Embed Size (px)
Citation preview

11
ANESTHETIC
MANAGEMENT OF THE
PATIENT WITH VALVULAR
HEART DISEASE
ANESTHETIC
MANAGEMENT OF THE
PATIENT WITH VALVULAR
HEART DISEASE
Peggy Contrera, MSN, CRNAPeggy Contrera, MSN, CRNA
CWRU/CC School of Nurse AnesthesiaCWRU/CC School of Nurse Anesthesia
Department of Cardiothoracic AnesthesiaDepartment of Cardiothoracic Anesthesia
Cleveland Clinic Health SystemCleveland Clinic Health System 22
Physiology
In Action!!!
Physiology
In Action!!!
33
Anesthetic Management of
Valvular Heart Disease
Anesthetic Management of
Valvular Heart Disease
�� Abnormal pressure and volume loadsAbnormal pressure and volume loads
�� Structural and functional mechanisms Structural and functional mechanisms
of compensationof compensation
�� Events that signal the limits of Events that signal the limits of
compensation (dysrhythmias, CHF)compensation (dysrhythmias, CHF)
�� Secondary complications (endocarditis Secondary complications (endocarditis
or emboli)or emboli)
44
Factors affecting blood flow
across the valve
Factors affecting blood flow
across the valve
1.1. Valve Area Valve Area �� Stenotic lesions Stenotic lesions �� ffixed ixed
�� Regurgitant lesions Regurgitant lesions �� vvariable based on loading conditions ariable based on loading conditions (preload and afterload)(preload and afterload)
2.2. Square root of the hydrostatic pressure gradient Square root of the hydrostatic pressure gradient across the valveacross the valve
3.3. Duration of flow whether systole or diastoleDuration of flow whether systole or diastole
GoalsGoals�� Stenotic lesions Stenotic lesions �� maximize or enhance transvalvular flowmaximize or enhance transvalvular flow
�� Regurgitant lesions Regurgitant lesions �� minimize regurgitant transvalvular minimize regurgitant transvalvular flowflow
55
Ventricular FunctionVentricular Function
Systolic FunctionSystolic Function
�� Ability to contract and generate a force against an afterload Ability to contract and generate a force against an afterload
�� Directly related to contractility which is Directly related to contractility which is independentindependent of of changes in preload and afterloadchanges in preload and afterload
�� Cardiac output however, does change based on preload and Cardiac output however, does change based on preload and afterloadafterload
�� ESV/ESPESV/ESP
Diastolic FunctionDiastolic Function
�� Ability to relax and accept preload Ability to relax and accept preload
�� EDP/EDVEDP/EDV
�� Directly related to complianceDirectly related to compliance
Both systolic and diastolic function require energy and can be Both systolic and diastolic function require energy and can be compromised by ischemia!compromised by ischemia!
66
Ventricular HypertrophyVentricular Hypertrophy

77
Ventricular HypertrophyVentricular Hypertrophy
Concentric Hypertrophy:Concentric Hypertrophy:
�� Occurs with pressure Occurs with pressure overload overload
�� Parallel replication of Parallel replication of sarcomeres sarcomeres
�� ↑↑ wall thickness (volume wall thickness (volume constant)constant)
�� Wall tension = P x R/2h. Wall tension = P x R/2h. Laplace's Law Laplace's Law
Eccentric HypertrophyEccentric Hypertrophy
�� Occurs with volume Occurs with volume overload overload
�� Results in an Results in an ↑↑ chamber chamber size (heart dilates)size (heart dilates)
88
The Cardiac Cycle and
The Pressure -Volume Loop
The Cardiac Cycle and
The Pressure -Volume Loop
Phase 1Phase 1: Diastolic Filling : Diastolic Filling
Phase 2Phase 2: Isovolumetric : Isovolumetric ContractionContraction
Phase 3Phase 3: Systolic Ejection: Systolic Ejection
Phase 4Phase 4: Isovolumetric : Isovolumetric RelaxationRelaxation
��Systole C Systole C →→ F (phases 2 & 3)F (phases 2 & 3)
��Diastole F Diastole F →→ C (phases 1 & 4)C (phases 1 & 4)�� ESVESV
