Embed Size (px)
Citation preview

Anesthetic Implications for Trisomy 21, 18 and 13
Anne Baetzel, MDUniversity of Michigan
C. S. Mott Children’s Hospital
Learning Objectives
• Describe pre‐operative testing for patients with Trisomy 21
• Identify anatomic and physiologic differences in Trisomy 21 and their impact on anesthesia
• Outline congenital defects associated with Trisomy 18 and implications for anesthesia
• Discuss ethics of treating patients with Trisomy 18 and 13

Disclosures
• None

To Proceed or Not Proceed?45 yo woman with Down syndrome presents for dental restorations and extractions. Her parents are both recently deceased and power of attorney has shifted to her younger brother who’s not certain of her health status. She currently resides in an assisted living facility. In pre‐op she is cooperative on physical exam, but you note a well‐healed sternotomy scar. She is neurologically intact and her only medication is levothyroxine. Vital signs are all WNL. What information do you require in order to proceed?• Echocardiogram?• Thyroid function tests?• Complete blood count?• Flexion/extension cervical spine films?• Sleep study?• Disposition?

Embryology…
• Meiotic non‐disjunction• Sperm or egg cell now has extra copy of ch 21• Combines with normal gamete 47 chromosomes• 95%: 3 free copies• 3‐4%: unbalanced translocations• 1%: mosaicism
https://embryology.med.unsw.edu.au/embryology/index.php/Trisomy_21

Incidence
• Most common chromosome disorder in live‐born infants
• In the US, ~1/700 live births• ~5400 infants born each year with Trisomy 21

Affected Organ Systems
• Neurologic• Cardiac• Pulmonary• Hematologic• Gastrointestinal• Endocrine• Upper airway

Cognitive Impairment
• Variable degree of impairment• IQ range, 20‐70• Attention problems, ADHD, OCD behaviors, noncompliant behaviors not uncommon
• Implications for parental separation, induction technique, post‐operative behavior
Dietary Supplements
• Promoted to address cognitive aspects of T21• Inquire specifically about supplements!• Examples include carnitine, curcumin, folic acid, ginkgo biloba, piracetam, MSB Methyl Plus, NuTriVene, Speak
• Piracetam may act as platelet inhibitor• None endorsed by main advocacy organizations
Neurologic
• Absent Moro reflex• Generalized hypotonia• Joint laxity• Hearing loss—conductive, sensorineural or mixed (38‐78%)
• Deficiency in language production• Increased risk of seizures, incl infantile spasms• Increased risk of Moya moya disease• Neuropathological changes typical of Alzheimer’s develop by fifth decade of life
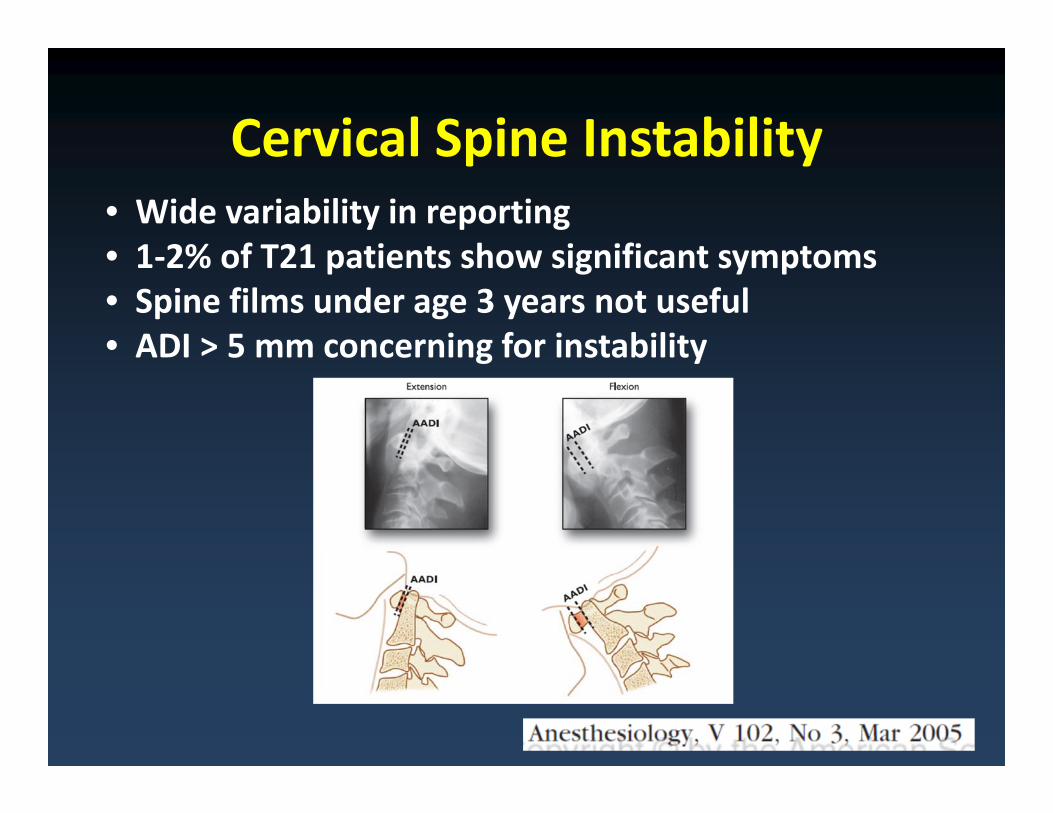
Cervical Spine Instability• Wide variability in reporting• 1‐2% of T21 patients show significant symptoms• Spine films under age 3 years not useful• ADI > 5 mm concerning for instability

