Embed Size (px)
Citation preview
Anna C. Wilson, PhD
Assistant Professor
Anesthesiology and Perioperative Medicine
Overview� Background and theory
� Chronic pain in adolescence� Fear-avoidance beliefs in adolescence � Parent factors in adolescent chronic pain
� Aims and methods of current study
� Results and conclusions� Future directions
Chronic and Recurrent Pain is a
Significant Pediatric Health Problem
� 20-40% of children and adolescents in community samples experience persistent pain (Perquin et al., 2000; Stanford et al., 2008)
� More severe persistent pain in 8%� Pain accompanied by moderate to severe disability in
5% (Huguet & Miro, 2008)
� Most common locations: head, abdomen, limbs
� Multiple pains are common
� More commonly reported in girls than boys� Peak incidence: ages 14-15 years (Stanford et al., 2008)
� Comorbid anxiety and depression common

Fear-avoidance beliefs
� Cognitions (thoughts and beliefs) about pain being linked to physical activity or movement
� “Physical activity makes my pain worse” or “I cannot do movements that make my pain worse”
� Fear-avoidance beliefs are related to higher levels of pain and disability: Well-supported in adults with chronic low back pain (e.g., Jensen et al., 2001; Poiraudeau et al., 2006)
� Few measures of fear-avoidance beliefs that have been used in children and adolescents

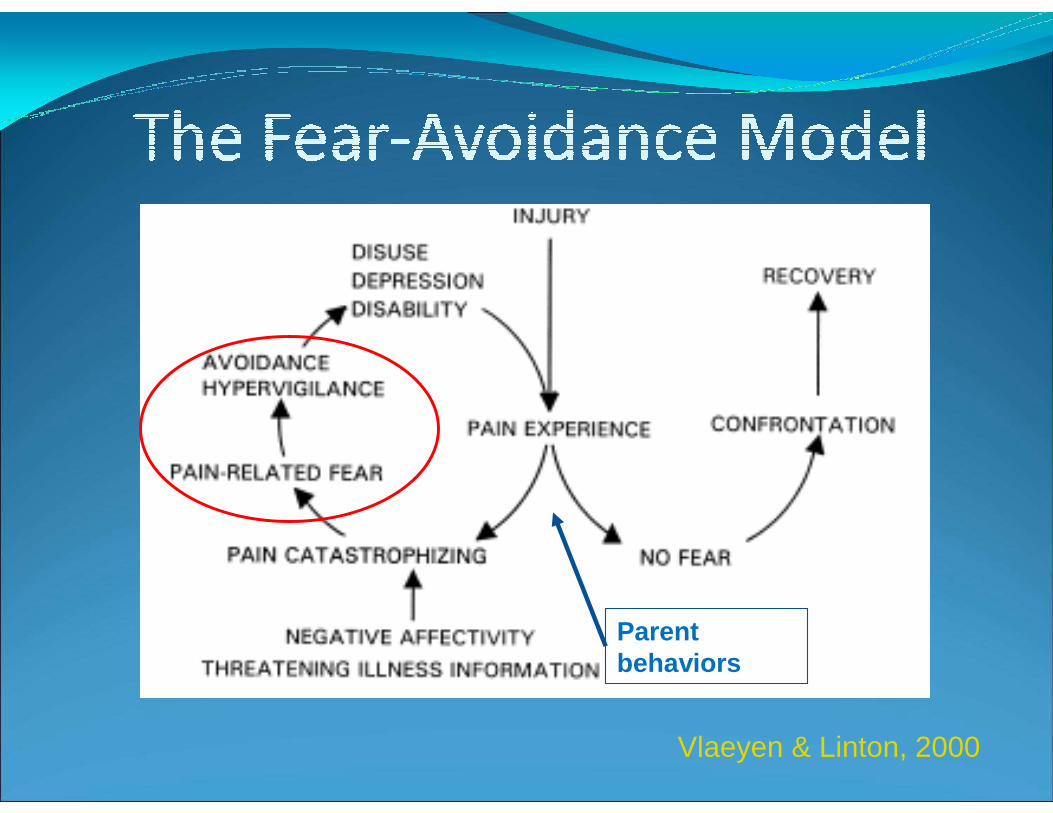
Vlaeyen & Linton, 2000

� Cognitions and avoidance behaviors develop within a family context
� Parental responses to child pain may influence cognitions about pain, including fear-avoidance
� Children and parents play a role in appraising or judging pain to be more or less threatening
Vlaeyen & Linton, 2000
Parent behaviors