�� EDVEDV
�� SVSV
99
Pressure -Volume
Relationships
Pressure -Volume
Relationships
��PreloadPreload
��AfterloadAfterload
��Compliance (EDPVR)Compliance (EDPVR)
��Contractility (ESPVR)Contractility (ESPVR)
��EF EF
��Systolic DysfunctionSystolic Dysfunction
��Diastolic DysfunctionDiastolic Dysfunction
1010
ESPVR Reflects ContractilityESPVR Reflects Contractility
1111
Alterations in
Preload and Afterload
Alterations in
Preload and Afterload
1212
Systolic (ESPVR) and
Diastolic Dysfunction (EDPVR)
Systolic (ESPVR) and
Diastolic Dysfunction (EDPVR)

1313
All Valvular DefectsAll Valvular Defects
1414
Each Valve DefectEach Valve Defect
EtiologyEtiology
Natural HistoryNatural History
AnatomyAnatomy
PathophysiologyPathophysiology
PressurePressure--Volume RelationshipVolume Relationship
MurmurMurmur
Anesthetic ConsiderationsAnesthetic Considerations�� Homodynamic GoalsHomodynamic Goals
�� MonitoringMonitoring
�� Anesthetic TechniqueAnesthetic Technique
�� Treatment of Untoward EventsTreatment of Untoward Events
Surgical OptionsSurgical Options
1515
Aortic StenosisAortic Stenosis
1616
Etiology of Aortic StenosisEtiology of Aortic Stenosis
Most serious valvular defectMost serious valvular defect
�� Carries the highest risk of sudden deathCarries the highest risk of sudden death
�� AS is present in 40% of pt w/ CADAS is present in 40% of pt w/ CAD
�� Independently Independently ↑↑ risk of MI 2.4 foldrisk of MI 2.4 fold�� Perioperative mortality is 11% w/ critical ASPerioperative mortality is 11% w/ critical AS
CongenitalCongenital�� Unicuspid (90% have AI)Unicuspid (90% have AI)
�� Bicuspid Bicuspid
�� TricuspidTricuspid
AcquiredAcquired�� Calcified (most common esp. w/Calcified (most common esp. w/↑↑↑↑↑↑↑↑ageageageageageageageage))�� RheumaticRheumatic
1717
Causes of AS as a
Function of Age
Causes of AS as a
Function of Age
From From PassikPassik CS, Ackermann DM, CS, Ackermann DM, PluthPluth JR, Edwards JR, Edwards
WD: Temporal changes in the causes of WD: Temporal changes in the causes of aoerticaoertic stenosisstenosis: :
A surgical A surgical patholologicpatholologic study of 645 cases. Mayo study of 645 cases. Mayo ClinClin
Proc 62;119, 1987Proc 62;119, 1987 1818
Natural HistoryNatural History
Long Asymptomatic PeriodLong Asymptomatic Period
Rx w/ statins and ACE inhibitorsRx w/ statins and ACE inhibitors
SurvivalSurvival
5 years after 5 years after
onset of onset of ANGINA*ANGINA*
3 years after 3 years after
onset of onset of SYCOPESYCOPE
2 years after 2 years after
onset of onset of CHF*CHF*
Sudden Death!Sudden Death!
***Caution when using nitrates to ***Caution when using nitrates to treat angina or CHF****treat angina or CHF****

1919
Anatomy of ASAnatomy of AS
VALVE AREA GRADIENTVALVE AREA GRADIENT(cm(cm22)) (mm Hg)(mm Hg)
Normal :Normal : 3 3 00
Mild (Stage 1)Mild (Stage 1) >1.5 >1.5 0 0 -- 20 20
Moderate (Stage 2)Moderate (Stage 2) 1.0 1.0 -- 1.5 1.5 20 20 –– 4040
Severe (Stage 2) Severe (Stage 2) < 1.0 < 1.0 >40>40
Critical (Stage 3)Critical (Stage 3) < 0.75< 0.75
Jet Flow > 4.5 m/sec or an Jet Flow > 4.5 m/sec or an ↑↑0.3 m/sec/year or 0.3 m/sec/year or
LV EF < 50%LV EF < 50%
2020
Pathophysiology of Aortic StenosisPathophysiology of Aortic Stenosis
Aortic Stenosis
Obstruction to LV Ejection
Chronic LV Pressure Overload�Parallel Replication of Sarcomeres
Concentric LV Hypertrophy
Pressure Gradient Created Across the Valve
2121
Pathophysiology of ASPathophysiology of AS
Concentric Hypertrophy (normal chamber size)Concentric Hypertrophy (normal chamber size)
Decreased ComplianceDecreased Compliance
�� ↑↑ LVEDPLVEDP
�� ↑↑ Reliance on atrial kick (40% of LVEDV)Reliance on atrial kick (40% of LVEDV)
CO and EF are initially normal (donCO and EF are initially normal (don’’t let this fool you!)t let this fool you!)