AAP Recommendations
• Previous recommendation—one set of lateral cervical spine films between ages 3 and 5 years
• Newest guideline—routine films for ASYMPTOMATIC children NOT RECOMMENDED at ANY age
• Wide variability even within practitioners in the same institution

Intraoperative Experience
• Only a handful of injuries• Neck flexion carries greatest risk of subluxation
• Neck rotation <60 degrees does not impair SSEP’s in symptomatic patients
• No specific guidelines from anesthesia societies for neck immobilization

Patient Positioning
Maintain neutral position
• Intubation• Tonsillectomy & adenoidectomy
• Myringotomy and tympanoplastytubes
• DLB• Esophagoscopy• Cleft palate repair• Port placement
Treat all T21 patients as having potential for acute dislocation

Care of the Cervical Spine
• Routine x‐rays under the age of three not recommended
• Careful pre‐op history and physical exam• Routine use of video laryngoscopy• Maintain in‐line stabilization• Protrusion position• Neck in neutral position, rotation <60o

Hypotonia
• Slow feeding, choking with feeds, recurrent pneumonia, persistent respiratory symptoms
• After induction, even more pronounced airway/soft tissue collapsenatural airway obstruction
https://clinicalgate.com/genetics/

Cardiovascular Disease
• Most prevalent malformation associated with Down Syndrome
• Fetal diagnostic rate 56%• Atrioventriculoseptal defect most common• ASD• VSD• Tetralogy of Fallot

• Retrospective study• 96 children with Down Syndrome • Matched to similar cohort of patients
without DS• Higher prevalence, greater degree of
bradycardia with Sevoflurane induction in patients with DS


Pulmonary Hypertension
• Higher incidence of PAH in DS children• Most often due to increased PVR • Congenital heart disease L R shunt• Increased incidence of PPHN (1.2% vs. 0.1%)• Upper airway obstruction• Lower airway abnormalities

ENT
• Stenotic ear canals• Frequent otitis media• Increased frequency of choanal atresia• Enlarged tonsils (extreme hypertrophy of lingual tonsils)
• Enlarged adenoids• Small epiglottis
https://www.boredpanda.com/mom‐fighting‐son‐down‐syndrome

Airway Differences
Anatomic Abnormalities• Flattened nasal bridge• Macroglossia• Shallow hypopharyngeal
dimensions• Tracheal stenosis• Congenital subglottic
stenosis• Airway malacia• Microdontia
Functional Abnormalities• Pharyngeal muscle
hypotonia• Hypertrophy of tonsillar
and adenoid tissue• Increased secretions• Frequent infections


Endotracheal Tube Selection
• Subglottic stenosis—acquired or congenital• Endotracheal tube should be at least TWO sizes smaller than you would typically select
• Increased incidence of post‐intubation stridor

