Embed Size (px)
Citation preview

1
Anesthesiology
Glen T. Porter, MD
Faculty Advisor: Francis B. Quinn, MD, FACS
The University of Texas Medical Branch
Department of Otolaryngology
Galveston, Texas
June 2004

2
History 1540 Valerius Cordus synthesizes ether
1842 Dr. Crawford Long (Georgia) first uses inhaled ether to anesthetize patient for surgery
1845 Dr. Horace Wells attempts to demonstrate use of Nitrous oxide in surgery
1846 William Morton (dentist) uses ether anesthesia at Massachusetts General Hospital (soon to become the ether dome). Dr. John Warren removes a neck mass.
1846 Nitrous oxide used for anesthesia
1847 Dr. James Simpson introduces Chloroform anesthesia
1853 Queen Victoria undergoes anesthesia performed by Dr. John Snow

3
Crawford Long
Horace Wells W. Thomas Morton
History

4
History
1878 Endotracheal tube invented
1885 Halstead introduces nerve block anesthesia with cocaine
1934 Sodium thiopentone (IV anesthesia)
1934 Curare
1940’s clinical use of muscle relaxants
1950s Introduction of flourinated inhalational anesthetic agents

5
Anesthesia
Anesthesia=abolition of sensation
Analgesia=abolition of pain
General anesthesia renders the patient
unconscious and usually includes paralysis
Local anesthesia (analgesia) blocks
conduction of sensory nerves from the
operative site
“Triad of anesthesia”: asleep, pain-free, still

6
Stages of Anesthesia
Stage I (analgesia stage) – Conscious and rational
– Perception of pain is diminished
Stage II (delirium stage) – Unconscious
– Body responds reflexively and irrationally
– Breath holding, pupils dilated
– Muscle tone intact
Stage III (surgical anesthesia) – Increasing degrees of muscular relaxation
– Unable to protect airway
Stage IV (medullary depression) – Depression of cardiovascular and respiratory
centers

7
Inhalational Anesthesia
Effect is mediated by concentration of agent present in the nervous system
Each agent’s anesthesia effect mediated by solubility, metabolism, alveolar ventilation, cardiac output, potency
Minimum Alveolar Concentration (MAC) is a measure of relative potency
MAC=amount of an agent in which 50% of patients do not move with surgical stimulus.

8
Nitrous Oxide
Discovered 1776 by David Priestly
Largely recreational use until mid 1800’s
Colorless, tasteless, odorless
Low potency (MAC=105%)
Usually used with additional agent to achieve surgical anesthesia
Weak anesthetic
Powerful analgesic
Poor solubility (rapid onset/offset time)

9
Nitrous Oxide
Systemic effects
– Mild myocardial depression (usually innocuous)
– Severe cardiac depression with underlying
hemodynamic compromise
– No effect on respiration/neuromuscular junction
Side effects
– Blood:gas partition coefficient of nitrous oxide is 34
times greater than that of nitrogen.
Second gas effect
Pressure changes in air-filled spaces
– Prolonged exposure can result in megaloblastic or
aplastic anemia, B-12 deficiency (inhibits methionine
synthetase)

10
Nitrous oxide

11
Halothane
Synthesized by Suckling in 1956
First of the fluorinated anesthetics
Distinctive aroma, non-flammable, highly
potent (MAC=0.75%)
Poor analgesic properties
Very soluble in blood/fatty tissues with
potential for longer offset time

12
Halothane
Systemic Effects – Reduces/eliminates sympathetic response (including
baroresponse)
– Depresses respiratory drive. Respiration is rapid, shallow, and unvaried predisposing to atelectasis
– Decreases airway reflexes
– Decreases myocardial contractility and heart rate resulting in decreased cardiac output and hypotension
– Myocardial sensitization to exogenous catecholemines
Side Effects – Hepatitis
Thought to be mediated by allergic response to byproducts
– Malignant hyperthermia

