Embed Size (px)
Citation preview

In the Name of Allah Most Merciful Most Compassionate

Sherif M El Hadi MDAnaesthesia Department
Faculty of Medicine
Alexandria
Anaesthesia for Interventional Neuroradiology

Development of Interventional Neuroradiology (INR)
New imaging
technology
Catheter systems
Detachable balloons,
coils
Vascular embolic
agents

Method
Digital road map is created Vascular system is imaged by
angiographic dye Projected onto a live fluoroscopy image Bone and soft tissue has been
subtracted (DSA) Accessed typically through the femoral
system

Method
Systemic heparinization Catheter system is advanced under
direct visualization into the cerebrovascular system
Superselective catheter advanced into the vessels to be treated


Indications of INR
Selective occlusion Aneurysm ablation-GDC coiling Endovascular embolization of AVM Sclerotherapy of venous angiomas

Indications of INR
Selective increase in blood flow Balloon angioplasty Thrombolysis of acute stroke Carotid angioplasty with stent
Arterial delivery: Chemotherapy or embolic in tumor

Preoperative Assessment
Allergies Contrast media reaction
5%-8% incidence of untoward systemic reactions
Allergies to Iodine and shellfish Protamine

Preoperative Assessment
Medications Anticoagulation Antihypertensive Anticonvulsants Blood sugar control

Preoperative Assessment
Cardiovascular and pulmonary history
Neurological history Physical exam
Impaired consciousness favors General Anaesthesia

Transportation
Guiding the medical management of critical patients during transport to and from the
radiology suites

Transport of Patient
Emergency Room
Intensive Care Unit
Operating Theatre
Radiology Suite

Anesthetic Objectives (1)
Maintenance of patient immobility and physiologic stability
Manipulating systemic or regional blood flow ..

Anesthetic Objectives (2)
Managing anticoagulation Treating and managing sudden
unexpected complications during the procedure
Rapid recovery from anesthesia to facilitate neurological evaluation..

Radiation exposure
Exposure decreases proportionally to the square of the distance from the source of the radiation
Digital subtraction angiography (DSA) delivers more radiation than fluoroscopy
Optimal protection-apron, thyroid shield, communication ..

Anaesthetic Technique
Intravenous Sedation Goals are to alleviate
Pain (introduction of contrast/prolonged immobilization, distention or traction on cerebral arteries)
Anxiety (if high risk of bad outcome) Discomfort (prolonged immobility)

Anaesthetic Technique
Intravenous Sedation (continued) Patient immobilty Rapid recovery to allow neurologic
examination Be prepared to secure the airway Various techniques, propofol
infusion ..


Mild Sedation Moderate Deep Sedation
Increasing sedative dose
DANGER

Dangers of IV sedation
Poor control of the airway, potential: •Hypoxia •Hypercapnia•Stertorous breathing and aspiration
Side effects of IV sedatives•Dysphoria•Prolonged somnolence•Extrapyramidal symptoms

Benefits of IV sedation
Techniques needing cooperation of patient
The Wada test before occlusion of a vessel

Wada test
It judges which hemisphere is dominant for specific function.
e.g. If speech arrest or other language impairment (dysphasia, paraphasia) were observed immediately following drug injection into one hemisphere, then the injected side was judged to be dominant for language.

Wada test using propofol For the Wada test, a solution of
propofol dispensed at a concentration of 1mg/ml in 10 mL of saline.
The dose of propofol ranges from 10- 17 mg/ bolus enough for producing transient contralateral hemiplegia and aphasia

General Anaesthesia

Rationale for general anesthesia
Improved images Airway control in the supine position Induced hypotension facilitated Improved control of elevated ICP Augmentation of blood pressure with
occlusive disease Facilitating rescue operations

Propofol
No accumulation with prolonged useTIVA – rapid BP control
Antiemetic (short-lived) Inhibition of airway reflexes Permits SSEP and MEP monitoring.

Zone of ischaemia
CBFPropofol
Propofol + hypocapnia

Opioids
Decreased CMRO2 (Max. 35%)
Decreased CBF with higher doses
(Max. 50%)
Depressed airway reflexes
Autonomic tolerance to noxious
stimuli.

Problems
Muscle RigidityHypotension Increased ICP???

Nitrous oxide:
Vacuolation of mitochondria and cytoplasmic reticulum of posterior cingulated gyri of rats after nitrous oxide.Jetovic-Todorovic. Nature 1998.

Nitrous oxide:
Thiopentone, isoflurane increase survival time in mice if given before exposure to ischaemia
Nitrous oxide eliminates this protective effect
N2O alone decreases survival time.

Nitrous oxide:
Protein synthesis: Cytoskeletal proteins damage ↑ Pro-apoptotic proteins when used
with isoflurane, midazolam and ketamine.

Halothane
CMRO2
Concentration
1 MAC 2 MAC 3 MAC
Min. metabolic rate to
maintain membrane
integrity

Sevoflurane and Desflurane
Speedier recovery than isoflurane Low solubility in blood and tissues
rapid recovery Desflurane increases BP and HR on
induction

Sevoflurane and Desflurane
Effect on ICP Desflurane > isoflurane > sevoflurane
BUT
Differences disappear with hyperventilation
Holmstrom A. J Neurosurg Anesthesiol. 2004

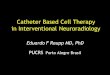
Intracranial aneurysm ablation

Intracranial aneurysm ablation

Intracranial aneurysm ablation

Intracranial aneurysm ablation
Complications Distal thromboembolism Rupture Recurrence and hemorrhage
(incomplete obliteration) No guarantee the aneurysm is
removed from the circulation. BP control essential


Seven coils to obliterate aneurysm

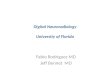
Vasospasm
Larger arteries: balloon angioplasty, Small arteries:
Intraarterial vasodilators Papaverine: hypotension, ↑ ICP,
worsened vasospasm, seizures Nimodipine (Biondi 2004) Nicardipine (Badjatia, 2004)

Effect of angioplasty on spastic segment

AV malformation
Before surgical resection or solely treated by embolization
Factors leading to rupture: High feeding artery pressure Draining stenosis
Potential risk of cerebral edema after embolization of AVM Steroid pretreatment and fluid
restriction

Carotid artery stenting
Bradycardia and hypotension: 7% (Mlekusch, 2004) Anticholinergic agents Prophylactic transvenous pacemaker
inserted Thromboembolism, dissection, TIA,
stroke


Thank You