Endocrine Disease
• Hypothyroidism most common • TSH check as newborn, at 6 months, at 1 year and then annually
• Check sooner if signs of dysfunction• Congenital hypothyroidism, 1% risk• Risk of hypothyroidism increases with increasing age
Endocrine
• Reduced resting metabolic rate• Higher frequency of obesity• Propensity for diabetes mellitus

Hematologic Disease
• During newborn period ‐‐Neutrophilia in up to 80%‐‐Thrombocytopenia in up to 66%‐‐Polycythemia in up to 34%
• Transient myeloproliferative disease in 10% of neonates
‐‐very high WBC count (stroke, thrombosis)‐‐decrease in other cell lines‐‐plasmapheresis if WBC >125,000‐‐increased risk of leukemia later in life

Hematologic, cont’d
• Equal frequency of AML and ALL‐‐1 in 300• AML typically arises between 1‐5 years old• Large percentage present first with myelodysplastic syndrome
• ALL has similar presentation to non‐T21 patients
• 10‐20 fold increased risk in patients with T21• Similar survival rates

Risk for Prematurity
• Rate of preterm delivery ~25% (vs. 6.3%)• Average weight of DS babies ~450 gm less than non‐DS babies
• T21 babies may be more sensitive to stressors in the neonatal period
• At higher risk than equivalent non‐T21 babies
http://noahsdad.com/did‐i‐cause‐down‐syndrome/

Ophthalmic Features
Brushfield Spots
Epicanthalfolds
Up‐slanting palpebral fissures
Ambylopia

Ophthalmic Disorders
• Strabismus• Cataracts (15%)• Nystagmus• Severe refractive errors (50%)

GI system
• Constipation• Hirschsprungdisease (<1%)
• Duodenal atresia (12%)
• Annular pancreas
• Celiac disease• GERD

• Obesity/skin folds• Xerodermia• Smaller diameter vessels
• Vascular pattern abnormality
• Notoriously more challenging
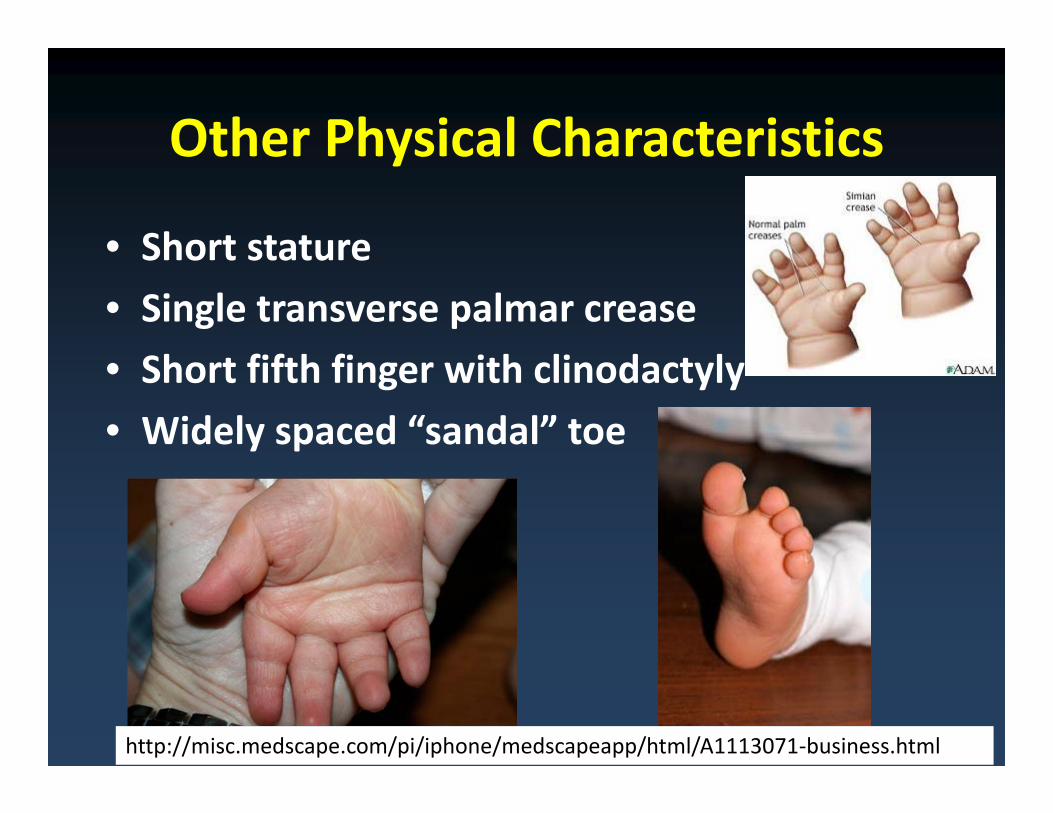
Other Physical Characteristics
• Short stature• Single transverse palmar crease• Short fifth finger with clinodactyly• Widely spaced “sandal” toe
http://misc.medscape.com/pi/iphone/medscapeapp/html/A1113071‐business.html