Very Vulnerable to IschemiaVery Vulnerable to Ischemia�� ↑↑ Demand d/t Demand d/t ↑↑ muscle mass and wall tensionmuscle mass and wall tension
�� ↓↓ Supply d/t Supply d/t ↓↓ diastolic time and diastolic time and ↑↑ LVEDPLVEDP�� ↑↑ HR can be disastrousHR can be disastrous
�� Maintaining diastolic BP is essentialMaintaining diastolic BP is essential
�� CPR is often ineffectiveCPR is often ineffective
2222
2323
Acute AS the Pressure -Volume LoopAcute AS the Pressure -Volume Loop
2424
Pressure Gradient
Across the Valve
Pressure Gradient
Across the Valve

2525
Physical FindingsPhysical Findings
�� Mid systolic Mid systolic
�� Ejection murmur Ejection murmur
�� RSB, 2nd ICSRSB, 2nd ICS
ECG ECG –– LVHLVH
2626
MonitoringMonitoring
ECG:ECG: LVHLVH
AA--Line:Line:
�� Slow upstroke Slow upstroke �� pulsuspulsustardustardus
�� Late peak w/ loss of the Late peak w/ loss of the dicroticdicrotic notch causing a notch causing a narrow pulse pressure narrow pulse pressure ��pulsuspulsus parvusparvus
PAPPAP waveformwaveform
�� Great beat to beat respiratory Great beat to beat respiratory variationvariation
Echo: Echo:
�� Narrowed orifice (causing jet)Narrowed orifice (causing jet)
�� LVHLVH
2727
Homodynamic GoalsHomodynamic Goals
PP-- Full: adequate intravascular volume to fill Full: adequate intravascular volume to fill noncompliant ventricular chambernoncompliant ventricular chamber
AA-- Already elevated, but relatively fixed; coronary Already elevated, but relatively fixed; coronary
perfusion pressure must be maintainedperfusion pressure must be maintained
CC-- Usually not a problem; inotropes may be helpful Usually not a problem; inotropes may be helpful
preinduction in endpreinduction in end--stage AS with hypotensionstage AS with hypotension
RR-- Not too slow (Not too slow (↓↓↓↓↓↓↓↓ CO), not too fast (ischemia)CO), not too fast (ischemia)
RhyRhy-- Sinus!! Cardioversion if hemodynamic crash fromSinus!! Cardioversion if hemodynamic crash from
supraventricular dysrhythmiasupraventricular dysrhythmia
MVO2MVO2-- Ischemia is an everIschemia is an ever--present risk; tachycardia andpresent risk; tachycardia and
hypotension must be avoidedhypotension must be avoided2828
HEMODYNAMIC GOALSHEMODYNAMIC GOALS
PA pressures remain relatively PA pressures remain relatively
normal until endnormal until end--stage aortic stage aortic
stenosis.stenosis.
MaintainMaintainPVRPVR
Afterload is elevated, but relatively Afterload is elevated, but relatively
fixed; coronary perfusion pressure fixed; coronary perfusion pressure
must be maintained. must be maintained.
Avoid hypotension.Avoid hypotension.
IncreasedIncreasedSVRSVR
Usually not a problem; Usually not a problem; inotropesinotropes may may
be helpful be helpful preinductionpreinduction in endin end--stage stage
aortic stenosis with hypotension.aortic stenosis with hypotension.
MaintainMaintainContractilityContractility
Avoid extremes of HR.Avoid extremes of HR. Decreased CO Decreased CO
with very slow HR, ischemia with with very slow HR, ischemia with
fast HR. Maintain Sinus Rhythm.fast HR. Maintain Sinus Rhythm.