� Specific parent responses to child pain behaviors may serve to inadvertently reinforce or encourage pain behaviors
� Protective or solicitous responses to child pain associated with higher pain intensity and disability (Claar et al., Pain, 2008; Chambers et al., J Ped Psych, 2002)
� Behaviors include: � Frequent attending to pain symptoms
� Allowing activity withdrawal from less preferred activities (e.g., chores, school attendance)
� Giving special privileges or rewards

� 1. Describe fear-avoidance beliefs and correlates in a sample of adolescents with chronic pain
� 2. Examine fear-avoidance beliefs and depressive symptoms as predictors of disability
� 3. Test fear-avoidance beliefs as a potential moderator and mediator of parental protectiveness

� n = 42 adolescents with chronic pain (pain 1x/wk or more, present for >3 months), recruited through outpatient pediatric specialty care clinics at a university children’s hospital (pain clinic, gastroenterology, neurology)� Abdominal pain (n = 23)
� Headache (n = 11)
� Musculoskeletal pain (n = 8)
� 11-17 years old, Mean age 14.90 (SD = 2.11)� 73.8% female
� 88.1% Caucasian; 7.1% Hispanic; <3% other ethnicity
� Mean annual family income $50-69K

� Pain characteristics
� Usual pain intensity, 0-10 NRS
� Pain frequency in last 3 months
� Fear and Avoidance Beliefs Questionnaire –Physical Activity 5-item subscale (FABQ-PA; Waddell et al., 1993)
� Depressive Symptoms: 10-item Major Depressive Disorder subscale of Revised Children’s Anxiety and Depression Scale (RCADS; Chorpita et al., 2005)

� Parental Protectiveness: Adult Responses to Children’s Symptoms 15-item Protect subscale (Van Slyke & Walker, 2006)� Item examples: “When your child has aches and
pains, how often do you…pay more attention than usual to your child; give your child special privileges; bring your child special treats or little gifts”
� Physical Activity Limitations: Child Activity Limitations Interview (CALI; Palermo et al., 2004)� Assesses difficulty doing physical and routine
activities because of pain

Variable M (SD)
Pain Intensity (0-10) 6.57 (1.74)
Depressive Symptoms 55.98 (13.50)
Disability (CALI): Adolescent Report
19.86 (6.19)
Disability (CALI): Parent report
21.05 (6.09)
Parental Protectiveness 1.79 (.51)

� Adolescents reported moderate levels of fear-avoidance (FABQ-PA, M = 11.52)
� Slightly lower than samples of adults with chronic low back pain (FABQ-PA, M = 14.0-14.2)
� FABQ-PA had slightly low internal consistency: Chronbach’s alpha = .69

� As hypothesized, the FABQ-PA was significantly correlated with:
� Parent-report disability (r = .42, p < .01)� Child-report disability (r = .44, p < .01)
� Parental protectiveness (r = .47, p < .01)
� FABQ-PA was not related to:
� Depressive symptoms� Usual pain intensity
� Pain location


CALI: Child report CALI: Parent report
∆R2β at final
step ∆R2β at final
step
Step 1:
Household Income
Usual Pain Intensity
.38***
-.23
.47***
.08
.09
.23
Step 2:
Depressive Symptoms
.00
-.03
.02
.05
Step 3:
Fear-avoidance Beliefs
.16**
.42**
.17**
43**
Total R2: .54*** .27*
* p < .05, ** p < .01, *** p < .001

� Tested two models: fear-avoidance as a moderator and as a mediator
Parental
Protectiveness
Child Activity
Limitations
Fear-Avoidance
Beliefs

� Tested two models: fear-avoidance as a moderator and as a mediator
Parental
Protectiveness
Child Activity
Limitations
Fear-Avoidance
Beliefs

� Tested two models: fear-avoidance as a moderator and as a mediator
Parental
Protectiveness
Child Activity
Limitations
Fear-Avoidance
Beliefs