http://thatdadblog.com/category/why‐does‐wil‐fly/

Pre‐operative Preparation
• Annual thyroid function testing• Annual CBC• No need for routine cervical spine x‐ray• Cardiac studies if history of CHD• Induction plan tailored to patient cooperativity

Intraoperative Concerns
• Bradycardia with induction• Natural airway collapse• Smaller ETT size• Cervical spine instability• Increased likelihood of PHTN

Postoperative Concerns
• Suitability for outpatient procedures• Stridor

Trisomy 18
• Prevalence in live‐born infants 1/3600‐1/8500• 91% of infants die before age 1 year• Paradigm shift away from non‐intervention • Since 2004—4 case series of surgery for CHD

Diagnostic Criteria• Prenatal growth deficiency• Cleft lip and palate• Micrognathia• “Rocker‐bottom” feet• Clenched hands• Prominent occiput• Polydactyly• Renal anomalies• Heart defects• Shortened sternum• Microcephaly• Neurodevelopmental delay
https://www.everylifecounts.ie/stories/emily‐elizabeth/

Evolving Management
• Shift to strong parental authority• Poorly defined limits of parental autonomy• Disclosure of all information to make sound decisions
• Improved critical care• Rise of the internet, support groups

Words and phrases to avoid
• “It,” “that,” “vegetable,” “a T18”• “Incompatible with life”• “Futile”• “Hopeless”• “Waste of money/time/energy”• “Lethal”• Parents want providers to see their child as having value, being unique, as being a person

To Treat or Not to TreatEthical justification for non‐treatment
• Do no harm• Provide burdensome
treatment• Increase suffering• Limited benefit• Foster consumer model of
medicine
Ethical justification for treatment
• Parents’ right• Survive infancy• Enjoy reasonable quality of
life• Loved by family members• Self‐fulfilling prophecy
GOAL DIRECTED TREATMENT PLAN
http://arclegalfunding.org

Airway
• Prominent occiput• Short palpebral fissures• Abnormal dental position• Micrognathia• Cleft lip and/or palate, 60‐80%• Difficult mask fit• Difficult intubation potential

T18 and CHD
• 1990—first reported cases of surgery for CHD• Two prevailing beliefs—surgery for CHD does not prolong life of child with T18 & children with T18 do not die as a result of CHD‐‐mistaken
• SOFT surgery registry with 132 documented surgeries for heart defect
• No surgeries for ductal‐dependent lesions• Post‐operative course more complicated• Lower hospital survival rate

In summary
• Duty of parents: give due consideration to best interests of their child
• Duty of physician: facilitate proper exercise of parental authority, fiduciary duty to protect child from harm and suffering
• Overall inability to predict survival• Defer burdensome intervention until likely that child will survive beyond 6 months
• Just distribution of limited societal resources

Trisomy 13
• Also called Patau syndrome• Live birth rate 1/10,000‐1/20,000• Total prevalence ~1.5/10,000• Typically caused by translocation• Only 5% live longer than 6 months
http://trisomy13‐samara.blogspot.com/

Cardinal features• Cleft lip and/or palate, 60‐80%• Microphthalmia/anophthalmia• Postaxial polydactyly of limbs• Holoprosencephaly• Cardiac defects, 80%• Omphalocele• Cystic kidneys• Thin posterior (or missing) ribs• “Shield chest”• Polydactyly• Clinodactyly• Severe developmental delay
https://ghr.nlm.nih.gov/condition/trisomy‐13