Slow NormalSlow Normal
SinusSinusHeart RateHeart Rate
Need increased preload to fill Need increased preload to fill
noncompliant LV.noncompliant LV.IncreasedIncreasedPreloadPreload
2929
Anesthetic TechniqueAnesthetic Technique
RegionalRegional
�� Maintain filling pressureMaintain filling pressure
�� Keep diastolic BP upKeep diastolic BP up
�� Adequate pain control (avoid tachycardia)Adequate pain control (avoid tachycardia)
GeneralGeneral
�� Etomidate and primary narcotic techniqueEtomidate and primary narcotic technique
�� Low dose inhalation Low dose inhalation
�� Junctional rhythm is a distinct disadvantageJunctional rhythm is a distinct disadvantage
3030
Surgical OptionsSurgical Options
Repair: rarely possibleRepair: rarely possible
Replacement:Replacement:
BioprosthesisBioprosthesis
Porcine( pig valve) orPorcine( pig valve) or
Bovine (cow pericardium sewn Bovine (cow pericardium sewn on frame)on frame)�� No anticoagulationNo anticoagulation
�� Lasts 10Lasts 10--20 years20 years
MechanicalMechanical�� Require anticoagulationRequire anticoagulation
�� Careful antibiotic prophylaxisCareful antibiotic prophylaxis
�� Lasts a lifetimeLasts a lifetime
Other OptionsOther Options�� HomograftsHomografts (cadaver valves)(cadaver valves)
�� Ross Procedure (Pulmonary Valve placed in Aortic Position)Ross Procedure (Pulmonary Valve placed in Aortic Position)
�� PercutaneousPercutaneous AVRAVR

3131
Hypertrophic Cardiomyopathy
(HCM)
Hypertrophic Cardiomyopathy
(HCM)
AKA:AKA:
HOCM: HOCM:
Hypertrophic Obstructive Hypertrophic Obstructive
CardiomyopathyCardiomyopathy
IHSS: IHSS:
Idiopathic Hypertrophic Idiopathic Hypertrophic
SubaorticSubaortic StenosisStenosis
3232
HOCMHOCM
3333
HCMHCM
Etiology: Etiology: �� Genetic (mutation of the BGenetic (mutation of the B--myacinmyacin heavy chain)heavy chain)
�� Most common genetically transmitted CVDMost common genetically transmitted CVD
�� Leading Cause of Death in Athletes < 35Leading Cause of Death in Athletes < 35
Natural HistoryNatural History�� LVH in septum, apex and LVH in septum, apex and midventricalmidventrical (> 30 mm)(> 30 mm)
�� Not all patients are at equal risk, family Not all patients are at equal risk, family hxhx of sudden of sudden
death or documented obstruction are death or documented obstruction are ↑↑↑↑↑↑↑↑ riskriskriskriskriskriskriskrisk�� SxSx include: syncope, dyspnea, palpitations, PND, CHF, fatigueinclude: syncope, dyspnea, palpitations, PND, CHF, fatigue
�� MR causes LA enlargement making the patient prone to AMR causes LA enlargement making the patient prone to A--fibfib
�� SxSx worsen with worsen with ↑↑ HR, HR, ↓↓ preload, hypotension, PPV, and peeppreload, hypotension, PPV, and peep
�� Obstruction is worse with MR caused by SAM ( systolic Obstruction is worse with MR caused by SAM ( systolic anterior motion of the mitral valve)anterior motion of the mitral valve)
3434
HCM- Medical ManagementHCM- Medical Management
MedicationsMedications--�� Beta blockers to control HR and Beta blockers to control HR and ↓↓ outflow obstructionoutflow obstruction
�� Ca channel blockers to improve ventricular filling and Ca channel blockers to improve ventricular filling and ↓↓ ischemiaischemia
�� Disopyramide to Disopyramide to ↓↓ contractilitycontractility
�� Amiodarone for atrial dysrhythmiasAmiodarone for atrial dysrhythmias
ProceduresProcedures--�� Ethanol ablation of septal perforatorsEthanol ablation of septal perforators
�� AICDAICD
�� Asynchronous RV Asynchronous RV prexcitationprexcitation biventricular pacingbiventricular pacing
3535
Septal MyectomySeptal Myectomy
3636
Hemodynamic Goals in HOCMHemodynamic Goals in HOCM

3737
HOCM: HEMODYNAMIC GOALSHOCM: HEMODYNAMIC GOALS
Usually not a problem.Usually not a problem.MaintainMaintainPVRPVR
Increased afterload reduces the Increased afterload reduces the
gradient across LVOT.gradient across LVOT. Thickened Thickened
myocardium requires increased myocardium requires increased
diastolic BP.diastolic BP.
IncreasedIncreasedSVRSVR
Decreased contractility reduces Decreased contractility reduces
gradient across LVOT.gradient across LVOT. BetaBeta--
blockade is beneficial.blockade is beneficial.
DecreasedDecreasedContractilityContractility
Decreased HR reduces oxygen Decreased HR reduces oxygen
demand of thickened myocardium. demand of thickened myocardium.
May also allow time for adequate LV May also allow time for adequate LV
filling.filling.
DecreasedDecreasedHeart RateHeart Rate
Increased preload reduces the Increased preload reduces the
gradient across LVOT. Avoid gradient across LVOT. Avoid
hypovolemia.hypovolemia.
