-
European Journal of Radiology 82 (2013) 1633 1637
Contents lists available at ScienceDirect
European Journal of Radiology
jo ur nal ho me page: www.elsev ier .co
Endovascular treatment of aneurisms: Pre, intra amanagement
S. Bracar ,1
a Universit de b INSERM U 94c Department od Department o pital
C
a r t i c l
Article history:Received 29 NReceived in reAccepted 7 Feb
Keywords:Cerebral aneurEndovascular
ComplicationsAnticoagulatioAntiplatelet thThrombo-embolism
lar afocusmorr
eitherd ra
h clin
1. Introduction
There isliterature cendovasculcussion to amedicationno
recomm
Several mment to excRisks vary within whicthus be tail
Among intra and pthromboemThus adjuvaand treatin
Corresponradiology, BatiFrance. Tel.: +3
E-mail add(C. Barbier), al(R. Anxionnat)
1 DepartmeLepoire. Hopit
of subarachnoid hemorrhage (SAH) and treatments to avoid
0720-048X/$ http://dx.doi.o no identiable consensus across teams
or in theoncerning the pharmacological accompaniment ofar aneurysm
treatment. We will limit the present dis-
review of the principles and rationale of the use of theses; any
discussion of protocols is strictly illustrative withendatory
intent.ethods are available in endovascular aneurysm treat-
lude the affected vascular section from the
circulation.according to the treatment option and the conditionsh
the surgery is performed. Associated treatments mustored on a
case-by-case basis.the most frequent risks of endovascular repair
areostoperative hemorrhagic rupture, a rare event, andbolic
complications, which are much more frequent.nt pharmaceuticals are
largely focused on preventingg these latter. Additionally
symptomatic treatment
ding author at: Department of Diagnostic and Interventional
Neuro-ment Jean Lepoire. Hopital Central, CHU Nancy, 54035 Nancy
cedex,33 83851773.resses: [email protected] (S. Bracard),
[email protected]@chu-nancy.fr (A.L. Derelle),
[email protected] of Diagnostic and Interventional
Neuroradiology, Batiment Jeanal Central, CHU Nancy, 54035 Nancy
cedex, France.
vasospasm will enter into play in cases of ruptured
aneurisms.
2. Thromboembolic complications
The most frequent risk in endovascular aneurysm treatmentis
thromboembolic complications. Their analysis in the
literaturevaries according to how they are considered: only
symptomaticcomplications, intraoperative occlusions, probable
ischemic abnor-malities on systematic postoperative MRIs, etc.
Thromboemboliccomplications have become less frequent and the
management oftheir consequences has improved. Nonetheless, they
remain themain risk in endovascular approaches.
The frequency of intraoperative thromboembolic complicationsin
multicenter series can vary, ranging for example from 7% inthe
ATENA study (considering only non-ruptured aneurisms) [1]to 12.5%
in the CLARITY study [2]; morbidity and mortality was3.8% in this
latter.
The inuence of employed techniques varies across assess-ments.
Sluzewski et al. [3,4] found that remodeling resulted inlarger
risks but this tendency was not detected in Altay et al.s
metaanalysis [5] and Pierot et als recent review of the literature
[6]. Theuse of stents increased the risk of stroke per operative
and in therst 48 h by 10% [710].
The size of the aneurysm and its neck are risk factors,
withthromboembolic events being more frequent in large and
giant
see front matter 2013 Elsevier Ireland Ltd. All rights
reserved.rg/10.1016/j.ejrad.2013.02.012da,b,c,, C. Barbierd, A.L.
Derelled, R. Anxionnata,b,c
Lorraine, France7, Francef Diagnostic and Interventional
Neuroradiology. CHU Nancy cedex, Francef Diagnostic and
Interventional Neuroradiology. CHU Nancy, Batiment Jean Lepoire.
Ho
e i n f o
ovember 2012vised form 5 February 2013ruary 2013
ismstreatment
nerapy
a b s t r a c t
The most frequent risk in endovascuadjuvant pharmaceuticals are
largely tomatic treatment of subarachnoid heplay in cases of
ruptured aneurisms.