References• Bai W et al. Hemodynamic Changes in Children with Down Syndrome during and following Inhalation
Inductions of Anesthesia with Sevoflurane. Journal of Clinical Anesthesia 2010; 22: 592‐597.• Borland LM et al. Frequency of Anesthesia‐Related Complications in Children with Down Syndrome
under General Anesthesia for Noncardiac Procedures. Pediatric Anesthesia 2004; 14: 733‐738.• Bull, MJ and Committee on Genetics. Clinical Report—Health Supervision for Children with Down
Syndrome. Pediatrics 2011; 128 (No 2): 393‐406.• Carey JC Trisomy 18 and Trisomy 13 Syndromes. In Management of Genetic Syndromes, Third Edition,
Edited by Suzanne B. Cassidy 2010; Chapter 54: 807‐823.• Courreges P et al. Anaesthetic Management for Edward’s Syndrome. Paediatric Anesthesia 2003; 13:
267‐269.• Janvier A et al. The Experience of Families with Children with Trisomy 13 and 18 in Social Networks.
Pediatrics 2012; 130: 293‐298.• Lewanda AF et al. Preoperative Evaluation and Comprehensive Risk Assessment for Children with Down
Syndrome. Pediatric Anesthesia 2016; 26: 356‐362.• Lorenz JM and Hardart GE. Evolving Medical and Surgical Management of Infants with Trisomy 18. Curr
Opin Pediatrics 2014, 26:169‐176.• Rosa RFM et al. Trisomy 18: Frequency, Types and Prognosis of Congenital Heart Defects in a Brazilian
Cohort. American Journal of Medical Genetics Part A 158A: 2358‐2361.• Sulemanji DS et al. Vascular Catheterization is Difficult in Infants with Down Syndrome. Acta
Anaesthesiol Scand 2009; 53: 98‐100.


CHD and T13
• VSD, ASD, PDA most common• Individualized goals of therapy• Treat when symptoms interfere with life• Maximize other therapeutic options• Limiting pulmonary blood flow?• Minimally‐invasive methods?• Would the infant’s life be long enough to die from fixed pulmonary hypertension?

Respiratory
• Development of pulmonary hypertension• Laryngomalacia• Recurrent aspiration• Susceptibility to RSV• Development of OSA in older children• Referral to sleep specialist? Home monitoring? Oxygen therapy? Synagis?

Neurologic
• Hypotonia during infancy, hypertonia in later childhood
• Seizures, 25‐50%• Central apnea • Holoprosencephaly
http://prenatalpediatrics.org/conditions/brain/holoprosencephaly/#.Wq1Z6lrwaCg

Growth and Feeding
• Weight and length remain <3rd percentile, Trisomy‐specific growth charts used
• Feeding difficulties in surviving neonates remain biggest challenge
• Suck, swallow reflexes may be diminished• GERD• Malrotation• Cleft lip and palate• Consider gastrostomy tube placement at 6 months? Nissen fundoplication has been performed

Ears and Hearing
• Middle ear and temporal bone abnormalities common
• Moderate to severe sensorineural hearing loss
• Microtia• Meatal atresia• Hearing test at >6 months
http://www.earaidnepal.org/education/teaching/teachingimages.html

Ophthamologic
• Microphthalmia• Anophthalmia• Coloboma• Ocular findings associated with holoprosencephaly
• Congenital cataracts• Early onset glaucoma