IncreasedIncreasedPreloadPreload
3838
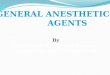
SAMSAMIntraoperative
transesophageal
echocardiography
images
demonstrating systolic anterior
motion of the
anterior mitral
valve leaflet (upper
right panel) and an interleaflet gap
(lower left panel)
through which a jet
of mitral
regurgitation (lower
right panel) is centrally directed
into the left atrium
3939
Aortic InsufficiencyAortic Insufficiency
4040
Etiology of AIEtiology of AI
Congenital: (rarely an isolated lesion)Congenital: (rarely an isolated lesion)
Acquired:Acquired:�� AcuteAcute
•• Infective endocarditisInfective endocarditis
•• Dissections of the thoracic aorta d/t Dissections of the thoracic aorta d/t MarfanMarfan’’ss or thoracic or thoracic traumatrauma
�� ChronicChronic
•• RHD is the most common causeRHD is the most common cause
•• Aortic root Aortic root annuloaortectasiaannuloaortectasia from from
•• AgingAging
•• Chronic HTN Chronic HTN
•• Connective tissue disorders Connective tissue disorders
•• Appetite suppressant meds (Appetite suppressant meds (fenfluraminefenfluramine))
4141
Natural History of AINatural History of AI
AcuteAcute�� Sudden LV failureSudden LV failure
�� Pulmonary congestionPulmonary congestion
�� Systemic hypotensionSystemic hypotension
ChronicChronic�� Long asymptomatic period (20 years) Long asymptomatic period (20 years)
�� Regurgitant flow Regurgitant flow �� volume overload. volume overload.
•• Volume overload Volume overload �� ↑↑ SV SV �� HTN HTN ��PPressure Overload.ressure Overload.
�� Progressive eccentric hypertrophy of LVProgressive eccentric hypertrophy of LV
�� When failure finally occurs, When failure finally occurs, damage is irreversibledamage is irreversible
�� LV function is both an early and late predictor of LV function is both an early and late predictor of mortality after AVRmortality after AVR
�� Survival after Survival after sxsx begin is 5begin is 5--10 years10 years
4242
Anatomy: AV Incompetence Anatomy: AV Incompetence
Angina, CHF,Angina, CHF,
Irreversible LV Irreversible LV
dysfunctiondysfunction
>60%>60%4+4+Severe Severe
(wide open)(wide open)
Dyspnea & Dyspnea &
CHFCHF4040--60%60%2+ 2+
3+3+
ModerateModerate
MinimalMinimal< 40%< 40%1+1+MildMild
SymptomsSymptomsRegurgitantRegurgitant
FractionFraction
GradeGradeClassificationClassification

4343 4444
Pathophysiology of Aortic RegurgitationPathophysiology of Aortic Regurgitation
Backward flow of blood from aorta into LV (Diastolic)
Increased LV volume
and pressure
Increased SV (Frank-Starling Mechanism)
Peak systolic pressure increased because of
increased SV ejected into aorta
Increased diastolic wall-tension produces eccentric hypertrophy
Rapid fall of aortic pressure during diastole
Increased pulse pressure
Increased LA pressure
Increased pulmonary
venous pressure
Pulmonary edema
4545
Pressure Volume RelationshipPressure Volume Relationship
4646
Classic Murmur of AI Classic Murmur of AI
Decrescendo diastolic @ 2Decrescendo diastolic @ 2ndnd ICS RSB ICS RSB
4747
Homodynamic GoalsHomodynamic Goals
PP-- Normal Normal -- Full: adequate intravascular volume to fill Full: adequate intravascular volume to fill compliant ventriclecompliant ventricle
AA-- Reduction beneficial with vasodilators or anesthetics;Reduction beneficial with vasodilators or anesthetics;
Increases augment regurgitant flowIncreases augment regurgitant flow
CC-- Usually adequateUsually adequate
RR-- Modest tachycardia reduces ventricular volume, Modest tachycardia reduces ventricular volume, raises aortic diastolic pressureraises aortic diastolic pressure
RhyRhy-- Usually sinusUsually sinus
MVO2MVO2-- Not usually a problemNot usually a problem
4848
AORTIC REGURGITATION:
HEMODYNAMIC GOALS
AORTIC REGURGITATION:
HEMODYNAMIC GOALS
PA pressures remain relatively PA pressures remain relatively
normal except in patients with endnormal except in patients with end--
stage disease.stage disease.
MaintainMaintainPVRPVR
Afterload reduction is helpful in Afterload reduction is helpful in
improving forward flow.improving forward flow.DecreasedDecreasedSVRSVR
Must be maintained.Must be maintained.MaintainMaintainContractilityContractility
Increased HR reduces diastolic time Increased HR reduces diastolic time
and reduces and reduces regurgitantregurgitant fraction.fraction.
Also raises diastolic BP and Also raises diastolic BP and
decreases LVEDP.decreases LVEDP.
IncreasedIncreasedHeart RateHeart Rate
Because of increased LV volumes, Because of increased LV volumes,
need increased preloadneed increased preload to maintain to maintain
forward flow. Avoid hypovolemia.forward flow. Avoid hypovolemia.