Consensus exists in the literature nto be administered. The
principles andiscussion of protocols according witm/locate /e j
rad
nd post operative
entral, CHU Nancy, 54035 Nancy cedex, France
neurysm treatment is thromboembolic complications. Thused on
preventing and treating these latter. Additionally symp-hage (SAH)
and treatments to avoid vasospasm will enter into
for the necessity of heparin or antiplatelets nor for the
dosestionale of the use of these medications are reviewed with
aical situations and technical choices.
2013 Elsevier Ireland Ltd. All rights reserved.
-
1634 S. Bracard et al. / European Journal of Radiology 82 (2013)
1633 1637
aneurysms. In the Clarity study [2], risks were 28% for
aneurysmsover 10 mm vs. 10.7% for those under 10 mm.
Finally, an increased frequency of thromboembolic events
isassociated with SAH [2,5].
The intantiplateletof thrombo
3. Interest
Consensof heparin recommendintravascul
In publisgenerally lereported. Mboluses rancontinuousbetween
20boembolic risks in theor extracran
Protocoland often ccontrols.
The Wororadiologythe results ding teams in a continuthen 1000
U
There arthe eld of ithe endova
Heparinare not accemonitoringmonly betwof the hepa
Loading weight to rinterventio80 U/kg areor
cardiolomaintaineding to reguadaptation bosis treatmAfter a bo18
U/kg/h agram.
Preoperabefore the advantage aneurism rdose in the
At the enmally stoppinfusion forarin (LMWHbe falling
oanticoagula
Any rationo convincilogical pers
However, LMWH is relevant for the prevention of deep
veinthrombosis (DVT). DVT risks are elevated after a SAH (18% in
theRay et al. study) and vary according to the severity of bleeding
andthe duration of hospitalization [16]. This rate justies the use
of
at pity r
iplat
reat charassocationt andons.
inte ofteenterantipent, ed rativeliograceiv(1.6%iplatn), cl
antip
e rol
actious ftimulatelgen aationiplat
of tboxaagreatidetudi
pirin
irin ambo
path 40ect ise n
caseomotmennt. Homp
onlo clicts atelet
opido
owingrelra and postoperative use of anticoagulants ands has been
proposed to reduce the frequency and gravityembolic
complications.
and use of heparin
us exists in the literature neither for the necessitynor for the
quantities to be administered. Heparin ised during interventions
due to the use of multiplear tools in procedures that can last
several hours.hed multicenter studies, the use of anticoagulants
wasft to the judgment of the investigators and thus notajor
monocenter studies [1113] have reported initialging from 3000 to
5000 IU followed by 2040 IU/kg/hly to maintain a monitored
activated clotting time (ACT)0 and 300 s. This tactic is a
compromise between throm-and hemorrhagic risks, noting that
thromboembolicse procedures are lesser than those found in
stentingial angioplasty.s found in the literature or proposed by
institutions varyomprise a standardized loading dose and no
specied
rld Federation of Interventional and Therapeutic Neu- (WFITN)
surveyed its members in 2006 and publishedand its recommendations
on its website. Most respon-reported the use of intraoperative
heparin but only 69%ous infusion. The WFITN recommends a 5000 U
bolus,/h continuously, with (monitored) ACT at about 200 s.e a
number of recommendations for heparin use outsidenterventional
neuroradiology that may be adaptable toscular treatment of
aneurisms [14].
use must be monitored. Blood heparin concentrationsssible during
our interventions. The normally employed
method is ACT, with guideline values >200 s, most com-een 250
and 300 s. It is recommended to test the efcacyrin regularly during
the intervention.and continuous doses must be adapted to the
patientsapidly attain and maintain ACT objectives during then,
which may take several hours. Doses from 70 to
proposed in heparin use protocols in intensive caregy to obtain
efcacious anticoagulation. This is then
via infusion, with doses adjusted as needed accord-lar (at least
hourly) ACT monitoring. A practical dosetable is frequently used to
manage heparin in throm-ent and can be adapted for use in aneurisms
[15].
