon V, Heyne N, Richter K, Khosla MC, Fechter K: [7-D-ALA]-angiotensin 1-7 blocks renal actions of angiotensin 1-7 in the anesthetized rat. J.Cardiovasc.Pharmacol. 1998, 32:164-167.
Viswanathan M, Saavedra JM: Expression of angiotensin II AT2 receptors in the rat skin during experimental wound healing. Peptides 1992, 13:783-786.
Viswanathan M, Seltzer A, Saavedra JM: Heterogeneous expression of angiotensin II AT1 receptors in neointima of rat carotid artery and aorta after balloon catheter injury. Peptides 1994, 15:1205-1212.
Walsh MP, Horowitz A, Clement-Chomienne O, Andrea JE, Allen BG, Morgan KG: Protein kinase C mediation of Ca(2+)-independent contractions of vascular smooth muscle. Biochem.Cell Biol. 1996, 74:485-502.
Webb RC: Angiotensin II-induced relaxation of vascular smooth muscle. Blood Vessels 1982, 19:165-176.
Welches WR, Santos RA, Chappell MC, Brosnihan KB, Greene LJ, Ferrario CM: Evidence that prolyl endopeptidase participates in the processing of brain angiotensin. J.Hypertens. 1991, 9:631-638.
Widdop RE, Sampey DB, Jarrott B: Cardiovascular effects of angiotensin-(1-7) in conscious spontaneously hypertensive rats. Hypertension 1999, 34:964-968.
Wilcox CS, Lin L: Vasoconstrictor prostaglandins and angiotensin-dependent renovascular hypertension. J. Nephrol. 1993, 6:124-133.
Wise H, Jones RL: Focus on prostacyclin and its novel mimetics. Trends Pharmacol.Sci. 1996, 17:17-21.
Wojcikiewicz RJ, Tobin AB, Nahorski SR: Desensitization of cell signalling mediated by phosphoinositidase C. Trends Pharmacol.Sci. 1993, 14:279-285.
Wright JW, Harding JW: Brain angiotensin receptor subtypes in the control of physiological and behavioral responses. Neurosci.Biobehav.Rev. 1994, 18:21-53.
Wright JW, Krebs LT, Stobb JW, Harding JW: The angiotensin IV system: functional implications. Front Neuroendocrinol. 1995, 16:23-52.
Wright JW, Bechtholt AJ, Chambers SL, Harding JW: Angiotensin III and IV activation of the brain AT1 receptor subtype in cardiovascular function. Peptides 1996, 17:1365-1371.
Yamada K, Iyer SN, Chappell MC, Ganten D, Ferrario CM: Converting enzyme determines plasma clearance of angiotensin-(1-7). Hypertension 1998, 32:496-502.
145

Yamamoto K, Chappell MC, Brosnihan KB, Ferrario CM: In vivo metabolism of angiotensin I by neutral endopeptidase (EC 3.4.24.11) in spontaneously hypertensive rats. Hypertension 1992, 19:692-696.
Ye M, Flores G, Batlle D: Angiotensin II and angiotensin-(1-7) effects on free cytosolic sodium, intracellular pH, and the Na(+)-H+ antiporter in vascular smooth muscle. Hypertension 1996, 27:72-78.
Yoshida H, Kakuchi J, Guo DF, Furuta H, Iwai N, van der Meer-de Jong, Inagami T, Ichikawa I: Analysis of the evolution of angiotensin II type 1 receptor gene in mammals (mouse, rat, bovine and human). Biochem.Biophys.Res.Commun. 1992, 186:1042-1049.
Zhang BX, Muallem S: Feedback inhibition of Ca2+ release by Ca2+ is the underlying mechanism of agonist-evoked intracellular Ca2+ oscillations in pancreatic acinar cells. J.Biol.Chem. 1992, 267:24387-24393.
Zhuo J, Moeller I, Jenkins T, Chai SY, Allen AM, Ohishi M, Mendelsohn FA: Mapping tissue angiotensin-converting enzyme and angiotensin AT1, AT2 and AT4 receptors. J.Hypertens. 1998, 16:2027-2037.
Zini S, Fournie-Zaluski MC, Chauvel E, Roques BP, Corvol P, Llorens-Cortes C: Identification of metabolic pathways of brain angiotensin II and III using specific aminopeptidase inhibitors: predominant role of angiotensin III in the control of vasopressin release. Proc.Natl.Acad.Sci.U.S.A 1996, 93:11968-119
146