13
Enflurane Introduced in 1972
Stable, nonflammable, pungent odor
MAC=1.68%
Systemic effects – Respiratory drive depressed (more than halothane), hypoxemia
response blunted
– Depresses cardiac contractility and heart rate more than Halothane
– Less sensitization of myocytes to exogenous catecholamines
– Metabolism 1/10th that of Halothane—less hepatotoxic
– Rare cases of fluoride toxicity (hyperthyroid, rifampin) Nephrogenic diabetes insipidus
Side effects – Similar to other fluorinated agents
– Epileptiform EEG at deep levels Avoid in patients with seizure d/o

14
Isoflurane
Nonflammable
Properties similar to Halothane and
Enflurane
Pungent odor
Less soluble than Halothane/Enflurane,
more rapid induction/recovery
MAC=1.3%

15
Sevoflurane
Fluorinated ether compound
Similar properties to other fluorinated agents
Mild respiratory/cardiac depression
Not bronchoirritant
Rapid onset/offset secondary to low lipid solubility
As enflurane, may cause renal and hepatic side effects

16
Desflurane
Newer agent
Low blood and lipid solubility with rapid
onset/offset
High incidence of bronchoirritation with
cough, laryngeal spasm, breath holding
Minimal metabolism resulting in few side
effects

17
Intravenous Anesthetic Agents
Barbiturates/other
– Thiopental
– Etomidate
– Ketamine
– Propofol
– Benzodiazepines
Narcotic agonists (opiods)/antagonists

18
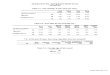
Thiopental
Barbiturate with alkaline formulation. May cause severe complications if extravasation or intraarterial injection occurs.
Unconsciousness within 10-15 seconds
Depresses neuronal activity—may decrease ICP
Poor analgesic
Varied effect on cardiovascular system
Decreased ventilatory drive, short period of apnea after bolus
Short duration secondary to rapid redistribution
Metabolized in liver

19
Thiopental distribution

20
Etomidate
Onset, elimination, ability to produce unconsciousness similar to Thiopental
Short duration of action secondary to rapid redistribution
Less cardiopulmonary depression
Can cause local pain and myoclonic movements with injection
Cortisol suppression and Addisonian crises reported in debilitation patients

21
Ketamine
Similar in structure to PCP
Dissociative anesthesia, intense analgesia, amnesia
Slow nystagmus with eyes open
Systemic effects similar to sympathetic stimulation
Respiratory function not depressed, airway protection not effected
Rapid onset, lasts 10-15 minutes
Side effect is unpleasant dreams/hallucinations during emergence. Benzodiazepines shown to decrease this.

22
Propofol
Substituted phenol
Rapid onset, short duration (metabolized)
Dilates peripheral vasculature leading to
decreased blood pressure—may be significant
in patients with blunted sympathetic response
Short period of apnea after administration
Venous irritation

23
Benzodiazepines
Good for amnesia/sedation—via potentiation at GABA receptors
Diazepam onset 2-3 minutes (IV), Lorazepam (Ativan) onset 10-15 minutes, both have long half-life (Diazepam (Valium)<Lorazepam)
Pain with injection (except midazolam)
Midazolam (Versed) 2x more potent than diazepam
Can depress respiration when used with opiods
Flumazenil is antidote

24
Narcotic agonists/antagonists
Analgesia, dpressed sensorium, respiratory depression
Effects are dose-related
Minimal cardiovascular effects, though vasodilatory effects can be serious in patients with hypovolemia
Side effects include bradycardia (doesn’t usually effect output), n/v, chest wall rigidity, seizure activity, decrease GI motility

25
Narcotics
Several receptors – Mu: analgesia, respiratory depression, euphoria,
dependance
– Kappa: spinal analgesia, sedation, meiosis
– Omega: hallucinations, dysphoria, tachycardia
Meperidine, Morphine, Fentanyl, Sufentanil, Remifentanil
Nalorphine: agonist/antagonist—less analgesia, less respiratory depression
Naloxone: reverses analgesia/respiratory depression (30 minutes)

26
Muscle Relaxants
Used clinically since 1940’s. 1960’s led to
the “balanced anesthesia” concept.
Important to provide motion-free surgical
field
Work at neuromuscular junction
Nondepolarizing vs. Depolarizing
– Competitive inhibition of endplate nicotinic
receptor vs. receptor binding with
depolarization