lus injection of 70 U/kg, we used to continue withnd adjust
according to ACT level and this kind of nomo-
tive oral anticoagulants are usually stopped 5 daysintervention
and replaced by heparin, which has theof being easily antagonized
in cases of intraoperativeupture. Administration of protamine
sulfate dose forlast hour will rapidly terminate heparinization.d
of aneurism treatment, heparin administration is nor-ed but not
antagonized. Some teams continue heparin
2448 h. Follow-up with low molecular weight hep-) has been
advised by certain teams, but this seems to
ut of favor. The WFITN does not recommend pursuingtion
postoperatively.nale for postoperative use of heparin is unclear.
Indeed,ng clinical results have been published, and from a
bio-pective it seems more pertinent to use antiplatelets.
LMWHmorbid
4. Ant
To tspace ity of aaggregprevenplicati
Theevokedmulticing 3 treatmreportrespecof angwho redidnt
Ant(aspirinewer
4.1. Th
Theof varimore sfrom pbrinoaggreg
Antreleasethromand ticeptibbeing s
4.2. As
Aspof throCOX-1matelyThe effafter th50% oflacks hto
treafrequebolic cdosagewith ntic effeantipla
4.3. Cl
Follclopidoreventative doses, especially as these latter present
littleisk [17].
elets
an aneurism, a foreign body is placed within a vascularcterized
by high-velocity blood ow and the possibil-iated intimal insults.
These conditions activate platelet
mechanisms and thus justify the use of antiplatelets to treat
intra and post-procedure thromboembolic com-
rest of the preventative use of antiplatelets has beenn, but has
not yet been subjected to randomized or large,
studies to assess specic protocols. In a study involv-latelet
protocols: no treatment, only post-procedurepre and post-procedure
treatment, Yamada et al. [18]tes of symptomatic thromboembolic
complications ofy 16%, 2.3% and 1.9%. They also reported a reduced
ratephically visible clots during the procedure in patientsed
pre-procedure antiplatelets compared to those who
and 4.5% respectively).elets employable in practice are
acetylsalicylic acidopidogrel, and more rarely urbiprofen, as well
as thelatelets prasugrel and ticagrelor.
e of platelets in thrombus formation
vation of platelets induces the formation and liberationactors
including ADP and thromboxane A2, and further-lates the formation
of thrombin. This reaction spreadset to platelet and a linking
process begins involvingnd surface glycoprotein receptors,
resulting in platelet.elet drugs are designed to inhibit the
production andhese different factors: acetylsalicylic acid is the
mainne inhibitor; clopidogrel and the newer drugs prasugrellor
inhibit ADP receptors; and Abciximab, tiroban and
are glycoprotein IIb/IIIa inhibitors. Other molecules areed.
cts by inhibiting prostaglandin H synthase, a precursorxane A2,
thus provoking a prolonged inhibition of theway. Aspirins
antiplatelet activity will appear approxi-60 min after the
administration of a dose of 75100 mg.
irreversible. Normal platelet activity will return 7 daysal
dose. Resistance to acetylsalicylic acid in as much ass has been
suggested, but the data behind this numbergeneity, and comprises in
particular poor compliancet; truly insufcient response to aspirin
is much lessowever, when it does occur, the risk of
thromboem-lications is greatly augmented and increasing aspiriny
increases the risk of aspirin-related complicationsnical benets.
Aspirin and clopidogrel have synergis-nd thus their association
generally results in efcacious
activity [19].
grel
g a loading dose of 300 mg, the antiplatelet effect of is
observable after 2 h and remains stable for 48 h. As
-
S. Bracard et al. / European Journal of Radiology 82 (2013) 1633
1637 1635
for aspirin, normal platelet activity resumes 7 days after the
naldose. Effects are obtained within 48 h with doses of 75 mg per
day,but the objective of 50% inhibition is obtained only after 47
daysof treatment.