IncreasedIncreasedPreloadPreload

4949
MonitoringMonitoring
��ECGECG
��AA--line: line:
•• Rapid upstroke with low Rapid upstroke with low dicrotic notchdicrotic notch
•• Wide pulse pressure (80Wide pulse pressure (80--100 mmHg)100 mmHg)
•• Double peaked (Double peaked (biferiensbiferiens))
•• BoundingBounding
��CVPCVP
��PA Catheter (giant V wave PA Catheter (giant V wave on wedge trace)on wedge trace)
��TEETEE
•• Grade regurgitant Grade regurgitant fxfx
•• Assess adequacy of repair Assess adequacy of repair or replacementor replacement
5050
Anesthetic ManagementAnesthetic Management
Regional AnesthesiaRegional Anesthesia
�� Afterload reduction reduces regurgitant Afterload reduction reduces regurgitant fxfxand enhances forward flowand enhances forward flow
�� Maintain intravascular volumeMaintain intravascular volume
General AnesthesiaGeneral Anesthesia
�� Use agents that maintain or elevate HRUse agents that maintain or elevate HR
�� Potent agents are OKPotent agents are OK
�� Etomidate/Narcotic technique good for poor Etomidate/Narcotic technique good for poor LVFLVF
�� Maintain intravascular volumeMaintain intravascular volume
5151
Surgical OptionsSurgical Options
Indications:Indications:
�� All symptomatic patientsAll symptomatic patients
�� Asymptomatic patients with Asymptomatic patients with �� LV LV fxfx
Options:Options:
�� Repair with annuloplasty ring or valvular Repair with annuloplasty ring or valvular plicationplication
�� Replace with mechanical or biologic valveReplace with mechanical or biologic valve
�� Experimental Experimental percutaneouspercutaneous AV AV replacementreplacement
5252
Mitral StenosisMitral Stenosis
5353
EtiologyEtiology
CongenitalCongenital
AcquiredAcquired
�� Rheumatic FeverRheumatic Fever (2 (2 xx’’ss as frequent in as frequent in women)women)
�� Sometimes after radiation of the chest Sometimes after radiation of the chest from breast or other CAfrom breast or other CA
�� Rheumatoid Arthritis, lupus or Rheumatoid Arthritis, lupus or carcinoidcarcinoid syndromesyndrome
5454
Natural HistoryNatural History
��Stenosis begins 2 yrs Stenosis begins 2 yrs after RHDafter RHD
��20 yr asymptomatic20 yr asymptomatic
��SxSx begin in 40begin in 40’’ss-- 5050’’ss
��Heart failure is most Heart failure is most common presentationcommon presentation
��40% develop a40% develop a--fibfib
��SxSx develop w/pregnancy, develop w/pregnancy, anemia, infectionanemia, infection

5555
Anatomy of MSAnatomy of MS
VALVE AREA VALVE AREA SYMPTOMSSYMPTOMS(cm(cm22))
Normal :Normal : 44--6 6
Mild (Stage 1)Mild (Stage 1) 1.51.5--2.5 2.5 with exercisewith exercise
Moderate (Stage 2)Moderate (Stage 2) 1.0 1.0 -- 1.5 1.5 mild exertion mild exertion
onset of aonset of a--fibfib
Severe (Stage 3) Severe (Stage 3) < 1.0 < 1.0 at restat rest
5656
Pathophysiology of MSPathophysiology of MS
�� LV LV fxfx usually maintained (15% LV dysfunction)usually maintained (15% LV dysfunction)
�� PG = PG = (Cardiac Output)(Cardiac Output)22
Diastolic Filling TimeDiastolic Filling Time
�� AA--fib fib →→ ��PG (2PG (2o rapid HR) → pulmonary edema
� Pulmonary HTN (80%)
� 5-15 x’s ↑ In PVR
� V/Q mismatches (reversal in normal apex to base perfusion gradient)
5757
Pathophysiology of Mitral StenosisPathophysiology of Mitral Stenosis
Obstruction to LA emptying
Increased LA pressure
Increased LA size
Atrial fibrillation
Increased pulmonary artery pressure
Decreased LV filling
RV overload
Increased pulmonary venous pressure
Pulmonaryedema
5858
5959
Pressure Volume RelationshipsPressure Volume Relationships
6060
Pressure Volume LoopPressure Volume Loop

6161
Murmur MSMurmur MS
Diastolic rumbling murmur Diastolic rumbling murmur
Heard best at the apexHeard best at the apex
6262
Hemodynamic Goals MSHemodynamic Goals MS
PP-- Enough to maintain flow across stenosisEnough to maintain flow across stenosis
AA-- Avoid Avoid ↑↑↑↑↑↑↑↑ RV afterload (pulmonary vasoconstrictors)RV afterload (pulmonary vasoconstrictors)
? ? inotropesinotropes for systemic hypotensionfor systemic hypotension