� Results: No support found for moderation model� The association between protectiveness and activity
limitations is not altered by child fear-avoidance
Parental
Protectiveness
Child Activity
Limitations
Fear-Avoidance
Beliefs
.29*
n.s.
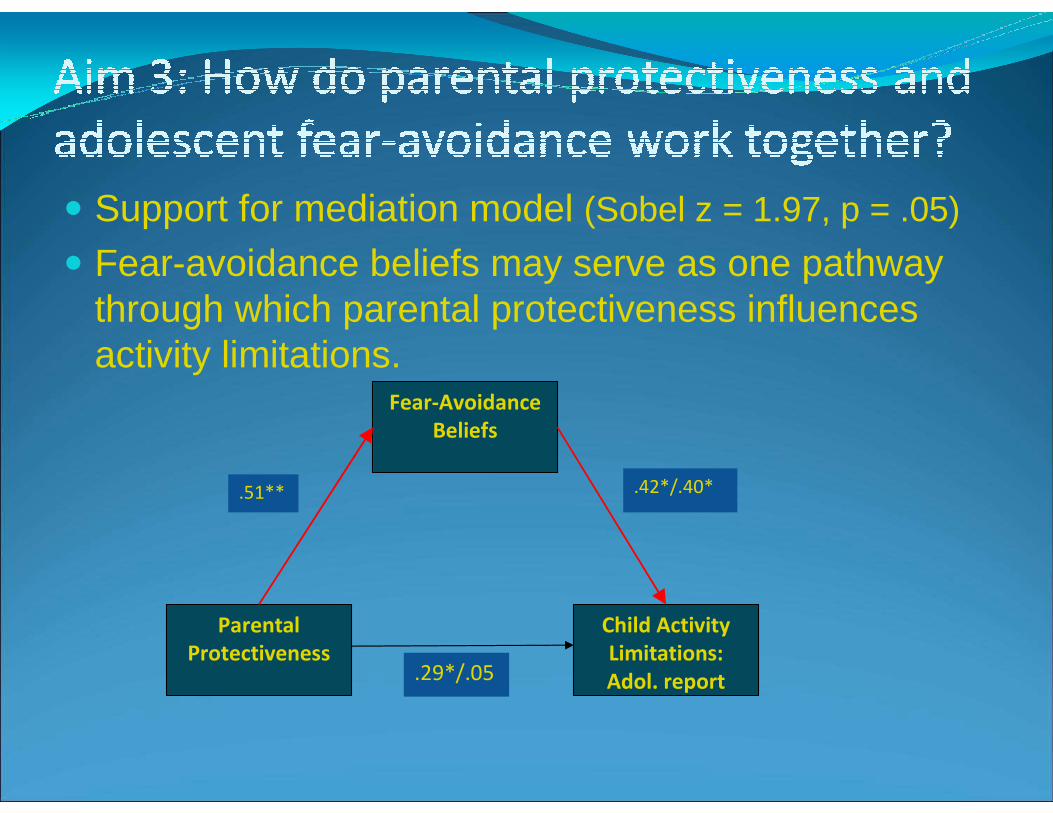
� Support for mediation model (Sobel z = 1.97, p = .05)
� Fear-avoidance beliefs may serve as one pathway through which parental protectiveness influences activity limitations.
Parental
Protectiveness
Child Activity
Limitations:
Adol. report
Fear-Avoidance
Beliefs
.51** .42*/.40*
.29*/.05

� As in adult chronic pain populations, fear-avoidance beliefs play an important role in adolescent disability
� Fear-avoidance beliefs seem to be important for adolescents with a variety of pain problems
� Fear-avoidance beliefs may be less tied to depressive symptoms and pain intensity in adolescents than in adults
� Parental behaviors in response to adolescent pain may influence adolescent cognitions and fears which in turn increase activity limitations

� Strengths:� Associations demonstrated across reporters
(adolescent and parent)
� Fear-avoidance beliefs examined in a mixed pain problem sample (not only back or musculoskeletal pain)
� Limitations:
� Cross-sectional study limits our ability to draw conclusions about the direction of these effects
� Relatively small sample limited power to detect moderation
� Did not examine anxiety symptoms
� Examine role of parental behaviors and cognitions in shaping adolescent cognitions over time
� Examine additional parental behaviors and beliefs:
� Parent catastrophizing about their child’s pain� Parent modeling of pain behaviors
� Enhance understanding of how adolescent fear-avoidance beliefs relate to other pain-related cognitions such as catastrophizing
� Both parent behaviors and adolescent fear-avoidance cognitions may be potential intervention targets

� Pediatric Health Pilot Project (PI: Wilson): Oregon Clinical and Translational Research Institute (OCTRI), grant # UL1 RR024140 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research
� Colleagues and collaborators:
� Tonya Palermo, PhD
� Amy Lewandowski, PhD� Caitlin Murray, BA





