Genitourinary
• Cystic dysplasia• Increased frequency of UTI’s• Renal failure uncommon• Screening ultrasound recommended for all T13 infants
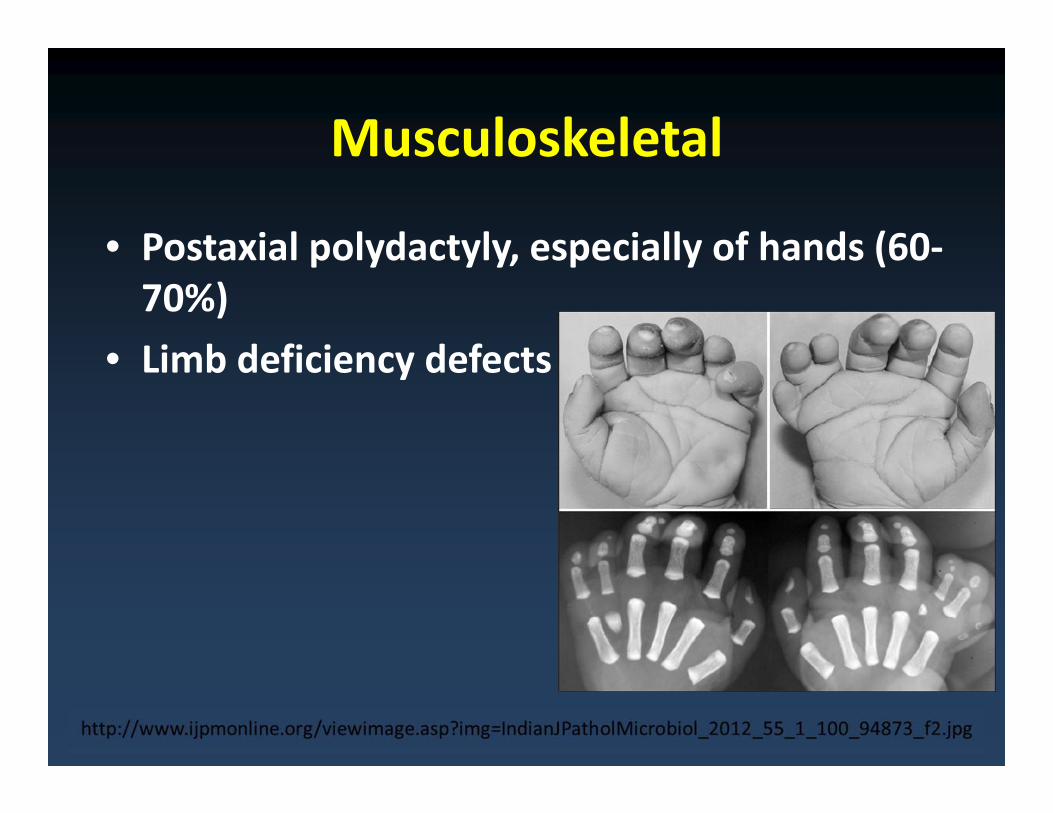
Musculoskeletal
• Postaxial polydactyly, especially of hands (60‐70%)
• Limb deficiency defects
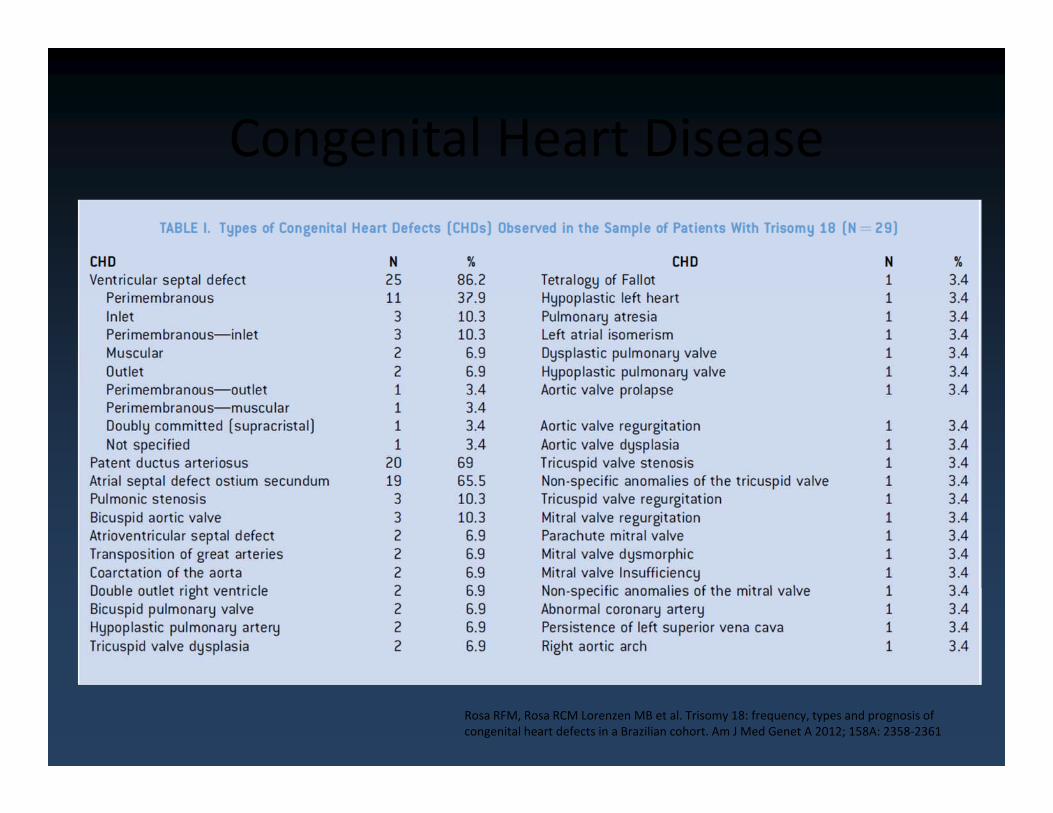
Congenital Heart Disease
Rosa RFM, Rosa RCM Lorenzen MB et al. Trisomy 18: frequency, types and prognosis of congenital heart defects in a Brazilian cohort. Am J Med Genet A 2012; 158A: 2358‐2361