CC-- LV usually OK until after CPB; right ventricle may beLV usually OK until after CPB; right ventricle may be
impaired if there is longimpaired if there is long--standing pulmonary standing pulmonary hypertensionhypertension
RR-- Slow to allow time for ventricular fillingSlow to allow time for ventricular filling
RhyRhy-- Often atrial fibrillation; control ventricular responseOften atrial fibrillation; control ventricular response
MVO2MVO2-- Not a problemNot a problem
CPBCPB-- Vasodilators may help post CPB RV failure; control ofVasodilators may help post CPB RV failure; control of
ventricular response may be difficultventricular response may be difficult
6363
Hemodynamic GoalsHemodynamic Goals
Avoid TachycardiaAvoid Tachycardia
�� Continue/Administer meds that control HRContinue/Administer meds that control HR
�� Treat new onset A fib aggressively (control ventricular rate)Treat new onset A fib aggressively (control ventricular rate)
Avoid Exacerbations of PHTAvoid Exacerbations of PHT
�� Avoid hypoxia, Avoid hypoxia, hypercarbiahypercarbia and acidosisand acidosis
�� Avoid NAvoid N22OO
�� Avoid trendelenburg positionAvoid trendelenburg position
�� Rx PHT w/ hypocapnia, NTG, and Nitric OxideRx PHT w/ hypocapnia, NTG, and Nitric Oxide
�� Watch for RV failure and consider Watch for RV failure and consider MilrinoneMilrinone
Maintain adequate intravascular volumeMaintain adequate intravascular volume
Treat hypotension with volumeTreat hypotension with volume (vasoconstrictors can worsen (vasoconstrictors can worsen PHT)PHT)
Early use of inotropes if neededEarly use of inotropes if needed
6464
MonitoringMonitoring
EKGEKG
AA--lineline
Pa Pa CathCath
�� PCWP or LAP will be > LVEDPPCWP or LAP will be > LVEDP
�� With tachycardia, LAP With tachycardia, LAP �� while LVEDP while LVEDP ��
TEETEE
�� Check adequacy of repairCheck adequacy of repair
�� Check for leaksCheck for leaks
�� Check for regurgitation after Check for regurgitation after commissurotomycommissurotomy
6565
Anesthetic TechniqueAnesthetic Technique
RegionalRegional
�� Caution d/t residual anticoagulationCaution d/t residual anticoagulation
�� Avoid hypotension. Avoid hypotension.
�� Position for adequate ventilationPosition for adequate ventilation
�� Maintain intravascular volumeMaintain intravascular volume
GeneralGeneral
�� Consider Etomidate/narcotic technique for PHT or Consider Etomidate/narcotic technique for PHT or severe LVsevere LV
�� Inhalation agents OK Inhalation agents OK except Nexcept N22OO
�� Avoid agents that Avoid agents that �� HRHR
�� Maintain intravascular volumeMaintain intravascular volume
6666
Surgical OptionsSurgical Options
CommissurotomyCommissurotomy--fused leaflets are separatedfused leaflets are separated
DecalcificationDecalcification
Replacement with bioprosthetic or mechanical valveReplacement with bioprosthetic or mechanical valve
If full sternotomyIf full sternotomy-- Maze or Pulmonary Vein Isolation Maze or Pulmonary Vein Isolation to treat Ato treat A--fibfib
Left atrial appendage ligation or resectionLeft atrial appendage ligation or resection
AA--fib treated with radiofrequency (heat) ablation or fib treated with radiofrequency (heat) ablation or cryotherapycryotherapy (freeze) ablation(freeze) ablation

6767
Mitral Insufficiency
or Regurgitation
Mitral Insufficiency
or Regurgitation
6868
Etiology of MREtiology of MR
CongenitalCongenital--rarerare
AcquiredAcquired-- both acute and chronicboth acute and chronic
�� RHDRHD-- rarerare
�� Most commonly encountered valve lesionMost commonly encountered valve lesion
�� Mitral Valve Prolapse (MVP)Mitral Valve Prolapse (MVP)•• Most common causeMost common cause
•• 15% will develop chronic MR15% will develop chronic MR
�� ChronicChronic•• LVH w/ annular dilation (eccentric hypertrophy)LVH w/ annular dilation (eccentric hypertrophy)
•• MVPMVP
•• MyxomatousMyxomatous degenerationdegeneration
•• FenfluramineFenfluramine appetite suppression appetite suppression