Studies iresulted in to a 300 mgperiprocedu
Insufcicases. The ffactors maythe treatmequantity ofand
obesityhyper reactreduced bypatients. Th[22], whichand proton
Insufcirisks of throantiplateletare routinelpidogrel, an
The objealso be expVASP assayresponders
If initial may be condoubling ofies have sufrom 75 to 1
If neitheseveral new
4.4. New an
Prasugrediology whoptimizatioinhibition cprises a 60prodrug.
Itsdrug takes attained in conrmed athe expense
Ticagrelopeak occursimen of 90PLATO studpidogrel in expense
of
Unlike tprasugrel, trhagic compplatelets re
5. GPIIb/IIIeptibatide
GPIIb/IIIinvolved instrong anti
tiroban, and greater than 10 h for Abciximab. Reversibility
isaverage to poor, necessitating the emergency use of
concentratedplatelets in cases of hemorrhagic complications.
Furthermore, aplatelet count in urgent conditions is necessary to
rule out acute
bocyre uural mab ol cosion
sche
ptur
uch bal
use ural t befo
use is re
stop patieolecu
e anysmsmenion vpasmle fortoma
ome seveting telets ear
tecgrelstentards,eurisnes se is
rupt
For si use is re
stoptopeeckeFITent d
Coilinally, t
mg/ess idistereiplatgreln cardiology demonstrated that a 600 mg
loading dosea more intense and rapid antiplatelet effect
compared
loading dose (ISAR CHOICE [20]), and a reduction inral
thromboembolic complications (ARMYDA-2 [21]).ent response to
clopidogrel is observed in 5 to 11% ofactors resulting in this
resistance are multiple. Genetic
result in faulty platelet receptors or in dysfunction ofnts
metabolizing enzymes resulting in an insufcient
the active metabolite. Patient factors such as diabetes may play
a role as may platelet-specic factors such asivity or increased
turn-over. Clopidogrel efcacy is also
some medications commonly used in cardiovascularis includes
statins, such as atorvastatin or simvastatin
decrease clopidogrel efcacy as their dosage increases,pump
inhibitors such as omeprazole.ent antiplatelet activity is
associated with increasedmboembolic events; thus, pre-operative
evaluation of
response is recommended. Two platelet inhibition testsy used:
the ow cytometric VASP assay, specic to clo-d the Verify Now P2Y12
assay [23].ctive is a >40% inhibition of platelet function; this
mayressed as a residual platelet reactivity of
-
1636 S. Bracard et al. / European Journal of Radiology 82 (2013)
1633 1637
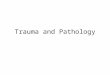
Fig. 1. Ruptured ICA aneurism before (A) and after coiling (B)
with a platelet aggregation on the surface of coils (arrow).
Complete disappearance 20 min after a standarddose of abciximab
(C).
days before the intervention; less ideally: an additional
loadingdose may be proposed. Efcacy is then reveried. If
insufcientresponse persists, in place of clopidogrel, ideally: 10
mg/day of pra-sugrel should be administered for 4 days prior to the
intervention;less ideally: a 60 mg loading dose of prasugrel should
be adminis-tered at least 1 h before the intervention.
The use of heparin intraoperatively according to habitual
pro-tocols is recommended. After the intervention, heparin
infusionsmay be stopped but they should not be antagonized.
Postoperatively: aspirin 75 mg/day and clopidogrel 75 mg/dayare
continued for 6 weeks to 3 months, then 75 mg/day of aspirinfor the
patients lifetime.
6.3. Flow diverters
Flow diverting stents are made of tightly-spaced mesh and
thuspresent a large metallic surface to blood, resulting in a
greaterlikelihood of intra-stent thrombosis or acute thrombosis in
theaneurysm sac with a risk of rupture [27].
Preparation is the same as with other stents, but
postopera-tively a two-drug antiplatelet regimen is usually
maintained for612 months and then replaced by clopidogrel.
7. Management of intraoperative thromboemboliccomplications
The management of intraoperative thromboembolic eventsdemands
the constant verication and correction of thepatients biological
and clinical parameters, arterial pres-sure and the degree of
anticoagulation if needed. ACT mustbe greater than 250 s. If this
is not the case a 2000 IU bolusis indicated. IV nimodipine should
be started (10 ml/h) andintra-arterial nimodipine or papaverine
considered (Figs. 1and 2).