Neurodevelopmental Delay
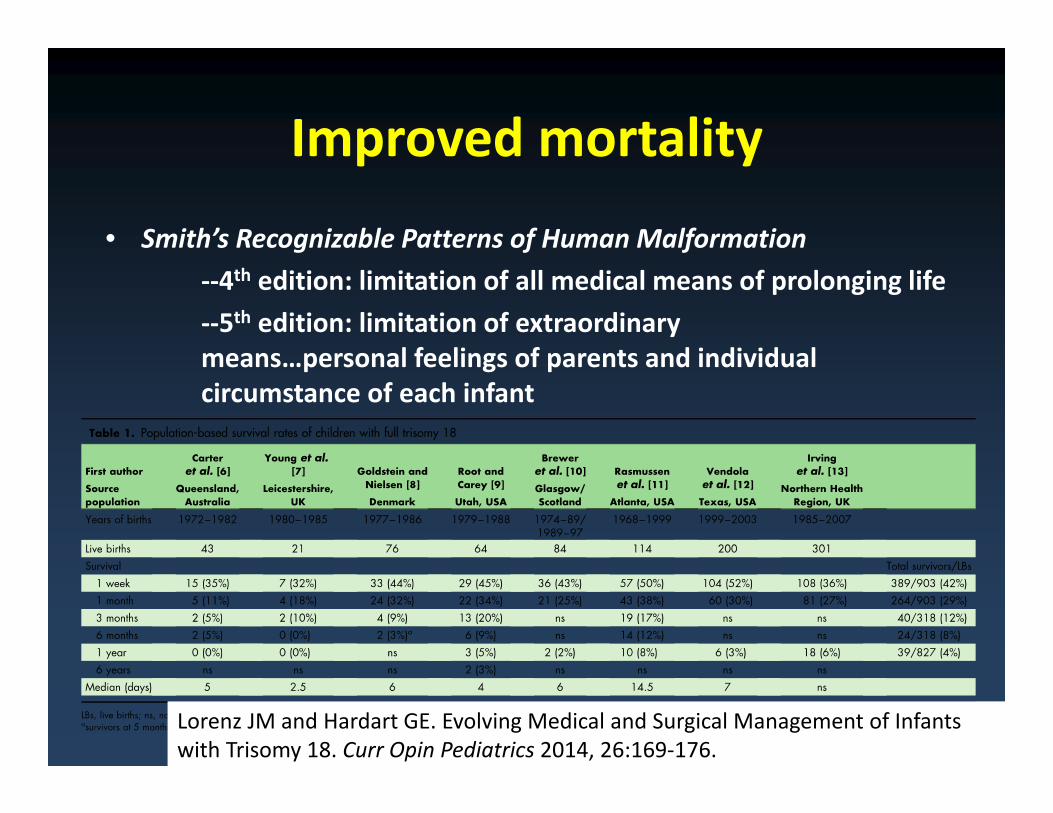
Improved mortality
• Smith’s Recognizable Patterns of Human Malformation‐‐4th edition: limitation of all medical means of prolonging life‐‐5th edition: limitation of extraordinary means…personal feelings of parents and individual circumstance of each infant
Lorenz JM and Hardart GE. Evolving Medical and Surgical Management of Infants with Trisomy 18. Curr Opin Pediatrics 2014, 26:169‐176.