�� AcuteAcute•• Papillary muscle dysfunctionPapillary muscle dysfunction
•• Ruptured chordea Ruptured chordea tendineatendinea (most often (most often d/td/t ischemia)ischemia)
•• Bacterial endocarditisBacterial endocarditis
6969
Natural HistoryNatural History
��VariableVariable
��Long asymptomatic period Long asymptomatic period
w/ eccentric hypertrophy of w/ eccentric hypertrophy of
LA and LVLA and LV
��SxSx of forward heart failure of forward heart failure
develop (fatigue, weakness)develop (fatigue, weakness)
��Dysfunction is significant if Dysfunction is significant if
EF is EF is ≤≤ 50%50%
7070
Anatomy: MV Incompetence Anatomy: MV Incompetence
CHF,CHF,
Irreversible LV Irreversible LV
dysfunctiondysfunction
>60%>60%4+4+Severe Severe
(stage 3)(stage 3)
Fatigue, Fatigue,
weakness, CHFweakness, CHF3030--60%60%2+2+--3+3+Moderate Moderate
(stage 2)(stage 2)
MinimalMinimal< 30%< 30%1+1+Mild Mild
(stage 1)(stage 1)
SymptomsSymptomsRegurgitantRegurgitant
FractionFraction
GradeGradeClassificationClassification
7171
PathophysiologyPathophysiology
Chronic MRChronic MR
�� LV volume load LV volume load →→ eccentric hypertrophyeccentric hypertrophy
�� Regurgitant volume determined by Regurgitant volume determined by atrial/ventricular pressure gradientatrial/ventricular pressure gradient
�� Ventricular size directly correlates with annulus Ventricular size directly correlates with annulus sizesize
�� Vasodilators may improve hemodynamics (Vasodilators may improve hemodynamics (�� LV LV size)size)
�� Patients with Patients with sxsx have underlying LV dysfunctionhave underlying LV dysfunction
Acute MRAcute MR
�� LAP and PAP LAP and PAP �� →→ pulmonary edema and RHFpulmonary edema and RHF
�� In Acute MI w/ MR In Acute MI w/ MR →→ ischemia is usually present ischemia is usually present and survival is poorand survival is poor
7272

7373
Pathophysiology of Mitral RegurgitationPathophysiology of Mitral Regurgitation
Backward flow of blood from LV to LA (Systolic)
Increased LA volume and
pressure
Increased LV filling(Increased LVEDV)
Increased SV
Blood ejected into aorta
Left atrial enlargement
Increased pulmonary
venous pressures
Pulmonaryedema
7474
Pressure Volume RelationshipPressure Volume Relationship
7575
Pressure Volume Loop in Chronic MRPressure Volume Loop in Chronic MR
7676
Murmur (Pansystolic or Holosystolic)Murmur (Pansystolic or Holosystolic)
7777
Hemodynamic Goals In MRHemodynamic Goals In MR
7878
Hemodynamic ConsiderationsHemodynamic Considerations
�� Mild TachycardiaMild Tachycardia
�� Low SVR (peripheral venodilation)Low SVR (peripheral venodilation)
�� ExceptionException: in patients with MVP who : in patients with MVP who
have redundant leaflets because have redundant leaflets because
higher HR and Low SVR will cause higher HR and Low SVR will cause
more obstruction to flowmore obstruction to flow

7979
MonitoringMonitoring
��EKGEKG
��AA--lineline
��CVPCVP
��PA PA CathCath-- classic classic
giant V wavegiant V wave
��TEETEE
8080
Anesthetic TechniqueAnesthetic Technique
RegionalRegional-- benefits from benefits from �� afterloadafterload
GeneralGeneral
�� Inhalation/STP is OK for normal LVInhalation/STP is OK for normal LV
�� Etomidate/Narcotic for impaired LVEtomidate/Narcotic for impaired LV
8181
Surgical OptionsSurgical Options
““Mini Mitral Valve RepairMini Mitral Valve Repair”” (Cosgrove Ring for (Cosgrove Ring for AnnuloplastyAnnuloplasty))
Robotically Assisted MV repair or Robotically Assisted MV repair or replacementreplacement
PercutaneousPercutaneous mitral valve repair (Emitral valve repair (E-- Valve)Valve)
Repair flail leaflet, Chordae or papillary Repair flail leaflet, Chordae or papillary musclemuscle
Replacement with biologic or mechanical Replacement with biologic or mechanical valvevalve
If Full Sternotomy: Maze or PV Isolation for If Full Sternotomy: Maze or PV Isolation for AA--fibfib
8282
8383
Thanks for Your AttentionThanks for Your Attention
A Pleasure and a Privilege!A Pleasure and a Privilege!