Fibrinolytics such as rTpa are rarely employed. GPIIb/IIIa
recep-tor antagonists (Abciximab, tiroban and eptibatide) are
widelyused and re-establish patency in approximately 80% of
cases[28,29].
Fig. 2. Right abranches is deof the distal brzygo ACA aneurism
on AP and oblique view before (9h45) and immediately at the end of
creased (10h28) with a worsening on 10h34 control angio. Standard
bolus injection of abanches on the late control angiogram.treatment
(10h23). On nal AP control angiogram, the lling of distalciximab at
10h35 with progressive improvement and a normal lling
-
S. Bracard et al. / European Journal of Radiology 82 (2013) 1633
1637 1637
When clots are accessible in a proximal artery, a
thrombectomymay also be considered as part of the approach.
Conict of interest
The authors conrm they have no conicts of interest.
References
[1] Pierot L, et al. Endovascular treatment of unruptured
intracranial aneurysms:comparison of safety of remodeling technique
and standard treatment withcoils. Radiology 2009;251(3):84655.
[2] Pierot L, et al. Ruptured intracranial aneurysms: factors
affecting the rate andoutcome of endovascular treatment
complications in a series of 782 patients(CLARITY study). Radiology
2010;256(3):91623.
[3] Sluzewski M, et al. Rupture of intracranial aneurysms during
treatment withGuglielmi detachable coils: incidence, outcome, and
risk factors. Journal ofNeurosurgery 2001;94(2):23840.
[4] van Rooij WJ, et al. Procedural complications of coiling of
ruptured intracranialaneurysms: incidence and risk factors in a
consecutive series of 681 patients.American Journal of
Neuroradiology 2006;27(7):1498501.
[5] Altay T, et al. Thromboembolic events associated with
endovasculartreatment of cerebral aneurysms. Journal of
Neurointerventional Surgery2011;3(2):14750.
[6] Pierot L, et al. Safety and efcacy of balloon remodeling
technique duringendovascular treatment of intracranial aneurysms:
critical review of the lit-erature. American Journal of
Neuroradiology 2012;33(1):125.
[7] Shapiro M, et al. Stent-supported aneurysm coiling: a
literature survey of treat-ment and follow-up. American Journal of
Neuroradiology 2012;33(1):15963.
[8] Golshani K, et al. Stent-assisted coil emboilization of
ruptured intracranialaneurysms: A retrospective multicenter review.
Surgical Neurology Interna-tional 2012;3:p84.
[9] Lodi YM, et al. Stent assisted coiling of the ruptured wide
necked intracranialaneurysm. Journal of Neurointerventional Surgery
2012;4(4):2816.
[10] Bodily KD, et al. Stent-assisted coiling in acutely
ruptured intracranialaneurysms: a qualitative, systematic review of
the literature. American Journalof Neuroradiology
2011;32(7):12326.
[11] Park HK, et al. Periprocedural morbidity and mortality
associated with endovas-cular trea2005;26(
[12] Qureshi Acomplicalogical an
[13] Hussein ulation mNeurorad
[14] Hirsh J, healthcar2001;103
[15] Raschke R, Reilly B. Monitoring heparin therapy. Annals of
Internal Medicine1994;120:16970.
[16] Ray WZ, et al. incidence of deep venous thrombosis after
subarachnoid hem-orrhage. Journal of Neurosurgery
2009;110:10104.
[17] Vance AZ, et al. Safety of intravenous heparin
administration after endovasculartreatment for ruptured
intracranial aneurysms. Journal of NeurointerventionalSurgery
2009;1(2):13641.
[18] Yamada NK, et al. Effect of antiplatelet therapy on
thromboembolic complic-tions of elective coil embolization of
cerebral aneurisms. American Journal ofNeuroradiology
2007;28:177882.