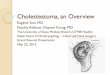
27
Paralytic agents--Anatomy

28
Neuromuscular junction

29
Depolarization

30
Nondepolarizing Agents
Bind to and competitively inhibit end-plate nicotinic receptors
Intermediate-acting (15-60 minutes) – Atracurium, vecuronium, mivacurium
– Relatively independent of renal function for clearance
– Less circulatory effect
Long-acting (>60 minutes) – Pancuronium, metocurine, d-tubocurarine, gallamine
– More hemodynamic effects
– Tubocurarine blocks autonomic ganglia, may cause mast cell degranulation
– Pancuronium inhibits vagal and muscarinic receptors and produces tachycardia

31
Reversal of Muscle Relaxation
Effect is reversed when the ratio of ACh at the NMJ is increased
Neostigmine, edrophonium, acetylcholine (anticholinesterases)
Reversal agents can cause bradycardia by stimulation of heart muscarinic receptors
Preadministration of muscarinic blockers are effective in avoiding this side effect (atropine, glycopyrrolate)

32
Depolarizing Muscle Relaxants
Bind to and depolarize end-plate ACh nicotinic receptors
The depolarization continues as long as receptor is occupied
Typically short duration of effect as drug is hydrolysed by plasma cholinesterases
Patients with abnormal cholinesterase are at risk for prolonged paralysis
Sustained depolarization produces transient fasiculations which can result in postoperative myalgias and extravasation of potassium in patients with damaged myocytes. Prior administration of low-dose non-depolarizing paralytic can attenuate incidence

33
Succinylcholine
Only depolarizing paralytic used clinically
Sinus bradycardia, junctional arhythmias, even sinus arrest can follow administration—likely secondary to muscarinic receptors on heart (blocked with atropine)
Increased intraocular pressure, intragastric pressure, trismus reported.
Malignant hyperthermia

34
Rapid-Sequence Induction
Preoxygenation
Anesthesia-inducing drugs (barbiturates,
benzodiazepines, opiods, etomidate,
ketamine, or propofol)
Succinylcholine
Intubation

35
Local Anesthetics
Reversibly inhibit the generation and conduction of impulses from a particular area of the body
Effect is secondary to conduction blockade by decreasing permeability of nerve membranes to sodium
Binds to sodium channel and blocks it
All but cocaine are vasodilators and therefore usually are mixed with epinephrine
Ester/Amide family of drugs
Esters metabolized by plasma cholinesterase, amides metabolized by liver p-450 system

36
Local Anesthetics

37
Local Anesthetics
Lipophilic/hydrophilic ends
Non-ionized form crosses membranes
more readily
– Drugs have less effect in acidic environment
(infection)
– Addition of HCO3 to acidic preparations may
increase potency and decrease pain

38
Local Anesthetics

39
Local Anesthetic Injection –
The Target

40
Local anesthetic injection - Otologic

41
Local anesthetic - Intranasal

42
Local Anesthesia - Maxilla

43
Local Anesthesia -
Mandible

44
Nontraditional Anesthesia Acupuncture – Acupuncture with electrical stimulation gave 50-65% decrease in
opiod use, decreased PCA use time, and decreased N/V after intraabdominal surgery (Wang, 1997, Hamza, 1999, Kotani, 2001)
– Decreased N/V after tonsillectomy in adults (NIH consensus, 1998)
– Pain control antagonized by naloxone (Sjolund, 1979)
– Thought to stimulate large nerve fibers which changes pain perception in the spinal cord transmitted by small fibers. Endorphins also increased.
Acupressure
TENS (transcutaneous electrical nerve stimulation) – 10-30% reduction in post-op pain and need
for analgesics (Tyler, 1982)
Capsiacin
Hypnosis

45
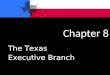
Tidbits, odds
& ends
Malampatti
classification
Thyromental distance
Grading the intubation
view
SP system
Closed system
anesthesia
6.5cm

46
Anesthesiology
Glen T. Porter, MD
Faculty Advisor: Francis B. Quinn, MD, FACS
The University of Texas Medical Branch
Department of Otolaryngology
Galveston, Texas
June 2004