[19] Fox KA, et al. Benets and risks of the combination of
clopidogreland aspirin in patients undergoing surgical
revascularization for non-ST-elevation acute coronary syndrome: the
Clopidogrel in Unstable angina toprevent Recurrent icchemic Event
(CURE) trial. Circulation 2004;110(10):12028.
[20] von Beckerath N, et al. Absorption, metabolization, and
antiplatelet effectsof 300-, 600-, and 900-mg loading doses of
clopidogrel: results of theISAR-CHOICE (Intracoronary Stenting and
Antithrombotic Regimen: Choosebetween 3 High Oral doses for
Immediate Clopidogrel Effect) Trial.
Circulation2005;112(19):294650.
[21] Patti G, et al. Outcome comparison of 600- and 300-mg
loading doses of clo-pidogrel in patients undergoing primary
percutaneous coronary interventionfor ST-segment elevation
myocardial infarction: results from the ARMYDA-6 MI(Antiplatelet
therapy for Reduction of MYocardial Damage during
Angioplasty-Myocardial Infarction) randomized study. Journal of the
American College ofCardiology 2011;58(15):15929.
[22] Lau WC, et al. Atorvastatin reduces the ability of
clopidogrel to inhibit plateletaggregation: a new drug-drug
interaction. Circulation 2003;107:327.
[23] van Werkum JW, et al. A head-to-head comparison between the
Veri-fyNow P2Y12 assay and light transmittance aggregometry for
monitoring theindividual platelet response to clopidogrel in
patients undergoing electivepercutaneous coronary intervention.
Journal of Thrombosis and Haemostasis2006;4(11):25168.
[24] Wiviott SD, et al. Prasugrel versus clopidogrel in patients
with acute coronarysyndromes. New England Journal of Medicine
2007;357(20):200115.
[25] Wallentin WL, et al. Ticagrelor versus clopidogrel in
patients with acute coro-nary syndromes. New England Journal of
Medicine 2009;361:104557.
[26] Turmialan LM, et al. Intracranial hemorrhage associated
with stent-assistedcoil embolization of cerebral aneurysms: a
cautionary report. Journal of Neu-rosurgery 2008;108:11229.
csar Z, et al. Intra-aneurysmal thrombosis as a possible cause
of delayedurysmiologys T, etplica
cases eningturedcoprot6;27:tment of intracranial aneurysms.
American Journal of Neuroradiology3):50614.I, et al. Prevention and
treatment of thromboembolic and ischemictions associated with
endovascular procedures: Part I pathophysio-d pharmacological
features. Neurosurgery 2000;46(6):134459.HM, Georgiadis AL, Qureshi
AI. Point-of-care testing for anticoag-onitoring in
neuroendovascular procedures. American Journal ofiology
2012;33(7):121120.et al. Guide to anticoagulant therapy: Heparin: a
statement fore professionals from the American Heart Association.
Circulation(24):29943018.
[27] Kulanerad
[28] Riecom42
[29] Brurupgly200 rupture after ow-diversion treatment. American
Journal of Neuro- 2011;32(1):205.
al. Abciximab is a safe rescue yherapy in thromboembolic
eventsting cerebral aneurysm coil embolization: single center
experience inand review of the literature. Stroke
2009;40:17507.
R, et al. Intraprocedural thrombus formation during coil
placementin intracranial aneurysms: treatment with systemic
application of theein IIb/IIIa antagonist tiroban. American Journal
of Neuroradiology132631.
Endovascular treatment of aneurisms: Pre, intra and post
operative management1 Introduction2 Thromboembolic complications3
Interest and use of heparin4 Antiplatelets4.1 The role of platelets
in thrombus formation4.2 Aspirin4.3 Clopidogrel4.4 New antiplatelet
drugs
5 GPIIb/IIIa receptor antagonists (Abciximab, tirofiban and
eptifibatide)6 Use schemas6.1 Ruptured aneurisms6.2 Unruptured
aneurisms6.2.1 For simple coiling and possible remodeling6.2.2
Coiling and stenting
6.3 Flow diverters
7 Management of intraoperative thromboembolic
complicationsConflict of interestReferences